Feb 22, 2026

Three weeks into your semaglutide protocol, something strange happens. You are exhausted. Genuinely, bone-deep tired. But the moment your head hits the pillow, your brain decides it is wide awake. You lie there. Minutes stretch. An hour passes. You check the clock, do the math on how many hours of sleep you can still get, and the anxiety of that calculation makes everything worse.
Sound familiar? You are not imagining it. And you are not alone.
Thousands of semaglutide users report sleep disruptions after starting treatment, from difficulty falling asleep to waking at 3 AM with a racing mind. The frustrating part is that clinical trials tell one story while real-world experience tells another. The official prescribing information for both Ozempic and Wegovy does not list insomnia as a common side effect. Yet scroll through any GLP-1 forum or community, and sleep complaints dominate the conversation. So what is actually going on? The answer involves a complex interplay between gastrointestinal side effects, metabolic changes, hormonal shifts, and even the way your brain processes neurotransmitters, all triggered or amplified by semaglutide and the rapid changes it produces in your body. This guide breaks down every mechanism, every contributing factor, and every evidence-based strategy for getting better sleep while maximizing your results on semaglutide.
What clinical trials actually say about semaglutide and sleep
Let us start with the data. In the STEP clinical trial program for Wegovy (semaglutide 2.4mg), insomnia rates were roughly the same in the semaglutide group as in the placebo group. That is a significant finding. It suggests that semaglutide itself, as a molecule binding to GLP-1 receptors, does not directly cause insomnia through some pharmacological mechanism the way a stimulant would.
But here is where it gets complicated.
Clinical trials measure specific, predefined endpoints. Sleep quality often is not one of them. Participants report side effects, and those reports get categorized. Nausea gets its own box. Headache gets its own box. But "I have been tossing and turning for two weeks" might not get coded as insomnia if the participant does not use that specific word. The gap between clinical trial data and patient experience is real, and it matters.
What the trials DID capture is fatigue. About 11% of Wegovy users reported unusual tiredness during clinical trials. That number is meaningful. If 11% of people feel significantly more tired during the day, some portion of that group is almost certainly experiencing disrupted nighttime sleep. Fatigue during the day and poor sleep at night are two sides of the same coin. You cannot separate them clinically, even though the trial structure often does.
The side effect profile of semaglutide also includes gastrointestinal symptoms that directly interfere with sleep quality. Nausea affects up to 20% of users. Heartburn and acid reflux affect roughly 2%. Abdominal discomfort is common during dose escalation. Each of these symptoms can fragment sleep without the patient ever connecting the two experiences. You might wake at 2 AM feeling "off" without realizing it was mild nausea or reflux that pulled you from deep sleep.
The FDA Adverse Event Reporting System data
Beyond clinical trials, the FDA Adverse Event Reporting System (FAERS) collects real-world reports from patients and healthcare providers. Analysis of FAERS data for semaglutide does show sleep-related complaints, including insomnia, sleep disturbance, and abnormal dreams. These reports cannot prove causation. Someone taking semaglutide who develops insomnia might be experiencing stress, another medication interaction, or simply the normal sleep disruptions that come with significant life changes. But the volume of reports suggests the phenomenon is worth investigating.
A 2023 study published in the journal examining GLP-1 receptor agonists and mental health outcomes found reports of sleep disturbances across multiple social media platforms. Researchers analyzed posts from Reddit, TikTok, and other platforms, identifying patterns of sleep complaints among GLP-1 users. While social media analysis has obvious limitations, it captures experiences that clinical trials miss.
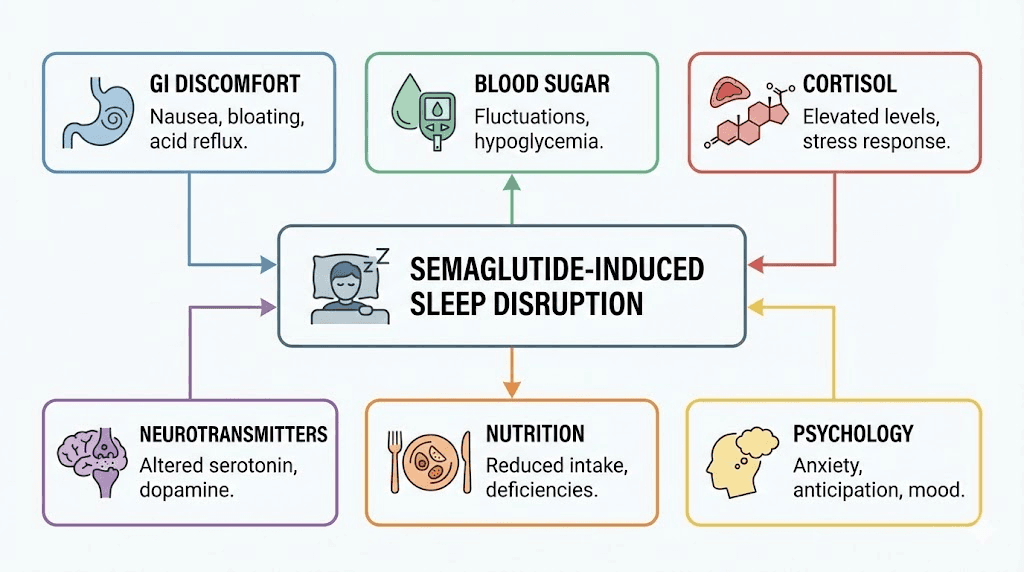
Six reasons semaglutide disrupts your sleep
If semaglutide does not directly cause insomnia, why are so many people struggling to sleep? The answer is not one mechanism but six, often working simultaneously. Understanding each one is the first step toward fixing the problem.
1. Gastrointestinal discomfort at night
This is the most common and most underestimated sleep disruptor on semaglutide. The medication slows gastric emptying, which is part of how it reduces appetite and promotes weight loss. But slowed gastric emptying means food sits in your stomach longer. If you eat dinner at 7 PM and lie down at 10 PM, your stomach may still be working on that meal, and when you lie flat, stomach acid can creep toward your esophagus.
The result? Heartburn, mild nausea, bloating, or a vague feeling of discomfort that prevents you from relaxing into sleep. Many people do not even recognize these symptoms as GI-related. They just know they feel "unsettled" when they try to sleep.
This is especially problematic during dose escalation phases. Each time your dose increases, your GI system needs time to adjust. The first two weeks after a dose increase are typically the worst for nighttime discomfort.
2. Blood sugar fluctuations during sleep
Semaglutide is a GLP-1 receptor agonist that directly affects insulin secretion and blood glucose regulation. For people with type 2 diabetes, this is the primary therapeutic effect. For people using it for weight loss, it still influences blood sugar, even if levels were previously normal.
Nocturnal hypoglycemia, blood sugar dropping too low during sleep, can cause nighttime awakenings, sweating, vivid dreams, and a racing heart. Your body detects the low blood sugar and releases counter-regulatory hormones (cortisol, adrenaline, glucagon) to bring levels back up. These hormones wake you up. Sometimes dramatically.
The risk increases when semaglutide is combined with other diabetes medications like sulfonylureas or insulin. But it can happen even in non-diabetic individuals, particularly if they skip meals or eat very little during the day (which semaglutide makes easy to do through appetite suppression).
3. Cortisol and stress hormone changes
Rapid weight loss, regardless of the method, triggers hormonal changes. Your body interprets significant calorie reduction as a potential threat, and it responds by adjusting stress hormones. Cortisol, the primary stress hormone, plays a critical role in your sleep-wake cycle. It should be lowest at bedtime and peak in the early morning. When cortisol patterns shift, either through elevated nighttime levels or disrupted rhythms, sleep suffers.
Research shows that weight loss can temporarily dysregulate cortisol production. Semaglutide users losing weight rapidly may experience elevated evening cortisol that makes it difficult to wind down. This is not a drug effect per se. It is a weight loss effect. But since semaglutide drives the weight loss, the two become inseparable from the patient perspective.
4. Neurotransmitter modulation
GLP-1 receptors exist throughout the brain. That is part of why semaglutide reduces appetite, it acts on central nervous system pathways that regulate hunger and satiety. But these same brain regions also influence mood, arousal, and sleep architecture.
GLP-1 receptor activation affects several neurotransmitters relevant to sleep. Serotonin, dopamine, GABA, and glutamate all participate in the sleep-wake cycle. Altered levels of serotonin and dopamine can produce vivid or unusual dreams, difficulty falling asleep, or changes in sleep stage duration. Some users report spending less time in deep sleep or experiencing fragmented REM cycles.
This mechanism is the least understood but potentially the most significant for long-term sleep quality on semaglutide. Research into the neuropsychiatric effects of GLP-1 medications is still in its early stages.
5. Reduced caloric intake and nutritional deficiencies
Semaglutide dramatically reduces appetite. Most users eat 20-40% fewer calories without trying. That is the point. But severe caloric restriction can deplete nutrients essential for sleep.
Magnesium, B vitamins, iron, and tryptophan all play roles in sleep quality. When your total food intake drops significantly, so does your intake of these nutrients unless you actively supplement. Nutritional planning on semaglutide is not optional. It is a critical component of the protocol.
Magnesium deficiency alone can cause insomnia, restless legs, and frequent nighttime awakenings. B6 deficiency disrupts melatonin production. Iron deficiency causes restless leg syndrome that makes falling asleep almost impossible.
6. Behavioral and psychological factors
This one gets overlooked, but it matters. Starting semaglutide is a significant life change. You are reshaping your relationship with food, potentially dealing with body image shifts, managing new physical sensations, and possibly confronting emotions that food previously helped manage.
Anxiety about weight loss progress, excitement about results, worry about plateaus, or stress about the cost and logistics of treatment can all contribute to a busy mind at bedtime. These psychological factors are real contributors to insomnia that get dismissed as "just stress" when they deserve targeted attention.
The vivid dreams phenomenon
We need to talk about the dreams.
Across GLP-1 user communities, one of the most consistently reported sleep-related changes is vivid, intense, sometimes disturbing dreams. Users describe cinematic dream sequences that feel real enough to carry emotional weight into the following morning. Some report pleasant dreams. Others describe anxiety-driven or unsettling scenarios. Nearly all report that the dreams feel qualitatively different from their normal dreaming experience.
Vivid dreams are not officially listed as a side effect of Ozempic or Wegovy by Novo Nordisk. But the volume of anecdotal reports is striking. Several mechanisms could explain this phenomenon.
First, GLP-1 receptor activation in the brain influences serotonin and dopamine levels. Both neurotransmitters play central roles in REM sleep, the sleep stage most associated with dreaming. Even modest changes in neurotransmitter balance can produce more vivid, memorable dreams.
Second, nocturnal blood sugar fluctuations can trigger counter-regulatory hormone release that partially rouses you during REM cycles. When you wake briefly during a dream, you are far more likely to remember it. The dreams may not actually be more vivid, you may simply be waking during more of them.
Third, and this is less glamorous but probably most common, GI discomfort causing micro-awakenings throughout the night disrupts normal sleep architecture. Your brain cycles through sleep stages differently, spending more time in light sleep and REM rather than progressing through the normal deep-sleep-heavy early cycles. More REM time equals more dreaming.
For most people, vivid dreams are more annoying than harmful. But if they become distressing, if they are causing nightmare-level anxiety, or if they are disrupting your ability to feel rested, they deserve attention. The strategies later in this guide address dream intensity alongside general sleep improvement.
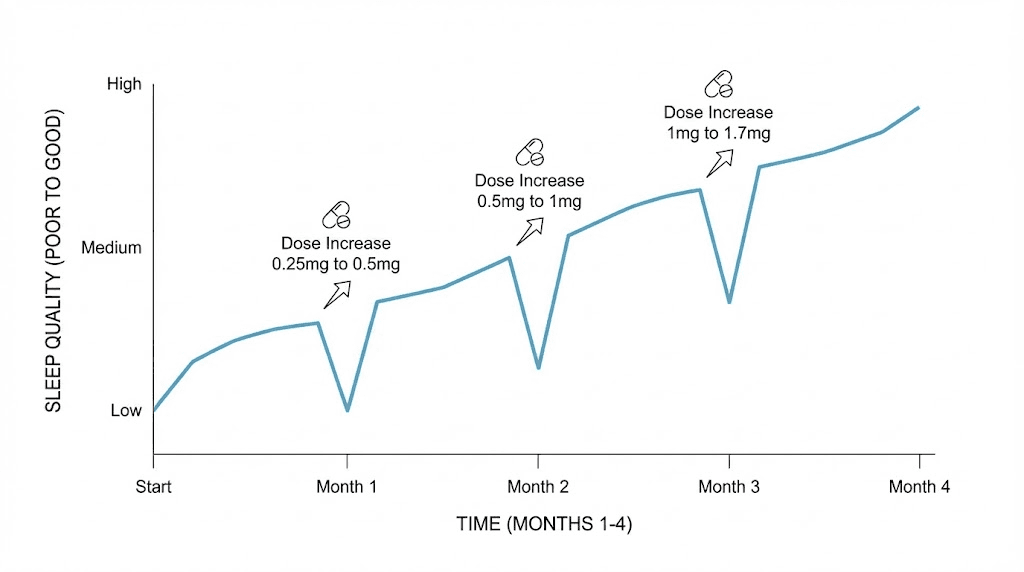
Timeline of sleep changes on semaglutide
Understanding when sleep disruptions typically occur helps you prepare and respond appropriately. The pattern is remarkably consistent across user reports.
Weeks 1-2: initial adjustment
The most common window for sleep disruption. Your body is adjusting to semaglutide for the first time. GI side effects peak. Nausea is most intense. Your appetite drops suddenly, and your eating patterns shift. Blood sugar patterns change. All of these factors converge to create the perfect storm for disrupted sleep.
Most users report the worst sleep during this initial period. If you can get through weeks 1-2, things typically improve.
Weeks 3-4: partial adaptation
Your body begins adapting to the current dose. GI symptoms often moderate. Nausea becomes less frequent. Sleep quality begins to improve for many users, though not all. This is the period where identifying specific triggers (meal timing, food choices, hydration) becomes critical.
Each dose escalation: mini-restart
Every time your dose increases, expect a mini version of weeks 1-2. Your body needs to adjust to the higher dose, and GI symptoms typically resurface for 1-2 weeks before settling down. Plan for this. Knowing it is temporary makes it manageable.
Months 2-3: new baseline
By this point, most users have established a new sleep pattern. For many, sleep actually improves compared to pre-semaglutide baselines, especially if weight loss has improved conditions like sleep apnea or reduced nighttime pain from carrying excess weight. The people still struggling at this stage typically have identifiable, addressable factors.
Month 4 and beyond: stabilization
Long-term users generally report normalized sleep. The initial disruption fades. Many report better overall sleep quality than before starting treatment. This is particularly true for users who experienced significant weight loss that resolved obstructive sleep apnea or reduced inflammatory markers.
The sleep apnea connection: when semaglutide actually helps sleep
Here is the other side of the story, and it is an important one.
For people with obesity-related obstructive sleep apnea (OSA), semaglutide can dramatically improve sleep quality. OSA causes repeated breathing interruptions during sleep, leading to daytime fatigue, poor sleep quality, cardiovascular risk, and a host of other health problems. It affects an estimated 22 million Americans and is directly linked to excess body weight.
The mechanism is straightforward. Excess weight, particularly around the neck and upper airway, creates soft tissue that collapses during sleep and blocks breathing. Weight loss reduces this tissue. Airways stay open. Breathing improves. Sleep improves.
Clinical evidence backs this up. The SURMOUNT-OSA study, which tested tirzepatide (a related GLP-1/GIP receptor agonist), demonstrated significant improvements in the Apnea-Hypopnea Index (AHI), the standard measure of sleep apnea severity. Participants saw reductions in sleep interruptions, improvements in blood oxygen levels, and better daytime alertness. Semaglutide shows similar benefits through the same weight loss mechanism.
A scoping review published examining GLP-1 receptor agonists and obstructive sleep apnea found consistent evidence that these medications reduce OSA severity. The benefits come from multiple pathways: reduced upper airway fat deposition, improved respiratory control, anti-inflammatory effects, and overall metabolic improvement.
So there is a paradox. In the short term, semaglutide can disrupt sleep through the mechanisms we discussed earlier. In the long term, it can significantly improve sleep by treating the underlying conditions (excess weight, inflammation, metabolic dysfunction) that were causing poor sleep in the first place.
If you had undiagnosed or untreated sleep apnea before starting semaglutide, you may experience a period where sleep gets worse before it gets dramatically better. This is worth knowing because it affects how you interpret your experience and whether you persist through the initial difficult period.
12 evidence-based strategies for better sleep on semaglutide
Enough about why it happens. Let us fix it. These strategies are organized from most impactful to supplementary. Start with the top three. If those are not enough, work your way down.
Strategy 1: time your injection earlier in the day
This is the single most effective change for many users. Taking your semaglutide injection in the morning rather than evening gives your body the full day to process the initial wave of GI side effects before bedtime. Nausea, appetite changes, and gastric motility effects peak in the hours following injection and then gradually diminish.
A morning injection means the strongest effects occur during waking hours when you can manage them with activity, hydration, and eating. By bedtime, the acute effects have moderated.
If you currently inject in the evening and struggle with sleep, try switching to morning for your next injection. Many users report noticeable improvement within one dose cycle.
Strategy 2: adjust meal timing around bedtime
This matters more on semaglutide than it does for most people. Because semaglutide slows gastric emptying, your stomach needs MORE time to process food, not less. Eating your last meal at least 3-4 hours before bedtime is the minimum recommendation. For some users, 4-5 hours works better.
The goal is to lie down with an empty or near-empty stomach. This eliminates the major triggers for nighttime nausea, heartburn, and bloating. Keep your evening meal lighter and lower in fat, as fatty foods take the longest to digest.
If you absolutely must eat closer to bedtime, choose easily digestible options. Lean protein, simple carbohydrates, and warm liquids move through the stomach faster than heavy, fatty meals. Check our semaglutide diet plan for specific meal recommendations.
Strategy 3: elevate your upper body while sleeping
If nighttime acid reflux is contributing to your sleep disruption, this simple physical change can be transformative. Elevating the head of your bed by 6-8 inches (using a wedge pillow or bed risers, not just extra pillows) uses gravity to keep stomach acid where it belongs.
Extra pillows alone often do not work because they only elevate your head, not your entire upper body. Your esophagus is still at an angle that allows reflux. A proper wedge or bed elevation maintains the correct incline from your waist up.
Strategy 4: manage blood sugar stability
Preventing nocturnal hypoglycemia requires paying attention to your food intake throughout the day. On semaglutide, it is easy to undereat, sometimes dramatically. But going to bed with very low blood sugar sets you up for a 2-3 AM awakening when counter-regulatory hormones kick in.
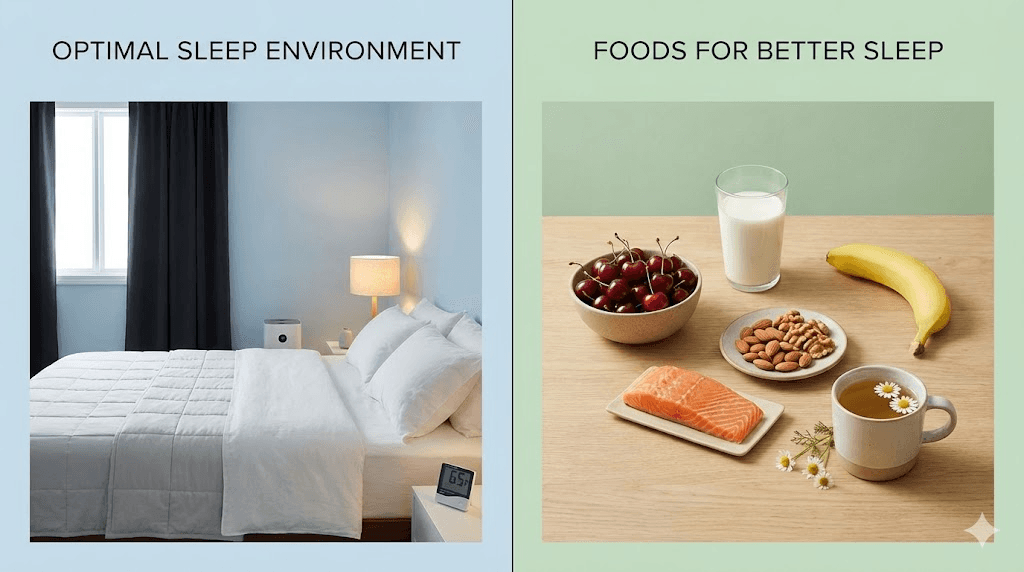
A small snack containing protein and complex carbohydrates before bed can help stabilize blood sugar overnight. Think a handful of nuts with a few crackers, a small portion of Greek yogurt, or a cheese stick with whole grain toast. Nothing large enough to trigger GI distress, just enough to maintain blood sugar stability.
If you are using semaglutide alongside other diabetes medications, discuss nocturnal hypoglycemia prevention specifically with your healthcare provider. Medication adjustments may be necessary.
Strategy 5: supplement strategically
Reduced food intake means reduced nutrient intake. Several supplements directly support sleep quality.
Magnesium glycinate (200-400mg before bed) is the standout. Magnesium promotes muscle relaxation, calms the nervous system, and supports melatonin production. The glycinate form is the best tolerated for sleep because glycine itself has calming properties. Magnesium citrate works too but may worsen loose stools, a common semaglutide side effect.
Vitamin B6 (25-50mg, taken earlier in the day) supports the conversion of tryptophan to serotonin to melatonin. Deficiency disrupts this pathway and impairs natural melatonin production. Since semaglutide users eat less and may consume fewer B6-rich foods (poultry, fish, potatoes, bananas), supplementation makes sense.
Vitamin B12 deficiency has been reported in long-term GLP-1 users. While B12 does not directly cause insomnia, deficiency can contribute to fatigue, neurological symptoms, and mood changes that indirectly affect sleep.
Melatonin (0.5-3mg, 30-60 minutes before bed) can help reset disrupted sleep-wake cycles. Start with the lowest effective dose. More is not better with melatonin, higher doses can actually worsen sleep quality for some people.
Strategy 6: optimize sleep hygiene fundamentals
This sounds basic, and it is. But when your body is already struggling with sleep on semaglutide, poor sleep hygiene tips you from manageable disruption to genuine insomnia.
The non-negotiables: consistent bedtime and wake time (yes, even on weekends), cool bedroom temperature (65-68 degrees F), complete darkness, and limited screen exposure for 30-60 minutes before bed. Blue light from screens suppresses melatonin production by up to 50%. When your melatonin production is already stressed by reduced B6 intake and metabolic changes, you cannot afford that additional hit.
Strategy 7: address acid reflux specifically
If heartburn is your primary sleep disruptor, target it directly. Beyond elevating your upper body and adjusting meal timing, consider these approaches.
Avoid trigger foods in the evening: citrus, tomatoes, chocolate, caffeine, spicy foods, and alcohol. On semaglutide, your GI system is already sensitized. Foods that never bothered you before may now cause reflux, especially when eaten close to bedtime. Track which foods to avoid on semaglutide are particularly problematic for your sleep.
Over-the-counter antacids or H2 blockers (like famotidine) taken before bed can provide significant relief. For persistent reflux, a proton pump inhibitor (PPI) may be appropriate. Discuss options with your healthcare provider.
Sleep on your left side. This positions your stomach below your esophageal sphincter, making acid reflux mechanically less likely. It is a simple change that can make a meaningful difference.
Strategy 8: manage nausea proactively
If nausea rather than reflux is your primary sleep disruptor, different strategies apply.
Ginger tea before bed has mild antiemetic (anti-nausea) properties and is well-tolerated. Fresh ginger steeped in hot water for 10-15 minutes works. Ginger supplements (250mg) are another option.
Peppermint can help with nausea but may worsen acid reflux by relaxing the lower esophageal sphincter. Use it only if reflux is not your issue.
Keep your bedroom cool. Heat exacerbates nausea. If you tend to feel warm at night (which some semaglutide users report), use lighter bedding and consider a fan or air conditioning.
Acupressure wristbands (Sea-Bands) provide mild nausea relief for some people. They are inexpensive, drug-free, and worth trying.
Strategy 9: implement a wind-down routine
Semaglutide-related metabolic changes can make your nervous system more reactive, especially during dose adjustments. A deliberate wind-down routine signals your brain that sleep is approaching.
The most effective elements: a warm bath or shower 60-90 minutes before bed (the subsequent body temperature drop promotes sleepiness), gentle stretching or yoga, reading (physical book, not screen), deep breathing exercises, or progressive muscle relaxation.
Avoid stimulating content, intense exercise, or stressful conversations in the hour before bed. Your cortisol levels may already be elevated from the weight loss process. Do not add more cortisol triggers when you are trying to sleep.
Strategy 10: stay hydrated, but strategically
Dehydration is surprisingly common on semaglutide. Reduced food intake means reduced water intake from food sources. GI side effects like vomiting and diarrhea can further deplete fluids. Dehydration causes headaches, muscle cramps, and restlessness that interfere with sleep.
Aim for adequate hydration throughout the day, but taper fluid intake in the 2-3 hours before bed to avoid nighttime bathroom trips. A disrupted bladder wake cycle compounds whatever other sleep challenges you are facing.
Strategy 11: monitor and adjust your dose timing
If you take your weekly semaglutide injection on the same day each week (as prescribed), pay attention to which nights are worst. Many users find that sleep disruption is most pronounced 24-72 hours after injection, when peak drug levels and peak GI effects coincide.
If your worst nights consistently fall on specific days after injection, consider whether adjusting your injection day could help. For example, if Thursday injections mean terrible sleep Friday and Saturday, switching to Sunday or Monday might push the disruption to weeknights when the stakes feel lower, or to earlier in the week when your schedule is more flexible.
Strategy 12: know when to talk to your doctor
Some sleep disruption during semaglutide treatment is expected and manageable. But certain symptoms warrant medical attention.
Seek help if insomnia persists beyond 4-6 weeks without improvement, if you experience breathing pauses during sleep (a partner notices this), if you develop symptoms of severe depression or anxiety alongside sleep changes, if nocturnal hypoglycemia events are frequent (waking drenched in sweat with rapid heartbeat), or if your daytime function is significantly impaired (falling asleep while driving, unable to work effectively, severe mood changes).
Your healthcare provider may recommend a sleep study, medication adjustments, or short-term sleep aids to break the cycle. Dose adjustments, including temporarily reducing the dose or extending the titration schedule, can sometimes resolve sleep issues while maintaining the therapeutic benefits of treatment.
Semaglutide insomnia vs. tirzepatide insomnia
A natural question for anyone researching GLP-1 medications and sleep is whether tirzepatide causes similar sleep disruptions. The short answer: yes, the mechanisms are largely the same because they stem from GI side effects and weight loss rather than from the specific drug molecule.
Both semaglutide and tirzepatide can disrupt sleep through the same six mechanisms outlined above. GI discomfort, blood sugar fluctuations, cortisol changes, neurotransmitter effects, nutritional deficiencies, and psychological factors all apply to both medications.
One difference worth noting: tirzepatide acts on both GLP-1 and GIP receptors, while semaglutide acts only on GLP-1 receptors. The dual mechanism means tirzepatide may produce somewhat different neurotransmitter effects, though research on sleep-specific outcomes comparing the two is limited.
For users considering switching between semaglutide and tirzepatide, sleep disruption patterns are unlikely to be the deciding factor. The GI-driven sleep issues are similar with both. Focus on which medication provides better overall outcomes for weight management and metabolic health, and manage sleep as a secondary issue using the strategies in this guide.
The conversion between the two medications can temporarily worsen sleep as your body adjusts to a new compound, similar to starting treatment for the first time. Expect 2-4 weeks of adjustment if switching.
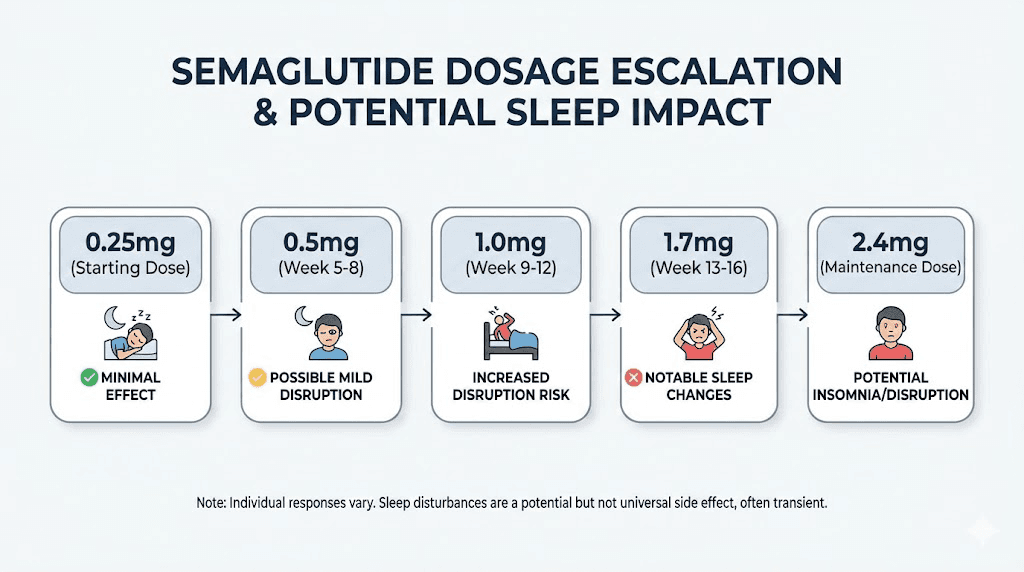
How semaglutide dosage affects sleep quality
Dose matters. Higher doses of semaglutide produce more pronounced GI side effects, stronger appetite suppression, more significant metabolic changes, and consequently more potential for sleep disruption.
The standard semaglutide dosage escalation follows a gradual titration schedule specifically to minimize side effects. Rushing through dose increases or starting at too high a dose dramatically increases the risk of sleep-disrupting side effects.
Here is what users typically report at each dose level:
0.25mg (starting dose): Mild GI effects. Sleep disruption is minimal for most users. This is the adjustment phase where your body gets acquainted with the medication.
0.5mg: GI effects increase modestly. Some users notice their first sleep changes here. Usually mild and transient.
1.0mg: A significant step up. This is where many users first experience noticeable sleep disruption. Nausea, heartburn, and appetite suppression all intensify. The strategies in this guide become most important at this dose and above.
1.7mg: Strong effects. Higher-dose users report more pronounced GI symptoms and more frequent sleep complaints. Nutritional deficiency risks also increase because appetite is significantly suppressed.
2.4mg (maximum Wegovy dose): Maximum therapeutic dose. GI effects are most pronounced. Sleep disruption potential is highest but so are the weight loss benefits. At this dose, implementing all 12 strategies simultaneously often becomes necessary.
If you are using compounded semaglutide, ensure accurate dosing with proper reconstitution and measurement. Inaccurate dosing can produce unpredictable side effects including sleep disruption.
Semaglutide, sleep, and weight loss: the interconnected cycle
Poor sleep and weight management are deeply interconnected, and understanding this relationship matters for anyone on semaglutide.
Sleep deprivation increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone). It impairs glucose tolerance, increases cortisol, and promotes fat storage, particularly visceral fat. In other words, poor sleep actively fights against everything semaglutide is trying to accomplish.
This creates a problematic cycle. Semaglutide disrupts sleep. Disrupted sleep increases hunger and cravings. Increased hunger and cravings make the weight loss process harder. Harder weight loss increases frustration and psychological stress. Increased stress further disrupts sleep.
Breaking this cycle is not just about comfort. It is about maximizing the effectiveness of your semaglutide treatment. Users who sleep well lose more weight, maintain muscle mass better, experience fewer cravings, and report higher satisfaction with their results.
Research on weight loss and sleep shows that people sleeping fewer than 6 hours per night lose significantly less fat and more muscle compared to those sleeping 7-8 hours, even with identical calorie intake. On semaglutide, where the goal is typically fat loss while preserving lean mass, this finding is highly relevant.
The practical takeaway: treating sleep disruption on semaglutide is not a luxury. It is a critical component of optimizing your results. Every strategy you implement for better sleep is simultaneously a strategy for better weight loss outcomes.
When semaglutide insomnia signals something else
Not every sleep problem during semaglutide treatment is caused by semaglutide. Sometimes the medication unmasks or coincides with independent sleep conditions that need their own treatment.
Undiagnosed sleep apnea
Paradoxically, starting semaglutide can make you more aware of existing sleep apnea. Before treatment, you may have been so accustomed to poor sleep that it felt normal. As other aspects of your health improve on semaglutide, the persistent fatigue and nighttime awakenings from untreated sleep apnea become more noticeable by contrast.
If you snore loudly, wake with dry mouth or headaches, or feel exhausted despite seemingly adequate sleep time, discuss a sleep study with your healthcare provider. Treating sleep apnea alongside semaglutide often produces dramatic improvements in both sleep quality and weight loss progress.
Thyroid dysfunction
Both hypothyroidism and hyperthyroidism can cause sleep disturbances. Rapid weight loss can occasionally affect thyroid function. If you develop insomnia alongside other symptoms (unexplained anxiety, heart palpitations, heat intolerance, or conversely fatigue, cold intolerance, and constipation), get your thyroid levels checked.
Medication interactions
If you take other medications alongside semaglutide, consider whether interactions or timing issues could be contributing to sleep problems. Stimulant medications, certain antidepressants, corticosteroids, beta-agonist inhalers, and decongestants can all cause insomnia. When combined with the GI effects of semaglutide, the cumulative impact on sleep can be significant.
Review all your medications with your prescriber if sleep problems are persistent and severe.
Perimenopause and hormonal transitions
For women in their 40s and 50s, insomnia on semaglutide may partially or entirely be related to perimenopause rather than the medication itself. Hormonal fluctuations during this transition are notorious sleep disruptors. Peptides for menopause and weight management is a growing area of research precisely because these populations often need multi-faceted approaches.
Weight loss from semaglutide can actually affect estrogen levels, since fat tissue produces estrogen. Rapid loss of fat tissue means a rapid change in estrogen production, which can exacerbate perimenopausal symptoms including insomnia, hot flashes, and night sweats.
Real-world sleep improvement protocols
Let us put the strategies together into practical protocols based on the type of sleep disruption you are experiencing.
Protocol A: difficulty falling asleep (sleep onset insomnia)
Most likely causes: Elevated cortisol, neurotransmitter changes, anxiety, or residual nausea
Action plan:
Inject semaglutide in the morning
Last meal 4+ hours before bed
Magnesium glycinate 300-400mg at 8 PM
30-minute wind-down routine starting 60 minutes before bed
Warm shower 90 minutes before sleep
If racing thoughts persist, try a guided meditation app or progressive muscle relaxation
Consider low-dose melatonin (0.5-1mg) 30 minutes before bed
Expected improvement: 1-2 weeks for noticeable change
Protocol B: middle-of-the-night awakenings
Most likely causes: Blood sugar fluctuations, acid reflux while lying flat, or GI discomfort
Action plan:
Small protein-carb snack before bed (stabilize blood sugar)
Elevate head of bed 6-8 inches
Sleep on left side
No trigger foods after 4 PM
Famotidine (Pepcid) 20mg before bed if reflux is suspected
If you wake, do NOT check the clock or your phone, keep the room dark, practice slow breathing
Expected improvement: Often immediate with dietary and positional changes
Protocol C: vivid dreams disrupting sleep quality
Most likely causes: Neurotransmitter changes, blood sugar dips during REM, or sleep fragmentation from GI issues
Action plan:
All elements of Protocol B (blood sugar stability, GI management)
Avoid stimulating content 2 hours before bed
Journaling before sleep to "offload" emotional content
B6 supplementation (25-50mg with dinner, not at bedtime)
If dreams are anxiety-themed, consider whether daytime stress management needs attention
Expected improvement: Dream intensity typically moderates over 3-4 weeks as your body adjusts
Protocol D: daytime fatigue despite adequate sleep time
Most likely causes: Poor sleep quality (frequent micro-awakenings), nutritional deficiencies, undiagnosed sleep apnea, or insufficient caloric intake
Action plan:
Track actual sleep quality with a wearable or sleep tracking app
Ensure minimum 1200 calories daily (many semaglutide users eat far less)
Comprehensive blood panel: B12, iron/ferritin, vitamin D, magnesium, thyroid
Consider a sleep study if fatigue persists despite adequate intake and supplements
20-minute morning sunlight exposure to anchor circadian rhythm
Expected improvement: Depends on underlying cause. Nutritional corrections show improvement in 2-4 weeks. Sleep apnea treatment shows rapid improvement.
Supplements and natural sleep aids: what works and what does not
The supplement market for sleep is enormous and mostly garbage. Here is an honest assessment of what actually has evidence behind it, particularly in the context of semaglutide use.
Strong evidence
Magnesium glycinate: Legitimate sleep support. Promotes GABA receptor activity, reduces cortisol, relaxes muscles. The glycinate form is superior for sleep because glycine itself is a calming neurotransmitter. Dosage: 200-400mg before bed. Well-tolerated. Minimal interaction risk with semaglutide.
Melatonin (low dose): Effective for resetting sleep-wake cycles, particularly during dose adjustment periods. Start at 0.5mg and increase only if needed. Doses above 3mg often reduce effectiveness and can cause next-day grogginess. Timing matters, take it 30-60 minutes before your target bedtime.
Moderate evidence
L-theanine: An amino acid found in green tea that promotes alpha brain wave activity (the relaxed-but-alert state). Dosage: 200-400mg before bed. Some users find it helpful for the racing-mind type of insomnia. No significant interactions with semaglutide.
Glycine: 3 grams before bed has shown modest sleep quality improvements in studies. It lowers core body temperature and promotes relaxation. Safe and inexpensive.
Ashwagandha: An adaptogenic herb that may lower cortisol levels. Relevant if stress-related cortisol elevation is contributing to your insomnia. Dosage: 300-600mg of KSM-66 extract. Takes 2-4 weeks for full effect.
Limited evidence (probably not worth it)
Valerian root: Mixed results in studies. Mild effects at best. The smell is unpleasant. There are better options.
CBD: Inconsistent evidence for sleep. Higher doses may help, but quality control issues in the supplement market make dosing unreliable. Legal status varies.
5-HTP: A serotonin precursor that theoretically supports sleep. However, it can interact with medications affecting serotonin and may worsen nausea in semaglutide users. Approach with caution.
Avoid
High-dose melatonin (10mg+): More is not better. High doses can cause next-day drowsiness, headaches, and paradoxically worsen sleep quality.
Diphenhydramine (Benadryl) for regular use: Antihistamine sleep aids lose effectiveness quickly, cause next-day grogginess, and have anticholinergic effects linked to cognitive impairment with long-term use. Fine for occasional use. Not a solution for chronic sleep issues.
Alcohol as a sleep aid: Alcohol fragments sleep architecture, reduces REM quality, and interacts with semaglutide GI effects. Alcohol and semaglutide is a combination that amplifies almost every sleep-disrupting mechanism discussed in this guide.
The exercise and sleep connection on semaglutide
Regular physical activity is one of the most effective insomnia treatments available, often matching or exceeding the effectiveness of sleep medications. On semaglutide, exercise serves double duty: it supports weight loss AND promotes better sleep.
But timing matters. Moderate exercise completed 4-6 hours before bedtime promotes the deepest, most restorative sleep. Intense exercise within 2-3 hours of bedtime can elevate cortisol and core body temperature enough to delay sleep onset.
For semaglutide users, the ideal approach is moderate exercise in the late afternoon or early evening. Walking, cycling, swimming, or resistance training completed by 6-7 PM sets up optimal sleep conditions. The post-exercise cortisol decline and body temperature drop coincide with bedtime, promoting natural sleepiness.
Be realistic about exercise capacity on semaglutide, especially during dose escalation. Reduced caloric intake means reduced available energy. Pushing through intense workouts when you are eating significantly less can spike cortisol and worsen sleep rather than improve it. Moderate, consistent activity beats sporadic intense sessions.
If you are too tired to exercise, that itself is information. It suggests your sleep issue may be severe enough to warrant medical attention, or that your caloric intake is too low to support your activity level.
Long-term outlook: does semaglutide insomnia resolve?
Yes. For the vast majority of users, sleep disruption on semaglutide is temporary.
The typical trajectory follows a U-shaped curve. Sleep quality dips during the initial weeks and during each dose increase, then gradually returns to baseline or improves beyond baseline as GI side effects resolve and weight loss produces health benefits.
Most users report their best sleep ever once they reach a stable maintenance dose and have lost significant weight. The combination of resolved or improved sleep apnea, reduced inflammation, better blood sugar regulation, improved cardiovascular function, and reduced physical discomfort from carrying excess weight creates conditions for genuinely excellent sleep.
A minority of users experience persistent sleep issues. For these individuals, the cause is usually identifiable: unaddressed nutritional deficiencies, untreated sleep apnea, medication interactions, or hormonal factors unrelated to semaglutide. Working with a healthcare provider to identify the specific cause almost always produces a solution.
The key message: do not let temporary sleep disruption derail your semaglutide progress. Manage it actively using the strategies in this guide, and expect improvement over weeks to months.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed side effect management strategies, dosage calculators, and personalized protocol support that addresses challenges like sleep disruption from the start of treatment.
Frequently asked questions
Does semaglutide directly cause insomnia?
No. Clinical trial data shows that insomnia rates are similar between semaglutide and placebo groups. However, semaglutide can indirectly disrupt sleep through gastrointestinal side effects, blood sugar fluctuations, cortisol changes from weight loss, and reduced nutritional intake. These indirect effects are real and significant for many users.
How long does semaglutide insomnia last?
Most users experience the worst sleep disruption during the first 2-4 weeks of starting treatment or after each dose increase. Sleep typically normalizes within 4-6 weeks at a stable dose. If insomnia persists beyond this window, an identifiable cause (nutritional deficiency, reflux, sleep apnea) is usually responsible.
Should I take semaglutide in the morning or evening for better sleep?
Morning injection is generally recommended for better sleep outcomes. This allows the peak GI side effects (nausea, appetite changes) to occur during waking hours rather than disrupting nighttime rest. Many users report noticeable improvement simply by switching from evening to morning injections.
Can semaglutide cause vivid dreams?
Many users report vivid, intense dreams on semaglutide, though this is not officially listed as a side effect. Possible mechanisms include GLP-1 receptor effects on serotonin and dopamine in the brain, nighttime blood sugar fluctuations triggering partial awakenings during REM sleep, and sleep fragmentation from GI discomfort creating more time in REM stages.
Will switching from semaglutide to tirzepatide fix my insomnia?
Switching medications is unlikely to resolve sleep issues because both GLP-1 agonists produce similar GI side effects and metabolic changes. Tirzepatide users report similar sleep disruptions. Focus on managing the underlying causes rather than switching medications.
Does semaglutide improve sleep over time?
Yes. Long-term semaglutide users frequently report better sleep than before treatment, particularly those who experience significant weight loss. Improved sleep apnea, reduced inflammation, better blood sugar control, and decreased physical discomfort all contribute to long-term sleep quality improvements.
What supplements help with semaglutide insomnia?
Magnesium glycinate (200-400mg before bed) has the strongest evidence. Low-dose melatonin (0.5-3mg) helps reset disrupted sleep cycles. L-theanine (200-400mg) can calm a racing mind. B12 supplementation addresses potential deficiencies from reduced food intake. Always discuss supplements with your healthcare provider, especially when taking other medications.
Can I take sleep medication while on semaglutide?
Prescription sleep medications can generally be used alongside semaglutide, but discuss this with your prescriber. Over-the-counter options like diphenhydramine (Benadryl) should only be used occasionally due to tolerance and side effects. Avoid using alcohol as a sleep aid, as it worsens both sleep quality and semaglutide GI effects.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your nights stay restful, your doses stay effective, and your results stay consistent.