Feb 20, 2026

You are wasting peptide. Every week, someone draws the wrong amount from a compounded tirzepatide vial, injects too much or too little, and wonders why their body reacts with nausea that knocks them out for three days. Or worse, they feel nothing at all. The starting dose is supposed to be simple. It is 2.5 mg once per week. But "simple" falls apart the moment you hold a vial labeled 10mg/mL in one hand and an insulin syringe in the other, staring at tiny hash marks, doing math you are not confident about.
That gap between knowing the dose and actually measuring it correctly is where most mistakes happen.
Compounded tirzepatide does not come in a pre-filled pen like Mounjaro or Zepbound. There is no dial to click to 2.5 mg. Instead, you get a vial with a concentration printed on the label, and you have to calculate how many units to draw on a syringe. Get it right and the starting phase is smooth, manageable, even unremarkable. Get it wrong and you either underdose (wasting weeks with no appetite suppression) or overdose (spending days on the couch with GI distress that makes you want to quit entirely). This guide walks through every calculation, every concentration, every scenario you will encounter during those critical first weeks on compounded tirzepatide. Whether you are brand new to tirzepatide dosing or switching from a brand-name version, the math and the strategy matter more than most people realize.
What the standard compounded tirzepatide starting dose is
The standard starting dose for compounded tirzepatide is 2.5 mg injected subcutaneously once per week. This is not a guess, not a suggestion, and not a range. It is the same introductory dose used in every major clinical trial, including SURMOUNT-1, which enrolled over 2,500 participants and ran for 72 weeks. The FDA approved this exact starting dose for both Mounjaro (for type 2 diabetes) and Zepbound (for weight management). Compounded versions use the same active molecule, so the starting protocol follows the same logic.
Why 2.5 mg specifically? Because tirzepatide is a dual-action peptide. It activates both GLP-1 and GIP receptors simultaneously, which makes it significantly more potent than single-receptor medications like semaglutide. That dual mechanism means the body needs time to adjust. Starting higher, even at 5 mg, dramatically increases the risk of nausea, vomiting, and diarrhea. The SURMOUNT-1 trial data showed that participants who followed the gradual titration schedule starting at 2.5 mg had significantly better tolerability than those protocols that skipped the introductory phase.
You stay at 2.5 mg for a minimum of four weeks. Not three. Not "until you feel ready." Four full weeks. This allows your GI tract to adapt to the slowed gastric emptying that tirzepatide causes. It lets your body adjust to the new hormonal signaling. And it gives you a baseline to assess tolerability before increasing.
Some providers start patients even lower, at 1.0 to 1.5 mg, particularly if the patient has a history of GI sensitivity or is concerned about side effects. We will cover that microdosing approach in detail later. But the standard, evidence-backed starting point is 2.5 mg weekly.
One critical detail that trips people up: 2.5 mg is not the therapeutic dose. It is the acclimation dose. You should not expect significant weight loss at 2.5 mg. In the SURMOUNT-1 trial, the real results, 16% to 22.5% total body weight reduction, came at the 5 mg, 10 mg, and 15 mg maintenance doses over 72 weeks. The starting dose exists purely to get your body ready for those higher, effective doses without making you miserable in the process.
If you are using a compounded tirzepatide dosage calculator, always verify that your calculated volume matches the 2.5 mg target. Double-check the concentration on your vial label against the calculator input. A mismatch between your vial concentration and the calculator setting is the single most common source of dosing errors.
How compounded tirzepatide differs from brand-name versions
The active ingredient is identical. Compounded tirzepatide contains the same 39-amino-acid peptide sequence as Mounjaro and Zepbound. It activates the same receptors, produces the same physiological effects, and follows the same dose-response curve. The differences are in packaging, delivery format, and regulatory status.
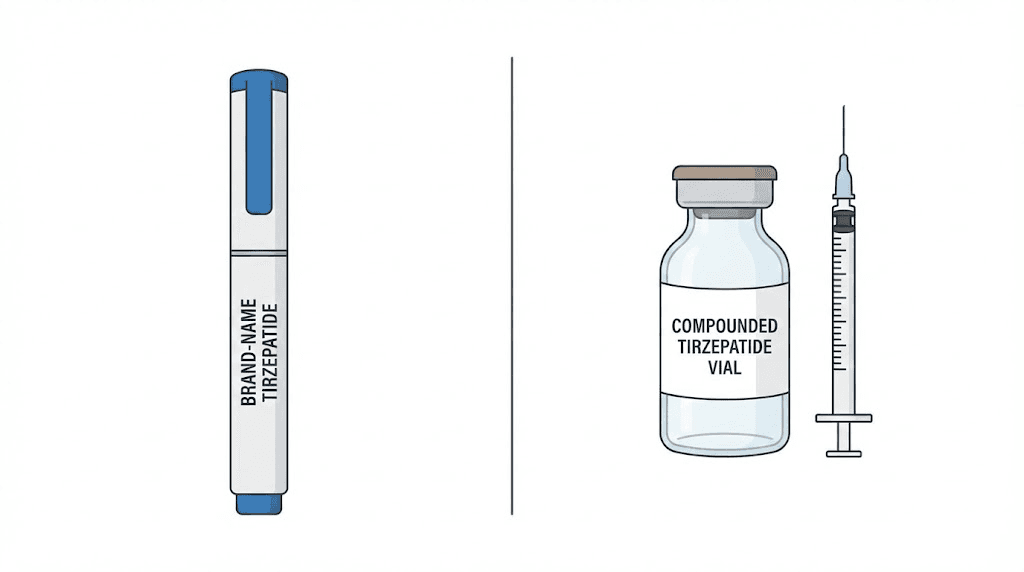
Brand-name tirzepatide comes in pre-filled, single-dose autoinjector pens. Each pen contains one exact dose. You click a button, the pen injects a precisely measured amount, and you throw it away. No math. No syringes. No concentration calculations. The pens come in fixed doses: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg.
Compounded tirzepatide is different. It typically arrives as a multi-dose vial containing a liquid solution at a specific concentration. Common concentrations include 5 mg/mL, 10 mg/mL, 20 mg/mL, and 30 mg/mL. You draw your dose from the vial using an insulin syringe, which means you need to calculate the correct volume based on the concentration. This is where the dosage chart in units becomes essential. The same 2.5 mg dose requires vastly different syringe volumes depending on which concentration you have.
There are practical implications to this difference.
First, accuracy becomes your responsibility. With a pre-filled pen, the manufacturer guarantees dose precision. With a compounded vial, precision depends on your ability to read the syringe correctly and draw the right amount. Using a tirzepatide dose chart specific to your concentration eliminates most of the guesswork, but you still need to execute the draw carefully.
Second, compounded tirzepatide is not FDA-approved. The compounding pharmacies that produce it are regulated by state boards of pharmacy and, in some cases, by the FDA under Section 503B. But the specific compounded product has not gone through the full clinical trial and approval process that Mounjaro and Zepbound completed. This does not mean the peptide itself is different. It means the manufacturing process has not been independently validated to the same extent. For a comprehensive overview of what this means in practice, the compound dosage chart guide covers the practical details.
Third, concentrations vary between pharmacies. One pharmacy might send you a 10 mg/mL vial. Another might compound at 20 mg/mL. This means a dosing chart from one provider may not apply to your specific vial. Always check your label. The dosing chart in units resource on SeekPeptides covers multiple concentrations so you can find the right reference regardless of what your pharmacy provides.
Some compounded versions also include additional ingredients like B12, glycine, or niacinamide. These additions can affect reconstitution, storage, and sometimes tolerability. If your vial contains tirzepatide with B12 or tirzepatide with glycine, the dosing math for tirzepatide itself remains the same. The additions do not change how many milligrams of tirzepatide are in each milliliter.
Converting your starting dose to syringe units
Here is the formula. Memorize it or write it down, because you will use it every week.
(Desired dose in mg / Concentration in mg per mL) x 100 = Syringe units
That is it. One formula covers every concentration and every dose you will ever need.
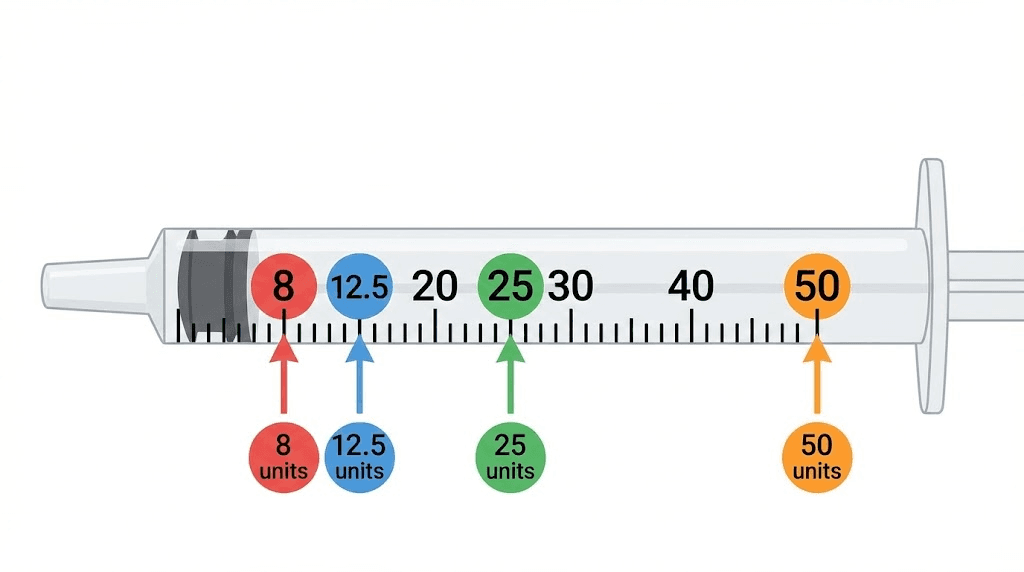
Let us break it down with the starting dose. You want 2.5 mg. Your vial says 10 mg/mL. So: (2.5 / 10) x 100 = 25 units. You draw to the 25-unit line on your insulin syringe. Done.
The "x 100" part exists because insulin syringes are calibrated in units, not milliliters. A standard U-100 insulin syringe holds 1 mL total, divided into 100 units. So when you calculate that you need 0.25 mL of solution, multiplying by 100 converts that to 25 units on the syringe. If you are unfamiliar with insulin syringe markings, the tirzepatide dosage in units guide includes visual references that make the markings easier to interpret.
A few critical details about syringe selection. Most people use a 1 mL (100-unit) insulin syringe with a 29 or 30 gauge needle. For the starting dose at most concentrations, this syringe works perfectly. The exception is the 5 mg/mL concentration, where 2.5 mg requires 50 units (0.50 mL), which fills half the syringe. That is manageable but leaves less room for error if you accidentally pull past the line.
For concentrations of 20 mg/mL and above, the volumes get very small. A 2.5 mg dose from a 20 mg/mL vial is only 12.5 units. On a 100-unit syringe, the markings at that range can be difficult to read precisely. Some people switch to a 0.3 mL (30-unit) insulin syringe for these small volumes. The markings are larger and easier to read, which improves accuracy. The dosage chart in mL can help you visualize these volumes across different syringe sizes.
Common conversion mistakes to watch for: confusing mg with mL, using the wrong concentration in the formula, and misreading syringe markings. If your calculated number does not seem right, recalculate. Always. A misplaced decimal turns a 2.5 mg dose into a 25 mg dose, which is a medical emergency waiting to happen.
Starting dose calculations by concentration
Every compounding pharmacy uses different concentrations. Your vial might be 5 mg/mL, 10 mg/mL, 20 mg/mL, or 30 mg/mL. The starting dose is always 2.5 mg, but the number of units you draw changes dramatically based on what concentration you have. Below is a breakdown for each common concentration, along with the exact math so you can verify every number yourself.
Starting dose at 5 mg/mL
Formula: (2.5 / 5) x 100 = 50 units
At 5 mg/mL, you draw 50 units on your insulin syringe. This is 0.50 mL of liquid, which is exactly half of a standard 1 mL insulin syringe. The advantage of this concentration is precision. The 50-unit mark is clearly visible and easy to hit accurately. The disadvantage is volume. As you titrate up to higher doses, the injection volumes become large. At 5 mg, you would need 100 units (a full syringe). At 7.5 mg, you would need 150 units, which exceeds a single syringe and requires splitting the injection across two sites. For a full breakdown, see the injection dosage chart.
Starting dose at 10 mg/mL
Formula: (2.5 / 10) x 100 = 25 units
This is the most commonly prescribed concentration for compounded tirzepatide. At 25 units for the starting dose, the volume is small enough for comfort but large enough for accuracy. Most tirzepatide dosing guides reference this concentration as the default. You can comfortably titrate all the way to 10 mg (100 units) on a single syringe. Going to 15 mg would require 150 units, which again means two injections. The 10 mg dosage chart covers every dose level at this concentration.
Starting dose at 20 mg/mL
Formula: (2.5 / 20) x 100 = 12.5 units
Here is where precision becomes tricky. The 12.5 unit mark falls between two lines on most 100-unit insulin syringes, where each small line represents 2 units. You need to draw to halfway between the 12 and 14 unit marks. This is doable, but it requires a steady hand and good eyesight. Some people find it easier to use a 30-unit or 50-unit syringe where the markings are more spread out. The benefit of 20 mg/mL is that higher doses remain manageable. Even 15 mg is only 75 units, well within a single syringe. Check the 20 mg/mL dosing chart for a complete reference at this concentration.
Starting dose at 30 mg/mL
Formula: (2.5 / 30) x 100 = 8.3 units
This is the most concentrated option and the hardest to measure accurately at the starting dose. Drawing 8.3 units on a standard insulin syringe is extremely precise work. You are aiming for a point roughly one-third of the way between the 8 and 10 unit marks. At this level of precision, even a tiny error in reading the syringe can mean a 10% to 15% dose variation. A 30-unit syringe is strongly recommended for this concentration. The upside is that the maximum dose of 15 mg requires only 50 units, making high-dose injections very compact and comfortable. The 30 mg dosage chart provides exact measurements for every dose tier.
Quick reference table for 2.5 mg starting dose
Concentration | Units to draw | Volume in mL | Syringe recommendation |
|---|---|---|---|
5 mg/mL | 50 units | 0.50 mL | 100-unit (1 mL) syringe |
10 mg/mL | 25 units | 0.25 mL | 100-unit (1 mL) syringe |
20 mg/mL | 12.5 units | 0.125 mL | 30-unit or 50-unit syringe |
30 mg/mL | 8.3 units | 0.083 mL | 30-unit syringe |
If your concentration is not listed here, use the formula. It works for any concentration. And if you want to double-check your math, the peptide calculator on SeekPeptides lets you plug in your exact vial concentration and desired dose to get the precise syringe volume.
The microdosing approach to starting tirzepatide
Not everyone starts at 2.5 mg. Some people start lower.
Microdosing tirzepatide typically means beginning at 1.0 to 1.5 mg per week, sometimes even lower at 0.5 mg. The idea is straightforward: introduce the peptide even more gradually than the standard protocol to minimize side effects and allow the body to adapt at its own pace. This approach has gained significant attention in the weight management community, though it is important to understand that no clinical trials have studied tirzepatide at doses below 2.5 mg. All efficacy and safety data come from the 2.5 mg starting dose and above.
Why would someone choose to microdose? Several reasons. People with a history of severe GI sensitivity often struggle even at 2.5 mg. Individuals who have previously tried semaglutide and experienced significant nausea may want an even gentler introduction to tirzepatide. Smaller individuals, particularly those under 130 pounds, sometimes find that 2.5 mg produces disproportionately strong effects relative to their body weight. And some people simply prefer a cautious approach to any new medication.
The tirzepatide microdose chart provides detailed breakdowns for sub-2.5 mg dosing at various concentrations. Here is what common microdoses look like in practice:
Microdose | Units at 10 mg/mL | Units at 20 mg/mL |
|---|---|---|
0.5 mg | 5 units | 2.5 units |
1.0 mg | 10 units | 5 units |
1.5 mg | 15 units | 7.5 units |
2.0 mg | 20 units | 10 units |
Notice the challenge with higher concentrations at microdoses. Drawing 2.5 units from a 20 mg/mL vial is nearly impossible to do accurately with a standard insulin syringe. If you plan to microdose, a 10 mg/mL concentration is strongly recommended because the volumes are large enough to measure reliably.
A typical microdosing schedule might look like this: 1.0 mg weekly for two weeks, then 1.5 mg for two weeks, then 2.0 mg for two weeks, then the standard 2.5 mg for four weeks before considering an increase to 5 mg. This stretches the acclimation period from four weeks to ten weeks, which is a significant time investment. But for people who are highly sensitive to GI side effects, those extra weeks can mean the difference between completing a full course of treatment and abandoning it after two miserable injections.
The tradeoff is clear. Microdosing reduces side effects but delays the onset of meaningful weight loss. At doses below 2.5 mg, appetite suppression is minimal for most people. The real metabolic benefits, the glucose regulation, the significant appetite reduction, the measurable weight loss, typically begin at the 5 mg dose and become pronounced at 10 mg and above. Microdosing is a comfort strategy, not an efficacy strategy. For more detail on the microdosing approach and weekly progression, the full chart covers every step.
What to expect during your first four weeks
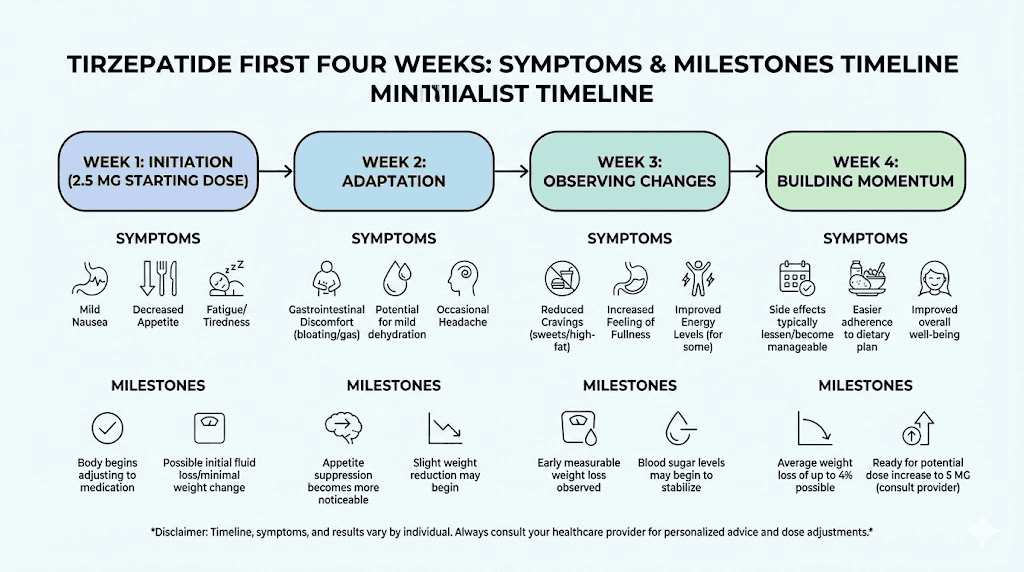
The first four weeks on 2.5 mg are an adjustment period. Your body is encountering a new signaling molecule that affects digestion, appetite, blood sugar, and gastric motility all at once. Knowing what to expect week by week prevents unnecessary anxiety and helps you distinguish normal adaptation from genuine problems.
Week one
Most people feel something within 24 to 48 hours of their first injection. The most common early sensation is mild nausea, reported by 13% to 24% of patients in clinical trials depending on the dose. At the 2.5 mg starting dose, nausea rates are on the lower end of that range. It typically feels like the queasiness you get from eating slightly too much, not severe vomiting. Some people notice a subtle decrease in appetite, almost like they simply forget to feel hungry for a few hours. Others feel nothing at all during the first week. Both responses are normal.
You might also experience mild bloating or a feeling of fullness after small meals. This is the slowed gastric emptying taking effect. Your stomach is processing food more slowly than usual, which is part of how tirzepatide reduces overall food intake. If you want to understand more about how fast tirzepatide works and what timeline is realistic, the complete breakdown covers onset expectations in detail.
Week two
Side effects that appeared in week one typically peak during days 8 through 14. If you are going to experience nausea, constipation, or diarrhea, this is usually when it is most noticeable. The good news: these symptoms are transient for the vast majority of people. Studies show that GI side effects at the starting dose resolve within one to two weeks for most participants.
Appetite suppression may become more consistent during week two. You might find that you eat smaller portions naturally, without conscious effort. Some people report changes in food preferences, particularly reduced cravings for high-calorie, high-sugar foods. This is not universal, but it is common enough to mention. If you are curious about how long it takes for tirzepatide to suppress appetite, the timeline varies but many people notice meaningful changes by the end of week two.
Week three
By week three, your body has typically adapted to the 2.5 mg dose. Nausea, if it occurred, has usually faded. Appetite suppression is more noticeable and consistent. Some people report losing 2 to 4 pounds during the first three weeks, mostly from reduced food intake rather than direct metabolic effects. Others see no scale change yet, which is also completely normal at this introductory dose.
This is the week where patience matters most. The temptation to increase the dose early is strong, especially if side effects have resolved and you feel "ready for more." Resist that temptation. The four-week minimum at each dose level is not about side effects. It is about allowing your receptor systems to fully adapt so that the next dose increase is tolerable. Rushing titration is one of the most common mistakes beginners make with peptide protocols.
Week four
Assessment week. By the end of week four, you should have a clear picture of how your body handles tirzepatide. Questions to ask yourself: Did I experience significant side effects? Have they resolved? Is appetite suppression noticeable? Am I tolerating the injections well? Are there any unusual symptoms that concern me?
If the answer to these questions is positive, meaning side effects were manageable and you tolerated the dose well, you are ready to increase to 5 mg. If you experienced persistent nausea, severe GI distress, or other concerning symptoms throughout the full four weeks, it may be worth staying at 2.5 mg for an additional two to four weeks before increasing. Some people also choose to step up to an intermediate dose like 3.5 mg or 4 mg rather than jumping directly to 5 mg. Your provider can help determine the best approach based on your individual response.
Weight loss during the first four weeks is typically modest. Clinical trial data shows an average of 2 to 5 pounds lost during the 2.5 mg phase. The significant weight loss begins at the 5 mg dose and accelerates at 10 mg and 15 mg. For context, participants in SURMOUNT-1 achieved average weight reductions of 16% at 5 mg, 21.4% at 10 mg, and 22.5% at 15 mg over 72 weeks. Those numbers come from the higher maintenance doses, not the starting dose. To see the full progression, the tirzepatide before and after resource documents real timelines.
Managing starting dose side effects
Side effects at 2.5 mg are generally mild. But "mild" does not mean nonexistent, and being prepared makes a significant difference in how comfortably you get through the first month.
Nausea management
Nausea is the most commonly reported side effect, affecting roughly 13% to 20% of people at the starting dose. It typically begins 24 to 48 hours after injection and lasts one to three days. For most people, it feels like low-grade queasiness rather than active vomiting.
Practical strategies that work: eat smaller meals throughout the day instead of two or three large ones. Avoid greasy, spicy, or heavily seasoned foods during the first week after each injection. Stay upright for at least 30 minutes after eating. Ginger tea or ginger chews can help settle the stomach. Some people find that injecting in the evening rather than the morning allows them to sleep through the worst of the nausea. The foods to avoid on tirzepatide guide lists specific trigger foods that commonly worsen nausea.
If nausea is severe or persists beyond four or five days after each injection, contact your provider. Persistent severe nausea at the starting dose may indicate that you need a slower titration approach, possibly starting with a microdose protocol.
Constipation and digestive changes
Slowed gastric emptying means food moves through your system more slowly. For some people, this translates to constipation. Staying hydrated is the single most effective countermeasure. Aim for at least 64 ounces of water daily, more if you are active. Fiber-rich foods help, but introduce them gradually. A sudden increase in fiber on top of slowed digestion can make bloating worse. If constipation becomes an ongoing issue, the tirzepatide constipation treatment guide covers both dietary and supplemental approaches.
Fatigue and energy changes
Some people report feeling tired during the first week or two. This makes sense. Your body is adjusting to reduced caloric intake, altered blood sugar patterns, and a new hormonal signal. The fatigue is usually temporary and resolves as your system adapts. If you want to understand the full picture of whether tirzepatide makes you tired, the relationship between reduced calories and energy output plays a major role. Some people actually report increased energy once they adapt, as documented in the tirzepatide and energy resource. The broader topic of GLP-1 fatigue applies here as well, since tirzepatide activates the GLP-1 receptor pathway.
Headaches
Headaches during the first week are often related to dehydration or reduced food intake rather than a direct effect of tirzepatide. When you eat less, you also tend to drink less, and your electrolyte balance shifts. Make a conscious effort to stay hydrated and maintain electrolyte intake, particularly sodium, potassium, and magnesium. If headaches persist, the tirzepatide headaches guide covers both prevention and management strategies.
Muscle and body aches
A small percentage of people report muscle pain or general body aches, particularly during the first two weeks. This is less common than nausea or digestive changes, but it does happen. Tirzepatide muscle pain and body aches are discussed in detail in their respective guides. Gentle movement, adequate protein intake, and proper hydration tend to help. If aches are severe or accompanied by dark urine, seek medical attention immediately as this could indicate a more serious reaction.
Injection site reactions
Mild redness, swelling, or itching at the injection site is common and usually resolves within a few hours. Rotating injection sites between the abdomen, thigh, and upper arm reduces the likelihood of persistent irritation. For proper technique, the stomach injection guide and the broader GLP-1 injection site guide cover best practices in detail.
Sleep disruption
Some users report difficulty sleeping during the first one to two weeks, particularly if they inject in the evening. Tirzepatide insomnia is not one of the most common side effects, but it affects a meaningful subset of users. If you notice sleep disruption, try switching your injection day or time. Many people find that injecting in the morning on a day when they can rest if needed (like a Friday or Saturday) is optimal.
When and how to increase from the starting dose
After four weeks at 2.5 mg, the standard next step is 5 mg weekly. This is not optional or aggressive. The clinical trials uniformly describe 2.5 mg as the introductory dose, with 5 mg as the first therapeutic dose. The real treatment begins at 5 mg.
The decision to increase should be based on tolerability, not impatience. If you tolerated 2.5 mg well, meaning side effects were absent or manageable and resolved within a few days of each injection, move to 5 mg. If you had persistent issues at 2.5 mg, consider staying at that dose for two to four more weeks or stepping up to an intermediate dose of 3.5 or 4 mg.
When you increase to 5 mg, expect a temporary return of side effects. This is normal. Each dose increase essentially reintroduces the adaptation period. Nausea may return for three to five days. Appetite suppression will likely intensify. Digestive changes may re-emerge briefly. These effects are typically milder than what you experienced at the initial 2.5 mg dose because your body has already partially adapted to the mechanism.
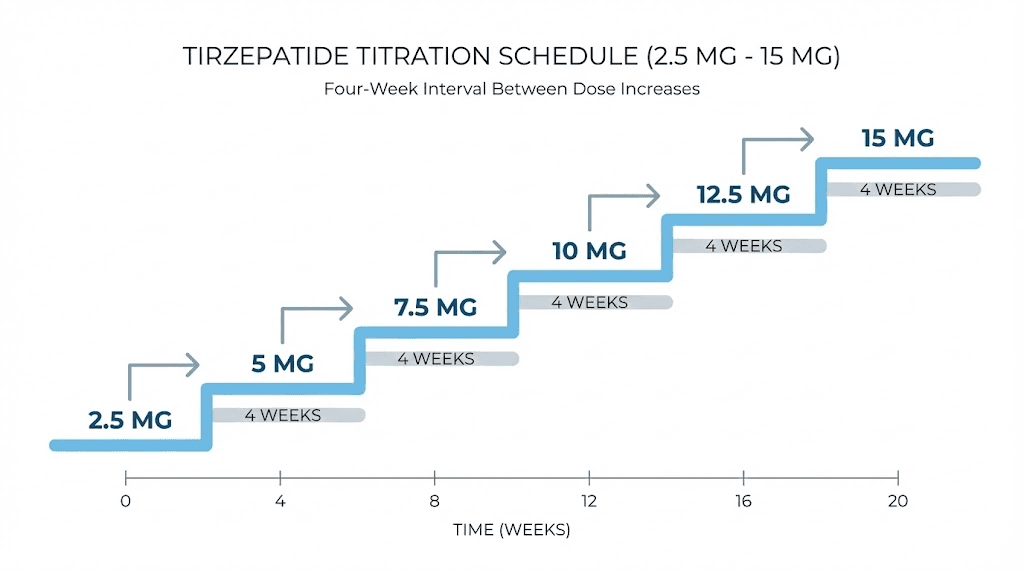
The pattern repeats at each subsequent increase: 5 mg to 7.5 mg, 7.5 mg to 10 mg, and so on. Always wait a minimum of four weeks at each dose before increasing. Some providers recommend staying at each dose for six to eight weeks if the patient is responding well and tolerating the current level without significant issues. There is no rush. The full conversion chart for dosing maps out what each increase looks like in syringe units at your specific concentration.
Maximum dose is 15 mg weekly. Not everyone reaches this level. Many people achieve their goals at 7.5 mg or 10 mg. The "right" maintenance dose is the lowest dose that produces satisfactory results with tolerable side effects. Chasing the maximum dose when you are already seeing good results at a lower dose adds side effect risk without proportional benefit. Your dosing for weight loss guide can help you find the right target based on your progress.
Complete titration schedule from start to maintenance
The standard titration follows a predictable pattern. Each step lasts a minimum of four weeks. Some people spend longer at certain doses. The schedule below represents the most common approach based on clinical trial protocols and provider guidelines.
Phase | Dose | Duration | Units at 10 mg/mL | Units at 20 mg/mL | Primary purpose |
|---|---|---|---|---|---|
Introduction | 2.5 mg | 4 weeks minimum | 25 units | 12.5 units | GI adaptation |
First therapeutic | 5 mg | 4 weeks minimum | 50 units | 25 units | Appetite suppression begins |
Building | 7.5 mg | 4 weeks minimum | 75 units | 37.5 units | Weight loss acceleration |
Moderate | 10 mg | 4 weeks minimum | 100 units | 50 units | Significant metabolic effects |
Higher | 12.5 mg | 4 weeks minimum | 125 units (split) | 62.5 units | Enhanced results |
Maximum | 15 mg | Ongoing | 150 units (split) | 75 units | Peak therapeutic dose |
Note the "split" designation for higher doses at the 10 mg/mL concentration. Once you exceed 100 units (1 mL), you cannot draw the full dose into a single insulin syringe. You would need to split the injection into two draws and two injection sites. This is one reason why many people who plan to titrate to higher doses prefer starting with a 20 mg/mL concentration. At 20 mg/mL, even the maximum 15 mg dose requires only 75 units, which fits comfortably in a single syringe. The compound tirzepatide dosing chart shows exact unit counts at every dose and concentration.
For a visual reference showing how these conversions work across different dose levels, the 25-unit dosage chart explains how specific unit counts translate to milligram doses. Similarly, guides covering how many units is 2.5 mg, how many units is 5 mg, and how many units is 7.5 mg provide concentration-specific answers for the most commonly asked dose conversions.
What about the reverse calculation? Some people look at their syringe and want to know what dose they are actually injecting. Resources covering how many mg is 20 units, how many mg is 30 units, how many mg is 40 units, and how many mg is 50 units walk through those reverse calculations for every concentration.
The speed of titration matters less than consistency. Someone who reaches 10 mg in 16 weeks with steady adherence will have better outcomes than someone who rushes to 15 mg in 8 weeks and quits because the side effects are unbearable. Slow and steady is not just a cliche here. It is the strategy backed by clinical evidence.
Common starting dose mistakes and how to avoid them
Mistakes during the starting phase are surprisingly common. Most are preventable with the right information. Here are the ones that trip people up most frequently, along with how to avoid each one.
Using the wrong concentration in calculations
This is the most dangerous mistake. If your vial is 20 mg/mL but you calculate as if it is 10 mg/mL, you will inject double your intended dose. A 2.5 mg dose calculated at 10 mg/mL is 25 units. But 25 units from a 20 mg/mL vial delivers 5 mg, double the starting dose. Always read the concentration directly from your vial label before calculating. Never rely on memory or assume it is the same as last time. The dosage chart in units organized by concentration can serve as a quick cross-reference.
Increasing the dose too quickly
The four-week minimum at each dose exists for good reason. Some people feel great at 2.5 mg after two weeks and decide to jump to 5 mg early. This almost always results in worse side effects than would have occurred with proper timing. Your GI tract needs the full four weeks to adapt, even if you feel fine after two. The complete dosing guide emphasizes this timeline for a reason.
Skipping the starting dose entirely
Some people, particularly those who have used semaglutide or other GLP-1 medications previously, think they can skip 2.5 mg and start at 5 mg. While some providers do allow experienced patients to start at 5 mg, this is a clinical decision that should be made with medical guidance. Tirzepatide has a dual mechanism (GLP-1 plus GIP) that is different from semaglutide, and even experienced GLP-1 users can experience new or different side effects. Starting at 2.5 mg, even briefly, gives your body time to adapt to the GIP receptor activation specifically.
Injecting at inconsistent intervals
Tirzepatide is a once-weekly injection. The keyword is "weekly." That means the same day each week, at approximately the same time. Injecting on Monday one week, Thursday the next, and Sunday after that creates inconsistent blood levels that can worsen side effects and reduce effectiveness. Pick a day. Stick to it. If you need to shift your injection day, the general guidance is that you can take tirzepatide a day early if necessary, but make it the exception rather than the habit. For guidance on optimal timing, the best time to take your GLP-1 shot resource covers scheduling strategies.
Not eating enough protein
Reduced appetite is a feature, not a bug. But it can lead to inadequate protein intake if you are not intentional about your diet. At the starting dose, this is less of a concern because appetite suppression is modest. But establishing good habits now matters. Aim for at least 0.7 to 1.0 grams of protein per pound of body weight daily. This protects muscle mass during weight loss, which becomes increasingly important as you titrate to higher doses. The tirzepatide diet plan and what to eat on tirzepatide guides both emphasize protein-forward eating strategies. For supplemental protein options, protein shakes designed for GLP-1 users offer convenient solutions when solid food feels unappealing.
Ignoring hydration
This sounds basic. It is basic. But dehydration is behind many of the most common complaints during the starting phase: headaches, constipation, fatigue, dizziness. Tirzepatide does not directly cause dehydration, but eating less means you get less water from food. Nausea can make you avoid drinking. And if you do experience diarrhea, fluid loss increases. Aim for 80 to 100 ounces of water daily during the starting phase. Add electrolytes if needed.
Comparing your progress to others
Online communities are full of people sharing their results. Some report dramatic changes in the first week. Others share frustration about slow progress. The reality is that individual responses to tirzepatide vary enormously based on starting weight, metabolic health, insulin sensitivity, genetics, diet, activity level, and dozens of other factors. Your starting dose experience will be unique. The timeline for tirzepatide results shows the typical range, but your personal trajectory may fall anywhere within it. If you are not seeing results, the troubleshooting guide for weight loss on tirzepatide covers the most common reasons and fixes.
Reconstitution basics for your starting dose
Some compounded tirzepatide arrives as a ready-to-use liquid in a vial. Others arrive as lyophilized (freeze-dried) powder that requires reconstitution before use. If yours arrives as a liquid, you can skip this section. If it is a powder, read carefully.
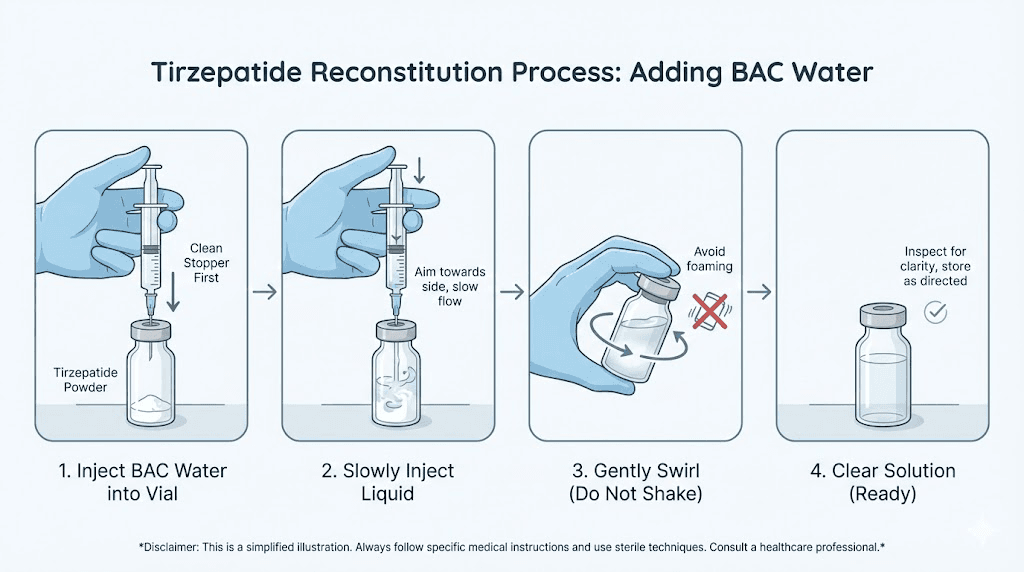
Reconstitution means adding a specific volume of diluent to the powder to create an injectable solution at your target concentration. The most common diluent for compounded tirzepatide is bacteriostatic water (BAC water), which contains 0.9% benzyl alcohol to prevent bacterial growth. This is the preferred diluent for multi-dose vials because it allows the solution to remain sterile across multiple needle punctures over several weeks.
The process is straightforward but demands attention to detail. Clean everything with alcohol swabs first: the vial stopper, the BAC water vial stopper, and the injection site on your skin. Draw the correct volume of BAC water into a syringe. Insert the needle into the tirzepatide vial and inject the water slowly along the inside wall of the vial. Do not spray it directly onto the powder. Do not shake the vial. Gently roll it between your palms until the powder dissolves completely. The solution should be clear and colorless. If it is cloudy, contains particles, or appears discolored, do not use it.
The volume of BAC water you add determines the concentration. For a 10 mg vial, adding 1 mL creates a 10 mg/mL solution. Adding 2 mL creates a 5 mg/mL solution. The tirzepatide reconstitution guide walks through this process step by step with photos for every stage. The reconstitution chart shows exact volumes for every vial size and target concentration.
If you are new to reconstitution entirely, the broader peptide reconstitution guide covers universal principles that apply to all peptides, including tirzepatide. Understanding how to mix peptides with BAC water and how much bacteriostatic water to add are foundational skills that will serve you throughout your use of any compounded peptide.
For a printable reference you can keep near your supplies, the reconstitution chart PDF and the reconstituting tirzepatide chart both provide at-a-glance references. The peptide reconstitution calculator lets you input your vial size and desired concentration to get exact water volumes.
Storage requirements for compounded tirzepatide
Proper storage starts the moment your vial arrives. Get it into the refrigerator promptly.
Compounded tirzepatide, whether liquid or reconstituted from powder, should be stored at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). This is standard refrigerator temperature. Place the vial in the main body of the fridge, not in the door where temperature fluctuates with every opening. Not in the back where it might freeze against the cooling element. The middle shelf, toward the center, is ideal. The tirzepatide refrigeration guide covers the reasoning and best placement in detail.
Never freeze tirzepatide. Freezing damages the peptide structure irreversibly. A vial that has been frozen should be discarded, even if it looks normal after thawing. The molecular bonds that make tirzepatide effective are disrupted by ice crystal formation, and there is no way to reverse that damage.
How long does it last? For multi-dose vials, most compounding pharmacies assign a beyond-use date (BUD) of 28 to 90 days from the date the vial is first punctured. This varies by pharmacy and formulation. Always check the label or accompanying documentation for your specific product. The shelf life guide breaks down storage timelines for different formulations. Understanding tirzepatide expiration ensures you do not use product that has degraded past its effective window.
Room temperature storage is acceptable for short periods. Most compounded tirzepatide can be kept at room temperature (up to 77 to 86 degrees Fahrenheit) for up to 21 days. This allows for travel or situations where refrigeration is temporarily unavailable. If the vial has been at room temperature for longer than 21 days, discard it. The out-of-fridge storage guide covers travel scenarios and emergency storage solutions.
For broader peptide storage principles that apply to tirzepatide and every other compound you might use, the peptide storage guide provides a comprehensive framework.
Diet and lifestyle at starting dose
The starting dose is the perfect time to build habits that will support your results long term. Appetite suppression at 2.5 mg is modest, which means you still have enough hunger signals to make conscious food choices rather than being forced into them by complete appetite loss (which can happen at higher doses).
Protein prioritization
This cannot be overstated. When you eat less total food, the composition of what you do eat matters enormously. Protein preserves lean muscle mass during weight loss, supports metabolic rate, and improves satiety. Aim for 25 to 30 grams of protein at each meal. Good sources include chicken, fish, eggs, Greek yogurt, cottage cheese, and lean beef. If hitting protein targets feels difficult with reduced appetite, protein shakes formulated for GLP-1 users can bridge the gap. The complete tirzepatide meal plan provides structured daily templates.
Foods to prioritize and avoid
At the starting dose, your digestive system is adjusting to slowed gastric emptying. Foods that are easy to digest will be your allies. Lean proteins, cooked vegetables, whole grains, and fruits work well for most people. Foods that commonly cause problems during the adjustment period include fried foods, very fatty meals, raw vegetables in large quantities, carbonated beverages, and high-sugar desserts. The complete food avoidance list and the what to eat guide provide specific recommendations organized by meal type.
Alcohol considerations
A common question during the starting phase is whether you can drink alcohol. The short answer is that alcohol is not contraindicated with tirzepatide, but it does interact with the medication effects in ways you should understand. Tirzepatide slows gastric emptying, which means alcohol stays in your stomach longer and can be absorbed differently than you are used to. Many people report feeling the effects of alcohol faster and more intensely while on tirzepatide. One drink might feel like two or three. The alcohol and tirzepatide guide covers the full interaction profile and practical strategies for social drinking.
Supplements worth considering
Reduced food intake can lead to micronutrient gaps. A quality multivitamin is a reasonable baseline. Beyond that, specific supplements can support the starting phase: magnesium for constipation prevention and sleep quality, B vitamins for energy, and electrolytes for hydration. Some people also take fiber supplements to support digestive regularity. The supplements to take with tirzepatide guide ranks the most evidence-supported options and explains dosing for each. If your compound already contains B12 or niacinamide, you may not need additional supplementation of those specific nutrients.
Exercise at starting dose
Do not overhaul your exercise routine during the first four weeks. Your body is adapting to tirzepatide while simultaneously adjusting to reduced caloric intake. Adding intense new exercise on top of that creates three simultaneous stressors, which increases fatigue and can worsen side effects. If you already exercise regularly, continue at your current level. If you do not exercise, start with walking. Fifteen to thirty minutes of daily walking is sufficient during the starting phase and supports digestion, mood, and sleep quality.
Resistance training becomes increasingly important as you titrate to higher doses and lose more weight. Building and maintaining muscle mass during weight loss preserves metabolic rate and improves body composition outcomes. But the first four weeks are not the time to start a heavy lifting program. Focus on establishing the tirzepatide routine first, then layer in structured exercise as your body adapts. For a comprehensive approach to diet planning on tirzepatide, the full plan integrates nutrition, supplementation, and activity recommendations by dose level.
Switching from semaglutide to compounded tirzepatide
If you are currently on semaglutide (compounded, Ozempic, or Wegovy) and switching to compounded tirzepatide, the starting dose question takes on additional nuance. You are not starting from zero. Your body is already adapted to GLP-1 receptor activation. But tirzepatide adds GIP receptor activation on top of that, which is a new mechanism your system has not encountered.
The conservative approach is to start tirzepatide at 2.5 mg regardless of your semaglutide dose. This is the safest path because it allows your body to adapt to the dual-receptor mechanism gradually. Even if you were on 2.4 mg of semaglutide (the maximum dose), the GIP component of tirzepatide is entirely new to your system. The switching guide walks through the full transition process.
Some providers allow patients who tolerated semaglutide well to start tirzepatide at 5 mg. This skips the introductory phase and gets to the first therapeutic dose faster. The rationale is that patients who have already adapted to GLP-1 activation have a lower risk of GI side effects at the starting dose. This approach works for many people, but it is a clinical decision that should be made in consultation with a provider who knows your history.
Timing the switch is important. Wait at least seven days after your last semaglutide injection before taking your first tirzepatide dose. Both medications are weekly injections, so the simplest approach is to take your last semaglutide dose on its normal day, then start tirzepatide seven days later on the same weekday. This maintains consistent weekly dosing without overlap.
For dose equivalence between the two medications, the semaglutide to tirzepatide conversion chart provides a framework. However, there is no exact one-to-one conversion because the medications work through different receptor profiles. The switching dosage chart and the dose conversion chart both account for this complexity. For those going in the opposite direction, the tirzepatide to semaglutide conversion resource covers that scenario as well.
Expect some adjustment even if your semaglutide transition was smooth. The GIP receptor activation produces effects that are distinct from pure GLP-1 stimulation. You might notice different appetite patterns, different energy levels, or different GI responses than you experienced on semaglutide. The side effect comparison between the two medications highlights what is similar and what differs. For a broader comparison, the dosage comparison chart shows how the medications stack up across all dose levels.
If you switched because semaglutide stopped working, a phenomenon sometimes called "GLP-1 plateau," tirzepatide dual mechanism often re-initiates weight loss. The tirzepatide not working guide covers what to do if you hit a similar plateau on tirzepatide. Understanding how tirzepatide affects metabolism can help set realistic expectations for the transition period.
Choosing your compounding pharmacy
Not all compounding pharmacies are equal. The quality, concentration options, pricing, and support vary significantly between providers. Since your starting dose experience depends partly on the quality of the compounded product, choosing the right pharmacy matters.
Several pharmacies have established reputations in the compounded tirzepatide space. Empower Pharmacy is one of the largest 503B outsourcing facilities, with the Empower dosage chart covering their specific formulations. Other providers like Priority Meds, Orderly Meds, and Lavender Sky each have their own formulations and concentration options. For cost-conscious users, the affordable tirzepatide and compounded tirzepatide cost guide compare pricing across providers.
Provider-specific dosing charts from pharmacies like Southend Pharmacy, Mochi Health, and Olympia Pharmacy exist because each pharmacy may compound at different concentrations. Always use the dosing chart specific to your pharmacy and concentration. A generic chart from a different provider can lead to dosing errors.
What to look for when choosing a pharmacy: 503B registration (indicates higher manufacturing standards), third-party testing for purity and potency, clear labeling with concentration and beyond-use date, responsive customer support, and transparent sourcing of active pharmaceutical ingredients. The Peptide Sciences guide covers one additional sourcing option, and the peptide cost calculator helps you compare total treatment costs across providers based on your expected titration schedule.
Injection technique for beginners
If this is your first time self-injecting, the process can feel intimidating. It should not be.
Subcutaneous injection means the needle goes into the fatty tissue just below the skin. Not into muscle. Not into a vein. Just into the soft layer of fat that everyone has, particularly around the abdomen, thighs, and upper arms. The needles used for tirzepatide injection are small, typically 29 to 31 gauge and 0.5 inches long. Most people describe the sensation as a brief pinch that lasts less than a second.
The abdomen is the most common injection site, specifically the area around the belly button but at least two inches away from the navel itself. The stomach injection guide shows the exact zones with visual references. Pinch a fold of skin, insert the needle at a 90-degree angle, push the plunger slowly and steadily, wait five seconds after the plunger is fully depressed, then withdraw the needle. That is the entire process.
Rotate injection sites. Do not inject in the same spot every week. Move at least one inch from the previous injection site. Alternating between left and right sides of the abdomen, or rotating between abdomen, thigh, and upper arm, prevents lipohypertrophy (the development of hard lumps under the skin from repeated injection in the same location). The GLP-1 injection location guide maps out a rotation pattern. For general technique applicable to all injectable peptides, the GLP-1 injection technique guide and the broader peptide injection guide cover everything from preparation to disposal.
Common injection mistakes include injecting too quickly (which can increase pain and cause medication to leak back out), not pinching enough skin (which can result in intramuscular injection rather than subcutaneous), and pulling the needle out too soon (which can cause medication to leak). Take your time. There is no rush. A slow, deliberate injection is always better than a fast, sloppy one.
Alternative forms of tirzepatide
While injectable tirzepatide is the standard, some people explore alternative delivery methods. These are worth understanding even if you are starting with injections, because you might consider switching formats later.
Oral tirzepatide is in development and has shown promising results in clinical trials. The oral versus injection comparison examines the differences in bioavailability, dosing, and convenience. For a deeper look at the form factor debate, the tablets versus injections analysis covers practical considerations. Some compounding pharmacies also offer sublingual tirzepatide drops, though absorption rates differ from injectable forms. The broader injectable versus oral peptides comparison on SeekPeptides provides context for understanding how delivery method affects bioavailability across all peptide types.
Stacking and combination protocols
Some users combine tirzepatide with other compounds during or after the starting phase. While this is a more advanced topic, understanding the landscape helps you make informed decisions as you progress through your protocol.
The combination of phentermine and tirzepatide is one of the most commonly discussed. Phentermine is a traditional appetite suppressant that works through a different mechanism than tirzepatide. Some providers prescribe both together, particularly during the starting phase when tirzepatide appetite suppression has not fully developed. The phentermine comparison provides useful context for understanding how these different approaches to appetite suppression interact.
Other combinations include AOD-9604 with tirzepatide for targeted fat metabolism and cagrilintide with tirzepatide for enhanced amylin receptor activation. These are not starting dose considerations, but knowing they exist helps you plan your longer-term strategy. For exploring multiple peptide combinations, the peptide stack calculator evaluates compatibility and timing. The peptide dosing guide provides general principles, and the peptide dosage chart covers standard dose ranges across commonly used compounds.
If you are considering any combination protocol, the peptide safety and risks guide should be mandatory reading. The getting started with peptides overview provides foundational knowledge that applies regardless of which compounds you use.
Comparing tirzepatide with other weight loss peptides
Understanding where tirzepatide fits in the broader landscape of weight management peptides helps you confirm whether it is the right choice for your goals, particularly before committing to a starting dose and full titration schedule.
The most common comparison is semaglutide versus tirzepatide. Semaglutide activates only GLP-1 receptors. Tirzepatide activates both GLP-1 and GIP receptors. In head-to-head clinical data, tirzepatide produces approximately 5% to 7% greater total body weight reduction than semaglutide at comparable treatment durations. The dual mechanism also produces somewhat different side effect profiles, which the side effect comparison details thoroughly. If you are considering semaglutide instead, understanding how fast semaglutide works relative to tirzepatide can inform your decision.
Newer competitors are emerging. Survodutide is a dual GLP-1/glucagon receptor agonist in clinical trials showing promising weight loss results. Mazdutide is another dual agonist being developed primarily in China. Orforglipron is notable because it is an oral GLP-1 agonist, potentially eliminating the need for injections entirely. These medications are all in various stages of development and approval, and their specific starting doses and titration schedules differ from tirzepatide. The broader semaglutide versus tirzepatide comparison page and the peptides for fat loss overview provide additional context.
Understanding the relationship between GLP-1 medications and brand names helps navigate the often confusing naming landscape. And for those concerned about long-term dependency, learning about GLP-1 withdrawal and fatigue patterns on these medications provides a more complete picture of the treatment arc.
Monitoring your response to the starting dose
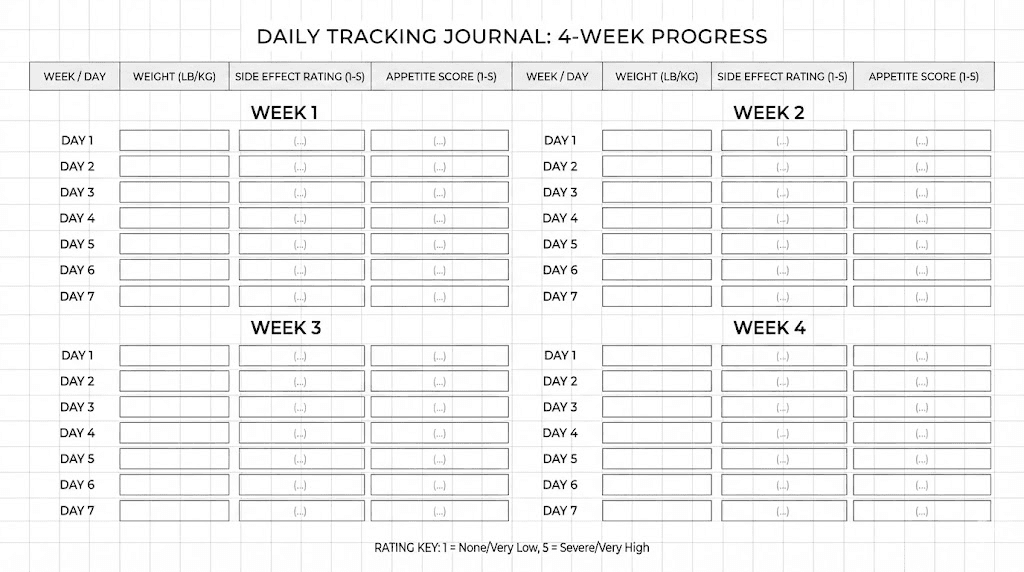
Data beats feelings. Track these metrics from day one so you have objective information when deciding whether to increase your dose, adjust your approach, or troubleshoot problems.
Weight: Weigh yourself at the same time each day, ideally first thing in the morning after using the bathroom and before eating or drinking. Daily weight fluctuates by 1 to 3 pounds due to water retention, food volume, and hormonal shifts. The trend over four weeks matters more than any single day reading. A simple moving average (average of the past 7 days) smooths out fluctuations and reveals the true trajectory.
Side effects: Keep a brief daily log noting any nausea, digestive changes, energy levels, or other symptoms. Include severity (1 to 10 scale) and duration. This log becomes invaluable when discussing dose adjustments with your provider. It also helps you identify patterns, like side effects that consistently appear on injection day plus two but resolve by day four.
Appetite: Rate your appetite at each meal on a simple scale. This helps you distinguish between true appetite suppression from tirzepatide and reduced eating from nausea or food aversion. True appetite suppression feels like genuinely not being hungry. Food aversion from nausea feels like wanting to eat but being unable to. The distinction matters for titration decisions.
Measurements: Waist circumference is often a more reliable indicator of progress than scale weight during the early weeks. Measure at the same point (typically at the navel) weekly. Some people lose inches before pounds, as body composition shifts can precede scale changes. The before and after results documentation shows how tracking multiple metrics paints a more complete picture. The results for men specifically may differ from general population data due to differences in body composition and hormonal profiles.
Special considerations for your starting dose
Pregnancy and fertility
Tirzepatide is not recommended during pregnancy. More importantly, tirzepatide can increase fertility even in people who previously had difficulty conceiving. Weight loss and improved insulin sensitivity can restore ovulation in women with PCOS or obesity-related anovulation. The phenomenon of getting pregnant on tirzepatide is well-documented and something to be aware of, especially at the starting dose when you might not think the medication is "doing much." Use reliable contraception if pregnancy is not desired.
Hair loss concerns
Some users report hair shedding during the first few months of GLP-1 treatment. This is typically related to the caloric deficit and rapid weight loss rather than a direct drug effect, and it is more common at higher doses than at the starting dose. The GLP-1 hair loss guide covers causes, prevention, and treatment strategies. Adequate protein intake is the single most important protective factor.
Anxiety
Rarely, some individuals report increased anxiety when starting tirzepatide. Whether this is a direct pharmacological effect or related to the stress of starting a new medication and changing eating patterns is debated. The tirzepatide and anxiety guide examines the evidence and provides management strategies. If you have a pre-existing anxiety disorder, discuss this with your provider before starting.
Frequently asked questions
What happens if I accidentally inject more than 2.5 mg as my starting dose?
A single accidental overdose at the starting phase, such as injecting 5 mg instead of 2.5 mg, is unlikely to cause serious harm but will likely produce more pronounced side effects. Expect increased nausea, possibly vomiting, and significant appetite suppression for several days. Stay hydrated, eat small bland meals when possible, and monitor for severe symptoms. Contact your provider if symptoms are severe or you are unable to keep fluids down. Going forward, double-check your dosage chart in units and verify the concentration on your vial before every injection.
Can I split my starting dose into two injections per week?
Some providers recommend splitting the weekly dose into two smaller injections (for example, 1.25 mg twice per week instead of 2.5 mg once per week). The rationale is that smaller, more frequent doses may produce steadier blood levels and reduce peak-related side effects. This is not the standard protocol from clinical trials, and there is limited data on its effectiveness. Discuss this approach with your provider if you are interested. The compound dosage chart can help you calculate half-dose volumes.
How quickly will I lose weight on the 2.5 mg starting dose?
Weight loss at the starting dose is modest, typically 1 to 5 pounds over four weeks, and not everyone sees scale changes at all. The 2.5 mg dose is an acclimation dose, not a therapeutic dose. Meaningful weight loss typically begins at 5 mg and becomes significant at 10 mg and above. The tirzepatide timeline guide covers realistic expectations at each dose level.
Should I take my starting dose with food or on an empty stomach?
Tirzepatide is injected subcutaneously, so food in your stomach does not affect absorption. You can inject with or without food. However, many people find that injecting after a light meal reduces the severity of nausea compared to injecting on a completely empty stomach. Experiment to find what works best for you. Review the best time to take your GLP-1 shot for additional timing strategies.
Is the starting dose the same for men and women?
Yes. The standard 2.5 mg starting dose applies regardless of sex. Clinical trials used the same starting dose and titration schedule for all participants. Body weight, metabolic rate, and hormonal differences can influence how individuals respond, but the starting dose itself does not change. The tirzepatide results for men and general before and after results show the range of outcomes across both sexes.
What if I feel nothing at the starting dose?
Feeling nothing at 2.5 mg is normal and does not mean the medication is not working. The starting dose is sub-therapeutic for weight loss. Its purpose is adaptation, not results. Many people experience no noticeable appetite suppression, no side effects, and no weight change at 2.5 mg. This does not predict how you will respond at higher doses. Complete the full four weeks and move to 5 mg as planned. If you still feel nothing at 5 mg after four weeks, the troubleshooting guide covers potential causes and solutions.
Can I use a compounded tirzepatide vial that has been at room temperature for travel?
Most compounded tirzepatide can be kept at room temperature (up to 86 degrees Fahrenheit) for up to 21 days without significant degradation. For travel, this provides a reasonable window. Use an insulated pouch if possible, avoid leaving the vial in direct sunlight or a hot car, and return it to refrigeration as soon as you can. The out-of-fridge storage guide provides specific travel recommendations.
Do I need to use the semaglutide dosage calculator if switching from Ozempic to compounded tirzepatide?
The semaglutide dosage calculator is designed for semaglutide dosing specifically, not for tirzepatide conversion. When switching, use the semaglutide to tirzepatide conversion chart for dose mapping guidance, and then use the peptide calculator or compounded tirzepatide dosage calculator to determine the correct syringe volume for your tirzepatide concentration.
External resources
For those serious about getting their compounded tirzepatide protocols right from the very first injection, SeekPeptides provides the most comprehensive dosing resources available, with evidence-based guides, concentration-specific calculators, and a community of thousands who have navigated these exact calculations and titration decisions.
In case I do not see you, good afternoon, good evening, and good night. May your starting dose stay accurate, your titration stay patient, and your results stay consistent.