Feb 26, 2026

Your stomach feels like a balloon. You ate half of what you normally would, three hours ago, and somehow it still feels like the food is sitting there, expanding, pressing against everything. You have read that semaglutide causes some digestive upset. You expected nausea, maybe. But this relentless, uncomfortable fullness that turns every meal into an exercise in regret? Nobody warned you about this part.
You are not imagining it. And you are not alone.
Bloating is one of the most common and least discussed side effects of semaglutide therapy. Clinical trial data shows that up to 50% of participants experienced some form of abdominal distension during treatment, with symptoms most pronounced during dose escalation and the early weeks. The mechanism is straightforward but the experience is anything but simple. Semaglutide works by activating GLP-1 receptors that deliberately slow how fast your stomach empties. That delayed gastric emptying is part of what makes the medication effective for weight loss and blood sugar control. But it also means food sits in your stomach longer than your body is accustomed to, and your digestive system needs time to adapt to this new pace.
This guide covers everything researchers and users need to know about semaglutide bloating. What causes it at the cellular level. How long it typically lasts. Which foods make it dramatically worse. What actually works to reduce it. When bloating crosses the line from normal adjustment into something that needs medical attention. And how to tell the difference between temporary discomfort and a signal that your protocol needs adjustment. SeekPeptides has compiled the clinical evidence, real-world management strategies, and specific protocols that help users navigate this common side effect without abandoning treatment that is otherwise working.
Why semaglutide causes bloating in the first place
Understanding the mechanism behind semaglutide bloating is not just academic. It changes how you approach the problem entirely.
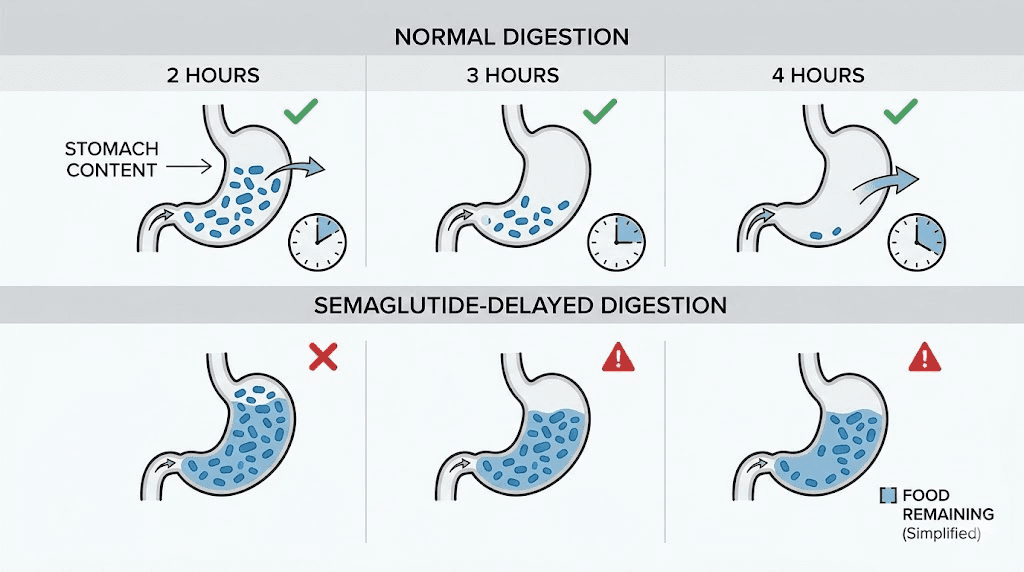
Semaglutide is a GLP-1 receptor agonist. That means it mimics a hormone your body already produces, glucagon-like peptide-1, but at much higher and more sustained levels than natural production allows. One of the primary effects of GLP-1 receptor activation is slowing gastric motility. Your stomach normally empties its contents into the small intestine within about 2 to 4 hours after a meal. On semaglutide, that process takes significantly longer.
How much longer? Research published in clinical gastroenterology journals found that semaglutide increased gastric retention of solid food by 25.5% at the 2-hour mark, 38.0% at 3 hours, and 30.0% at 4 hours compared to baseline. In practical terms, participants on semaglutide still had 37% of a solid meal remaining in their stomach at the 4-hour mark. The placebo group? Zero retention at that same timepoint.
That retained food creates mechanical distension. The stomach walls stretch. Stretch receptors fire. And your brain interprets those signals as that uncomfortable, pressurized fullness that makes you want to unbutton your pants after eating what used to be a normal-sized meal.
The gas production problem
Bloating on semaglutide is not just about food sitting in the stomach. When gastric emptying slows, the entire downstream digestive process changes. Food that lingers longer in the stomach can undergo additional fermentation before it even reaches the small intestine. Once it does reach the intestines, the altered transit time means bacteria have more opportunity to produce gas from partially digested carbohydrates and fibers.
This is why certain foods that never bothered you before suddenly become problems on semaglutide. Foods high in fermentable carbohydrates, things like beans, cruciferous vegetables, onions, and certain fruits, now have extra time to interact with gut bacteria. The result is more gas, more distension, and more of that bloated feeling that makes meal planning on semaglutide genuinely challenging.
There is also the constipation factor. Semaglutide slows intestinal motility along the entire digestive tract, not just the stomach. Constipation on semaglutide is reported by a significant percentage of users, and constipation directly contributes to bloating. When stool moves slowly through the colon, it creates a backlog effect. Gas gets trapped behind it. The abdomen distends. And the combination of delayed gastric emptying on top with slow colonic transit below creates a compression effect that makes bloating feel worse than either issue would on its own.
How GLP-1 receptor activation changes your entire gut
The effects extend beyond simple slowing. GLP-1 receptors are distributed throughout the gastrointestinal tract. Activating them changes the secretion of digestive enzymes, alters bile acid cycling, and modifies the electrical patterns that coordinate muscular contractions along the intestinal wall. Research on GLP-1 agonists and the gut microbiome shows that treatment can shift bacterial populations, potentially increasing species like Akkermansia muciniphila while decreasing overall microbial diversity. These shifts can change gas production patterns and how your body handles different food types.
Some users on compounded semaglutide formulations report different bloating profiles compared to brand-name versions. This may relate to differences in absorption kinetics, though formal comparison data remains limited. Regardless of the formulation, the core mechanism is the same. GLP-1 activation slows your gut, and your gut needs time to find a new equilibrium.
How common is semaglutide bloating and what the clinical data actually shows
Numbers matter here because they set expectations. And when your expectations match reality, you make better decisions about whether to push through, adjust, or seek help.
The STEP clinical trial program, which evaluated semaglutide at the 2.4mg weekly dose for weight management, provides the most robust data. Across STEP 1 through STEP 3, 82.2% of patients taking semaglutide experienced some form of gastrointestinal adverse event, compared to 53.9% in the placebo group. That is a substantial gap that confirms GI effects are genuinely medication-related, not just anxiety or coincidence.
Here is the breakdown by specific symptom:
Symptom | Semaglutide group | Placebo group | Difference |
|---|---|---|---|
Nausea | 44% | 17% | +27% |
Diarrhea | 30% | 16% | +14% |
Vomiting | 24% | 6% | +18% |
Constipation | 24% | 11% | +13% |
Abdominal pain | 20% | 10% | +10% |
Bloating/distension | Up to 50% | ~15% | +35% |
A critical nuance: 99.5% of gastrointestinal adverse events in these trials were classified as non-serious. And 98.1% were rated as mild to moderate in severity. Severe GI events that required dose reduction or treatment discontinuation were relatively rare. This means that while bloating is common, it is overwhelmingly manageable in clinical settings.
Bloating frequency varies by semaglutide dose
Dose matters enormously. Users on the lower semaglutide doses experience significantly less bloating than those who have escalated to the full therapeutic dose. The standard titration schedule exists specifically to give the GI tract time to adapt at each level before increasing the medication load.
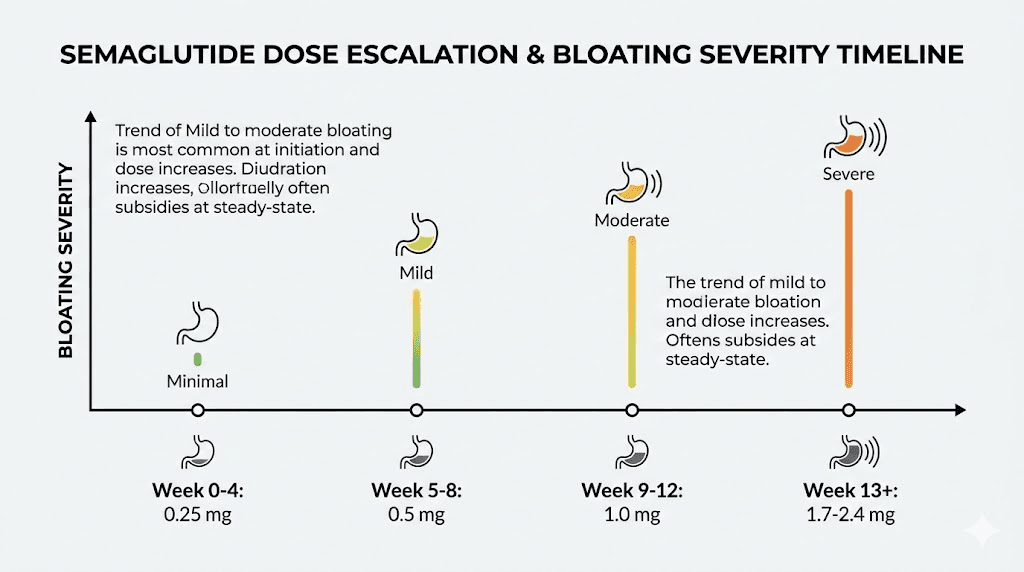
The typical dose escalation for semaglutide dosing follows this pattern:
Weeks | Weekly dose | Typical bloating severity |
|---|---|---|
Weeks 1-4 | 0.25 mg | Mild or absent |
Weeks 5-8 | 0.5 mg | Mild, intermittent |
Weeks 9-12 | 1.0 mg | Moderate, most noticeable |
Weeks 13-16 | 1.7 mg | Moderate, beginning to adapt |
Week 17+ | 2.4 mg | Variable, often improving |
Each dose increase can trigger a fresh wave of bloating that typically peaks 3 to 5 days after the increase and then gradually subsides over the following 1 to 2 weeks. Users who understand this pattern are far less likely to panic or discontinue treatment prematurely. The timeline for semaglutide to work closely parallels this adjustment period, with weight loss benefits accelerating as the body adapts to each dose level.
When does semaglutide bloating start and how long does it typically last
Timing is everything when you are trying to decide whether to push through or make changes.
Most users report bloating onset within the first 1 to 2 weeks of starting semaglutide or within the first week after each dose escalation. The bloating tends to be most intense during the first 2 to 4 weeks of a new dose level. After that initial adjustment period, the digestive system begins to recalibrate, and symptoms gradually decrease.
The broader clinical data is encouraging. Research indicates that gastrointestinal symptoms, including bloating, are substantially reduced after approximately 20 weeks of consistent use. This does not mean they disappear entirely for everyone, but the trend is clearly toward improvement over time.
Week-by-week bloating timeline
Based on clinical trial data and real-world reports, here is what to expect:
Weeks 1-2: Bloating appears as the medication reaches steady-state levels. Many users describe a heavy, full feeling after meals, even small ones. This is the GLP-1 receptors starting to modulate gastric emptying. Meals that took 2-3 hours to clear your stomach now take 4-6 hours.
Weeks 3-4: Bloating often peaks during this period if you remain at the starting dose, or it resurges if you have just escalated. The body is producing compensatory responses. Some days are worse than others. Many users notice that injection timing affects how severe the bloating is relative to meals.
Weeks 5-8: For many users, this is when adaptation begins. The degree of gastric emptying delay stabilizes as the body adjusts to consistent GLP-1 receptor stimulation. Bloating episodes become less frequent and less severe, though they may still flare after particularly large meals or trigger foods.
Weeks 9-16: Most users who will adapt have done so by this point. Bloating becomes episodic rather than constant. Learning which foods trigger it (covered in detail below) makes a substantial difference. This is also the period where users typically escalate through the higher doses, so each increase can temporarily reset the clock.
Weeks 17-20+: Clinical data shows significant reduction in GI symptoms by this stage. The digestive system has established a new normal. Residual bloating tends to be mild and predictable, usually related to specific dietary choices rather than the medication itself.
Why some people adapt faster than others
Individual variation is significant. Factors that influence adaptation speed include baseline gut motility (people who already had slower digestion may adapt faster because the change is less dramatic), diet composition, physical activity level, stress, and genetic variation in GLP-1 receptor sensitivity. People who follow a careful semaglutide diet plan from day one tend to experience less severe bloating than those who maintain their pre-treatment eating habits.
Users taking semaglutide with B12 or semaglutide methylcobalamin compounds report variable differences in GI tolerance, though controlled comparison data is limited. The addition of B vitamins does not directly address the gastric emptying delay, but may support overall digestive function through different pathways.
The difference between normal semaglutide bloating and gastroparesis
This is the section that could save you a trip to the emergency room. Or, more importantly, get you there when you actually need to go.
Normal semaglutide bloating and medication-induced gastroparesis exist on a spectrum, but they are not the same thing. Understanding where one ends and the other begins is critical for every semaglutide user.
Normal bloating looks like this
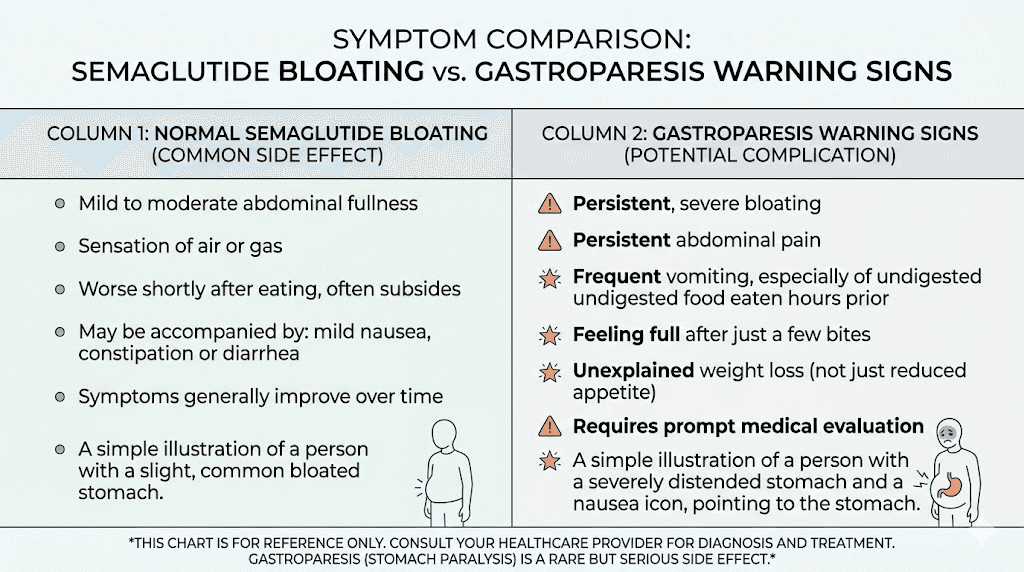
Uncomfortable fullness after meals. Visible abdominal distension that resolves within several hours. Increased gas. Mild cramping. Symptoms that are worse after certain foods and better after others. A pattern that gradually improves over weeks. The ability to eat, even if smaller amounts. Regular (if slower) bowel movements.
This is your body adjusting. It is unpleasant but not dangerous.
Gastroparesis warning signs
Gastroparesis means the stomach has essentially stopped emptying, or emptied so slowly that food remains for 12+ hours. Case reports published in PMC have documented semaglutide-induced gastroparesis, particularly in patients with pre-existing risk factors or those who escalated doses too rapidly. The warning signs include:
Severe, worsening abdominal pain that does not resolve
Vomiting undigested food many hours after eating (4+ hours)
Complete inability to keep food down for more than 24 hours
Feeling full after just a few bites consistently across multiple days
Visible, persistent abdominal distension that does not fluctuate
Unintentional weight loss beyond what is expected from the medication
Inability to pass gas or have bowel movements for 3+ days
If you experience these symptoms, stop taking semaglutide and contact your healthcare provider immediately. Gastroparesis can lead to dehydration, nutritional deficiencies, and bezoar formation (solidified masses of undigested food in the stomach).
Risk factors for semaglutide-induced gastroparesis
Published case reports highlight several patterns. Rapid dose escalation increases risk significantly. Research shows that side effects across multiple systems are more common when doses increase too quickly. Pre-existing diabetes with autonomic neuropathy is another major risk factor, as diabetic neuropathy already compromises gastric nerve function. History of prior GI surgery, hypothyroidism, and certain medications that independently slow motility (opioids, anticholinergics) all compound the risk.
One case report documented a patient who developed gastroparesis after rapid escalation from low-dose to therapeutic-dose semaglutide within weeks rather than following the standard monthly titration. The symptoms resolved after semaglutide discontinuation and prokinetic treatment, but full recovery took several weeks. This underscores why the gradual dose escalation schedule exists and why following proper semaglutide dosing protocols is not optional.
Foods that make semaglutide bloating dramatically worse
Diet is the single most controllable factor in managing bloating on semaglutide. What you eat matters more on this medication than it ever did before, because the delayed gastric emptying amplifies the effects of every dietary choice.
High-FODMAP foods become your enemy
FODMAP stands for fermentable oligosaccharides, disaccharides, monosaccharides, and polyols. These are short-chain carbohydrates that are poorly absorbed in the small intestine and rapidly fermented by gut bacteria. Under normal circumstances, many people tolerate FODMAPs without issues. But when gastric transit is slowed by semaglutide, these compounds spend more time in contact with intestinal bacteria, producing significantly more gas.
The high-FODMAP foods most likely to trigger semaglutide bloating include:
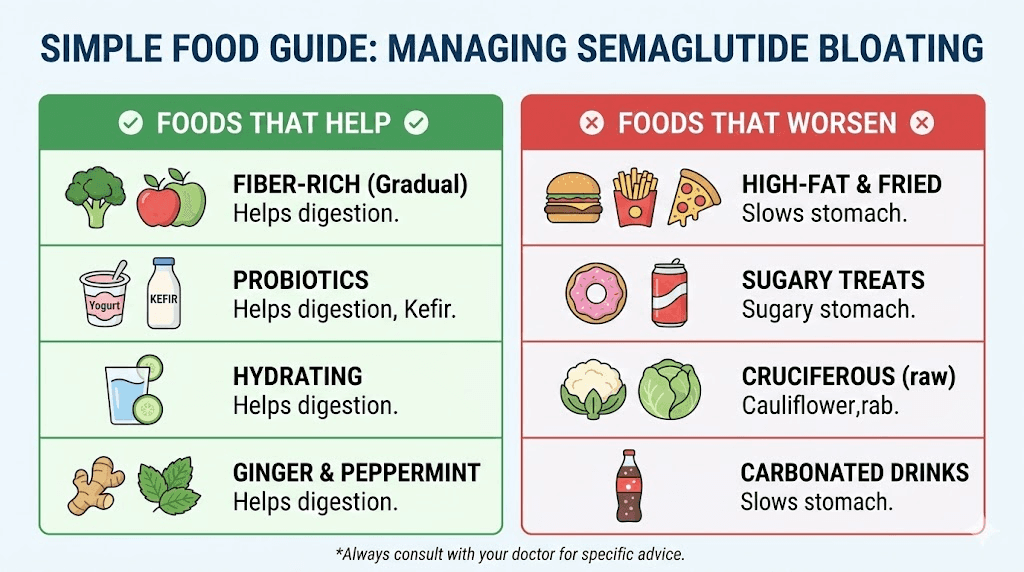
Vegetables: Onions, garlic, asparagus, artichokes, cauliflower, mushrooms, and snow peas. Cruciferous vegetables like broccoli, cabbage, and Brussels sprouts are particularly problematic because they contain both FODMAPs and sulfur compounds that increase gas production through multiple pathways.
Fruits: Apples, pears, watermelon, cherries, mangoes, and dried fruits. These contain high levels of fructose or sorbitol that ferment readily in a slow-moving gut.
Grains: Wheat and rye in large quantities. The fructans in these grains become more problematic when digestion is delayed.
Legumes: Beans, lentils, and chickpeas. These are notorious gas producers even without semaglutide. On it, they become almost guaranteed to cause severe bloating.
Dairy: Milk, soft cheeses, yogurt, and ice cream if you have any degree of lactose sensitivity. Semaglutide does not cause lactose intolerance, but it can unmask mild sensitivities that previously went unnoticed.
Users following a structured eating plan for GLP-1 therapy consistently report less bloating than those eating without consideration for these triggers. The principles are similar across semaglutide and tirzepatide, though tirzepatide users may have slightly different trigger profiles due to the additional GIP receptor activation.
Carbonated beverages are a direct cause
This one is simple. Carbonated drinks introduce carbon dioxide directly into a stomach that is already struggling to empty. The gas has nowhere to go quickly because the pyloric sphincter is holding tighter than usual under GLP-1 influence. The result is immediate, sometimes dramatic, abdominal distension.
Sparkling water, sodas, beer, champagne, kombucha. All of them will make bloating worse. If bloating is a significant issue, eliminate carbonation completely for at least 2 weeks and assess the difference. Many users report this single change reduces their bloating by 30-40%.
High-fat meals slow things down even further
Fat independently delays gastric emptying. Combined with semaglutide, which is already delaying it, high-fat meals create a compounding effect that can leave food in your stomach for 8+ hours. Fried foods, heavy cream sauces, fatty cuts of meat, and oil-heavy dishes are among the worst offenders.
This does not mean you need to eliminate fat entirely. Healthy fats in moderate amounts are important for nutrient absorption and satiety. But the portion and preparation method matter. Baked chicken breast causes far less bloating than fried chicken. Avocado in reasonable amounts is tolerated better than a cheese-heavy pasta. The foods to avoid on GLP-1 therapy overlap significantly with the list of foods that worsen bloating, which makes compliance easier once you identify the pattern.
Artificial sweeteners and sugar alcohols
Sugar alcohols like sorbitol, mannitol, xylitol, and maltitol are found in sugar-free candies, gum, protein bars, and many "diet" products. These compounds are already poorly absorbed under normal conditions, which is why they cause gas and bloating for many people even without medication. Add semaglutide to the equation and the fermentation potential multiplies.
Even some artificial sweeteners that do not contain sugar alcohols can affect gut bacteria in ways that increase gas production. If you are consuming sugar-free products regularly and experiencing significant bloating, try eliminating them for a trial period.
Foods that actually help reduce semaglutide bloating
Not everything is about avoidance. Some foods actively assist your digestive system in managing the slower transit time.
Low-FODMAP options that work
Proteins: Chicken, turkey, fish, eggs, and firm tofu are all well-tolerated and unlikely to cause additional gas production. Protein is also critical for maintaining muscle mass during semaglutide weight loss, making it doubly important.
Vegetables: Zucchini, bell peppers, carrots, spinach, lettuce, tomatoes, and green beans are generally well-tolerated. These provide fiber without the high fermentation potential of cruciferous vegetables.
Grains: Rice, oats, and quinoa tend to cause less bloating than wheat-based products. Sourdough bread is often better tolerated than regular bread because the fermentation process breaks down some of the problematic fructans.
Fruits: Bananas (especially slightly unripe), blueberries, strawberries, oranges, and grapes are lower in FODMAPs and less likely to trigger gas production.
Ginger and peppermint as natural prokinetics
Ginger has demonstrated prokinetic effects in clinical studies, meaning it helps stimulate gastric motility. For semaglutide users dealing with bloating, ginger tea after meals or small amounts of fresh ginger incorporated into food can provide genuine relief. The mechanism involves ginger compounds interacting with serotonin receptors in the GI tract, promoting coordinated muscular contractions.
Peppermint works through a different pathway. It relaxes the smooth muscle of the GI tract, which can relieve the cramping component of bloating. Peppermint tea between meals is a well-studied approach. Enteric-coated peppermint oil capsules are even more effective for lower GI bloating because they bypass the stomach and release in the intestines where they are most needed.
Neither ginger nor peppermint will override the fundamental gastric emptying delay that semaglutide causes. But both can reduce the severity of bloating symptoms while your body adapts.
Proven strategies to reduce semaglutide bloating
Beyond food choices, several evidence-based approaches can make a meaningful difference. Some are simple behavioral changes. Others involve specific supplements or techniques. All of them work best when combined rather than used in isolation.
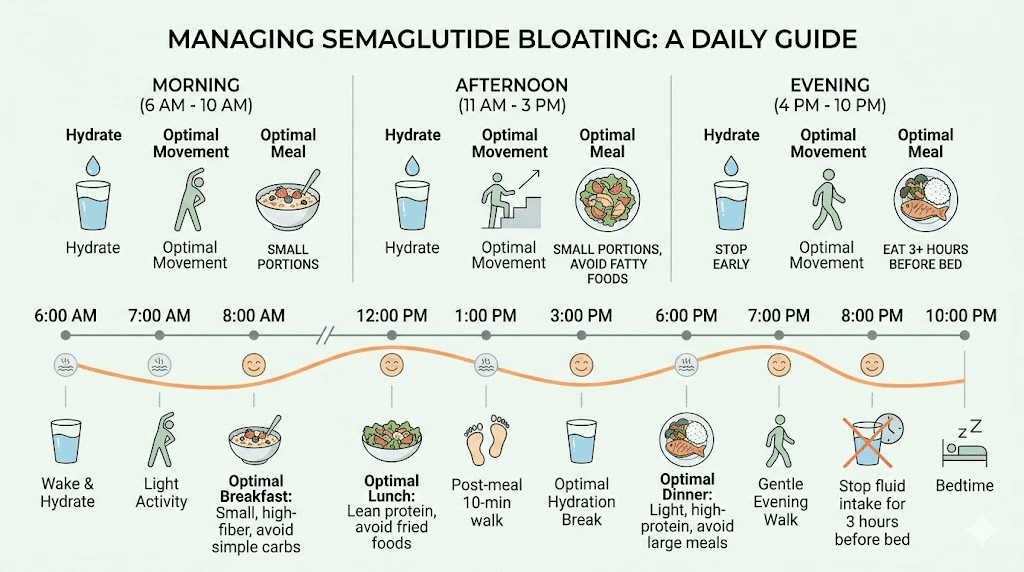
Eat smaller, more frequent meals
This is the single most effective strategy. A stomach that is already emptying slowly simply cannot handle the same meal volumes it processed before semaglutide. Three large meals need to become five or six smaller ones. Aim for portions that are 50-60% of your pre-semaglutide meal size.
The math works like this. If your stomach now takes 5-6 hours to empty instead of 2-3, then eating a large meal every 4 hours means your stomach never fully empties before the next meal arrives. That creates a stacking effect where each meal adds to the distension from the previous one. Smaller meals give your stomach a chance to make meaningful progress between eating sessions.
Chew thoroughly and eat slowly
Rushed eating causes you to swallow air, which adds directly to gastric distension. Chewing food into smaller particles also reduces the mechanical work your stomach needs to do, potentially speeding up the emptying process even under GLP-1 influence. Aim for 20-30 chews per bite. It feels excessive at first but becomes automatic within a week.
Stay upright after meals
Gravity assists gastric emptying. Lying down after eating removes this advantage and can worsen reflux, which often coexists with bloating on semaglutide. Stay upright for at least 30-60 minutes after meals. A gentle 10-15 minute walk after eating is even better because the physical movement stimulates peristalsis throughout the GI tract.
Time your injection strategically
Some users find that semaglutide injection timing affects their bloating pattern. The medication reaches peak plasma levels approximately 1 to 3 days after injection. If your worst bloating consistently falls on certain days, try adjusting your injection day so that peak levels coincide with days when you can eat most carefully and have the most control over your diet.
For example, if you inject on Friday and find Saturday and Sunday bloating unbearable because of weekend social eating, consider switching to Monday or Tuesday injection instead. The appetite suppression timeline also shifts with injection timing, which can help you naturally eat less during peak bloating periods.
Hydration matters more than you think
Adequate water intake supports digestive function and helps soften stool, reducing the constipation component of bloating. But timing matters. Drinking large amounts of water during meals fills stomach volume and can worsen immediate postprandial bloating. Instead, focus on sipping water throughout the day between meals.
Aim for at least 64 ounces daily, more if you are physically active or in a warm climate. Some users find that warm water is tolerated better than cold, possibly because warmth relaxes gastric smooth muscle.
Physical activity as digestive support
Regular exercise is one of the most underrated bloating remedies. Physical activity stimulates the migrating motor complex, the wave-like contractions that move food and gas through the intestines. Even moderate activity like walking, cycling, or yoga can significantly reduce bloating within 30 minutes.
Yoga specifically has evidence supporting its use for digestive complaints. Poses that involve twisting the torso can help release trapped gas. Forward folds compress the abdomen and stimulate peristalsis. Consistent yoga practice has been shown to improve overall GI motility in multiple clinical studies. If semaglutide fatigue makes vigorous exercise difficult, gentle movement is still beneficial and often more practical during the adaptation period.
Supplements and over-the-counter remedies that actually work
Not every supplement marketed for bloating deserves your money. Here is what the evidence supports, what might help, and what is a waste of time.
Simethicone (Gas-X, Mylanta Gas)
Simethicone works by reducing the surface tension of gas bubbles in the stomach and intestines, allowing them to coalesce into larger bubbles that are easier to pass. It does not reduce gas production, but it makes existing gas less uncomfortable and easier to expel. For semaglutide bloating that involves significant gas, simethicone provides reliable, fast-acting relief with essentially zero side effects. It is not absorbed systemically and does not interact with semaglutide.
Take 80-125mg after meals as needed. Some users find taking it prophylactically before meals that they know will be triggering is more effective than waiting for symptoms.
Digestive enzymes
Alpha-galactosidase (sold as Beano) specifically breaks down the complex sugars in legumes and cruciferous vegetables that your body cannot digest on its own. If you do not want to completely eliminate these foods, taking alpha-galactosidase before meals that contain them can substantially reduce gas production.
Broader digestive enzyme supplements containing lipase (for fats), protease (for proteins), and amylase (for starches) may help some users by supporting the digestive process that is being slowed by semaglutide. The evidence for these is less robust than for simethicone, but many users report subjective improvement.
Probiotics with specific strains
Not all probiotics are equal for bloating. Research on GLP-1 agonists and gut microbiome interactions suggests that specific strains may be more beneficial than others. Lactobacillus reuteri DSM 17938 has evidence for improving GI motility. Bifidobacterium lactis HN019 has been studied for reducing bloating and constipation. Multi-strain products that include these species along with Lactobacillus acidophilus may provide the best overall support.
Start with a low-dose probiotic and increase gradually. Introducing too many new bacteria into a gut that is already under the stress of altered motility can temporarily worsen bloating before it improves. Give any probiotic trial at least 2-3 weeks before judging effectiveness.
Fiber supplements (use carefully)
This is a nuanced area. Fiber can help reduce constipation-related bloating but can also worsen gas-related bloating depending on the type. Soluble fiber like psyllium husk (Metamucil) absorbs water and softens stool, helping move things along the colon. Start with a very small dose (half the recommended amount) and increase slowly.
Avoid insoluble fiber supplements if bloating is your primary concern. Insoluble fiber adds bulk but does not dissolve in water, and it can increase gas production in a slow-moving gut. The slow-fermenting soluble fibers are the better choice for semaglutide users because they support microbial metabolism while minimizing the rapid gas production that causes distension.
What does not work (save your money)
Activated charcoal for semaglutide bloating is popular in online forums but has significant drawbacks. It can interfere with medication absorption, including semaglutide itself. The timing required to avoid interactions (2 hours before or after any other medication or food) makes it impractical for daily use. And its effectiveness for the type of bloating caused by delayed gastric emptying is minimal.
Detox teas, colon cleanses, and extreme elimination diets are also unnecessary and potentially harmful. The bloating is caused by a known mechanism with a known timeline for improvement. Drastic interventions create more problems than they solve.
Adjusting your semaglutide protocol to reduce bloating
Sometimes the answer is not about managing symptoms around the medication but rather adjusting the medication itself. This should always be discussed with your healthcare provider, but understanding the options helps you have a more productive conversation.
Slower dose escalation
If bloating is severe at a particular dose, staying at that dose for an additional 2-4 weeks before escalating can make a significant difference. The standard titration schedule is a guideline, not a mandate. Extending the time at each dose level gives your GI tract more adjustment time and often results in better tolerance at higher doses when you eventually reach them.
This is particularly relevant for users who experienced little to no bloating at lower doses but find the transition to the 1.0mg or 1.7mg level overwhelming. Your body may simply need more time. Rushing through the titration to reach the therapeutic dose faster often backfires with worsening GI symptoms and higher discontinuation rates.
Dose reduction and stabilization
For users who have reached the full 2.4mg dose and find bloating intolerable despite dietary modifications and OTC remedies, dropping back to 1.7mg or even 1.0mg may be appropriate. Research shows that weight loss still occurs at lower doses, though more slowly. The tradeoff between tolerability and rate of weight loss is a personal decision, but staying on a tolerable dose long-term is almost always better than cycling on and off the maximum dose.
Compounded formulations and alternatives
Some users who struggle with bloating on standard semaglutide find that semaglutide with glycine formulations offer better GI tolerance. Glycine is an amino acid with its own GI-calming properties that may partially offset the motility-slowing effects of semaglutide. Similarly, semaglutide combined with B12 is reported by some users to cause fewer digestive issues, though this could relate to overall improved metabolic function rather than a direct anti-bloating effect.
For users considering alternatives, understanding the side effect differences between semaglutide and tirzepatide is valuable. Switching between GLP-1 agonists is sometimes the answer when one medication causes intolerable GI effects but the therapeutic benefits are too significant to abandon entirely.
How semaglutide bloating compares across different GLP-1 medications
Bloating is not unique to semaglutide. Every medication that activates GLP-1 receptors will slow gastric emptying to some degree. But the severity and character of bloating can differ between agents.
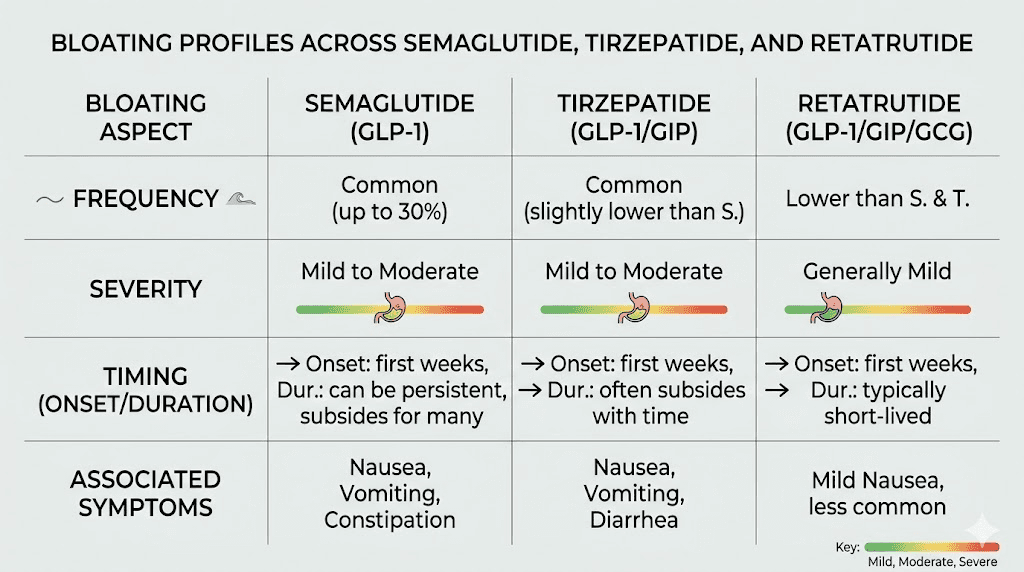
Semaglutide versus tirzepatide bloating
Tirzepatide is a dual GLP-1/GIP receptor agonist that also causes significant GI side effects. However, the GIP receptor activation may modify the bloating profile somewhat. Some users who switch from semaglutide to tirzepatide report less bloating but more nausea, while others experience the opposite pattern. The dosage equivalence between the two medications is not straightforward, which complicates direct comparison.
In head-to-head clinical trials, the overall GI adverse event rates are broadly similar between semaglutide 2.4mg and tirzepatide at its maximum dose. Constipation patterns on tirzepatide show similar frequency to semaglutide, suggesting that the delayed transit mechanism affects the entire GI tract similarly regardless of whether one or two receptors are being activated.
Oral versus injectable semaglutide
Oral semaglutide formulations may produce a different bloating profile because the medication is absorbed through the GI tract rather than reaching it systemically after subcutaneous injection. Some users report more upper GI symptoms (nausea, early satiety) with oral formulations but less lower GI bloating. Others find the opposite. Individual response varies significantly, and there is limited head-to-head data specifically comparing bloating severity between formulations.
Newer triple agonists
Retatrutide, the investigational triple agonist targeting GLP-1, GIP, and glucagon receptors, showed higher overall GI event rates in Phase 2 trials at its highest doses. The addition of glucagon receptor activation creates additional metabolic effects that may modify the bloating experience, though detailed comparative data on specific symptoms like bloating is limited. As this class of medications continues to expand, understanding the GI implications of each receptor target becomes increasingly important.
The gut microbiome connection and why it matters for semaglutide bloating
Emerging research is revealing a bidirectional relationship between GLP-1 agonists and the gut microbiome that has direct implications for bloating management.
Studies have shown that semaglutide treatment increases populations of Akkermansia muciniphila, a bacteria associated with healthy metabolic function, while decreasing overall microbial diversity. This shift in bacterial composition can change gas production patterns, alter the types of short-chain fatty acids being produced, and modify how your gut processes different foods.
What does this mean practically? It means that bloating on semaglutide is not purely a motility issue. The medication is changing who lives in your gut, and those new residents process food differently than the ones they replaced. This is one reason why bloating patterns can shift over time even at a stable dose. Your microbiome is adapting along with the rest of your digestive system.
Supporting your microbiome during semaglutide treatment
Prebiotic foods that feed beneficial bacteria can help support a healthier microbial transition. But here is the catch: many prebiotic foods are high in FODMAPs, which means they can worsen bloating in the short term. The strategy is to introduce them gradually and in small amounts.
Fermented foods like plain yogurt, kefir, sauerkraut, and kimchi provide both probiotics and prebiotics. Start with very small servings (a tablespoon) and increase as tolerated. These foods can feel counterintuitive when your stomach is already uncomfortable, but consistent small exposures help build a more resilient microbial community that ultimately produces less problematic gas.
Fiber from slow-fermenting sources is preferable to rapid-fermenting options. Oats, chia seeds in moderation, and cooked vegetables produce less immediate gas than raw cruciferous vegetables or large amounts of fruit. The goal is to feed your gut bacteria without overwhelming them.
Special considerations for specific populations
Not everyone experiences semaglutide bloating the same way, and certain groups face unique challenges.
Users with pre-existing IBS
Irritable bowel syndrome affects approximately 10-15% of the global population, and many IBS sufferers also seek treatment for weight management. Adding semaglutide to an already sensitive GI tract can be particularly challenging. The baseline motility patterns in IBS (which can be either too fast or too slow depending on the subtype) interact with semaglutide delayed emptying in complex ways.
IBS-C (constipation-predominant) sufferers may experience amplified bloating because their colonic transit is already slow. IBS-D (diarrhea-predominant) sufferers sometimes actually report improvement in their diarrhea on semaglutide because the slowed transit normalizes their previously too-rapid motility. But bloating often increases as a tradeoff.
If you have IBS, working with a gastroenterologist alongside your prescribing provider is strongly recommended when starting semaglutide. The combination of a low-FODMAP diet (which many IBS patients already follow) with gradual semaglutide titration tends to produce the best outcomes.
Users on combination medications
Several medications can compound the bloating effect of semaglutide. Opioid pain medications slow GI motility independently and can create severe constipation and bloating when combined with semaglutide. Anticholinergic medications (some antidepressants, antihistamines, and bladder medications) also reduce GI motility. Calcium channel blockers can affect smooth muscle function throughout the digestive tract.
If you take any of these medications and experience severe bloating on semaglutide, mention the combination to your healthcare provider. Dose timing adjustments or medication alternatives may reduce the cumulative GI impact. Users considering combining phentermine with semaglutide should be aware that phentermine can also affect GI function, though typically in the opposite direction (stimulant effects may partially offset semaglutide slowing).
Users with gallbladder concerns
Rapid weight loss from any cause increases the risk of gallstone formation. Semaglutide-mediated weight loss is no exception. Gallbladder sludge and stones can cause bloating, right upper quadrant pain, and nausea that mimics but is distinct from semaglutide GI side effects. If your bloating is primarily in the upper right abdomen and worsens specifically after fatty meals with sharp or colicky pain, gallbladder involvement should be evaluated.
A complete weekly protocol for managing semaglutide bloating
Pulling everything together into a structured approach makes it far more likely that you will actually implement these changes consistently. Here is a week-by-week management protocol.
Protocol for the first 4 weeks of a new dose
Daily structure:
5-6 small meals rather than 2-3 large ones
Low-FODMAP food choices at every meal
No carbonated beverages
64+ ounces of water sipped between meals
10-15 minute walk after lunch and dinner
Simethicone as needed after meals (80-125mg)
Ginger tea after the largest meal of the day
Weekly monitoring:
Rate your bloating 1-10 each day
Note which foods triggered the worst episodes
Track bowel movement frequency
If constipation develops, add psyllium husk (start at half dose)
Assessment at week 4:
If bloating has decreased by 50% or more, continue current management and proceed with dose escalation if scheduled
If bloating remains severe despite strict dietary compliance, discuss extended time at current dose with your provider
If warning signs of gastroparesis appear at any point, stop semaglutide and seek immediate medical evaluation
Long-term maintenance protocol
Once you have adapted to your target dose and bloating has become manageable:
Gradually reintroduce moderate-FODMAP foods one at a time, spacing reintroductions 3 days apart to identify individual triggers
Maintain smaller meal sizes as a permanent habit (this supports both bloating management and weight maintenance)
Continue daily walking or other regular physical activity
Keep simethicone available for occasional flares, especially during social eating situations where food choices are less controlled
Consider a maintenance probiotic with Lactobacillus and Bifidobacterium strains
Researchers who track their protocols through SeekPeptides member tools find that systematic logging of food triggers and symptom patterns accelerates the identification of personal bloating triggers. What bothers one person may be perfectly tolerated by another. The only way to know your specific trigger profile is to track it carefully.
When to talk to your doctor about semaglutide bloating
Most semaglutide bloating is manageable with the dietary and lifestyle strategies described above. But certain situations warrant professional medical evaluation without delay.
Seek medical attention if you experience
Bloating that worsens progressively over 2+ weeks despite strict dietary compliance
Severe abdominal pain that limits daily activities
Inability to eat more than a few bites without feeling painfully full
Vomiting undigested food 4+ hours after eating
No bowel movement for 4+ days despite fiber and hydration
Blood in stool or vomit
Unexplained fever with abdominal distension
Right upper quadrant pain (possible gallbladder involvement)
Signs of dehydration (dark urine, dizziness, rapid heart rate)
Your healthcare provider may order imaging studies, adjust your semaglutide dose, prescribe prokinetic medications to support gastric emptying, or evaluate for conditions unrelated to semaglutide that may be contributing to the symptoms.
Questions to ask your provider
Going to an appointment prepared makes the conversation more productive. Consider asking:
Should I stay at my current dose longer before escalating?
Would a prokinetic medication like metoclopramide be appropriate for short-term use?
Should I have a gastric emptying study to rule out gastroparesis?
Are any of my other medications contributing to the bloating?
Would switching to a different GLP-1 agonist be worth trying?
Understanding the expected timeline for semaglutide effects helps you frame these questions. If bloating is your only significant side effect and weight loss is progressing, the risk-benefit calculation may favor persistence with management strategies. If bloating is accompanied by other concerning symptoms or weight loss has stalled, a protocol change may be warranted.
Alcohol and semaglutide bloating
Drinking alcohol on semaglutide introduces several bloating-specific risks. Alcohol irritates the GI lining, increases stomach acid production, and can independently slow gastric emptying. Combined with semaglutide, even moderate alcohol consumption can produce dramatic bloating that lasts well into the next day.
Beer is the worst offender because it combines alcohol with carbonation and fermentable carbohydrates. Wine is slightly better tolerated but still problematic for many users. Clear spirits in small amounts tend to cause the least additional bloating, though they still carry the other risks of alcohol consumption during GLP-1 therapy.
If you choose to drink occasionally while on semaglutide, eat a small, low-fat, low-FODMAP meal first. Limit yourself to 1-2 drinks maximum. Avoid beer and carbonated mixers entirely. And expect some degree of increased bloating for 24-48 hours afterward.
The psychological impact of persistent bloating
This is rarely discussed but genuinely important. Persistent bloating on semaglutide can create a frustrating paradox. You are taking the medication to improve your body composition and health, but the visible abdominal distension makes you feel like your midsection looks worse, not better. This can undermine motivation, trigger body image concerns, and lead to premature discontinuation of a medication that is otherwise working well.
Understanding that bloating is temporary and not the same as fat gain is crucial. The distension from gas and retained food is not adding body fat. Your weight loss is still happening underneath the bloating. Many users report a dramatic "whoosh" effect when bloating finally resolves at a stable dose, where weeks of hidden weight loss suddenly become visible.
If the psychological impact of bloating is significant, consider taking measurements (waist circumference) at the same time each day, first thing in the morning before eating when bloating is typically at its minimum. This gives you a more accurate picture of actual body composition changes rather than the variable distension that fluctuates throughout the day.
SeekPeptides members often find that connecting with others who have navigated the same adjustment period provides invaluable perspective. Knowing that thousands of others have pushed through the same uncomfortable weeks and come out the other side with both the bloating resolved and significant weight loss achieved can make the temporary discomfort much more tolerable.
Semaglutide bloating and exercise performance
For physically active users, bloating raises practical concerns about exercise timing and performance. Training with a distended, uncomfortable abdomen is not just unpleasant. It can actually impair performance by limiting diaphragmatic movement, causing side stitches, and reducing the desire to push hard during workouts.
Timing solution: Schedule your most intense training sessions during your lowest-bloating periods. For most users, this means morning workouts before eating, or evening workouts at least 3-4 hours after the last meal. The energy effects of semaglutide may also influence optimal training timing.
Training type considerations: High-impact activities (running, jumping) tend to be more uncomfortable during bloating than low-impact options (cycling, swimming, weight training). Core-intensive exercises can worsen the sensation of abdominal pressure. During peak bloating periods, prioritize training modalities that are less affected by abdominal distension.
Competition/event preparation: If you have a specific athletic event, consider timing your dose escalation around it. Do not increase your semaglutide dose in the week before a competition or race. The 3-5 day post-escalation bloating peak could significantly impact performance.
Frequently asked questions
Does semaglutide bloating ever go away completely?
For most users, yes. Clinical data shows that GI symptoms including bloating are substantially reduced after approximately 20 weeks of consistent use at a stable dose. Some users experience complete resolution. Others retain mild, intermittent bloating that is easily managed with dietary awareness. Fewer than 5% of clinical trial participants discontinued treatment specifically due to GI adverse events, suggesting that the vast majority found their symptoms tolerable over time.
Is bloating worse with higher semaglutide doses?
Generally, yes. The GI effects of semaglutide are dose-dependent. Each dose increase can trigger a temporary resurgence of bloating that subsides as the body adapts. The specific dose measured in units correlates with the degree of gastric emptying delay, which directly drives bloating severity.
Can I take a probiotic with semaglutide?
Yes. Probiotics do not interact with semaglutide and are generally safe to take concurrently. Look for strains with evidence for GI motility support, particularly Lactobacillus reuteri DSM 17938 and Bifidobacterium lactis HN019. Start with a low dose and increase gradually to avoid temporary worsening of bloating.
Should I take semaglutide with food to reduce bloating?
Semaglutide is a subcutaneous injection, so it does not need to be taken with food. However, eating patterns around your injection day can affect how you experience bloating. Some users find that eating lighter on injection day and the following day reduces the initial GI impact. Using the semaglutide dosage calculator to ensure accurate dosing also helps prevent inadvertent overdosing that would worsen side effects.
Will switching to compounded semaglutide help with bloating?
Compounded semaglutide contains the same active ingredient as brand-name products, so the fundamental GI effects are the same. However, some compounded formulations include additional ingredients like glycine or methylcobalamin that may modestly improve GI tolerance. Individual responses vary, and switching formulations is worth discussing with your provider if bloating remains problematic.
Is semaglutide bloating dangerous?
In the vast majority of cases, no. Clinical trial data shows that 99.5% of GI adverse events were classified as non-serious and 98.1% as mild to moderate. However, severe cases can progress to gastroparesis, which requires medical attention. Knowing the full spectrum of semaglutide effects helps you distinguish between normal adaptation and concerning symptoms.
Does the time of day I inject semaglutide affect bloating?
There is no definitive clinical data on this, but user reports suggest that morning injections may produce more daytime bloating while evening injections shift the peak GI effects to overnight (when you are sleeping and not eating). Experiment with timing to find what works best for your schedule and eating patterns.
Can semaglutide bloating cause weight gain?
No. Bloating is caused by gas and retained food, not fat accumulation. It can make the scale fluctuate by 2-5 pounds on any given day due to retained food and water, but this is not true weight gain. Users concerned about not losing weight on semaglutide should focus on weekly weight trends rather than daily fluctuations, which are heavily influenced by bloating status.
External resources
For researchers serious about optimizing their GLP-1 protocols while managing side effects effectively, SeekPeptides provides the most comprehensive resource available. Members access evidence-based protocol guides, personalized dosing tools, side effect management databases, and a community of thousands who have navigated these exact challenges. From peptide calculators to detailed dosage charts, the platform gives you the tools to make informed decisions rather than guessing your way through treatment.
In case I do not see you, good afternoon, good evening, and good night. May your stomach stay comfortable, your meals stay enjoyable, and your GLP-1 journey stay on track.