Feb 24, 2026

What if the biggest factor holding back your semaglutide results is not the dose, the brand, or even the injection schedule? What if it is what you eat?
Most people start semaglutide expecting the medication to handle everything. They assume the appetite suppression will kick in, the weight will drop, and nutrition will sort itself out naturally. For some, it does. For many others, the wrong food choices sabotage results, amplify side effects, and accelerate muscle loss that nobody warned them about. Research shows that roughly 40 percent of the weight lost on semaglutide comes from lean mass, including muscle. That number is not inevitable. It depends almost entirely on what lands on your plate.
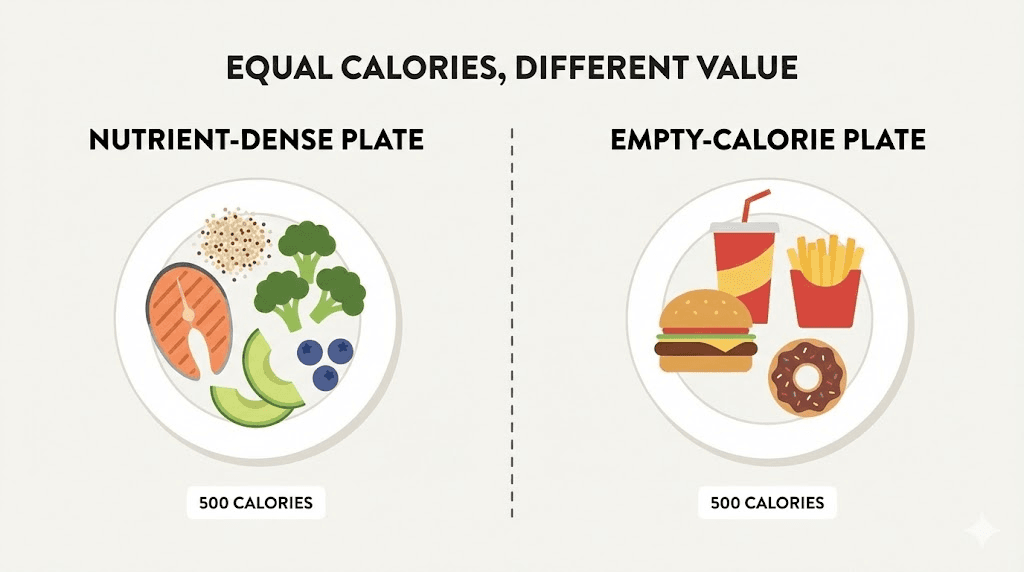
The challenge is that semaglutide fundamentally changes how your body processes food. Gastric emptying slows dramatically. Appetite signals shift. Caloric intake drops by 24 percent on average across all meals. When you eat less overall, every bite carries more weight. The nutrients you choose, the protein you prioritize, and the foods you avoid all matter more than they did before you started the medication. A 2,000-calorie diet has room for nutritional mistakes. A 1,200-calorie diet does not.
This guide covers the specific foods that make semaglutide work harder, the foods that fight against it, and the practical eating strategies that protect muscle, prevent nutrient deficiencies, and maximize weight loss. Whether you are in the first week of your 0.25 mg starting dose or months into a full compounded semaglutide protocol, what you eat determines whether the medication delivers transformative results or disappointing ones. SeekPeptides built this resource because the medication is only half the equation. The food is the other half.
Why nutrition matters more on semaglutide than off it
Semaglutide belongs to the GLP-1 receptor agonist class. It mimics the glucagon-like peptide-1 hormone that your body produces naturally after eating. This hormone tells your brain you are full, slows the rate at which food leaves your stomach, and helps regulate blood sugar by stimulating insulin release. The medication amplifies all of these effects far beyond what natural GLP-1 achieves.
The result is profound appetite suppression. Clinical trials show participants eating 24 percent fewer calories per day without deliberate restriction. That sounds like a dream until you realize the implications. If your total intake drops from 2,000 calories to roughly 1,500, you have 25 percent less nutritional real estate to work with. Every meal needs to deliver more nutrition per calorie. Every food choice carries greater consequence.
Here is what happens when nutrition falls short on semaglutide. The body still needs protein, vitamins, minerals, and essential fatty acids regardless of how many calories you consume. When intake drops and food quality stays poor, the body pulls from its own reserves. Muscle tissue breaks down for amino acids. Bone density suffers from inadequate calcium and vitamin D. Energy crashes because iron and B vitamins fall short. The scale moves in the right direction, but the body composition underneath tells a different story.
The STEP clinical trials that led to semaglutide FDA approval documented this pattern clearly. Participants lost an average of 14.9 percent of their body weight over 68 weeks on the 2.4 mg dose. Impressive numbers. But body composition analysis revealed that approximately 40 percent of total weight lost came from lean mass. For someone losing 50 pounds, that means roughly 20 pounds of muscle tissue gone alongside 30 pounds of fat. Understanding how GLP-1 medications work helps explain why nutrition decisions matter so much during treatment.
The good news? This ratio is not fixed. Research from the Endocrine Society presented at ENDO 2025 demonstrated that higher protein intake significantly reduces lean mass loss during GLP-1 treatment. The ratio of fat to muscle loss improves dramatically when nutrition is optimized. The medication handles appetite. Your food choices handle everything else.
The protein priority: protecting muscle while losing fat
Protein is not just important on semaglutide. It is the single most critical nutrient in your entire diet during treatment. Nothing else comes close.
When caloric intake drops, the body enters a catabolic state where it breaks down its own tissues for energy and raw materials. Fat tissue is the primary target, which is the whole point. But muscle tissue gets caught in the crossfire. The body cannot selectively burn only fat. It takes from both pools simultaneously. The only way to shift the ratio toward more fat loss and less muscle loss is to flood the system with dietary protein so the body does not need to cannibalize its own muscle for amino acids.
Research on weight loss and muscle preservation consistently shows that protein intake determines lean mass outcomes during caloric restriction. A study published in Diabetes, Obesity and Metabolism examined lean body mass changes during GLP-1 therapy and found that participants consuming higher protein diets preserved significantly more muscle than those eating standard diets.
How much protein you actually need
The general dietary recommendation for protein is 0.8 grams per kilogram of body weight per day. That target was designed for sedentary individuals maintaining their weight. It is woefully inadequate for someone on semaglutide who is actively losing weight.
Current evidence supports substantially higher targets:
Minimum for muscle preservation: 1.2 grams of protein per kilogram of body weight daily
Recommended range: 1.2 to 1.6 grams per kilogram daily
Active individuals doing resistance training: 1.6 to 2.2 grams per kilogram daily
For a 180-pound (82 kg) person, this translates to roughly 98 to 131 grams of protein per day at the recommended range, or up to 180 grams daily if combining semaglutide with serious resistance training. That amount of protein sounds manageable until you realize your appetite has been cut by a quarter. Fitting 120-plus grams of protein into 1,200 to 1,500 calories requires deliberate planning.
The protein-first eating strategy
Because semaglutide suppresses appetite so effectively, many people find themselves unable to finish meals. They take a few bites and feel full. If those first bites are bread, rice, or vegetables, the protein never gets eaten. The solution is simple but non-negotiable. Eat protein first at every meal.
This strategy ensures that even if you cannot finish your plate, the most critical macronutrient has already been consumed. Start with the chicken breast, the eggs, the fish, or the Greek yogurt. Then move to vegetables. Then to grains or other carbohydrates. If you reach your fullness threshold before clearing the plate, the nutritional damage is minimized because the protein is already in.
Aiming for 20 to 30 grams of protein per meal distributes your daily target across three to four eating opportunities. For someone targeting 120 grams daily, that means four meals averaging 30 grams each, a number that most protein-rich foods can deliver in a reasonably sized serving. This approach aligns with what optimized dosing protocols recommend for any compound that affects metabolism. The medication handles the pharmacology. Your eating strategy handles the nutrition.
Why losing muscle matters beyond aesthetics
Muscle loss during weight loss is not just a cosmetic concern. Research presented at the Endocrine Society meeting showed that losing more muscle during semaglutide treatment was linked to less improvement in insulin resistance. In other words, preserving muscle is not optional for metabolic health. It is essential.
Muscle tissue is metabolically active. It burns calories at rest. It regulates blood sugar by absorbing glucose from the bloodstream. It supports joint stability, balance, and functional capacity. When muscle loss accompanies fat loss, the metabolic benefits of weight reduction are partially offset. The scale shows improvement, but the metabolic picture is less clear.
For older adults, the stakes are even higher. Age-related muscle loss, known as sarcopenia, already threatens functional independence. Adding semaglutide-induced lean mass loss on top of age-related decline accelerates the problem. Women and older adults appear particularly vulnerable to muscle loss during GLP-1 treatment, making protein intake and resistance training even more critical for these groups. Resources on peptide strategies for women over 40 explore this intersection in greater detail.

Best protein sources for semaglutide users
Not all proteins are created equal when your stomach empties at half its normal speed. Heavy, greasy protein sources that would digest fine normally can sit in a semaglutide-slowed stomach for hours, causing bloating, nausea, and discomfort. The best protein sources are lean, easy to digest, and nutrient-dense.
Chicken breast
The gold standard. A 4-ounce serving of grilled chicken breast delivers 35 grams of protein with only 4 grams of fat and roughly 187 calories. It digests relatively easily, causes minimal gastrointestinal distress, and works in virtually any meal format. Baked, grilled, or poached, chicken breast is the most efficient protein source available for semaglutide users.
Fish and seafood
Salmon, cod, tilapia, shrimp, and tuna all provide excellent protein with additional benefits. Salmon delivers omega-3 fatty acids that support cardiovascular health and reduce inflammation. A 4-ounce fillet provides roughly 25 grams of protein. White fish like cod and tilapia are even leaner, offering 20 to 25 grams of protein per serving with minimal fat. Shrimp is particularly efficient at 24 grams of protein per 4-ounce serving with under 1 gram of fat.
The omega-3 content in fatty fish provides benefits that extend beyond simple protein delivery. These essential fatty acids support brain health, reduce systemic inflammation, and may help with mood regulation, something relevant given that some semaglutide users report sleep disruptions and mood changes during treatment.
Eggs
Two large eggs provide 12 grams of protein, along with choline, vitamin D, and B vitamins that semaglutide users commonly lack. Eggs are easy to prepare, gentle on the stomach, and extremely versatile. Scrambled, hard-boiled, or made into an omelet with vegetables, they fit into any meal of the day.
The concern about egg cholesterol has been largely dismissed by modern nutrition research. For most people, dietary cholesterol has minimal impact on blood cholesterol levels. The nutrient density of eggs makes them one of the best per-calorie investments during caloric restriction.
Greek yogurt
A single cup of plain nonfat Greek yogurt contains roughly 20 grams of protein. It also delivers probiotics that support gut health, something particularly valuable during semaglutide treatment since the medication affects gastrointestinal function directly. The smooth texture makes it easier to consume during episodes of mild nausea, and it works as a base for both sweet and savory preparations.
Choose plain, unflavored varieties. Flavored Greek yogurts often contain 15 to 20 grams of added sugar per serving, which undermines the blood sugar benefits semaglutide provides. Add your own berries or a small amount of honey if sweetness is needed.
Cottage cheese
One cup of low-fat cottage cheese provides 28 grams of protein. It is one of the most protein-dense foods available per calorie. The casein protein in cottage cheese digests slowly, providing a sustained amino acid release that supports muscle preservation between meals. This makes it an excellent evening snack for protecting muscle during overnight fasting periods.
Turkey
Ground turkey and turkey breast provide lean protein comparable to chicken with slightly different mineral profiles. A 4-ounce serving of turkey breast delivers roughly 30 grams of protein. Ground turkey works well in stir-fries, wraps, and meatball preparations that are gentle on a semaglutide-sensitive stomach.
Legumes and beans
Black beans, lentils, chickpeas, and edamame provide plant-based protein alongside fiber that supports digestion. One cup of cooked lentils delivers 18 grams of protein and 15 grams of fiber. The combination makes legumes exceptionally filling, which can be a double-edged sword on semaglutide. Start with smaller portions. Half a cup alongside a lean protein source adds protein without overwhelming a suppressed appetite.
Legumes also function as prebiotics, feeding beneficial gut bacteria. This matters because semaglutide alters the gut environment, and supporting a healthy microbiome can help manage digestive side effects. The GLP-1 probiotic research explores this gut-brain-medication connection further.
Tofu and tempeh
For plant-based eaters, tofu and tempeh provide complete proteins that are easy to digest. A half-cup serving of firm tofu delivers roughly 20 grams of protein. Tempeh is even more protein-dense at 21 grams per half cup, with the added benefit of fermentation-derived probiotics. Both absorb flavors well and can be prepared in ways that minimize gastrointestinal irritation.
Protein powders
When whole food protein feels impossible due to appetite suppression, a protein shake becomes a practical solution. Whey protein isolate delivers 25 to 30 grams of protein per scoop in a form that requires no chewing and minimal stomach volume. Blend it with unsweetened almond milk, a handful of spinach, and half a cup of frozen berries for a nutrient-dense meal replacement that goes down easier than solid food during high-nausea periods.
Casein protein works better for evening shakes due to its slower digestion profile. Plant-based options like pea protein or rice protein blends serve those with dairy sensitivity, though they may require two scoops to match the amino acid profile of whey. Using the SeekPeptides peptide calculator alongside a nutrition tracker helps ensure daily protein targets are consistently met regardless of appetite fluctuations.
Best vegetables and fruits for semaglutide users
Vegetables and fruits provide vitamins, minerals, fiber, and antioxidants that become critically important when total food intake drops. The key is choosing options that deliver maximum nutrition without excessive volume or digestive burden.
Non-starchy vegetables: your foundation
Non-starchy vegetables should form the base of every meal after protein. They provide bulk, fiber, and micronutrients with minimal calories. The best options for semaglutide users include:
Spinach and leafy greens. Packed with iron, folate, and vitamins A, C, and K. One cup of cooked spinach delivers 6 grams of protein alongside its micronutrient load. Greens are easy to incorporate into omelets, smoothies, and side dishes. They digest quickly and rarely cause gastrointestinal issues.
Broccoli. Three grams of protein per cup plus sulforaphane, a compound with anti-inflammatory and potential anti-cancer properties. Steam or roast lightly. Raw broccoli can cause gas and bloating, especially with slowed gastric emptying.
Zucchini. Low calorie, high water content, and gentle on the stomach. Spiralized zucchini serves as a pasta substitute that pairs well with lean protein and marinara. The high water content supports hydration, which becomes important during semaglutide treatment.
Bell peppers. One medium bell pepper delivers more vitamin C than an orange. The sweetness satisfies cravings without added sugar. Red peppers have the highest nutrient density of all colors. Slice and pair with hummus for a protein-and-vegetable snack.
Cucumbers. Nearly 96 percent water. They hydrate, provide crunch, and contribute potassium. When nausea makes solid food unappealing, cucumber slices often remain tolerable.
Mushrooms. A unique combination of B vitamins, selenium, and vitamin D (especially if sun-exposed). Mushrooms also provide a meaty, umami flavor that makes reduced-calorie meals feel more satisfying.
Asparagus. Rich in folate and prebiotic fiber that feeds beneficial gut bacteria. Roast with a light coating of olive oil and garlic for a side dish that supports both nutrition and digestion.
Starchy vegetables: use strategically
Starchy vegetables like sweet potatoes, butternut squash, and corn provide more carbohydrates and calories than their non-starchy counterparts. They are not off limits, but they require strategic use on semaglutide.
A half cup of roasted sweet potato provides complex carbohydrates for sustained energy alongside beta-carotene and potassium. This is particularly useful on days with resistance training when your muscles need glycogen replenishment. Pairing a small portion of starchy vegetables with lean protein and non-starchy vegetables creates a balanced plate that supports activity levels without excess calories. Understanding how cycle planning works helps structure nutrition around training days versus rest days.
Avoid making starchy vegetables the centerpiece of any meal. A quarter plate of sweet potato alongside a half plate of lean protein and non-starchy vegetables hits a better balance than a full baked potato with a small piece of chicken on the side.
Best fruits for semaglutide users
Fruits provide natural sugars, fiber, vitamins, and hydration. The best choices for semaglutide users are low-glycemic options that do not spike blood sugar.
Berries. Blueberries, strawberries, raspberries, and blackberries are the best fruits for semaglutide users. Low glycemic index. High antioxidant content. Moderate fiber. A half cup of mixed berries contains roughly 40 calories and minimal impact on blood sugar. They work in smoothies, on Greek yogurt, or eaten plain as a snack.
Apples. One medium apple provides 4 grams of fiber and satisfies sweetness cravings. The pectin fiber in apples functions as a prebiotic. Slice and pair with a tablespoon of almond butter for a balanced snack that combines protein, healthy fat, and complex carbohydrates.
Citrus fruits. Oranges, grapefruits, and clementines deliver vitamin C and hydration. Note that citrus can trigger acid reflux in some semaglutide users, especially in the first weeks of treatment. If heartburn is present, limit citrus until the body adapts.
Avocado. Technically a fruit. One third of a medium avocado provides 5 grams of fiber, 7 grams of monounsaturated fat, and 2 grams of protein. The healthy fat content supports hormone production and vitamin absorption. Avocado also provides potassium that helps prevent electrolyte imbalances during weight loss.
Watermelon and cantaloupe. High water content makes these melons excellent for hydration. They are easy to eat during low-appetite periods and provide natural sweetness without excessive caloric density. A cup of watermelon is 92 percent water and delivers lycopene and citrulline alongside its natural sugars.
Best whole grains and complex carbohydrates
Carbohydrates are not the enemy on semaglutide. The wrong carbohydrates are. Refined grains and simple sugars cause rapid blood sugar spikes that work against semaglutide mechanism of action. Complex carbohydrates provide sustained energy, fiber for digestion, and B vitamins that support metabolism.
Quinoa
The standout choice. One cup of cooked quinoa provides 8 grams of protein alongside 5 grams of fiber and 39 grams of complex carbohydrates. It is one of the few plant foods that provides all nine essential amino acids, making it a complete protein. Quinoa works as a base for grain bowls, a side dish alongside protein, or a breakfast porridge alternative to oatmeal.
Oats
Steel-cut or rolled oats provide beta-glucan fiber that specifically supports cholesterol management and blood sugar stability. A half cup of dry oats delivers 5 grams of protein and 4 grams of fiber. Overnight oats prepared with Greek yogurt and berries create a protein-rich breakfast that requires zero morning preparation.
Avoid instant flavored oatmeal packets. They typically contain 12 to 15 grams of added sugar per serving. The blood sugar spike from sweetened oatmeal undermines the glucose regulation that semaglutide provides.
Brown rice
A reliable staple. One cup of cooked brown rice provides 5 grams of protein, 3.5 grams of fiber, and 45 grams of complex carbohydrates. The glycemic index sits lower than white rice, meaning slower glucose absorption and more stable energy levels. Brown rice pairs well with virtually any lean protein and vegetable combination.
Sweet potatoes
Previously mentioned under vegetables, sweet potatoes deserve recognition as a complex carbohydrate source. One medium sweet potato provides 4 grams of fiber, 27 grams of complex carbohydrates, and 103 percent of daily vitamin A needs. The orange flesh indicates high beta-carotene content, a powerful antioxidant that supports immune function during the physiological stress of rapid weight loss.
Whole grain bread and wraps
Whole wheat bread and whole grain tortillas provide convenient carbohydrate vehicles for protein-rich fillings. Look for options with at least 3 grams of fiber per serving and whole grain flour as the first ingredient. A whole wheat wrap with sliced turkey, avocado, and spinach creates a portable high-protein meal that works for busy schedules. Many people on semaglutide find wraps easier to eat than sandwiches because the portion feels smaller and less overwhelming when appetite is suppressed.
Lentils and chickpeas (dual category)
These foods blur the line between protein and carbohydrate sources. One cup of cooked chickpeas provides 15 grams of protein, 12 grams of fiber, and 45 grams of carbohydrates. They function as both a protein contributor and a complex carbohydrate source, making them exceptionally efficient for calorie-restricted diets. Roasted chickpeas serve as a crunchy snack alternative to chips, with dramatically better nutritional value.
Best healthy fats for semaglutide users
Fat has the highest caloric density of any macronutrient at 9 calories per gram, compared to 4 calories per gram for protein and carbohydrates. This makes portion control essential. But eliminating fat entirely is a mistake that leads to hormone disruption, poor vitamin absorption, and dry skin and hair.
The key is choosing healthy fat sources and controlling portions carefully.
Olive oil. The Mediterranean diet staple. One tablespoon provides 14 grams of primarily monounsaturated fat. Use for light cooking and salad dressings. The polyphenols in extra virgin olive oil provide anti-inflammatory benefits that extend beyond simple caloric value.
Avocado. Already discussed as a fruit, but its fat profile deserves emphasis. Monounsaturated fat from avocado supports satiety between meals. A quarter to a third of a medium avocado per serving adds healthy fat without excessive calories.
Nuts and seeds. Almonds, walnuts, chia seeds, flaxseeds, and pumpkin seeds provide healthy fats alongside protein and fiber. The portion control challenge is real. A quarter cup of almonds contains 207 calories. Pre-portioned servings prevent accidental overconsumption.
Walnuts specifically provide alpha-linolenic acid, a plant-based omega-3 fatty acid. Chia seeds deliver 5 grams of fiber per tablespoon alongside omega-3 content. Flaxseeds provide lignans with potential hormone-balancing properties. These small additions to meals create outsized nutritional impact.
Fatty fish. Salmon, mackerel, sardines, and herring provide EPA and DHA omega-3 fatty acids in their most bioavailable form. Two to three servings of fatty fish per week provides the omega-3 intake associated with cardiovascular protection and reduced inflammation in clinical studies.
What to limit: saturated fats from red meat, full-fat dairy, butter, and coconut oil. These fats slow gastric emptying further on top of semaglutide already slowed digestion, increasing nausea risk. They also carry higher cardiovascular risk profiles than unsaturated alternatives. A small amount of butter on vegetables will not derail results, but making saturated fat a dietary staple during semaglutide treatment creates unnecessary digestive burden and health risk.
Foods that make semaglutide work harder
Certain foods create synergistic effects with semaglutide mechanism of action. They support the same metabolic pathways the medication targets, amplifying results beyond what either diet or medication achieves alone.
Prebiotic fiber foods
Semaglutide affects the gut environment. The medication slows gastric emptying and alters motility patterns throughout the digestive tract. Prebiotic fibers feed the beneficial bacteria that maintain healthy gut function under these changed conditions.
The best prebiotic foods include garlic, onions, leeks, asparagus, bananas (slightly underripe), Jerusalem artichokes, and chicory root. These foods contain inulin, fructooligosaccharides, and other fermentable fibers that specifically nourish Bifidobacterium and Lactobacillus species. A healthy microbiome supports better gut health outcomes and may reduce the gastrointestinal side effects that many semaglutide users experience.
Research on GLP-1 specific probiotics suggests that the gut microbiome directly influences GLP-1 receptor sensitivity. Supporting gut bacteria through prebiotic foods may enhance the medication effectiveness at the receptor level.
Resistant starch foods
Resistant starch passes through the small intestine undigested, functioning similarly to fiber. It feeds gut bacteria in the colon and produces short-chain fatty acids that support intestinal health. Cooled and reheated potatoes, overnight oats, green bananas, and cooked-then-cooled rice all contain resistant starch.
The practical application is straightforward. Cook a batch of rice or potatoes, refrigerate overnight, then reheat. The cooling process transforms some of the digestible starch into resistant starch, lowering the glycemic impact and adding prebiotic benefit. This simple preparation change improves the nutritional profile of common foods without changing their taste or appearance.
Fermented foods
Yogurt, kefir, sauerkraut, kimchi, and miso provide live probiotic cultures that directly populate the gut with beneficial bacteria. During semaglutide treatment, when the gut environment is altered by slowed motility, maintaining microbial diversity becomes especially important.
Fermented foods also tend to be easier to digest than their unfermented counterparts. Kefir is often tolerated by people who struggle with regular milk. Fermented vegetables like sauerkraut provide fiber alongside probiotics. These foods serve double duty, supporting both nutrition and digestive comfort during treatment.
Ginger
Ginger deserves its own mention because it directly addresses the most common semaglutide side effect. Nausea. Fresh ginger, ginger tea, and crystallized ginger all provide gingerol compounds that reduce nausea through serotonin receptor antagonism in the gut. Clinical studies on ginger for nausea show effectiveness comparable to some anti-nausea medications.
Adding fresh ginger to stir-fries, sipping ginger tea between meals, or keeping crystallized ginger on hand for acute nausea episodes provides a food-based management strategy that complements the medication rather than adding another pharmaceutical to the mix.
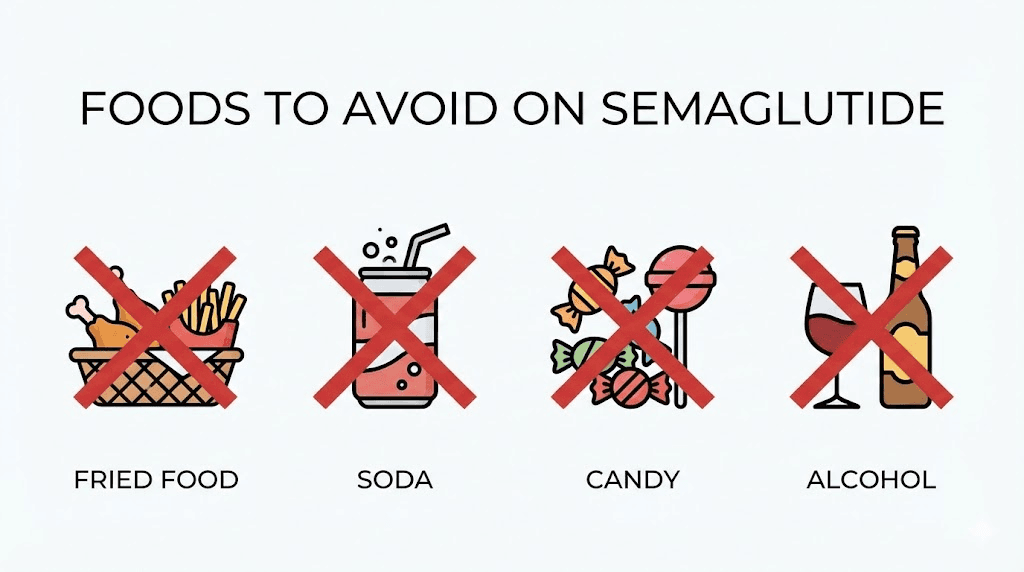
Foods to avoid on semaglutide and why each one matters
Some foods fight directly against what semaglutide is trying to accomplish. Others amplify side effects to the point of misery. Knowing which foods to limit, and understanding why, prevents the trial-and-error approach that makes the first weeks of treatment unnecessarily difficult.
Fried and greasy foods
This is the number one food category to avoid. Fried foods are high in saturated fat, which takes the longest of any macronutrient to digest. On semaglutide, where gastric emptying is already slowed by 30 to 50 percent, adding a high-fat meal creates a digestive traffic jam. Food sits in the stomach for hours. Nausea intensifies. Bloating becomes severe. Acid reflux worsens.
French fries, fried chicken, onion rings, fish and chips, donuts, and fast food burgers fall into this category. So do cream-based soups, alfredo sauces, and heavily buttered dishes. If the food leaves a grease stain on a napkin, it will likely cause problems during semaglutide treatment.
This does not mean all fat is banned. The healthy fats discussed earlier, olive oil, avocado, nuts, and fatty fish, digest differently and in smaller amounts. The issue is concentrated, saturated, and trans fats in large portions.
Sugary foods and beverages
Semaglutide helps regulate blood sugar through insulin signaling. Consuming large amounts of sugar works directly against this mechanism. A can of regular soda contains 39 grams of sugar. That sugar hits the bloodstream rapidly, causing a glucose spike that forces the pancreas to produce a surge of insulin, even with semaglutide on board.
The more concerning issue is that sugary foods represent wasted caloric real estate. A 250-calorie candy bar provides zero protein, minimal vitamins, and no fiber. Those same 250 calories could deliver 35 grams of protein from a chicken breast or 20 grams of protein from a cup of Greek yogurt with berries. When total intake is limited by appetite suppression, every calorie needs to earn its place.
The foods to limit include regular soda, fruit juice, candy, cookies, cake, ice cream, sweetened yogurts, and breakfast cereals with more than 8 grams of sugar per serving. Sugar-sweetened coffee drinks are a particularly sneaky source. A medium caramel frappuccino can contain 50 or more grams of sugar.
Alcohol
Alcohol and semaglutide create a problematic combination for several reasons. Alcohol irritates the stomach lining, compounding the gastrointestinal effects of the medication. It provides empty calories, 7 per gram, without nutritional value. It impairs judgment around food choices. And it can cause unpredictable blood sugar fluctuations, especially in people using semaglutide for type 2 diabetes management.
Some semaglutide users report that their alcohol tolerance decreases significantly during treatment. One or two drinks may produce effects that previously required three or four. This altered tolerance creates both safety and caloric concerns.
Complete abstinence is not strictly necessary for everyone. But limiting alcohol to occasional, moderate consumption, one drink for women, two for men, on days without gastrointestinal symptoms, represents a reasonable approach. Clear spirits with non-caloric mixers carry the least digestive burden if alcohol is consumed.
Spicy foods
Spicy foods trigger capsaicin receptors in the stomach lining, increasing acid production and potentially exacerbating nausea and heartburn. During the first four to eight weeks of semaglutide treatment, when the body is adjusting to slowed gastric emptying, spicy foods can make nausea significantly worse.
This is not a permanent restriction for most people. Once the body adapts to the medication and gastrointestinal side effects subside, moderate spice is usually tolerable. But during the adjustment phase, mild seasonings serve everyone better than hot sauces and chili flakes.
Carbonated beverages
Sparkling water, soda, and carbonated energy drinks introduce gas into an already slow-moving digestive system. The carbonation expands in the stomach, creating bloating and pressure that compounds the fullness from slowed gastric emptying. Some people on semaglutide find that even a few sips of sparkling water produces uncomfortable bloating.
Still water, herbal tea, and non-carbonated beverages cause none of these issues. If sparkling water is a strong preference, sipping small amounts throughout the day rather than consuming a full glass at once can minimize the bloating effect.
Highly processed foods
Ultra-processed foods, packaged snacks, fast food, frozen dinners with long ingredient lists, combine multiple problematic elements. High sodium causes water retention and bloating. Artificial additives may exacerbate gastrointestinal sensitivity. High sugar and fat content delivers calories without nutrition. And the hyperpalatability engineering of processed foods can override semaglutide appetite suppression in some individuals, leading to overconsumption of the exact foods that should be avoided.
The general principle is simple. The less processing between the farm and your plate, the better the food works alongside semaglutide. Whole foods, prepared simply, with minimal added ingredients, create the dietary foundation that maximizes the medication effectiveness.
How to eat on semaglutide: timing, portions, and strategy
Knowing what to eat matters. Knowing how to eat on semaglutide matters just as much. The medication changes the mechanics of digestion, and eating strategies need to adapt accordingly.
Smaller, more frequent meals
The standard three-meals-a-day structure often fails on semaglutide. A full dinner plate that felt normal before treatment now feels insurmountable. The stomach holds the same volume, but it empties at half the speed. Trying to force a full-sized meal creates nausea, bloating, and discomfort that discourages eating altogether.
Four to six smaller meals spread throughout the day works better for most semaglutide users. Each meal should fit comfortably on a small plate or in a medium bowl. Think appetizer portions, not entree portions. A palm-sized piece of protein, a fist-sized portion of vegetables, and a thumb-sized portion of healthy fat represents a reasonable meal framework.
This approach also distributes protein intake more evenly, which research shows is more effective for muscle preservation than consuming all daily protein in one or two large meals. The body can only utilize roughly 25 to 40 grams of protein per meal for muscle protein synthesis. Spreading protein across four to six eating occasions maximizes the anabolic window at each meal.
Eat slowly and deliberately
The slowed gastric emptying from semaglutide means fullness signals arrive faster than expected. People who eat quickly on semaglutide often overshoot their comfortable fullness threshold before the signal reaches the brain. The result is sudden, intense nausea that can last for hours.
Take 20 to 30 minutes to eat each small meal. Put the fork down between bites. Chew thoroughly. This pacing allows real-time feedback from the stomach to reach the brain before overconsumption occurs. Many semaglutide users describe a specific moment during a meal where appetite simply switches off. Eating slowly helps you notice that moment before it is too late.
Stop eating before you feel full
On semaglutide, the difference between comfortably satisfied and uncomfortably stuffed is smaller than it was before treatment. A few extra bites that previously would have been inconsequential can now trigger nausea and bloating that persists for hours.
Aim for 80 percent fullness. If your stomach feels satisfied but not stretched, stop. Wrap the remaining food and save it for later. The concept of finishing your plate does not serve semaglutide users well. Listening to satiety signals becomes the most important eating skill during treatment.
Do not skip meals
Appetite suppression can be so effective that some people simply stop eating for extended periods. Skipping meals might feel natural when hunger disappears, but it creates problems. Protein intake drops below the threshold needed for muscle preservation. Nutrient deficiencies accumulate. Energy crashes. And when hunger finally returns, it often returns with intensity that leads to poor food choices and overeating.
Even when appetite is minimal, eating something protein-rich every three to four hours keeps the metabolism stable and ensures minimum nutrient intake. A few spoonfuls of Greek yogurt, a protein shake, or a handful of almonds counts as a mini-meal during low-appetite periods. The best approaches to weight loss all share one thing in common: consistency in nutrition, even when the medication makes eating feel unnecessary.
Time meals around your injection
Many semaglutide users find that nausea peaks in the 24 to 48 hours following their weekly injection. Planning lighter meals during this window and saving larger protein-rich meals for days when appetite is stronger creates a practical rhythm.
Injection day and the following day: focus on easy-to-digest foods. Smoothies, Greek yogurt, scrambled eggs, broth-based soups, and mild protein sources.
Days three through seven: appetite typically stabilizes or improves. This is when larger portions, more complex meals, and harder-to-digest foods are better tolerated.
Tracking this pattern over the first few weeks helps establish a predictable eating schedule that maximizes nutrition on good days and minimizes discomfort on challenging ones. Understanding your semaglutide dosing schedule helps coordinate meal planning with injection timing.
Week by week: how appetite changes and what to eat at each stage
Appetite on semaglutide does not change in a straight line. It evolves through distinct phases as the dose escalates and the body adapts. Understanding what to expect at each stage helps prevent both overconsumption and dangerous undereating.
Weeks 1-4: the adjustment phase (0.25 mg)
The starting dose of 0.25 mg is not a therapeutic dose for weight loss. It exists solely to let the gastrointestinal system adjust. Appetite suppression at this level is mild for most people. Some notice almost no change.
Use this window to establish good eating habits before they become harder. Practice the protein-first strategy. Build meals around lean protein, vegetables, and whole grains. Start experimenting with smaller, more frequent meals. Identify which foods sit well and which cause discomfort.
Nausea is most common during this phase but is usually mild. Stick to bland, easy-to-digest foods when it occurs. Crackers, dry toast, plain rice, and clear broths help settle the stomach. Ginger tea between meals provides additional relief.
Weeks 5-8: appetite shifts (0.5 mg)
The first dose increase to 0.5 mg brings more noticeable appetite changes. Most people report reduced hunger between meals, fewer cravings, and smaller portions feeling satisfying. Some describe a quieting of what researchers call food noise, the persistent background thoughts about eating.
This is typically when caloric intake begins dropping measurably. The protein-first strategy becomes critical. Without deliberate effort, protein intake often falls along with total calories, creating the conditions for muscle loss. Track protein for at least the first few weeks at this dose to establish awareness of actual intake versus perceived intake.
Gastrointestinal side effects may return temporarily with the dose increase. Apply the same food strategies: smaller portions, avoid fatty and fried foods, and eat slowly.
Weeks 9-16: the therapeutic window (1.0 to 1.7 mg)
Appetite suppression strengthens significantly at these doses. Most semaglutide users find their daily intake naturally settling between 1,000 and 1,500 calories. The risk of nutrient deficiency increases proportionally.
Meal planning becomes essential rather than optional. Every meal needs to be calculated for maximum nutritional density. Protein shakes may become necessary to hit daily targets when whole food intake drops below comfortable levels. Multivitamin supplementation, discussed in the supplements section below, should begin no later than this phase.
Some people at these doses experience genuine difficulty eating. Food loses its appeal entirely. Meals feel like chores. This is the phase where common mistakes happen. People celebrate the weight loss without realizing they are also losing muscle, depleting nutrient stores, and setting up metabolic problems that become apparent months later.
Weeks 17 and beyond: maintenance dose (2.4 mg)
At the full therapeutic dose, appetite suppression is at its strongest. The body has adapted to the gastrointestinal effects, meaning nausea and digestive discomfort have typically resolved. But appetite remains profoundly suppressed.
This is the phase where diligent nutrition planning pays the greatest dividends. The people who established good habits during the adjustment phase coast through this period with strong nutrition. Those who relied solely on appetite suppression to control intake often find themselves malnourished despite ongoing weight loss.
Regular blood work becomes important at this stage to check for the nutrient deficiencies that accumulate during sustained caloric restriction. Iron, vitamin D, B12, and magnesium are the most commonly depleted nutrients. Your medical provider should be monitoring these markers alongside standard metabolic panels. For a broader view of how peptide safety intersects with nutrition, ongoing monitoring is always part of the protocol.
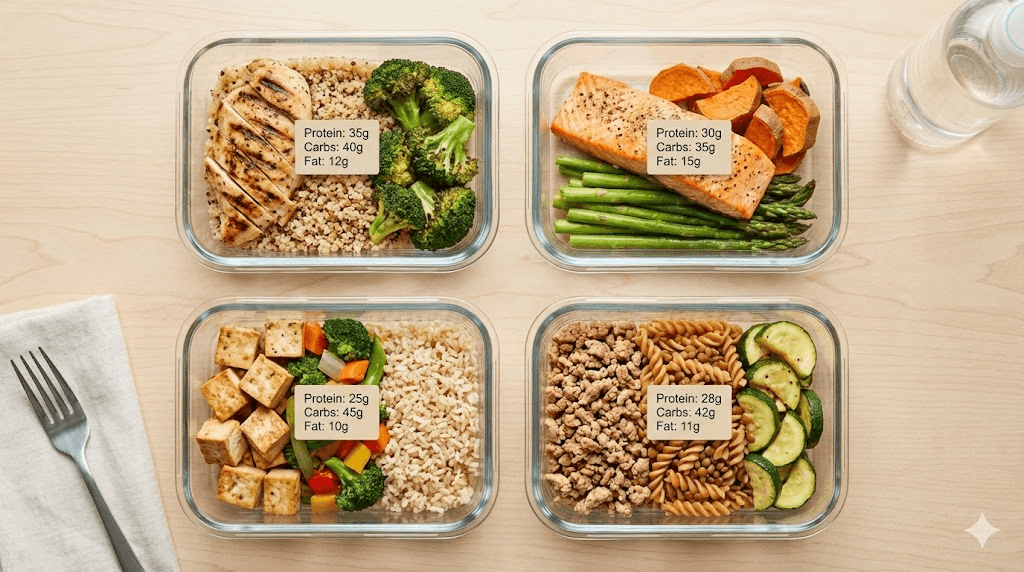
Sample meal plans for semaglutide users
Theory is helpful. Practical examples are better. Below are sample daily meal plans designed for semaglutide users at different caloric levels, all prioritizing protein, micronutrient density, and digestive comfort.
1,200-calorie plan (strong appetite suppression)
Breakfast (300 calories, 25g protein): Two scrambled eggs with spinach and one quarter of an avocado. Side of five strawberries.
Mid-morning snack (150 calories, 20g protein): Three quarters cup plain Greek yogurt with a tablespoon of chia seeds.
Lunch (350 calories, 30g protein): Four ounces grilled chicken breast over mixed greens with cherry tomatoes, cucumber, and one tablespoon olive oil vinaigrette. Half cup cooked quinoa.
Afternoon snack (100 calories, 10g protein): One hard-boiled egg and six almonds.
Dinner (300 calories, 30g protein): Four ounces baked cod with roasted broccoli and a half cup of brown rice. Lemon and herbs for seasoning.
Daily totals: 1,200 calories, 115 grams protein, 40 grams fiber from whole food sources.
1,500-calorie plan (moderate appetite suppression)
Breakfast (350 calories, 30g protein): Protein smoothie with one scoop whey protein, one cup unsweetened almond milk, half cup frozen berries, one tablespoon almond butter, and a handful of spinach.
Mid-morning snack (150 calories, 14g protein): Half cup cottage cheese with a quarter cup blueberries.
Lunch (400 calories, 35g protein): Whole wheat wrap with four ounces sliced turkey, one quarter avocado, lettuce, tomato, and mustard. Small apple on the side.
Afternoon snack (150 calories, 10g protein): One quarter cup mixed nuts with two dried apricots.
Dinner (400 calories, 35g protein): Four ounces grilled salmon, one cup steamed asparagus, and a half cup roasted sweet potato. Olive oil and garlic for flavor.
Evening (50 calories, 6g protein): Small cup of bone broth.
Daily totals: 1,500 calories, 130 grams protein, 35 grams fiber.
1,800-calorie plan (mild appetite suppression or training days)
Breakfast (400 calories, 35g protein): Three-egg omelet with mushrooms, bell peppers, and one ounce feta cheese. One slice whole grain toast. Half a grapefruit.
Mid-morning snack (200 calories, 20g protein): One cup Greek yogurt with granola and berries.
Lunch (450 calories, 35g protein): Grilled chicken grain bowl with half cup quinoa, roasted vegetables, chickpeas, and tahini dressing.
Afternoon snack (200 calories, 15g protein): Protein bar (look for options with less than 5 grams added sugar and at least 15 grams protein).
Dinner (450 calories, 35g protein): Four ounces lean steak with one cup roasted Brussels sprouts and a medium baked sweet potato. Side salad with olive oil and balsamic vinegar.
Evening (100 calories, 10g protein): Half cup cottage cheese.
Daily totals: 1,800 calories, 150 grams protein, 40 grams fiber.
These plans represent templates, not rigid prescriptions. Swap proteins, change vegetables, adjust portions based on your appetite on any given day. The constants are protein targets, meal frequency, and nutrient density. The variables are specific foods, preparation methods, and exact portions. SeekPeptides members access detailed protocol guides and calculators that help customize nutrition plans to individual goals and medication schedules.
Hydration: the overlooked factor
Water does not show up on most semaglutide food lists. It should. Dehydration is one of the most common and most overlooked problems during GLP-1 treatment.
When appetite decreases, thirst often decreases alongside it. People who previously drank water with meals find themselves eating less and therefore drinking less. The gastrointestinal side effects of semaglutide, particularly nausea, vomiting, and diarrhea, accelerate fluid loss. And the metabolic process of burning fat itself requires adequate hydration to function optimally.
How much water semaglutide users need
The general recommendation is a minimum of 64 ounces (eight cups) of water daily, but this baseline often falls short for semaglutide users. A more individualized target is half your body weight in ounces. A 180-pound person would aim for 90 ounces daily. Add an additional 16 ounces for each hour of physical activity.
These numbers sound manageable until you realize that nausea makes large volumes of water unappealing, and slowed gastric emptying means water sits in the stomach longer than usual, contributing to fullness and bloating. The solution is frequent, small sips rather than infrequent large glasses.
Hydration strategies that work
Keep a water bottle visible at all times. Set hourly reminders if needed. Sip between meals rather than with meals, as drinking large amounts of water alongside food compounds the fullness effect and may worsen nausea. Herbal teas count toward hydration totals and provide flavor variety without calories. Ginger tea specifically offers the dual benefit of hydration and nausea relief.
Electrolyte balance matters alongside total fluid intake. When food intake drops and water intake increases, the ratio of electrolytes to fluid can shift. Adding a pinch of salt to meals, consuming potassium-rich foods like bananas and avocado, and considering a sugar-free electrolyte supplement helps maintain balance. Signs of electrolyte imbalance include muscle cramps, fatigue, dizziness, and headaches, symptoms that overlap with semaglutide side effects and may be mistakenly attributed to the medication alone.
Water-rich foods also contribute to hydration. Watermelon, cucumber, celery, lettuce, and broth-based soups provide fluid alongside nutrients. On days when drinking water feels particularly challenging, these foods help bridge the gap between actual intake and target.
Signs of dehydration to watch for
Dark yellow urine is the most reliable indicator. Aim for pale straw color throughout the day. Other signs include headaches, dry mouth, fatigue, dizziness when standing, constipation, and reduced urine output. Constipation specifically deserves attention because it is already a common semaglutide side effect. Dehydration makes it substantially worse. Adequate water intake is the first and most effective treatment for semaglutide-related constipation before adding any fiber supplements or laxatives.
Supplements and nutrient deficiency prevention
A joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society specifically addressed nutritional priorities during GLP-1 therapy. Their conclusion was clear: caloric restriction of 16 to 39 percent during semaglutide treatment creates significant risk for insufficient intake of essential vitamins and minerals.
The nutrients most commonly at risk include iron, calcium, magnesium, zinc, and vitamins A, D, E, K, B1, B12, and C. This is not a theoretical concern. These deficiencies develop because reduced caloric intake means reduced nutrient intake, even when food quality is high. You simply cannot get the recommended daily allowance of all essential nutrients from 1,200 to 1,500 calories without strategic supplementation.
Essential supplements for semaglutide users
A high-quality multivitamin. This is the baseline. Choose a reputable brand that provides at least 100 percent of the daily value for iron, B vitamins, vitamin C, vitamin D, and zinc. Take it with food to maximize absorption and minimize stomach irritation.
Vitamin D3 with K2. Vitamin D deficiency is endemic in the general population and worsens during weight loss. Vitamin D supports bone health, immune function, and mood. Vitamin K2 directs calcium to bones rather than arteries. A combined supplement providing 2,000 to 5,000 IU of D3 and 100 to 200 mcg of K2 covers most needs. Get baseline levels tested and adjust accordingly.
Magnesium. Involved in over 300 enzymatic reactions. Supports muscle function, sleep quality, and bowel regularity. Magnesium glycinate is the best-tolerated form with the least gastrointestinal irritation, an important consideration on semaglutide. A dose of 200 to 400 mg taken at bedtime also supports sleep, relevant given that some users report sleep disruptions on semaglutide.
Vitamin B12. Methylcobalamin (methylated B12) is the preferred form. B12 supports energy production, nerve function, and red blood cell formation. Deficiency causes fatigue, weakness, and neurological symptoms that mimic semaglutide side effects. Sublingual tablets bypass potential absorption issues in the gastrointestinal tract.
Omega-3 fatty acids. If fatty fish consumption is less than two servings per week, a fish oil or algae-based omega-3 supplement providing at least 1,000 mg combined EPA and DHA fills the gap. These essential fatty acids support cardiovascular health, brain function, and inflammation management.
Calcium. Particularly important for women and older adults during rapid weight loss, which can accelerate bone density loss. A supplement providing 500 to 600 mg of calcium citrate (the better-absorbed form) taken separately from iron-containing supplements ensures adequate intake.
When to start supplementing
Ideally, supplementation begins when semaglutide treatment begins. Waiting until deficiency symptoms appear means the damage has already progressed. Proactive supplementation prevents the problem rather than treating it after the fact.
Blood work before starting semaglutide establishes baseline levels. Follow-up testing every three to six months identifies emerging deficiencies before they cause symptoms. Common panels to request include complete metabolic panel, vitamin D, B12, iron studies, and magnesium. Your medical provider can add or remove tests based on individual risk factors.
The intersection of peptide research and nutrition science continues to evolve. Staying current with evidence-based recommendations ensures that supplementation strategies align with the latest findings rather than outdated or generic advice.
Managing nausea through food choices
Nausea is the most commonly reported side effect of semaglutide. It affects 20 to 44 percent of users depending on the dose level. While nausea typically improves over the first few weeks at each dose, strategic food choices can reduce its severity and duration dramatically.
Foods that help with semaglutide nausea
Plain crackers and dry toast. The BRAT diet approach (bananas, rice, applesauce, toast) works for semaglutide nausea just as it does for other types. Bland, starchy foods absorb stomach acid and provide easy-to-digest calories during acute nausea episodes.
Ginger in any form. Fresh ginger root, ginger tea, ginger chews, and even ginger ale (flat, to avoid carbonation issues) all provide nausea relief. Gingerol compounds in ginger antagonize serotonin receptors in the gut that trigger the nausea response. Clinical studies demonstrate effectiveness at doses of 250 mg to 1 gram of ginger per day.
Broth-based soups. Clear chicken broth, vegetable broth, and miso soup provide hydration, electrolytes, and mild nutrition without the volume or fat content that triggers nausea. Bone broth adds collagen protein as a bonus. Sip slowly throughout the day during high-nausea periods.
Cold foods. Many semaglutide users report that cold foods are better tolerated than hot foods during nausea episodes. The aroma from hot foods can intensify queasiness. Cold Greek yogurt, chilled fruit, smoothies, and cold protein shakes bypass this trigger.
Peppermint tea. Peppermint has mild antispasmodic properties that relax the smooth muscle of the gastrointestinal tract. A cup of peppermint tea after eating can reduce bloating and post-meal nausea. Avoid peppermint if acid reflux is present, as it can relax the lower esophageal sphincter and worsen heartburn.
Eating patterns that minimize nausea
Eat before the nausea peak. Most semaglutide users find nausea worst in the morning and after the first meal of the day. Having a small, bland breakfast immediately upon waking, before nausea has a chance to build, often helps. An empty stomach on semaglutide frequently feels worse than a gently fed one.
Avoid lying down immediately after eating. The slowed gastric emptying means food remains in the stomach longer. Lying down increases the risk of acid reflux and worsens the sensation of fullness that contributes to nausea. Stay upright for at least 30 minutes after eating.
Time heavy meals away from injection day. If you inject on Fridays, plan lighter meals for Friday and Saturday, and save larger protein-rich meals for midweek when appetite is typically better. This injection-aware eating pattern reduces the worst nausea episodes while ensuring adequate nutrition across the full week.
Common nutrition mistakes on semaglutide
After reviewing research and hearing from thousands of semaglutide users, patterns emerge. The same mistakes appear repeatedly, and nearly all of them are preventable.
Mistake 1: treating semaglutide as a license to eat anything
The appetite suppression is so effective that some people assume food quality does not matter anymore. They eat less, but what they eat is processed food, fast food, and sugar. Weight loss occurs initially because the caloric deficit from appetite suppression overrides poor food quality. But muscle loss accelerates, nutrient deficiencies develop, and the weight loss plateau arrives sooner and harder than it should.
Semaglutide does not change what your body needs nutritionally. It changes how much you eat. If the reduced intake consists of nutritionally empty food, the body suffers even as the scale improves.
Mistake 2: not tracking protein
This is the most damaging mistake. Without tracking, most semaglutide users underestimate their protein intake by 30 to 50 percent. They think they are eating enough protein because they have chicken at dinner. But dinner provides 30 grams, and the rest of the day provided maybe 20 grams from scattered sources, totaling 50 grams against a target of 120. Tracking protein for even two weeks reveals the gap and allows correction before significant muscle loss occurs.
Mistake 3: skipping meals entirely
When appetite disappears, the temptation to skip meals feels natural. Why eat when you are not hungry? Because your body still needs fuel, protein, vitamins, and minerals regardless of whether your brain sends a hunger signal. Extended fasting on semaglutide does not produce better results. It produces worse body composition, more muscle loss, and higher deficiency risk.
Mistake 4: drinking calories instead of eating protein
Fruit juice, sweetened coffee drinks, smoothies loaded with fruit but no protein, and alcoholic beverages all consume caloric budget without contributing to protein targets. A large fruit smoothie from a popular chain can contain 400 calories and 80 grams of sugar with 2 grams of protein. Those 400 calories could have been a protein-rich meal that preserved muscle and provided lasting satiety.
Mistake 5: avoiding all fat
The fear of fat on semaglutide leads some people to eliminate fats entirely. This creates problems. Fat-soluble vitamins (A, D, E, K) require dietary fat for absorption. Hormones require cholesterol and fatty acids for production. Cell membranes require phospholipids. Skin and hair suffer from fat deprivation. Including small amounts of healthy fats at each meal supports all of these functions without derailing weight loss.
Mistake 6: ignoring hydration
Already discussed in its own section, but it bears repeating here. Dehydration is stealthy. It builds gradually and produces symptoms that overlap with semaglutide side effects. Many people attribute their headaches, fatigue, and constipation entirely to the medication when inadequate water intake is the primary cause. Addressing hydration often resolves symptoms that seemed medication-related.
Mistake 7: not adapting as the dose changes
What works at 0.25 mg may not work at 1.0 mg. Appetite drops further with each dose increase. Meals that felt appropriate at the starting dose become too large at higher doses. Calorie and protein targets that worked early in treatment need adjustment as intake patterns shift. Nutrition strategy should evolve with each dose escalation, not remain static. For people considering switching medications, the semaglutide to tirzepatide switching guide covers how nutrition needs change between GLP-1 and GLP-1/GIP compounds.
Frequently asked questions
Can I eat whatever I want on semaglutide?
Technically, yes. Practically, no. Semaglutide does not restrict what you can eat, but it dramatically changes the consequences of poor food choices. With reduced caloric intake from GLP-1 appetite suppression, every calorie needs to deliver nutrition. Eating junk food in smaller quantities still results in nutrient deficiencies, muscle loss, and suboptimal body composition outcomes.
How much protein do I need on semaglutide?
Research supports 1.2 to 1.6 grams of protein per kilogram of body weight daily for muscle preservation during GLP-1 treatment. For active individuals combining semaglutide with resistance training for muscle maintenance, targets of 1.6 to 2.2 grams per kilogram are appropriate. Eat protein first at every meal to ensure targets are met before fullness hits.
What should I eat when I feel nauseous on semaglutide?
Bland, easy-to-digest foods work best during nausea episodes. Plain crackers, dry toast, clear broth, cold Greek yogurt, bananas, and ginger tea all help settle the stomach. Avoid fatty, fried, or spicy foods during high-nausea periods. Cold foods are often better tolerated than hot foods because strong aromas can worsen queasiness.
Should I take vitamins while on semaglutide?
Yes. A joint advisory from four major medical organizations specifically recommends supplementation during GLP-1 therapy. At minimum, take a high-quality multivitamin, vitamin D3, and consider additional magnesium, B12, and omega-3 fatty acids. Get baseline blood work and repeat every three to six months to monitor for emerging deficiencies.
Can I drink alcohol on semaglutide?
Moderate, occasional alcohol consumption is not strictly prohibited, but it comes with increased risks during semaglutide treatment. Alcohol irritates the stomach, provides empty calories, impairs food choices, and can cause unpredictable blood sugar fluctuations. Many users report significantly reduced alcohol tolerance. If you choose to drink, limit consumption and expect stronger effects from less alcohol than before treatment.
Why am I not losing weight on semaglutide despite eating well?
Several factors can stall weight loss despite good nutrition. The dose may not yet be at therapeutic levels. Water retention can mask fat loss temporarily. Caloric intake may be higher than perceived, especially from cooking oils, dressings, and beverages. Medication interactions can affect semaglutide efficacy. And weight loss naturally slows as the body approaches a lower set point. If semaglutide versus tirzepatide results differ, the dual-receptor mechanism of tirzepatide may offer an alternative for non-responders.
How do I prevent muscle loss on semaglutide?
Three strategies work together. First, consume adequate protein, minimum 1.2 grams per kilogram of body weight daily. Second, perform resistance training two to three times per week. Third, avoid extreme caloric restriction by eating regular small meals rather than skipping meals entirely. Research shows that combining high protein intake with consistent exercise during GLP-1 treatment preserves the most lean mass. The muscle preservation strategies that work for other peptide protocols apply equally to semaglutide treatment.
Is it normal to not feel hungry at all on semaglutide?
Complete appetite suppression is common, especially at higher doses. While this might feel like the medication working perfectly, it can lead to dangerously low caloric intake if not managed. Even without hunger, aim to eat a minimum of 1,000 to 1,200 calories daily with at least 80 to 100 grams of protein. Set meal reminders if necessary. Think of eating on semaglutide as a task to complete for health rather than a response to hunger signals.
External resources
Nutritional Priorities to Support GLP-1 Therapy - Joint Advisory (PMC)
Endocrine Society: Protein Intake and Muscle Loss Prevention on GLP-1
Effects of Semaglutide on Appetite, Energy Intake, and Food Preference (PMC)
For those serious about maximizing their semaglutide results through evidence-based nutrition, SeekPeptides provides the most comprehensive resource available. Members access personalized protocol guides, dosage calculators, detailed nutrition frameworks, and a community of researchers who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your protein stay high, your nausea stay low, and your results stay consistent.