Feb 21, 2026
You started tirzepatide expecting weight loss. What you got instead was a bathroom emergency.
Maybe it hit you 24 hours after your first injection. Maybe it waited until the second week, lurking quietly before turning your digestive system upside down. Either way, you are now asking the same question thousands of other people have typed into Google at 2 AM while clutching their stomach: how long does this last?
Here is the honest answer. For most people, tirzepatide-related diarrhea resolves within 3 to 7 days after each dose change. Clinical trials put the average duration at roughly 3 days. But averages hide a lot of individual variation, and some people deal with this for 2 to 4 weeks before their body fully adjusts. The good news is that it almost always gets better. The body adapts. The gut calms down. And there are specific, proven strategies that can speed that process along considerably.
This guide covers everything: the exact clinical data on duration by dose, why tirzepatide causes diarrhea in the first place, a complete management protocol that actually works, what foods help and which ones make it worse, when diarrhea signals something more serious, and how tirzepatide compares to semaglutide for GI side effects. Whether you are on your first week or struggling through a dose escalation, you will find the answers here.
How long tirzepatide diarrhea actually lasts: the clinical data
Let us start with what the research actually says, not vague reassurances, but specific numbers from real clinical trials.
In the SURPASS and SURMOUNT trial programs involving thousands of participants, diarrhea was one of the most commonly reported gastrointestinal side effects. The data paints a clear picture. Most episodes resolve within days, not weeks. But timing matters enormously, and the dose you are on changes the equation.
Average duration by the numbers
A systematic review and meta-analysis published in Cureus analyzed data from six randomized controlled trials involving 4,586 participants. The average duration of a diarrhea episode on tirzepatide was approximately 3 days. That is the median. Some people experienced it for just one day. Others dealt with intermittent symptoms for up to 2 to 4 weeks, particularly during the initial dose escalation period.
The important distinction is between a single episode and ongoing symptoms. A single bout of diarrhea after your injection might last 1 to 3 days. But if you are escalating doses every 4 weeks, you might experience a fresh round of GI symptoms with each increase, making it feel continuous even though each individual episode is relatively short.
Duration by dose level
The dose matters. A lot.
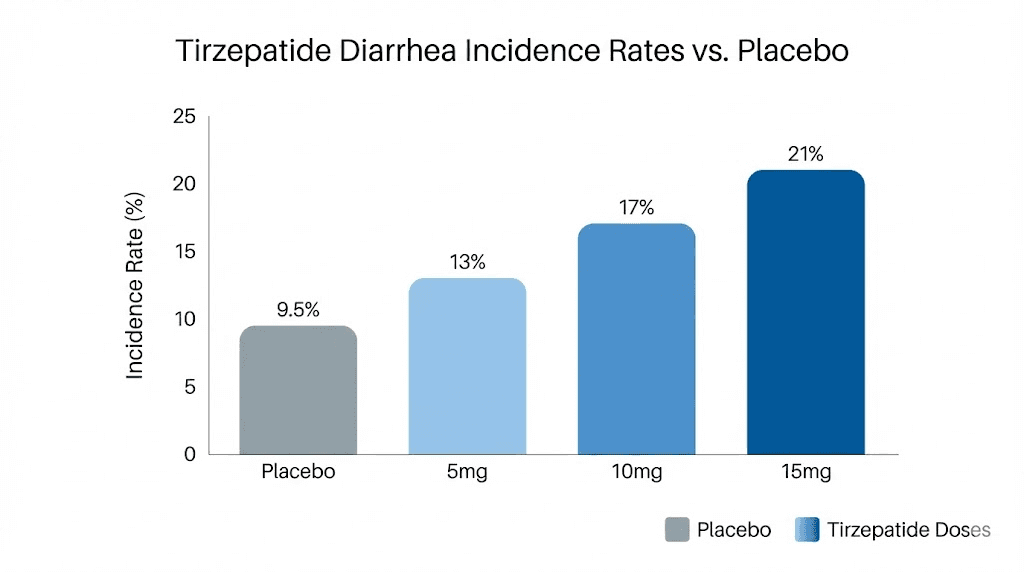
In the SURMOUNT-1 trial, diarrhea rates were clearly dose-dependent. At the 5 mg dose, 18.7% of participants reported diarrhea. At 10 mg, that number climbed to 21.2%. And at the 15 mg dose, 23.0% experienced it. The pattern is consistent: higher doses mean higher likelihood of diarrhea, but also potentially longer duration before the body adjusts.
Across all the SURPASS trials for type 2 diabetes, diarrhea occurred in 12% to 22% of participants depending on dose. The pooled analysis showed overall GI adverse event rates of 39% at 5 mg, 46% at 10 mg, and 49% at 15 mg. These numbers include all GI symptoms, not just diarrhea, but they illustrate the dose-response relationship clearly.
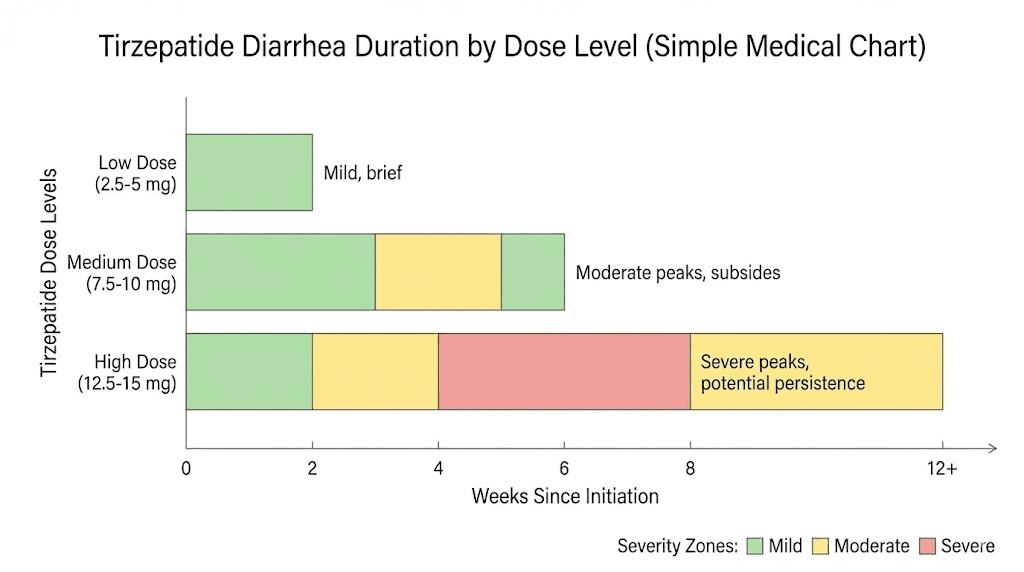
What does this mean practically? If you are on the starting dose, your diarrhea is more likely to resolve quickly, often within 2 to 3 days. If you just jumped to a higher dose, give yourself a full week before panicking. And if you are at the maximum 15 mg, your adjustment period might stretch to 2 to 3 weeks.
When it typically appears and resolves
Most people notice diarrhea within 24 to 48 hours after their injection. It peaks around days 2 to 3 and then gradually improves. By day 5 to 7, the majority of people report significant improvement. This pattern tends to repeat with each dose escalation, though many people find that subsequent adjustments produce milder symptoms as the body develops some tolerance to the medication.
There is a critical detail most guides miss. The severity and duration tend to decrease with each dose increase you survive. Your first escalation from 2.5 mg to 5 mg might be rough. But the jump from 10 mg to 15 mg, while it produces symptoms in more people statistically, often feels less severe for any given individual because the gut has already partially adapted to the GLP-1 and GIP receptor stimulation.
Why tirzepatide causes diarrhea in the first place
Understanding the mechanism helps you manage it better. This is not random. There are specific, well-studied reasons why tirzepatide affects your digestive system so profoundly.
The dual agonist effect
Tirzepatide is a dual GLP-1 and GIP receptor agonist. That means it mimics two gut hormones simultaneously, something no other weight loss medication on the market does in quite the same way. This dual action is what makes it so effective for weight loss and blood sugar control. But it also means a double dose of gastrointestinal stimulation.
GLP-1 slows gastric emptying. Your stomach takes longer to push food into the small intestine. This is actually a feature, not a bug, because it helps you feel full longer and reduces appetite. But it also disrupts the normal rhythm of your digestive tract.
GIP, the other hormone tirzepatide mimics, plays a different role. It increases intestinal fluid secretion. More fluid in your intestinal lumen means looser stools. Combined with the altered motility from GLP-1 stimulation, you get the perfect recipe for diarrhea, especially when the body has not had time to adapt.
Altered intestinal motility
Here is where it gets counterintuitive. While tirzepatide slows how quickly food leaves your stomach, it can actually speed up transit through the intestines. The muscular contractions that push food through your gut, called peristalsis, get disrupted. When things move too fast through the colon, there is not enough time for water to be absorbed back into the body. The result? Loose, watery stools.
This altered motility works through two pathways. The first is parasympathetic, operating through the vagus nerve. The second is direct central nervous system stimulation. Both pathways get activated when you introduce a potent GLP-1 agonist into the system, and both contribute to the disruption of normal bowel habits.
Gut microbiome changes
Research suggests that GLP-1-based therapies modify the gut microbiome. The composition of bacteria in your gut shifts, and this can affect fermentation patterns, gas production, and fluid balance. These changes are not inherently bad. Some researchers believe they may even contribute to the metabolic benefits of tirzepatide. But during the transition period, while your microbiome is adjusting, digestive symptoms like diarrhea, bloating, and gas are common.
The microbiome adjustment is one reason probiotics can help during the early weeks of treatment. We will get to that in the management section.
Increased bile acid secretion
GLP-1 receptor agonists can alter bile acid metabolism. Bile acids play a crucial role in fat digestion, and when their secretion pattern changes, it can draw excess water into the colon. This is the same mechanism behind bile acid diarrhea, a condition well-known in gastroenterology. On tirzepatide, this effect is usually mild and temporary, but it contributes to the overall GI disruption during the adjustment period.
The complete management protocol that actually works
Knowing why it happens is useful. Knowing how to make it stop is essential. Here is a structured approach based on clinical recommendations and what experienced users report actually works. Not generic advice. Specific, actionable steps you can implement today.
Phase 1: The first 72 hours (acute management)
When diarrhea first hits after a new dose, your immediate priorities are hydration and damage control.
Hydration is non-negotiable. Diarrhea causes rapid fluid and electrolyte loss. You need to replace both. Plain water is not enough. You need sodium, potassium, and glucose to drive proper absorption. Oral rehydration solutions work best. Sports drinks are a decent second choice, though they often contain too much sugar. Bone broth is an underrated option that provides sodium, potassium, and easy-to-absorb protein.
Aim for at least 8 to 10 glasses of fluid per day, more if episodes are frequent. Sip consistently rather than drinking large amounts at once, which can trigger another round of GI distress. If you are also avoiding alcohol during this period, which you absolutely should be, replace those social drinks with electrolyte water or herbal tea.
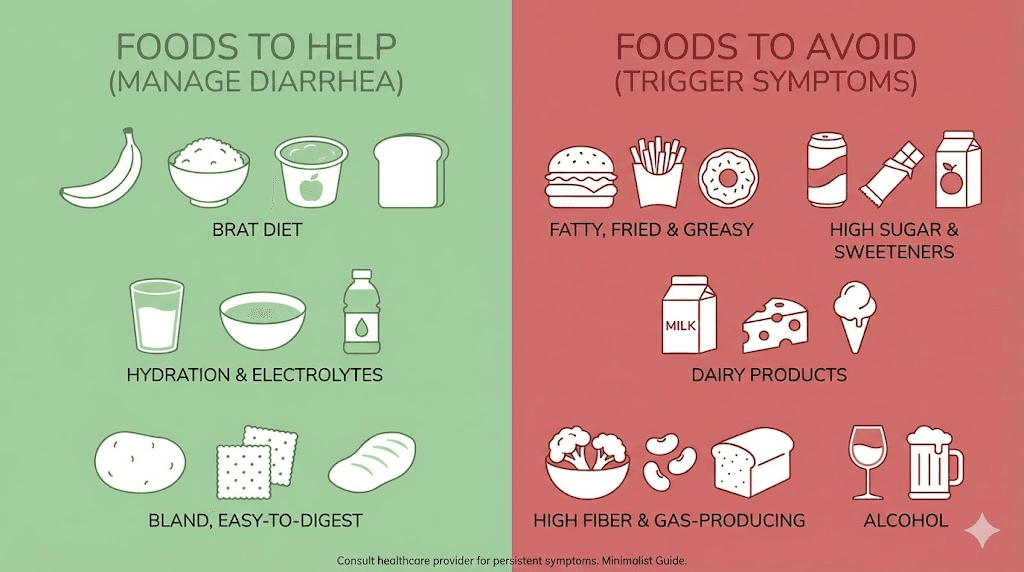
The modified BRAT approach. The classic BRAT diet (bananas, rice, applesauce, toast) has fallen out of favor with nutritionists because it lacks complete nutrition. But for the first 24 to 48 hours of acute diarrhea, it remains genuinely helpful. These foods are low in fiber, easy to digest, and contain pectin that helps firm up stools. Bananas in particular are excellent because they replace lost potassium.
Do not stay on BRAT for more than 2 days. It is a bridge, not a destination. After the acute phase, gradually reintroduce lean proteins, cooked vegetables, and well-tolerated grains.
Over-the-counter options. Loperamide (Imodium) can provide relief for acute episodes. It works by slowing intestinal motility, directly counteracting one of the mechanisms causing the diarrhea. However, talk to your prescribing physician before making this a regular strategy, as it can mask symptoms that might indicate a need for dose adjustment. Bismuth subsalicylate (Pepto-Bismol) is another option that can reduce stool frequency and provide some comfort.
Phase 2: Days 3 to 7 (stabilization)
By this point, the worst should be subsiding. Now is the time to rebuild your digestive function.
Introduce probiotics. Specific strains show evidence for managing antibiotic and medication-induced diarrhea. Lactobacillus rhamnosus GG and Saccharomyces boulardii have the strongest evidence base. You can get these through supplements or through fermented foods like yogurt, kefir, and sauerkraut. Start with a small serving and increase gradually.
Probiotics work by restoring the balance of your gut microbiome, which tirzepatide is actively reshaping. They do not prevent diarrhea entirely, but they can reduce duration and severity. Many experienced users consider them essential for the first few months of treatment.
Fiber strategy. This is where most guides get it wrong. They say either eat more fiber or eat less fiber. The truth is more nuanced. During active diarrhea, reduce insoluble fiber (bran, raw vegetables, nuts) which speeds up transit. But gradually increase soluble fiber (oats, sweet potatoes, psyllium husk) which absorbs water and adds bulk to stools. The key word is gradually. Too much too fast will make things worse.
Meal timing and size. Smaller, more frequent meals are significantly easier on your system than three large ones. This is true on tirzepatide generally, but especially important during GI flare-ups. Eat 5 to 6 smaller meals rather than 2 to 3 large ones. This reduces the volume your stomach needs to process at any given time, which means less disruption to intestinal motility.
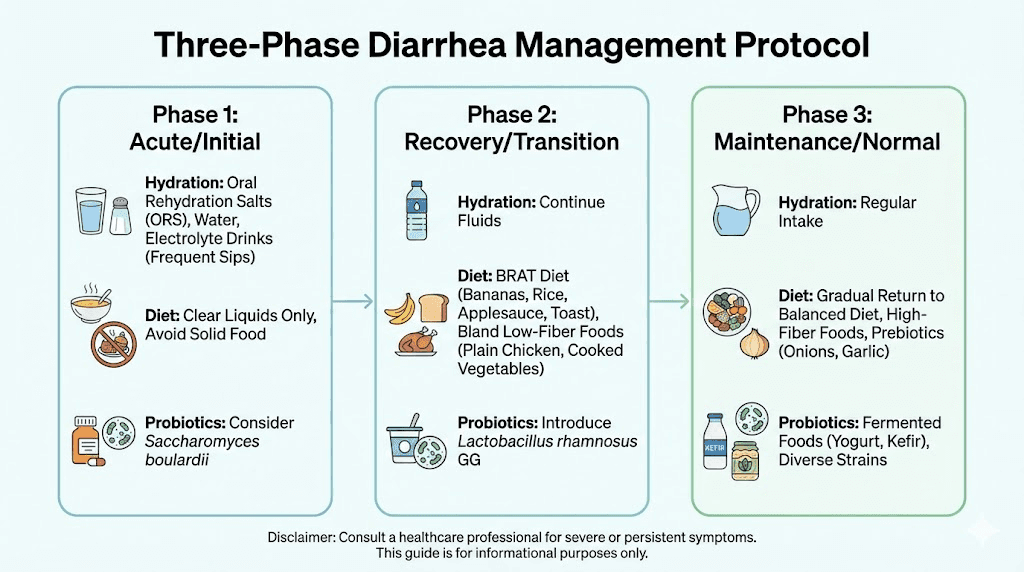
Phase 3: Weeks 2 to 4 (long-term adaptation)
If you are still experiencing some symptoms at this point, do not panic. Many people need a full 2 to 4 weeks to fully adapt, especially at higher doses. The goal now is optimization.
Food journal. Track what you eat and when symptoms flare. Patterns will emerge quickly. Some people discover that dairy is a trigger. Others find that high-fat meals cause problems while lean protein is fine. The foods to avoid on tirzepatide list is a starting point, but your individual triggers may be different.
Timing your injection. Some users report better GI tolerance when they inject on a specific day relative to their schedule. If you inject on Friday, you have the weekend to manage any symptoms at home rather than dealing with them at work. This is not a medical recommendation, just a practical tip from people who have been through it. Finding the best time to take your GLP-1 shot can make a meaningful difference in how disruptive the side effects feel.
Exercise adjustment. Light movement, particularly walking, can help normalize intestinal motility. But intense exercise during a flare-up can make diarrhea worse. Stick to gentle activity like walking or light yoga until symptoms stabilize, then gradually return to your normal routine.
Foods that help and foods that make it worse
Diet is the single most controllable factor in managing tirzepatide diarrhea. Getting this right can cut your symptom duration in half. Getting it wrong can extend your misery for weeks.
Foods that help firm things up
Bananas are your best friend during a flare. They contain pectin, which absorbs intestinal fluid and adds bulk to stools. They also provide potassium, which you are losing with every episode. Eat them slightly underripe for maximum pectin content.
White rice is easy to digest and binding. Brown rice, despite being healthier in normal circumstances, contains too much insoluble fiber for an irritated gut. Stick with white during active symptoms.
Plain cooked chicken or turkey provides lean protein without the fat that triggers bile acid secretion. Bake or poach it. Do not fry.
Oatmeal, specifically plain rolled oats cooked with water, provides soluble fiber that absorbs excess fluid. Avoid instant oatmeal with added sugars. Top with sliced banana for a double dose of gut-calming food.
Bone broth is genuinely helpful. It provides electrolytes, easy-to-absorb amino acids like glycine and glutamine that support gut lining repair, and fluid. Some tirzepatide users take glycine supplements specifically for gut support, and bone broth is a natural way to get it.
Potatoes, specifically boiled or baked without skin, are bland, binding, and provide potassium. Sweet potatoes are also excellent once you are past the acute phase, as they contain soluble fiber.
Foods to avoid during flare-ups
Fatty and fried foods are the number one trigger. Fat stimulates bile acid release and accelerates colonic transit. If you are eating fast food while on tirzepatide, your diarrhea will be dramatically worse. This is not the time for burgers, pizza, or anything deep-fried.
Dairy can be problematic even if you are not normally lactose intolerant. GI disruption can temporarily reduce lactase production in the small intestine. If dairy seems to trigger symptoms, eliminate it for 2 weeks and then reintroduce gradually. The exception is yogurt with live cultures, which may actually help due to the probiotic content.
Caffeine stimulates intestinal motility. Coffee, energy drinks, and strong tea can all worsen diarrhea. If you cannot give up coffee entirely, switch to a single small cup in the morning and see if that is tolerable. Avoid it entirely during the acute phase.
Alcohol is a gut irritant and a diuretic. Both properties make diarrhea worse. You are already losing fluids. Alcohol accelerates that loss while simultaneously irritating an already inflamed digestive tract. Avoid it completely during flare-ups. If you are wondering about the general interaction, check our guide on drinking alcohol on tirzepatide.
Sugar alcohols (sorbitol, mannitol, xylitol) found in sugar-free products have a well-documented laxative effect. Read labels carefully. Many protein bars, diet drinks, and sugar-free candies contain these and can dramatically worsen GI symptoms.
Spicy foods irritate the gut lining and can stimulate peristalsis. Save the hot sauce for after your body has fully adjusted. Raw vegetables, while healthy in normal circumstances, contain high amounts of insoluble fiber that can worsen diarrhea. Cook your vegetables thoroughly during the adjustment period.
The ideal tirzepatide diarrhea diet (sample day)
Breakfast: Plain oatmeal with half a banana and a small drizzle of honey. Ginger tea.
Mid-morning snack: Plain crackers with a thin layer of peanut butter. Electrolyte water.
Lunch: Baked chicken breast with white rice and steamed carrots. Bone broth on the side.
Afternoon snack: Applesauce or a small plain yogurt with live cultures.
Dinner: Poached white fish with mashed potatoes (no skin) and cooked zucchini. Chamomile tea.
Evening: Small banana if hungry. Peppermint tea.
This provides adequate nutrition while minimizing triggers. As symptoms improve, gradually reintroduce more variety. The full tirzepatide eating guide covers long-term nutrition strategies in detail, and our tirzepatide diet plan provides a complete weekly framework.
Tirzepatide diarrhea versus other GI side effects
Diarrhea does not exist in isolation on tirzepatide. Understanding how it fits into the broader picture of GI side effects helps you manage the whole experience more effectively.
The GI side effect spectrum
Nausea is the most common GI side effect overall, affecting roughly 25% to 30% of users across all doses. Constipation affects about 6% to 7%. And diarrhea sits in between at 12% to 23% depending on dose. Some people experience nausea and diarrhea simultaneously, which is particularly unpleasant. Others cycle between constipation and diarrhea as the gut tries to find a new normal.
The interesting thing is that nausea and diarrhea tend to follow opposite patterns. Nausea is usually worst in the first few days after injection and fades by mid-week. Diarrhea can peak a bit later, around days 2 to 4, and may persist slightly longer. This means your worst day overall might be day 2 or 3 after injection, when both symptoms overlap.
Headaches are another common companion during the adjustment period, often linked to dehydration from fluid loss. If you are managing diarrhea properly with adequate hydration, headaches should improve as well. The muscle pain some people report can also be connected to electrolyte imbalances caused by persistent diarrhea.
Diarrhea versus constipation on tirzepatide
Here is something that confuses many people. Tirzepatide slows gastric emptying, which you would think would cause constipation, not diarrhea. And indeed, some people do experience constipation rather than diarrhea. The difference comes down to individual gut physiology, diet, hydration status, and the balance between gastric slowing and intestinal fluid secretion.
Some people even experience both, alternating between the two. If this is happening to you, focus on consistent hydration and a moderate fiber intake. Too little fiber contributes to constipation. Too much worsens diarrhea. Finding the middle ground, around 20 to 25 grams of mostly soluble fiber per day, helps stabilize things in both directions.
Can tirzepatide diarrhea affect nutrient absorption?
This is a legitimate concern that does not get enough attention. Persistent diarrhea can reduce the absorption of vitamins and minerals, particularly B vitamins, magnesium, potassium, and fat-soluble vitamins (A, D, E, K). If you are experiencing diarrhea for more than a few days per month, consider supplementing key nutrients.
Compounded formulations that include B12 or glycine may partially address the B vitamin concern, but they do not replace the need for a well-rounded diet once symptoms stabilize. Users on tirzepatide with B12 formulations sometimes report slightly better GI tolerance, though the evidence for this is anecdotal rather than clinical.
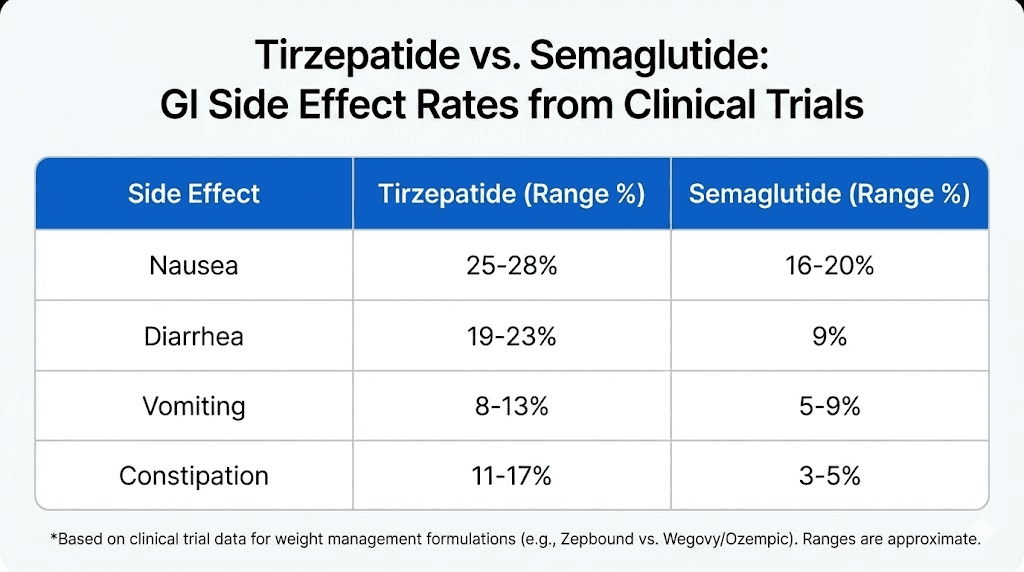
How tirzepatide diarrhea compares to semaglutide
If you are choosing between tirzepatide and semaglutide, or considering switching between them, the diarrhea comparison matters.
Head-to-head data
In the SURPASS-2 trial, which directly compared tirzepatide to semaglutide 1 mg, diarrhea rates were 13% to 16% with tirzepatide (depending on dose) versus 12% with semaglutide. The difference was modest. A Bayesian network meta-analysis found slightly higher diarrhea risk ratios for tirzepatide (1.81 to 2.18 versus placebo) compared to semaglutide (1.66 to 1.80 versus placebo), but both were in the same general range.
Some head-to-head comparisons in real-world settings show nearly identical rates, with 23% for semaglutide and 24% for tirzepatide. The bottom line: if you are switching from semaglutide to tirzepatide hoping for less diarrhea, you might be disappointed. The rates are comparable.
Where the GI profiles differ
The real differences show up in other GI symptoms. Vomiting is more common with semaglutide (21% versus 15% with tirzepatide). Constipation is slightly more common with semaglutide as well (29% versus 27%). So while diarrhea rates are similar, the overall GI experience can feel different between the two medications.
Fatigue on semaglutide may also be more pronounced than on tirzepatide, though both medications can cause it. The GLP-1 fatigue connection is complex and involves appetite reduction, caloric deficit, and direct central nervous system effects.
Tirzepatide does tend to produce more weight loss at equivalent treatment durations, which is the main reason many people choose it despite similar side effect profiles. The tradeoff between efficacy and side effects is something to discuss with your healthcare provider. For a detailed comparison of dosing, see our semaglutide to tirzepatide conversion chart.
Dose escalation strategies to minimize diarrhea
The dose escalation schedule is the single biggest factor in how severe your diarrhea gets. Going too fast is the most common mistake, and it is entirely preventable.
The standard escalation timeline
The approved tirzepatide escalation schedule starts at 2.5 mg for 4 weeks, then increases to 5 mg. From there, increases happen in 2.5 mg increments every 4 weeks as tolerated, up to a maximum of 15 mg. This gradual approach exists specifically to minimize GI side effects, including diarrhea.
The key phrase is "as tolerated." If you are experiencing persistent diarrhea at your current dose, there is no rule saying you must escalate on schedule. Many prescribers recommend staying at a dose for 6 to 8 weeks instead of 4 if GI symptoms are not resolved. The tirzepatide dosing chart provides the standard framework, but individual adjustment is expected and normal.
Microdosing as a diarrhea reduction strategy
Some users and prescribers have adopted a microdosing approach to dose escalation. Instead of jumping from 5 mg directly to 7.5 mg, they make smaller incremental increases. This is more common with compounded tirzepatide, where flexible dosing is possible.
The theory is sound. Smaller increases mean smaller disruptions to GI function, which means less diarrhea at each step. The tradeoff is slower progress toward your target dose. But if the alternative is dropping out of treatment entirely because the side effects are unbearable, a slower escalation is clearly preferable.
Reconstitution and administration factors
For those using compounded tirzepatide, proper reconstitution matters. Incorrect reconstitution can lead to inconsistent dosing, which means your body gets hit with variable amounts of medication rather than a steady, predictable dose. This inconsistency can worsen GI symptoms because the gut never fully adapts to a stable level.
Injection technique also plays a role. Proper subcutaneous injection ensures consistent absorption. If you are injecting too shallowly or into a area with poor blood flow, the medication may absorb unevenly, creating peaks and valleys that trigger GI symptoms. Rotating injection sites and following proper technique reduces this variability.
Storage matters too. If your tirzepatide has been improperly stored or exposed to temperature fluctuations, the peptide may degrade unevenly. Partially degraded medication can produce unpredictable effects, including worse GI symptoms. Always check proper storage guidelines and refrigeration requirements.
When tirzepatide diarrhea signals something more serious
Most tirzepatide diarrhea is benign and self-limiting. But not always. Knowing the red flags can prevent a minor side effect from becoming a medical emergency.
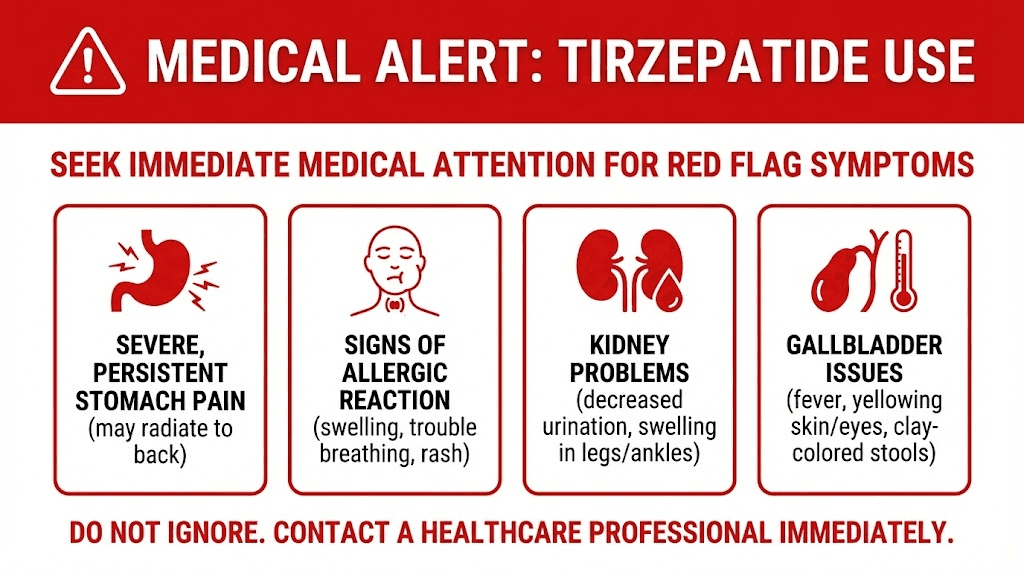
Red flags that require immediate medical attention
Blood in your stool. This is never normal on tirzepatide and should be evaluated immediately. Fresh red blood or dark, tarry stools both warrant urgent medical attention.
Fever above 101 degrees Fahrenheit (38.3 Celsius) alongside diarrhea suggests an infection rather than a medication side effect. Tirzepatide does not cause fever. If you have both, something else is going on.
Signs of severe dehydration: very dark urine, dizziness when standing, rapid heartbeat, dry mouth that does not improve with drinking, confusion, or inability to keep fluids down. Severe dehydration from persistent diarrhea has been linked to acute kidney injury in rare cases. This is the most dangerous complication and the reason hydration management is so critical.
Diarrhea lasting more than 48 hours without any improvement, especially if it is severe (more than 6 watery stools per day). While mild diarrhea can persist for days, severe diarrhea that is not responding to basic management needs medical evaluation.
Severe abdominal pain, particularly if it is localized to one area rather than general cramping. Tirzepatide can, in rare cases, contribute to pancreatitis, which presents with severe upper abdominal pain radiating to the back.
When to call your prescriber (not emergency, but important)
Diarrhea that persists beyond 4 weeks at a stable dose. By this point, your body should have adapted. Persistent symptoms may indicate the dose is too high or that another cause should be investigated.
Diarrhea that returns or worsens after an initial improvement. This pattern is unusual for simple medication adjustment and could suggest a food intolerance, infection, or other contributing factor.
Unintentional weight loss beyond what is expected. Tirzepatide causes weight loss, yes. But if you are losing more than 1 to 2 pounds per week consistently, and diarrhea is a major symptom, you may be losing fluid weight and muscle rather than fat. Your prescriber can help distinguish between healthy weight loss and problematic fluid depletion.
Any new symptoms appearing alongside worsening diarrhea. Joint pain, skin changes, or hair thinning combined with persistent diarrhea could indicate nutritional deficiencies that need addressing.
Special situations and tirzepatide diarrhea
Not everyone fits the standard profile. Certain circumstances change the diarrhea equation significantly.
Diarrhea on compounded versus brand-name tirzepatide
Users of compounded tirzepatide sometimes report different GI profiles than those on brand-name Mounjaro or Zepbound. This can be due to differences in excipients, concentration, or peptide purity. Some compounded formulations from specific pharmacies like Empower or others include additives like niacinamide or glycine that may affect GI tolerance.
If you switched from brand-name to compounded (or vice versa) and noticed a change in diarrhea severity, the formulation difference is a likely explanation. Discuss with your prescriber whether adjusting the compounding pharmacy or formulation might help.
Diarrhea after switching from semaglutide
People who switch from semaglutide to tirzepatide sometimes expect no adjustment period because they were already on a GLP-1 medication. This is incorrect. Tirzepatide adds GIP receptor agonism on top of GLP-1, and the gut needs to adapt to this additional stimulation. Expect some degree of GI readjustment, including possible diarrhea, even if you tolerated semaglutide perfectly.
The conversion between medications is not straightforward. Our dose conversion chart provides guidance, but your prescriber should determine the appropriate starting dose based on your history.
Diarrhea and exercise on tirzepatide
High-intensity exercise during a diarrhea flare can make things worse for two reasons. First, vigorous exercise diverts blood away from the digestive tract, which disrupts normal absorption. Second, the physical jostling of running or jumping can stimulate peristalsis. Stick to walking, gentle cycling, or swimming during active symptoms. The combination of exercise-induced dehydration and diarrhea-induced fluid loss can be dangerous if not managed carefully.
Diarrhea and other medications
Several common medications can worsen diarrhea when combined with tirzepatide. Metformin, which is frequently co-prescribed, is notorious for causing GI side effects including diarrhea. If you are taking both, the combined effect can be significant. Phentermine combined with tirzepatide can also alter GI function. Antibiotics, magnesium supplements, and certain blood pressure medications are other common culprits. Review all your medications with your prescriber if diarrhea is persistent.
The psychological side of dealing with tirzepatide diarrhea
This part rarely gets discussed, but it matters. Persistent GI symptoms can significantly impact quality of life and medication adherence.
Anxiety and anticipation
Many people develop anticipatory anxiety around their injection day. They know diarrhea might follow, so they start worrying about it days in advance. This stress response can actually worsen GI symptoms through the gut-brain axis. Cortisol and other stress hormones directly influence intestinal motility and fluid secretion.
The solution is not to pretend the concern does not exist. It is to prepare. Have your management supplies ready (electrolytes, bland foods, medication if approved). Schedule your injection when you have access to a bathroom for the next 48 hours. Control what you can control, and the anxiety decreases naturally.
Anxiety on tirzepatide is a recognized phenomenon, and GI distress can contribute to it. If anticipatory anxiety is significantly affecting your quality of life, discuss it with your healthcare provider.
Social impact and planning
Diarrhea is not just physically uncomfortable. It is socially limiting. People skip events, avoid travel, and restructure their schedules around potential bathroom needs. This isolation can contribute to frustration and even depression.
Practical strategies help. Some users plan their injections around their social calendar. Others keep an emergency kit in their car or bag with anti-diarrheal medication, wet wipes, and a change of clothes. These seem like small things, but they provide the confidence to maintain a normal life during the adjustment period.
Deciding whether to continue treatment
If diarrhea is severe enough to consider stopping tirzepatide, have a thorough conversation with your prescriber before making that decision. Options include slowing the escalation, reducing the dose, trying a different formulation, or adding supportive medications. Troubleshooting the approach is almost always better than abandoning it entirely, given the significant benefits tirzepatide provides for weight management and metabolic health.
In the clinical trials, treatment discontinuation due to diarrhea was uncommon. Most participants who experienced it chose to continue because the benefits outweighed the temporary discomfort. But if your quality of life is genuinely suffering, dose adjustment is a reasonable and evidence-supported response.
Long-term outlook: does tirzepatide diarrhea go away permanently?
Yes, for the vast majority of people. This is the most important takeaway from the clinical data.
The adaptation curve
Research from the SURPASS and SURMOUNT trials consistently shows that GI adverse events decrease over time. The first 4 to 8 weeks are the hardest. By month 3, most people have adapted significantly. By month 6, GI side effects are typically minimal or absent at a stable dose.
The key word is "stable dose." Every dose increase restarts the adaptation process to some degree. But each subsequent adaptation tends to be easier and shorter than the previous one. Your gut is learning to function with GLP-1 and GIP receptor stimulation as a baseline rather than a disruption.
What if it does not go away?
For a small minority, roughly 1% to 3% based on trial data, GI symptoms persist despite dose stabilization and management strategies. In these cases, the prescriber may recommend:
Switching to a pure GLP-1 agonist like semaglutide, removing the GIP component. Some people tolerate one receptor agonist better than the dual approach.
Lowering the maintenance dose. You do not need to be on the maximum dose. Many people achieve excellent results at 5 mg or 10 mg with dramatically fewer side effects than at 15 mg.
Adding an adjunctive medication specifically for GI management, such as a low-dose cholestyramine for bile acid diarrhea or a motility agent.
Investigating other causes. Persistent diarrhea that does not improve might be coincidental, not caused by tirzepatide. Celiac disease, inflammatory bowel disease, and other conditions should be ruled out if symptoms are unexpectedly persistent.
The bottom line on duration
For most people: 3 to 7 days per dose change. For the adjustment period overall: 4 to 8 weeks of intermittent symptoms. For the long term: resolution in nearly all cases once the dose stabilizes. The body adapts. You just need to support it through the transition.
Practical tips from experienced tirzepatide users
Clinical trials provide the data. But people who have actually been through it offer the practical wisdom that makes the difference between suffering through and managing well.
The weekend injection strategy
Inject on Friday afternoon or evening. If diarrhea hits, your worst days (Saturday and Sunday) are at home where you have full access to your bathroom, your bland food supplies, and the ability to rest. By Monday, the acute phase is usually over. This strategy alone has made the difference for thousands of users in terms of quality of life and ability to maintain their normal work schedule.
The electrolyte pre-loading approach
Some experienced users start increasing their electrolyte intake 24 hours before their injection, not after symptoms appear. The logic is straightforward: if you enter the potential diarrhea window already well-hydrated with balanced electrolytes, any fluid loss is less impactful and symptoms may be milder.
The ginger protocol
Ginger has evidence-based anti-nausea and GI-calming properties. Many tirzepatide users keep ginger tea, ginger chews, or ginger capsules on hand. Taken 30 minutes before meals and at the first sign of GI distress, ginger can reduce both nausea and diarrhea severity. It is not a cure, but it is a safe, natural addition to your management toolkit.
The bathroom mapping strategy
This sounds oddly specific, but it is genuinely useful advice from experienced users. During the first few weeks, know where every accessible bathroom is along your commute, at your workplace, and during any regular activities. This knowledge removes the panic element from urgent situations and reduces the stress that makes symptoms worse.
The temperature trick
Room temperature or warm foods and beverages are easier on a disrupted gut than cold or hot items. Ice-cold water can trigger cramping. Very hot food can stimulate peristalsis. Aim for moderate temperatures during flare-ups, and you may notice a subtle but real improvement.
Tirzepatide diarrhea in clinical context: what the numbers really mean
Let us put the diarrhea risk in proper perspective with comprehensive trial data.
Incidence rates across all major trials
Trial | Population | Tirzepatide diarrhea rate | Comparator rate |
|---|---|---|---|
SURPASS-1 | Type 2 diabetes | 12-17% | 9% (placebo) |
SURPASS-2 | Type 2 diabetes | 13-16% | 12% (semaglutide) |
SURMOUNT-1 | Obesity/overweight | 19-23% | 8% (placebo) |
Meta-analysis (6 RCTs) | Mixed | 16.24% overall | 8.63% overall |
The risk ratio from the meta-analysis was 2.07, meaning tirzepatide roughly doubles the chance of diarrhea compared to placebo. That sounds dramatic until you realize that roughly 84% of tirzepatide users never experience clinically significant diarrhea at all.
Severity breakdown
Among those who do experience diarrhea, the overwhelming majority, over 85%, report mild to moderate severity. Severe diarrhea requiring treatment modification occurred in approximately 1% to 2% of trial participants. And treatment discontinuation specifically due to diarrhea was less than 1% across all trials.
This means that even among the roughly 16% who get diarrhea, serious cases are uncommon. Most people manage it with basic dietary adjustments and hydration, without any need for dose changes or medication.
Comparison with other GLP-1 medications
Medication | Diarrhea rate | Nausea rate | Constipation rate | Vomiting rate |
|---|---|---|---|---|
Tirzepatide 5 mg | 14.6% | 15-20% | 6% | 5% |
Tirzepatide 10 mg | 16.8% | 20-25% | 6% | 8% |
Tirzepatide 15 mg | 17.3% | 25-30% | 7% | 10% |
Semaglutide 2.4 mg | ~20-23% | ~44% | ~29% | ~21% |
Placebo | ~8% | ~7% | ~4% | ~3% |
Notice something interesting. While tirzepatide has slightly lower diarrhea rates than semaglutide at the highest comparison doses, semaglutide has significantly higher nausea and vomiting rates. If you are primarily concerned about diarrhea specifically, the two medications are quite similar. If you are concerned about overall GI comfort, tirzepatide may actually have a slight advantage despite the dual receptor mechanism.
Building a complete tirzepatide diarrhea management plan
Let us pull everything together into a structured, actionable plan you can follow from day one.
Before starting tirzepatide
Stock up on supplies. Electrolyte packets or sports drinks. Bland food staples (rice, bananas, crackers, chicken broth). Ginger tea or ginger supplements. A quality probiotic containing Lactobacillus rhamnosus GG or Saccharomyces boulardii. Anti-diarrheal medication (loperamide) with prescriber approval.
Clean up your diet 1 to 2 weeks before starting. Reduce alcohol, caffeine, high-fat foods, and processed foods. This gives your gut a better baseline before the medication adds its own stress. The complete foods to avoid list is worth reviewing in advance.
Schedule your first injection for a Thursday or Friday. This gives you the weekend to manage any initial symptoms at home.
Week 1: Expect some disruption
Eat small, frequent, bland meals. Hydrate aggressively with electrolyte-containing fluids. Start probiotics if you have not already. Avoid trigger foods completely. Track symptoms in a journal noting timing, severity, and what you ate.
Weeks 2 to 4: Gradual improvement
Symptoms should be decreasing. Start reintroducing foods one at a time to identify personal triggers. Maintain adequate hydration. Continue probiotics. If symptoms have not improved at all by week 3, contact your prescriber.
Dose escalation days
Treat each dose increase like a mini restart. Pull back to bland foods for 48 to 72 hours. Increase fluid intake the day before and day of your increased dose. Have anti-diarrheal medication available. Resume normal eating once symptoms stabilize, usually within 3 to 5 days.
Ongoing maintenance
Once stable, most people can return to a normal diet with a few permanent modifications: slightly smaller meals, consistent hydration, reduced intake of known trigger foods, and continued probiotic use. Many people find their relationship with food permanently improves on tirzepatide, not just because of appetite reduction, but because the adjustment period teaches them which foods their body handles best.
SeekPeptides provides comprehensive protocol guides for members navigating the tirzepatide journey, including detailed management strategies for GI side effects, personalized dosing guidance, and access to a community of experienced users who have been through exactly what you are experiencing now.
Frequently asked questions
How long does tirzepatide diarrhea last after the first injection?
Most people experience diarrhea for 1 to 3 days after their first injection. The initial 2.5 mg dose is low specifically to minimize GI side effects, so first-injection diarrhea is typically mild. If it lasts beyond 5 days, contact your prescriber to discuss management strategies before your next dose.
Does tirzepatide diarrhea get worse with higher doses?
Statistically yes. Diarrhea rates increase from 14.6% at 5 mg to 17.3% at 15 mg in clinical trials. However, many individuals find that their body has partially adapted by the time they reach higher doses, so their personal experience may not worsen. The dose escalation schedule exists specifically to allow gradual adaptation. Using a dosage calculator can help ensure accurate dosing throughout the escalation.
Can I take Imodium for tirzepatide diarrhea?
Loperamide (Imodium) can be used for acute episodes with prescriber approval. It slows intestinal motility, which directly addresses one mechanism of tirzepatide diarrhea. However, it should not be used as a long-term daily solution, as it can mask symptoms that might indicate a need for dose adjustment. Always discuss with your healthcare provider first.
Is diarrhea a sign that tirzepatide is working?
Not exactly. Diarrhea indicates that the medication is affecting your GI system, which confirms it is active in your body. But you can have full therapeutic benefit without any diarrhea at all. Many people lose significant weight on tirzepatide with zero GI side effects. The presence or absence of diarrhea does not predict how much weight you will lose.
Should I stop tirzepatide if I have severe diarrhea?
Do not stop any medication without consulting your prescriber. Severe diarrhea usually warrants a dose reduction rather than complete cessation. Your prescriber may recommend returning to the previous dose, extending the time at your current dose, or adding supportive medications. Stopping abruptly can cause its own issues, and the troubleshooting guide covers strategies for managing difficult side effects while maintaining treatment.
Does the oral form of tirzepatide cause less diarrhea than injections?
Early data on oral tirzepatide versus injectable formulations suggests similar GI side effect profiles, though oral tablets may produce more localized upper GI symptoms initially. The sublingual drops format may have slightly different absorption characteristics that affect GI tolerance, but comprehensive comparative data is still limited.
Can tirzepatide diarrhea cause dehydration?
Yes, particularly if it is frequent or severe. Dehydration is the most clinically significant risk of persistent diarrhea on tirzepatide. Signs include dark urine, dizziness, rapid heartbeat, dry mouth, and reduced urination. Aggressive fluid and electrolyte replacement is essential. In rare cases, severe dehydration has been linked to acute kidney injury, which is why monitoring hydration status is critical during the adjustment period.
Will probiotics prevent tirzepatide diarrhea?
Probiotics will not prevent it entirely, but they can reduce duration and severity. Strains with the strongest evidence for medication-related diarrhea include Lactobacillus rhamnosus GG and Saccharomyces boulardii. Starting probiotics before or at the same time as tirzepatide may provide the best results, as they help maintain gut microbiome stability during the transition.
External resources
FDA Drug Safety and Availability (U.S. Food and Drug Administration)
Gastrointestinal adverse events in the SURPASS clinical trials (Diabetes, Obesity and Metabolism)
Tirzepatide versus semaglutide once weekly (New England Journal of Medicine)
For those serious about optimizing their tirzepatide protocol and managing every aspect of their peptide journey, SeekPeptides offers the most comprehensive resource available. Members access evidence-based guides, detailed side effect management protocols, and a community of thousands who have navigated these exact challenges successfully.
In case I do not see you, good afternoon, good evening, and good night. May your gut stay settled, your hydration stay strong, and your results stay worth every temporary discomfort.