Feb 21, 2026

Before you panic about that dizzy spell after your semaglutide injection, stop. Take a breath. And read this.
Dizziness is one of the most commonly reported side effects of semaglutide, affecting roughly 8% of users in clinical trials. That number sounds manageable on paper. But when the room tilts sideways thirty minutes after your weekly dose, percentages stop mattering. What matters is understanding why it is happening, whether it is normal, and what you can do about it right now.
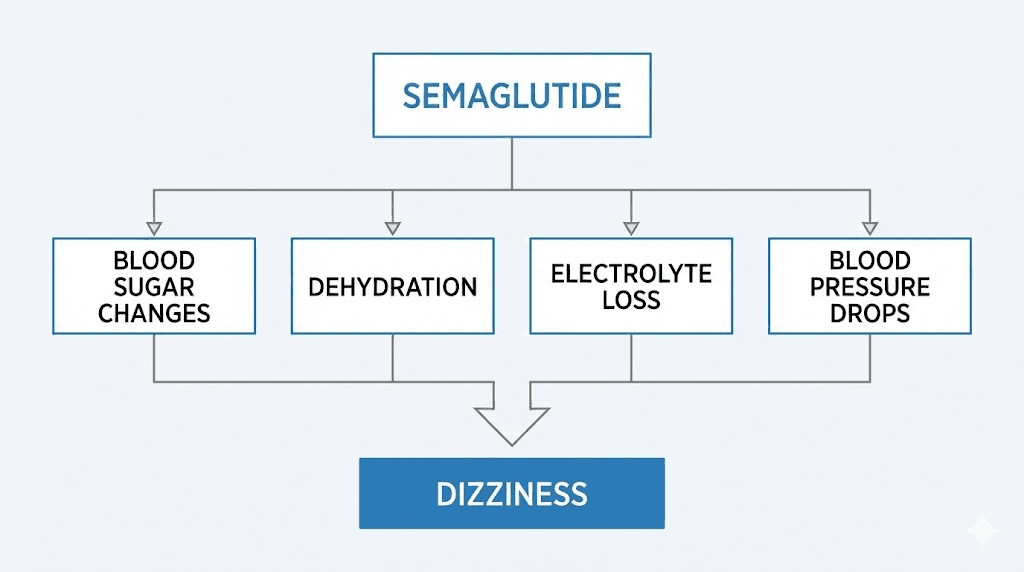
The causes are not always obvious. Blood sugar shifts. Dehydration from gastrointestinal side effects. Blood pressure drops. Electrolyte imbalances. Sometimes a combination of all four hitting at once. And here is what most articles will not tell you: the dizziness often has a predictable pattern tied to dose escalation, meal timing, and hydration status. Understanding that pattern is the difference between managing it effectively and suffering through weeks of unnecessary discomfort.
This guide covers everything. The mechanisms behind semaglutide-related dizziness, based on clinical trial data and a major real-world study of over 419,000 users. The specific triggers most people miss. Seven practical management strategies that actually work. And the warning signs that mean you need to call your doctor immediately. Whether you are just starting your semaglutide protocol or dealing with persistent lightheadedness months into treatment, this is the reference you will keep coming back to.
Why semaglutide causes dizziness
Semaglutide is a GLP-1 receptor agonist that mimics a naturally occurring hormone in your body. It regulates appetite, slows gastric emptying, and modulates blood sugar levels. These are all positive mechanisms for weight loss and blood sugar control. But each one of them can also contribute to dizziness through different pathways.
The dizziness is not random. It follows a logic rooted in how the medication changes your physiology. Understanding these mechanisms gives you the power to prevent most episodes before they start.
Blood sugar fluctuations and the GLP-1 connection
GLP-1 receptor agonists work by enhancing insulin secretion when blood glucose levels are elevated. This is called glucose-dependent insulin release. In theory, this mechanism should prevent blood sugar from dropping too low because insulin only increases when glucose is already high.
In practice, it is not always that clean.
When semaglutide suppresses appetite significantly, and it does for most people, food intake drops. Sometimes dramatically. If you are eating 40-50% fewer calories than before, your body has less glucose coming in throughout the day. Combined with semaglutide appetite suppression, this creates windows where blood sugar dips lower than your body is accustomed to. Not clinically dangerous hypoglycemia in most cases, but enough to trigger dizziness, lightheadedness, and that familiar foggy feeling.
The risk escalates sharply when semaglutide is combined with other blood sugar-lowering medications. Sulfonylureas and insulin do not have the same glucose-dependent safety mechanism. They push blood sugar down regardless of current levels. Add semaglutide to either of these, and the hypoglycemia risk jumps considerably. Symptoms include shaking, sweating, confusion, rapid heartbeat, and yes, significant dizziness.
For non-diabetic users taking semaglutide purely for weight loss, true hypoglycemia is uncommon. But the reduced caloric intake creates a state that mimics low blood sugar symptoms. Your body is getting less fuel than it expects. The brain notices. Dizziness follows.
SeekPeptides members frequently report that eating consistent, protein-rich meals eliminates the majority of blood sugar-related dizziness episodes. The solution is not to fight the appetite suppression, but to ensure the calories you do consume are stable, sustained-energy sources.
Dehydration from gastrointestinal side effects
This is the cause most people underestimate.
Semaglutide slows gastric emptying. That is one of its primary mechanisms. Food stays in the stomach longer, which reduces hunger and promotes satiety. But it also commonly triggers nausea, vomiting, and diarrhea, particularly during the early weeks of treatment and after each dose increase.
Clinical trials show nausea affects roughly 20% of users on standard doses and up to 44% on higher Wegovy doses. Vomiting, diarrhea, and constipation add to the fluid loss. When you are losing fluids through GI symptoms while simultaneously eating and drinking less due to appetite suppression, dehydration develops faster than most people realize.
Dehydration reduces blood volume. Less blood volume means less blood reaching the brain when you stand up or change positions. The result is orthostatic dizziness, that sudden lightheadedness when you go from sitting to standing. It can also cause persistent, low-grade dizziness throughout the day that never fully resolves until fluid status improves.
The connection between semaglutide GI effects and dizziness is so consistent that most healthcare providers now recommend increasing water intake to 2-3 liters daily before starting the medication. Not as a suggestion. As a requirement.
Electrolyte imbalances you might not notice
Vomiting and diarrhea do not just remove water from the body. They strip essential electrolytes. Sodium. Potassium. Magnesium. Chloride. These minerals regulate nerve function, muscle contraction, and fluid balance. When they drop below normal levels, the nervous system responds with symptoms including dizziness, muscle cramps, heart palpitations, and cognitive fog.
Potassium deserves special attention. Low potassium (hypokalemia) directly affects the vestibular system, the inner ear structures responsible for balance. Even mild potassium deficiency can amplify feelings of dizziness and spatial disorientation. Combined with dehydration, it creates a feedback loop. You feel dizzy, so you eat and drink less, which worsens the electrolyte deficit, which makes the dizziness worse.
Most standard blood panels do not catch subtle electrolyte shifts unless you specifically request them. If your dizziness persists beyond the first few weeks, ask for a comprehensive metabolic panel that includes magnesium levels (not typically included in basic panels).
Monitoring your electrolytes becomes even more important if you are following a semaglutide diet plan that restricts certain food groups, as these restrictions can compound mineral deficiencies from GI-related losses.
Blood pressure changes and orthostatic hypotension
Semaglutide lowers blood pressure. For most people, this is a benefit. Clinical data shows a modest reduction of 2-6 mmHg in systolic blood pressure, primarily driven by weight loss and increased sodium excretion (natriuresis). But for some users, particularly those already taking antihypertensive medications, this blood pressure reduction tips the balance too far.
Orthostatic hypotension is defined as a drop of 20 mmHg or more in systolic blood pressure within three minutes of standing. In Wegovy clinical trials, hypotension-related adverse events occurred in 1.3% of semaglutide-treated patients compared to 0.4% on placebo. That is more than three times the rate. And the risk was notably higher in patients already taking blood pressure medications.
The mechanism involves multiple factors. Weight loss itself reduces blood pressure. Semaglutide-induced natriuresis removes sodium and water. GI side effects cause fluid loss. And GLP-1 receptor agonists produce a modest increase in heart rate of 2-5 beats per minute, which may reflect changes in autonomic nervous system tone.
When blood pressure drops too quickly upon standing, the brain temporarily loses adequate blood flow. The room spins. Vision darkens at the edges. You might feel like you are about to faint. This is different from the general lightheadedness caused by dehydration or low blood sugar, though all three can occur simultaneously.
If you are taking medications for hypertension alongside semaglutide, regular blood pressure monitoring is not optional. It is essential. Your prescriber may need to reduce your antihypertensive dose as semaglutide takes effect and your weight decreases. The combination that was appropriate when you started may become too aggressive three months in.
How common is semaglutide dizziness
Numbers tell a clearer story than anecdotes. Clinical trials and real-world studies provide a detailed picture of how frequently dizziness occurs, who is most at risk, and how the risk evolves over time.
Clinical trial incidence rates
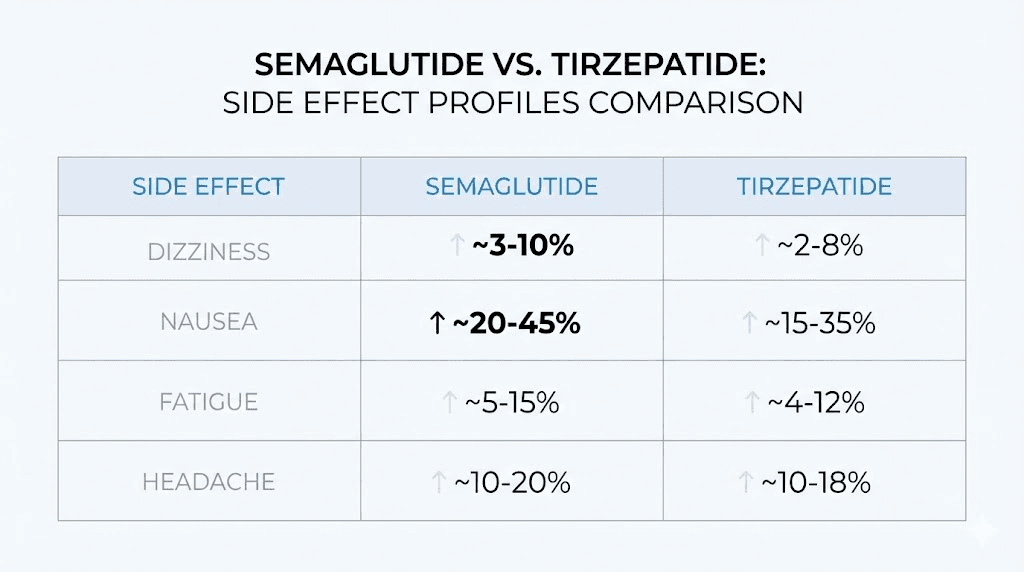
Across semaglutide clinical trials, dizziness was reported by approximately 8% of both adult and adolescent participants. To put that in perspective, fatigue occurs at similar rates, while nausea (the most common side effect) affects 20-44% depending on the dose.
Eight percent means roughly 1 in 12 users will experience dizziness at some point during treatment. But this number comes with important context. Clinical trials capture any report of dizziness, regardless of severity or duration. A single mild episode that resolved in minutes counts the same as persistent daily dizziness lasting weeks. Most reported cases fell on the milder end of the spectrum.
The incidence was not evenly distributed across doses. Dizziness occurred more frequently during dose escalation phases than during maintenance dosing. This pattern strongly suggests the body adapts to semaglutide over time, and most dizziness represents a temporary adjustment period rather than a permanent side effect.
Compare this to other GLP-1 side effects: nausea (20-44%), constipation (12-24%), diarrhea (15-30%), and burping or sulfur burps (variable rates). Dizziness at 8% is meaningful but far from the most common complaint.
Real-world vestibular disorder findings
A landmark retrospective cohort study published in Biomedicines analyzed data from 419,497 semaglutide users matched with controls across 64-68 healthcare organizations. The findings added a new dimension to understanding semaglutide-related dizziness by looking at vestibular disorders specifically, conditions affecting the inner ear and balance system.
The results were striking.
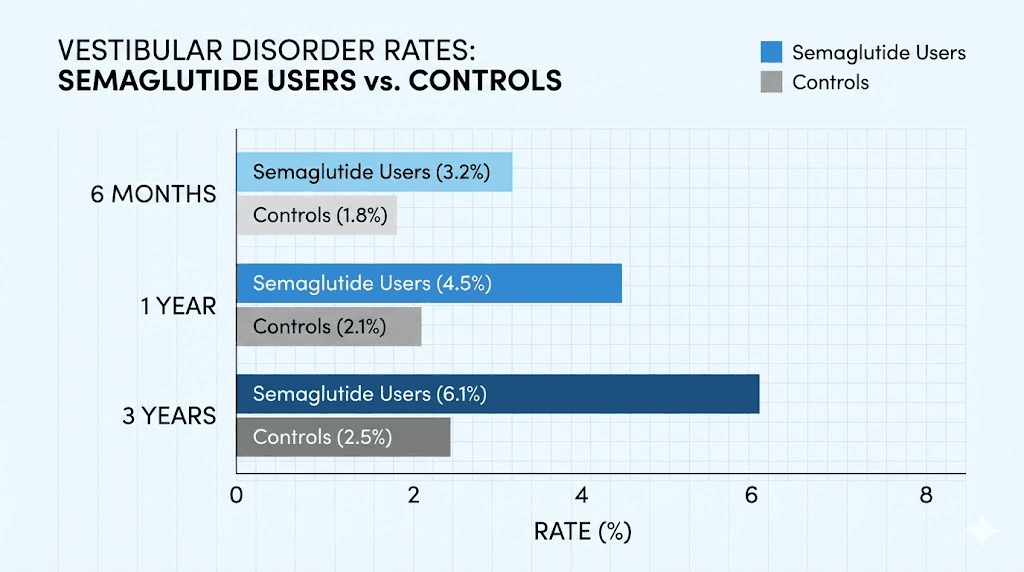
Semaglutide users showed significantly higher rates of vestibular disorders compared to matched controls at every time point measured. At six months, 0.12% of semaglutide users developed vestibular disorders compared to 0.03% of controls. At one year, the rates were 0.22% versus 0.06%. By three years, 0.41% of semaglutide users had been diagnosed with vestibular conditions compared to 0.16% of controls.
The hazard ratios were consistently elevated: 4.02 at six months, rising to 4.95 at three years. In plain language, semaglutide users were roughly four to five times more likely to develop vestibular disorders than non-users.
Among those who developed vestibular conditions, benign paroxysmal positional vertigo (BPPV) was the most common diagnosis at 69.8%. Other peripheral vertigo accounted for 12.4%, and vestibular neuronitis for 3.9%. The median time to BPPV diagnosis was 2.8 months after starting semaglutide.
An interesting finding from this study: when comparing semaglutide versus tirzepatide, semaglutide showed a higher vestibular disorder risk. At three years, the relative risk was 2.04 (meaning semaglutide users had roughly double the risk compared to tirzepatide users). The researchers suggested that tirzepatide dual GIP/GLP-1 receptor action might provide some protective effect unavailable through the GLP-1-only mechanism of semaglutide.
Dizziness versus vertigo: understanding the difference
Not all dizziness is the same, and the distinction matters for both treatment and prognosis.
General dizziness or lightheadedness typically feels like unsteadiness, a floating sensation, or feeling faint. It is usually caused by dehydration, blood sugar changes, or blood pressure drops. It resolves when the underlying cause is addressed. Lie down, drink water, eat something, and it passes.
Vertigo is different. Vertigo creates a spinning sensation, as though you or the room are rotating. It often comes with nausea (separate from semaglutide-induced nausea), difficulty walking, and sometimes hearing changes or ringing in the ears. Vertigo indicates involvement of the vestibular system, the inner ear structures that govern balance.
If you experience spinning-type dizziness rather than general lightheadedness, that is worth a specific conversation with your healthcare provider. The 2.8-month median time to BPPV diagnosis in the study above suggests these vestibular effects can develop relatively early in treatment. BPPV specifically can be treated effectively with positioning maneuvers (the Epley maneuver), but it requires proper diagnosis first.
Understanding which type of dizziness you are experiencing helps you respond appropriately. General lightheadedness usually responds to the management strategies covered below. True vertigo may require specific vestibular evaluation and treatment beyond basic hydration and nutrition adjustments.
When semaglutide dizziness typically starts and how long it lasts
Timing matters. Knowing when to expect dizziness, and when it should resolve, helps you plan ahead and avoid unnecessary worry.
The dose escalation pattern
The standard semaglutide titration schedule moves through progressively higher doses over 16-20 weeks. For Wegovy (weight loss dosing), the schedule typically looks like this:
Weeks 1-4: 0.25 mg weekly
Weeks 5-8: 0.5 mg weekly
Weeks 9-12: 1.0 mg weekly
Weeks 13-16: 1.7 mg weekly
Week 17 onward: 2.4 mg maintenance
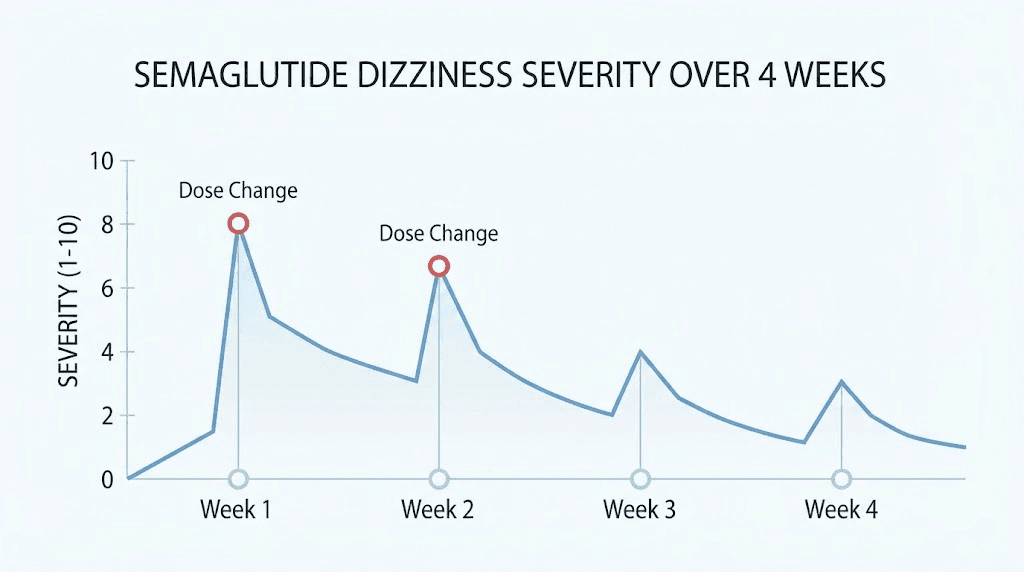
Dizziness most commonly appears during the first one to two weeks after each dose increase. The body needs time to adjust to the stronger effect on gastric emptying, appetite suppression, and blood sugar regulation. Most users report that dizziness at each dose level resolves within 7-14 days as tolerance develops.
This means you might experience brief dizzy episodes at weeks 1, 5, 9, 13, and 17. Each time should be milder than the last as your body adapts. If the dizziness does not improve within two weeks at a given dose, that is a signal to consult with your prescriber before escalating further.
Some compounded semaglutide protocols use different titration schedules, allowing for more gradual increases. This can reduce the intensity of side effects at each step, though it extends the time to reach therapeutic doses.
First injection dizziness
The very first semaglutide injection often produces the most noticeable side effects because your body has zero tolerance to the medication. Even at the lowest starting dose of 0.25 mg, some users experience dizziness within hours of their first injection.
This first-dose dizziness typically falls into one of two categories. Vasovagal response is the first. Some people experience lightheadedness simply from the act of self-injection, particularly if they are anxious about needles. This resolves quickly and is not related to the medication itself. The second category is pharmacological effect, where the medication begins working within hours, affecting blood sugar regulation and gastric motility before the body has adapted.
First-injection dizziness usually peaks within 24-48 hours and subsides by day 3-5. If you are concerned, plan your first injection for a day when you do not need to drive or operate machinery. A quiet day at home gives your body space to adjust without pressure.
Choosing the best time of day for your injection can also influence how you experience initial side effects. Many users find that injecting in the evening allows them to sleep through the peak of first-day symptoms.
The adaptation timeline
Most semaglutide-related dizziness follows a predictable pattern of improvement:
Days 1-3 after dose change: Peak dizziness likelihood. Blood sugar patterns are shifting, GI effects are strongest, and hydration status may be disrupted by nausea or reduced intake.
Days 4-7: Noticeable improvement for most users. The body begins adapting to the new dose level. Episodes become shorter and less intense.
Days 8-14: Most users report resolution or near-resolution. Residual mild lightheadedness may occur with positional changes but does not interfere with daily activities.
Weeks 3-4 at stable dose: Dizziness is typically absent. The body has fully adapted. This stability continues until the next dose escalation.
If your dizziness does not follow this general pattern, or if it worsens rather than improves over the first two weeks at a dose, that is meaningful clinical information. Persistent or worsening dizziness warrants evaluation rather than simply waiting it out. Your prescriber may recommend holding at your current dose longer before escalating, or investigating other contributing factors.
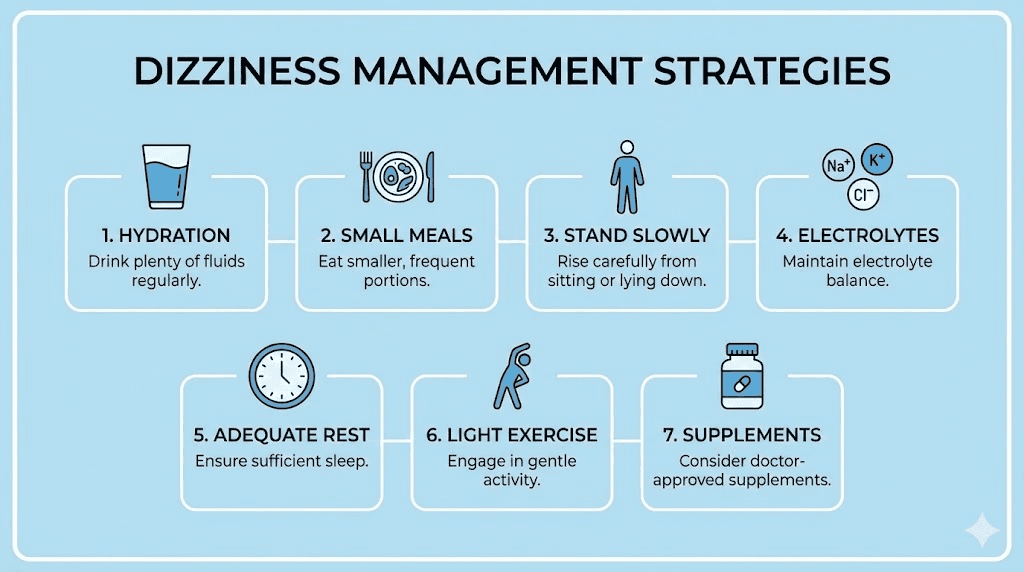
Seven practical ways to manage semaglutide dizziness
Theory is useful. Practical strategies are better. These seven approaches address the root causes of semaglutide-related dizziness and can significantly reduce or eliminate episodes for most users.
Hydration strategies that actually work
Telling someone to drink more water is easy advice. Making it practical is harder. Here is what actually moves the needle.
Target 2.5-3 liters of total fluid intake daily. This is significantly more than the standard 8-glasses recommendation, and the increase accounts for the additional fluid losses from semaglutide GI effects. Start hydrating before symptoms appear, not after.
Front-load your hydration. Drink 500ml (about 16 ounces) within the first hour of waking, before eating anything. This replenishes overnight losses and sets a strong baseline for the day. Then maintain steady intake, 200-250ml every hour or so, rather than trying to catch up with large volumes later.
Water alone may not be enough if you are experiencing vomiting or diarrhea. Add electrolyte drinks or oral rehydration solutions to replace what GI symptoms are stripping away. Look for products with sodium, potassium, and magnesium. Avoid high-sugar sports drinks, as the sugar content can exacerbate blood sugar swings.
Track your hydration. It sounds tedious, but a simple water bottle with time markings or a phone app makes a measurable difference. Users who track consistently report fewer dizziness episodes within the first week of improving their hydration habits.
Eating patterns to stabilize blood sugar
Semaglutide suppresses appetite effectively. Too effectively, for some people. The temptation to skip meals when you genuinely are not hungry is strong. But skipping meals is the fastest path to blood sugar-related dizziness.
Eat on a schedule, not on appetite. Set three meal times regardless of hunger level. Even if you can only manage half a portion, getting consistent nutrition prevents the blood sugar dips that trigger lightheadedness.
Prioritize protein at every meal. Protein stabilizes blood sugar more effectively than carbohydrates and takes longer to digest, providing sustained energy. A semaglutide-friendly food list should emphasize lean proteins, healthy fats, and complex carbohydrates at each sitting.
Avoid large, carb-heavy meals on an empty stomach. When you do eat after a long gap, a high-carbohydrate meal can cause a rapid blood sugar spike followed by a crash. This rebound effect produces dizziness even in people not taking GLP-1 medications. On semaglutide, the effect is amplified.
Consider small snacks between meals if dizziness occurs reliably at specific times. A handful of nuts, a piece of cheese, or a protein shake for GLP-1 users can bridge the gap without fighting the appetite suppression. The goal is not to eat more overall, but to distribute calories more evenly throughout the day.
The foods to avoid on semaglutide are equally important. High-fat meals that slow digestion further, extremely spicy foods, and large portions of simple carbohydrates tend to worsen both GI symptoms and the dizziness that follows.
Positional change techniques
If orthostatic dizziness is your primary issue, the fix is mechanical, not medical.
Never stand up quickly. Sit on the edge of your bed for 30-60 seconds before standing in the morning. When getting up from a chair, pause at the standing position for a moment before walking. These brief pauses give your cardiovascular system time to adjust blood flow to your brain.
If dizziness strikes while standing, sit or lie down immediately. Do not try to push through it. Falls are the primary danger from orthostatic dizziness, and a single bad fall can cause injuries far worse than the inconvenience of sitting down for two minutes.
Cross your legs and squeeze your thigh muscles before standing. This simple maneuver increases venous return to the heart and temporarily boosts blood pressure, reducing the likelihood of lightheadedness upon standing. Clenching your fists and flexing your arm muscles works through the same mechanism.
Electrolyte management
Basic electrolyte supplementation can resolve dizziness that hydration alone does not fix. Focus on the three minerals most commonly depleted by semaglutide GI effects.
Sodium: If you are not on a sodium-restricted diet, adding a pinch of salt to water or meals helps maintain fluid balance. Sodium deficiency is one of the most common causes of persistent lightheadedness during GLP-1 treatment, particularly in users who eat very little due to appetite suppression.
Potassium: Bananas, avocados, sweet potatoes, and leafy greens are rich sources. If dietary intake is insufficient due to reduced appetite, potassium supplements can help, but should not exceed recommended daily amounts without medical guidance, as excess potassium carries its own risks.
Magnesium: Often overlooked, magnesium plays a critical role in nerve function and is commonly depleted by diarrhea. Magnesium glycinate is well-absorbed and gentle on the stomach, making it a good choice for semaglutide users already dealing with GI sensitivity.
If you are considering which supplements to take alongside GLP-1 medications, electrolytes should be at the top of the list. Many users report dramatic improvement in dizziness within 48 hours of starting consistent electrolyte supplementation.
Timing your injections strategically
When you inject matters more than most people realize. The best time of day to take semaglutide is partly a personal preference, but if dizziness is a concern, specific timing strategies can help.
Many users find that injecting in the evening, particularly right before bed, allows them to sleep through the peak GI effects that occur in the first 12-24 hours. If nausea-driven dehydration is contributing to your dizziness, sleeping through the worst of it means you wake up only needing to rehydrate rather than dealing with active nausea all day.
Others prefer morning injections so they can actively manage hydration and food intake during the hours when side effects peak. There is no universally correct answer. The right approach depends on your specific symptom pattern.
Consistency matters more than the specific day. Inject on the same day each week at roughly the same time. This gives your body a predictable rhythm to adapt to, rather than varying the timing and creating irregular side effect windows.
Choosing the best injection site can also influence absorption rate. Abdominal injections tend to absorb fastest, which may produce more intense but shorter-lived side effects. Thigh injections absorb more slowly, potentially smoothing out the initial impact.
Exercise modifications during dizzy periods
Exercise is beneficial during semaglutide treatment, both for weight loss outcomes and overall wellbeing. But exercising while dizzy is asking for trouble.
During the first few days after a dose increase, when dizziness is most likely, modify your routine. Replace high-intensity workouts with walks. Skip exercises that involve rapid position changes (burpees, deadlifts from floor to standing, inversions). Avoid outdoor cycling or activities where a dizzy spell could result in a dangerous fall.
Stay seated during strength training where possible. Machine-based exercises and seated dumbbell work maintain training stimulus without the balance demands of standing compound movements. Swimming is particularly well-suited for dizzy periods because the water supports your body and falling is not a concern.
Hydrate aggressively before, during, and after exercise. Exercise-induced fluid loss on top of semaglutide-related dehydration is a reliable trigger for dizziness. Bring electrolyte drinks to the gym rather than plain water during the adjustment phases.
As dizziness resolves (typically within 7-14 days at each dose level), gradually return to your normal training. If you are working toward weight loss goals and struggling with exercise consistency due to side effects, know that semaglutide drives significant weight loss even without intense exercise. Do not push through dizziness just to maintain a workout schedule.
Supplements and supportive nutrients
Beyond electrolytes, certain supplements may help reduce semaglutide-related dizziness through different mechanisms.
B vitamins: Some semaglutide formulations include B12 for good reason. Reduced food intake can lead to B vitamin deficiencies over time, and B12 deficiency specifically causes dizziness and neurological symptoms. If your formulation does not include B12, consider supplementing separately.
Glycine: This amino acid supports multiple metabolic processes and may help with GI tolerance. Some compounded semaglutide preparations include glycine, and users report improved side effect profiles.
Ginger: For dizziness driven primarily by nausea, ginger supplementation (250mg four times daily) has evidence supporting its anti-nausea effects. It does not address all causes of semaglutide dizziness, but if your lightheadedness is closely tied to nausea episodes, ginger may provide meaningful relief.
Iron: If you are eating significantly less than before starting semaglutide, iron deficiency can develop, particularly in menstruating women. Iron deficiency anemia causes dizziness independent of semaglutide. A simple blood test can rule this out.
SeekPeptides provides comprehensive supplement guides for users navigating GLP-1 treatment, including evidence-based recommendations for managing common side effects through nutrition and supplementation.
Semaglutide dizziness compared to other side effects
Dizziness does not exist in isolation. Understanding how it relates to other semaglutide side effects helps you identify root causes and choose the right management approach.
How dizziness relates to nausea
Nausea and dizziness are frequent companions during semaglutide treatment, but they are not the same thing. Nausea is a gastrointestinal symptom caused by slowed gastric emptying and changes in gut signaling. Dizziness is a neurological or cardiovascular symptom caused by the downstream effects of nausea (dehydration, reduced intake) or by independent mechanisms (blood pressure changes, vestibular effects).
Here is the practical distinction: treating nausea directly (with antiemetics, ginger, or dietary modifications) can prevent the dehydration that causes secondary dizziness. But if your dizziness occurs without nausea, treating it as a nausea problem will not help. You need to address blood sugar, blood pressure, or hydration directly.
Users who experience both symptoms simultaneously should prioritize managing nausea first. Stop the fluid loss, and the dizziness often resolves on its own. The GI side effect management strategies apply broadly across nausea, constipation, diarrhea, and the secondary dizziness they produce.
The fatigue and dizziness overlap
Semaglutide fatigue and dizziness share several root causes: caloric deficit, dehydration, and blood sugar instability. Many users describe a combined experience of feeling tired, foggy, and lightheaded rather than isolated dizziness or isolated fatigue.
This overlap suggests systemic underfeeding or dehydration rather than a medication-specific effect. Your body is not getting enough fuel or fluids to support normal function. The brain, being the most energy-demanding organ, signals distress through both fatigue and dizziness.
GLP-1 fatigue that accompanies dizziness usually responds to the same interventions: better hydration, more consistent meals, and electrolyte supplementation. If you are addressing dizziness alone without seeing improvement, look at the fatigue component. They are likely the same problem presenting through different symptoms.
Does semaglutide give you energy over time? Many users report that after the initial adjustment period, energy levels actually improve. Weight loss reduces physical burden, better blood sugar control eliminates energy crashes, and improved sleep quality contributes to daytime alertness. The fatigue-dizziness combination is typically a phase, not a permanent state.
Semaglutide versus tirzepatide: dizziness comparison
For users considering switching medications due to persistent dizziness, the comparison between semaglutide and tirzepatide side effects is relevant.
The vestibular disorder study mentioned earlier found that semaglutide carried a higher risk of vestibular disorders than tirzepatide. At three years, semaglutide users had roughly double the relative risk (RR 2.04). The researchers hypothesized that tirzepatide dual action on both GIP and GLP-1 receptors might provide a protective effect.
However, both medications cause dizziness through the shared mechanisms of GI side effects, dehydration, and blood sugar changes. Tirzepatide fatigue and tirzepatide headaches follow similar patterns to semaglutide. The side effect profiles overlap considerably.
If you are currently on semaglutide and experiencing persistent dizziness that does not respond to management strategies, discussing a switch to tirzepatide with your prescriber is reasonable. The conversion chart can guide dose equivalency, though your prescriber should make the final dosing decision.
Conversely, if you switched from tirzepatide to semaglutide and noticed new or worsened dizziness, this aligns with the study data. The reverse switch back is a valid consideration.
When semaglutide dizziness signals something serious
Most semaglutide-related dizziness is manageable and self-limiting. But some presentations warrant immediate medical attention. Knowing the difference can prevent a minor side effect from becoming a serious problem.
Warning signs that need immediate attention
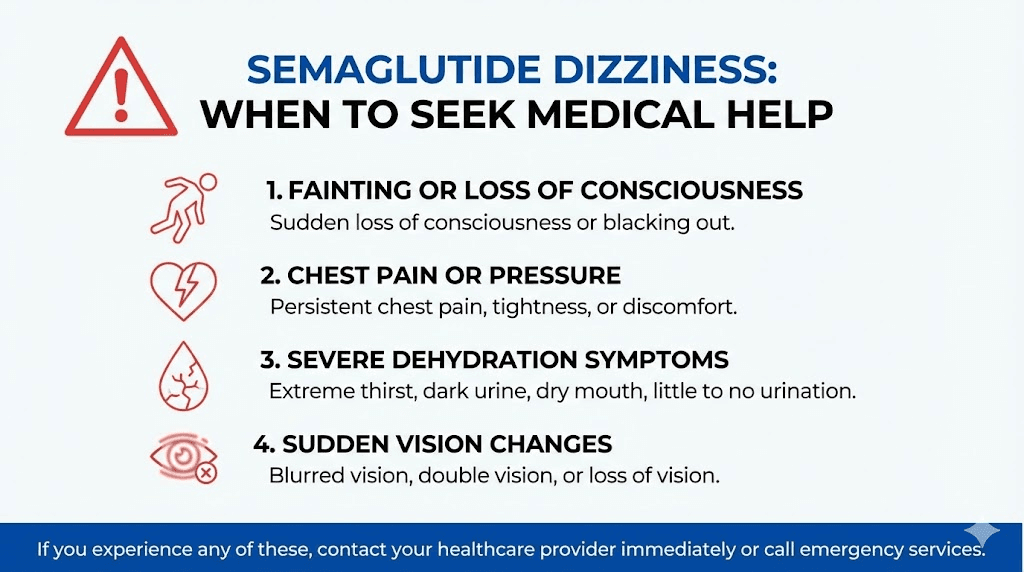
Call your healthcare provider or seek emergency care if your dizziness is accompanied by any of the following:
Fainting or near-fainting. A single lightheaded moment is normal. Actually losing consciousness is not. Fainting indicates blood pressure has dropped low enough to temporarily stop adequate brain perfusion. This needs evaluation, period.
Chest pain or palpitations. Dizziness combined with chest discomfort, racing heart, or irregular heartbeat could indicate a cardiac issue unrelated to semaglutide or could signal severe electrolyte imbalance affecting heart rhythm. Do not wait this out.
Severe, unrelenting dizziness lasting more than 24 hours. Brief episodes after dose changes are expected. Dizziness that does not improve at all after a full day, especially if you are well-hydrated and have eaten, suggests something beyond typical adjustment.
Signs of severe dehydration: very dark urine or no urination for 8+ hours, dry cracked lips, rapid heartbeat at rest, confusion, or inability to keep any fluids down. This is a medical situation requiring possible IV fluid replacement.
Vision changes. If dizziness comes with blurred vision, double vision, or vision loss, seek immediate evaluation. This could indicate neurological involvement that requires urgent assessment.
Severe headache. Dizziness paired with the worst headache of your life warrants emergency evaluation to rule out cerebrovascular events.
The general principle: dizziness that is brief, mild, and improving does not require emergency care. Dizziness that is severe, worsening, or accompanied by other concerning symptoms does.
Dizziness with other medications
Semaglutide does not exist in a vacuum. Many users take it alongside other medications, and drug interactions can amplify dizziness significantly.
Blood pressure medications (antihypertensives): The most common interaction. As semaglutide promotes weight loss and directly lowers blood pressure, your existing antihypertensive dose may become too strong. This creates additive blood pressure lowering, resulting in orthostatic hypotension and dizziness. Regular blood pressure monitoring and dose adjustments are critical.
Diabetes medications (insulin, sulfonylureas): Combined hypoglycemia risk is real and documented. If you are taking insulin or sulfonylureas with semaglutide, blood sugar monitoring should be frequent, especially during dose titration. Your prescriber may need to reduce your insulin dose as semaglutide takes effect.
Diuretics (water pills): Diuretics increase fluid loss. Semaglutide causes fluid loss through GI effects and natriuresis. The combination can accelerate dehydration and electrolyte depletion, dramatically increasing dizziness risk.
Users who combine semaglutide with phentermine should be particularly aware, as phentermine can also affect blood pressure and heart rate. The interaction profile between these medications deserves careful monitoring.
Always provide your prescriber with a complete list of medications, supplements, and over-the-counter products you are taking. Some interactions are subtle and only become apparent when all factors are considered together.
When to consider stopping or dose adjustments
Stopping semaglutide should not be a first reaction to dizziness. But it is appropriate in certain circumstances.
Persistent dizziness despite adequate management: If you have optimized hydration, nutrition, and electrolytes, given each dose level a full 3-4 weeks to adapt, and dizziness still significantly impairs your daily life, dose reduction or medication change is reasonable.
Recurrent falls: If dizziness has caused you to fall more than once, the injury risk outweighs the medication benefit until the issue is resolved. Your prescriber may hold you at a lower dose or switch to a different approach.
Vestibular symptoms: If you develop true vertigo (spinning sensation) rather than general lightheadedness, vestibular evaluation is appropriate before continuing dose escalation. BPPV can be treated specifically with repositioning maneuvers, and treatment may resolve the issue without requiring medication changes.
The good news: most users do not need to stop. Dose adjustment, slower titration, or addressing underlying factors (dehydration, electrolytes, concurrent medications) resolves dizziness for the vast majority. Discontinuation for dizziness alone is uncommon in clinical practice.
Be aware that semaglutide withdrawal can occur if you stop abruptly, with appetite returning rapidly. If stopping is necessary, discuss a tapering approach with your prescriber.
Long-term outlook: does semaglutide dizziness go away
For most users, the answer is yes. Understanding the long-term trajectory helps set realistic expectations and reduces anxiety during the adjustment period.
The majority experience resolution
Clinical data and real-world reports consistently show that semaglutide-related dizziness is most intense during the titration phase and improves significantly once a stable maintenance dose is reached. The 8% incidence rate from clinical trials captures any dizziness event, but the proportion of users with persistent dizziness at their maintenance dose is much lower.
The typical long-term pattern looks like this. Months 1-4 (during dose escalation) bring intermittent dizziness, usually brief and tied to dose increases. Months 5-6 (early maintenance) show significant improvement, with most users reporting no dizziness at their stable dose. Months 7+ (established maintenance) are characterized by minimal to no dizziness for the vast majority of users.
Users who continue to experience dizziness beyond six months of stable dosing represent a small subset and typically have identifiable contributing factors: ongoing inadequate hydration, concurrent medications causing additive effects, undiagnosed vestibular conditions, or electrolyte imbalances from chronically reduced food intake.
For those tracking their progress, semaglutide one-month results often show the most side effects alongside the earliest weight changes. By months 2-3, the side effect profile typically softens considerably while weight loss continues.
Persistent dizziness and what it means
If dizziness persists beyond three months at a stable dose and you have addressed hydration, nutrition, electrolytes, and medication interactions, further investigation is warranted.
Request a comprehensive workup including: complete metabolic panel (with magnesium), CBC to check for anemia, thyroid function tests, blood pressure monitoring (ideally 24-hour ambulatory monitoring), and if vertigo symptoms are present, referral for vestibular function testing.
The real-world study on vestibular disorders showed that risks continued to accumulate over time (0.12% at 6 months to 0.41% at 3 years), suggesting that some vestibular effects may develop later in treatment rather than only during initial titration. If you develop new dizziness or vertigo after months of stable treatment, do not assume it is a normal semaglutide effect. Get it evaluated.
For researchers using peptide protocols alongside GLP-1 medications, understanding the full spectrum of peptide safety and risks helps contextualize side effects and make informed decisions about continuing, modifying, or stopping treatment.
For those serious about optimizing their peptide protocols with evidence-based guidance, SeekPeptides offers comprehensive protocols, detailed side effect management guides, and a community of thousands of researchers who have navigated these exact questions.
Frequently asked questions
How long does semaglutide dizziness last?
Most semaglutide-related dizziness lasts 3-14 days after starting the medication or increasing the dose. Individual episodes typically last minutes to hours. Persistent dizziness lasting more than two weeks at a stable dose warrants medical evaluation to rule out dehydration, electrolyte imbalances, or blood pressure issues. Reference the semaglutide timeline guide for detailed week-by-week expectations.
Can semaglutide cause vertigo?
Yes. A large real-world study of over 419,000 semaglutide users found a significantly elevated risk of vestibular disorders, with hazard ratios of 4-5 times higher than non-users. Benign paroxysmal positional vertigo (BPPV) was the most common vestibular diagnosis, occurring at a median of 2.8 months after starting treatment. If you experience spinning sensations rather than general lightheadedness, discuss vestibular evaluation with your healthcare provider.
Does dizziness mean my semaglutide dose is too high?
Not necessarily. Dizziness during dose escalation is common and usually resolves within 1-2 weeks as the body adapts. However, severe or persistent dizziness that does not improve with hydration and proper nutrition may indicate that the current dose increase was too aggressive. Your prescriber may recommend staying at your current dose longer before escalating. Check the semaglutide dosage chart to understand standard titration timelines.
Should I eat before or after my semaglutide injection to prevent dizziness?
Having a balanced meal 1-2 hours before your injection can help stabilize blood sugar and reduce dizziness risk. Avoid injecting on a completely empty stomach. After injection, continue eating regular meals on schedule even if appetite is reduced. Following a structured semaglutide diet plan with consistent meal timing helps prevent blood sugar-related dizziness throughout the week.
Is semaglutide dizziness worse than tirzepatide dizziness?
Research suggests it may be, at least for vestibular-type dizziness. The real-world cohort study found semaglutide users had roughly double the risk of vestibular disorders compared to tirzepatide users at three years (relative risk 2.04). For general lightheadedness caused by GI effects and dehydration, both medications carry similar risks. If persistent dizziness is a major concern, discuss the side effect differences with your prescriber.
Can I drive while experiencing semaglutide dizziness?
You should not drive during active dizzy episodes. If dizziness is unpredictable and occurring frequently, particularly during the first few days after a dose change, avoid driving until symptoms stabilize. Plan your injection timing so that the peak side effect window (first 24-48 hours) does not coincide with situations requiring full alertness and coordination.
Does drinking alcohol make semaglutide dizziness worse?
Yes. Alcohol is a vasodilator that lowers blood pressure and acts as a diuretic that promotes fluid loss. Both effects compound the mechanisms already causing semaglutide-related dizziness. Even moderate alcohol consumption can trigger or worsen lightheadedness during treatment. The alcohol and semaglutide interaction deserves careful consideration, particularly during dose escalation phases.
Will taking semaglutide with B12 reduce dizziness?
Semaglutide with B12 formulations may help prevent dizziness related to B12 deficiency, which can develop over time due to reduced food intake on GLP-1 medications. B12 deficiency causes neurological symptoms including dizziness, tingling, and cognitive fog. However, B12 supplementation will not address dizziness caused by dehydration, blood pressure changes, or blood sugar instability. It addresses one potential contributing factor, not all of them.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your balance stay steady, your hydration stay consistent, and your protocols stay effective.