Feb 6, 2026

You have been following the protocol perfectly. The dosing is precise. Your injections go smoothly every week. Yet the fatigue hits hard, the nausea lingers longer than expected, and you wonder if something is missing from your approach.
The missing piece might be vitamin b12.
Compounded semaglutide with b12 has become increasingly common in weight loss clinics and compounding pharmacies across the country. The combination sounds promising. Add a vitamin known for energy support to a medication proven for weight loss. But the reality is more complex than marketing materials suggest, and the research tells a different story than many providers claim.
This guide examines what actually happens when you combine semaglutide with vitamin b12. We will explore the limited research available, analyze the theoretical benefits against the evidence, review proper dosing protocols for those who choose this approach, and help you determine whether adding b12 to your semaglutide protocol makes sense for your specific situation. The answer depends on factors most guides completely ignore.
Understanding semaglutide mechanisms and vitamin b12 relationship
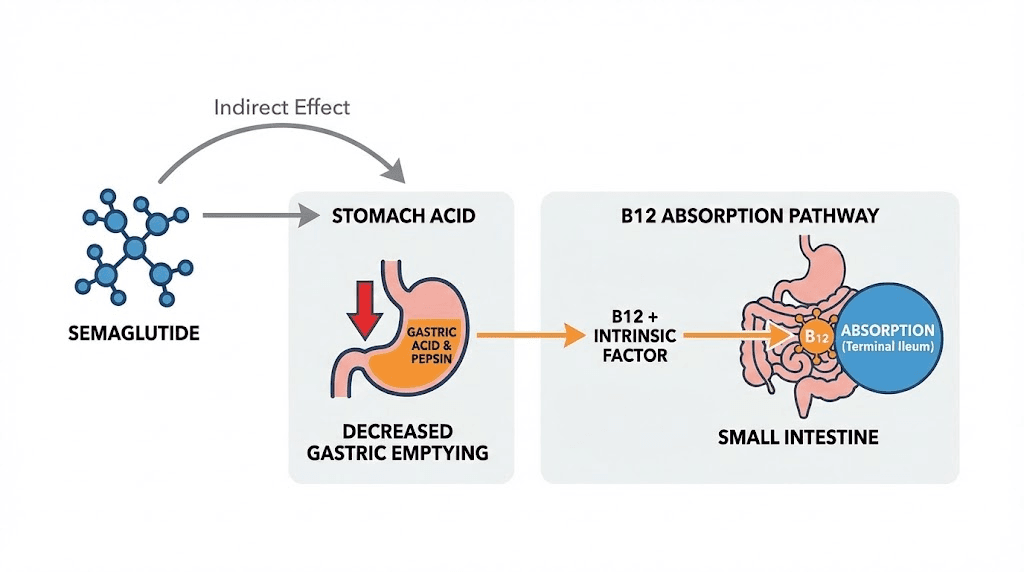
Semaglutide operates through glucagon-like peptide-1 receptor activation. The medication slows gastric emptying significantly.
This mechanism matters for b12 absorption. Semaglutide reduces stomach acid production as a secondary effect of delayed gastric emptying. Stomach acid plays a critical role in separating vitamin b12 from dietary proteins, the first step in b12 absorption. Without adequate stomach acid, b12 remains bound to food proteins and passes through the digestive system unabsorbed.
The intrinsic factor complication adds another layer. Intrinsic factor, produced by parietal cells in the stomach lining, binds to free b12 and enables absorption in the terminal ileum. Semaglutide does not directly affect intrinsic factor production, but the reduced stomach acid environment can compromise the initial separation step that makes b12 available for intrinsic factor binding.
Research on this connection remains limited. One study examining patients who had undergone bariatric surgery and subsequently used semaglutide found mean vitamin b12 levels decreased from 567 to 494 mcg per deciliter over 12 months. This represents a statistically significant drop. However, these patients had multiple risk factors for b12 deficiency beyond semaglutide use, including previous gastric surgery that permanently alters stomach anatomy and reduces intrinsic factor production.
Isolating semaglutide as the sole cause proves difficult. Patients using semaglutide typically reduce caloric intake by 20 to 40 percent, often cutting back on b12-rich foods like meat, fish, eggs, and dairy products. The medication itself causes appetite suppression that makes eating these nutrient-dense foods less appealing. This dietary pattern change may contribute to declining b12 levels as much as or more than any absorption issue.
The false-low b12 phenomenon complicates assessment further. Some research indicates semaglutide associates with laboratory results showing low b12 levels that do not reflect actual tissue deficiency. The mechanism behind this laboratory artifact remains unclear, but it means some patients may receive unnecessary b12 supplementation based on misleading test results.
Vitamin b12 exists in multiple forms. Cyanocobalamin represents the synthetic form most commonly used in supplements and compounded formulations.
The body must convert cyanocobalamin through several steps before it becomes biologically active. Methylcobalamin and adenosylcobalamin represent the two active forms that participate directly in cellular metabolism.
Methylcobalamin serves as a cofactor for methionine synthase, an enzyme critical for DNA synthesis, neurotransmitter production, and homocysteine metabolism. When methylcobalamin levels drop, homocysteine accumulates, potentially increasing cardiovascular risk. Neurological function depends heavily on adequate methylcobalamin for myelin sheath maintenance and neurotransmitter synthesis.
Adenosylcobalamin functions in mitochondria as a cofactor for methylmalonyl-CoA mutase. This enzyme participates in fatty acid and amino acid metabolism. Deficiency leads to methylmalonic acid accumulation, which can cause neurological damage over time. Energy production suffers when adenosylcobalamin levels fall below optimal ranges.
The conversion from cyanocobalamin to active forms requires several enzymatic steps and adequate amounts of other nutrients including folate, riboflavin, and various minerals. Some individuals carry genetic variations that reduce conversion efficiency. These people may need direct supplementation with methylcobalamin or adenosylcobalamin rather than cyanocobalamin.
Compounding pharmacies typically use cyanocobalamin when creating semaglutide with b12 formulations. This choice reflects cost and stability considerations rather than optimal bioavailability. Cyanocobalamin remains stable in solution longer than methylcobalamin, simplifying storage and extending shelf life. The cost differential can be substantial, with cyanocobalamin costing roughly one-tenth the price of methylcobalamin in pharmaceutical quantities.
Research evidence on semaglutide and b12 combination therapy
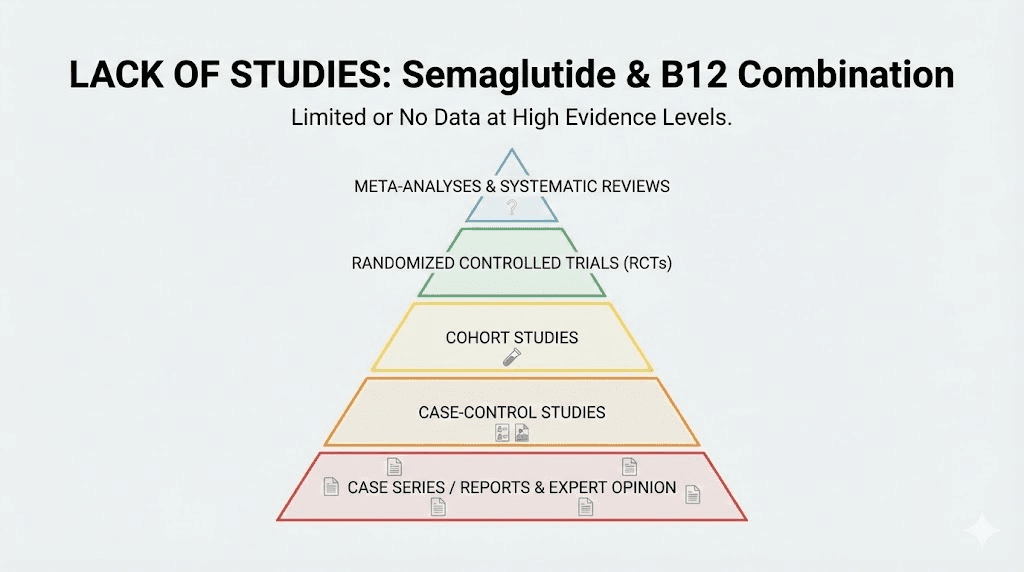
No published studies have examined semaglutide with b12 as a combined formulation. This absence of research represents a critical gap.
The compounded combinations available through various pharmacies lack FDA approval. The FDA has not reviewed safety data, efficacy data, or quality control standards for these mixed formulations. Each compounding pharmacy creates its own protocol without standardized ratios, concentrations, or quality assurance processes beyond state board requirements.
Clinical trials of brand-name semaglutide products like Wegovy and Ozempic did not include b12 supplementation as part of the study protocols. These trials tracked numerous safety parameters and laboratory values, but vitamin b12 levels were not routinely monitored or reported in the published results. The lack of monitoring means we cannot determine from existing clinical trial data whether semaglutide causes clinically significant b12 deficiency in typical patients.
The single study showing decreased b12 levels involved a specific high-risk population. Patients had undergone laparoscopic sleeve gastrectomy before starting semaglutide. Bariatric surgery permanently reduces stomach size and removes portions of the stomach that produce intrinsic factor. These patients face elevated b12 deficiency risk regardless of medication use.
Standard practice after bariatric surgery includes routine b12 monitoring and supplementation. The addition of semaglutide to this already high-risk group showed further b12 decline, but whether this represents a medication effect, dietary changes from additional appetite suppression, or natural progression of post-surgical deficiency remains unclear. The study design did not include a control group of post-bariatric patients not using semaglutide for comparison.
Other GLP-1 receptor agonists have undergone more extensive b12 research. Metformin, though not a GLP-1 agonist, shares the property of reducing stomach acid and interfering with b12 absorption. Long-term metformin use clearly associates with increased b12 deficiency rates. Studies consistently show 10 to 30 percent of metformin users develop low b12 levels over years of use.
The metformin research suggests plausibility for similar effects with semaglutide, but the mechanisms differ enough that direct extrapolation remains uncertain. Metformin affects b12 absorption through multiple pathways including interference with calcium-dependent membrane binding in the ileum. Semaglutide primarily affects the earlier step of acid-dependent separation from dietary proteins.
Liraglutide, another GLP-1 receptor agonist with a longer track record than semaglutide, has not generated significant reports of b12 deficiency in clinical practice. Post-marketing surveillance data spanning millions of patient-years does not show elevated rates of documented b12 deficiency among liraglutide users compared to general population rates. This suggests that GLP-1 receptor activation alone may not substantially increase deficiency risk.
The theoretical mechanism for concern exists. The practical evidence remains limited.
This gap between theory and data creates the environment where compounded combinations proliferate without solid scientific foundation.
Claimed benefits of adding b12 to semaglutide protocols
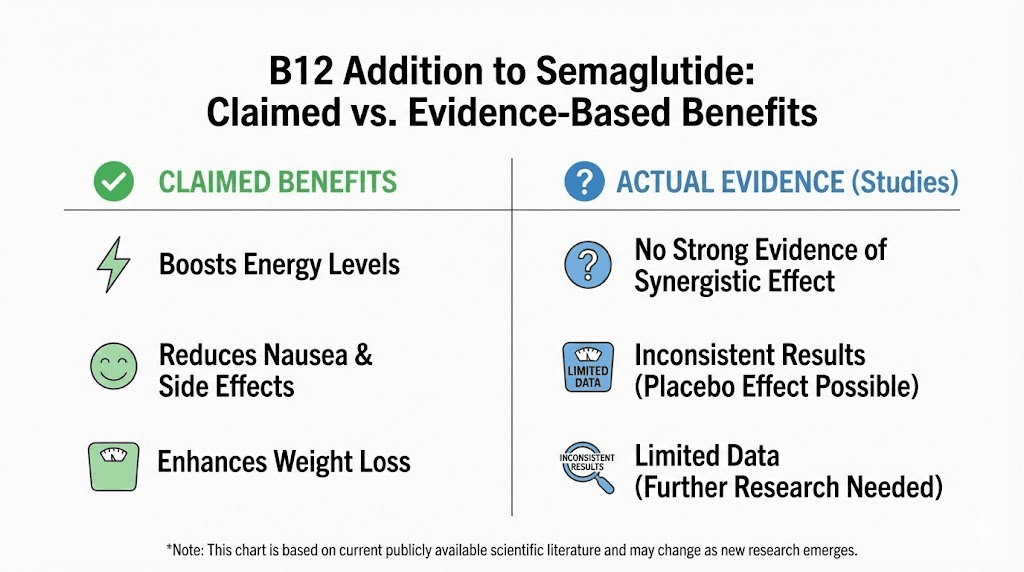
Providers and compounding pharmacies market several benefits when promoting semaglutide with b12 combinations. Each claim deserves scrutiny.
Energy support and fatigue reduction
Vitamin b12 plays essential roles in energy metabolism. The claim makes biological sense. Fatigue represents one of the most commonly reported side effects during semaglutide use, particularly in the first 4 to 8 weeks of treatment.
But attributing this fatigue to b12 deficiency requires evidence that deficiency has actually developed. The timeline does not support this mechanism. Vitamin b12 stores in the liver typically last 3 to 5 years. Someone starting semaglutide with normal b12 stores would not develop true deficiency-related fatigue within weeks or even months.
The fatigue during early semaglutide use more likely results from caloric restriction, changes in eating patterns, and the medication adjusting appetite and satiety signals. Patients often reduce caloric intake by 500 to 1000 calories daily. This energy deficit naturally causes fatigue as the body adapts.
Some patients report improved energy after adding b12 injections to their protocol. This subjective improvement could reflect placebo effect, improved overall nutritional status from paying more attention to diet, natural adaptation to the medication over time, or actual b12 repletion if deficiency existed. Separating these possibilities without controlled studies remains impossible.
The route of administration matters. Injectable b12 bypasses all absorption issues, providing 100 percent bioavailability regardless of stomach acid levels or intrinsic factor status. This makes injectable supplementation a reasonable approach for anyone with confirmed or suspected absorption problems, though it does not prove the combination provides benefits beyond separate administration.
Nausea management
Marketing materials frequently claim b12 reduces nausea associated with semaglutide use. This claim lacks supporting evidence.
Vitamin b12 does not have established anti-nausea properties in medical literature. The vitamin does not interact with serotonin receptors, dopamine receptors, or other pathways targeted by proven anti-nausea medications. No mechanism of action explains how b12 would reduce nausea caused by delayed gastric emptying.
Clinical experience with b12 injections for other indications does not include nausea reduction as a known effect. Patients receiving b12 for pernicious anemia, neurological conditions, or documented deficiency do not report nausea improvement unless their nausea stemmed from the deficiency itself.
The timing further undermines this claim. Semaglutide-related nausea typically peaks 24 to 48 hours after injection and gradually improves over the following days. If b12 provided acute anti-nausea effects, we would expect immediate relief after b12 injection. Patient reports do not consistently show this pattern.
Better nausea management strategies have proven effectiveness. Eating smaller meals, avoiding high-fat foods, staying hydrated, and dosing escalation protocols all reduce nausea rates in clinical trials and practice. These approaches address the actual mechanism causing nausea rather than adding unrelated compounds.
Enhanced fat metabolism
The claim that b12 enhances fat metabolism during weight loss oversimplifies b12's metabolic roles. Adenosylcobalamin does participate in fatty acid metabolism through methylmalonyl-CoA mutase. This enzyme processes odd-chain fatty acids and certain amino acids.
Humans consume and metabolize primarily even-chain fatty acids. Odd-chain fatty acids represent a small fraction of dietary fat intake. The methylmalonyl-CoA mutase pathway processes only this minor component of overall fat metabolism. Even with b12 deficiency, this pathway continues functioning at reduced efficiency rather than stopping completely.
Semaglutide drives weight loss through appetite suppression and reduced caloric intake, not through enhanced fat oxidation. The medication does not directly increase metabolic rate or preferentially promote fat burning. Weight loss occurs because people eat less, creating an energy deficit that forces the body to use stored fat.
Adding b12 does not change this fundamental mechanism. No evidence suggests that optimizing b12 status accelerates weight loss beyond what would occur with adequate nutrition overall. The focus on b12 specifically appears to be marketing rather than science.
Muscle preservation
Some formulations include glycine along with b12, claiming this combination preserves muscle mass during weight loss. This claim conflates several different mechanisms and ingredients.
Glycine, an amino acid, may support muscle protein synthesis when combined with adequate protein intake and resistance training. Research on glycine supplementation shows modest benefits for collagen synthesis and some metabolic parameters. These effects have nothing to do with b12.
Vitamin b12 supports overall protein metabolism but does not preferentially preserve muscle. Muscle preservation during weight loss depends primarily on protein intake (typically 1.2 to 1.6 grams per kilogram body weight), resistance training, and the rate of weight loss. Slower weight loss with adequate protein and exercise preserves muscle more effectively than any vitamin supplementation.
The real concern about muscle loss during semaglutide use stems from very rapid weight loss in some patients. Losing 2 to 3 pounds per week or more increases the proportion of lean mass lost alongside fat. This has nothing to do with b12 status and everything to do with excessive caloric deficit and insufficient protein intake relative to the rate of weight change.
Who actually needs b12 supplementation during semaglutide use
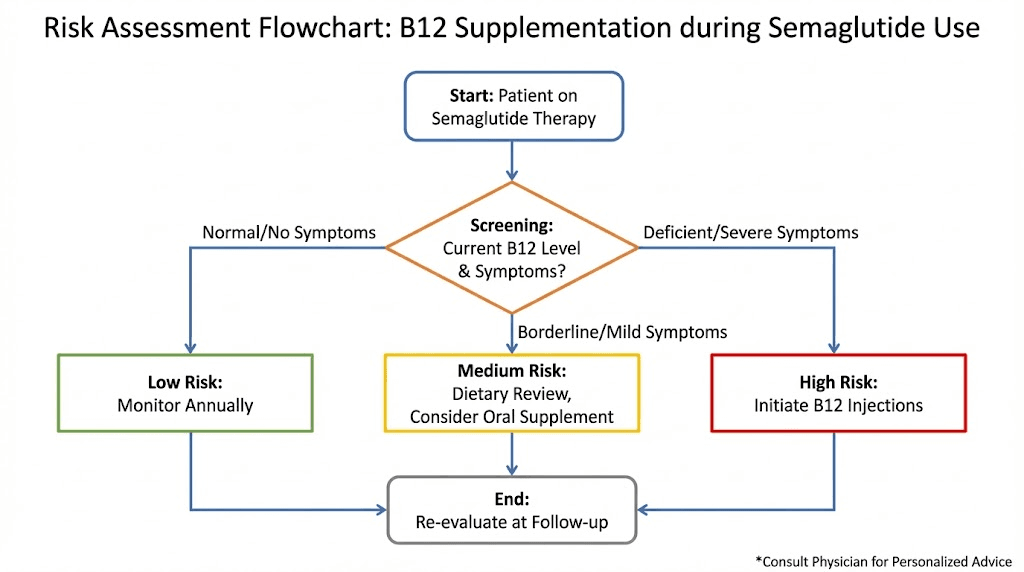
Not everyone using semaglutide requires b12 supplementation. Risk factors determine who benefits.
Pre-existing b12 deficiency or low-normal levels
Anyone starting semaglutide with documented b12 deficiency or levels in the low-normal range (200 to 400 pg per milliliter) should receive supplementation. These individuals lack adequate stores to sustain them through months of potentially reduced absorption and dietary intake.
Testing b12 levels before starting semaglutide provides a baseline. This simple blood test costs $20 to $50 and gives clear information about whether supplementation makes sense from the start. Many patients have undiagnosed low b12 even before medication use, particularly among certain risk groups.
Previous bariatric surgery
Patients with any history of gastric bypass, sleeve gastrectomy, or other bariatric procedures require lifelong b12 monitoring and supplementation. The surgical alterations permanently compromise b12 absorption through multiple mechanisms. Adding semaglutide to this situation creates a double hit on absorption capacity.
These patients should use b12 supplementation regardless of whether their semaglutide formulation includes it. The doses in compounded combinations may not provide adequate amounts for someone with surgical absorption limitations. Separate high-dose oral b12 (1000 to 2000 mcg daily) or regular b12 injections (1000 mcg weekly or monthly) offer more reliable repletion.
Vegetarian and vegan diets
Vitamin b12 comes almost exclusively from animal products. Vegetarians who consume eggs and dairy may get adequate amounts. Vegans have no reliable dietary b12 sources unless they consume fortified foods or supplements.
Vegans using semaglutide face a challenging combination. They already have minimal b12 intake. The medication may further reduce absorption of the small amounts obtained from fortified foods. These patients need b12 supplementation as a baseline requirement, separate from any theoretical benefits of combination products.
Advanced age over 60
Stomach acid production naturally declines with age. By age 60, approximately 10 to 30 percent of people have reduced acid output. This condition, called hypochlorhydria or achlorhydria when severe, impairs b12 absorption even without medication effects.
Older adults using semaglutide combine age-related absorption decline with medication effects that may further reduce acid production. These patients warrant either baseline supplementation or at minimum testing b12 levels every 6 to 12 months during treatment to catch declining levels before deficiency develops.
Prolonged use beyond 12 months
Short-term semaglutide use of several months likely does not deplete b12 stores in people who start with adequate levels. The liver stores 3 to 5 years worth of b12 under normal circumstances.
However, prolonged use of a year or more combined with reduced dietary intake could gradually deplete these stores. Patients planning long-term or indefinite semaglutide use should consider periodic b12 testing and supplementation if levels drop below optimal ranges. This represents a precautionary approach rather than a requirement based on proven deficiency risk.
Concurrent use of medications that affect b12 absorption
Several common medications interfere with b12 absorption through various mechanisms. Metformin tops this list, with well-documented effects on b12 levels. Proton pump inhibitors like omeprazole reduce stomach acid dramatically. H2 blockers like ranitidine have similar but less severe effects.
Patients taking any of these medications along with semaglutide experience multiple simultaneous hits to b12 absorption. These individuals need supplementation and regular monitoring to prevent deficiency from developing over months to years of treatment.
Proper dosing protocols for b12 supplementation with semaglutide
When supplementation makes sense, proper dosing depends on the form used and the individual situation.
Injectable methylcobalamin dosing
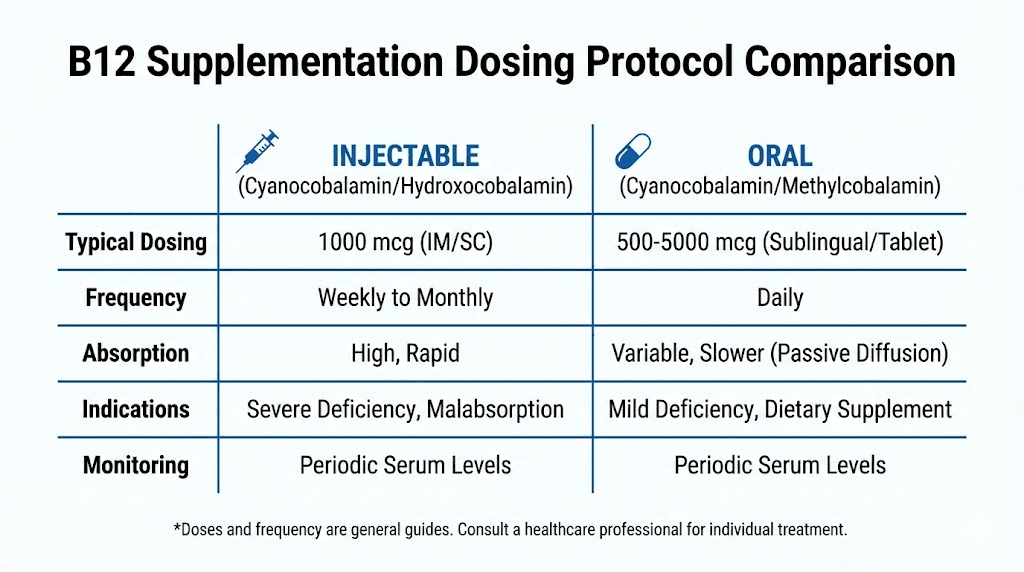
Injectable b12 provides the most reliable absorption. This route bypasses all gastrointestinal issues. Methylcobalamin represents the preferred form for injection due to immediate bioavailability without requiring metabolic conversion.
Standard maintenance dosing ranges from 1000 mcg weekly to 1000 mcg monthly. The wide range reflects individual variation in requirements and the difficulty of over-dosing b12. The vitamin has extremely low toxicity. Excess amounts excrete through urine without causing harm.
For documented deficiency, loading doses of 1000 mcg daily or several times weekly for 1 to 2 weeks rapidly restore tissue levels. After loading, transition to maintenance dosing of 1000 mcg every 1 to 4 weeks depending on response and follow-up testing.
The injection can occur intramuscularly or subcutaneously. Subcutaneous administration works well for self-injection, using the same techniques employed for semaglutide. The insulin syringe approach familiar to semaglutide users applies equally well to b12 injections.
When using compounded semaglutide with b12, the b12 dose varies by pharmacy. Common formulations include 0.5 to 1.0 mg (500 to 1000 mcg) b12 per semaglutide dose. This provides weekly b12 supplementation when semaglutide is dosed weekly. The convenience of a single injection appeals to many patients.
High-dose oral b12 protocols
Oral b12 can overcome absorption issues through mass action. Taking 1000 to 2000 mcg orally daily allows approximately 1 to 3 percent passive absorption even without intrinsic factor. This small percentage provides adequate amounts when the dose is sufficiently high.
Sublingual and oral forms show similar absorption in most research. The sublingual myth persists but lacks solid evidence. B12 tablets dissolve in saliva and get swallowed, entering the same absorption pathways as regular oral supplements. The minor benefits of sublingual administration do not justify the typically higher cost.
Cyanocobalamin costs less than methylcobalamin for oral supplementation. Either form works for most people. Those with certain genetic variations affecting b12 metabolism may benefit from methylcobalamin specifically. Testing MTHFR and other relevant genetic markers can identify these individuals, though routine genetic testing for b12 supplementation decisions remains controversial.
Timing oral b12 does not matter significantly. Take it whenever convenient. Consistency matters more than optimal timing. Daily supplementation provides steady tissue levels.
Monitoring and adjusting supplementation
Test b12 levels every 6 to 12 months during semaglutide use. This interval catches declining levels before symptoms develop. Testing costs remain modest and provide valuable guidance for adjusting supplementation.
Target levels above 400 pg per milliliter. Some practitioners aim for 600 to 800 pg per milliliter as optimal. No clear evidence defines the ideal level within the normal range. Higher within normal appears safe and may provide margin against future decline.
Methylmalonic acid and homocysteine testing provide functional assessment of b12 status. These metabolites accumulate when b12 function becomes inadequate, sometimes before serum b12 drops below normal range. Elevated methylmalonic acid or homocysteine with normal-ish b12 suggests functional deficiency requiring supplementation.
Adjust doses based on testing results and symptoms. If levels remain low despite supplementation, increase the dose or frequency. If levels climb high into normal range and symptoms resolve, continue the current protocol. Individual variation in requirements and absorption means no single protocol fits everyone.
Comparing standalone supplementation versus compounded combinations
The choice between taking separate b12 supplements and using compounded semaglutide with b12 involves several tradeoffs.
Compounded combinations offer convenience. One injection instead of two. This simplicity appeals to people who dislike injections or want to minimize complexity in their protocol. The single injection ensures b12 administration occurs regularly as long as semaglutide continues.
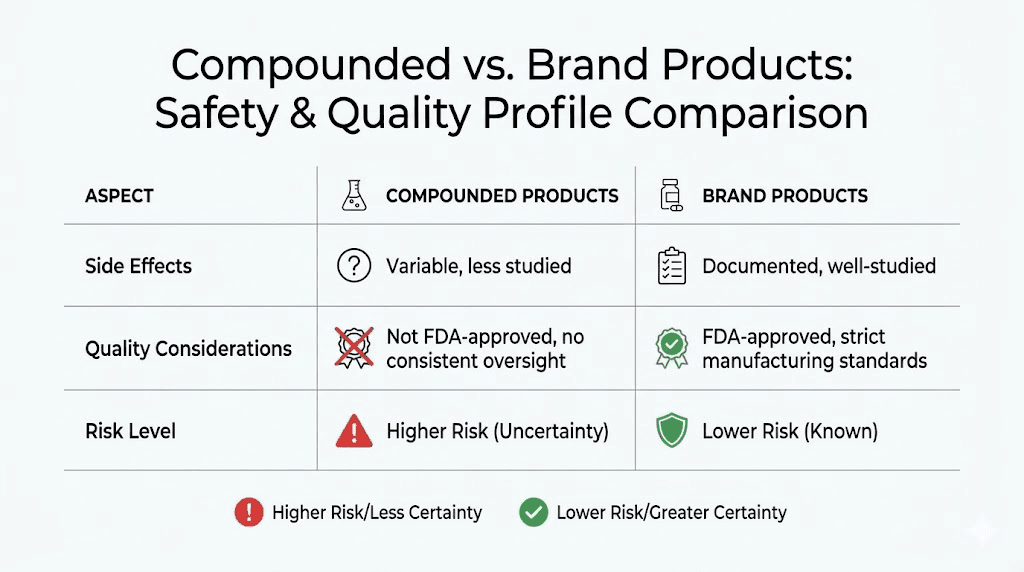
However, compounded formulations lack FDA approval and quality oversight beyond state pharmacy board standards. Each pharmacy creates its own mixture. Potency, sterility, and stability may vary. The cost typically exceeds brand-name semaglutide even accounting for the added b12.
Separate supplementation provides flexibility. Adjust b12 dose independently of semaglutide dose changes. Use oral b12 to avoid additional injections. Switch between cyanocobalamin and methylcobalamin based on testing and response. This approach costs less overall and allows more precise management of each component.
For patients confirmed to need b12 supplementation, either approach works. The choice comes down to personal preference regarding convenience versus flexibility and cost. For patients without clear indication for b12 supplementation, using a compounded combination means paying extra for an additive that may provide no benefit.
Side effects and safety considerations for semaglutide with b12
Vitamin b12 has remarkably low toxicity. No established upper limit exists because excess b12 excretes through kidneys without causing harm. This safety profile makes supplementation low-risk even when not strictly necessary.
Potential injection site reactions
Compounded formulations sometimes cause more injection site irritation than single-ingredient products. This may result from the combination of compounds, variations in pH, or preservatives used in the mixture. Some patients report increased redness, swelling, or discomfort at injection sites when using compounded semaglutide with b12 compared to brand-name semaglutide alone.
Rotating injection sites helps minimize cumulative irritation. Use different areas of the abdomen, thighs, or upper arms for each injection. Avoid injecting into the same spot more than once every 4 to 6 weeks. This allows tissue recovery and reduces the buildup of irritation.
Allergic reactions to b12 formulations
True allergy to b12 itself remains extremely rare. However, allergic reactions to preservatives or other ingredients in b12 formulations occur occasionally. Benzyl alcohol, commonly used as a preservative in injectable b12 products, can cause reactions in sensitive individuals.
Symptoms of preservative allergy include itching, hives, facial swelling, or difficulty breathing. These require immediate medical attention and discontinuation of the product. Switching to preservative-free formulations typically resolves the issue for people who need b12 but react to standard preparations.
Interactions with other supplements and medications
Vitamin b12 has few significant interactions. It works synergistically with folate in DNA synthesis and homocysteine metabolism. Taking both together makes sense for most people, though folate status should be adequate before starting high-dose b12 to avoid masking folate deficiency.
Potassium supplements taken concurrently with b12 injections may theoretically reduce b12 effectiveness, but this interaction rarely causes clinical problems. Most people take b12 and potassium at different times naturally, preventing any potential interference.
Vitamin C in extremely high doses (more than 1000 mg taken with a b12 supplement) may reduce b12 absorption when taken together. Spacing them by several hours eliminates this minor concern. Most people do not take vitamin C doses high enough to cause meaningful interaction anyway.
Quality control concerns with compounded products
Compounding pharmacies operate under different regulatory oversight than pharmaceutical manufacturers. The FDA does not approve compounded products before sale. State boards of pharmacy provide primary oversight, but standards and enforcement vary by state.
Quality issues occasionally emerge. Potency may differ from labeled amounts. Sterility breaches can introduce contamination. Stability problems may reduce effectiveness over time if products are not stored properly.
Choosing reputable compounding pharmacies with proper certifications helps minimize these risks. Look for 503B outsourcing facilities that voluntarily submit to FDA inspection. Verify the pharmacy is accredited by the Pharmacy Compounding Accreditation Board. These credentials indicate commitment to quality standards beyond minimum state requirements.
Cost considerations and insurance coverage
Compounded semaglutide with b12 typically costs $200 to $400 per month depending on dose and pharmacy. This usually exceeds brand-name semaglutide costs for patients with insurance coverage. Insurance rarely covers compounded formulations.
Separate b12 supplementation costs $5 to $30 per month for oral forms or $15 to $50 per month for injectable b12 if purchasing syringes and supplies separately.
This makes the standalone approach more economical for most patients.
The economic calculus changes if insurance does not cover brand-name semaglutide. Some patients turn to compounded versions for affordability. In this scenario, choosing a compounded version with b12 added costs only slightly more than compounded semaglutide alone, making the combination potentially worthwhile even without clear medical necessity.
Alternatives to semaglutide with b12 compounded formulations
Several approaches achieve the same goals without using compounded combinations.
Brand-name semaglutide plus separate b12 supplementation
This represents the most straightforward alternative. Use FDA-approved semaglutide products like Wegovy or Ozempic. Add b12 supplementation separately based on testing and risk factors.
This approach provides maximum flexibility. Adjust each component independently. Change b12 form or dose without affecting semaglutide. Switch between oral and injectable b12 based on preference and response. The quality assurance of FDA-approved semaglutide products provides peace of mind about potency and sterility.
Alternative GLP-1 receptor agonists
If semaglutide causes significant side effects or concerns about b12 status arise, other GLP-1 medications offer alternatives. Tirzepatide combines GLP-1 activity with GIP receptor agonism. This dual action may provide better weight loss outcomes for some patients.
Liraglutide has longer safety data and does not appear to cause b12 issues in clinical practice. The daily injection requirement deters some patients but provides steady levels without the peaks and troughs of weekly dosing.
Dulaglutide offers weekly dosing like semaglutide but with different pharmacokinetics that some patients tolerate better. Comparing options with your provider makes sense if side effects or concerns arise.
Nutritional optimization instead of supplementation
Focusing on b12-rich foods may provide adequate amounts for many patients. Animal products contain the most bioavailable b12. Beef, lamb, fish, eggs, and dairy products all supply substantial amounts.
A 3-ounce serving of beef provides approximately 2.5 mcg b12. Three eggs contain about 1.5 mcg. A cup of milk has 1.2 mcg. Meeting the recommended daily intake of 2.4 mcg becomes easy with modest animal product consumption.
The challenge during semaglutide use involves reduced appetite making it harder to consume adequate amounts of any food, including b12-rich options. Prioritizing nutrient-dense foods becomes critical. Focus protein intake on b12-rich sources rather than plant-based proteins during active weight loss.
Fortified foods offer another option. Many plant-based milk alternatives, breakfast cereals, and nutritional yeast products contain added b12. These work well for people following plant-based diets or who cannot tolerate large amounts of animal products.
Testing before supplementing
The most logical approach involves testing b12 status before adding supplementation. This simple blood test costs $20 to $50 and provides clear information about whether supplementation makes sense.
Test at baseline before starting semaglutide. Check again after 6 to 12 months of use. If levels remain normal, supplementation likely provides no benefit. If levels decline, adding b12 becomes appropriate with clear justification.
This evidence-based approach avoids unnecessary supplementation costs and simplifies the protocol for people who do not need additional b12. It identifies the subset of patients who truly benefit from supplementation.
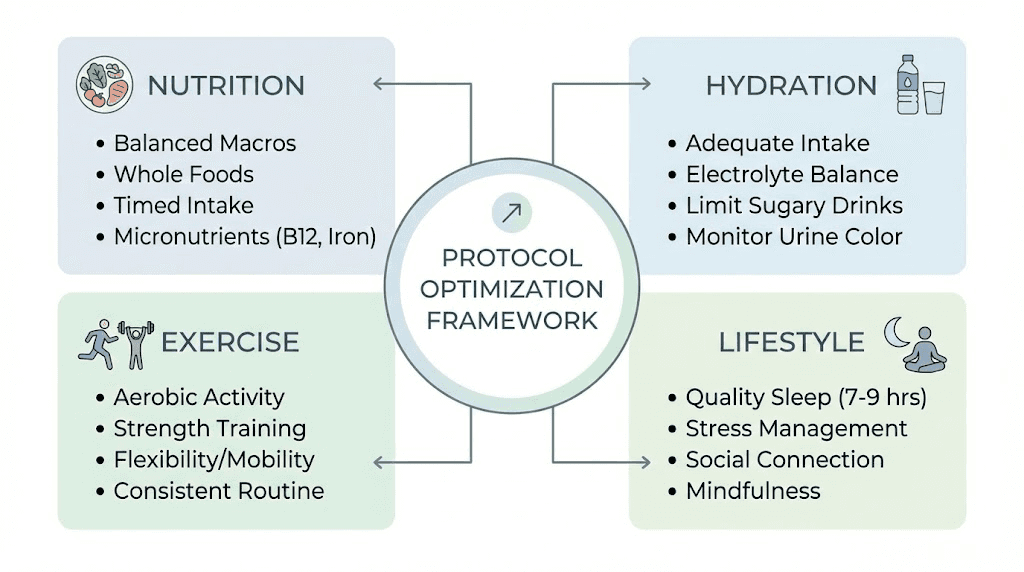
Optimizing semaglutide outcomes without b12 addition
Many strategies improve semaglutide results without adding b12 to the formulation.
Proper dose escalation to minimize side effects
Nausea and fatigue, the symptoms often attributed to b12 needs, more commonly result from starting doses too high or escalating too quickly. The standard escalation protocol exists for good reason.
Start with 0.25 mg weekly for 4 weeks. This allows the body to adapt to delayed gastric emptying gradually. Increase to 0.5 mg weekly for the next 4 weeks. Continue increasing by 0.25 to 0.5 mg every 4 weeks until reaching the target dose or maximum tolerated dose.
Some patients benefit from even slower escalation. Staying at each dose level for 6 weeks instead of 4 reduces side effects for sensitive individuals. There is no rush. Slower escalation with better tolerance produces better long-term adherence and results than aggressive dosing that causes misery.
Microdosing approaches have gained popularity. Some patients use 0.125 mg or even lower starting doses and make tiny incremental increases. While this falls outside standard protocols, it may work for people extremely sensitive to medication effects.
Strategic meal timing and composition
Working with semaglutide mechanisms rather than fighting them improves tolerance. The medication slows gastric emptying. This means food sits in the stomach longer. Large meals or high-fat meals exacerbate this, leading to nausea and discomfort.
Eating smaller meals more frequently works better. Instead of three large meals, try four to six smaller eating occasions throughout the day. Each meal should contain 200 to 400 calories rather than 600 to 800.
Lower fat content helps. Fat triggers the strongest slowing of gastric emptying. While healthy fats remain important for nutrition, concentrating them all in one meal creates problems. Distribute fat intake across the day in smaller amounts.
Prioritize protein. Adequate protein intake during weight loss preserves muscle mass more effectively than any supplement. Aim for 1.2 to 1.6 grams per kilogram body weight daily. Choose lean protein sources that are easier to digest when gastric emptying is slowed.
Hydration and electrolyte balance
Reduced food intake means reduced water and electrolyte intake from food. Many people feel fatigued because they are mildly dehydrated and depleted in sodium, potassium, and magnesium, not because they need b12.
Aim for adequate fluid intake. The old rule of eight glasses daily provides a starting point. Adjust based on thirst, urine color, and activity level. Pale yellow urine indicates good hydration. Dark yellow suggests drinking more.
Sodium intake often drops dramatically during weight loss. People avoid processed foods and eat more whole foods, which contain less sodium. This can lead to mild hyponatremia causing fatigue, weakness, and lightheadedness. Adding a bit more salt to meals or drinking broth helps maintain sodium balance.
Potassium and magnesium may need attention too. Leafy greens, avocados, and bananas provide potassium. Nuts, seeds, and leafy greens supply magnesium. Consider supplementation if dietary intake seems inadequate.
Exercise and movement
Physical activity combats fatigue through multiple mechanisms. Regular movement improves energy levels, mood, and sleep quality. These benefits have nothing to do with b12 but significantly impact how people feel during weight loss.
Resistance training preserves muscle mass better than any nutritional supplement. Two to three sessions weekly focusing on major muscle groups makes a substantial difference in body composition changes during weight loss.
Daily walking or other moderate activity supports overall health and wellbeing. Start with 10 to 15 minutes daily if previously sedentary. Build gradually to 30 to 60 minutes most days. This improves outcomes without requiring b12 addition.
Sleep and stress management
Fatigue often stems from insufficient sleep rather than nutrient deficiency. Prioritizing 7 to 9 hours nightly improves energy more reliably than supplementation.
Stress management matters too. Weight loss represents a physical and psychological stressor. Adding mindfulness practices, adequate rest days from exercise, and maintaining social connections supports overall wellbeing during this process.
Clinical scenarios and decision-making framework
Different patient situations call for different approaches.
Scenario 1: Healthy individual starting semaglutide with normal baseline b12
A 45-year-old with no health conditions starts semaglutide for weight loss. Baseline b12 level tests at 550 pg per milliliter. No medications that affect b12 absorption. Regular diet includes animal products. No history of absorption issues.
Recommendation: No b12 supplementation needed at start. Continue normal diet emphasizing protein and nutrient density. Retest b12 in 12 months. Add supplementation only if levels decline below 400 pg per milliliter or symptoms suggest deficiency.
This represents the most common situation. Most patients starting semaglutide do not need b12 supplementation. Testing after a year catches any developing issues before they become problematic.
Scenario 2: Vegan patient with low-normal b12 considering semaglutide
A 38-year-old vegan is prescribed semaglutide. Baseline b12 tests at 280 pg per milliliter, low-normal range. Currently takes no b12 supplements. Diet consists entirely of plant foods with minimal fortified products.
Recommendation: Start b12 supplementation immediately, independent of semaglutide use. Use 1000 to 2000 mcg oral b12 daily or 1000 mcg injected weekly. Retest after 2 to 3 months to verify repletion. Continue supplementation indefinitely given dietary pattern.
Vegans need b12 supplementation regardless of medication use. The semaglutide component matters less than the baseline deficiency risk. Addressing b12 proactively prevents future issues.
Scenario 3: Post-bariatric surgery patient adding semaglutide
A 52-year-old had gastric bypass 5 years ago. Currently maintains 80-pound weight loss but has regained 20 pounds. Provider prescribes semaglutide to address regain. Patient takes multivitamin with b12 but has not checked levels recently.
Recommendation: Test b12 before starting semaglutide. If low or low-normal, switch to high-dose b12 supplementation separate from multivitamin (1000 to 2000 mcg daily oral or regular injections). Monitor levels every 6 months given high-risk status. Ensure other nutrients affected by bypass remain adequate as well.
Bariatric surgery patients have permanent malabsorption issues. They represent a high-risk group requiring careful monitoring and aggressive supplementation as needed. The standard multivitamin b12 content may not suffice.
Scenario 4: Elderly patient on multiple medications including metformin
A 68-year-old with type 2 diabetes takes metformin, a proton pump inhibitor for reflux, and is starting semaglutide for additional glucose control and weight loss. No recent b12 testing. Takes no current supplements.
Recommendation: Test b12 immediately. If normal, start 1000 mcg oral b12 daily as prevention given multiple risk factors (age, metformin, PPI, now semaglutide). If low or low-normal, use higher dose supplementation or injectable b12. Retest every 6 months. This patient has four simultaneous factors compromising b12 status, making supplementation prudent even with normal baseline levels.
Scenario 5: Patient experiencing significant fatigue and nausea on semaglutide
A 40-year-old 6 weeks into semaglutide reports severe fatigue and persistent nausea. Current dose is 0.5 mg weekly after 4 weeks at 0.25 mg. Diet has decreased dramatically. Sleep remains good. No other symptoms.
Recommendation: Test b12, but do not wait for results to make changes. Reduce semaglutide dose back to 0.25 mg to improve tolerance. Implement dietary strategies for nausea (smaller meals, lower fat, adequate protein). Add ginger tea or other proven nausea remedies. Check hydration and electrolyte status. If b12 comes back low, add supplementation. If normal, continue supportive measures without b12 addition.
This scenario illustrates why most fatigue and nausea do not result from b12 deficiency. The timeline is too short. The symptoms more likely reflect medication intolerance requiring dose adjustment and supportive care rather than vitamin supplementation.
Frequently asked questions
Does semaglutide cause b12 deficiency?
Limited evidence exists that semaglutide directly causes b12 deficiency in most patients. One study showed decreased levels in post-bariatric surgery patients, but this high-risk group had multiple confounding factors. The theoretical mechanism involves reduced stomach acid, but clinical significance remains unclear. Testing b12 levels during treatment provides the best way to identify any individual decline rather than assuming everyone needs supplementation.
Should I take b12 with semaglutide even if my levels are normal?
No compelling evidence supports routine b12 supplementation for people with normal levels starting semaglutide. The vitamin has low toxicity, so supplementation carries minimal risk, but also likely provides no benefit if stores are adequate. Testing b12 after 6 to 12 months of semaglutide use makes more sense than presumptive supplementation. This approach identifies people who actually need it while avoiding unnecessary supplements and costs for others.
Which form of b12 is best with semaglutide?
Methylcobalamin provides immediate bioavailability without requiring metabolic conversion, making it theoretically superior. However, cyanocobalamin works well for most people and costs significantly less. Injectable forms bypass absorption issues entirely and work regardless of stomach acid or intrinsic factor status. For people with confirmed absorption problems or documented deficiency, injectable methylcobalamin represents the gold standard. For prevention in people with normal absorption, oral cyanocobalamin suffices.
How much does compounded semaglutide with b12 cost?
Prices vary widely by pharmacy and dose but typically range from $200 to $400 per month. This often exceeds brand-name semaglutide costs for patients with insurance coverage. The compounded versions appeal primarily to people without insurance coverage who find brand-name prices prohibitive. Adding b12 to compounded semaglutide usually increases cost by $20 to $50 monthly compared to semaglutide alone.
Can I just take oral b12 instead of getting injections?
High-dose oral b12 (1000 to 2000 mcg daily) provides adequate absorption through passive diffusion even without intrinsic factor. This approach works well for prevention and for treating mild to moderate deficiency. Severe deficiency or neurological symptoms require injectable b12 for faster repletion. Injectable forms also ensure compliance since you cannot forget a shot you have already received, whereas remembering daily pills can challenge some people.
Will adding b12 help me lose more weight on semaglutide?
No evidence supports enhanced weight loss from adding b12 to semaglutide protocols. The vitamin does not increase metabolic rate, enhance fat burning, or improve the appetite suppression that drives semaglutide weight loss. If b12 deficiency exists and causes fatigue that limits physical activity, correcting the deficiency may indirectly support weight loss by enabling more movement. Otherwise, b12 addition affects weight outcomes minimally or not at all.
Should I stop b12 supplementation when I stop semaglutide?
This depends on why you started supplementation. If you began b12 due to pre-existing deficiency, dietary restrictions, or other risk factors independent of semaglutide, continue supplementation after stopping the medication. If b12 was added specifically for theoretical semaglutide effects and your levels test normal, stopping supplementation makes sense. Retest 3 to 6 months after stopping semaglutide to establish new baseline status.
Can I get enough b12 from food while on semaglutide?
People who consume adequate animal products can often maintain sufficient b12 from diet alone, even during semaglutide use. The challenge involves reduced appetite making it harder to consume enough of any food. Prioritizing b12-rich sources like beef, fish, eggs, and dairy helps. Vegans and vegetarians need supplementation regardless of semaglutide. People with absorption issues need supplementation even with adequate dietary intake. Testing determines whether dietary intake suffices for your individual situation.
External resources
The decision to use semaglutide with b12 combination therapy depends entirely on individual circumstances. Most patients starting with normal b12 levels and no significant risk factors do not require supplementation. Those with pre-existing deficiency, dietary restrictions, absorption issues, or multiple risk factors benefit from either adding b12 to their compounded semaglutide or taking it separately.
Testing rather than guessing provides the clearest guidance. A simple blood test before starting semaglutide and periodic monitoring during treatment identifies who actually needs supplementation. This evidence-based approach avoids unnecessary costs and complexity while ensuring people who truly benefit from b12 addition receive appropriate supplementation.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions about medication combinations, supplementation strategies, and optimizing weight loss outcomes.
In case I do not see you, good afternoon, good evening, and good night. May your protocols stay effective, your supplementation stay appropriate, and your results stay consistent.