Mar 3, 2026

Tired of conflicting information about tirzepatide alternatives? You are not alone. Thousands of people find themselves searching for another option, whether because of side effects, supply shortages, cost, or simply because tirzepatide did not work the way they expected. The frustrating part is that most "alternatives" articles give you a list of drug names with no real comparison data, no switching protocols, and no honest assessment of what actually works.
That changes here.
This guide breaks down every meaningful tirzepatide alternative available right now, from FDA-approved GLP-1 receptor agonists to non-GLP-1 prescription medications, from pipeline drugs showing remarkable clinical trial results to natural compounds with growing research behind them. We cover the clinical data, the mechanisms, the realistic weight loss expectations, and the practical considerations that actually matter when choosing an alternative. Whether you need to switch from tirzepatide to semaglutide, explore emerging options like orforglipron, or find something entirely different, every option worth considering is covered in the sections that follow.
SeekPeptides tracks these developments closely, and members get access to detailed protocol comparisons and switching guides that go far beyond what any single article can cover.
Why people look for tirzepatide alternatives
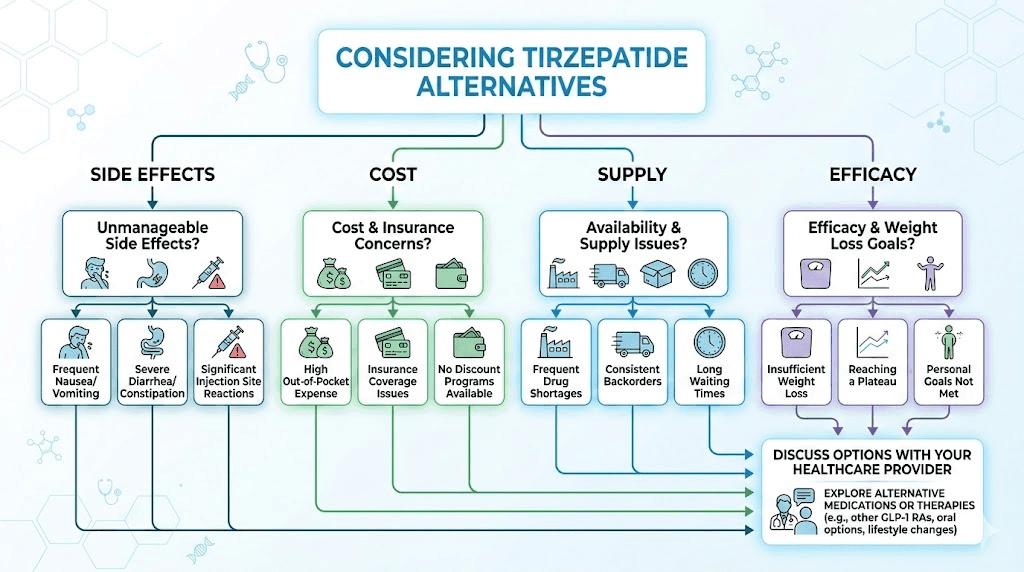
Before diving into the alternatives themselves, it helps to understand why someone might need one. The reason matters because it changes which alternative makes the most sense.
Side effects that do not resolve. Tirzepatide works through dual GIP and GLP-1 receptor activation, which makes it exceptionally effective. But that dual mechanism also means more potential for gastrointestinal side effects. Some people experience persistent constipation, diarrhea, headaches, or body aches that never fully subside, even after months of dose titration. For these individuals, a single-receptor GLP-1 agonist like semaglutide often produces fewer side effects while still delivering meaningful weight loss.
Cost is another major driver. Brand-name Zepbound and Mounjaro carry substantial price tags without insurance coverage. The FDA decision on compounded tirzepatide availability added more uncertainty. People who were paying $250 to $400 per month for compounded versions suddenly found themselves facing brand-name prices of $1,000 or more. That is a deal-breaker for many.
Then there are supply issues. Tirzepatide has faced intermittent shortages since its launch, and some dosage strengths become unavailable for weeks at a time. When you are on a weight loss timeline and your medication disappears, you need a backup plan.
Some people hit a plateau where tirzepatide stops working. Others discover they cannot tolerate injections and want an oral alternative. Some have medical conditions that make tirzepatide inappropriate, such as a personal or family history of medullary thyroid carcinoma. And some are simply curious whether something newer or better has come along.
Whatever the reason, the landscape of alternatives has never been broader. Let us walk through them systematically.
FDA-approved GLP-1 alternatives
The most direct alternatives to tirzepatide are other FDA-approved GLP-1 receptor agonists. These share a similar mechanism of action, though with important differences in how they work and what results they produce.
Semaglutide (Wegovy, Ozempic)
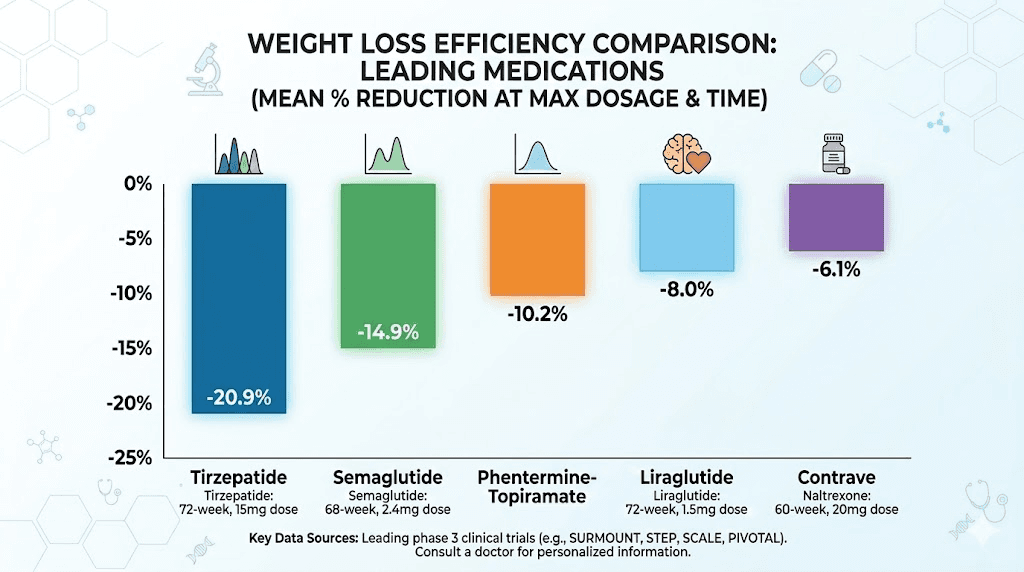
Semaglutide is the closest competitor to tirzepatide and the most commonly chosen alternative. It works as a pure GLP-1 receptor agonist, meaning it targets only one of the two receptors that tirzepatide activates. In head-to-head comparisons, the semaglutide vs tirzepatide data shows tirzepatide produces slightly more weight loss on average, about 17.8% body weight reduction at the highest dose compared to 13.9% for semaglutide 2.4 mg over 72 weeks. But that average gap does not tell the full story.
Some individuals respond better to semaglutide than tirzepatide. The side effect profiles differ meaningfully. Semaglutide tends to cause less nausea at equivalent therapeutic doses in some patients, and the dosing schedule is straightforward with well-established titration protocols.
A major development: oral semaglutide (Wegovy tablets) received FDA approval in late 2025, producing average weight loss of 13 to 14% of body weight in daily tablet form. That is a game-changer for people who want the benefits of a GLP-1 agonist without injections. Our guide on oral semaglutide drops covers the delivery options in detail.
For researchers looking at compounded semaglutide, this remains more widely available than compounded tirzepatide following the FDA regulatory changes. The cost difference is significant, often $150 to $300 per month for compounded versions versus $1,300 or more for brand-name Wegovy.
Key data points for semaglutide as a tirzepatide alternative:
Average weight loss: 13.9% to 16% of body weight over 68 to 72 weeks
Mechanism: GLP-1 receptor agonist only (single target)
Delivery: Weekly injection or daily oral tablet
Appetite suppression onset: Most users notice reduced hunger within the first 1 to 2 weeks
Time to meaningful results: 4 to 8 weeks for noticeable weight loss
If you are considering making the switch, our tirzepatide to semaglutide conversion chart provides the exact dosing equivalencies your provider will need.
The typical semaglutide titration protocol for weight management starts at 0.25 mg weekly for four weeks, then increases to 0.5 mg for another four weeks, followed by 1.0 mg, 1.7 mg, and finally 2.4 mg, each for four-week periods. This five-step escalation over 16 to 20 weeks allows the body to adjust gradually, minimizing the gastrointestinal effects that cause most people to abandon treatment. The semaglutide dosage chart in units and syringe dosage chart make this process easier for those using compounded versions.
One detail that matters enormously: timing. Research on the best time of day to take semaglutide suggests consistency matters more than the specific hour, but many users report fewer nausea issues when injecting in the evening. If you are switching from tirzepatide, keeping the same injection day of the week simplifies the transition and helps maintain a routine.
For those using compounded semaglutide, understanding the different concentrations is essential. A 5 mg vial requires different injection volumes than a 10 mg vial. The units-to-mg conversion guide and concentration-specific charts for 5 mg/2 mL and 5 mg vial formats prevent dosing errors that can either waste medication or cause unnecessary side effects.
What about long-term efficacy? The STEP trials showed that weight loss with semaglutide continues to accumulate through 68 weeks, with most patients reaching a plateau around 60 to 68 weeks at the 2.4 mg dose. This is slightly shorter than the typical response curve with tirzepatide, where weight loss often continues through 72+ weeks. But the difference in the long-term trajectory is less dramatic than the peak weight loss numbers suggest. Many patients who plateau on one medication see renewed progress when switching to another, which is one reason physicians rotate between GLP-1 options for long-term management.
Liraglutide (Saxenda, Victoza)
Liraglutide was the first GLP-1 receptor agonist approved specifically for weight management under the brand name Saxenda. It requires daily injections rather than weekly, which many people consider a drawback. But there are scenarios where liraglutide makes sense as a tirzepatide alternative.
The daily dosing actually provides more granular control. If you are highly sensitive to GLP-1 agonists and experienced severe side effects on tirzepatide even at the lowest dose, liraglutide allows you to titrate in smaller increments over a longer period. Some physicians use this approach for patients who could not tolerate tirzepatide or semaglutide at any dose.
Average weight loss with liraglutide runs about 5 to 8% of body weight, which is notably less than both tirzepatide and semaglutide. That makes it a less attractive first-choice alternative for pure weight loss. However, it has the longest safety track record of any GLP-1 agonist used for weight management, with data going back over a decade.
Liraglutide also has established cardiovascular benefit data, reducing major adverse cardiovascular events in the LEADER trial. For someone choosing a tirzepatide alternative specifically because of cardiovascular concerns, this track record matters.
Dulaglutide (Trulicity)
Dulaglutide is FDA-approved for type 2 diabetes, not specifically for weight management, but it does produce moderate weight loss as a side effect. Average weight reduction runs about 3 to 5% of body weight, making it the least effective GLP-1 option for pure weight loss purposes.
Where dulaglutide has value as an alternative is in its injection device. The Trulicity pen is widely considered the easiest GLP-1 injector to use, with a hidden needle that many injection-anxious patients prefer. It also has strong cardiovascular outcome data from the REWIND trial.
Realistically, dulaglutide is not a strong tirzepatide alternative for weight loss. But for someone with type 2 diabetes who cannot tolerate tirzepatide and needs a proven A1C reducer with some weight loss benefit, it fills a specific niche.
Exenatide (Byetta, Bydureon)
Exenatide was the first GLP-1 receptor agonist approved in the United States, and it still has a place in the landscape. Byetta requires twice-daily injections, which most people find impractical. Bydureon BCise is the extended-release version given once weekly.
Weight loss with exenatide is modest, typically 3 to 5% of body weight. Where it occasionally serves as a tirzepatide alternative is in specific insurance situations. Some insurance plans cover exenatide but not newer GLP-1 agonists, making it the only accessible option for certain patients. Its shorter half-life also means it clears the system faster if side effects occur, which some physicians prefer for patients who had severe reactions to longer-acting agents like tirzepatide or semaglutide.
How GLP-1 alternatives compare on key metrics
Beyond raw weight loss numbers, several factors differentiate these GLP-1 alternatives in practice. Time to onset varies: semaglutide typically produces noticeable appetite suppression within 1 to 2 weeks, while liraglutide may take slightly longer due to its lower dose titration starting point. The best timing for GLP-1 shots is consistent across all injectable alternatives, just pick a day and stick with it.
A1C reduction for those with type 2 diabetes also varies. Tirzepatide leads with up to 2.4% A1C reduction at the highest dose. Semaglutide achieves about 1.5 to 1.8% reduction. Liraglutide and dulaglutide typically produce 1.0 to 1.5% reductions. If A1C management is your primary goal with weight loss as secondary, these differences matter significantly.
Cardiovascular outcomes data is strongest for liraglutide (LEADER trial) and semaglutide (SELECT trial), with semaglutide showing a 20% reduction in major adverse cardiovascular events in people with established cardiovascular disease and overweight or obesity. Tirzepatide cardiovascular outcome data from the SURPASS-CVOT trial is expected soon but not yet published. This gap in the evidence is relevant for anyone whose healthcare provider prioritizes proven cardiovascular protection.
Non-GLP-1 prescription alternatives
Not everyone can take, or wants to take, a GLP-1 receptor agonist. The good news is that several non-GLP-1 medications offer legitimate weight management benefits through entirely different mechanisms. These can also be combined with GLP-1 agonists in some cases, creating a combination approach that addresses multiple pathways.
Phentermine and topiramate (Qsymia)
This combination medication works through two distinct mechanisms. Phentermine is a sympathomimetic amine that suppresses appetite by increasing norepinephrine and dopamine in the brain. Topiramate is an anticonvulsant that also reduces appetite and increases satiety, though its exact weight loss mechanism is not fully understood.
The combination produces average weight loss of 7 to 10% of body weight over one year, which is less than tirzepatide but meaningful. Our detailed comparison of phentermine vs tirzepatide breaks down exactly when each option makes more sense.
One significant advantage: Qsymia is available in oral form and has been on the market since 2012. It is well-understood, relatively affordable compared to GLP-1 agonists, and works through a completely different pathway. For someone who cannot tolerate any GLP-1 medication, phentermine is not a GLP-1, it targets entirely different receptors, making it suitable for people who had adverse reactions to the GLP-1 class.
Some physicians prescribe phentermine alongside tirzepatide or alongside semaglutide to enhance appetite suppression, though this combination approach requires careful medical supervision.
Downsides include potential cardiovascular effects (increased heart rate, elevated blood pressure), insomnia, dry mouth, and the stimulant properties of phentermine that make it unsuitable for people with certain heart conditions or anxiety disorders. Topiramate can cause cognitive effects, including difficulty with word-finding and concentration, which some people find unacceptable. The medication is also teratogenic, meaning it can cause birth defects, and requires reliable contraception during use. Women planning pregnancy in the near future should not use Qsymia. For a comprehensive phentermine vs GLP-1 comparison, our guide covers every dimension of the decision.
Bupropion and naltrexone (Contrave)
Contrave combines two well-known medications. Bupropion is an antidepressant and smoking cessation aid. Naltrexone is an opioid antagonist used in addiction medicine. Together, they target the reward system in the brain, reducing food cravings and the emotional component of eating.
Average weight loss with Contrave is about 5 to 6% of body weight, which is modest compared to tirzepatide. But this medication addresses something that GLP-1 agonists do not directly target: reward-driven eating. If your weight management challenge is more about emotional eating, food cravings, and behavioral patterns rather than pure appetite, Contrave may address the root issue more effectively than any GLP-1 agonist.
It is an oral medication taken twice daily, which some prefer over injections. The most common side effects are nausea, constipation, headache, and insomnia. Unlike GLP-1 agonists, it does not affect gastric emptying, so the gastrointestinal side effects tend to be milder.
Orlistat (Xenical, Alli)
Orlistat works through a completely different mechanism. Rather than affecting appetite or satiety hormones, it blocks the absorption of about 30% of dietary fat by inhibiting pancreatic lipase in the gut. The unabsorbed fat passes through the digestive system.
Average weight loss is about 3 to 5% of body weight. The mechanism is straightforward and does not interact with GLP-1 pathways at all, making it safe to use for people who had severe reactions to tirzepatide or other incretin-based therapies.
The significant downside is the gastrointestinal effects of unabsorbed fat: oily stools, flatulence, fecal urgency, and potential fecal incontinence if dietary fat intake is too high. These effects are directly tied to fat consumption, which some view as a built-in behavioral modification tool.
Alli, the over-the-counter version, is available at half the prescription strength without a doctor visit. This makes orlistat the most accessible weight loss medication available.
Metformin
Metformin is not FDA-approved for weight loss, but it produces modest weight reduction in many patients and is frequently prescribed off-label for weight management, particularly in people with insulin resistance or prediabetes. Some researchers combine metformin with tirzepatide for enhanced metabolic effects.
Average weight loss with metformin alone is about 2 to 5% of body weight. Its primary value as a tirzepatide alternative is not in pure weight loss but in its metabolic benefits: improved insulin sensitivity, reduced fasting glucose, and potential longevity effects that are currently being studied. It is also one of the most affordable prescription medications available, often costing under $10 per month.
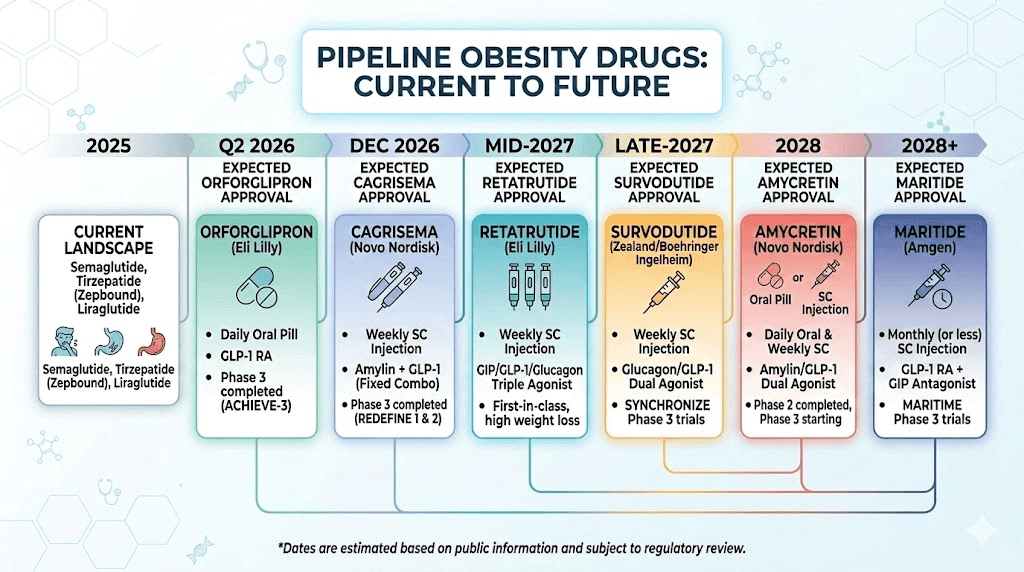
Emerging alternatives in the pipeline
The next generation of weight management medications is remarkably promising. Several candidates in phase 2 and phase 3 clinical trials are showing weight loss that matches or exceeds tirzepatide. Understanding these pipeline options helps you plan ahead and have informed conversations with your healthcare provider about what might be available soon.
Retatrutide (the triple agonist)
If tirzepatide is a dual agonist (GLP-1 plus GIP), retatrutide is its more ambitious successor: a triple agonist that activates GLP-1, GIP, and glucagon receptors simultaneously. This additional glucagon receptor activation drives increased energy expenditure and fat oxidation, something neither tirzepatide nor semaglutide directly provides.
The clinical data is striking. Phase 2 trials showed average weight loss of 24.2% of body weight at the 12 mg weekly dose over 48 weeks. That is the highest weight reduction ever recorded in an obesity clinical trial. Our full comparison of retatrutide vs tirzepatide and the three-way comparison with semaglutide cover the clinical data in depth.
Retatrutide is currently in phase 3 trials, with Eli Lilly (the same company behind tirzepatide) running the program. Approval is not expected before late 2026 or 2027 at the earliest. The retatrutide availability timeline and projected costs are covered in our dedicated guides.
Side effects in trials have been predominantly gastrointestinal, similar to tirzepatide but with somewhat higher rates of nausea, diarrhea, and vomiting. The addition of glucagon receptor activation also raises potential concerns about increases in heart rate and blood pressure that need long-term monitoring.
For those following the research peptide space, retatrutide starting doses, dosage charts, and injection protocols are all available on SeekPeptides.
Orforglipron (oral GLP-1 from Eli Lilly)
Orforglipron represents perhaps the most exciting development in the weight loss medication landscape: a small-molecule oral GLP-1 receptor agonist that you take as a daily pill. Unlike oral semaglutide (which is a peptide that requires careful absorption management), orforglipron is a small molecule that absorbs readily without food restrictions.
Phase 3 results from the ATTAIN-1 trial showed the highest dose (36 mg) produced average weight loss of 12.4% of body weight, with about 40% of participants losing 15% or more of their body weight at 72 weeks. The ATTAIN-2 trial in people with type 2 diabetes showed 10.5% average weight loss with meaningful A1C reductions of 1.8%. And in a first-of-its-kind trial called ATTAIN-MAINTAIN, orforglipron successfully maintained weight loss in people transitioning from injectable GLP-1 medications.
That last point is particularly relevant. If you are currently on injectable tirzepatide and want to switch to an oral medication without regaining weight, orforglipron may eventually offer that pathway. Our comprehensive orforglipron vs tirzepatide comparison covers the clinical data in detail.
Eli Lilly has submitted orforglipron to the FDA for approval, with regulatory decisions expected in 2026. If approved, it would be the first oral small-molecule GLP-1 agonist for weight management, potentially transforming access for the millions of people who prefer pills over injections.
CagriSema (semaglutide plus cagrilintide)
CagriSema is the Novo Nordisk combination therapy that pairs semaglutide with cagrilintide, an amylin analog. Amylin is a hormone co-secreted with insulin from pancreatic beta cells that independently reduces appetite and slows gastric emptying. By combining GLP-1 and amylin pathways, CagriSema targets weight loss through two complementary mechanisms.
Phase 1b trials showed participants lost an average of 17.1% of their body weight over 32 weeks, which is comparable to tirzepatide. The mechanism is particularly interesting because amylin and GLP-1 affect different brain regions involved in appetite regulation, potentially producing more robust and sustained appetite suppression than either approach alone.
Our comparison of CagriSema vs tirzepatide analyzes how these two combination approaches stack up. For those interested in cagrilintide specifically, SeekPeptides maintains detailed guides on cagrilintide sourcing and dosing protocols.
Survodutide
Developed by Boehringer Ingelheim and Zealand Pharma, survodutide is a dual GLP-1 and glucagon receptor agonist. Unlike tirzepatide (which targets GLP-1 and GIP), survodutide swaps the GIP component for glucagon, which drives increased energy expenditure and fatty acid oxidation.
This is significant because it means survodutide may help with weight loss through both reduced appetite (GLP-1) and increased calorie burning (glucagon). Phase 2 data showed average weight loss of up to 18.7% at 46 weeks, putting it in competitive territory with tirzepatide.
Survodutide is currently in phase 3 trials for obesity, with additional studies examining its effects on metabolic dysfunction-associated steatohepatitis (MASH), a liver condition that affects many people with obesity. Our survodutide vs tirzepatide analysis covers the differences in mechanism and early clinical results.
Amycretin
Novo Nordisk is developing amycretin as a dual GLP-1 and amylin receptor agonist in a single molecule. Unlike CagriSema (which combines two separate drugs), amycretin is one compound that activates both pathways simultaneously.
Phase 2 results showed weight loss of up to 14.5% at 36 weeks, which is promising for a relatively short trial duration. Importantly, amycretin is being developed in both injectable and oral formulations, potentially offering another oral alternative to injectable tirzepatide. Novo Nordisk advanced amycretin to phase 3 trials in early 2026.
MariTide (maridebart cafraglutide)
Amgen is taking a fundamentally different approach with MariTide. This is a GLP-1 receptor agonist conjugated to a monoclonal antibody that antagonizes (blocks) GIP receptors. That is the exact opposite of tirzepatide, which activates GIP receptors. This deliberate contrast in approach suggests the obesity field has not yet determined whether GIP activation or GIP blockade produces better long-term outcomes.
Phase 2 data showed average weight loss of 17 to 20% of body weight over 52 weeks. The real differentiator is the dosing schedule: once every four weeks. Monthly injections rather than weekly ones could significantly improve adherence and quality of life for patients.
MariTide is currently in phase 3 trials, with Amgen positioning it as a new paradigm for obesity treatment.
Head-to-head comparison of tirzepatide alternatives
With so many options, a side-by-side comparison makes the decision clearer. This table includes both currently available medications and key pipeline candidates.
Alternative | Mechanism | Avg weight loss | Delivery | Frequency | Status |
|---|---|---|---|---|---|
Tirzepatide | GLP-1 + GIP dual agonist | 17 to 22% | Injection | Weekly | FDA approved |
Semaglutide (inj) | GLP-1 agonist | 14 to 16% | Injection | Weekly | FDA approved |
Semaglutide (oral) | GLP-1 agonist | 13 to 14% | Oral tablet | Daily | FDA approved |
Liraglutide | GLP-1 agonist | 5 to 8% | Injection | Daily | FDA approved |
Phentermine/topiramate | Sympathomimetic + anticonvulsant | 7 to 10% | Oral capsule | Daily | FDA approved |
Contrave | Antidepressant + opioid antagonist | 5 to 6% | Oral tablet | Twice daily | FDA approved |
Orlistat | Lipase inhibitor | 3 to 5% | Oral capsule | 3x daily with meals | FDA approved / OTC |
Retatrutide | GLP-1 + GIP + glucagon triple agonist | 22 to 24% | Injection | Weekly | Phase 3 |
Orforglipron | Small molecule GLP-1 agonist | 10 to 12% | Oral tablet | Daily | FDA submission |
CagriSema | GLP-1 + amylin agonist (combination) | 15 to 17% | Injection | Weekly | Phase 3 |
Survodutide | GLP-1 + glucagon dual agonist | 14 to 19% | Injection | Weekly | Phase 3 |
MariTide | GLP-1 agonist + GIP antagonist | 17 to 20% | Injection | Monthly | Phase 3 |
Several observations stand out. First, retatrutide leads in raw weight loss efficacy, but it is not yet available. Second, semaglutide injectable remains the most accessible high-efficacy alternative available right now. Third, orforglipron stands to revolutionize the field by offering oral convenience with legitimate GLP-1 efficacy. And fourth, MariTide monthly dosing, if it delivers on phase 3, could redefine convenience.
The right alternative depends on your priorities. If maximum weight loss is the goal and you can handle injections, semaglutide is the current answer. If you want to avoid needles entirely, oral semaglutide or (eventually) orforglipron are the paths forward. If cost is the primary concern, affordable alternatives including compounded options and older medications deserve a close look.
When you should NOT switch from tirzepatide
Before exploring alternatives, consider whether switching is actually the right move. Sometimes the answer is to stay the course.
Side effects in the first 4 to 8 weeks are normal. Almost every person starting tirzepatide experiences some gastrointestinal discomfort during dose titration. Nausea, reduced appetite, mild constipation or diarrhea, these typically resolve as the body adjusts. Switching medications during this adjustment period means starting the side effect cycle all over again with a new drug. Our guide on what to expect after the first dose helps set realistic expectations.
A temporary plateau is not treatment failure. Weight loss with any GLP-1 agonist follows a nonlinear pattern. Weeks of rapid loss are followed by periods of stability. Some people panic at a two-week plateau and want to switch, when the reality is that their body is adjusting to its new weight set point before the next phase of loss begins. True treatment failure means no meaningful weight loss after 12 or more weeks at the maximum tolerated dose. The difference between a plateau and failure is time. Our article on why some people gain weight on tirzepatide explains the common reasons behind stalls and what to adjust before considering a switch.
Dose optimization has not been completed. If you have not reached the highest dose you can tolerate, you have not given tirzepatide a fair trial. Some people respond minimally at 5 mg but dramatically at 10 or 15 mg. The tirzepatide dosage chart shows the recommended escalation, and some physicians even explore splitting doses twice weekly for people who metabolize the medication quickly.
Hunger is manageable but imperfect. No weight loss medication eliminates hunger entirely. If tirzepatide has reduced your appetite by 60 to 70% and you are losing weight, switching because you still feel some hunger on tirzepatide may not improve your situation. Understanding what realistic appetite suppression looks like helps calibrate expectations.
The bottom line: switch when there is a clear, specific reason that is unlikely to resolve with time or dose adjustment. Do not switch because the first few weeks are uncomfortable or because progress is slower than you expected.
Compounded alternatives and what happened
The compounding story deserves its own section because it directly affects anyone looking for an affordable tirzepatide alternative.
During tirzepatide shortages, the FDA allowed licensed compounding pharmacies (both 503A and 503B facilities) to produce compounded tirzepatide. This made the medication available at dramatically lower prices, often $250 to $425 per month compared to over $1,000 for brand-name versions. Millions of people accessed tirzepatide this way.
In early 2025, the FDA announced that tirzepatide was no longer on the shortage list, triggering a regulatory process that required most compounding pharmacies to stop making tirzepatide. The deadline for 503A pharmacies was February 2025, with 503B facilities given until March 2025. This left many patients suddenly without their affordable supply.
The key alternatives that emerged from this situation:
Compounded semaglutide remains more widely available. Semaglutide was on the shortage list longer, and compounding pharmacies that had been producing it continued under different regulatory timelines. For many people who lost access to compounded tirzepatide, switching to compounded semaglutide was the most straightforward path to continuing treatment at an affordable price. Our switching guide with dosage charts covers the transition protocol.
Some pharmacies offer compounded tirzepatide variants. Certain compounding pharmacies began offering tirzepatide compounded with additional ingredients like glycine and B12, B6, or niacinamide, arguing these are different formulations. The legality of this approach remains contested.
503B outsourcing facilities that meet specific requirements may continue to compound in certain circumstances. The regulatory landscape is evolving, and staying current on what is actually available requires ongoing monitoring.
Pharmacy-specific alternatives: For those who had been using specific compounding pharmacies for tirzepatide, many of these same pharmacies now offer compounded semaglutide as an alternative. Empower Pharmacy, Olympia Pharmacy, and Belmar Pharmacy all provide compounded semaglutide options. For tirzepatide-specific pharmacy information, our guides on providers like Empower tirzepatide, Red Rock Pharmacy, Strive Pharmacy, and Priority Meds cover what each facility currently offers.
Understanding compounded tirzepatide expiration dates and shelf life matters for anyone with remaining stock. These products typically last 28 to 90 days when refrigerated, depending on the formulation. Proper storage following our expiration guidelines ensures you get full value from existing supplies while transitioning to an alternative.
The broader takeaway: the compounding landscape has shifted, but affordable alternatives still exist. They just require more research and potentially a medication switch to find the right balance of cost, efficacy, and accessibility.
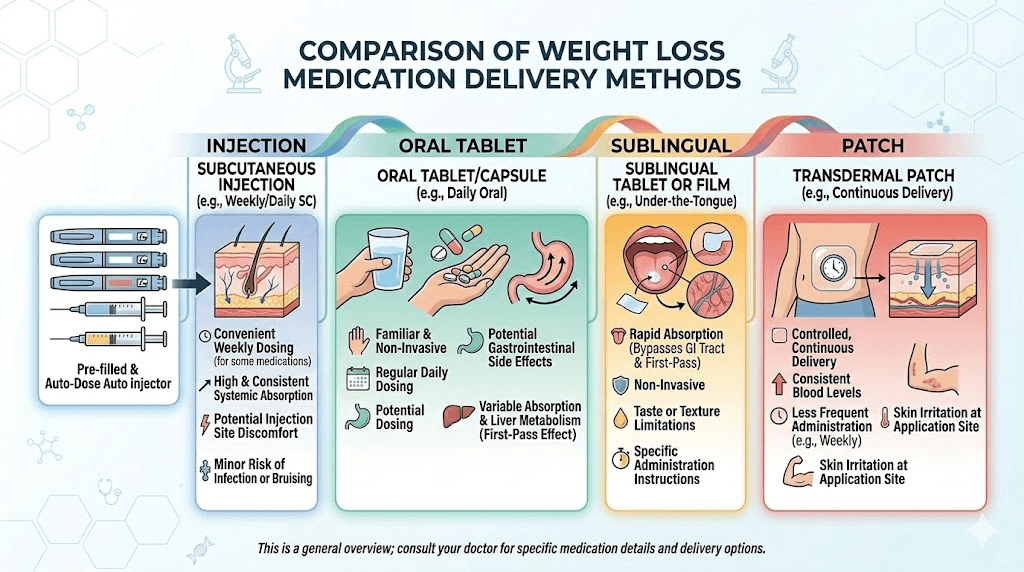
Oral alternatives to injectable tirzepatide
For many people, the injection itself is the problem. Whether due to needle phobia, injection site reactions, or simply a preference for oral medications, the demand for non-injectable alternatives is massive. Here is what is available and what is coming.
Currently available oral options:
Oral semaglutide (Rybelsus for diabetes, Wegovy tablets for weight loss) is the only FDA-approved oral GLP-1 agonist available now. It requires taking the tablet on an empty stomach with no more than 4 ounces of water, then waiting at least 30 minutes before eating or drinking anything else, or taking other medications. This restriction exists because semaglutide is a peptide that needs specific absorption conditions.
Our guides on tirzepatide tablets vs injections and oral vs injection delivery discuss why a true oral tirzepatide does not yet exist and what alternatives fill that gap. The tirzepatide drops and orally dissolving tablet formulations represent compounding innovations, but their bioavailability compared to injectable tirzepatide varies.
Sublingual semaglutide is another non-injection route available through some compounding pharmacies. Sublingual delivery bypasses the digestive system by absorbing through the tissue under the tongue, potentially offering better bioavailability than oral tablets.
Coming soon: Orforglipron, as discussed above, will be a small-molecule oral GLP-1 agonist without the absorption restrictions of peptide-based oral formulations. Amycretin is also being developed in oral form. Within the next 1 to 2 years, the oral options landscape will look dramatically different.
For those interested in non-oral, non-injection delivery, GLP-1 patches (Onmorlo) represent another emerging delivery method that eliminates both needles and pills.
Natural and over-the-counter alternatives
Let us be honest upfront: no natural compound produces weight loss anywhere close to tirzepatide. But some supplements have legitimate research behind them, and for people who cannot or choose not to use prescription medications, they represent the best available options.
Berberine
Berberine has been marketed as "natural Ozempic," which is both misleading and contains a kernel of truth. This plant alkaloid, found in goldenseal, barberry, and Oregon grape, does activate AMPK (adenosine monophosphate-activated protein kinase), which plays a role in glucose and lipid metabolism. Some research shows it can improve insulin sensitivity and modestly reduce blood sugar levels.
The honest data: a meta-analysis found berberine treatment decreased body weight by an average of about 2.07 kg (4.5 pounds). Compare that to tirzepatide average of 20+ kg in clinical trials. Berberine is better characterized as a metabolic health supplement than a weight loss drug.
Our guide on berberine and semaglutide together explores whether combining these approaches offers additive benefits. The short answer: berberine may support metabolic health alongside GLP-1 therapy but should not be considered a replacement.
Important caution: berberine has hypoglycemic properties and can interact with diabetes medications, blood thinners, and certain other drugs. It is not regulated by the FDA, so quality and potency vary dramatically between brands.
GLP-1 supporting supplements and probiotics
A growing category of supplements claims to naturally boost GLP-1 levels. Products like Pendulum GLP-1 Probiotic use specific bacterial strains (particularly Akkermansia muciniphila) that may increase endogenous GLP-1 production in the gut. Other products like ReSM postbiotic and Advanced Bionutritionals GLP-1 Plus take similar approaches.
The evidence for these products is early-stage. While the underlying science of gut bacteria influencing GLP-1 production is sound, the clinical data showing meaningful weight loss from probiotic supplementation alone is limited. Reviews of products like Tranont GLP-1, Ellie GLP-1, and GLP-1 vitamin supplements are available across the SeekPeptides blog for those wanting detailed breakdowns.
Other brands in this space include Evolv GLP-1, MMIT GLP-1, Thrive GLP-1, LifeVantage MindBody, Replenza GLP-1, and GLP-1 Companion. The market is growing rapidly, but buyer beware: most claims outpace the evidence.
Dietary approaches that support GLP-1 activity
Certain foods and eating patterns naturally stimulate GLP-1 release from intestinal L-cells. While these approaches will not produce pharmaceutical-level weight loss, they can complement any medication or serve as a starting point for people not ready for prescription drugs.
High-protein meals consistently stimulate the most GLP-1 release. Fiber-rich foods, particularly fermentable fibers, feed gut bacteria that influence GLP-1 production. Specific foods associated with increased GLP-1 secretion include eggs, nuts, avocados, and fermented foods like yogurt and sauerkraut.
Our dietary guides for best foods to eat on semaglutide, tirzepatide foods to avoid, tirzepatide diet plans, and GLP-1 breakfast ideas all apply equally well to anyone on a tirzepatide alternative, as the nutritional principles are the same regardless of which medication you use.
Time-restricted eating (intermittent fasting) also shows some evidence of enhancing GLP-1 sensitivity, though the research is still developing. A common protocol is the 16:8 approach, eating within an 8-hour window and fasting for 16 hours. Some studies suggest this pattern increases endogenous GLP-1 production during the fasting period, priming the body for better glucose regulation when eating resumes.
Combined with regular exercise, particularly resistance training to preserve lean mass during weight loss, dietary approaches can meaningfully supplement any medication regimen. The semaglutide diet plan and tirzepatide meal plan we publish work with any GLP-1 alternative because the underlying nutritional science is the same: prioritize protein, choose whole foods, limit processed carbohydrates, and eat adequate fiber to support gut health.
The key takeaway with natural alternatives: they are not replacements for pharmaceutical options. They are supplementary tools. Berberine will not produce 15% body weight loss. Probiotics will not replicate GLP-1 receptor activation. But these approaches can support metabolic health, ease the transition between medications, and provide value for people who are not candidates for or do not want prescription drugs. Understanding their limitations honestly is more helpful than overpromising.
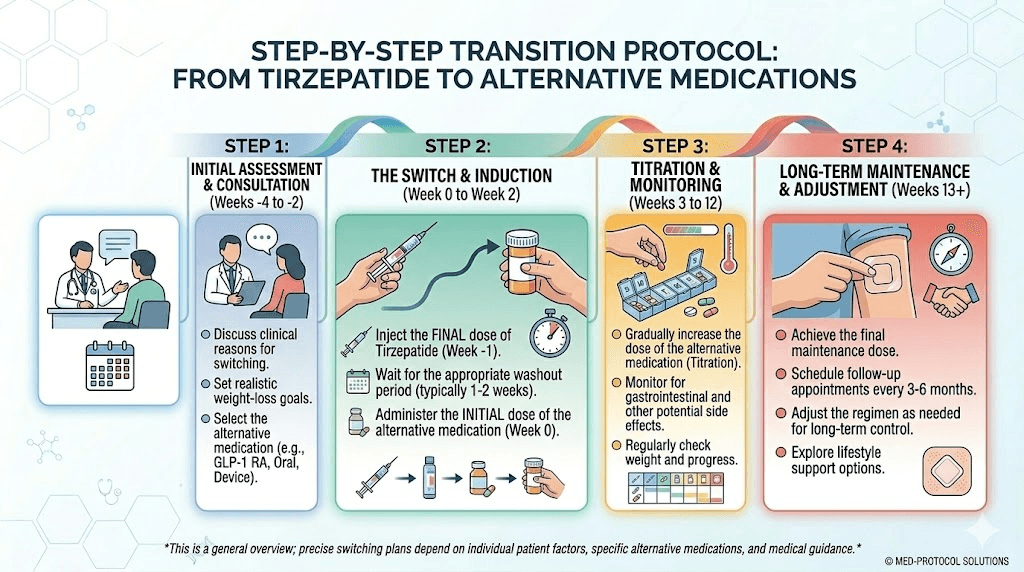
How to switch from tirzepatide to an alternative
Switching medications is not as simple as stopping one and starting another. The approach depends on which alternative you are switching to, your current tirzepatide dose, and your reasons for switching. Here is what the evidence shows.
Switching to semaglutide
This is the most common switch, and the protocol is well-established. The general approach is to start semaglutide at the lowest dose (0.25 mg weekly for injectable, or the lowest available oral dose) regardless of what tirzepatide dose you were on. This is because tirzepatide activates both GLP-1 and GIP receptors, while semaglutide only activates GLP-1. Your body needs time to adjust to the different receptor activation profile.
Most healthcare providers recommend waiting one week after the last tirzepatide injection before starting semaglutide. Some allow starting the very next week. The timing matters because overlapping two GLP-1 active medications can significantly increase gastrointestinal side effects.
Our detailed switching from tirzepatide to semaglutide dosage chart provides week-by-week titration schedules based on your previous tirzepatide dose. The conversion chart shows approximate dosage equivalencies for providers.
Expect some fluctuation during the transition. Many people experience a temporary increase in appetite as tirzepatide washes out (its half-life is about 5 days) before semaglutide reaches therapeutic levels. This window can be managed with dietary strategies from our list of foods to eat while on semaglutide guide and high-protein approaches.
Switching to retatrutide
For researchers transitioning from tirzepatide to retatrutide, the protocol considerations are different because retatrutide adds glucagon receptor activation. Our guide on switching from tirzepatide to retatrutide and the retatrutide dosage schedule after high-dose tirzepatide cover the specific considerations involved.
The key difference: because retatrutide adds a third receptor target, starting doses should be conservative even if you were on high-dose tirzepatide. The glucagon receptor component can cause additional effects on blood glucose and energy expenditure that require monitoring.
Switching to a non-GLP-1 medication
If you are switching to phentermine/topiramate, Contrave, or another non-GLP-1 medication, the transition is simpler in some ways but more complex in others. You can typically start the new medication immediately after stopping tirzepatide, since these medications work through entirely different pathways.
However, expect a more noticeable rebound in appetite. Tirzepatide provides powerful appetite suppression through hormonal pathways that non-GLP-1 medications do not replicate. Understanding how to wean off tirzepatide and manage the transition can help minimize weight regain during the switch.
For anyone transitioning away from tirzepatide, regardless of the alternative chosen, our guide on how to maintain weight loss after tirzepatide provides evidence-based strategies for keeping the weight off during and after the transition.
Which alternative is right for you
Choosing the right tirzepatide alternative depends on answering a few key questions honestly. Here is a decision framework based on the most common scenarios.
If your primary concern is cost: Compounded semaglutide offers the best balance of efficacy and affordability. At $150 to $300 per month, it delivers 14 to 16% average weight loss. Affordable compounded options and insurance coverage guides can help reduce costs further. Phentermine/topiramate is another affordable option with decent efficacy.
If tirzepatide side effects are the issue: Semaglutide (single-receptor) often causes fewer gastrointestinal effects than dual-receptor tirzepatide. If even semaglutide is too much, liraglutide daily dosing allows more granular titration. If all GLP-1 agonists cause problems, non-GLP-1 options like Contrave or Qsymia work through entirely different pathways. Check our guides on specific side effects like insomnia, dry mouth, fatigue, and headaches to see if your specific side effect is manageable with adjustments before switching.
If you want to avoid injections: Oral semaglutide (available now), orforglipron (pending FDA approval), or oral amycretin (in development) are your GLP-1 options. Qsymia and Contrave are already available in oral form. GLP-1 patches offer another non-injection route. Learn how to navigate your options with our guide on what to say when requesting GLP-1 options.
If tirzepatide stopped working: A plateau on one GLP-1 medication does not necessarily mean another will fail. Some people respond better to single-receptor agonists, others to dual-receptor, and the emerging triple-receptor agonists may work for those who plateaued on dual therapy. If semaglutide did not work and you tried tirzepatide, or tirzepatide stopped producing results, switching to a completely different mechanism (like Contrave for reward-driven eating) may address the underlying cause.
If you are pregnant, planning pregnancy, or breastfeeding: All GLP-1 agonists are contraindicated in pregnancy. Our guides on tirzepatide while breastfeeding, GLP-1 while breastfeeding, and pregnancy on tirzepatide cover the specific safety concerns. Dietary and lifestyle approaches become the primary tools during this period.
If you want maximum weight loss: Among currently available options, injectable semaglutide at the highest dose comes closest to tirzepatide efficacy. Among pipeline options, retatrutide leads in raw weight loss data. For researchers interested in protocols, SeekPeptides members access detailed comparison tools and dosage comparison charts that help identify the optimal approach based on individual factors.
If you have specific health conditions: People with Hashimoto thyroiditis or autoimmune conditions may benefit from microdosing approaches. Those concerned about kidney health should review information about semaglutide and kidney stones. Cardiovascular concerns may favor alternatives with strong CVOT data like liraglutide.
Combining alternatives with other compounds
One approach gaining attention is combining a primary weight loss medication with complementary compounds. This is distinct from the pharmaceutical combination drugs discussed above (CagriSema, Qsymia) and instead involves adding supportive compounds to a primary therapy.
Common combinations being explored:
GLP-1 agonists plus metabolic support: Adding compounds like glycine, B12, methylcobalamin, or L-carnitine to semaglutide protocols is common in compounding pharmacy formulations. These additions target energy metabolism, methylation support, and fat oxidation pathways that GLP-1 agonists do not directly address. Similar combinations exist with tirzepatide, including glycine, vitamin B6, and levocarnitine blends.
Peptide stacking for researchers: Some researchers explore combinations like AOD-9604 with tirzepatide alternatives or tesamorelin with retatrutide to target fat loss through multiple pathways. The peptide stack calculator on SeekPeptides helps researchers plan these combinations safely.
Nutritional supplementation: Regardless of which alternative you choose, supplements to take alongside GLP-1 medications can address common nutritional gaps. GLP-1 agonists reduce food intake, which means reduced micronutrient intake. Key supplements include a quality multivitamin, omega-3 fatty acids, magnesium, and adequate protein supplementation to preserve lean muscle mass during weight loss.
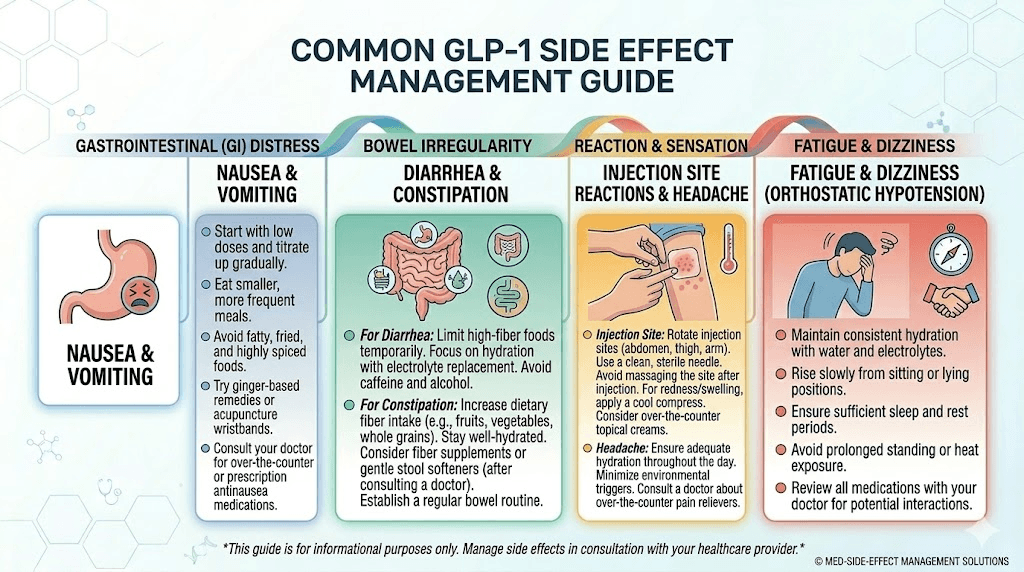
Managing side effects across tirzepatide alternatives
Every weight loss medication comes with potential side effects. Understanding what to expect and how to manage them makes the transition smoother regardless of which alternative you choose.
Gastrointestinal effects are the most common across all GLP-1 agonists. Nausea, constipation, bloating, and burping typically peak during dose escalation and improve over 4 to 8 weeks. Eating smaller, more frequent meals helps. Avoiding high-fat and high-sugar foods reduces nausea. Staying hydrated is essential.
Fatigue is reported with most alternatives, including GLP-1 agonists (semaglutide fatigue and GLP-1 fatigue generally) and non-GLP-1 options. Reduced caloric intake naturally reduces energy availability. Ensuring adequate protein, staying active, and checking for micronutrient deficiencies (particularly iron, B12, and vitamin D) helps manage this. If your alternative makes you feel the opposite, know that some people actually find semaglutide gives them energy.
Injection site reactions affect users of injectable alternatives. Common presentations include redness, itching, and minor swelling. Our guides on GLP-1 injection site reactions, reaction treatment, and best injection sites for weight loss provide management strategies and proper technique to minimize reactions.
Hair loss is a concern that crosses all rapid weight loss approaches, whether medication-assisted or not. It is typically related to the rate of weight loss and nutritional changes rather than the specific medication. Adequate protein intake (0.8 to 1.0 grams per pound of body weight) and micronutrient supplementation help prevent this.
Dizziness, insomnia, and changes in libido are less common but reported across GLP-1 alternatives. Blood clot concerns and menstrual changes are topics we cover in depth for those with specific health concerns.
Practical tools and resources for any alternative
Regardless of which tirzepatide alternative you choose, several practical resources apply universally.
Dosing calculators: The semaglutide dosage calculator and general peptide calculator help determine accurate dosing for injectable options. For cost comparisons between alternatives, the peptide cost calculator provides month-by-month projections.
Reconstitution guides: If you are using compounded alternatives, proper reconstitution is critical. Our guides on how to reconstitute semaglutide and reconstitution calculator ensure accurate preparation. Understanding bacteriostatic water ratios is essential for maintaining potency.
Injection technique: For injectable alternatives, proper technique matters for absorption and comfort. Our guides on how to inject GLP-1, where to inject, best injection sites for semaglutide, and syringe injection technique apply to most injectable alternatives.
Storage: Proper storage preserves medication efficacy. Whether you are storing semaglutide (shelf life in the fridge, what happens if it gets warm) or retatrutide (how long it lasts), temperature control matters. Our guide on traveling with semaglutide and traveling with tirzepatide covers on-the-go storage solutions.
Tracking results: Monitor your progress regardless of which alternative you use. Our GLP-1 plotter tool helps visualize weight loss trends. Compare your results to typical timelines like semaglutide one-month results, first week on semaglutide, or before and after semaglutide to set realistic expectations.
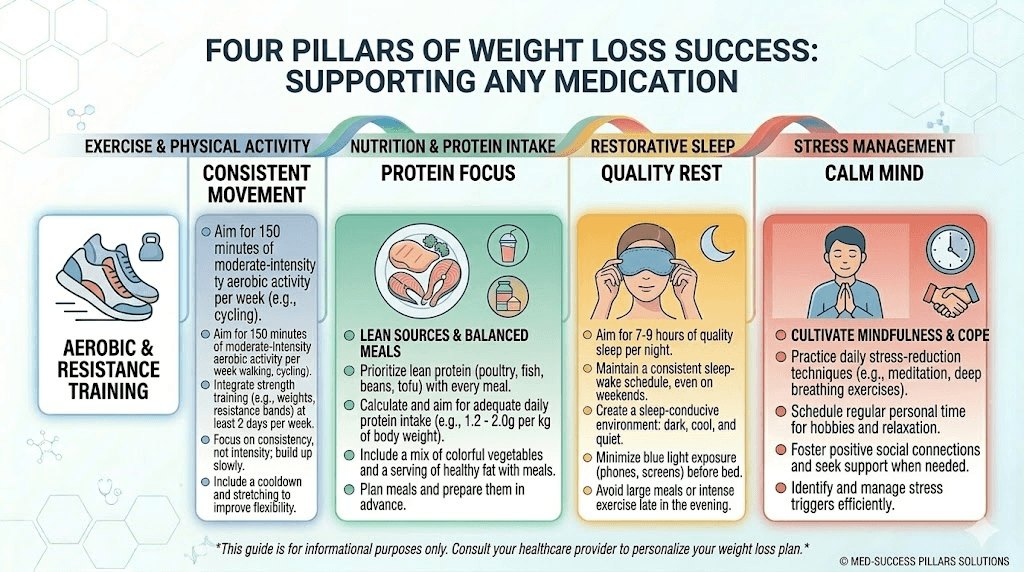
Lifestyle factors that enhance any alternative
No weight loss medication works in a vacuum. The people who see the best results with any tirzepatide alternative are those who combine medication with strategic lifestyle modifications. These are the factors that consistently separate good outcomes from exceptional ones.
Exercise selection matters more than volume. Resistance training preserves lean muscle mass during rapid weight loss, which is crucial because GLP-1 agonist-driven weight loss can include significant muscle loss (up to 30 to 40% of total weight lost can be lean mass without intervention). Aim for 2 to 3 resistance training sessions per week. Moderate cardio (walking 30 to 45 minutes daily) supports overall metabolic health and improves insulin sensitivity. You can lose weight on GLP-1 agonists without exercise, but outcomes are significantly better with it.
Protein intake is non-negotiable. Whether you are on semaglutide, phentermine, or any other alternative, consuming 0.8 to 1.0 grams of protein per pound of body weight protects against muscle loss. This requires conscious effort because appetite suppression from GLP-1 agonists makes eating enough protein challenging. Protein shakes and strategic meal timing help meet targets.
Sleep quality directly affects weight loss hormones. Poor sleep increases ghrelin (hunger hormone), decreases leptin (satiety hormone), and impairs insulin sensitivity. If your alternative is causing insomnia or sleep disruption, addressing this is essential for both medication efficacy and overall health. Aim for 7 to 9 hours per night. Consistent sleep and wake times matter more than total hours. Avoiding screens for 60 minutes before bed and keeping the bedroom cool (65 to 68 degrees Fahrenheit) are evidence-based sleep hygiene fundamentals.
Stress management and hydration round out the lifestyle fundamentals. Chronic stress elevates cortisol, which promotes visceral fat storage and can counteract the metabolic benefits of any weight loss medication. Even 10 minutes of daily meditation, deep breathing, or walking in nature measurably reduces cortisol levels. Dehydration, meanwhile, can mimic hunger and lead to unnecessary caloric intake. Aim for at least half your body weight in ounces of water daily, more if you exercise or live in a warm climate.
Alcohol deserves special mention. Many people overlook alcohol as a factor in weight loss stalls. Alcohol provides 7 calories per gram (nearly as calorie-dense as fat), reduces inhibitions around food choices, disrupts sleep quality, and can interact with GLP-1 medications. Our guides on drinking on tirzepatide, drinking on semaglutide, and best alcohol choices apply equally to any alternative. The honest answer: minimizing alcohol consumption significantly improves results with any weight loss approach.
These basics sound simple because they are. They are also the factors most people neglect while focusing exclusively on which medication to take. The medication creates the opportunity for weight loss by reducing appetite and improving metabolic function. But the lifestyle factors determine how much of that opportunity gets converted into actual, sustainable results.
The future of tirzepatide alternatives
The weight loss medication landscape is evolving faster than any other area of pharmacology. Several trends are shaping what alternatives will look like in the next 2 to 5 years.
More mechanisms, more targets. We are moving from single-agonists (semaglutide) to dual-agonists (tirzepatide) to triple-agonists (retatrutide) and beyond. The trend toward multi-receptor targeting will likely continue, with researchers exploring combinations that add amylin, glucagon, and other metabolic hormone pathways.
Oral formulations will dominate. Orforglipron, oral amycretin, and next-generation oral formulations will make injectable GLP-1 agonists the exception rather than the rule within a few years. This shift will dramatically expand access and reduce the barrier to treatment.
Monthly and less frequent dosing. MariTide once-monthly dosing is just the beginning. Long-acting formulations that require dosing only every 4 to 12 weeks are in development, which would eliminate the weekly injection burden entirely.
Personalized approaches. As we accumulate more data on genetic and metabolic predictors of drug response, the ability to match patients with the right medication from the start will improve. Rather than trial-and-error switching between alternatives, pharmacogenomic testing may guide first-line treatment selection. Early research suggests that variations in GLP-1 receptor genetics, GIP receptor sensitivity, and metabolic enzyme profiles influence who responds best to which agent. Within a few years, a simple genetic test before starting treatment could save months of ineffective therapy and unnecessary side effects.
Combination therapies. The most effective future approaches will likely combine mechanisms, just as CagriSema combines GLP-1 and amylin pathways. Rational combination of medications targeting different aspects of energy balance, including appetite reduction, fat absorption, energy expenditure, and reward system modulation, could produce results exceeding any single agent. The era of one-size-fits-all obesity treatment is ending. The future is personalized, multi-mechanism, and increasingly accessible.
For researchers and patients staying current on these developments, SeekPeptides provides ongoing coverage of clinical trial results, regulatory decisions, and practical protocol guidance as new alternatives become available. Members get access to comprehensive comparison tools, evidence-based protocol builders, and a community of experienced researchers navigating these same decisions.
Frequently asked questions
What is the closest alternative to tirzepatide?
Injectable semaglutide (Wegovy) is the closest currently available alternative. It targets the GLP-1 receptor that tirzepatide also activates, producing 14 to 16% average weight loss compared to tirzepatide 17 to 22%. The semaglutide vs tirzepatide comparison page breaks down the detailed differences.
Is there an oral alternative to tirzepatide?
Oral semaglutide (Wegovy tablets) is available now and produces 13 to 14% weight loss. Orforglipron, a small-molecule oral GLP-1 agonist, has been submitted for FDA approval and may become available in 2026. Our orforglipron vs tirzepatide guide covers the upcoming option in detail.
Can I switch from tirzepatide to semaglutide without gaining weight?
Most people can switch successfully with careful dose management. Starting semaglutide at the lowest dose and titrating up while maintaining dietary discipline minimizes weight regain. Some temporary appetite increase during the transition is normal. The switching dosage chart provides the step-by-step protocol.
What alternative works if tirzepatide did not work for me?
If tirzepatide was ineffective, consider why. If the issue was side effects preventing dose escalation, semaglutide (different receptor profile) may be tolerated better. If you reached full dose without results, a non-GLP-1 alternative like Contrave (targeting reward pathways) may address the underlying issue differently. Some people respond better to phentermine-based approaches.
Is retatrutide better than tirzepatide?
Phase 2 data suggests retatrutide produces more weight loss (24.2% vs 22.5% at maximum doses). However, retatrutide is not yet FDA-approved, has a higher rate of adverse events, and lacks the long-term safety data that tirzepatide has. Our detailed comparison covers both the promise and the limitations.
Are natural alternatives to tirzepatide effective?
Natural alternatives like berberine produce modest metabolic benefits but cannot replicate the weight loss efficacy of tirzepatide or any prescription GLP-1 agonist. Average weight loss from berberine is about 4.5 pounds versus 40+ pounds from tirzepatide. Natural approaches work best as complementary strategies alongside medication or as starting points for people not ready for prescriptions.
What is the cheapest alternative to tirzepatide?
Metformin (under $10 per month) is the cheapest prescription option but produces only modest weight loss. Compounded semaglutide ($150 to $300 per month) offers the best cost-to-efficacy ratio among GLP-1 options. Phentermine alone costs $15 to $40 per month and produces meaningful appetite suppression.
Can I use two alternatives together?
Some combinations are medically appropriate under physician supervision. Phentermine with semaglutide is increasingly common. Metformin with GLP-1 agonists is standard for type 2 diabetes. Never combine multiple GLP-1 agonists (semaglutide and tirzepatide together is not recommended). Always consult your healthcare provider before combining medications.
How do I qualify for a tirzepatide alternative?
Qualification criteria vary by medication. Most GLP-1 agonists for weight management require a BMI of 30 or higher, or 27 or higher with at least one weight-related condition. Our guide on BMI requirements for GLP-1 and how to qualify for semaglutide covers the eligibility criteria for each option. Knowing what to say when requesting GLP-1 options from your provider can help navigate the conversation effectively.
Will my insurance cover tirzepatide alternatives?
Coverage varies dramatically by insurer, plan, and specific medication. Semaglutide (Wegovy) has broader insurance coverage than some newer options. Blue Cross Blue Shield GLP-1 coverage policies have been expanding, and many employers now include weight management medications in their formularies. Phentermine/topiramate and Contrave are often covered with lower copays than GLP-1 agonists because they have been available longer and cost less.
How long should I try an alternative before deciding it does not work?
Give any new weight loss medication at least 12 to 16 weeks at the therapeutic dose before concluding it is ineffective. That means 12 weeks after completing the dose titration period, not 12 weeks from your first dose. Some people see dramatic results in weeks 12 to 20 that were not apparent earlier. If you reach the maximum tolerated dose and see less than 5% body weight reduction after 16 weeks at that dose, it is reasonable to discuss alternatives with your provider.
Can I restart tirzepatide later if I stop?
Yes, you can restart tirzepatide if you switch to an alternative and decide to return. However, most providers recommend starting at the beginning dose regardless of your previous dose. Your body loses its tolerance to GLP-1 receptor activation during time off, and jumping back to a high dose can cause severe gastrointestinal side effects. The retitration typically takes 12 to 16 weeks to reach your previous dose.
External resources
FDA: Medications containing semaglutide for diabetes or obesity
New England Journal of Medicine: Tirzepatide once weekly for the treatment of obesity
Obesity Medicine Association: Weight loss medications overview
In case I do not see you, good afternoon, good evening, and good night. May your alternatives stay effective, your transitions stay smooth, and your weight loss journey stay on track.