Feb 26, 2026

Before you skip your next dose, stop. The decision to wean off tirzepatide is not as simple as putting the vial back in the fridge and moving on with life. It requires planning. It requires strategy. And most importantly, it requires understanding what your body is about to go through, because the research on what happens after stopping tirzepatide is sobering.
The SURMOUNT-4 trial showed that 82.5% of participants who stopped tirzepatide regained at least 25% of their lost weight within one year. Some regained half. Others regained nearly all of it. That is not a scare tactic. That is clinical data from one of the largest and most rigorous tirzepatide weight loss studies ever conducted.
But here is what those headlines do not tell you. Not everyone regains the weight. The people who kept it off did specific things before, during, and after their taper that protected their results. They built habits while the medication was still working. They tapered gradually rather than stopping cold. They monitored the right markers and adjusted when things started slipping. This guide covers every step of that process, from the pharmacology of why tapering matters to the exact dose reduction schedule, the lifestyle changes that actually work, and the warning signs that mean you should slow down or reconsider. Whether you have reached your goal weight on tirzepatide, you are dealing with side effects you cannot tolerate, or cost is forcing the decision, what you do in the next 8 to 12 weeks will determine whether your results stick or disappear. SeekPeptides has assembled every piece of evidence, every protocol detail, and every practical strategy you need to make this transition safely.
Why people decide to stop tirzepatide
The reasons fall into a few distinct categories, and understanding yours matters because it shapes how you should approach the taper.
You reached your goal weight
This is the most common reason. You started tirzepatide to lose weight. It worked. Now you are wondering whether you need to keep injecting every week, whether the dosing schedule is still necessary when the scale shows the number you wanted. The answer is more nuanced than a simple yes or no. Reaching a goal weight does not mean the metabolic adaptations that caused weight gain in the first place have resolved. Your body still remembers its previous set point, and it will fight to return there once the medication is removed.
That said, many people do successfully transition off. The key is understanding that "reaching your goal" is the starting line of maintenance, not the finish line of treatment.
Side effects became intolerable
Some people experience persistent headaches, severe constipation, ongoing diarrhea, or crushing fatigue that does not improve with time. Others develop anxiety, insomnia, or body aches that interfere with daily life. Joint pain and hair thinning push others toward discontinuation. Menstrual changes concern some women. Injection site reactions make weekly dosing unpleasant for a smaller subset. When side effects outweigh benefits, stopping makes sense. But even in these cases, a gradual taper is usually preferable to an abrupt stop.
Cost is a barrier
Tirzepatide is not cheap. Even more affordable compounded versions represent a significant monthly expense for many households. Insurance coverage remains inconsistent, and supply chain disruptions can make access unpredictable. Even pharmacy-specific options like Empower Pharmacy tirzepatide face periodic availability challenges. If cost is your primary driver, consider whether lower cost compounded options or dose reduction strategies might let you continue at a lower expense before committing to full discontinuation.
You want to try a different approach
Some people want to switch from tirzepatide to semaglutide or explore other peptides for weight management. Others want to try managing their weight through lifestyle alone, perhaps after reading about weight management without medication. Some are interested in next-generation options like survodutide, CagriSema, or mazdutide. Both paths benefit from a structured taper rather than an abrupt change.
Medical reasons
Pregnancy planning is a significant one. Tirzepatide and breastfeeding do not mix, and anyone who becomes pregnant on tirzepatide needs to discontinue immediately under medical supervision. Upcoming surgery (guidelines for resuming GLP-1 medications after surgery apply here), new medications with interactions, or changes in health status can also necessitate stopping. Understanding the timeline of tirzepatide effects helps plan around medical events.
Does tirzepatide actually require tapering?
Technically, no. And that single word, "technically," deserves a closer look.
Tirzepatide does not create physical dependence the way opioids or benzodiazepines do. There is no withdrawal syndrome. Your body will not go into shock if you stop taking it tomorrow. The FDA prescribing information does not mandate gradual dose reduction. From a purely pharmacological standpoint, you can stop at any dose, at any time, without dangerous physical consequences.
But pharmacology is not the whole picture.
What tirzepatide does create is a metabolic environment your body adapts to. It suppresses appetite through GLP-1 and GIP receptor activation. It slows gastric emptying. It changes how your brain responds to food cues. It alters insulin sensitivity and glucose metabolism. When you remove the drug abruptly, all of those changes reverse. Not gradually. Not gently. They come back in a rush that most people are completely unprepared for.
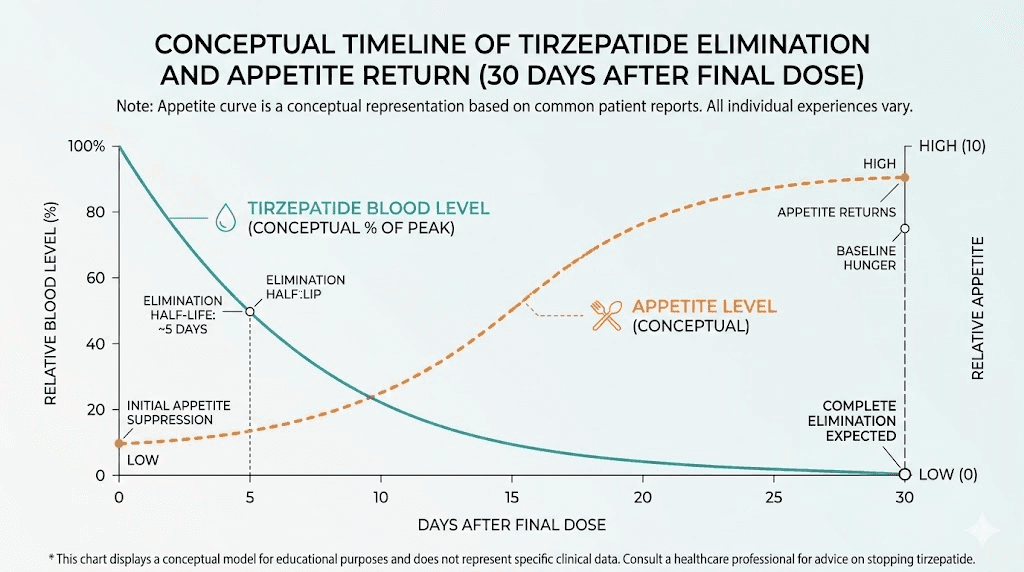
The appetite suppression that made eating less feel effortless? Gone within 25 to 30 days, which is roughly how long it takes for tirzepatide to fully clear your system given its approximately 5-day half-life. The appetite suppression timeline reverses almost as quickly as it started. Suddenly you are hungry again. Not a little hungry. The kind of hungry that makes a whole pizza seem reasonable at 10 PM on a Tuesday.
This is why tapering matters even though it is not strictly required. A gradual dose reduction, following a structured dose chart, gives your body, your brain, and your habits time to adjust to each new level of appetite and metabolic activity. It creates a bridge between medicated weight management and unmedicated weight management. Without that bridge, most people fall.
The half-life factor
Tirzepatide has a half-life of approximately 5 days. That means if you are on 15 mg, five days after your last injection you still have roughly 7.5 mg worth of active drug in your system. After 10 days, about 3.75 mg. After 25 to 30 days, the drug is essentially gone. Understanding the tirzepatide dosage mechanics helps you appreciate why the transition period is not immediate but also not infinitely long. The effects fade on a predictable curve, and your taper should account for that curve. Anyone familiar with how long tirzepatide takes to reach full effect can understand the reverse process in similar terms.
What the SURMOUNT-4 trial revealed about stopping
The SURMOUNT-4 trial is the most important study anyone considering discontinuation should understand. Published in JAMA in December 2023, it examined exactly what happens when people stop tirzepatide after achieving significant weight loss.
The study design
Researchers enrolled adults with obesity (BMI of 30 or higher, or 27 or higher with weight-related conditions) and treated everyone with tirzepatide for 36 weeks. Those who achieved at least 5% weight loss were then randomized into two groups. One group continued tirzepatide. The other switched to placebo, effectively stopping the medication. Both groups were followed for an additional 52 weeks.
The results
The numbers tell a clear story. People who continued tirzepatide lost an additional 5.5% of body weight over the following year. People who stopped regained an average of 14% of the weight they had previously lost. That is not 14% of their total body weight. That is 14% of the weight they had specifically lost through tirzepatide treatment.
But averages obscure the distribution. A post hoc analysis published in JAMA Internal Medicine broke down the weight regain into categories. Of the participants who stopped tirzepatide, 54 regained less than 25% of their lost weight. Another 77 regained 25% to 50%. A total of 103 regained 50% to 75%. And 74 regained 75% or more. By week 88, a full 82.5% of people who stopped had regained at least a quarter of what they lost.
The cardiometabolic reversal
Weight regain was not the only consequence. The improvements in blood pressure, cholesterol, insulin resistance, waist circumference, and glycemic parameters that tirzepatide produced also reversed in proportion to the amount of weight regained. Participants who regained less than 25% largely maintained their cardiometabolic improvements. Those who regained more saw those benefits erode significantly.
This finding is critical. It means that the goal of your taper should not just be minimizing weight regain but specifically keeping regain below that 25% threshold where the health benefits start to unravel.
What the successful minority did differently
The 17.5% who regained less than 25% were not random. Research suggests they shared common characteristics. They had established exercise routines before stopping. They had made genuine dietary changes rather than relying entirely on appetite suppression. They had support systems and monitoring in place. The tirzepatide before and after results that stick, whether documented in men or women, are almost always accompanied by lifestyle changes that began during treatment, not after.
The complete tirzepatide tapering schedule
There is no single FDA-approved tapering protocol because the FDA does not require one. What follows is a clinician-informed approach based on the available dose strengths, the pharmacology of the drug, and practical experience from providers who have guided hundreds of patients through this process.
The general principle
Reduce by one dose level (typically 2.5 mg, which you can verify using the unit-to-mg reference) every 4 to 8 weeks. Stay at each new dose until your appetite, energy, weight, and overall stability feel manageable. Do not rush. The tapering process should take 8 to 16 weeks depending on your starting dose, your tolerance for change, and how aggressively your appetite returns at each reduction.
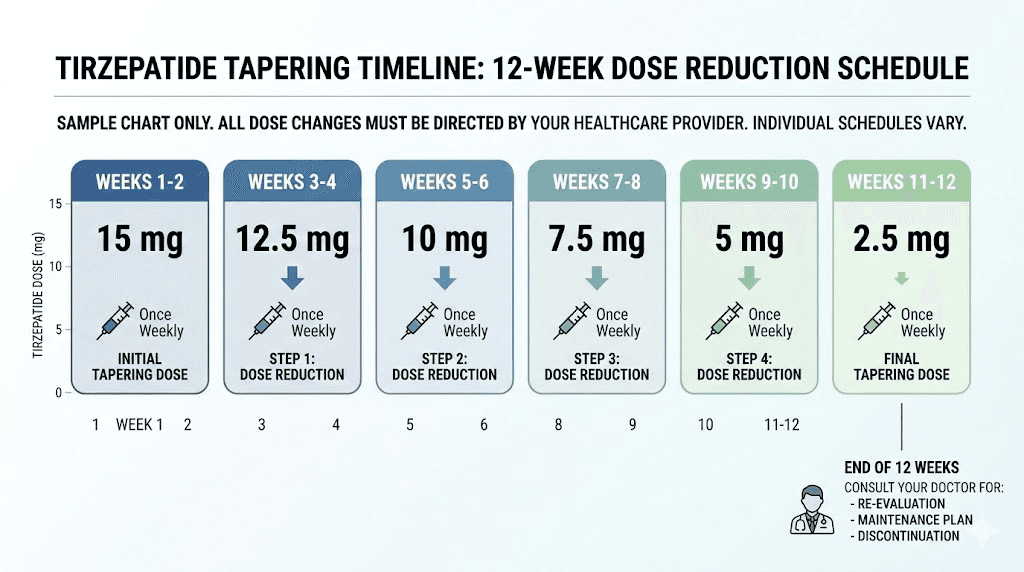
Tapering from 15 mg
If you are currently on the maximum 15 mg dose, here is a suggested schedule.
Weeks 1 through 4: Reduce to 12.5 mg weekly. This is a modest 2.5 mg drop. Most people notice minimal change at this step. Your appetite may increase slightly, but the overall suppression effect remains strong. Use this period to start tightening your dietary habits, confirming your exercise routine is solid, and reviewing your injection dosage chart to ensure accuracy at the new level.
Weeks 5 through 8: Reduce to 10 mg weekly. This is where many people first notice the appetite returning. The suppression is still present but less aggressive. Track your food intake carefully and monitor your weight weekly. If you regain more than 2 to 3 pounds, consider staying at 10 mg for an additional 2 to 4 weeks before moving to the next step. Use unit-to-mg conversion guides to verify your measurements are accurate at each level.
Weeks 9 through 12: Reduce to 7.5 mg weekly. The 7.5 mg dose is where the transition begins to feel real. Appetite suppression is noticeably weaker. Cravings may return, particularly in the evening and on weekends. This is a critical phase for reinforcing the habits you have been building.
Weeks 13 through 16: Reduce to 5 mg weekly. At 5 mg, you are on what was once your escalation dose. The medication is still active, still providing some appetite modulation, but the effect is significantly diminished compared to your maintenance dose. Many people find this the hardest step because the contrast with their previous level of control is stark. Review the unit conversions for lower doses and the weight loss dosing conversion chart to stay precise.
Weeks 17 through 20: Reduce to 2.5 mg weekly. The 2.5 mg dose is the lowest available. It provides modest GLP-1 and GIP receptor activation. Think of this as the training wheels phase. You are doing most of the work yourself, but the medication provides a small buffer.
Week 21 and beyond: Discontinue. After 4 weeks at 2.5 mg, stop injecting. The drug will clear your system over the next 25 to 30 days. During this clearance period, continue all monitoring and lifestyle strategies at maximum intensity.
Understanding the 30mg vial consideration
Many compounded tirzepatide products come in 30 mg vials designed for multiple injections across different dose levels. If you are in the middle of a vial when you start tapering, plan your dose reductions to align with your remaining supply. Wasting medication is expensive. For example, a 30 mg vial at the 7.5 mg dose level provides 4 weeks of injections, which aligns perfectly with a 4-week hold at each tapering step. The reconstitution chart and bacteriostatic water mixing guide ensure you get accurate doses from each vial during this process.
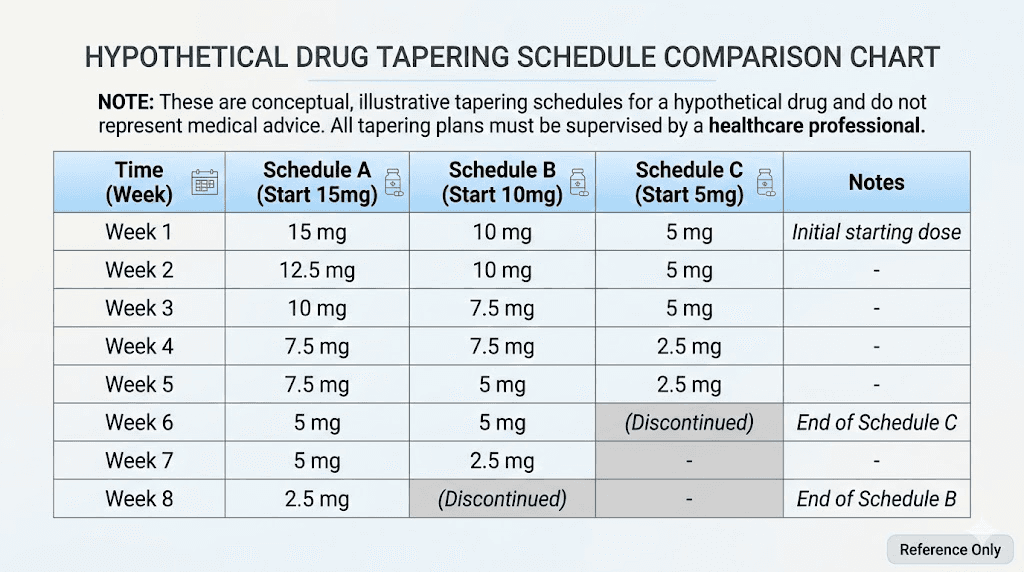
Tapering from 10 mg
If your maintenance dose is 10 mg, follow a condensed version. Reduce to 7.5 mg for 4 weeks, then to 5 mg for 4 weeks, then to 2.5 mg for 4 to 6 weeks before stopping. The total taper takes 12 to 14 weeks. The same principles apply, stay at each level until you feel stable before moving down.
Tapering from 5 mg
For those on 5 mg (review the mg-to-units conversion if using syringes), the simplest approach is to reduce to 2.5 mg for 4 to 6 weeks before discontinuing. Some providers suggest extending the 2.5 mg phase to 8 weeks if the patient has significant weight to protect. Check your dosage calculations to ensure accuracy at these lower doses, since small measurement errors have a larger proportional impact when the dose itself is small.
The compounded tirzepatide consideration
If you are using compounded formulations (whether from Empower Pharmacy or other compounding sources), tapering can actually be more flexible. Unlike brand-name tirzepatide which comes in fixed dose pens, compounded tirzepatide drawn from vials allows you to reduce in smaller increments. You could taper by 1 mg at a time rather than 2.5 mg, creating an even more gradual transition. Use a syringe dosage guide to ensure precise measurements during this process. The dosing chart in units becomes especially important when making these fine adjustments.
What to expect at each stage of your taper
Knowing what is coming helps you prepare rather than panic. Each dose reduction triggers a specific set of changes, and recognizing them as normal parts of the process, rather than signs of failure, is half the battle.
The first reduction (minimal impact)
Dropping from your maintenance dose by one level usually produces the least noticeable change. You might feel slightly hungrier between meals. Your portion sizes might creep up marginally. But the overall framework of appetite suppression remains intact. This is the easiest phase, and it is also the most important time to solidify habits because the real challenges come later.
Use this period to:
Establish a consistent meal prep routine
Lock in your exercise schedule (at least 150 minutes of moderate activity weekly)
Start tracking your weight and measurements weekly
Build a meal plan you can follow without the medication
Review foods to avoid and stock your kitchen accordingly
Understand the optimal injection timing for your current dose
The middle reductions (the challenge zone)
Dropping to roughly half your original maintenance dose is where most people struggle. The appetite suppression that once felt automatic now requires conscious effort to replicate through food choices and meal timing. Here is what typically happens.
Hunger returns in waves. Not the gentle "I could eat" hunger you experienced on medication. Real hunger. The kind that makes you think about food between meals, that makes restaurant commercials suddenly compelling, that makes the candy aisle at the grocery store feel like it is calling your name. This is normal. This is your body recalibrating. It does not mean you are failing.
Cravings intensify. This is the same phenomenon that makes alcohol more tempting on tirzepatide, but in reverse, everything becomes more tempting without it. High-calorie, high-carbohydrate foods are the primary targets. Your brain is receiving less GLP-1 signaling, which means the reward pathways associated with food become more active. Sugar and refined carbohydrates trigger a stronger dopamine response than they did when you were fully medicated. Having a strategy for managing these cravings, one that does not rely on willpower alone, is essential. Load your kitchen with the right foods and remove the ones that trigger overeating.
Gastric emptying speeds up. Tirzepatide slows how fast food moves through your stomach, which contributes to feeling full longer. As the dose decreases, food moves through faster, and that prolonged fullness diminishes. You may notice you feel hungry sooner after meals. Eating more fiber and protein at each meal can partially compensate for this change.
The final reduction and discontinuation
The transition from 2.5 mg to zero is psychologically the hardest step, even though the pharmacological difference is relatively small. There is a mental safety net that comes with knowing you still have "something" working. Removing that last dose can feel like stepping off a cliff.
In reality, 2.5 mg provides modest receptor activation. The jump from 2.5 to zero is smaller than the jump from 5 to 2.5 in terms of actual metabolic impact. But the psychological shift is significant. Prepare for it. Remind yourself that the habits you have built are the real engine of your weight management now, not the medication.
The 25 to 30 days after your final injection represent a critical window. The drug is still clearing your system, so the changes happen gradually rather than all at once. By day 10, you have roughly half the drug left. By day 20, about a quarter. By day 30, it is essentially gone. Many people report that the hardest period is days 14 through 21, when the drug levels have dropped enough for appetite to return noticeably but not enough time has passed for new habits to feel automatic.
Preparing your body before you start tapering
The single biggest mistake people make is starting their taper before they have built the infrastructure to succeed without medication. Think of it this way. Tirzepatide gave you a window of reduced appetite and improved metabolic function. That window was meant to be used for building sustainable habits, not just enjoying the weight loss. If you spent your time on medication eating less but not eating differently, tapering will be much harder.
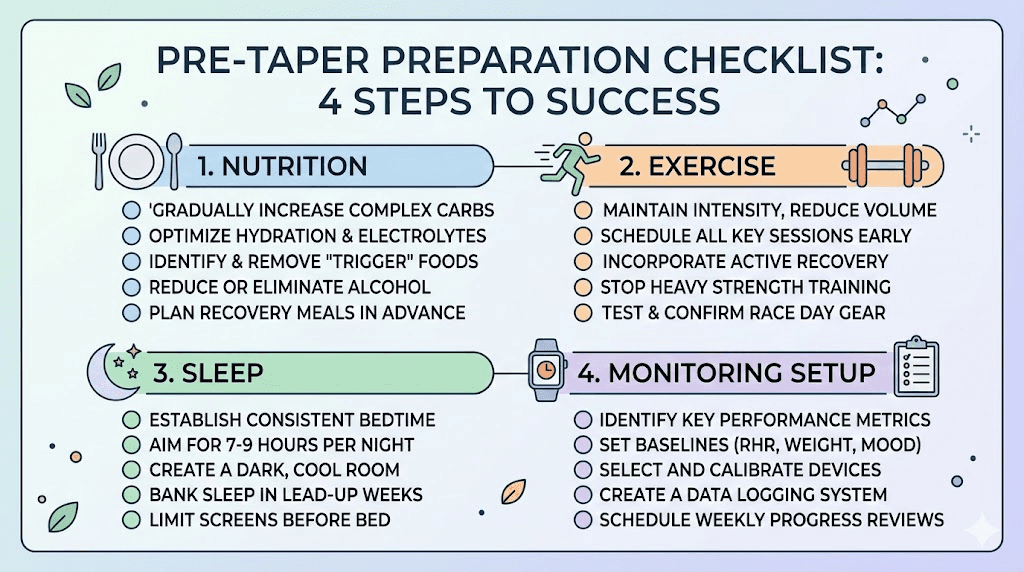
Establish your nutrition foundation
Before reducing your first dose, you should have a clear, practiced eating pattern that you can maintain independently. This means knowing exactly what you eat for breakfast, lunch, dinner, and snacks on a typical day. It means having go-to meals that are satisfying and nutritious. It means understanding how to eat at restaurants and social events without the medication doing the heavy lifting.
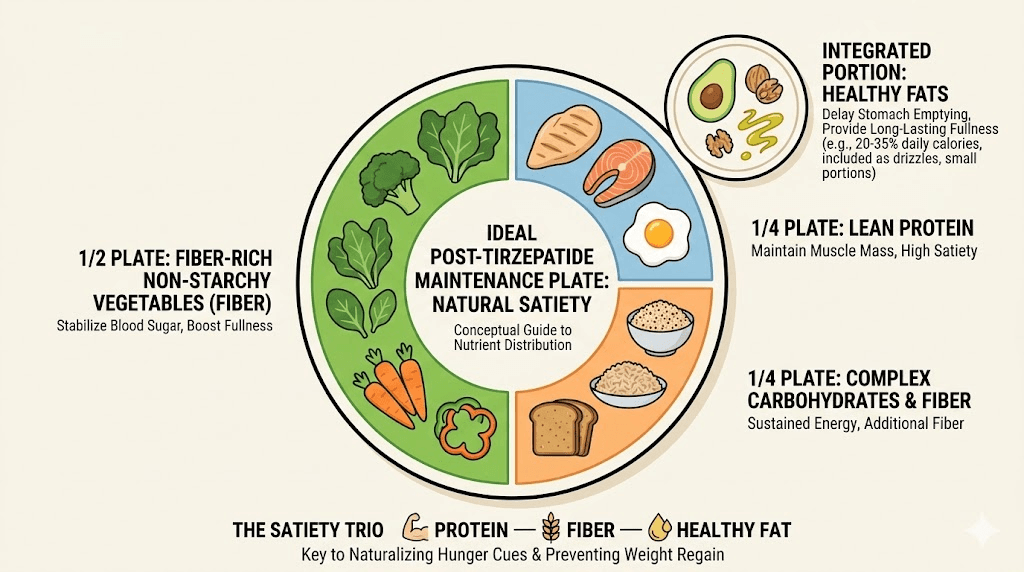
The tirzepatide diet plan you followed during treatment should transition into a maintenance diet, incorporating lessons from both the semaglutide diet plan framework and general peptide-supported fat loss principles. Protein intake becomes even more critical during tapering because protein is the most satiating macronutrient, meaning it keeps you fuller longer. Aim for 0.7 to 1 gram of protein per pound of your target body weight daily. Protein shakes can help hit these targets when whole food sources fall short.
Fiber is your other major ally. Soluble fiber slows gastric emptying, partially mimicking one of the effects tirzepatide provided. Aim for 25 to 35 grams daily from vegetables, legumes, whole grains, and fruits. The best foods during GLP-1 treatment remain the best foods after it ends. The foods that supported your GLP-1 treatment remain important after it ends.
Build your exercise routine while you still have the metabolic advantage
Starting a new exercise program while tapering adds unnecessary stress. Build the routine while you are still on your full dose, when energy is high and motivation is strong. Research consistently shows that people who exercise regularly during GLP-1 treatment have significantly better outcomes when they stop.
The minimum recommendation is 150 minutes of moderate-intensity cardio per week plus two sessions of resistance training. But for people coming off tirzepatide, more is better. Aim for 200 to 300 minutes of total activity if possible. The extra investment in exercise now pays compound interest once the medication is gone.
Address your sleep
Poor sleep increases hunger hormones, reduces insulin sensitivity, and makes weight management harder across every dimension. If you are not consistently getting 7 to 9 hours of quality sleep, fix this before you start tapering. Sleep disruptions from tirzepatide and GLP-1 related insomnia typically resolve as the dose decreases, which is one benefit of tapering, but your sleep hygiene practices need to be solid independently.
Get your support system in place
Tell your healthcare provider you are planning to taper. Set up regular check-ins, monthly at minimum, to monitor weight, metabolic markers, and overall progress. If you work with a dietitian or nutritionist, increase your appointment frequency during the taper. Join a community of people going through the same process. SeekPeptides members access detailed tapering protocols, community support, and expert guidance for navigating this exact transition, and the value of having experienced researchers and practitioners to consult cannot be overstated.
Exercise strategies that protect your results
Exercise is not optional during a tirzepatide taper. It is essential. And the type of exercise matters as much as the amount.
Resistance training preserves muscle mass
One of the legitimate concerns about GLP-1 medications is muscle loss during weight reduction. Studies show that up to 40% of the weight lost on tirzepatide can be lean mass rather than fat, particularly if resistance training is not part of the protocol. When you stop the medication, preserving the muscle you have is critical because muscle is metabolically active tissue that burns calories at rest. Losing it slows your metabolism and makes weight regain more likely.
Train each major muscle group at least twice per week. Focus on compound movements like squats, deadlifts, bench press, rows, and overhead press. These recruit the most muscle and produce the strongest metabolic stimulus. If you are new to resistance training, start with machines or bodyweight exercises and progress to free weights as your confidence and form improve.
Zone 2 cardio supports metabolic health
Zone 2 cardio, the intensity level where you can hold a conversation but feel like you are working, is the sweet spot for metabolic health during a taper. This type of exercise improves mitochondrial function, enhances fat oxidation, and supports insulin sensitivity without creating the excessive cortisol response that high-intensity training can produce.
Walking is the simplest form. Aim for 8,000 to 10,000 steps daily, with at least 30 minutes of intentional brisk walking. Cycling, swimming, and hiking all work equally well. The point is consistency, not intensity. If you previously relied on the metabolic boost from tirzepatide or the energy improvements it provided, exercise now takes over that role.
High intensity interval training in moderation
HIIT has its place, but during a taper it should be the smallest portion of your exercise mix. One to two HIIT sessions per week provides metabolic benefits without excessive stress. Too much high-intensity work while your body is readjusting to life without tirzepatide can increase cortisol, which promotes fat storage, particularly around the midsection. The strategies for targeting belly fat through exercise apply here as well.
The muscle preservation imperative
This point deserves repeating because it is that important. One of the most documented concerns with GLP-1 receptor agonist therapy is the loss of lean body mass during treatment. When you lose 50 pounds on tirzepatide, not all of that is fat. Research suggests that 25% to 40% can be lean tissue, primarily muscle. This lean mass loss becomes critically important during discontinuation because muscle is your metabolic engine. Every pound of muscle burns approximately 6 to 7 calories per day at rest, compared to roughly 2 calories per pound of fat. Lose 15 pounds of muscle during treatment, and your resting metabolic rate drops by roughly 90 to 105 calories daily. That deficit compounds week after week, month after month. Resistance training before and during your taper is the single most effective countermeasure. The people who maintained their results in the long-term studies were not just eating well. They were actively preserving and building muscle through progressive resistance training. If you are interested in additional support for muscle preservation, exploring peptides for muscle growth or the best muscle growth peptides alongside your exercise program is worth discussing with your provider.
Non-exercise activity thermogenesis
NEAT, the calories you burn through daily activities that are not formal exercise, accounts for a surprisingly large portion of total energy expenditure. Standing instead of sitting, taking stairs instead of elevators, walking while on phone calls, doing yard work, and generally staying physically active throughout the day all contribute. During a taper, increasing NEAT can offset some of the metabolic slowing that occurs as the medication clears your system.
Nutrition strategies after tirzepatide
The dietary approach that worked while you were on tirzepatide may need adjustment once the medication is gone. Here is how to adapt.
Prioritize protein at every meal
Protein should anchor every meal and most snacks. It provides the strongest satiety signal of any macronutrient, and it supports muscle preservation during the transition. A practical target is 30 grams of protein at each main meal and 15 to 20 grams at snacks. This might look like eggs and Greek yogurt at breakfast, chicken or fish with vegetables at lunch, and a protein-rich dinner with beans, tofu, or meat. High-protein meal strategies that supported your GLP-1 treatment translate directly to your maintenance phase.
Use fiber strategically
Fiber slows digestion and keeps you fuller longer, partially replacing the gastric emptying delay that tirzepatide provided. But not all fiber is equal. Soluble fiber from oats, beans, lentils, chia seeds, and psyllium husk forms a gel in the digestive tract that is particularly effective at extending satiety. Insoluble fiber from vegetables and whole grains adds bulk. You want both, with an emphasis on soluble fiber during the first months off medication.
Manage carbohydrates intelligently
You do not need to eliminate carbohydrates. But you do need to be strategic. Simple carbohydrates like sugar, white bread, and refined grains cause rapid blood sugar spikes followed by crashes that trigger hunger. Complex carbohydrates from whole grains, vegetables, and legumes provide sustained energy without the crash. Pairing carbohydrates with protein and fat at every meal slows their absorption and blunts the glucose response.
This matters more after stopping tirzepatide because the medication improved glucose metabolism directly. Without it, your body handles carbohydrates less efficiently, at least initially. The foods you were advised to avoid on GLP-1 medications remain worth avoiding, perhaps even more so, once the medication is gone.
Meal timing and structure
Eating at consistent times helps regulate hunger hormones and prevents the chaotic snacking that often accompanies returned appetite. Three structured meals plus one to two planned snacks works well for most people. Avoid skipping meals, which can lead to extreme hunger and overeating later. And avoid grazing, which adds calories without the satisfaction signal of a proper meal.
Some people find time-restricted eating helpful during the transition. Consuming all food within an 8 to 10 hour window can help manage total caloric intake while aligning with natural circadian rhythms. This is not mandatory, but if you experimented with it during treatment and found it helpful, continuing the practice makes sense.
Hydration
Water intake matters more than most people realize. Thirst is frequently misinterpreted as hunger, and dehydration reduces metabolic efficiency. Aim for at least half your body weight in ounces daily. More if you exercise intensely or live in a warm climate. Drinking a full glass of water before each meal can reduce total food intake by providing initial stomach volume.
The supplement question
Certain supplements that supported your tirzepatide regimen may continue to provide value during and after tapering. B12 supplementation addresses deficiencies that GLP-1 medications can cause, whether through standalone supplements or B12-enhanced compounds. Glycine supports multiple metabolic pathways. Some users also explore niacinamide or methylcobalamin combinations. Magnesium helps with sleep and muscle function. Omega-3 fatty acids support insulin sensitivity and reduce inflammation. None of these replace proper nutrition, but they fill gaps that the dietary transition might create.
Monitoring and tracking during your taper
What gets measured gets managed. During a tirzepatide taper, you need to track several variables to catch problems early and adjust your approach before small setbacks become large ones.
Weekly weigh-ins
Weigh yourself at the same time, on the same day, wearing the same thing (or nothing), once per week. Daily weigh-ins create too much noise from water fluctuations and can cause unnecessary stress. Weekly weigh-ins provide a clearer trend. If you see a consistent upward trend of more than 2 to 3 pounds over 2 to 3 consecutive weeks, that is a signal to evaluate whether you need to slow your taper, increase exercise, or tighten your nutrition.
Waist circumference
The scale does not tell the whole story. If you are exercising, particularly with resistance training, you may gain muscle while losing fat, which can keep the scale stable while your body composition improves. Measure your waist at the navel level once every two weeks. This metric correlates more strongly with metabolic health than scale weight and is a more sensitive indicator of fat regain.
Appetite tracking
Rate your hunger on a 1 to 10 scale three times daily, before each main meal. This helps you identify patterns. Are you hungrier in the morning or evening? Does hunger spike on certain days of the week? Does it correlate with sleep quality or stress levels? Understanding your hunger patterns lets you intervene proactively rather than reactively.
Blood sugar monitoring
If you have any history of insulin resistance, prediabetes, or type 2 diabetes, monitoring blood glucose during your taper is not optional. Tirzepatide directly improves glycemic control, and removing it can cause blood sugar to rise. A continuous glucose monitor provides the most detailed data, but even periodic fasting glucose checks with a finger-stick meter provide useful information. If your fasting glucose consistently rises above 100 mg/dL, consult your healthcare provider.
Energy and mood
Changes in energy and mood often precede changes on the scale. If you notice increasing fatigue, irritability, or motivation loss during a particular phase of your taper, it may indicate that the reduction was too aggressive or that your nutrition or sleep needs attention. Fatigue during GLP-1 transitions is common and manageable but should not be ignored.
Sleep quality
Track hours slept and subjective sleep quality. Poor sleep during a taper often signals that something needs adjustment. It could be stress, caffeine timing, or the metabolic shift itself. Addressing sleep problems quickly prevents the cascade of increased hunger, reduced willpower, and impaired decision-making that poor sleep triggers.
When stopping tirzepatide is not recommended
Not everyone should wean off. In some situations, continuing treatment, even at a reduced dose, is the medically appropriate choice.
Type 2 diabetes management
If tirzepatide was prescribed for blood sugar control and not just weight loss, stopping could have serious consequences for your glycemic management. The dual GIP and GLP-1 action of tirzepatide provides potent glucose-lowering effects that may be difficult to replicate with other medications, as the comparison of semaglutide and tirzepatide effects demonstrates. Discuss alternatives with your endocrinologist before making any changes.
Significant remaining weight to lose
If you have not yet reached a healthy BMI or if you still have substantial weight-related health risks, discontinuing prematurely may undermine your long-term health outcomes. The BMI considerations for GLP-1 therapy extend beyond initial qualification and into decisions about treatment duration.
History of severe weight cycling
If you have a history of losing and regaining large amounts of weight repeatedly, sometimes called yo-yo dieting, stopping tirzepatide without a robust maintenance plan carries higher risk. Weight cycling is associated with worsening metabolic function over time, and each cycle can make subsequent weight loss harder. For people with this history, a long-term maintenance dose may be more appropriate than discontinuation.
Active eating disorder
If you are managing binge eating disorder or another eating disorder that tirzepatide has helped control, stopping the medication requires coordination with a mental health professional who specializes in eating disorders. The appetite and impulse control changes that accompany discontinuation can trigger relapse in vulnerable individuals.
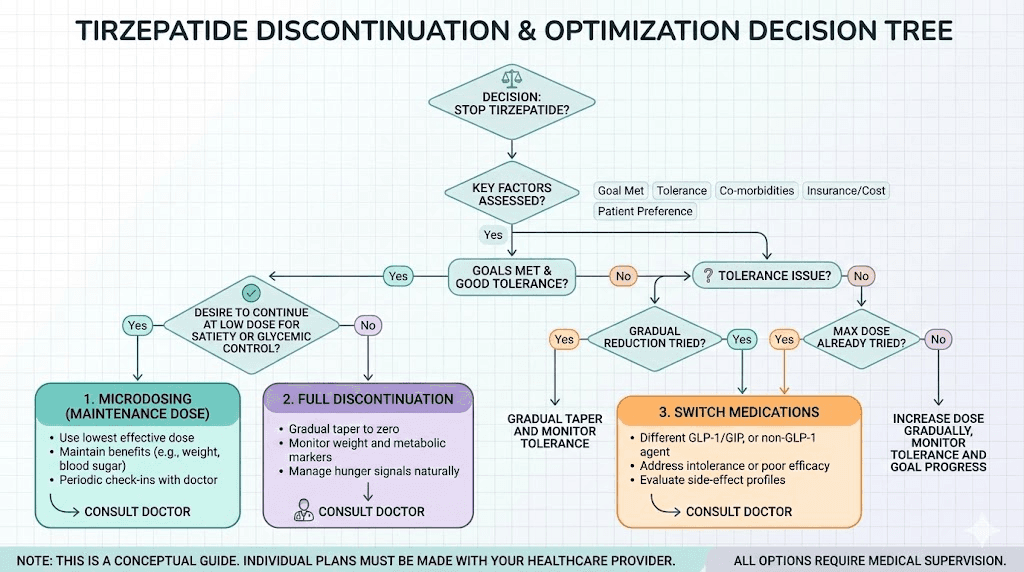
Alternatives to full discontinuation
Stopping entirely is not the only option. Several alternatives allow you to reduce cost or side effect burden while maintaining some benefits.
Maintenance microdosing
Instead of stopping completely, some people transition to a very low maintenance dose. The tirzepatide microdose chart outlines protocols where people use 1 to 2.5 mg weekly or even every other week long-term. This approach provides enough receptor activation to blunt appetite return without the full side effect profile or cost of standard doses. The microdose schedule can be customized based on individual response.
Dose splitting
Some researchers and clinicians have explored splitting the tirzepatide dose across two weekly injections rather than one. This can provide more stable drug levels and potentially allow a lower total weekly dose while maintaining adequate appetite suppression. It is an off-label approach but one that has logical pharmacological support.
Switching to a different GLP-1
If cost is the primary driver, switching from tirzepatide to semaglutide may offer a more affordable alternative while maintaining GLP-1 receptor activation. Semaglutide is available in both injectable and oral formulations, and you can use the semaglutide dosage calculator to find equivalent doses, and compounded versions can be significantly less expensive. Understanding the side effect differences between the two medications helps you make an informed decision.
Intermittent dosing
Some providers use an approach where patients take tirzepatide for a set period, stop for a set period, and resume if weight regain exceeds a threshold. For example, 6 months on, 3 months off, repeat if needed. This cyclical approach reduces total medication exposure and cost while providing a safety net against runaway weight regain. The concept is similar to how researchers approach dose timing flexibility, adapting the schedule to individual needs. How long you stay on GLP-1 medications is increasingly understood as a personalized decision rather than a one-size-fits-all prescription.
Adding supportive medications
Some clinicians add medications like phentermine or other appetite suppressants during the taper to smooth the transition. This bridging approach can help maintain appetite control while the tirzepatide dose decreases. It is a conversation to have with your prescriber, not something to pursue independently. Understanding the differences between phentermine and GLP-1 medications and the phentermine versus semaglutide comparison is important if this strategy interests you.
Common mistakes people make when weaning off
Learning from the mistakes of others is cheaper than making them yourself.
Stopping cold turkey
The most common and most damaging mistake. You feel great at your current weight. You decide you do not need the medication anymore. You stop. Three months later, half the weight is back. The research is unambiguous on this point. Gradual tapering produces better outcomes than abrupt discontinuation for the vast majority of people. Even if you are in a rush, a compressed 4 to 6 week taper is better than stopping overnight.
Tapering too fast
Reducing by multiple dose levels simultaneously or spending only 1 to 2 weeks at each level does not give your body time to adjust. Each dose reduction triggers hormonal and neurological recalibrations that take weeks, not days. Rushing the process is almost as bad as stopping cold. If you have been on a stable dose for months, your body needs time to adapt to each new level.
Not changing eating habits during treatment
If tirzepatide was your entire weight management strategy, meaning you ate whatever you wanted just in smaller amounts because the medication killed your appetite, you have a problem. The medication masked the need for dietary changes rather than eliminating it. Whether you were on oral tirzepatide or injectable forms, the mechanism is the same. When the medication goes away, the appetite returns, and without new eating habits to fall back on, old patterns re-emerge immediately.
Ignoring the scale during the taper
Some people avoid weighing themselves because they are afraid of what they might see. This is understandable but counterproductive. Early detection of weight regain allows early intervention. If you catch a 3-pound regain in week 2, you can adjust your approach. If you do not weigh yourself for 2 months and discover a 15-pound regain, the hole is much harder to climb out of. The troubleshooting approaches for tirzepatide plateaus and semaglutide plateau strategies apply during tapering as well.
Abandoning exercise when the medication stops working
A common pattern is that people exercise consistently during treatment, then stop exercising once the medication is discontinued, often because returned appetite and fatigue make it harder to find motivation. This is the exact worst time to stop exercising. Exercise is your most powerful tool for maintaining metabolic rate and managing appetite once the medication is gone. Treat it as non-negotiable. The people who explored alternative weight management peptides or weight loss stacks alongside exercise had better long-term outcomes than those who relied on any single intervention alone.
Comparing your progress to others
Everyone responds differently to tirzepatide discontinuation. Some people maintain 90% of their weight loss. Others struggle to keep 50%. Genetics, metabolic history, starting weight, duration of treatment, and lifestyle factors all play roles. Compare yourself to your own baseline, not to someone else on the internet.
Failing to have a Plan B
What happens if you taper off, do everything right, and still start regaining significant weight? Having a predetermined threshold, for example "if I regain more than 10 pounds, I will resume medication," prevents the slow creep of denial. Many people watch the weight come back pound by pound, telling themselves it will stop, until they have regained everything. Set a clear line in advance, and have a plan for what you will do if you cross it. Whether that means restarting tirzepatide, exploring newer options like orforglipron, or consulting with your provider about alternative strategies, knowing the plan in advance removes the emotional decision-making that accompanies weight regain.
Blood work and lab monitoring during your taper
Numbers do not lie. While the scale and your waistline provide external feedback, blood work reveals what is happening beneath the surface, and some of those changes matter more than the number on the scale.
Baseline labs before you start
Get comprehensive blood work done before you reduce your first dose. This creates a reference point to measure against as you taper. Request a fasting metabolic panel (glucose, HbA1c, insulin), a lipid panel (total cholesterol, LDL, HDL, triglycerides), inflammatory markers (CRP, ESR), thyroid function (TSH, free T3, free T4), and a complete blood count. If your tirzepatide compound included B6 or glycine, checking those levels at baseline is also worthwhile.
Mid-taper labs
When you reach the halfway point of your taper, roughly when you have reduced to half your original maintenance dose, repeat the labs. Compare against your baseline. Small increases in fasting glucose, LDL cholesterol, or inflammatory markers are expected and not cause for alarm. Large jumps, fasting glucose above 110 mg/dL, LDL increasing by more than 20%, or CRP doubling, warrant a conversation with your healthcare provider about whether to slow the taper or adjust other interventions.
Post-discontinuation labs
At 30, 60, and 90 days after your final dose, repeat the core panels. This timeline captures the metabolic transition as the drug fully clears and your body establishes a new equilibrium. The SURMOUNT-4 data showed that cardiometabolic markers deteriorated in proportion to weight regain, so these labs serve as an early warning system. If your numbers hold steady, your maintenance strategy is working. If they deteriorate significantly, intervention is needed before the trend becomes entrenched.
Hormone panels
For women, tirzepatide can affect reproductive hormones, and these effects reverse after stopping. If you experienced menstrual changes on tirzepatide, tracking these through discontinuation helps you understand when your cycle returns to baseline. For both men and women, monitoring cortisol levels provides insight into stress adaptation during the taper, since elevated cortisol promotes fat storage and undermines weight maintenance efforts.
The role of metabolic adaptation
Understanding why weight regain happens helps you fight it more effectively. It is not about willpower. It is about biology.
Adaptive thermogenesis
When you lose weight, your body reduces its energy expenditure beyond what would be expected from the change in body size alone. This phenomenon, called adaptive thermogenesis, means a person who weighs 180 pounds after losing 50 pounds burns fewer calories than a person who has always weighed 180 pounds. The deficit can be 200 to 300 calories per day, which adds up quickly.
Tirzepatide partially counteracts this adaptation through its metabolic effects, which is one reason it produces such dramatic weight loss results over time. When the medication is removed, adaptive thermogenesis reasserts itself, and your caloric needs are lower than you might expect for your current weight. This is why many people who eat "normally" after stopping still regain weight. Their version of normal is calibrated to a metabolic rate that no longer exists.
Hormonal rebound
Weight loss triggers increases in ghrelin (the hunger hormone) and decreases in leptin (the satiety hormone). These changes persist for months or even years after weight loss. Tirzepatide overrides these hormonal signals through its GLP-1 and GIP receptor activation. Without the medication, the hormonal environment actively promotes weight regain. Understanding that your increased hunger after stopping is hormonal, not a character flaw, helps you approach it strategically rather than emotionally.
Neural pathway changes
The brain reward circuitry changes in response to weight loss, making calorie-dense foods more rewarding and harder to resist. Tirzepatide dampens these reward signals. After discontinuation, food tastes better, feels more rewarding, and is harder to say no to. This is neuroscience, not weakness. Planning for it is essential. SeekPeptides members navigate these neurological transitions with the support of detailed protocols and a community of researchers who understand the science behind what you are experiencing.
A week-by-week guide for the first month off medication
The first 30 days after your final injection are the most critical. Here is what to expect and what to do.
Week 1: The grace period
You still have significant drug levels in your system. Appetite suppression remains noticeable. Weight is stable. This is the calm before the storm. If you have any remaining questions about reconstitution or injection sites, resolve them now since you will not need this knowledge much longer. Use this week to double down on meal prep, confirm your exercise schedule, and set up your monitoring systems. Do not be lulled into false confidence by how easy this week feels.
Week 2: First signs of change
Drug levels have dropped to roughly half. You may notice slightly increased appetite, particularly in the evening. Cravings may begin to resurface for foods you had lost interest in during treatment. Keep portion sizes controlled and stick to your meal plan. Continue exercising at your established intensity. This is manageable.
Week 3: The inflection point
This is typically the hardest week. Drug levels are low enough that appetite suppression is minimal. Hunger between meals becomes more pronounced. The mental challenge intensifies as you realize this is what life without medication feels like. Social eating situations become harder to navigate. This is the week where your preparation either pays off or its absence becomes painfully obvious.
Stay close to your support system. Lean on your meal plan. Exercise even when you do not feel like it. Track everything. This week passes. The discomfort peaks and then begins to stabilize as your body adapts to the new normal.
Week 4: Establishing the new baseline
The medication is essentially cleared from your system. What you experience this week is your new metabolic reality. Hunger levels stabilize, though they will be higher than they were on medication. Cravings become more predictable. Energy levels adjust. Your weight by the end of this week gives you a realistic baseline for what maintenance looks like going forward.
If your weight is within 3 to 5 pounds of where it was at your final dose, you are in good shape. If it has increased by more than 5 pounds, evaluate whether your nutrition and exercise need tightening, whether a low starting dose of medication might be appropriate to resume, or whether an entirely different approach like combining with AOD-9604 or exploring fat loss peptides is worth discussing with your provider. The strategies for when tirzepatide results plateau translate well to maintenance challenges, as many of the underlying principles are the same.
Long-term maintenance after tirzepatide
Getting through the taper is only half the battle. Staying off the medication while maintaining your results requires ongoing attention, though not the same level of intensity as the taper itself.
The first 6 months
This is the highest-risk period for regain. Monthly weigh-ins should continue. Exercise should remain a priority. Use the peptide calculator if you are considering any supportive protocols. Dietary habits should be maintained with minimal deviation. If you notice a sustained upward trend, act immediately rather than waiting to see if it resolves on its own. The troubleshooting mindset you used during treatment applies here too.
Months 6 through 12
By this point, most people have found their equilibrium. The weight has either stabilized, continued to creep up, or in some cases, continued to decrease as improved habits compound. Continue monitoring but shift to biweekly or monthly check-ins. Maintain your exercise routine. Allow some dietary flexibility but keep your core habits intact.
Beyond one year
If you have maintained your weight loss for a full year after stopping tirzepatide, you are in the minority, and congratulations are genuinely warranted. The habits you have built are now deeply established. Continue them. Weight management is a lifelong process, not a destination. Whether you eventually explore other peptide options or maintain through lifestyle alone, the foundation you built during this taper serves you indefinitely. The timeline of your weight loss journey extends well beyond the medication itself.
For researchers and practitioners serious about optimizing their peptide protocols and post-treatment maintenance, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
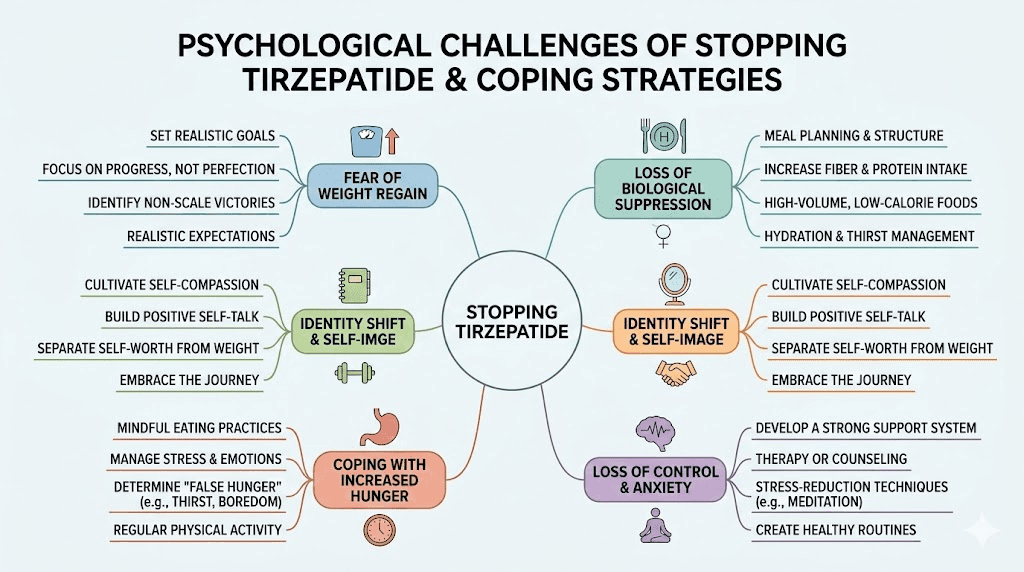
The psychological side of stopping
Nobody talks enough about this part. The physical taper gets all the attention, but the mental transition can be equally challenging.
Identity after medication
For many people, tirzepatide became part of their identity. "The medication that finally worked." "The thing that changed my life." Letting go of that creates a subtle grief, even when the decision is voluntary. You may feel vulnerable without it. You may question whether you can maintain results on your own. These feelings are normal and do not mean you are making the wrong choice.
Fear of regain
Having seen dramatic transformation results, the thought of losing that progress creates genuine anxiety. This fear can become paralyzing if left unchecked. Channel it into action instead. Fear of regain, when managed productively, becomes the motivation that keeps you exercising on days you do not want to and eating well when convenience food calls.
Social pressure and judgment
If people in your life know you were on tirzepatide, they may watch your weight with uncomfortable attention after you stop. Comments about "keeping it off" or unsolicited opinions about whether you should have stopped can be stressful. Set boundaries early. Your medical decisions are personal. Share your journey on your terms, not in response to other people's curiosity.
Decision fatigue around food
One underappreciated benefit of tirzepatide was that it reduced the mental energy spent thinking about food. When appetite is suppressed, food decisions are simpler. You eat less, you think about food less, and the constant internal negotiation about what and how much to eat quiets down. After stopping, that negotiation returns in full force. Every meal becomes a decision. Every snack requires evaluation. This is exhausting, especially in the first months. Automating your meals through meal prep, having go-to options, and following a structured meal plan reduces this cognitive load significantly.
Frequently asked questions
Can you stop tirzepatide cold turkey?
You can, because tirzepatide does not cause physical dependence or dangerous withdrawal symptoms. However, stopping abruptly significantly increases the risk of rapid weight regain and appetite rebound compared to a gradual taper. Most healthcare providers recommend a structured dose reduction over 8 to 16 weeks for the best long-term outcomes.
How long does it take for tirzepatide to leave your system?
With a half-life of approximately 5 days, tirzepatide takes 25 to 30 days to fully clear your system after the final injection. During this period, effects gradually diminish. By day 10, about half the drug remains. By day 20, roughly a quarter. By day 30, the drug is essentially undetectable, and any remaining appetite suppression has resolved.
Will I regain all the weight if I stop tirzepatide?
Not necessarily, but the odds are against maintaining full weight loss without intervention. The SURMOUNT-4 trial showed that 82.5% of people who stopped regained at least 25% of their lost weight within a year. However, the 17.5% who maintained their results typically had strong exercise routines, established dietary habits, and ongoing monitoring in place. Your preparation determines your outcome.
What is the best dose to taper from?
Any dose can be tapered. The process is the same regardless of starting dose, reduce by 2.5 mg every 4 to 8 weeks until you reach 2.5 mg, then discontinue. The total duration depends on your starting dose. Someone tapering from 10 mg needs less time than someone tapering from 15 mg. Use the tirzepatide dose chart to plan your specific schedule.
Should I switch to semaglutide instead of stopping entirely?
Switching to semaglutide from tirzepatide is a viable option, particularly if cost is the main reason for discontinuation. Semaglutide provides GLP-1 receptor activation (though not the GIP component that tirzepatide offers) and is available in potentially more affordable compounded forms. Understanding the differences between semaglutide and tirzepatide helps you decide whether this switch makes sense.
Can I use a lower tirzepatide dose long term instead of stopping?
Yes, and this is increasingly the recommended approach for people at high risk of regain. A maintenance microdose of 2.5 mg weekly or even every other week can provide enough appetite suppression to prevent significant regain while minimizing cost and side effects. Discuss this option with your healthcare provider.
Does tirzepatide cause withdrawal symptoms?
Tirzepatide does not cause classical withdrawal symptoms like those associated with opioids or benzodiazepines, and this applies regardless of whether you were using orally disintegrating tablets, sublingual formulations, or injections. There is no physical dependence. However, the return of appetite, changes in energy levels, shifts in mood, and alterations in digestive function that occur after stopping are sometimes described as "withdrawal-like" even though they are technically just the resolution of the drug effects. Understanding withdrawal-like symptoms from GLP-1 medications helps set realistic expectations.
How much weight is normal to regain after stopping?
Research suggests that some weight regain is nearly universal after stopping tirzepatide. The goal is to keep it below 25% of total weight lost, which is the threshold where cardiometabolic benefits remain largely preserved. Regaining 5 to 10 pounds after losing 40 to 50 is a realistic and acceptable outcome for most people. Regaining 20 to 30 pounds suggests the maintenance strategy needs strengthening.
When is the best time to start tapering?
The ideal time to begin tapering is after you have been at a stable weight for at least 2 to 3 months, have established consistent exercise and dietary habits, and have your support and monitoring systems in place. Avoid starting a taper during high-stress periods (holidays, major life changes, travel seasons) when adherence to new habits is naturally harder. Review the dosing fundamentals before planning your reduction steps.
Can I use supplements to help with the transition?
Certain supplements may support the transition. B12 and glycine address potential deficiencies from GLP-1 treatment. Fiber supplements like psyllium husk can help extend satiety. Protein supplements help hit daily targets. Magnesium and omega-3s support metabolic health. However, supplements are adjuncts to, not replacements for, proper nutrition, exercise, and monitoring. The supplement guide for tirzepatide users covers these options in detail.
External resources
SURMOUNT-4 Trial: Continued Treatment With Tirzepatide for Maintenance of Weight Reduction (JAMA)
Cardiometabolic Parameter Change by Weight Regain on Tirzepatide Withdrawal (JAMA Internal Medicine)
In case I do not see you, good afternoon, good evening, and good night. May your taper stay gradual, your habits stay strong, and your results stay permanent.