Feb 15, 2026

Drawing 10 units from one vial gives you 0.5 mg. Drawing 10 units from a different vial gives you 0.25 mg. Same syringe. Same marking. Completely different doses.
That is not a hypothetical scenario. The FDA has received hundreds of adverse event reports tied to compounded semaglutide dosing errors, with some patients accidentally injecting five to twenty times their intended dose. The problem is not carelessness. The problem is that "units" on an insulin syringe do not directly translate to milligrams of semaglutide, and the relationship between them changes with every concentration.
If you have ever stared at your syringe and wondered whether you are drawing the right amount, you are not alone. Millions of people use semaglutide for weight management and blood sugar control. Most of them received minimal instruction on how units actually work. The confusion between mg, mL, and units has sent people to emergency rooms. It has caused weeks of nausea that should never have happened. And it is almost entirely preventable with the right information.
This guide breaks down everything about semaglutide dosage in units. You will learn the universal conversion formula that works for any concentration. You will see complete charts for 1 mg/mL, 2.5 mg/mL, 5 mg/mL, and 10 mg/mL vials. You will understand how to read your syringe correctly, what the FDA recommends, and the specific mistakes that cause dangerous overdoses. Whether you are using a compounded vial or an FDA-approved pen, this is the reference you will keep coming back to.
Why semaglutide dosage is measured in units
Understanding why semaglutide uses units instead of a simpler measurement system starts with the syringe itself.
A standard U-100 insulin syringe holds exactly 1 mL of liquid. That 1 mL is divided into 100 equal markings. Each marking represents one "unit." The term comes from insulin dosing, where one unit equals a specific biological activity of insulin. But semaglutide is not insulin. When you draw semaglutide into an insulin syringe, the unit markings are simply measuring volume, not pharmacological potency.
Here is the critical distinction. Ten units on your syringe always equals 0.1 mL of liquid. Always. Regardless of what medication is inside. But 0.1 mL of a 5 mg/mL solution contains 0.5 mg of semaglutide, while 0.1 mL of a 2.5 mg/mL solution contains only 0.25 mg. The syringe measures volume. The concentration determines how much active ingredient is in that volume.
This is where every dosing error begins.
FDA-approved semaglutide pens like Ozempic and Wegovy sidestep this problem entirely. Their dose dials display milligrams directly. You select 0.25 mg or 0.5 mg, click the button, and the pen delivers the exact volume needed. No conversion required. No math involved.
Compounded semaglutide works differently. You receive a multi-dose vial containing a specific concentration of semaglutide dissolved in liquid. Your provider tells you to inject a certain number of milligrams. But your syringe only shows units. Bridging that gap requires understanding concentration, and that is exactly what most patient instructions fail to explain clearly.
The semaglutide dosage calculator on SeekPeptides can handle this math instantly. But knowing how to do it yourself is essential for catching errors before they reach your body.
The universal conversion formula
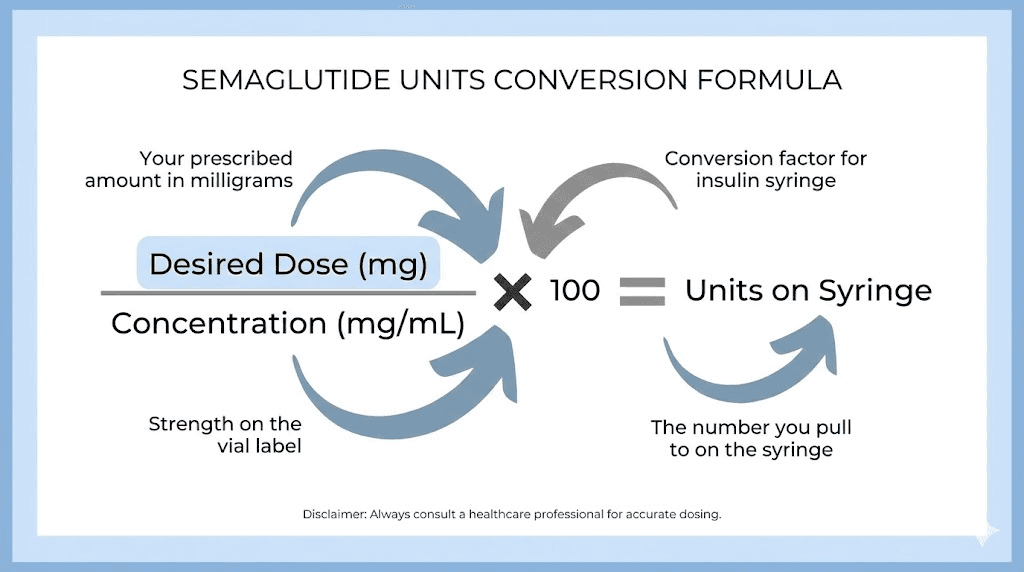
Every semaglutide unit-to-mg conversion uses the same formula. Learn this once and you can figure out the correct dose for any concentration.
Units = (Desired dose in mg / Concentration in mg per mL) x 100
That is it. Three numbers. One calculation. Let me walk through why it works.
The concentration tells you how many milligrams of semaglutide are dissolved in each milliliter of liquid. If your vial says 5 mg/mL, there are 5 milligrams in every 1 mL. Dividing your desired dose by the concentration gives you the volume in milliliters. Multiplying by 100 converts milliliters to syringe units, because 1 mL equals 100 units on a U-100 syringe.
Example with 5 mg/mL concentration
You want 0.25 mg of semaglutide. Your vial concentration is 5 mg/mL.
Units = (0.25 / 5) x 100 = 5 units
Draw to the 5-unit mark on your syringe. Done.
Example with 2.5 mg/mL concentration
Same 0.25 mg dose. Different vial, this one is 2.5 mg/mL.
Units = (0.25 / 2.5) x 100 = 10 units
You need 10 units now instead of 5. Double the volume for the same milligram dose. This is exactly the kind of difference that causes overdoses when someone switches concentrations without recalculating.
Example with 10 mg/mL concentration
Again, 0.25 mg desired. Vial is 10 mg/mL.
Units = (0.25 / 10) x 100 = 2.5 units
Only 2.5 units. That is a tiny amount of liquid, barely visible in the syringe barrel. This concentration requires extreme precision with your draw, and even half a unit of error represents a significant percentage of your dose.
The formula never changes. Only the concentration variable shifts. Reconstituting your own semaglutide gives you control over this concentration, but it also means you must know your exact numbers before drawing any dose.
Complete conversion charts by concentration
Below are the complete conversion tables for the four most common compounded semaglutide concentrations. Find your vial concentration, then look up your prescribed milligram dose to see exactly how many units to draw.
These charts assume you are using a standard U-100 insulin syringe. If you are using a different syringe type, these numbers will not apply. Always verify your syringe type before measuring. The full semaglutide conversion chart covers additional concentrations and edge cases.
1 mg/mL concentration chart
This is the most dilute common concentration. Each unit on your syringe contains 0.01 mg of semaglutide. Doses require relatively large draw volumes, which makes measurement easier but uses more liquid per injection.
Dose (mg) | Volume (mL) | Syringe units |
|---|---|---|
0.125 | 0.125 | 12.5 |
0.25 | 0.25 | 25 |
0.5 | 0.5 | 50 |
1.0 | 1.0 | 100 |
1.5 | 1.5 | 150 (requires larger syringe) |
2.0 | 2.0 | 200 (requires larger syringe) |
At 1 mg/mL, anything above 1 mg requires more than a single U-100 syringe can hold. You would need a 3 mL syringe or split the injection into two draws. Most providers avoid this concentration for higher doses because of the large injection volumes involved.
2.5 mg/mL concentration chart
This is the most widely prescribed compounded concentration according to pharmacy dispensing data. It offers a good balance between measurement precision and injection volume. Each unit contains 0.025 mg of semaglutide.
Dose (mg) | Volume (mL) | Syringe units |
|---|---|---|
0.125 | 0.05 | 5 |
0.25 | 0.1 | 10 |
0.5 | 0.2 | 20 |
1.0 | 0.4 | 40 |
1.5 | 0.6 | 60 |
1.7 | 0.68 | 68 |
2.0 | 0.8 | 80 |
2.4 | 0.96 | 96 |
Notice that even the maximum therapeutic dose of 2.4 mg fits within a single U-100 syringe at this concentration. That is one reason 2.5 mg/mL is so popular. For a detailed look at how compounded semaglutide differs from brand-name versions, the complete guide covers manufacturing, quality, and regulatory considerations.
5 mg/mL concentration chart
This is the most common concentration from compounding pharmacies. Each unit contains 0.05 mg of semaglutide. Smaller draw volumes mean less liquid per injection, but also less room for error on your syringe.
Dose (mg) | Volume (mL) | Syringe units |
|---|---|---|
0.125 | 0.025 | 2.5 |
0.25 | 0.05 | 5 |
0.5 | 0.1 | 10 |
1.0 | 0.2 | 20 |
1.5 | 0.3 | 30 |
1.7 | 0.34 | 34 |
2.0 | 0.4 | 40 |
2.4 | 0.48 | 48 |
At 5 mg/mL, notice that a 0.25 mg dose is only 5 units. That is a very small amount of liquid. If your syringe has markings every 2 units (which many do), you are aiming between two lines. Using a 5 mg/mL specific dosage chart alongside a fine-gauge syringe with single-unit markings reduces measurement error significantly.
10 mg/mL concentration chart
This high concentration is less common but available from some compounding pharmacies. Each unit contains 0.1 mg. Very small volumes are needed, which makes precision critical. This concentration is typically reserved for patients on maintenance doses who want minimal injection volume.
Dose (mg) | Volume (mL) | Syringe units |
|---|---|---|
0.25 | 0.025 | 2.5 |
0.5 | 0.05 | 5 |
1.0 | 0.1 | 10 |
1.5 | 0.15 | 15 |
2.0 | 0.2 | 20 |
2.4 | 0.24 | 24 |
At 10 mg/mL, a starting dose of 0.25 mg requires just 2.5 units. That is 0.025 mL of liquid. Measuring this accurately with a standard syringe is genuinely difficult. Many experienced researchers recommend using bacteriostatic water mixing guides to create lower concentrations that are easier to measure precisely.
How to read your syringe correctly
Knowing the conversion formula is only half the equation. You also need to read the physical syringe accurately. This sounds simple. It is not.
U-100 insulin syringes come in three common sizes: 0.3 mL (30 units), 0.5 mL (50 units), and 1 mL (100 units). The markings differ between them.
The 0.3 mL syringe (30 units)
This small syringe has markings for every single unit. Each line represents 1 unit, with longer lines at every 5-unit interval and numbers printed at every 5 or 10 units. This is the most precise option for small doses. If your dose is 25 units or less, use this syringe.
The close spacing between lines makes it easy to draw exactly 5 units, 7.5 units, or 12 units. For early-phase semaglutide dosing where precision matters most, this syringe type is ideal.
The 0.5 mL syringe (50 units)
Markings typically appear every 1 unit, with numbers at every 5 or 10 units. Good for mid-range doses. If your calculated dose falls between 15 and 50 units, this size works well.
The 1 mL syringe (100 units)
Some 1 mL syringes have markings every 2 units rather than every 1 unit. This means you cannot accurately measure odd-unit doses like 5, 15, or 25 units. The lines are farther apart, but each gap covers 2 units of liquid.
If you are told to draw 5 units and your syringe has markings at 4, 6, 8, 10, you need to estimate the midpoint between the 4 and 6 lines. That introduces error. For low doses at higher concentrations, switch to a 0.3 mL syringe with single-unit markings instead.
Reading technique that prevents errors
Hold the syringe at eye level with the tip pointing up. The plunger has a rubber gasket with two edges, a top edge closest to the needle and a bottom edge closer to your thumb. Always read from the top edge of the rubber gasket, the edge nearest the needle.
Reading from the wrong edge of the gasket is a common mistake that adds approximately 1-2 units of error. On a 5-unit dose, that is a 20-40% measurement error. On a 50-unit dose, it barely matters. Scale of impact depends on dose size, so smaller doses demand more careful technique.
If you are unsure which markings your syringe uses, the peptide calculator includes syringe-type guidance alongside dose calculations.
Standard semaglutide dosing protocol in units
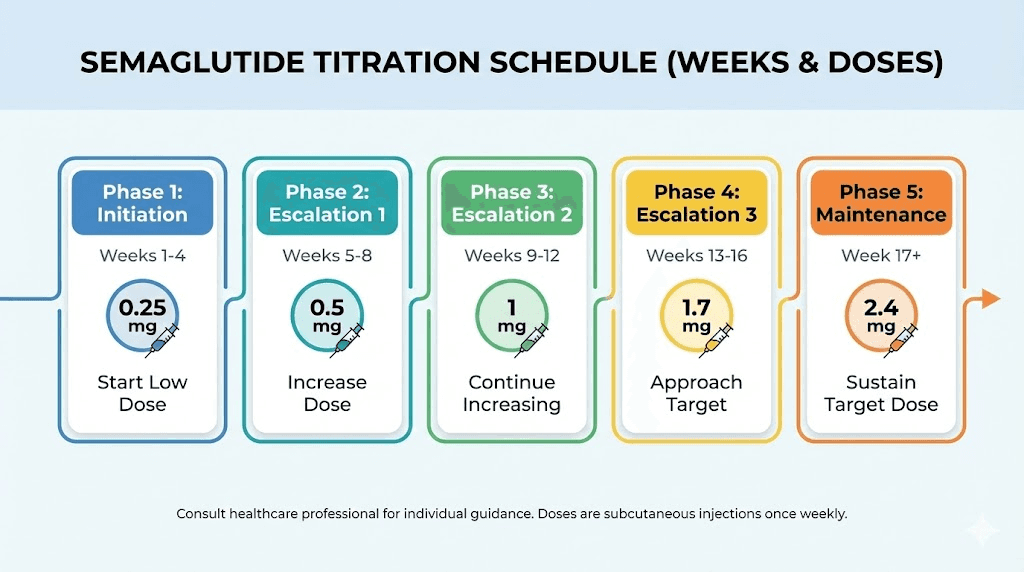
The FDA-approved titration schedule for semaglutide weight management follows a gradual ramp-up over 16 to 20 weeks. The reason for slow escalation is straightforward: gastrointestinal side effects like nausea, vomiting, and constipation are dose-dependent. Starting low and increasing slowly gives your GLP-1 receptors time to adjust.
Below is the standard schedule converted to units for each common concentration. These numbers assume you are following the standard titration pattern. Your healthcare provider may customize this based on your response, tolerance, and goals.
Phase 1: Initiation (weeks 1 through 4)
Dose: 0.25 mg once weekly
Concentration | Units to draw | Volume (mL) |
|---|---|---|
1 mg/mL | 25 | 0.25 |
2.5 mg/mL | 10 | 0.1 |
5 mg/mL | 5 | 0.05 |
10 mg/mL | 2.5 | 0.025 |
This phase is about tolerability, not results. Most people experience mild fatigue and decreased appetite without significant weight changes. The low dose establishes baseline tolerance.
Phase 2: Early escalation (weeks 5 through 8)
Dose: 0.5 mg once weekly
Concentration | Units to draw | Volume (mL) |
|---|---|---|
1 mg/mL | 50 | 0.5 |
2.5 mg/mL | 20 | 0.2 |
5 mg/mL | 10 | 0.1 |
10 mg/mL | 5 | 0.05 |
Most users begin noticing appetite suppression at this level. The step from 0.25 to 0.5 mg doubles your dose, which is the largest relative increase in the entire titration schedule. Pay attention to how your body responds during this jump.
Phase 3: Continued escalation (weeks 9 through 12)
Dose: 1.0 mg once weekly
Concentration | Units to draw | Volume (mL) |
|---|---|---|
1 mg/mL | 100 | 1.0 |
2.5 mg/mL | 40 | 0.4 |
5 mg/mL | 20 | 0.2 |
10 mg/mL | 10 | 0.1 |
At 1 mg, the appetite effects become pronounced for most people. Clinical response timelines show that this is typically where measurable weight loss begins. The 1 mg/mL concentration maxes out a standard U-100 syringe at this dose, which is one practical reason providers prefer higher concentrations for maintenance phases.
Phase 4: Upper escalation (weeks 13 through 16)
Dose: 1.7 mg once weekly
Concentration | Units to draw | Volume (mL) |
|---|---|---|
2.5 mg/mL | 68 | 0.68 |
5 mg/mL | 34 | 0.34 |
10 mg/mL | 17 | 0.17 |
Notice that 1 mg/mL concentration is not listed here. You would need 170 units (1.7 mL), which exceeds the capacity of a U-100 syringe. At this dose level, 2.5 mg/mL is the minimum practical concentration.
Phase 5: Maintenance dose (week 17 onward)
Dose: 2.4 mg once weekly (maximum therapeutic dose for weight management)
Concentration | Units to draw | Volume (mL) |
|---|---|---|
2.5 mg/mL | 96 | 0.96 |
5 mg/mL | 48 | 0.48 |
10 mg/mL | 24 | 0.24 |
At the maximum 2.4 mg dose, even 2.5 mg/mL is getting close to syringe capacity at 96 units. Some patients find that the 5 mg/mL concentration offers the best balance here, with 48 units being easy to measure and comfortable to inject. Understanding how long to stay on semaglutide at maintenance dose is a separate but equally important question.
Not everyone reaches 2.4 mg. Many people find their effective dose somewhere between 1.0 and 1.7 mg. If you are losing weight and tolerating the medication well at a lower dose, there is no requirement to keep escalating. More is not automatically better. Troubleshooting weight loss plateaus involves multiple factors beyond just increasing the dose.
Common dosing questions answered with exact unit conversions
People searching for semaglutide dosage in units often have very specific questions. Here are the most common ones with precise answers for every concentration.
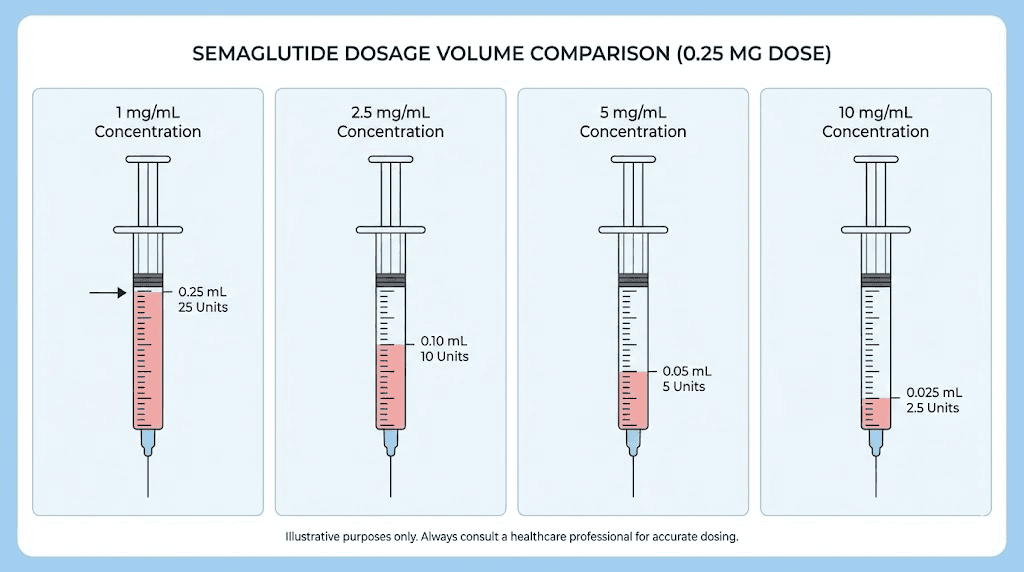
How many units is 0.25 mg of semaglutide?
This depends entirely on your concentration:
At 1 mg/mL: 25 units
At 2.5 mg/mL: 10 units
At 5 mg/mL: 5 units
At 10 mg/mL: 2.5 units
The 0.25 mg starting dose is where most measurement confusion begins because the unit counts are so different across concentrations. Someone switching from a 2.5 mg/mL vial to a 5 mg/mL vial who keeps drawing 10 units would inject double their intended dose.
How many units is 0.5 mg of semaglutide?
At 1 mg/mL: 50 units
At 2.5 mg/mL: 20 units
At 5 mg/mL: 10 units
At 10 mg/mL: 5 units
At this dose level, timing your injection becomes important for managing side effects. Most providers recommend injecting on a day when you can rest if nausea occurs.
How many units is 1 mg of semaglutide?
At 1 mg/mL: 100 units (full syringe)
At 2.5 mg/mL: 40 units
At 5 mg/mL: 20 units
At 10 mg/mL: 10 units
How many units is 2.4 mg of semaglutide?
At 2.5 mg/mL: 96 units
At 5 mg/mL: 48 units
At 10 mg/mL: 24 units
The maximum dose is not achievable with 1 mg/mL concentration using a standard U-100 syringe. You would need 240 units, which is 2.4 mL. This is why higher concentrations exist.
What does 20 units of semaglutide equal in mg?
Again, concentration determines everything:
At 1 mg/mL: 20 units = 0.2 mg
At 2.5 mg/mL: 20 units = 0.5 mg
At 5 mg/mL: 20 units = 1.0 mg
At 10 mg/mL: 20 units = 2.0 mg
The difference between 0.2 mg and 2.0 mg is tenfold. This single example illustrates why you must verify your concentration before every injection.
What does 40 units of semaglutide equal in mg?
At 1 mg/mL: 40 units = 0.4 mg
At 2.5 mg/mL: 40 units = 1.0 mg
At 5 mg/mL: 40 units = 2.0 mg
At 10 mg/mL: 40 units = 4.0 mg (exceeds maximum therapeutic dose)
What does 50 units of semaglutide equal in mg?
At 1 mg/mL: 50 units = 0.5 mg
At 2.5 mg/mL: 50 units = 1.25 mg
At 5 mg/mL: 50 units = 2.5 mg (above maximum therapeutic dose)
At 10 mg/mL: 50 units = 5.0 mg (dangerously above maximum dose)
The reverse conversion formula is just as straightforward: mg = (Units / 100) x Concentration in mg/mL. Use it whenever you know the units drawn but need to verify the milligram dose.
FDA safety warnings about semaglutide dosing errors
This is not theoretical. The FDA issued a specific safety communication about compounded semaglutide dosing errors after receiving hundreds of adverse event reports. Understanding what went wrong in these cases can prevent you from making the same mistakes.
The scale of the problem
As of April 2025, the FDA had received over 520 adverse event reports related to compounded semaglutide. Poison control centers have documented a nearly 1,500% increase in calls related to injectable weight-loss drugs. Many of these involved dosing errors rather than medication reactions.
The typical overdose scenario involves a five-fold to twenty-fold excess. A patient meant to take 0.25 mg accidentally injects 1.25 mg or even 5 mg. The consequences are severe: prolonged nausea lasting days instead of hours, vomiting that leads to dehydration, severe gastrointestinal distress, and in serious cases, acute pancreatitis requiring hospitalization.
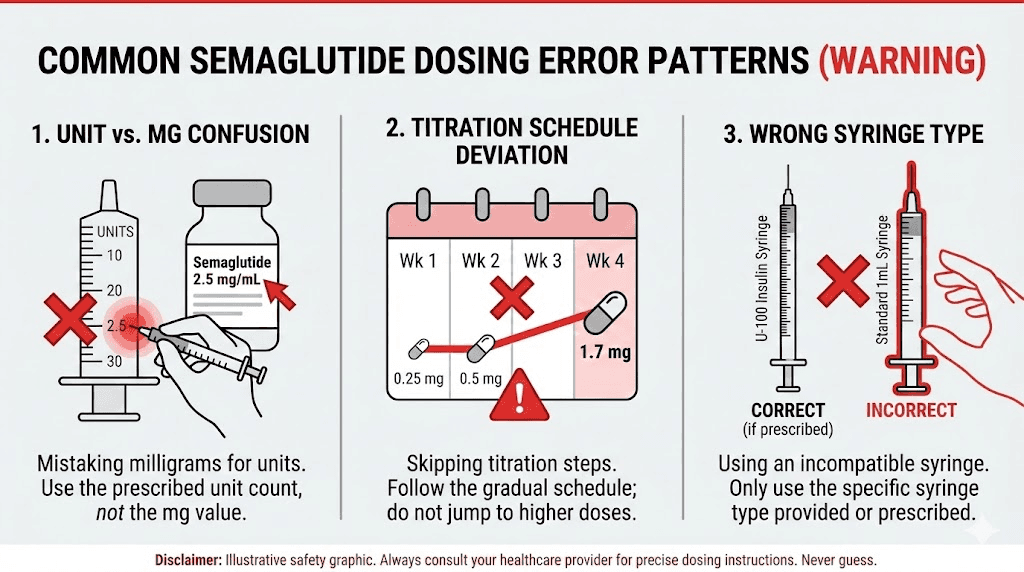
The three most common error patterns
Error 1: Confusing units with milligrams. A provider prescribes "0.25 mg" and the patient draws to the 25-unit mark thinking units and milligrams are the same thing. On a 5 mg/mL vial, 25 units equals 1.25 mg, which is five times the intended dose. This single mistake accounts for the largest share of reported overdoses.
Error 2: Using the wrong concentration in calculations. A patient previously used a 2.5 mg/mL vial and was drawing 10 units for their 0.25 mg dose. They switch to a 5 mg/mL vial from a different pharmacy but keep drawing 10 units. Now they are getting 0.5 mg instead of 0.25 mg. Doubled dose. This happens frequently when patients refill prescriptions and receive a different concentration without realizing it.
Error 3: Misreading syringe markings. A patient is told to inject 5 units. Their 1 mL syringe has markings every 10 units. They draw to what they think is the 5-unit line but are actually at the 50-unit line because they misread the scale. This ten-fold overdose scenario appears repeatedly in FDA reports and poison control case studies.
Every single one of these errors is preventable. Double-check three things before every injection: your vial concentration, your calculated units, and your syringe reading. That thirty-second verification has kept SeekPeptides community members safe through thousands of injections.
Compounded semaglutide vs. FDA-approved pens: the units difference
The dosing experience is fundamentally different between compounded vials and FDA-approved pens. Understanding both systems prevents confusion if you switch between them or discuss dosing with someone using a different format.
FDA-approved pens (Ozempic, Wegovy)
These pre-filled pens display doses in milligrams. You turn a dial to your prescribed dose (0.25 mg, 0.5 mg, 1.0 mg, etc.) and press the injection button. The pen delivers the exact volume needed from a fixed-concentration cartridge.
You never see units. You never calculate conversions. The pen handles everything mechanically. This is the safest delivery method from a dosing accuracy perspective because human math errors are eliminated entirely.
However, these pens lock you into specific dose increments. Ozempic offers 0.25, 0.5, 1.0, and 2.0 mg. Wegovy offers 0.25, 0.5, 1.0, 1.7, and 2.4 mg. You cannot select 0.375 mg or 0.75 mg or any dose between the fixed options. For some patients who benefit from gradual dose transitions, this inflexibility is a real limitation.
Compounded semaglutide vials
Compounded vials offer complete dose flexibility. With a syringe, you can draw exactly 7 units or 33 units or any amount you need. This allows for micro-titration, alternative delivery methods, and gradual dose adjustments that pens cannot provide.
The trade-off is responsibility. You must know your concentration, perform the conversion calculation, select the right syringe, and measure accurately. Every step introduces potential for error. The convenience of customization comes with the burden of correctness.
Many compounding pharmacies now include a printed dosing card specific to your vial concentration. Keep this card with your medication. Do not rely on memory or previous vial information, especially if your pharmacy sends a different concentration than your last fill. Empower Pharmacy and other major compounders typically standardize their concentrations, but always verify.
The semaglutide salt form issue
Some compounded products use semaglutide sodium or semaglutide acetate instead of the base form used in FDA-approved products. The FDA has specifically warned that these salt forms have not been shown to be safe and effective, and their pharmacokinetic profile may differ from base semaglutide.
If your compounded vial lists a salt form, discuss this with your provider. The dosing conversion math is the same, but the clinical equivalency is unconfirmed. This is a separate safety concern from the units-to-mg conversion issue, but it compounds the risk factors when using compounded products.
Reconstitution and how it affects your units
If you are reconstituting lyophilized (freeze-dried) semaglutide yourself, you control the final concentration. This gives you flexibility but also means your conversion charts are only as accurate as your reconstitution math.
How reconstitution creates concentration
A vial containing 5 mg of lyophilized semaglutide powder becomes a specific concentration based on how much bacteriostatic water you add:
Add 1 mL of water: 5 mg/mL concentration
Add 2 mL of water: 2.5 mg/mL concentration
Add 5 mL of water: 1 mg/mL concentration
More water means lower concentration, which means more units per dose but easier measurement. Less water means higher concentration, fewer units per dose, but harder precision. There is no right or wrong choice. It depends on your syringe type and dose range.
Best practice for reconstitution
Choose a reconstitution volume that places your most common dose between 10 and 50 units on your syringe. This range is easy to measure accurately on most syringe types and leaves room for dose adjustments in either direction.
For someone starting at 0.25 mg and planning to escalate to 1.0 mg:
At 2.5 mg/mL: 0.25 mg = 10 units, 1.0 mg = 40 units (ideal range)
At 5 mg/mL: 0.25 mg = 5 units, 1.0 mg = 20 units (workable but tight at low end)
The 2.5 mg/mL option keeps all doses in a comfortable measurement range. The complete reconstitution guide walks through the exact technique for dissolving the powder without damaging the peptide. And the peptide reconstitution calculator handles the math for any vial size and desired concentration.
Record your reconstitution details
Write on the vial or on tape attached to the vial:
Reconstitution date
Amount of water added
Final concentration
Expiration (typically 28 days refrigerated for compounded semaglutide storage)
This five-second step eliminates the most common reconstitution error: forgetting which concentration you created and guessing wrong weeks later.
Special considerations for different syringe types
Not everyone uses U-100 insulin syringes. Understanding how different syringe types affect your unit measurements prevents a category of error that most dosing guides completely ignore.
U-100 insulin syringes (standard)
These are the most common and the basis for all conversion charts in this guide. 100 units = 1 mL. Available in 0.3 mL, 0.5 mL, and 1 mL sizes. Needle gauges range from 28G to 31G, with 30G and 31G being most comfortable for subcutaneous injection.
U-40 insulin syringes
These syringes have 40 units per 1 mL instead of 100. They are designed for veterinary insulin and U-40 insulin formulations. If you accidentally use a U-40 syringe with a U-100 conversion chart, you will inject 2.5 times more liquid than intended.
How to tell the difference: U-40 syringes typically have a red cap or red markings. U-100 syringes typically have an orange cap. Always check the syringe packaging.
Tuberculin syringes
These syringes are marked in milliliters (0.1, 0.2, 0.3 mL, etc.) rather than units. To use a tuberculin syringe, skip the unit conversion entirely and calculate your dose in milliliters instead:
mL = Desired dose in mg / Concentration in mg per mL
For a 0.5 mg dose from a 5 mg/mL vial: 0.5 / 5 = 0.1 mL. Draw to the 0.1 mL mark. No unit conversion needed.
Some people prefer tuberculin syringes specifically because they eliminate the units confusion entirely. The markings correspond directly to liquid volume, which makes the math more intuitive for many users.
Weight-based dosing considerations
Standard semaglutide dosing is not weight-based. Everyone starts at 0.25 mg regardless of body weight. However, clinical response does correlate with weight, and understanding this relationship helps set realistic expectations for appetite suppression timelines and weight loss outcomes.
In the STEP clinical trials, patients weighing over 100 kg (220 lbs) tended to need the full 2.4 mg maintenance dose for optimal results, while those under 80 kg (176 lbs) sometimes achieved their goals at 1.0 or 1.7 mg. This is not a rule, just a pattern observed across thousands of trial participants.
The practical implication for dosing in units: if you are larger, you are more likely to reach higher doses, which means higher unit counts on your syringe. Using a concentration that keeps your maintenance dose in a comfortable measurement range (20-60 units) reduces daily friction and measurement error over months of use.
For people tracking their protocol in detail, SeekPeptides offers protocol tracking tools that account for weight-based response patterns and help optimize dose timing alongside other lifestyle factors.
Timing, storage, and their effect on dosing accuracy
Dosing accuracy is not just about reading your syringe correctly. Several practical factors affect how much active semaglutide actually reaches your body.
Temperature and viscosity
Cold semaglutide solution is slightly more viscous than room-temperature solution. Drawing from a vial straight out of the refrigerator can result in tiny air bubbles that displace medication volume. The difference is small, usually less than 1 unit, but on a 5-unit dose that represents up to 20% error.
Let your vial sit at room temperature for 10 to 15 minutes before drawing. This reduces air bubbles and makes the solution flow more consistently into the syringe. Semaglutide storage temperature requirements allow brief room-temperature exposure without affecting potency.
Air bubbles in the syringe
Small air bubbles are not dangerous when injecting subcutaneously. They will not cause an air embolism at these volumes. However, a large air bubble displaces medication and reduces your actual dose.
After drawing your dose, hold the syringe tip-up and gently tap the barrel to move bubbles to the top. Push the plunger slightly to expel the air. Then verify your dose measurement. This may mean you need to draw a small additional amount to reach your target units.
Degradation over time
Compounded semaglutide in solution has a limited shelf life. Most compounding pharmacies assign a 28-day beyond-use date after the vial is first punctured. As the peptide degrades, the actual active concentration decreases even though the label concentration remains the same.
By week 4, you might be getting 85-90% of the labeled potency. This usually does not matter clinically, but it is another reason to store properly and not stretch vials beyond their labeled expiration. Using expired semaglutide amplifies this concern significantly.
Switching concentrations safely
One of the highest-risk moments in semaglutide therapy is when you switch from one concentration to another. This happens more often than people expect. Your pharmacy might change suppliers. Your provider might adjust your prescription. You might start reconstituting your own and choose a different concentration.
The critical recalculation
When your concentration changes, every single unit count in your routine must be recalculated. There are no shortcuts. Do not assume you can "adjust by feel" or "draw a little more or less."
If you were drawing 10 units of 2.5 mg/mL (0.25 mg) and switch to 5 mg/mL, your new draw is 5 units for the same dose. If you forget and draw 10 units of the new concentration, you get 0.5 mg, which is double your dose.
The safe switching protocol
Write down your current dose in milligrams (not units)
Identify your new vial concentration (check the label, not memory)
Use the formula: Units = (mg dose / new concentration) x 100
Verify by working backward: (new units / 100) x new concentration = original mg dose
Have someone else check your math if possible
This protocol takes two minutes. It can prevent weeks of side effects or reduced efficacy. Some members of the SeekPeptides community keep a concentration change log specifically for tracking these transitions.
Switching from pens to vials
If you are transitioning from an FDA-approved pen (Ozempic or Wegovy) to compounded semaglutide vials, you are making a fundamental shift in how you measure doses. With the pen, you selected milligrams. With the vial, you measure units.
Know your pen dose in milligrams. Then calculate units based on your new vial concentration. Do not try to estimate based on how far you used to turn the pen dial. The physical mechanisms are completely unrelated.
Understanding side effect profiles across formulations also matters during switches, because compounded and brand-name products may produce slightly different response patterns even at equivalent doses.
Semaglutide units for diabetes vs. weight management
Semaglutide is FDA-approved for two separate conditions with different maximum doses. Using the wrong protocol for your purpose means either underdosing or overdosing.
Type 2 diabetes (Ozempic)
Maximum dose: 2.0 mg weekly. The titration schedule is similar but tops out one step earlier. The focus is on blood sugar control, with weight loss as a secondary benefit. In compounded units at 5 mg/mL, the maximum is 40 units.
Weight management (Wegovy)
Maximum dose: 2.4 mg weekly. The higher ceiling reflects clinical trial data showing additional weight loss benefit at 2.4 mg compared to 2.0 mg. In compounded units at 5 mg/mL, the maximum is 48 units.
Oral semaglutide (Rybelsus)
Oral semaglutide uses completely different dosing. It comes in 3 mg, 7 mg, and 14 mg tablets. These milligram amounts are much higher than injectable doses because oral bioavailability is approximately 1%. The 14 mg oral dose delivers roughly the same blood levels as a 1 mg injection.
You cannot convert oral milligram doses to injectable units. They are separate formulations with separate pharmacokinetics. Oral semaglutide formulations work through entirely different absorption mechanisms.
Practical injection technique for accurate dosing
Even with perfect math, poor injection technique can waste medication or deliver it incorrectly. Here is the complete process for accurate subcutaneous semaglutide injection.
Step 1: Prepare your workspace
Clean surface. Alcohol swabs. Your syringe (unopened). Your vial at room temperature. Your dosing card or reference chart. Good lighting. These basics matter more than people think.
Step 2: Clean and prime the vial
Wipe the vial rubber stopper with an alcohol swab. Draw air into your syringe equal to your intended dose in units. Insert the needle through the stopper and push the air into the vial. This equalizes pressure and makes drawing easier.
Step 3: Draw your dose
Invert the vial (tip down). Pull the plunger slowly to your target unit marking. Draw slightly past your target, then push back to exactly the right number. This technique helps eliminate air bubbles trapped at the needle hub.
Step 4: Verify before removing
While the needle is still in the vial, check your unit reading one more time. Ensure the plunger edge aligns with your target. Tap out any visible air bubbles. Adjust if needed. Only remove the needle when you are confident in the measurement.
Step 5: Inject
Pinch a fold of skin at your injection site. The abdomen (at least 2 inches from the navel), upper thigh, or back of the upper arm are standard sites. Insert the needle at a 45 to 90 degree angle depending on needle length and body composition. Push the plunger steadily, not rapidly. Hold for 5 to 10 seconds after complete injection before withdrawing.
Rotate injection sites weekly to prevent lipodystrophy, a condition where repeated injections in the same spot cause tissue changes that affect absorption. Injection site rotation guides show the optimal pattern for consistent absorption.
Tracking your doses: why a log matters
Keeping a dose log sounds tedious. It is also the single most effective tool for catching errors before they become problems.
Record these details for every injection:
Date and time
Vial concentration
Units drawn
Calculated mg dose
Injection site used
Any side effects in the following 48 hours
This log serves multiple purposes. It creates a reference for your next injection. It documents side effect patterns that help your provider adjust dosing. It catches mistakes, because if you wrote "10 units" last week but your vial says 5 mg/mL, you can verify that 10 units = 0.5 mg and confirm that matches your prescription.
Patterns become visible over weeks. Maybe you consistently feel more nauseous when injecting in the thigh versus the abdomen. Maybe your appetite suppression fades by day 6, suggesting your dose might need adjustment. Maybe results plateau around week four, prompting a conversation with your provider about escalation timing.
SeekPeptides members use built-in tracking tools to log every injection with automatic dose verification against their prescribed protocol. This kind of systematic tracking turns guesswork into data-driven decisions.
When semaglutide units seem wrong: troubleshooting
Sometimes the math checks out but something still feels off. Here are scenarios where your calculated units might be correct on paper but wrong in practice.
You are drawing air instead of medication
If you did not inject enough air into the vial before drawing, negative pressure can pull the plunger back when you try to draw medication. The syringe barrel fills partly with air and partly with solution. Your syringe shows the right number of units, but some of those units are air, not medication.
Solution: Always inject air equal to your dose volume before drawing. If you see large bubbles after drawing, expel everything back into the vial and start over.
Your vial is nearly empty
When only a small amount of liquid remains in the vial, drawing the full dose becomes difficult. You might pull the plunger past your target and suck in air, then push back to the right number, unknowingly leaving an air pocket in the middle of the liquid column.
Solution: When less than 2 doses remain in a vial, consider starting a new vial for consistency. The small amount wasted is worth the dosing accuracy gained.
Your dose was prescribed in an unfamiliar format
Some providers prescribe in units. Others in milligrams. Others in milliliters. If you receive instructions saying "inject 0.1 mL" and your syringe is marked in units, you need to convert: 0.1 mL = 10 units on a U-100 syringe.
If instructions say "inject 0.25 mg" and your syringe shows units, you need the full formula. If instructions say "inject 10 units" and you want to verify the mg dose, multiply: (10 / 100) x concentration.
When in doubt, call your pharmacy. They can tell you exactly how many units to draw for your specific vial. This is literally their job, and a two-minute phone call is infinitely better than a dosing error. Checking expected effects at your dose level can also help you gauge whether you are getting the right amount.
Semaglutide with B12 and other additives: do units change?
Many compounded semaglutide formulations include additional ingredients like vitamin B12 (cyanocobalamin), glycine, or niacinamide. These additives affect the total solution volume but do not change how you calculate your semaglutide dose in units.
When a pharmacy compounds semaglutide at 5 mg/mL with B12, the stated concentration refers to semaglutide specifically. The B12 is dissolved in the same liquid at its own concentration. Your 10 units still delivers 0.5 mg of semaglutide regardless of the B12 content.
However, verify this with your pharmacy. Some labels state the total solute concentration rather than individual ingredient concentrations. If the label says "semaglutide 5 mg/mL + B12 1 mg/mL" then your semaglutide calculations remain standard. If the label is unclear, ask.
Semaglutide with B12 combinations have become popular because B12 may help offset the fatigue some users experience. Glycine additions aim to improve tolerability. Neither should change your unit calculations, but always confirm with the dispensing pharmacy.
Comparing semaglutide units to tirzepatide units
If you are considering switching between semaglutide and tirzepatide, or if your provider discusses both options, understanding how their unit systems relate prevents a dangerous category of confusion.
Semaglutide and tirzepatide are different molecules with different potencies. You cannot convert semaglutide units directly to tirzepatide units. The semaglutide versus tirzepatide comparison covers clinical differences in detail.
However, the mechanical process of measuring units is identical. The same formula applies:
Units = (Desired dose in mg / Concentration in mg per mL) x 100
The only things that change are the target milligrams (tirzepatide uses 2.5, 5, 7.5, 10, 12.5, and 15 mg) and the concentration of your specific vial. Tirzepatide dosage in units works on the same principles, just with different numbers.
A side-by-side dosage chart makes the comparison clearer for anyone evaluating both options.
Advanced topics for experienced users
Microdosing semaglutide in units
Some providers prescribe sub-therapeutic doses of semaglutide for specific purposes. Doses of 0.0625 mg or 0.125 mg require extremely precise measurement.
At 5 mg/mL, 0.125 mg equals just 2.5 units. At 2.5 mg/mL, it equals 5 units. Microdosing is more practical with lower concentrations where the unit count is higher and easier to measure.
For sustained low-dose protocols, reconstituting 5 mg vials with extra water to create 1 mg/mL or even 0.5 mg/mL concentration makes measurement dramatically easier. At 1 mg/mL, 0.125 mg becomes 12.5 units, which is simple to measure on a 0.3 mL syringe.
Split dosing: twice-weekly injections
Some patients split their weekly dose into two half-doses given 3 to 4 days apart. The rationale is smoother blood levels and fewer side effects.
If your weekly dose is 1.0 mg at 5 mg/mL (20 units), a split protocol would be 0.5 mg (10 units) twice per week. The total weekly milligram dose stays the same. Only the individual injection unit counts change.
Record both injections in your dose log with separate dates and unit counts to maintain accurate tracking.
Dose adjustments between standard increments
The FDA titration schedule jumps from 0.25 to 0.5 to 1.0 mg. Some providers prescribe intermediate doses like 0.375 mg or 0.75 mg to manage side effects during transitions.
At 5 mg/mL, these intermediate doses work out to:
0.375 mg = 7.5 units
0.625 mg = 12.5 units
0.75 mg = 15 units
The flexibility of unit-based dosing from vials makes these custom doses possible. It is one of the practical advantages of compounded semaglutide over fixed-dose pens. Compounded semaglutide advantages extend beyond just cost savings.
Combining semaglutide with other medications: unit independence
Semaglutide units are specific to semaglutide. If you also take insulin, another peptide, or any injectable medication, each one has its own concentration and its own unit-to-mg relationship. Never assume that units are interchangeable between medications.
Common combinations that create confusion:
Semaglutide + insulin: Insulin units ARE standardized (1 unit = a fixed biological activity). Semaglutide "units" on the syringe are just volume measurements. Do not conflate them.
Semaglutide + phentermine: Phentermine is oral and dosed in milligrams. No unit overlap possible.
Semaglutide + tirzepatide: Not typically combined, but if transitioning, never draw from the wrong vial.
Label your vials clearly. Keep different medications in separate locations if possible. The five seconds spent confirming you grabbed the right vial prevents scenarios that have landed people in emergency departments.
Resources for verifying your dose
Never rely on a single source. Cross-reference your calculated dose using multiple tools:
The semaglutide dosage calculator handles the conversion formula instantly for any concentration
The reconstitution calculator helps if you are mixing your own vials
Your pharmacy dosing card (the printed sheet that came with your vial)
Your prescribing provider or pharmacist, available by phone for dose verification
If two sources give different answers, stop. Do not inject until the discrepancy is resolved. Call your pharmacy. The most common reason for conflicting calculations is using the wrong concentration value in the formula.
Frequently asked questions
Is 10 units of semaglutide the same as 10 mg?
No. This is the most dangerous misunderstanding in semaglutide dosing. Ten units on an insulin syringe equals 0.1 mL of liquid. The milligram content depends on your concentration. At 5 mg/mL, 10 units equals 0.5 mg. At 10 mg/mL, 10 units equals 1.0 mg. Units measure volume, not drug amount. Always verify your vial concentration before calculating.
Can I use the same unit chart if my pharmacy changes my concentration?
No. If your concentration changes, every unit count must be recalculated. Using a chart for the wrong concentration is one of the most common sources of dosing errors. Always check your vial label and match it to the corresponding chart before drawing any dose.
Why does my syringe show units instead of milligrams?
Because you are using an insulin syringe, which was designed to measure insulin in standardized units. When used for semaglutide, the unit markings represent volume (0.01 mL per unit on a U-100 syringe), not a standardized drug measurement. Semaglutide is prescribed in milligrams, but the syringe only measures volume in units.
What happens if I accidentally inject too many units?
Semaglutide overdose symptoms include severe nausea, persistent vomiting, abdominal pain, and in serious cases, acute pancreatitis or severe dehydration requiring hospitalization. If you suspect you have injected too much, contact your healthcare provider or poison control immediately. Do not wait for symptoms to appear. Early intervention is always better. Understanding the full spectrum of semaglutide effects helps you distinguish between normal side effects and overdose symptoms.
Do semaglutide units work the same as insulin units?
On the syringe, yes, both use U-100 markings where 100 units equals 1 mL. But the pharmacological meaning is completely different. One "unit" of insulin has a defined biological activity. One "unit" of semaglutide on a syringe is purely a volume measurement (0.01 mL). The terms are unfortunately identical but the meanings are not.
Can I draw semaglutide and insulin in the same syringe?
No. Never mix semaglutide and insulin in the same syringe. They should be injected separately at different sites. Mixing can alter the stability and activity of both medications. Use separate syringes for each injection.
How do I know if my syringe is U-100?
Check the packaging or the syringe barrel printing. U-100 syringes will be labeled "U-100" and typically have an orange cap. The barrel will show markings up to 100 (for 1 mL) or 50 (for 0.5 mL) or 30 (for 0.3 mL). If you see markings up to 40 with a red cap, you have a U-40 syringe, which requires different calculations.
What if my prescribed dose falls between two syringe markings?
If your syringe has markings every 2 units and your dose is an odd number (like 5 or 15 units), you need to estimate the midpoint between two lines. For better precision, switch to a smaller capacity syringe with single-unit markings. A 0.3 mL syringe with 1-unit increments eliminates this problem for doses up to 30 units.
External resources
PubMed: Administration errors of compounded semaglutide reported to a poison control center
Scientific American: People are overdosing on semaglutide drugs
For researchers serious about getting their semaglutide dosing right the first time and every time after, SeekPeptides offers the most comprehensive resource available: concentration-specific calculators, protocol tracking tools, expert-verified conversion charts, and a community of thousands who have navigated these exact dosing questions.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your measurements stay precise, and your results stay consistent.