Feb 28, 2026

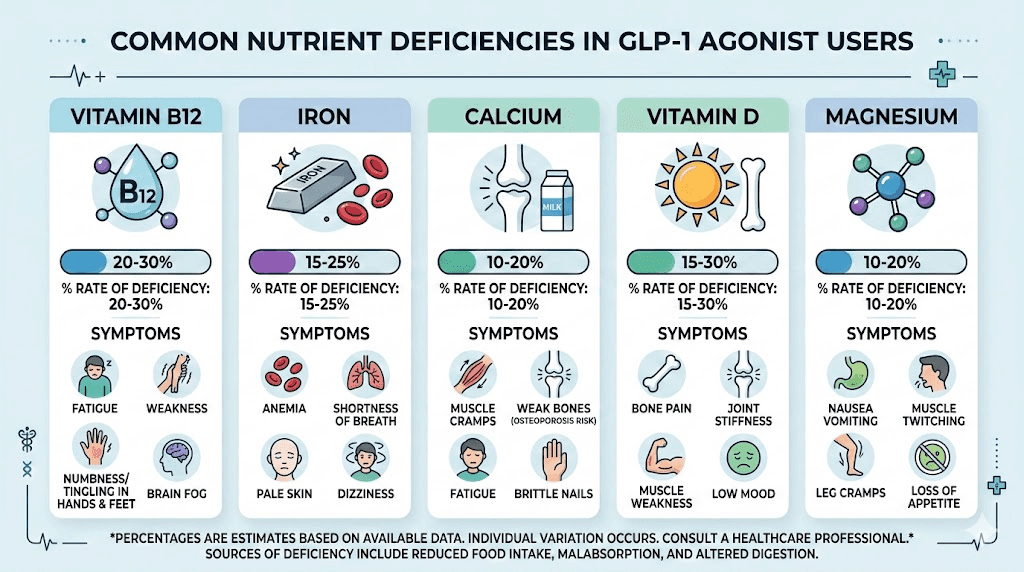
Nearly one in four people on GLP-1 medications develop a nutritional deficiency within their first year. Not a minor dip. A clinical deficiency, the kind that shows up on blood work and manifests as fatigue, brain fog, muscle cramps, and bone loss. A retrospective study of 461,382 GLP-1 users found that 22.4% received a new nutritional deficiency diagnosis within 12 months of starting therapy. Vitamin D led the list at 13.6%, followed by B vitamins, calcium, and iron.
The math is straightforward. GLP-1 receptor agonists like semaglutide and tirzepatide suppress appetite so effectively that caloric intake drops 16-39%. Fewer calories means fewer vitamins, fewer minerals, fewer of the building blocks your body needs to function. And this is not a small problem that resolves on its own. The longer you stay on therapy, the deeper the deficiency grows.
What makes this particularly tricky is that the symptoms of nutrient depletion often mimic GLP-1 side effects. That persistent fatigue? Could be the medication. Could also be a B12 deficiency slowly eroding your nerve function. The muscle cramps keeping you up at night? Maybe GLP-1 fatigue. Or maybe your magnesium levels have dropped below the threshold your muscles need to relax properly. Without targeted supplementation and regular blood work, you are essentially flying blind.
This guide covers every vitamin and mineral that matters during GLP-1 therapy. Not the generic advice you have seen recycled across health blogs. Specific nutrients, specific dosages, specific timing, and specific interactions you need to watch for. Whether you are on semaglutide, tirzepatide, or retatrutide, the nutritional gaps are real, and closing them can mean the difference between losing weight while feeling terrible and losing weight while actually thriving.
Why GLP-1 medications create vitamin deficiencies
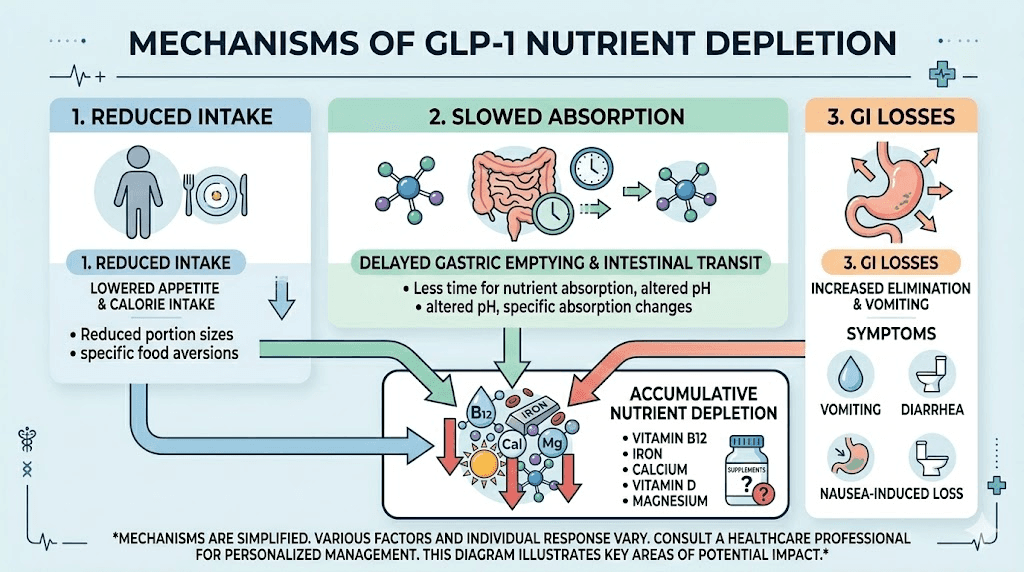
Understanding why these deficiencies happen is the first step toward preventing them. GLP-1 receptor agonists work through multiple mechanisms that directly impact nutrient absorption and intake, and each mechanism creates its own set of nutritional challenges.
Reduced food intake and caloric restriction
The primary mechanism is simple. You eat less. GLP-1 medications suppress appetite by acting on hunger centers in the brain and slowing gastric emptying. Research shows caloric reductions between 16% and 39% depending on the medication and dose. At the high end, someone consuming 2,000 calories daily might drop to 1,220 calories. That is below the threshold where most people can meet their micronutrient needs through food alone.
Think about it this way. Your body requires roughly the same amount of vitamins and minerals regardless of how many calories you consume. Vitamin D requirements do not decrease because your appetite shrunk. Your bones still need the same calcium. Your nerves still demand the same B12. But when food intake drops dramatically, the only way to bridge that gap is deliberate supplementation.
The joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society specifically flagged this concern. Their guidance recommends proactive supplementation for nutrients including iron, calcium, magnesium, zinc, and vitamins A, D, E, K, B1, B12, and C during active GLP-1 therapy.
Slowed gastric emptying and absorption changes
GLP-1 agonists slow digestion significantly. Food sits in your stomach longer. This is partly how they reduce appetite, but it also changes how nutrients are absorbed. Some vitamins and minerals require specific pH conditions and transit times for optimal absorption, and altered gut motility can disrupt these processes.
B12 absorption is particularly affected. This vitamin requires intrinsic factor, a protein produced by stomach cells, to be absorbed in the small intestine. When gastric emptying slows and stomach acid production changes, the entire B12 absorption cascade can break down. This is not theoretical. Case reports have documented severe B12 deficiency in GLP-1 users, including cases progressing to neurological symptoms.
The gut microbiome also shifts during GLP-1 therapy. Changes in transit time, stomach acid, and food composition alter the bacterial populations that help synthesize certain vitamins and facilitate mineral absorption. The downstream effects ripple through your entire nutritional status.
Gastrointestinal side effects compound the problem
Nausea affects 44% of semaglutide users and 28% of tirzepatide users in clinical trials. Vomiting hits 24% and 13% respectively. Diarrhea affects 30% and 23%. These are not minor inconveniences. Each episode of vomiting or diarrhea strips nutrients from your body before they can be absorbed.
When you are already eating less, losing nutrients through GI side effects creates a double hit. Your intake is down and your losses are up. This is why the first few months of GLP-1 therapy, when side effects are most common and dose titration is happening, represent the highest risk period for developing deficiencies.
Constipation, which affects roughly one in four users, presents its own challenges. While it does not directly cause nutrient loss, it often leads people to reduce fiber intake further, which compounds the problem of inadequate nutrition.
The weight loss factor
Rapid weight loss itself depletes certain nutrients. Fat-soluble vitamins, including A, D, E, and K, are stored in adipose tissue. As fat cells shrink during weight loss, these vitamins are released into circulation and then metabolized or excreted at higher rates. This paradoxically means that even though fat stores are releasing these vitamins, overall levels can still decline because the body is processing them faster than they are being replaced.
The STEP 1 trial for semaglutide showed average weight reduction of 13.6 kg, with 62% coming from fat mass and 38% from lean body mass. Losing that much tissue, both fat and muscle, requires adequate nutrients for tissue remodeling. Without them, side effects like hair loss and muscle weakness become more likely.
Essential vitamins for GLP-1 users
Not all vitamins carry equal risk during GLP-1 therapy. Some deplete faster. Some cause more severe symptoms when levels drop. Some interact with the medications in ways that require careful timing. Here is what the research actually shows for each critical vitamin, along with the specific forms and dosages that work best during peptide-based weight loss therapy.
Vitamin D: the most common deficiency
Vitamin D tops every list for a reason. In the large retrospective study of 461,382 GLP-1 users, vitamin D deficiency was diagnosed in 7.5% at six months and 13.6% at twelve months. GLP-1 users showed a 49% higher risk for vitamin D deficiency compared to people on SGLT2 inhibitors and a 32% higher risk compared to those on DPP-4 inhibitors. These are not small differences.
Why does vitamin D deplete so quickly? Three reasons working simultaneously. First, reduced food intake means less dietary vitamin D from fatty fish, fortified dairy, and eggs. Second, vitamin D is fat-soluble and gets redistributed during rapid fat loss. Third, many GLP-1 users were already borderline deficient before starting therapy, since obesity itself is associated with lower vitamin D levels due to sequestration in adipose tissue.
The consequences of vitamin D deficiency during weight loss are serious. Bone mineral density decreases, and one randomized trial demonstrated that GLP-1 therapy alone decreased bone mineral density while GLP-1 therapy plus exercise preserved it. Without adequate vitamin D, calcium absorption drops to roughly 10-15% of dietary intake compared to 30-40% with sufficient levels. For someone already eating less calcium, this creates a bone health crisis that will not announce itself until damage is done.
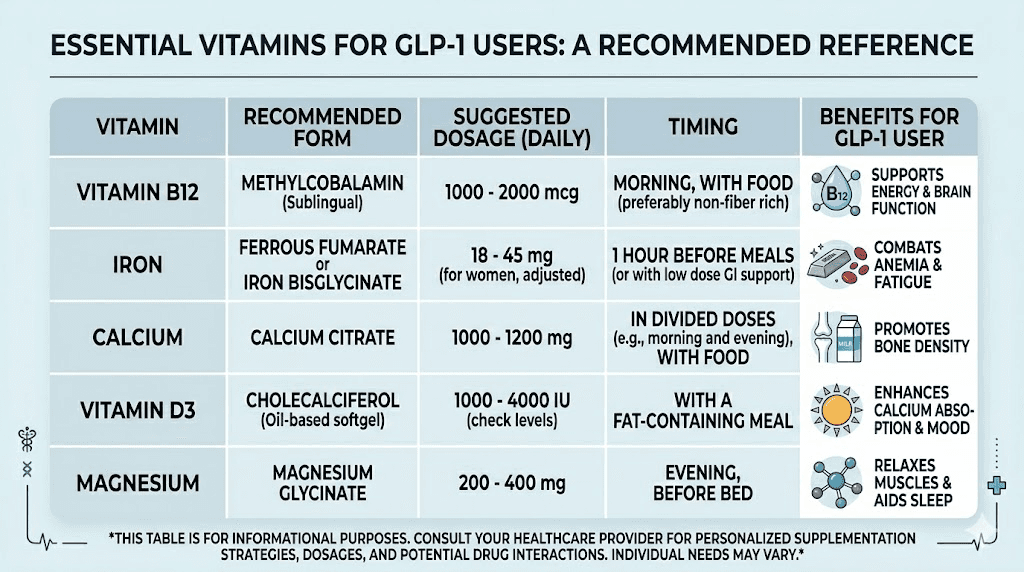
Recommended form: Vitamin D3 (cholecalciferol), paired with K2 (MK-7 form) for optimal calcium routing. D3 is more effective than D2 at raising and maintaining blood levels.
Suggested dosage: 2,000-5,000 IU daily, depending on baseline levels. Ask for a 25-hydroxyvitamin D blood test. Optimal range is 40-60 ng/mL. Many GLP-1 users need the higher end of supplementation.
Timing: Take with your largest meal containing fat, since D3 is fat-soluble and absorption improves significantly when consumed with dietary fat.
Vitamin B12: the silent nerve destroyer
B12 deficiency develops slowly and quietly. By the time symptoms appear, neurological damage may have already progressed. This makes it particularly dangerous for GLP-1 users, who are already dealing with a constellation of symptoms that can mask early B12 depletion.
The mechanism is well-understood. B12 absorption requires intrinsic factor from stomach parietal cells, adequate stomach acid to release B12 from food proteins, and normal small intestine function for absorption. GLP-1 medications disrupt at least two of these three steps. Slowed gastric emptying alters the timing of B12 release, and changes in stomach acid production can impair intrinsic factor binding.
Early symptoms include fatigue, weakness, and brain fog. These are easily dismissed as medication side effects or natural consequences of caloric restriction. But as deficiency deepens, numbness and tingling in hands and feet develop, followed by balance problems, depression, and in severe cases, irreversible nerve damage. Case reports in the medical literature have documented Wernicke encephalopathy and beriberi in GLP-1 users with severe B vitamin deficiencies.
Compounded GLP-1 formulations with B12 have become popular partly because of this deficiency risk. The addition of methylcobalamin or cyanocobalamin directly to the semaglutide or tirzepatide compound ensures B12 delivery bypasses the compromised digestive absorption pathway.
Recommended form: Methylcobalamin (active form) or cyanocobalamin. Sublingual or injectable forms bypass GI absorption issues entirely.
Suggested dosage: 1,000 mcg daily via sublingual tablet, or as directed if included in a compounded GLP-1 formulation.
Timing: Morning, away from other supplements that might compete for absorption. If using sublingual form, hold under tongue for 60-90 seconds before swallowing.
Other critical B vitamins
B12 gets most of the attention, but other B vitamins also deplete during GLP-1 therapy. B1 (thiamine) deficiency has produced some of the most alarming case reports, including Wernicke encephalopathy, a potentially fatal brain condition caused by severe thiamine depletion.
Folate (B9) works in tandem with B12 for DNA synthesis and red blood cell formation. When both are low, the risk of megaloblastic anemia increases significantly. This type of anemia causes oversized, dysfunctional red blood cells that cannot carry oxygen efficiently, leading to fatigue that no amount of sleep resolves.
B6 (pyridoxine) supports over 100 enzyme reactions in the body, including protein metabolism. During rapid weight loss with significant lean mass changes, adequate B6 becomes even more critical for maintaining metabolic function.
Recommended form: A quality B-complex containing methylated forms, specifically methylfolate (not folic acid) and methylcobalamin (not cyanocobalamin), plus the active forms of B1, B2, B3, B5, and B6.
Suggested dosage: Follow the label on a reputable B-complex supplement. Look for one that provides at least 100% DV for all B vitamins in their active, methylated forms.
Vitamin A: the overlooked fat-soluble
Vitamin A deficiency was identified as a significant concern in the joint advisory from four major medical organizations. As a fat-soluble vitamin stored in the liver and adipose tissue, its levels fluctuate during rapid weight loss. Reduced intake of vitamin A-rich foods like liver, eggs, sweet potatoes, and leafy greens compounds the problem.
Symptoms of vitamin A deficiency include dry eyes, night vision problems, and impaired immune function. Since many GLP-1 users focus their limited caloric intake on protein and fiber, vitamin A-rich foods often get pushed off the plate.
Recommended form: A combination of preformed vitamin A (retinyl palmitate) and provitamin A (beta-carotene) provides both immediate availability and safe long-term supplementation.
Suggested dosage: 2,500-5,000 IU daily as part of a multivitamin. Do not exceed 10,000 IU daily from supplements, as vitamin A toxicity is a real concern with fat-soluble vitamins.
Vitamin C: immune and collagen support
Vitamin C levels drop when fruit and vegetable intake decreases, which happens frequently during appetite suppression. Beyond immune function, vitamin C is essential for collagen synthesis, and during rapid weight loss, skin elasticity depends partly on adequate collagen production. It also enhances iron absorption, making it a critical co-factor for preventing iron deficiency anemia.
Recommended form: Buffered vitamin C (calcium ascorbate or sodium ascorbate) is gentler on the stomach, which matters for GLP-1 users already dealing with GI sensitivity.
Suggested dosage: 500-1,000 mg daily. Split into two doses if using higher amounts.
Vitamin E and vitamin K
Both vitamins E and K are fat-soluble and follow similar depletion patterns during GLP-1 therapy. Vitamin E serves as a powerful antioxidant protecting cells from oxidative stress, while vitamin K (particularly K2 in its MK-7 form) directs calcium into bones rather than arteries.
The synergy between vitamins D3 and K2 deserves special attention. Taking D3 without K2 increases calcium absorption but does not ensure that calcium reaches your bones. K2 activates osteocalcin, the protein that binds calcium to bone matrix. For bone health during weight loss, this combination is more important than either vitamin alone.
Recommended form: Natural vitamin E as mixed tocopherols (not synthetic dl-alpha-tocopherol). Vitamin K2 as MK-7 for its longer half-life and superior bioavailability.
Suggested dosage: Vitamin E at 200-400 IU daily. Vitamin K2 at 100-200 mcg daily, ideally paired with your vitamin D3 supplement.
Critical minerals during GLP-1 therapy
Minerals get less attention than vitamins in the GLP-1 conversation, but the deficiency rates are just as concerning. Calcium, magnesium, iron, and zinc all deplete significantly during therapy, and each carries its own set of consequences when levels fall below optimal ranges. Understanding which minerals you need, and how GLP-1 medications specifically affect their absorption, is essential for maintaining health during weight loss.
Calcium: the bone crisis nobody talks about
Rapid weight loss increases bone loss risk. This is not debatable. The research is clear. And GLP-1 medications produce rapid, substantial weight reduction, with clinical trial participants losing an average of 13.6 kg on semaglutide and up to 25% body weight in the SURMOUNT 3 tirzepatide trial. That level of weight loss, particularly when achieved over 3-4 months, significantly accelerates bone mineral density decline.
Calcium intake drops when you eat less. Dairy, sardines, fortified foods, and leafy greens all decrease when appetite is suppressed. Meanwhile, your body continues pulling calcium from bones to maintain blood calcium levels for muscle contraction, nerve signaling, and heart function. Without adequate dietary calcium plus supplementation, the deficit compounds week after week.
The bone health implications are particularly concerning for women over 40, post-menopausal women, and anyone with a family history of osteoporosis. These populations already face elevated bone loss risk, and adding GLP-1 therapy without calcium and vitamin D supplementation multiplies that risk substantially.
Recommended form: Calcium citrate (better absorbed, does not require stomach acid) rather than calcium carbonate (requires acidic environment, which may be compromised by GLP-1 effects on stomach).
Suggested dosage: 500 mg daily from supplements. Split into two doses of 250 mg if possible, since the body absorbs calcium more efficiently in smaller amounts. Target 1,000-1,200 mg total daily from food plus supplements.
Timing: Take separately from iron supplements (they compete for absorption). Take with meals for better absorption and to minimize GI upset.
Magnesium: the mineral your muscles are begging for
Magnesium deficiency may be the most under-diagnosed mineral issue in GLP-1 users. Standard blood tests measure serum magnesium, but only 1% of the body total magnesium circulates in blood. You can have severely depleted cellular magnesium and still show normal blood levels. This makes subjective symptoms, like muscle cramps, poor sleep, irritability, and heart palpitations, important diagnostic clues.
GLP-1 medications deplete magnesium through reduced food intake and, in users who also take metformin, through the additional depleting effect of that medication. The resulting deficiency causes symptoms that overlap significantly with common GLP-1 side effects. Muscle pain, insomnia, anxiety, and fatigue are all symptoms of both magnesium deficiency and GLP-1 therapy, making it nearly impossible to distinguish the cause without supplementation trials.
Magnesium also plays a critical role in glucose metabolism and insulin sensitivity. Since many GLP-1 users have type 2 diabetes or prediabetes, maintaining optimal magnesium levels supports the metabolic improvements these medications provide. Research suggests magnesium supplementation independently improves insulin sensitivity, creating a synergistic effect with GLP-1 therapy.
Recommended form: Magnesium glycinate for sleep and muscle relaxation. Magnesium citrate for constipation relief, which doubles as a benefit for GLP-1-induced constipation. Avoid magnesium oxide, which has poor absorption.
Suggested dosage: 200-400 mg daily. Start at the lower end and increase gradually. Higher doses of citrate can cause loose stools, which may actually be therapeutic for users dealing with GLP-1 constipation.
Timing: Evening is ideal for glycinate form, as it promotes relaxation and sleep. Can be taken with or without food.
Iron: especially critical for women
Iron deficiency anemia is a real risk during GLP-1 therapy, particularly for premenopausal women who lose iron monthly through menstruation. Reduced red meat intake, decreased overall food consumption, and potential GI bleeding from the gastroparesis-like effects of GLP-1 medications all contribute to declining iron stores.
Symptoms of iron deficiency include persistent fatigue that does not respond to rest, cold hands and feet, brittle nails, and unusual cravings. These can be easily attributed to caloric restriction or medication side effects, which is why blood work including ferritin levels is essential during GLP-1 therapy.
Not everyone on GLP-1 medications needs iron supplementation. Men and post-menopausal women rarely need it unless blood work confirms deficiency. Supplementing iron unnecessarily carries risks, including GI irritation that compounds existing side effects and potential iron overload in susceptible individuals.
Recommended form: Iron bisglycinate (gentlest on the stomach) or ferrous sulfate if budget is a concern. Take with vitamin C to enhance absorption.
Suggested dosage: Only as directed by blood work results. Typical therapeutic dose is 18-27 mg for maintenance or 45-65 mg for correcting deficiency. Do not self-prescribe iron supplements without lab confirmation.
Timing: Take on an empty stomach for best absorption. If stomach upset occurs, take with a small amount of food. Separate from calcium supplements by at least 2 hours.
Zinc: the immune and metabolism mineral
Zinc supports over 300 enzymatic reactions in the body, including immune function, protein synthesis, wound healing, and DNA creation. During rapid weight loss with significant tissue remodeling, zinc demands increase while intake typically decreases.
Zinc deficiency symptoms include impaired taste (which may worsen the taste changes some GLP-1 users experience), slow wound healing, frequent infections, and hair loss. Since hair loss is already a concern with rapid weight loss and GLP-1 therapy, maintaining zinc levels is one modifiable factor that can help mitigate this side effect.
Recommended form: Zinc picolinate or zinc citrate for superior absorption. Avoid zinc oxide, which absorbs poorly.
Suggested dosage: 15-30 mg daily. Do not exceed 40 mg daily long-term, as excessive zinc can deplete copper.
Timing: Take with food to prevent nausea. If taking iron supplements, separate zinc by at least 2 hours as they compete for absorption.
Supplements that support GLP-1 therapy effectiveness
Beyond filling nutritional gaps, certain supplements can actively enhance the benefits of GLP-1 therapy. These are not replacements for medication. They are complementary additions that support the metabolic, digestive, and body composition changes happening during treatment. SeekPeptides members frequently discuss these combinations in protocol forums, where real-world experiences help refine supplementation strategies.
Protein supplements: protecting lean body mass
This might be the single most important supplement category for GLP-1 users. The STEP 1 trial data revealed that 38% of weight lost on semaglutide came from lean body mass, not fat. That is a staggering amount of muscle loss. And muscle preservation requires adequate protein, which becomes increasingly difficult to achieve through food alone when appetite is suppressed.
The joint advisory from four major medical organizations recommends 1.2-1.6 g/kg/day of protein during active weight reduction with GLP-1 therapy. For a 180-pound person, that translates to roughly 98-131 grams of protein daily. When you are eating 1,200-1,500 calories because your appetite has disappeared, hitting those targets through food alone is nearly impossible without protein supplementation.
Whey protein combined with resistance training has been shown to preserve lean body mass during weight loss more effectively than either intervention alone. For those who cannot tolerate whey, plant-based protein blends combining pea, rice, and hemp proteins provide comparable amino acid profiles.
Recommended form: Whey protein isolate for highest bioavailability and lowest lactose content. Collagen peptides as a secondary protein source for skin, joint, and connective tissue support during weight loss.
Suggested dosage: 25-40 grams per serving, 1-2 servings daily to bridge the protein gap. Aim for 0.4-0.5 g/kg per meal, distributed across 3-4 eating occasions.
Timing: Within 1-2 hours after resistance training for maximal muscle protein synthesis. On rest days, spread throughout the day with meals.
Omega-3 fatty acids: the anti-inflammatory powerhouse
Omega-3 supplementation serves double duty during GLP-1 therapy. First, it provides anti-inflammatory support that can help manage the systemic inflammation associated with obesity and rapid metabolic change. Second, it supports cardiovascular health during a period when metabolic parameters are shifting significantly.
GLP-1 users often reduce their intake of fatty fish, nuts, and seeds, exactly the foods that provide omega-3s naturally. Supplementation ensures that EPA and DHA levels remain adequate for brain function, cardiovascular protection, and inflammation management. The recommended target is at least 1 gram of combined EPA and DHA daily.
Omega-3s also support the absorption of fat-soluble vitamins (A, D, E, K) when taken together, creating a practical synergy with your other supplements.
Recommended form: Triglyceride-form fish oil for superior absorption over ethyl ester forms. Alternatively, algae-based omega-3 for those avoiding fish products.
Suggested dosage: 1,000-2,000 mg of combined EPA and DHA daily. Look for products with at least 500 mg EPA and 250 mg DHA per serving.
Timing: Take with meals containing fat. Pair with your fat-soluble vitamin supplements (D3, K2, E) for optimal absorption of everything.
Probiotics: restoring gut balance
GLP-1 medications fundamentally alter gut motility, and with it, the microbiome. Slowed gastric emptying, changes in transit time, and altered food composition create an environment where beneficial bacterial populations can decline while less desirable strains flourish. This shift manifests as bloating, gas, digestive discomfort, and impaired nutrient absorption.
Probiotic supplementation aims to maintain microbial diversity and support digestive function during therapy. Research on GLP-1 specific probiotics suggests that certain strains, particularly Akkermansia muciniphila and specific Lactobacillus and Bifidobacterium species, may support metabolic health outcomes alongside GLP-1 medications.
The gut health connection extends beyond comfort. A healthy microbiome improves nutrient extraction from the limited food you are consuming, enhances vitamin K2 and certain B vitamin synthesis, and supports immune function. For GLP-1 users eating significantly less, maximizing nutrient extraction from every bite becomes critical.
Recommended form: Multi-strain probiotic containing Lactobacillus acidophilus, Bifidobacterium lactis, and ideally Akkermansia muciniphila. Spore-based probiotics survive stomach acid more effectively, which matters given the altered gastric environment.
Suggested dosage: 10-30 billion CFU daily. Start at the lower end to assess tolerance.
Timing: With meals for best survival through the stomach acid environment.
Fiber supplements: managing digestion and blood sugar
Fiber intake almost always drops during GLP-1 therapy. Fewer calories means less food, and fiber-rich foods like whole grains, vegetables, and legumes are often the first casualties of a suppressed appetite. Yet fiber serves critical functions during weight loss, including blood sugar regulation, cholesterol management, and preventing the constipation that plagues 11-24% of GLP-1 users.
The irony is that reduced fiber intake worsens constipation that the medication already causes. Supplemental fiber, particularly soluble fiber sources, can break this cycle while also supporting healthy eating patterns.
Recommended form: Psyllium husk for bulk-forming fiber. Partially hydrolyzed guar gum (PHGG) for well-tolerated soluble fiber. Inulin for prebiotic effects that feed beneficial gut bacteria.
Suggested dosage: 5-10 grams daily. Start with 2-3 grams and increase gradually over 1-2 weeks to prevent bloating.
Timing: Take with plenty of water, at least 30 minutes before or after other supplements to prevent interference with absorption.
Coenzyme Q10: energy at the cellular level
CoQ10 levels decline in GLP-1 users, and the effect compounds for anyone also taking statins, which deplete CoQ10 through their mechanism of action. Since many people on GLP-1 medications also manage cholesterol with statins, the double depletion can produce significant fatigue and muscle weakness.
CoQ10 is essential for mitochondrial energy production in every cell. When levels drop, the first symptoms are typically fatigue and exercise intolerance, both of which are already common during caloric restriction and GLP-1 therapy.
Recommended form: Ubiquinol (the active, reduced form) rather than ubiquinone, as ubiquinol does not require enzymatic conversion and is more bioavailable.
Suggested dosage: 100-200 mg daily. Higher doses for statin users.
Timing: With a meal containing fat for optimal absorption.
Berberine: the blood sugar synergy
Berberine is a plant compound that has demonstrated insulin-sensitizing effects comparable to metformin in some studies. It improves glucose metabolism by reducing hepatic glucose production and enhancing insulin receptor sensitivity. When combined with GLP-1 therapy, berberine may provide additive benefits for blood sugar control.
However, this combination requires monitoring. Both GLP-1 medications and berberine lower blood sugar, and the combined effect could potentially push levels too low, particularly during fasting or intense exercise. Anyone considering berberine alongside GLP-1 therapy should monitor blood glucose closely and work with a healthcare provider.
Recommended form: Berberine HCl at 98%+ purity. Some newer formulations use dihydroberberine for improved absorption.
Suggested dosage: 500 mg two to three times daily with meals. Start with 500 mg once daily and titrate up.
Timing: Immediately before or with meals for best effect on postprandial blood sugar.
Supplements to avoid or use with caution during GLP-1 therapy
Not every supplement plays nicely with GLP-1 medications. Some create dangerous interactions. Others amplify side effects. A few could undermine the therapeutic benefits entirely. Knowing what to avoid is just as important as knowing what to take, and the consequences of getting this wrong range from uncomfortable to genuinely dangerous.
Garcinia cambogia: liver damage risk
Garcinia cambogia, marketed heavily for weight loss, carries reports of elevated liver failure risk even without other medications. The FDA has flagged it for severe side effects. Combining it with GLP-1 medications, which also undergo hepatic processing, may increase liver strain beyond acceptable levels. There is no legitimate reason to take a marginally effective weight loss supplement alongside one of the most powerful weight loss medications available.
Ephedra and bitter orange: cardiovascular risk
Both ephedra (banned by the FDA) and bitter orange (its legal cousin) carry cardiovascular risks including elevated heart rate, blood pressure spikes, and in extreme cases, heart attacks and strokes. GLP-1 medications can also affect heart rate, and stacking stimulant-based supplements creates unpredictable cardiovascular stress. Avoid completely.
Blood sugar-lowering supplements: hypoglycemia risk
Supplements that independently lower blood sugar, including ginseng, chromium picolinate, alpha-lipoic acid at high doses, and cinnamon extract, can compound the glucose-lowering effects of GLP-1 medications. This does not mean you cannot take them. It means you need to monitor blood glucose more carefully and be aware of hypoglycemia symptoms, particularly shakiness, sweating, confusion, and irritability.
Chromium is particularly noteworthy because it appears in many multivitamins. At typical multivitamin doses (35-120 mcg), the interaction risk is minimal. But standalone chromium supplements at higher doses (200-1,000 mcg) could push blood sugar levels uncomfortably low, especially during higher dose phases of GLP-1 therapy.
Strong laxatives and diuretics
Detox teas, strong herbal laxatives (senna, cascara), and diuretic supplements can cause dehydration and electrolyte imbalances that compound GLP-1 side effects. Since GLP-1 medications already slow digestion and can cause nausea, vomiting, and diarrhea, adding laxatives or diuretics creates a significant dehydration and electrolyte depletion risk.
If constipation is your concern, gentler approaches like magnesium citrate, fiber supplements, and adequate hydration are far safer than stimulant laxatives.
Other GLP-1 agonists or mimetics
Combining multiple GLP-1 acting agents is explicitly not approved by the FDA. This includes taking semaglutide and tirzepatide together, stacking prescription GLP-1 medications with over-the-counter GLP-1 supplements, or adding natural GLP-1 boosting supplements at high doses to prescription therapy. The unpredictable combined effect on blood sugar and GI function creates risks that outweigh any potential benefit.
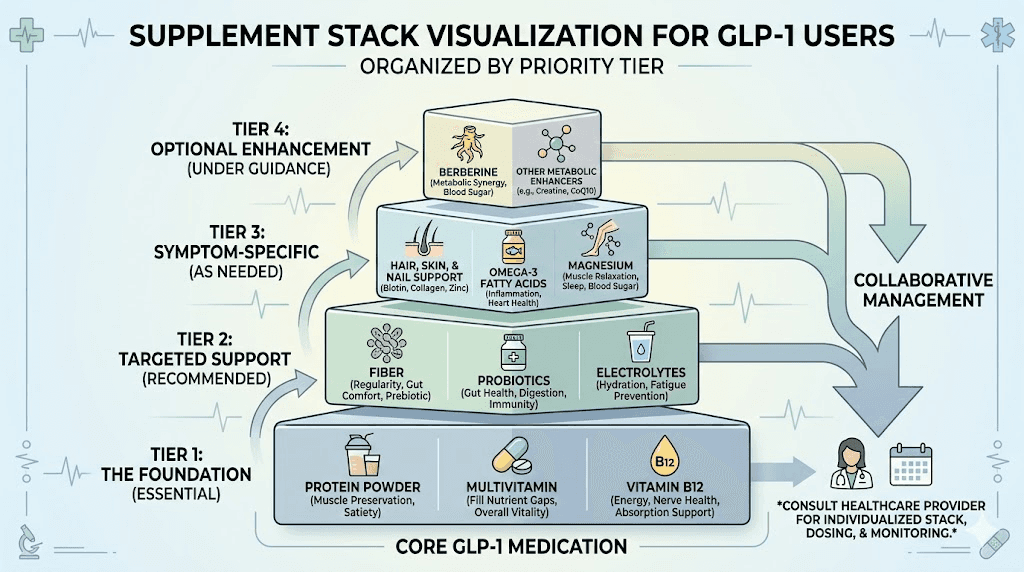
Building your GLP-1 vitamin protocol
Knowing what you need is one thing. Building a practical, sustainable supplementation routine is another. Too many supplements taken haphazardly leads to poor absorption, wasted money, and supplement fatigue that makes you quit entirely. A strategic approach accounts for absorption competition, timing synergies, and the realities of life on GLP-1 therapy. SeekPeptides members use structured protocols that account for these variables, and the results speak for themselves.
The essential tier: what everyone on GLP-1 should take
Regardless of diet quality, blood work, or specific GLP-1 medication, these supplements address the most common and consequential deficiencies. Consider them non-negotiable during therapy.
1. Vitamin D3 + K2 combination
2,000-5,000 IU D3 + 100-200 mcg K2 (MK-7)
Take with largest fat-containing meal
Protects bones, supports calcium routing, maintains immune function
2. B-complex with methylated forms
Includes methylcobalamin, methylfolate, and active B vitamin forms
Take in the morning for energy support
Prevents B12 neuropathy, supports energy metabolism, protects against anemia
3. Magnesium glycinate or citrate
200-400 mg daily
Take in the evening for sleep support (glycinate) or morning for constipation relief (citrate)
Reduces muscle cramps, improves sleep, supports glucose metabolism
4. Calcium citrate
500 mg daily, split into two doses
Take with meals, separate from iron
Prevents bone loss during rapid weight reduction
5. Protein supplement
25-40 grams per serving, 1-2 daily
Within 1-2 hours post-exercise, or with meals on rest days
Preserves lean body mass during weight loss
The supportive tier: based on individual needs
These supplements address specific concerns that not every GLP-1 user will experience. Add them based on symptoms, blood work results, or specific therapy goals.
Omega-3 fatty acids: 1,000-2,000 mg EPA/DHA daily for cardiovascular and anti-inflammatory support. Particularly important for users not eating fatty fish regularly.
Probiotics: 10-30 billion CFU multi-strain formula for digestive symptoms, bloating, and nutrient absorption optimization.
Iron: Only with confirmed deficiency via blood work. 18-65 mg depending on severity. Critical for premenopausal women.
Zinc: 15-30 mg daily for hair loss prevention, immune support, and taste preservation.
CoQ10: 100-200 mg ubiquinol for energy support, especially for statin users dealing with compounded GLP-1 fatigue.
Fiber: 5-10 grams daily for constipation management and blood sugar regulation.
Sample daily supplement schedule
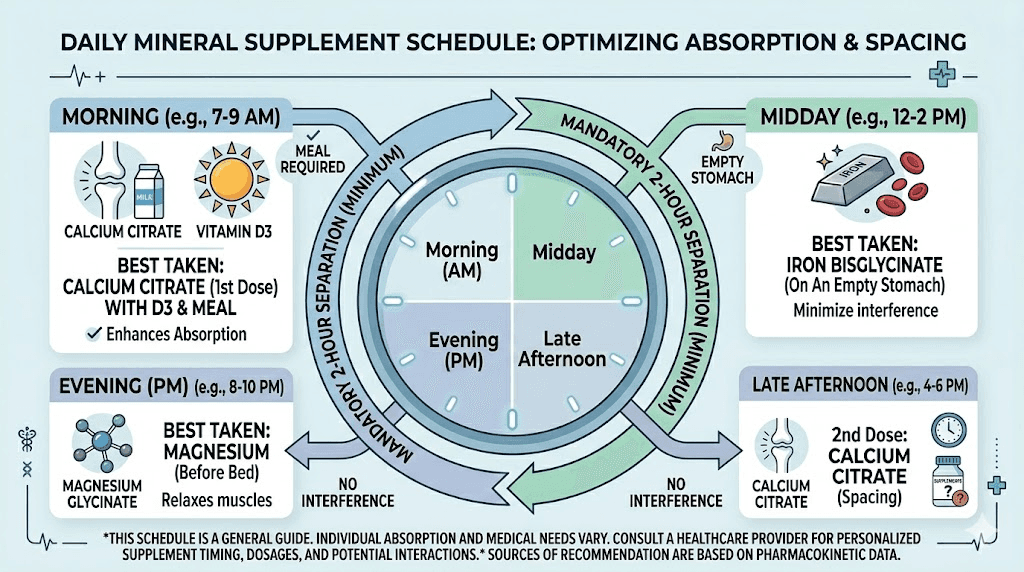
Timing matters. Some supplements compete for absorption when taken together, while others work synergistically. Here is a practical daily schedule that maximizes absorption and minimizes conflicts.
Morning (with breakfast):
B-complex
Iron (if needed, with vitamin C for absorption)
Fiber supplement (30 minutes before meal, with water)
Midday (with lunch):
Calcium citrate (first dose of 250 mg)
Probiotic
Protein shake (if not meeting protein targets through food)
Afternoon/dinner (with largest meal):
Vitamin D3 + K2
Omega-3 fish oil
CoQ10
Calcium citrate (second dose of 250 mg)
Zinc (if taking, with food)
Evening (before bed):
Magnesium glycinate
This schedule separates iron and calcium by several hours, groups fat-soluble supplements with the largest fat-containing meal, and places magnesium at bedtime for its sleep-promoting effects. Adjust based on your meal timing and when you experience the most GI stability.
Blood work: the only way to know what you actually need
Supplement protocols without blood work are educated guesses. Useful guesses, but guesses nonetheless. The only way to know your actual nutrient levels, and whether your supplementation is working, is regular laboratory testing. This is not optional during GLP-1 therapy. It is essential.
Recommended tests before starting GLP-1 therapy
Baseline values give you something to compare against. Get these tests before your first dose, or as early in therapy as possible.
25-hydroxyvitamin D: Target 40-60 ng/mL. Anything below 30 ng/mL requires aggressive supplementation
Vitamin B12 and methylmalonic acid: B12 alone can be misleading. Methylmalonic acid is a more sensitive marker of functional B12 status
Complete blood count (CBC): Establishes baseline red blood cell parameters for monitoring anemia development
Iron panel (ferritin, serum iron, TIBC): Ferritin below 30 ng/mL suggests depleted stores even with normal hemoglobin
Comprehensive metabolic panel: Includes calcium, magnesium (though serum magnesium is imperfect), and kidney function
RBC magnesium: More accurate than serum magnesium. Request specifically
Thyroid panel: TSH, free T3, free T4 for baseline thyroid function
Monitoring schedule during therapy
The first year of GLP-1 therapy carries the highest deficiency risk. Front-load your monitoring during this period.
At 3 months: Repeat vitamin D, B12, CBC, and iron panel. This catches early deficiencies before they become symptomatic.
At 6 months: Full repeat of baseline panel including metabolic panel and RBC magnesium. The six-month mark is when many deficiencies cross from subclinical to clinical.
At 12 months: Comprehensive panel including all baseline tests. Add DXA scan for bone density if weight loss exceeds 14% of starting body weight.
Annually thereafter: Continue monitoring vitamin D, B12, iron, and calcium markers. Adjust supplementation based on results rather than symptoms alone.
Red flags that warrant immediate testing
Do not wait for scheduled blood work if you experience any of these symptoms, which suggest significant nutrient depletion.
Numbness or tingling in hands or feet (B12 deficiency)
Severe muscle cramps or spasms, especially at night (magnesium or calcium)
Unusual fatigue that does not improve with rest (B12, iron, or vitamin D)
Significant hair loss beyond normal shedding (zinc, iron, or biotin deficiency)
Bone pain or stress fractures (vitamin D and calcium)
Heart palpitations or irregular heartbeat (magnesium or potassium)
Confusion or memory problems (B1, B12)
Special considerations by GLP-1 medication type
While all GLP-1 receptor agonists share core mechanisms, different medications create different nutritional profiles. Understanding these nuances helps you fine-tune your supplementation strategy based on which specific medication you are using.
Semaglutide (Ozempic, Wegovy, compounded)
Semaglutide produces nausea in approximately 44% of users, the highest rate among common GLP-1 medications. This means more frequent vomiting episodes and greater nutrient loss through the GI tract during dose titration. The first 4-8 weeks are the most critical period for supplementation adherence.
Semaglutide users should pay particular attention to B12 status, since studies specifically examining semaglutide have shown impaired B12 absorption. Compounded semaglutide with B12 addresses this directly by delivering B12 via injection rather than relying on oral absorption.
Semaglutide-glycine compounds have also gained popularity. Glycine supports collagen synthesis and may help with the skin laxity that accompanies rapid weight loss. For users dealing with both fatigue and skin changes, this combination addresses two concerns simultaneously.
Tirzepatide (Mounjaro, Zepbound, compounded)
Tirzepatide acts on both GIP and GLP-1 receptors, creating a dual mechanism that produces greater weight loss but also a distinct side effect profile. While nausea rates are lower than semaglutide (28% vs 44%), the dual receptor activation may create unique nutritional considerations that single-receptor agonists do not.
Tirzepatide-glycine-B12 compounds represent the most comprehensive approach to addressing nutritional support alongside therapy. The glycine provides amino acid support, B12 prevents deficiency, and the base medication handles weight management.
Tirzepatide with niacinamide is another combination that has gained attention. Niacinamide (vitamin B3) supports cellular energy production and skin health, addressing two common concerns during aggressive weight loss. For users already experiencing fatigue on tirzepatide, the added B3 may provide noticeable energy benefits.
Supplement strategies specific to tirzepatide should account for its longer half-life and different dosing schedule. Since tirzepatide is administered weekly, the pharmacokinetic profile creates different windows of GI sensitivity compared to semaglutide.
Retatrutide: the triple agonist
Retatrutide activates GLP-1, GIP, and glucagon receptors. This triple mechanism produces the most dramatic weight loss seen in clinical trials, with some participants losing up to 24% of body weight. That level of weight loss amplifies every nutritional concern discussed in this guide.
Triple agonist therapy means more aggressive appetite suppression, potentially lower caloric intake, and greater lean mass loss risk. Users on retatrutide protocols should be particularly vigilant about protein intake (targeting the upper range of 1.6 g/kg/day), vitamin D supplementation, and bone health monitoring.
Since retatrutide is still in clinical development, long-term nutritional data is limited compared to semaglutide and tirzepatide. This makes proactive supplementation and regular blood work even more important for early adopters.
Diet strategies to maximize nutrient intake on GLP-1
Supplements fill gaps, but food remains the foundation. When you are only eating 1,200-1,600 calories daily, every bite needs to earn its place. Nutrient density becomes the single most important dietary principle during GLP-1 therapy. Here is how to make limited calories work harder for your nutritional needs.
Prioritize protein at every eating occasion
Protein should be the first thing on your plate. Always. The 1.2-1.6 g/kg/day target means protein needs to account for 16-24% of total energy intake. Eggs, Greek yogurt, lean poultry, fish, and legumes deliver the most protein per calorie. Building meals around protein ensures you hit targets even when total food volume is low.
The timing of protein matters too. Distributing intake across 3-4 meals rather than concentrating it in one large meal maximizes muscle protein synthesis. Research shows that 0.4-0.5 g/kg per meal triggers the optimal anabolic response. Below this threshold per meal, muscle preservation suffers even if daily totals look adequate.
Eat the rainbow (for real this time)
Colorful fruits and vegetables provide the broadest micronutrient spectrum per calorie. Dark leafy greens deliver calcium, magnesium, iron, and folate. Orange vegetables provide vitamin A. Berries offer vitamin C and antioxidants. When calories are limited, variety matters more than volume.
A practical approach: aim for at least three different colors at each meal. This simple rule naturally increases the diversity of vitamins and minerals you consume without requiring complicated tracking.
Do not fear healthy fats
Fat-soluble vitamins (A, D, E, K) require dietary fat for absorption. Cutting fat too aggressively, which some GLP-1 users do to reduce nausea, actually impairs the absorption of critical supplements. Include small amounts of avocado, olive oil, nuts, or fatty fish at meals where you take fat-soluble supplements.
The right diet plan during GLP-1 therapy balances protein priorities with enough healthy fat to support supplement absorption and enough fiber to maintain digestive health. It is a narrow window, but it is achievable with planning.
Hydration: the forgotten nutrient
Dehydration is rampant among GLP-1 users. Reduced food intake means less water from food (which normally contributes 20% of daily fluid intake). GI side effects like vomiting and diarrhea increase fluid losses. And many users simply forget to drink because their overall consumption awareness has shifted.
Aim for at least 64 ounces of water daily, with an additional 8-16 ounces for every episode of GI side effects. Electrolyte supplementation (sodium, potassium, magnesium) may be necessary during periods of frequent vomiting or diarrhea.
The multivitamin question: are they enough?
Most GLP-1 users default to a daily multivitamin and call it a day. While better than nothing, standard multivitamins were designed for people eating 1,800-2,500 calories daily. They contain large amounts of nutrients easily obtained from food (like niacin and riboflavin) and inadequate amounts of the nutrients GLP-1 patients actually need most (like vitamin D, B12, magnesium, and calcium).
Where standard multivitamins fall short
A typical multivitamin contains 400-800 IU of vitamin D. GLP-1 users often need 2,000-5,000 IU. It contains 100-250 mg of calcium. GLP-1 users need 500 mg from supplements. It contains 25-50 mg of magnesium. GLP-1 users need 200-400 mg. And most multivitamins contain zero protein, zero omega-3s, and zero probiotics, three of the most critical supplements during therapy.
Think of a standard multivitamin as a foundation, not a solution. It covers trace nutrients (chromium, selenium, manganese, copper) at adequate levels, but the heavy-hitter nutrients need standalone supplements at therapeutic doses.
GLP-1 specific supplement packs
Companies like Nature Made have released GLP-1 companion supplement packs specifically formulated for users of these medications. These packs typically contain higher-dose vitamin D, B12, calcium with K2, and sometimes protein and fiber. They represent a step up from standard multivitamins, though they may still require additional standalone supplements depending on individual needs.
The advantage of these packs is convenience. The disadvantage is that one-size-fits-all formulations cannot account for individual deficiency patterns, which vary significantly based on baseline nutritional status, specific medication, dose, and diet quality.
Exercise and nutrient demands on GLP-1
Exercise is not optional during GLP-1 therapy. The joint advisory recommends minimum three times weekly strength training plus 150 minutes weekly of moderate aerobic activity. One trial demonstrated that GLP-1 therapy plus exercise preserved bone mineral density while GLP-1 therapy alone decreased it. That finding alone should make exercise non-negotiable.
But exercise increases nutrient demands. Active individuals need more protein, more magnesium, more B vitamins, and more electrolytes than sedentary people. If you are both exercising intensely and eating significantly less, the gap between nutrient needs and nutrient intake widens further.
Pre-workout nutrition on GLP-1
Training fasted on GLP-1 medications is risky. Hypoglycemia risk is real, and training without fuel when you have already been eating less all day is a recipe for poor performance and excessive muscle breakdown. A small protein-rich snack 60-90 minutes before training provides amino acids for muscle preservation and glucose for brain function.
Post-workout recovery
The post-workout window matters more for GLP-1 users than the general population. When overall protein intake is already borderline, the 1-2 hour window after resistance training represents the most efficient time for muscle protein synthesis. A protein shake with 25-40 grams of whey or plant protein, combined with easily digestible carbohydrates, supports recovery without overwhelming a sensitive stomach.
Electrolyte replacement after sweating is also critical. Sodium, potassium, and magnesium losses through sweat compound the depletion from reduced food intake. A quality electrolyte supplement without excess sugar helps maintain balance.
Long-term vitamin strategy: beyond the first year
GLP-1 therapy is increasingly a long-term proposition. Data shows that up to two-thirds of lost weight is regained within one year of discontinuation, which pushes many users toward extended or indefinite therapy. This means supplementation is not a temporary measure. It is a long-term commitment that needs to evolve as your body composition changes, your caloric intake stabilizes, and your metabolic parameters shift.
Adjusting as weight stabilizes
During active weight loss, nutrient demands peak. Once weight stabilizes, usually 12-18 months into therapy, some supplement doses can be reduced based on blood work. Vitamin D requirements may decrease as fat stores stop releasing and redistributing the vitamin. Protein supplementation may decrease as caloric intake stabilizes at maintenance levels.
However, certain supplements will likely remain necessary for the duration of therapy. B12 supplementation should continue as long as you are on a GLP-1 medication that impairs absorption. Magnesium and calcium supplementation should continue as long as caloric intake remains below levels that support adequate mineral intake from food alone.
Transitioning off GLP-1 therapy
If you discontinue GLP-1 therapy, appetite returns, caloric intake increases, and food-based nutrient intake typically rises. This is the time to reassess your supplement protocol. Blood work at 3 and 6 months post-discontinuation helps determine which supplements are still needed and which can be tapered.
Do not stop all supplements abruptly when stopping medication. Some deficiencies, particularly vitamin D and B12, take months to correct and can persist well beyond therapy discontinuation.
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, detailed supplementation protocols, and a community of thousands who have navigated these exact nutritional challenges.
Frequently asked questions
What is the most important vitamin to take on GLP-1 medications?
Vitamin D is the most commonly deficient nutrient in GLP-1 users, with 13.6% developing clinical deficiency within 12 months. A D3 + K2 combination at 2,000-5,000 IU daily addresses the most prevalent and consequential deficiency. However, B12 is arguably the most dangerous deficiency to miss, since neurological damage can be irreversible. Both should be considered essential. Use our peptide calculator to help track your dosing and supplementation alongside medication dosing.
Can I just take a multivitamin instead of individual supplements?
A multivitamin is a good starting point but insufficient alone. Standard multivitamins contain inadequate amounts of vitamin D (400-800 IU vs the 2,000-5,000 IU most GLP-1 users need), calcium (100-250 mg vs 500 mg needed from supplements), and magnesium (25-50 mg vs 200-400 mg needed). Use a multivitamin as a base and add standalone D3+K2, magnesium, calcium citrate, and B12 at therapeutic doses. GLP-1 specific supplement packs are a better option than standard multivitamins.
How soon should I start taking vitamins after starting GLP-1 therapy?
Immediately. Do not wait for symptoms or deficiency to appear on blood work. The joint advisory from four major medical organizations recommends proactive supplementation from the start of therapy. Deficiencies begin developing as soon as caloric intake drops, which happens within the first week for most users. Starting supplements on the same day you begin GLP-1 therapy prevents deficiencies rather than trying to correct them after the fact.
Does vitamin B12 in compounded semaglutide or tirzepatide actually help?
Yes. Injectable B12 bypasses the impaired oral absorption pathway that GLP-1 medications create. Compounded formulations with B12 deliver the vitamin directly into tissue, where it is absorbed without relying on intrinsic factor or normal gastric function. This is actually more reliable than oral B12 supplements for GLP-1 users with compromised digestive absorption.
Can berberine be taken safely with GLP-1 medications?
Yes, with monitoring. Berberine alongside semaglutide can provide additive blood sugar-lowering effects, which is beneficial for metabolic health but requires glucose monitoring to prevent hypoglycemia. Start with 500 mg once daily and increase gradually while checking blood sugar levels, particularly before meals and after exercise.
Should I take supplements on an empty stomach or with food?
It depends on the supplement. Fat-soluble vitamins (D3, K2, E, A, omega-3s, CoQ10) should always be taken with a meal containing fat. B vitamins can be taken with or without food, though food reduces nausea. Iron absorbs best on an empty stomach but can be taken with food if stomach upset occurs. Calcium citrate absorbs well with or without food. Magnesium is typically best at bedtime. See the detailed timing schedule in the protocol section above.
How long does it take to correct a vitamin deficiency on GLP-1?
It varies by nutrient. B12 deficiency can take 3-6 months to correct with consistent supplementation, and neurological symptoms may take longer to resolve. Vitamin D levels typically respond within 8-12 weeks at therapeutic doses. Iron deficiency anemia usually improves within 2-3 months with proper supplementation, though ferritin stores can take 6+ months to fully replete. Magnesium tissue levels can normalize within 4-6 weeks with consistent supplementation.
Will supplements interfere with my GLP-1 medication effectiveness?
The vitamins and minerals discussed in this guide do not interfere with GLP-1 receptor agonist effectiveness. However, fiber supplements should be taken 30+ minutes before or after other oral medications or supplements, as fiber can reduce absorption. Avoid taking supplements at the exact time of GLP-1 injection, not because of interaction, but because injection-site nausea combined with a stomach full of pills can increase discomfort.
External resources
American College of Lifestyle Medicine Joint Advisory on Nutritional Priorities During GLP-1 Therapy
Nutritional Deficiencies and Muscle Loss in GLP-1 Users: Retrospective Observational Study
Frontiers in Nutrition: Investigating Nutrient Intake During GLP-1 Receptor Agonist Use
In case I do not see you, good afternoon, good evening, and good night. May your nutrient levels stay optimal, your energy stay consistent, and your GLP-1 journey stay well-supported.