Feb 19, 2026

Everything you have read about tirzepatide and insomnia is probably wrong. Search online and you will find dozens of articles claiming this medication disrupts sleep. Forums are full of people blaming tirzepatide for their restless nights. Some even consider stopping a medication that is working brilliantly for weight loss because they cannot sleep.
Here is the truth. Tirzepatide is not listed as causing insomnia in the FDA prescribing information. The SURMOUNT and SURPASS clinical trials did not identify insomnia as a statistically significant adverse event compared to placebo. And in a twist that makes the insomnia narrative even more confusing, the FDA actually approved tirzepatide for treating obstructive sleep apnea, one of the most common sleep disorders on the planet, making it the first and only prescription medication approved for that specific indication.
So what is going on? Why do some users report fatigue during the day while others cannot fall asleep at night? The answer lies in understanding that tirzepatide does not directly cause insomnia. What it does is change your metabolism, your digestion, your hormones, and your eating patterns in ways that can indirectly disrupt sleep if you do not adapt your habits accordingly. And once you know which indirect mechanism is stealing your sleep, you can fix it. Often within days. This guide covers every documented cause of tirzepatide side effects related to sleep, the specific protocols that resolve them, and why this medication may actually improve your sleep quality over time.
Does tirzepatide actually cause insomnia? What the clinical trials show
The short answer is no. Not directly.
In the pivotal SURMOUNT-1 trial, which tested tirzepatide for weight loss in 2,539 adults without diabetes, insomnia was not reported as a common or statistically significant adverse event. The SURPASS trials for type 2 diabetes showed the same pattern. The most frequently reported side effects across all tirzepatide clinical trials are gastrointestinal, including nausea (reported in 12-29% of participants depending on dose), diarrhea (12-16%), constipation, and decreased appetite. Sleep disruption does not appear on this list.
Interestingly, fatigue and tiredness are reported far more commonly than insomnia. The medication tends to make people more drowsy, not less. This makes pharmacological sense. Tirzepatide activates GLP-1 and GIP receptors, which influence satiety, insulin secretion, and gastric motility. None of these pathways have a direct stimulatory effect on the central nervous system. The medication is not a stimulant. It does not increase adrenaline, cortisol, or any other wake-promoting neurotransmitter through its primary mechanism of action.
But real-world data tells a more nuanced story. A study analyzing social media posts about GLP-1 receptor agonists across Reddit, YouTube, and TikTok found that users mentioned sleep-related issues among their top concerns. The FDA Adverse Event Reporting System includes post-marketing reports of insomnia, anxiety, and sleep disturbance in patients taking tirzepatide. These reports exist. They are real. The question is what causes them, and the answer is almost always indirect.
Understanding this distinction matters because the treatment approach is completely different. If tirzepatide directly caused insomnia through receptor activity, you would need to either reduce the dose, change medications, or add a sleep medication.
Because the insomnia is indirect, caused by downstream effects you can control, the solutions are behavioral and nutritional rather than pharmacological. That is good news. It means you can keep taking a medication that is working effectively for weight loss while eliminating the sleep problems through targeted adjustments.
Five indirect causes of sleep problems on tirzepatide
Each of these mechanisms has a specific solution. Identifying which one, or which combination, applies to you is the first step toward sleeping well again.
Slowed gastric emptying and nighttime digestion
This is the most common culprit, and it is the one that most people miss. Tirzepatide deliberately slows gastric emptying to enhance satiety and reduce food intake. That is part of how it works for weight loss. Food stays in the stomach longer, you feel full sooner, and you eat less.
The problem is that slowed gastric emptying does not turn off when you go to bed. If you eat dinner at 7 PM and go to sleep at 10 PM, your stomach may still be actively processing that meal when you lie down. Under normal circumstances, a typical meal empties from the stomach in 2-4 hours. On tirzepatide, that timeline can extend to 4-8 hours or even longer, depending on the dose and the composition of the meal.
Active digestion prevents the body from entering deep, restorative sleep stages. Blood flow is directed to the digestive system rather than allowing the body to shift into rest-and-repair mode. Core body temperature stays elevated. The parasympathetic nervous system, which should dominate during sleep, competes with the metabolic demands of digestion. The result is lighter sleep, more frequent awakenings, and a feeling of not being rested even after spending adequate time in bed.
Users who follow a structured tirzepatide diet plan with attention to meal timing consistently report better sleep than those who eat without regard to when their last meal occurs.
Acid reflux and GERD from delayed stomach emptying
Gastroesophageal reflux disease is a documented risk with tirzepatide. A real-world study found new GERD development at a rate of 67.04 events per 1,000 person-years among tirzepatide users, compared to 51.46 in the comparison group. When food sits in the stomach longer and you lie down, the stomach contents are more likely to push back up into the esophagus.
Reflux at night is particularly disruptive to sleep. It may not always present as obvious heartburn. Sometimes it manifests as a persistent cough, a feeling of something stuck in the throat, or vague chest discomfort that makes it hard to get comfortable. Many people do not realize their sleep disruption is reflux-related because they do not experience the classic burning sensation.
The fix is the same as for slowed gastric emptying: stop eating well before bedtime. Additionally, sleeping with the head slightly elevated (4-6 inches) can reduce the frequency of nighttime reflux episodes. Avoiding specific trigger foods like spicy foods, citrus, chocolate, and high-fat meals in the evening also helps significantly.
Blood sugar fluctuations during the night
Tirzepatide improves insulin sensitivity and alters glucose metabolism. For most people, this is entirely beneficial. But the transition period, especially during the first few weeks or after dose increases, can produce blood sugar patterns that the body has not yet adapted to.
When gastric emptying is slowed, nutrients absorb gradually throughout the night rather than in the usual post-meal pattern. This creates a slow, continuous drip of glucose into the bloodstream during hours when the body expects fasting-level stability. The blood sugar may not drop dangerously low (true hypoglycemia on tirzepatide monotherapy is rare), but even mild fluctuations can trigger the sympathetic nervous system enough to cause brief awakenings.
This mechanism is more relevant for users combining tirzepatide with insulin or sulfonylureas, where the hypoglycemia risk is real and well-documented. If you are on combination therapy and experiencing nighttime awakenings with sweating, shakiness, or hunger, check your blood sugar during those episodes. This information is critical for your healthcare provider to adjust your diabetes medication doses appropriately.
For users on tirzepatide monotherapy, blood sugar related sleep disruption is usually mild and resolves as the body adapts to the new metabolic patterns, typically within 2-4 weeks of starting or increasing the dose.
Hormonal and metabolic shifts disrupting circadian rhythm
Weight loss itself changes hormones. Leptin, ghrelin, cortisol, thyroid hormones, and sex hormones all shift as body composition changes. These hormones do not just regulate appetite and metabolism. They also influence the circadian clock, the internal biological timer that determines when you feel awake and when you feel sleepy.
Tirzepatide accelerates these hormonal shifts by producing rapid weight loss. The SURMOUNT-1 trial demonstrated average weight reductions of 15-22.5% of body weight over 72 weeks. That level of change alters the hormonal landscape substantially. Leptin, which is produced by fat cells and helps regulate sleep architecture, drops as fat mass decreases. Ghrelin, which promotes wakefulness and is suppressed by tirzepatide, creates a complex interplay between appetite signaling and sleep-wake regulation.
Users tracking their tirzepatide before and after progress sometimes notice that sleep disruption coincides with periods of most rapid weight loss and then resolves as the rate of change slows. This pattern strongly suggests a hormonal adaptation mechanism rather than a direct drug effect.
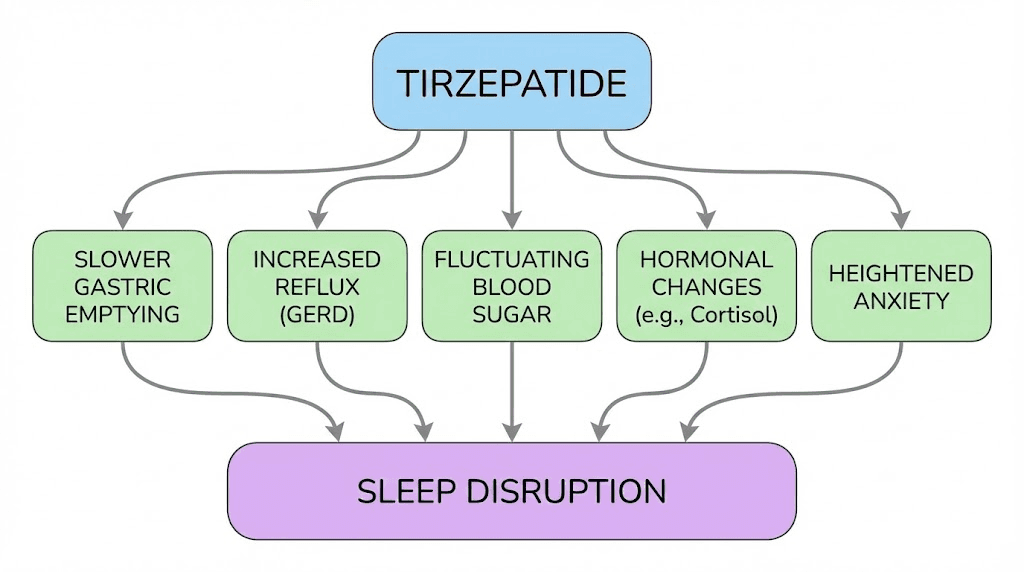
Anxiety and stress-related sleep disruption
Some users report that tirzepatide-related anxiety contributes to their sleep problems. The connection between anxiety and insomnia is well established. Racing thoughts, physical tension, and an inability to quiet the mind are classic features of anxiety-driven insomnia.
Tirzepatide may contribute to anxiety through several indirect pathways. Changes in blood sugar can trigger anxiety-like symptoms. Reduced caloric intake lowers the availability of amino acid precursors needed for serotonin and GABA production, both of which promote calm and sleep. The gastrointestinal distress that accompanies treatment can create anticipatory anxiety about nighttime symptoms. And for some users, the psychological stress of rapid body changes, medication side effects, and health-related decisions creates enough mental activation to interfere with sleep.
The distinction between medication-induced anxiety and pre-existing anxiety exacerbated by treatment is clinically important but practically less relevant for sleep management. Whether the anxiety is new or amplified, the same sleep interventions apply. Cognitive behavioral strategies, relaxation techniques, and targeted supplementation all help regardless of the anxiety source.
The paradox: tirzepatide actually improves sleep for many users
Here is where the story gets interesting. While some users struggle with insomnia, a larger number report that their sleep has dramatically improved since starting tirzepatide. The reason is weight loss, and its impact on one sleep disorder in particular.
FDA approval for obstructive sleep apnea
In December 2024, the FDA approved tirzepatide (marketed as Zepbound) for the treatment of moderate-to-severe obstructive sleep apnea in adults with obesity. This made tirzepatide the first and only prescription medication approved specifically for this indication. Obstructive sleep apnea affects an estimated 30 million Americans and is the most common cause of poor sleep quality, excessive daytime sleepiness, and nighttime awakenings in adults with obesity.
The significance of this approval cannot be overstated. The same medication that some users blame for their insomnia has been clinically proven to treat one of the most common sleep disorders. For users who had undiagnosed sleep apnea before starting tirzepatide, the weight loss from treatment may improve their sleep quality in ways they never expected.
SURMOUNT-OSA trial results
The SURMOUNT-OSA trial tested tirzepatide specifically for sleep apnea outcomes. The results were remarkable. In Study 1 (participants not using positive airway pressure therapy), tirzepatide reduced the apnea-hypopnea index by an average of 25.3 events per hour compared to 5.3 events per hour with placebo. That is a treatment difference of 20 events per hour, representing approximately a 63% reduction in sleep apnea severity.
In Study 2 (participants using PAP therapy), the results were even better, with an average AHI reduction of 29.3 events per hour versus 5.5 for placebo. Most impressively, up to 51.5% of participants met the criteria for disease resolution, meaning their sleep apnea was effectively eliminated by the weight loss alone.
These are not modest improvements. For context, the standard first-line treatment for sleep apnea (CPAP machines) typically reduces AHI by 50-70%. Tirzepatide achieved comparable results through weight loss, without requiring a machine, a mask, or nightly compliance.
Weight loss benefits for sleep quality
Even without sleep apnea, weight loss improves sleep quality through multiple mechanisms. Reduced abdominal fat decreases mechanical compression on the diaphragm, making breathing easier during sleep. Lower body weight reduces joint pain that can cause nighttime restlessness. Improved insulin sensitivity stabilizes blood sugar patterns during sleep. Reduced inflammation decreases the systemic stress signals that interfere with deep sleep.
Users who push through the initial adjustment period often find that their sleep at 3-6 months on tirzepatide is significantly better than it was before treatment. The temporary insomnia during the first few weeks is a transition cost, not a permanent feature of the medication.
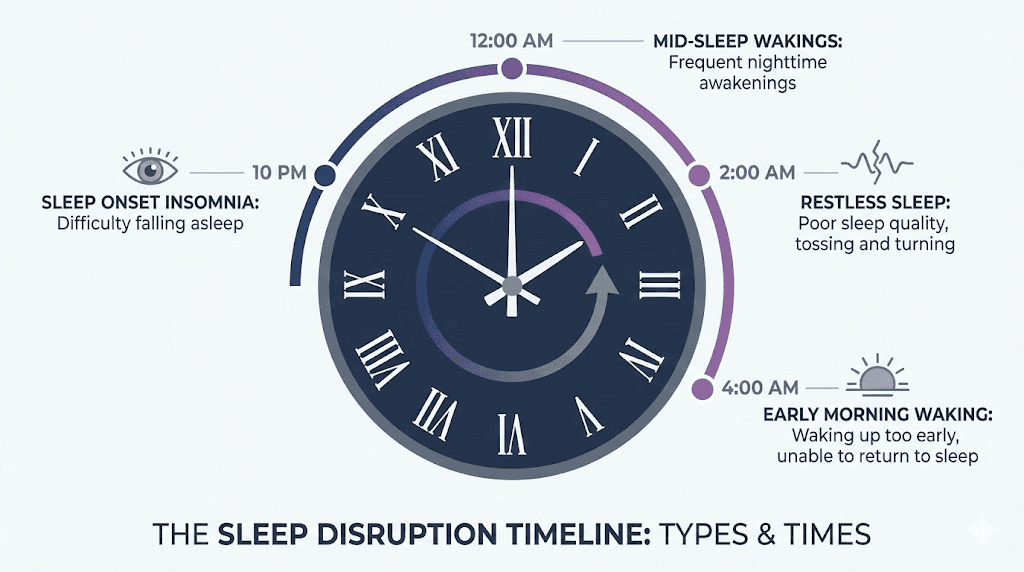
Types of sleep problems reported on tirzepatide
Not all insomnia is the same. Understanding your specific sleep pattern helps identify the cause and select the right intervention.
Difficulty falling asleep (sleep onset insomnia)
Trouble falling asleep within 20-30 minutes of lying down is the most commonly reported sleep problem on tirzepatide. It typically relates to active digestion from eating too close to bedtime, anxiety or racing thoughts from hormonal changes, or residual GI discomfort that prevents relaxation. If this is your pattern, the 3-4 hour eating rule and a structured wind-down routine are your primary tools.
Middle-of-night awakenings
Waking up between 1 AM and 4 AM and struggling to fall back asleep often points to blood sugar fluctuations or acid reflux. These awakenings may be brief (you fall back asleep within minutes) or prolonged (you lie awake for 30-60 minutes or more). Tracking whether the awakenings correlate with GI symptoms, hunger, or anxiety helps narrow the cause.
Users who experience middle-of-night awakenings with hunger pangs despite eating adequate calories during the day may benefit from a small protein-rich snack 2-3 hours before bed. Those with reflux-type awakenings should elevate the head of the bed and strictly observe the meal timing guidelines discussed later in this guide.
Light or fragmented sleep
Some users report that they fall asleep easily enough but the sleep feels shallow, unrefreshing, and fragmented. They spend adequate time in bed but wake up feeling unrested. This pattern typically relates to ongoing digestion preventing entry into deep sleep stages, undiagnosed or undertreated sleep apnea, or the metabolic transition that occurs during the first weeks of treatment.
Light sleep is particularly common during dose escalation periods. Each time the tirzepatide dose increases, the body needs to readjust to stronger appetite suppression, more pronounced gastric slowing, and faster weight loss. Sleep quality usually recovers within 1-2 weeks at each new dose.
Early morning waking
Waking up at 4-5 AM without being able to return to sleep can relate to cortisol rhythm shifts that accompany weight loss and metabolic change. Cortisol normally rises in the early morning hours to prepare the body for waking. If the cortisol curve shifts earlier due to hormonal changes from weight loss, you may find yourself wide awake before your alarm.
This pattern is usually self-limiting and resolves as the body establishes a new hormonal equilibrium. Light exposure management, consistent wake times, and avoiding caffeine after noon can help stabilize the pattern during the transition.
Vivid dreams and restlessness
A subset of users report unusually vivid dreams, increased dream recall, or restless sleep with frequent position changes. Changes in sleep architecture from the metabolic transition may alter the balance between REM (dream) sleep and non-REM deep sleep. Emerging research suggests GLP-1 receptor agonists may influence REM sleep patterns, though the evidence is preliminary.
Vivid dreams without other sleep complaints are not typically a concern unless they are distressing or associated with nighttime anxiety. If vivid dreams are accompanied by acting out dream content (kicking, punching, or yelling during sleep), discuss this with your healthcare provider as it may indicate a separate sleep disorder requiring evaluation.
Timeline: when insomnia starts and when it resolves
Sleep disruption on tirzepatide follows a predictable pattern for most users. Knowing what to expect at each stage helps you distinguish normal adjustment from a problem requiring intervention.
Week 1-2 (initiation at 2.5 mg): Sleep changes are minimal for most users at the starting dose. Some report mild difficulty falling asleep or slightly lighter sleep. Appetite suppression at 2.5 mg is modest, so the gastric emptying and dietary mechanisms are less pronounced. If sleep problems are significant at this dose, they likely relate to pre-existing factors amplified by the stress of starting a new medication.
Week 3-4 (still at 2.5 mg or escalation to 5 mg): This is when sleep disruption peaks for most users. Appetite suppression becomes more pronounced at 5 mg, gastric emptying slows further, and dietary patterns may shift significantly. Users who have not adjusted their meal timing to account for the medication effects are most likely to experience insomnia during this period.
Week 5-8 (dose escalation through 7.5 mg): Each dose increase can temporarily reintroduce sleep disruption for 7-10 days as the body adjusts to stronger effects. However, users who implemented the meal timing and sleep hygiene strategies at earlier doses typically tolerate escalation better. By this point, the body is adapting to the metabolic changes, and many users report that their sleep has actually improved compared to baseline.
Week 8-12 and beyond: Most tirzepatide-related sleep disruption has resolved by the 8-12 week mark. Users at higher doses (10-15 mg) who have addressed meal timing, GI management, and sleep hygiene typically report sleep quality that is equal to or better than pre-treatment, especially if they have lost significant weight and had any degree of sleep apnea before starting.
If insomnia persists beyond 12 weeks despite implementing all the strategies in this guide, a medical evaluation is warranted. Persistent insomnia may indicate an unrelated sleep disorder, a nutritional deficiency, or a need for protocol adjustments.
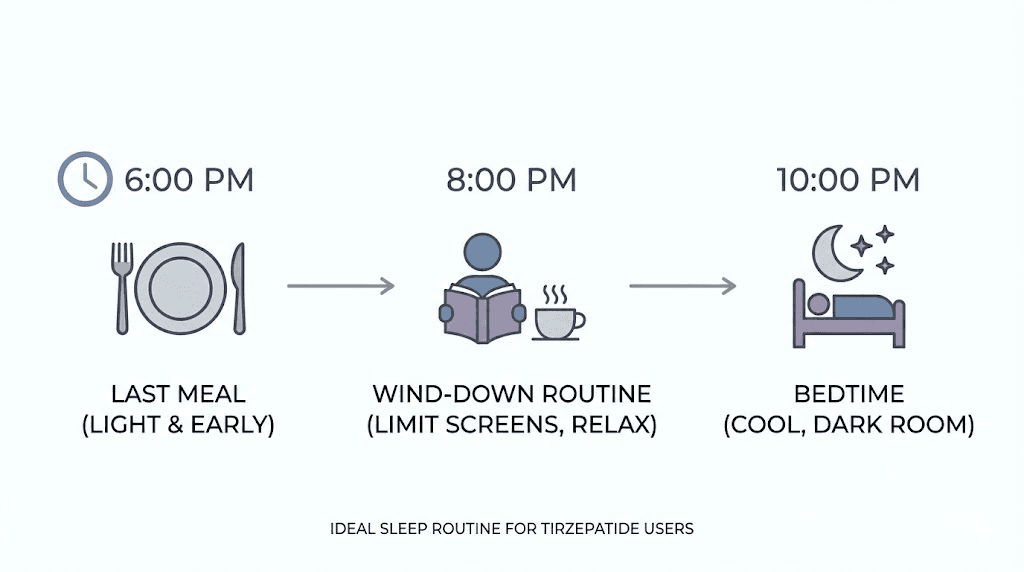
The 3-4 hour rule that fixes most tirzepatide sleep problems
If you take one thing from this entire guide, let it be this. Complete your last meal at least 3-4 hours before going to bed. This single change resolves the majority of sleep complaints from tirzepatide users.
The reasoning is straightforward. Tirzepatide slows gastric emptying significantly. A meal that would normally clear the stomach in 2-3 hours may take 5-8 hours on tirzepatide. By finishing your last meal 3-4 hours before bed, you give the digestive process a head start, reducing the likelihood that active digestion will interfere with sleep onset and deep sleep stages.
Practical timing examples:
If you sleep at 10 PM, finish your last meal by 6-7 PM
If you sleep at 11 PM, finish your last meal by 7-8 PM
If you sleep at midnight, finish your last meal by 8-9 PM
After your last meal, the only acceptable items are water, non-caffeinated herbal tea (chamomile and passionflower are excellent options), or a very small handful of berries if blood sugar maintenance requires it.
Users who implement this rule consistently report dramatic improvements, including faster sleep onset, 30-40 additional minutes of measured deep sleep per night, fewer middle-of-night awakenings, and improved morning energy levels. The improvement often appears within the first 2-3 nights, making this one of the fastest interventions available.
This approach also complements your meal planning strategy by simply shifting your eating window earlier in the day. Most tirzepatide users are already eating less food overall, so concentrating that food into an earlier window does not require eating more or changing what you eat, only when.
Complete sleep optimization protocol for tirzepatide users
Beyond the 3-4 hour eating rule, these strategies address the remaining causes of tirzepatide-related insomnia systematically.
Meal timing and composition
What you eat matters as much as when you eat. Evening meals should prioritize lean protein and non-starchy vegetables over heavy, high-fat, or spicy foods. Fat slows gastric emptying further, compounding the effect tirzepatide already has. Spicy and acidic foods increase reflux risk. Large volume meals take longer to process regardless of composition.
If your appetite only permits one substantial meal per day (which is common at higher tirzepatide doses), schedule that meal for midday rather than evening. Eating the right foods on tirzepatide becomes even more critical when sleep is affected, because every meal decision influences both nutritional status and nighttime comfort.
Keep your evening meal small and protein-forward. A 4-6 ounce portion of chicken or fish with steamed vegetables is ideal. Avoid raw salads in the evening, as the fiber content slows digestion further. Protein shakes can substitute for a solid dinner if your appetite is very low, as liquids empty from the stomach faster than solid food.
Injection timing strategy
Anecdotal reports suggest that the timing of your tirzepatide injection may influence sleep patterns, though this has not been studied formally. Some users report better sleep when they inject in the morning versus the evening. The theory is that peak medication effects, including the most pronounced gastric slowing, occur 24-72 hours post-injection. By injecting in the morning, the peak effects align more with daytime hours when active digestion is less disruptive.
If you currently inject in the evening and experience sleep problems, try switching to a morning injection for 2-3 weeks to see if the pattern changes. The best timing for GLP-1 injections remains a topic of ongoing discussion, but morning dosing is a reasonable first adjustment for sleep-affected users. You can also explore flexible injection scheduling if your routine requires adjustment.
Sleep hygiene practices
Sleep hygiene is the foundation of good sleep with or without medication. For tirzepatide users, these practices become non-negotiable rather than optional.
Consistent schedule: Go to bed and wake up at the same time every day, including weekends. Consistency trains the circadian clock and makes sleep onset predictable. A 30-minute variance is acceptable. More than that disrupts the pattern.
Light management: Get 10-15 minutes of bright natural light exposure within the first hour of waking. This resets the circadian clock and promotes appropriate melatonin release 14-16 hours later. In the evening, dim artificial lights and avoid screens for at least 30 minutes before bed. Blue light from screens suppresses melatonin production and delays sleep onset.
Caffeine cutoff: No caffeine after noon. The half-life of caffeine is 5-6 hours, meaning that half of the caffeine from a 2 PM coffee is still in your system at 8 PM. For sensitive individuals, the cutoff may need to be even earlier, at 10 AM. Caffeine combined with the metabolic changes from tirzepatide creates a compounding wakefulness effect that can be surprisingly powerful.
Temperature: Keep the bedroom at 65-68 degrees Fahrenheit (18-20 Celsius). The body needs to drop its core temperature slightly to initiate sleep. A cool room facilitates this natural process.
Evening routine design
Create a 30-60 minute wind-down routine that signals to the body and brain that sleep is approaching. The routine should be consistent, relaxing, and screen-free.
Effective wind-down activities include reading (physical book, not a screen), gentle stretching or yoga, meditation or deep breathing exercises, warm bath or shower (the subsequent cooling helps initiate sleep), journaling (particularly effective for anxiety-driven insomnia as it externalizes racing thoughts), and preparing for the next day (reduces morning-related anxiety).
Avoid stimulating activities during the wind-down period, including work emails, social media, news, intense exercise, and emotionally charged conversations. The goal is to gradually reduce sympathetic nervous system activation and allow the parasympathetic system to take over.
Supplements that help with sleep on tirzepatide
Several supplements can support sleep quality during tirzepatide treatment by addressing the specific mechanisms that cause disruption. These should complement, not replace, the behavioral strategies above.
Magnesium glycinate (200-400 mg elemental magnesium at bedtime): This is the most important sleep supplement for tirzepatide users. Magnesium promotes muscle relaxation, reduces nighttime cramping that can disrupt sleep, supports GABA receptor activity (the calming neurotransmitter), and helps regulate melatonin production. The glycinate form specifically provides the amino acid glycine as a bonus, which has its own sleep-promoting properties. Users taking a comprehensive supplement stack should ensure magnesium glycinate is included specifically at bedtime rather than earlier in the day.
Glycine (3 grams before bed): Glycine is a conditionally essential amino acid that lowers core body temperature when taken before bed, which is one of the key physiological triggers for sleep onset. Research shows that 3 grams of glycine before bed improves subjective sleep quality, reduces time to fall asleep, and decreases daytime fatigue. For tirzepatide users already taking tirzepatide compounded with glycine, the dose may already be partially covered, though evening supplementation provides additional benefit.
Melatonin (0.3-1 mg, 30-60 minutes before bed): A moderate drug interaction exists between melatonin and tirzepatide. The slowed gastric emptying may delay melatonin absorption and alter its effectiveness, with this effect most apparent at the start of treatment or after dose increases. Use the lowest effective dose (many people take far too much melatonin) and take it at the same time each night for consistency. Melatonin is most useful for circadian rhythm disruption and difficulty falling asleep, less so for middle-of-night awakenings.
L-theanine (200 mg before bed): This amino acid found in green tea promotes relaxation without sedation by increasing alpha brain wave activity. It is particularly effective for anxiety-related insomnia because it reduces mental activation without causing grogginess. L-theanine can be safely combined with magnesium glycinate and glycine.
Vitamin B12 (1000-2000 mcg methylcobalamin, morning): While not a direct sleep supplement, B12 deficiency can disrupt sleep patterns. Reduced food intake on tirzepatide increases deficiency risk. Take B12 in the morning rather than evening, as it supports energy metabolism and may be mildly stimulating for some people.
Vitamin D (2000-5000 IU, morning with food): Vitamin D receptors are present in brain regions that regulate sleep. Deficiency is linked to poor sleep quality, shorter sleep duration, and increased daytime sleepiness. Like B12, take vitamin D in the morning rather than evening, as evening supplementation has been anecdotally associated with disrupted sleep in some individuals.
Sleep problems at different tirzepatide dose levels
Sleep disruption risk varies by dose, primarily because higher doses produce more aggressive appetite suppression and gastric slowing.
2.5 mg (starting dose): Sleep problems are uncommon at this level. The gastric slowing effect is modest, and appetite suppression is mild. If significant insomnia occurs at 2.5 mg, other factors (stress, pre-existing sleep issues, caffeine, screen habits) are more likely responsible than the medication itself.
5 mg (first therapeutic dose): This is where sleep disruption most commonly begins. The jump from 2.5 mg to 5 mg significantly increases appetite suppression and gastric emptying delay. Users who do not adjust their meal timing at this dose are the most likely to develop insomnia. Implementing the 3-4 hour eating rule proactively before escalating to 5 mg can prevent sleep problems from developing.
7.5-10 mg: Users who managed sleep well at lower doses typically continue to sleep well at these levels. New sleep problems at 7.5-10 mg often relate to the accelerated weight loss and hormonal changes rather than increased GI effects, which the body has usually adapted to by this point. Microdosing approaches with slower escalation can reduce the sleep impact of dose transitions.
12.5-15 mg (maximum doses): At maximum doses, the side effect profile is well-established for each individual. Sleep quality at these doses is often significantly better than at treatment initiation because substantial weight loss has occurred, potentially resolving sleep apnea and reducing the mechanical factors that interfere with breathing and comfort during sleep.
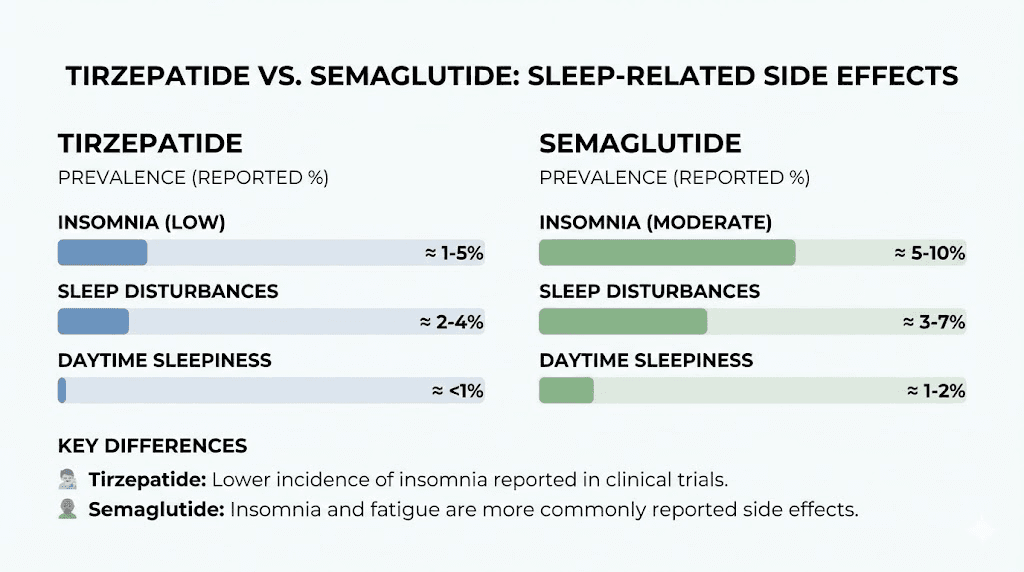
Tirzepatide insomnia versus semaglutide insomnia
Users comparing semaglutide and tirzepatide often ask whether one medication causes more sleep problems than the other. The answer is nuanced.
Neither medication lists insomnia as a common side effect. Both produce similar indirect mechanisms for sleep disruption through appetite suppression, gastric slowing, and metabolic changes. The key difference is that tirzepatide generally produces more weight loss, more quickly, which means the adjustment period may be more pronounced but the long-term sleep benefits (from greater weight loss and sleep apnea improvement) may also be greater.
Semaglutide is more commonly associated with fatigue than insomnia, while tirzepatide user communities report a slightly higher incidence of sleep disruption. This difference may relate to the dual GIP/GLP-1 mechanism of tirzepatide versus the GLP-1-only action of semaglutide, though this is speculative.
If sleep problems are severe on one medication and do not respond to the behavioral interventions in this guide, switching to the other is a reasonable discussion to have with your healthcare provider. The conversion chart between medications helps maintain therapeutic effect during the transition. Users who experience different side effect profiles on each medication often find that one suits their body chemistry better than the other.
When sleep problems require medical attention
Most tirzepatide-related sleep disruption resolves with the behavioral and supplemental interventions described above. However, certain patterns warrant professional evaluation.
Persistent insomnia beyond 4-6 weeks despite implementing all strategies in this guide suggests either an unrelated sleep disorder or a contributing factor that has not been identified. Sleep disorders like restless legs syndrome, periodic limb movement disorder, and circadian rhythm disorders can coexist with tirzepatide treatment and require separate diagnosis and management.
Loud snoring, gasping, or witnessed breathing pauses during sleep may indicate obstructive sleep apnea. While tirzepatide is FDA-approved to treat this condition through weight loss, users early in their treatment may not yet have lost enough weight for the benefit. A sleep study can determine if sleep apnea is contributing to poor sleep quality and whether temporary CPAP therapy is appropriate during the weight loss period.
Severe anxiety, panic attacks, or depressive symptoms accompanying insomnia require prompt evaluation. While mild anxiety is a recognized indirect effect of tirzepatide, severe mental health symptoms warrant a comprehensive assessment and potentially a referral to a psychiatrist who can evaluate the interaction between the medication and mental health.
Daytime impairment from sleep deprivation that affects work performance, driving safety, or daily functioning should not be tolerated as a medication side effect. If sleep loss is severe enough to impair your ability to function safely during the day, contact your healthcare provider. Short-term sleep medication may be appropriate while longer-term solutions are implemented.
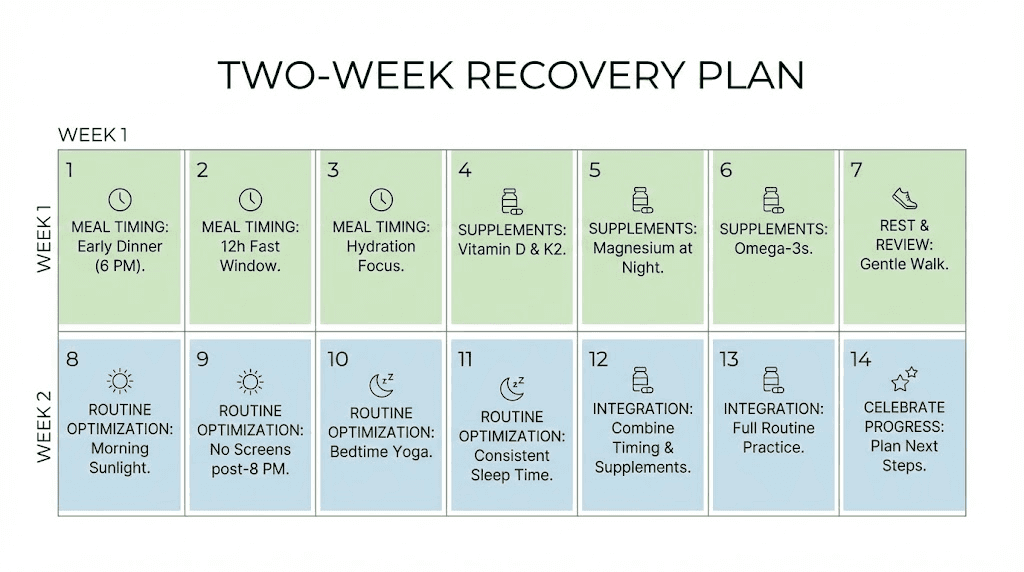
Your 2-week sleep recovery plan
If insomnia is currently affecting your tirzepatide experience, this structured plan systematically addresses the most common causes in order of impact and ease of implementation.
Days 1-3: the eating window shift
Goal: Eliminate the most common cause of tirzepatide insomnia.
Calculate your ideal last-meal time (bedtime minus 4 hours)
Complete all eating before this cutoff starting tonight
After cutoff: only water, herbal tea, or a small handful of berries
Track sleep onset time and any nighttime awakenings in a simple log
Many users notice improvement within the first 1-2 nights. If your insomnia was primarily caused by nighttime digestion, this alone may resolve it.
Days 4-7: supplements and environment
Goal: Add physiological support for sleep quality.
Begin magnesium glycinate (200-400 mg) at bedtime
Add 3 grams of glycine 30 minutes before bed
Set bedroom temperature to 65-68 degrees
Remove or cover all light sources in the bedroom
Stop all caffeine after noon (or 10 AM if sensitive)
Continue tracking sleep quality
Days 8-10: routine and rhythm
Goal: Establish circadian rhythm consistency.
Set a fixed wake time and stick to it every day, including weekends
Get 10-15 minutes of bright light within the first hour of waking
Create a 30-minute screen-free wind-down routine before bed
If you inject in the evening, switch to morning injection
Dim lights in the house 1-2 hours before bedtime
Days 11-14: evaluation and adjustment
Goal: Assess progress and fine-tune.
Review your 2-week sleep log for patterns
If sleep onset improved but you still wake at night, focus on reflux management (elevate head of bed, avoid evening trigger foods)
If anxiety is the remaining issue, add 200 mg L-theanine to your evening supplement stack
If no improvement after the full 2 weeks, schedule a healthcare provider appointment to discuss further options
Users who want comprehensive tracking throughout this process can leverage the tools available through SeekPeptides, which provides detailed protocol guides, dosing calculators, and community support from researchers who have navigated these exact challenges.
Frequently asked questions
Does tirzepatide directly cause insomnia?
No. Insomnia is not listed in the FDA prescribing information for tirzepatide and was not identified as a statistically significant adverse event in clinical trials. Sleep problems on tirzepatide are caused by indirect effects including slowed gastric emptying, acid reflux, blood sugar fluctuations, and hormonal changes from weight loss. These indirect causes are addressable through meal timing, sleep hygiene, and targeted supplementation.
What is the fastest way to fix tirzepatide insomnia?
Stop eating at least 3-4 hours before bedtime. This single change resolves the majority of tirzepatide-related sleep problems because it addresses the nighttime digestion issue caused by slowed gastric emptying. Most users notice improvement within 1-3 nights. Add magnesium glycinate at bedtime for additional benefit.
Can I take melatonin with tirzepatide?
Yes, though a moderate interaction exists. Tirzepatide slowed gastric emptying may delay melatonin absorption, making it less effective at the start of treatment or after dose increases. Use the lowest effective dose (0.3-1 mg) taken 30-60 minutes before bed. Consult your healthcare provider if you take other medications alongside both tirzepatide and melatonin.
Will tirzepatide insomnia go away on its own?
For most users, yes. Sleep disruption on tirzepatide typically appears during the first 2-4 weeks or after dose increases and resolves as the body adapts. Proactively implementing the 3-4 hour eating rule and sleep hygiene practices accelerates this resolution. If insomnia persists beyond 6 weeks despite interventions, consult your healthcare provider.
Is tirzepatide insomnia worse at higher doses?
Not necessarily. Each dose increase may temporarily reintroduce mild sleep disruption as the body adjusts, but users who have established good meal timing and sleep habits at lower doses typically tolerate escalation well. Sleep quality at higher doses is often better than at lower doses because more significant weight loss has occurred, potentially improving conditions like overall treatment response and sleep apnea.
Should I take tirzepatide in the morning or evening for better sleep?
Morning injection is generally preferred for users experiencing sleep problems. While injection timing has not been formally studied in relation to sleep, morning dosing aligns peak medication effects with daytime hours when active digestion is less disruptive to sleep. This is worth trying for 2-3 weeks if you currently inject in the evening and experience insomnia.
Can I switch to semaglutide if tirzepatide insomnia does not resolve?
This is a reasonable option to discuss with your healthcare provider if behavioral and supplemental interventions do not resolve your sleep problems. Some users tolerate one medication better than the other. Our guide to switching from tirzepatide to semaglutide covers the transition process, and the conversion chart helps maintain therapeutic dosing during the switch.
Does tirzepatide help with sleep apnea?
Yes. Tirzepatide is FDA-approved for treating moderate-to-severe obstructive sleep apnea in adults with obesity. The SURMOUNT-OSA trial showed a 63% reduction in sleep apnea severity, and up to 51.5% of participants achieved disease resolution. This makes tirzepatide paradoxically both a reported cause of short-term insomnia and a proven treatment for one of the most common long-term sleep disorders.
External resources
FDA Prescribing Information for Zepbound (tirzepatide) including OSA indication
SURMOUNT-OSA Trial Results (New England Journal of Medicine)
For researchers serious about optimizing every aspect of their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides covering side effect management, dosing optimization, and community support from thousands of experienced researchers. SeekPeptides members access detailed protocol builders and personalized guidance that address the real-world challenges of GLP-1 therapy, including exactly the kind of sleep optimization covered in this guide.
In case I do not see you, good afternoon, good evening, and good night. May your evenings stay peaceful, your sleep stay deep, and your mornings stay rested.