Feb 24, 2026

Before you skip your next tirzepatide dose because of that angry red welt on your abdomen, read this. That swollen, itchy patch staring back at you from the mirror is not a sign that something has gone terribly wrong. It is not a reason to panic. And it is definitely not a reason to abandon a protocol that may be working.
But it does need proper treatment.
Injection site reactions affect roughly 3.2% of tirzepatide users in clinical trials, compared to just 0.4% on placebo. That number climbs higher in real-world settings, where technique varies, formulations differ, and people do not always follow optimal injection protocols. The reactions range from a mild pink circle that fades in hours to angry welts that spread across the abdomen over days, causing burning, itching, and genuine discomfort. A published case report in Cureus documented a 76-year-old male whose tirzepatide injection site reaction spread across his entire lower abdomen over 10 days before resolving after discontinuation.
Here is the good news. The vast majority of these reactions respond to simple treatments you can start right now, at home, with supplies from any pharmacy. This guide covers every evidence-based treatment option, organized by reaction type, with specific protocols you can follow immediately. It also covers the prevention strategies that reduce your chances of experiencing reactions in the first place, the warning signs that require medical attention, and the long-term management approaches that keep reactions manageable as you continue your tirzepatide dosing protocol.
SeekPeptides has compiled the most comprehensive treatment resource available, drawing from clinical trial data, published case reports, dermatology research, and the real-world experiences of thousands of tirzepatide users. Whether you are dealing with your first reaction or your tenth, this guide gives you the exact steps to manage it effectively.
What tirzepatide injection site reactions actually look like
Not all injection site reactions are created equal. Understanding exactly what you are dealing with determines which treatment approach works best. Some reactions demand cold compresses. Others need antihistamines. A few require medical attention. The difference matters.
Across the SURPASS clinical trials, researchers categorized injection site reactions into several distinct presentations. Each one has a different underlying mechanism, a different timeline, and a different optimal treatment. Knowing which type you have is the first step toward effective tirzepatide side effect management.
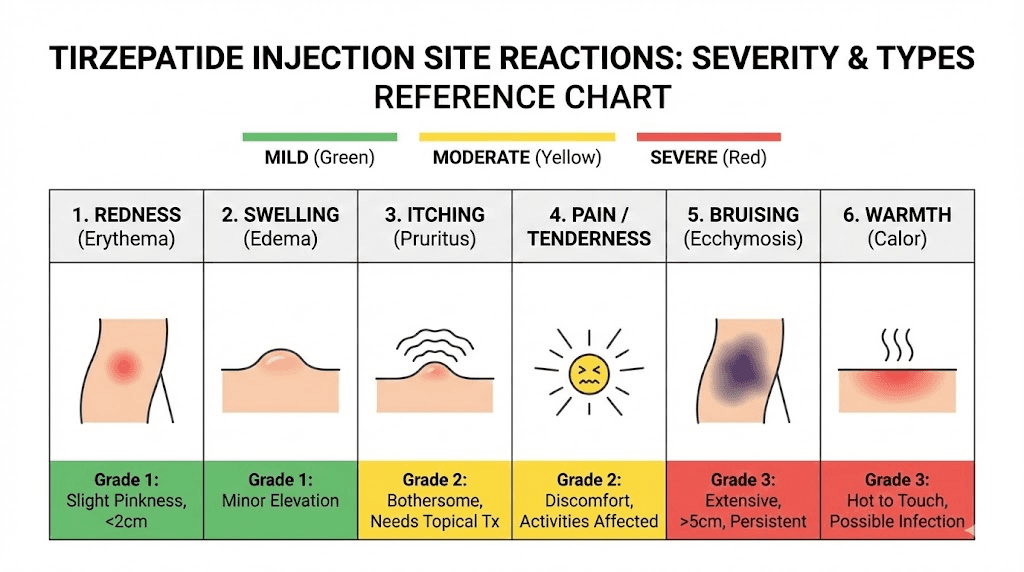
Redness and erythema
The most common presentation. A pink or red circle appears at the injection site, typically within 1 to 6 hours after injection. The redness usually measures 2 to 5 centimeters in diameter and feels warm to the touch. In mild cases, it fades within 24 hours without any intervention. In moderate cases, it persists for 2 to 3 days and may darken before resolving.
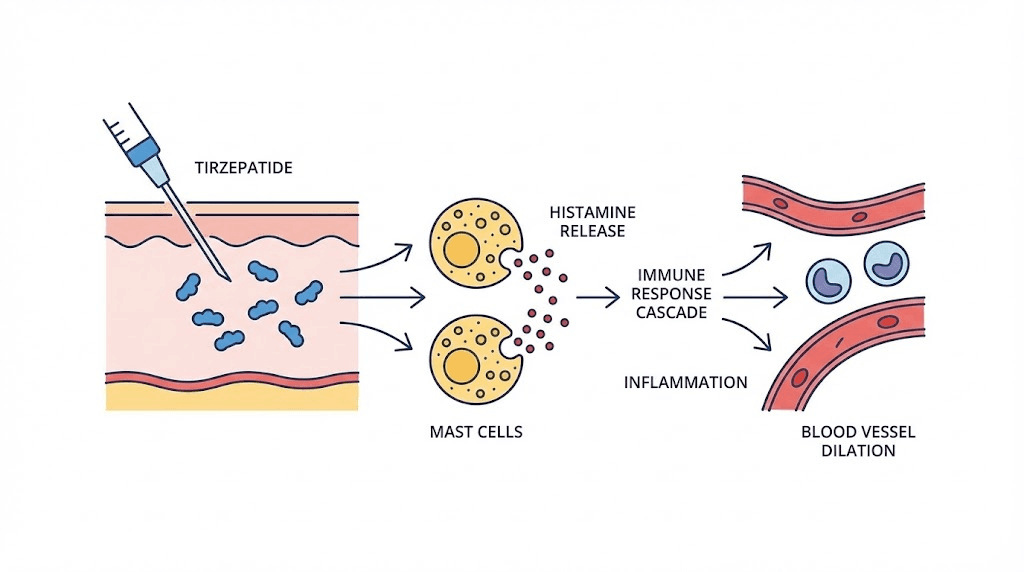
This is a localized inflammatory response. Your immune system recognizes the injected medication as foreign and sends white blood cells to the area, dilating blood vessels in the process. The result is redness and warmth, the classic signs of a normal immune response doing its job.
Itching and pruritus
Itching often accompanies redness but can also appear independently. It typically starts 2 to 12 hours after injection and peaks around 24 hours. The itch ranges from mildly annoying to intensely distracting, and scratching makes it significantly worse by releasing more histamine into the surrounding tissue.
Histamine is the primary culprit here. Mast cells in the skin degranulate in response to the injected medication, releasing histamine that activates nerve endings and creates that maddening itch. This is why antihistamines work so well for this specific symptom. Understanding the mechanisms behind tirzepatide side effects helps you target treatment more effectively.
Swelling and induration
Swelling at the injection site can range from subtle puffiness to a firm, raised area several centimeters across. Induration, the medical term for a hardened area under the skin, develops when the inflammatory response causes fluid accumulation and tissue thickening. It typically peaks at 24 to 48 hours and resolves over 3 to 7 days.
The amount of swelling often correlates with injection depth and speed. Injecting too fast can create a bolus of medication that triggers a stronger local reaction. Injecting too shallow, into the dermis rather than the subcutaneous fat, also increases swelling. Proper tirzepatide injection technique significantly reduces this type of reaction.
Bruising
Bruising occurs when the needle nicks a small blood vessel during injection. It presents as a purple or blue discoloration that gradually fades through green and yellow over 7 to 14 days. Bruising is technically not an injection site reaction in the same category as redness or itching, since it results from mechanical trauma rather than an immune response. But it causes cosmetic concern and discomfort.
People who take blood thinners, aspirin, or fish oil supplements bruise more easily. So do those who inject into areas with less subcutaneous fat. The abdomen generally produces less bruising than the thigh because it typically has a thicker fat layer, creating more distance between the needle and underlying blood vessels. Check our guide on where to inject GLP-1 medications for detailed site selection guidance.
Lumps and nodules
Firm lumps under the skin are surprisingly common with subcutaneous injections, and tirzepatide is no exception. These nodules form when the injected medication creates a depot, a concentrated pocket of fluid that the body absorbs gradually. Most lumps measure 0.5 to 2 centimeters in diameter, feel firm to the touch, and are painless or mildly tender.
They typically resolve within 5 to 10 days as the body absorbs the medication. Injecting too quickly, using cold medication straight from the refrigerator, or repeatedly injecting into the same spot all increase the likelihood of nodule formation. Experienced users who practice consistent tirzepatide injection protocols with proper site rotation rarely develop persistent nodules.
Pain and burning
A stinging or burning sensation during or immediately after injection affects some users, particularly at higher doses. The burning typically lasts 5 to 30 minutes and fades completely. Some users describe a brief sharp pain during needle insertion followed by a deeper burning sensation as the medication disperses under the skin.
Cold medication causes more burning than room-temperature medication. This is one of the simplest fixes available, as allowing the vial or pen to reach room temperature for 30 minutes before injection dramatically reduces the burning sensation. For users experiencing persistent pain, our guide on tirzepatide body aches covers broader pain management strategies.
Why injection site reactions happen with tirzepatide
Understanding the mechanisms behind injection site reactions transforms your approach from reactive to strategic. When you know why your body responds a certain way, you can predict reactions, prevent them, and treat them more effectively. The science here is straightforward, even if the reactions feel anything but.
Local immune response mechanisms
Your skin is your largest immune organ. It contains millions of immune cells whose entire purpose is detecting and responding to foreign substances. When tirzepatide enters the subcutaneous tissue, these immune cells recognize it as something that does not belong there. They launch a localized inflammatory response designed to contain and neutralize the perceived threat.
This response involves multiple cell types. Macrophages engulf and process the medication. Dendritic cells present fragments of it to T cells. Mast cells release histamine, prostaglandins, and other inflammatory mediators. The combined effect produces the redness, swelling, warmth, and itching that characterize most injection site reactions.
The reaction is local, not systemic. Your body is not rejecting tirzepatide. It is simply recognizing and responding to a foreign substance at the entry point. This is fundamentally different from a systemic allergic reaction, which involves the entire immune system and can be dangerous. Understanding this distinction is crucial for knowing when to treat at home and when to seek medical guidance for tirzepatide concerns.
Mast cell activation and histamine release
Mast cells are the primary drivers of injection site itching and redness. These cells sit in the connective tissue beneath the skin, loaded with granules containing histamine, heparin, and various enzymes. When triggered, they degranulate, releasing their contents into surrounding tissue.
Several factors trigger mast cell degranulation at injection sites. The physical trauma of needle insertion damages nearby mast cells, causing direct release. The pH of the injected solution, if it differs significantly from tissue pH, triggers additional degranulation. And in some individuals, components of the medication itself activate mast cell surface receptors.
The histamine released causes blood vessel dilation (redness), increased vascular permeability (swelling), and nerve ending stimulation (itching and pain). This entire cascade happens within minutes and peaks within hours. It is the same mechanism behind mosquito bites, poison ivy, and most other itchy skin reactions. That is why the same treatments, antihistamines and topical corticosteroids, work across all of these conditions.
Anti-tirzepatide antibody development
Here is where the data gets interesting. In pooled clinical trial data, injection site reactions occurred in 4.6% of tirzepatide-treated patients who developed anti-tirzepatide antibodies, compared to only 0.7% of those who did not develop antibodies. That is a six-fold difference.
Antibody development means the immune system has created specific proteins that recognize and bind to tirzepatide. When these antibodies encounter tirzepatide at the injection site, they activate a more targeted and often more vigorous immune response. This antibody-mediated reaction tends to be more consistent, occurring after every injection rather than sporadically, and may increase in intensity over time as antibody levels rise.
Not everyone who develops antibodies experiences clinical effects. Many people with detectable anti-tirzepatide antibodies have no injection site reactions at all, and the antibodies do not appear to reduce the medication effectiveness in most cases. But if you notice that your reactions are getting progressively worse over weeks or months, antibody development is a possible explanation worth discussing with a healthcare provider.
Dose-dependent relationship
Clinical trial data shows a correlation between tirzepatide dose and injection site reaction rates. Higher doses inject more medication into the same tissue area, creating a larger depot and triggering a proportionally stronger immune response. Users who escalate from 2.5mg of tirzepatide to 5mg and beyond sometimes notice that reactions worsen at each new dose level before stabilizing.
A case described in dermatology literature documented a 48-year-old woman whose localized erythematous reaction appeared specifically during dose escalation, lasting 5 to 6 days after each injection at the new dose. Once she stabilized at her maintenance dose, the reactions gradually diminished. This pattern suggests the immune system needs time to adapt to each new concentration level.
For users experiencing dose-dependent reactions, microdosing tirzepatide offers a gentler escalation approach. By moving up in smaller increments, you give your immune system more time to adjust, potentially reducing the intensity of site reactions at each step. Check the tirzepatide dose chart for standard escalation schedules, and discuss modifications with your provider if reactions are problematic.
Compounded vs brand formulation factors
Not all tirzepatide formulations are identical. Brand-name Mounjaro and Zepbound do not contain preservatives and come in single-use pens. Compounded tirzepatide, on the other hand, often comes in multi-dose vials that may contain preservatives like benzyl alcohol to prevent bacterial contamination. Some compounded formulations also include additives like niacinamide, vitamin B12, or glycine.
These additives can independently trigger injection site reactions. Benzyl alcohol is a known skin irritant at certain concentrations. Niacinamide can cause flushing. B12 (cyanocobalamin or methylcobalamin) occasionally causes localized reactions. If you switched from brand to compounded tirzepatide and noticed new injection site reactions, the formulation difference is a likely culprit. Our guides on tirzepatide glycine B12 compounds and tirzepatide methylcobalamin explain what each additive does and why it might cause reactions.
Immediate treatment protocols for injection site reactions
You have a reaction. It happened. Now what? The treatment you apply in the first few hours makes a significant difference in how quickly the reaction resolves and how uncomfortable the process becomes. Here are the evidence-based first-line treatments, ranked by effectiveness and ease of access.
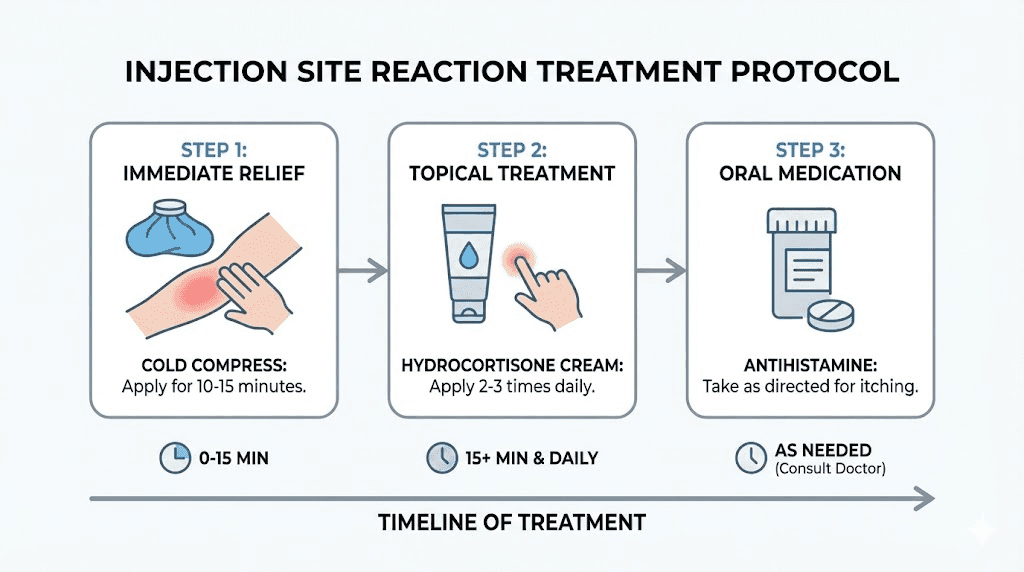
Cold compress application protocol
Cold is your best friend in the first 48 hours. It constricts blood vessels, reducing blood flow to the area and limiting the spread of inflammation. It numbs nerve endings, providing immediate itch and pain relief. And it slows the metabolic activity of immune cells, dampening the overall reaction intensity.
Step-by-step cold compress protocol:
Timing: Apply within 1 hour of noticing the reaction for best results
Preparation: Wrap ice pack or frozen gel pack in a thin cloth or paper towel, never place ice directly on skin
Application: Press gently against the affected area for 10 to 15 minutes
Frequency: Repeat every 2 to 3 hours during the first 24 hours
Duration: Continue cold compress therapy for the first 48 hours
Safety: Never exceed 15 minutes per application, check skin for signs of frostbite (white, waxy appearance)
A pre-injection cold application also helps. Pressing an ice pack against the injection site for 30 to 60 seconds before injecting constricts local blood vessels, reducing the chance of bruising and potentially dampening the initial immune response. This simple step takes almost no effort and can meaningfully reduce reaction severity.
For those managing their entire tirzepatide dosage protocol, integrating cold compress preparation into the injection routine ensures you are always ready. Keep a small gel pack in the refrigerator specifically for injection days.
Topical hydrocortisone 1% protocol
Over-the-counter hydrocortisone cream is the most effective topical treatment for injection site redness, itching, and swelling. It works by suppressing the local inflammatory response, reducing the production of prostaglandins and leukotrienes that drive swelling and itch.
Application protocol:
Product: Hydrocortisone 1% cream (available at any pharmacy without prescription)
Timing: Apply after noticing the reaction, not before injection
Amount: Thin layer covering the entire affected area plus a 1-centimeter margin
Frequency: Twice daily (morning and evening) until the reaction resolves
Duration: Typically 2 to 5 days, do not use for more than 7 consecutive days without medical guidance
Important: Do NOT apply hydrocortisone before injection, as it can interfere with medication absorption
For reactions that do not respond to 1% hydrocortisone, a healthcare provider can prescribe stronger topical corticosteroids (triamcinolone 0.1% or betamethasone 0.05%). However, these are rarely needed for standard injection site reactions. The same inflammation management principles apply to other GLP-1 medication side effects, making hydrocortisone a versatile addition to any injection supply kit.
Oral antihistamine protocol
Antihistamines block the histamine receptors that cause itching and redness. They are most effective when taken early, before the histamine cascade fully develops, though they still provide relief when taken after symptoms appear.
Recommended antihistamine options:
Cetirizine (Zyrtec): 10mg once daily, non-drowsy, fast-acting (within 1 hour), most effective for injection site itch
Loratadine (Claritin): 10mg once daily, non-drowsy, good for mild reactions
Fexofenadine (Allegra): 180mg once daily, non-drowsy, least sedating option
Diphenhydramine (Benadryl): 25 to 50mg every 6 hours, causes drowsiness but strongest anti-itch effect, best for severe reactions or nighttime use
Strategic timing approach:
Take a non-drowsy antihistamine 1 hour before your scheduled injection. This pre-loads histamine receptor blockade so that when mast cells degranulate during injection, the released histamine has fewer receptors to bind. Many experienced users report that this single step reduces reaction severity by 50% or more.
If you already take a daily antihistamine for allergies, you are partially protected. But consider timing your daily dose to coincide with your injection schedule for maximum benefit. For users tracking their complete tirzepatide supplement regimen, adding a strategic antihistamine is one of the most impactful additions.
One important caveat. Research suggests that premedication with antihistamines does not completely prevent injection site reactions. It reduces severity and duration, but reactions may still occur. Do not be discouraged if you took an antihistamine and still got a reaction. The reaction would likely have been worse without it.
OTC pain relievers for discomfort
When injection site reactions cause pain, tenderness, or significant discomfort, over-the-counter pain relievers provide additional relief. The two main options work through different mechanisms and have different strengths.
Ibuprofen (Advil, Motrin): 200 to 400mg every 4 to 6 hours as needed. Ibuprofen is an anti-inflammatory, meaning it both reduces pain and actively decreases the inflammatory response at the injection site. This dual action makes it the preferred choice for reactions involving significant swelling or redness. Maximum daily dose: 1200mg without medical supervision.
Acetaminophen (Tylenol): 650 to 1000mg every 4 to 6 hours as needed. Acetaminophen reduces pain but does not have significant anti-inflammatory effects. Choose this option if you cannot take NSAIDs due to stomach sensitivity, kidney concerns, or blood thinner use. Maximum daily dose: 3000mg.
Do not apply topical NSAIDs (like Voltaren gel) to injection sites, as they can interfere with medication absorption. Oral pain relievers provide systemic relief without this concern. Users experiencing broader pain issues might find our guide on tirzepatide and joint pain helpful for comprehensive pain management.
Calamine lotion for itch-dominant reactions
When itching is the primary complaint and redness is minimal, calamine lotion offers an alternative to hydrocortisone. The zinc oxide and ferric oxide in calamine create a cooling, soothing effect on the skin that reduces itch without the steroid component.
Apply a thin layer to the itchy area and allow it to dry. Reapply as needed throughout the day. Calamine is safe for extended use without the 7-day limitation that applies to hydrocortisone. It works best for mild to moderate itching and is particularly useful for people who prefer to avoid topical steroids.
Treatment strategies organized by reaction type
Different reactions require different approaches. A bruise does not respond to antihistamines. An itchy patch does not need ice. Matching your treatment to your specific reaction type produces faster results with less unnecessary intervention.
Treating redness and inflammation
Redness alone, without significant itch or swelling, responds best to cold therapy and anti-inflammatory measures.
Mild redness (less than 3 cm, fading within hours):
Cold compress for 10 minutes
No additional treatment needed
Monitor for expansion
Moderate redness (3 to 5 cm, lasting 1 to 3 days):
Cold compress every 2 to 3 hours for first 24 hours
Hydrocortisone 1% twice daily
Ibuprofen 200 to 400mg if uncomfortable
Significant redness (more than 5 cm, warm to touch, lasting more than 3 days):
Cold compress protocol as above
Hydrocortisone 1% twice daily
Oral antihistamine daily
Ibuprofen 400mg every 6 hours
If not improving by day 5, contact healthcare provider
Tracking the size of redness helps determine whether a reaction is improving or worsening. Use a pen to draw a circle around the redness margin and date it. If the redness expands beyond the circle in subsequent hours, the reaction is progressing and may need medical evaluation. This simple tracking technique gives you objective data rather than relying on subjective impressions about whether things look better or worse.
Treating persistent itching
Itching that persists beyond 24 hours or significantly impacts daily activities requires a more aggressive approach than single-agent therapy.
The anti-itch combination protocol:
Layer 1: Oral antihistamine (cetirizine 10mg in the morning)
Layer 2: Topical hydrocortisone 1% applied to affected area twice daily
Layer 3: Cold compress for breakthrough itch (10 minutes as needed)
Layer 4: Diphenhydramine 25mg at bedtime if itch disrupts sleep
Avoid scratching at all costs. Scratching causes mechanical mast cell degranulation, releasing additional histamine and creating a vicious itch-scratch cycle. If you cannot resist scratching, apply a cold compress to the area instead. The cold provides a competing sensation that satisfies the urge to scratch without causing additional inflammation.
Wearing loose, breathable clothing over the injection site also helps. Tight clothing creates friction that can worsen itch. Cotton fabrics are generally less irritating than synthetics. These same comfort strategies apply to managing other tirzepatide-related discomfort that interferes with daily life.
Treating swelling and lumps
Swelling and lumps follow a different treatment timeline than redness or itching. The key distinction is knowing when to use cold versus warm therapy.
First 48 hours (acute phase):
Cold compress only, 10 to 15 minutes every 2 to 3 hours
Do not massage the area
Ibuprofen 400mg every 6 hours if painful
Keep the area elevated when possible (propping up with a pillow if the injection was in the thigh)
After 48 hours (resolution phase):
Switch from cold to warm compress
Warm, damp cloth applied for 10 minutes, 3 to 4 times daily
Warmth increases blood flow, accelerating absorption of the medication depot and clearing inflammatory debris
Gentle massage is now acceptable, using light circular motions to help break up nodules
Most lumps resolve completely within 7 to 10 days. If a lump persists beyond 2 weeks, hardens significantly, or becomes increasingly painful, contact a healthcare provider. Persistent nodules occasionally require ultrasound evaluation to rule out other causes. For users managing their injection routine, proper tirzepatide reconstitution technique and correct injection depth help prevent nodule formation in the first place.
Treating bruising
Bruises follow their own timeline and respond to different interventions than inflammatory reactions.
Immediate (first 24 hours):
Cold compress for 10 to 15 minutes, repeat 3 to 4 times
Do not massage, rub, or apply heat
Pressure with a cotton ball for 30 to 60 seconds immediately after withdrawing the needle reduces bleeding
Days 2 to 3:
Switch to warm compress (10 minutes, 3 to 4 times daily)
Warmth promotes reabsorption of trapped blood
Arnica cream or gel can be applied (some evidence for faster bruise resolution, though not definitive)
Days 4 to 14:
Continue warm compresses if desired
Allow natural resolution, the bruise will transition through purple, blue, green, and yellow before fading
Vitamin K cream may help speed resolution (limited evidence)
If you bruise frequently with injections, review your technique. Are you inserting the needle at a proper 90-degree angle? Are you using a quick, dart-like insertion rather than slowly pushing the needle through the skin? Are you injecting into the correct tissue layer? Proper technique eliminates most injection bruising.
Treating pain and burning
Injection site pain has two phases. The acute burning during and immediately after injection, and the lingering soreness that may persist for hours to days.
For acute burning during injection:
Allow medication to reach room temperature (30 minutes out of refrigerator)
Inject slowly, taking 10 to 15 seconds for the full dose
Apply ice to the site for 30 to 60 seconds before injection to numb the area
Use a new, sharp needle (never reuse needles)
For lingering soreness after injection:
Cold compress for 10 to 15 minutes
Acetaminophen or ibuprofen for pain relief
Avoid touching, pressing, or rubbing the area
Wear loose clothing over the injection site
Users who switched from syringes to injection pens often report less injection pain because pens use thinner needles and deliver the medication at a more controlled rate. If you are using vials and syringes for compounded tirzepatide, consider discussing pen options with your provider. For comprehensive guidance on compounded tirzepatide dosing and administration, our calculator and guides walk you through the process.
Prevention strategies that actually work
The best injection site reaction is the one that never happens. Prevention is consistently more effective than treatment for reducing the overall burden of injection site reactions. These strategies, drawn from clinical evidence and the real-world experience of experienced tirzepatide users, address the most common root causes.
Proper injection technique
Technique problems cause more injection site reactions than any other factor. The difference between a reaction-free injection and an angry red welt often comes down to three variables: angle, depth, and speed.
Angle: Always inject at a 90-degree angle to the skin surface. This ensures the needle reaches the subcutaneous fat layer rather than depositing medication into the dermis (too shallow) or muscle (too deep). If you are very lean with minimal subcutaneous fat, pinch the skin to create a fold and inject into the center of that fold.
Depth: The needle should penetrate through the skin and into the subcutaneous fat layer, which sits between the skin and the muscle. For most people, this means the needle should be fully inserted. For very lean individuals, a shorter needle or pinched skin prevents intramuscular injection, which causes more pain and potentially different absorption kinetics.
Speed: Inject slowly and steadily. Rushing the injection creates a high-pressure bolus of medication that mechanically disrupts tissue and triggers a stronger inflammatory response. Take 10 to 15 seconds for the full injection. After completing the injection, wait 5 to 10 seconds before withdrawing the needle to allow the medication to distribute.
These fundamentals apply whether you are using brand-name pens or reconstituted tirzepatide from vials. Mastering injection technique eliminates the most preventable cause of injection site reactions.
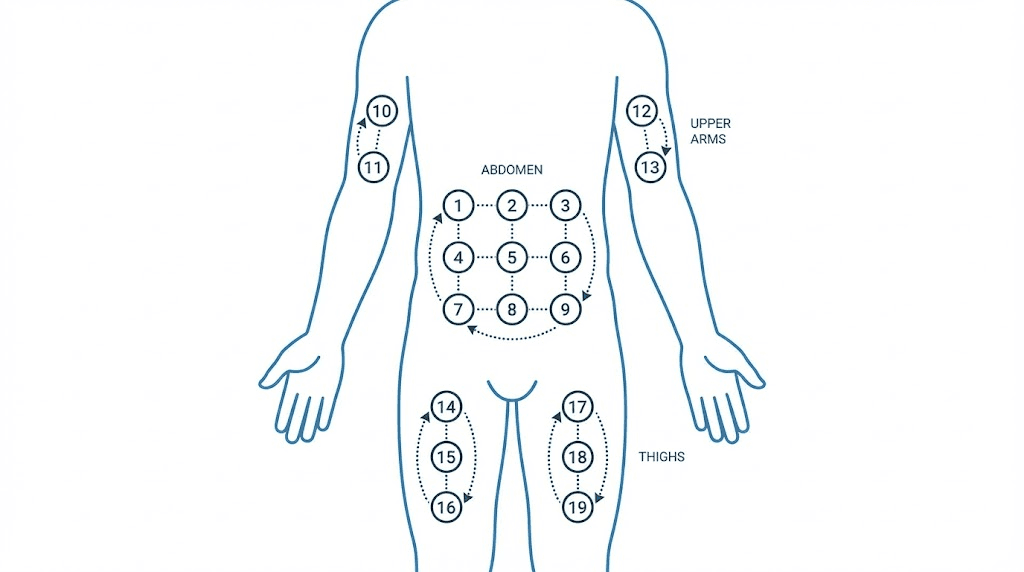
Site rotation system
Injecting into the same spot repeatedly is a guaranteed path to worsening reactions. The tissue becomes sensitized, developing localized immune memory that triggers faster and stronger responses with each subsequent injection. Lipodystrophy, the formation of permanent lumps or pits in the fat layer, is the long-term consequence of poor site rotation.
The three-region rotation system:
Region 1: Abdomen (at least 2 inches from the navel, alternating left and right sides)
Region 2: Front or outer thigh (middle third, alternating left and right legs)
Region 3: Upper arm (back of the arm, alternating sides, may need assistance)
Weekly rotation pattern:
Week 1: Left abdomen
Week 2: Right thigh
Week 3: Right abdomen
Week 4: Left thigh
Week 5: Left abdomen (different spot from Week 1)
Within each region, maintain at least 1 inch between consecutive injection sites. Some users find it helpful to mentally divide their abdomen into a grid pattern, moving systematically through each quadrant. This approach ensures no single area receives injections more than once every 4 to 6 weeks, giving tissue ample time to recover.
For detailed guidance on injection locations, our comprehensive guide on how to inject GLP-1 medications covers everything from site selection to needle disposal. The best injection site research for GLP-1 medications applies equally to tirzepatide.
Temperature preparation
Cold medication causes more injection site reactions than room-temperature medication. This is one of the most overlooked prevention strategies, and one of the simplest to implement.
The 30-minute rule: Remove tirzepatide from the refrigerator 30 minutes before injection. This allows the solution to reach room temperature, reducing the thermal shock to tissue and decreasing the viscosity of the solution for smoother injection.
Do not microwave, heat in hot water, or otherwise artificially warm the medication. Excessive heat degrades the peptide structure. Simply setting it on the counter at room temperature is sufficient. For those managing tirzepatide refrigeration and storage, this 30-minute window does not compromise medication stability.
If you use compounded tirzepatide from multi-dose vials, the same principle applies. Remove the vial from the fridge 30 minutes before drawing your dose. Check our guide on compounded tirzepatide room temperature stability for detailed time limits.
Skin preparation
Proper skin preparation reduces both infection risk and reaction risk.
The correct preparation sequence:
Clean the injection site with an alcohol swab using a single circular motion from center outward
Wait for the alcohol to dry completely (15 to 30 seconds)
Do not blow on the area or fan it to speed drying
Do not inject through wet alcohol, as this pushes alcohol into the tissue and causes stinging
Injecting through wet alcohol is one of the most common beginner mistakes and one of the easiest to fix. The alcohol irritates subcutaneous tissue and causes a burning sensation that gets misidentified as a medication reaction. Simply waiting an extra 15 seconds for complete drying eliminates this issue entirely.
Avoid injecting into skin that shows any of the following: bruising from previous injections, scars, stretch marks, areas of thickened skin, rashes, or sunburn. These areas have altered blood flow and immune cell distribution that increase reaction risk. Choose a clean, healthy area of skin each time. These preparation principles are universal for all peptide injections.
Injection speed and depth optimization
Speed and depth deserve additional emphasis because they are the most controllable variables and the most common sources of preventable reactions.
Speed optimization: Count to 10 slowly while depressing the plunger or holding the pen button. This ensures a controlled, even flow rate that distributes medication smoothly through the subcutaneous tissue rather than creating a concentrated bolus. After the full dose is delivered, continue holding the needle in place for 5 to 10 seconds. This prevents medication from leaking back through the needle track, which causes surface irritation and wastes medication.
Depth optimization: For abdominal injections, pinching a fold of skin is recommended for people with less than 2 inches of abdominal fat. Insert the needle into the center of the fold at a 90-degree angle. For the thigh, most people have sufficient subcutaneous fat to inject without pinching. The needle should go all the way in for standard insulin-length needles (4mm to 8mm).
Experienced users who have their tirzepatide mixing ratios and injection technique optimized rarely experience significant reactions. If you are new to self-injection, expect a learning curve. Reactions often decrease naturally as your technique improves over the first month.
When injection site reactions get worse with dose escalation
Dose escalation is where many users first encounter significant injection site reactions. You tolerated the starting dose just fine. But the moment you moved up, your body responded differently. This pattern is common, predictable, and manageable.
The antibody connection
Higher doses expose the immune system to larger quantities of the tirzepatide molecule, increasing the probability of antibody formation. Once antibodies form, each subsequent injection triggers a more targeted immune response at the injection site. The antibody-antigen interaction activates complement proteins and recruits additional immune cells, producing a reaction that is qualitatively different from the simple histamine-mediated response seen with initial injections.
This does not mean higher doses are unsafe or that you should avoid escalation. The SURPASS clinical trials used doses up to 15mg, and the majority of participants completed the trials without discontinuing due to injection site reactions. But awareness of this mechanism helps you prepare and respond appropriately.
If reactions first appeared or significantly worsened at a specific dose level, discuss the following options with your healthcare provider: extended time at the current dose before escalating further, smaller escalation increments, pre-injection antihistamine protocol, or exploring whether the therapeutic goals can be achieved at a lower dose.
Adjusting your approach at higher doses
At doses of 10mg and above, injection volume increases significantly, especially with compounded formulations. A larger injection volume means more medication concentrated in one area, which inherently triggers a stronger local response.
Strategies for higher-dose injections:
Split the injection: Some providers recommend splitting higher doses across two injection sites. For example, injecting half the dose in the left abdomen and the other half in the right thigh. This reduces the concentrated volume at each site and may decrease reaction severity.
Increase dilution: For compounded tirzepatide, using a larger volume of bacteriostatic water during reconstitution creates a less concentrated solution. While this means injecting a larger volume of fluid, the lower concentration reduces the intensity of the local immune response.
Extended injection time: At higher volumes, take even longer to inject, 15 to 20 seconds rather than 10. The slower rate allows tissue to accommodate the medication more gradually.
Pre-treatment protocol: Combine pre-injection antihistamine (1 hour before) with pre-injection ice (30 to 60 seconds before) and post-injection cold compress (10 to 15 minutes after) for maximum prevention.
Users who have worked through the full tirzepatide dosing escalation schedule often report that reactions peaked during the transition periods and subsided once they stabilized at each dose level. Patience and consistent technique carry you through.
Compounded tirzepatide and injection site reactions
Compounded tirzepatide introduces variables that brand-name formulations do not. Understanding these differences helps you identify whether your reactions stem from the tirzepatide itself or from the specific formulation you are using.
Preservatives and additives
Multi-dose vials of compounded tirzepatide typically contain bacteriostatic water with 0.9% benzyl alcohol as a preservative. Benzyl alcohol is generally well-tolerated, but at injection sites it can cause a localized stinging or burning sensation that some users mistake for a reaction to the tirzepatide itself.
Common additives in compounded formulations:
Niacinamide (vitamin B3): Can cause flushing, warmth, and redness at the injection site. If your injection site turns red and feels warm within minutes, niacinamide may be contributing.
Cyanocobalamin or methylcobalamin (B12): Occasionally causes injection site discomfort and redness. The tirzepatide B12 combination is common but not universally tolerated.
Glycine: Generally well-tolerated and may actually reduce injection site reactions by buffering the solution pH. Tirzepatide with glycine formulations tend to produce fewer complaints.
If you suspect an additive is causing your reactions, ask your compounding pharmacy about a formulation without the suspected additive. Some pharmacies offer plain tirzepatide without additional vitamins or supplements. Comparing your reaction history across different formulations from providers like Empower Pharmacy, Strive Pharmacy, or other affordable tirzepatide sources can help isolate the culprit.
Reconstitution and handling factors
How compounded tirzepatide is reconstituted and handled also affects injection site reactions. Incorrect reconstitution procedures can create problems that look like medication reactions but are actually preparation errors.
Common reconstitution errors that cause reactions:
Over-agitation: Shaking the vial vigorously creates foam and can denature the peptide, producing aggregated protein fragments that trigger stronger immune responses. Always swirl gently, never shake.
Wrong diluent: Using sterile water instead of bacteriostatic water, or vice versa, changes the solution properties. Always use the diluent specified by your pharmacy.
Contamination: Not cleaning the vial stopper with alcohol before drawing, or touching the needle to non-sterile surfaces, introduces bacteria that can cause true infection rather than simple reactions.
Incorrect volume: Using too little diluent creates an overly concentrated solution that is more irritating to tissue.
Our comprehensive tirzepatide reconstitution guide walks through the correct procedure step by step. For precise volume calculations, use the compounded tirzepatide dosage calculator to ensure accurate dilution ratios.
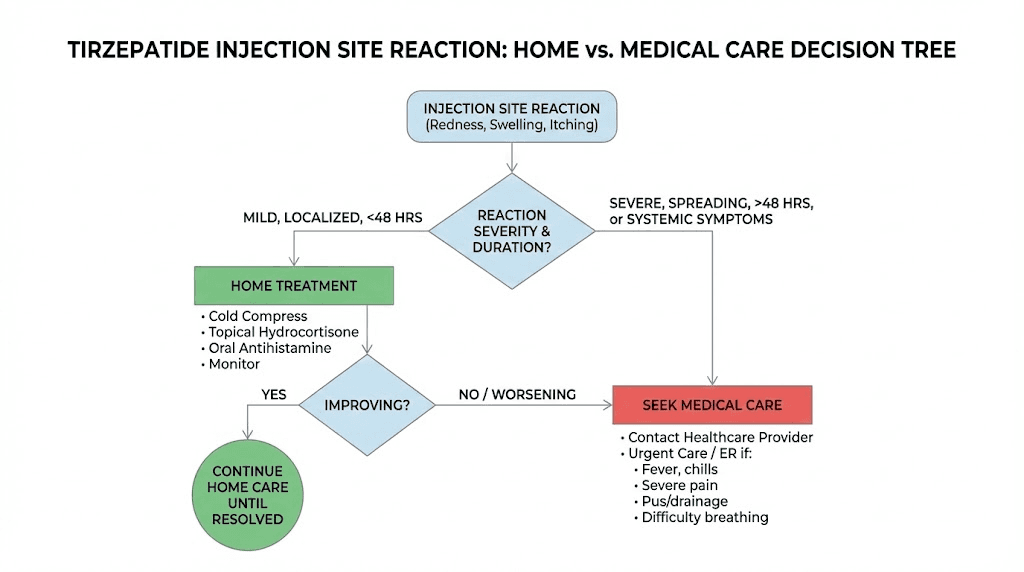
When to contact a healthcare provider
Most injection site reactions are self-limiting and respond to home treatment. But a small percentage require medical evaluation. Knowing the difference can prevent unnecessary anxiety while ensuring that genuine problems receive prompt attention.
Warning signs that need medical attention
Seek medical evaluation within 24 to 48 hours if you experience:
Redness that continues expanding beyond 48 hours after injection
Redness diameter exceeding 10 centimeters
Increasing pain (not decreasing) after 48 hours
Warmth and hardness accompanied by fever above 100.4 F (38 C)
Pus, drainage, or fluid oozing from the injection site
Red streaks extending outward from the injection site (sign of lymphangitis)
Reaction that has not shown any improvement after 7 days
Seek emergency medical care immediately if you experience:
Hives or rash spreading beyond the injection site to other body areas
Swelling of the face, lips, tongue, or throat
Difficulty breathing, wheezing, or shortness of breath
Dizziness, lightheadedness, or feeling faint
Rapid heartbeat
Severe abdominal pain
These emergency symptoms suggest a systemic allergic reaction (anaphylaxis), which is rare but documented with tirzepatide. A case report published in Cureus described a biphasic anaphylactic reaction occurring 20 minutes after tirzepatide injection, with diffuse urticaria, throat swelling, shortness of breath, and wheezing. This resolved with emergency treatment but required 24-hour monitoring due to the biphasic nature.
Allergic reactions vs local reactions
The distinction between a local injection site reaction and a systemic allergic reaction is critical for determining the appropriate response.
Local reaction characteristics:
Confined to the injection site and immediately surrounding area
Symptoms include redness, swelling, itching, pain, and warmth at the injection site only
No systemic symptoms (no fever, no hives elsewhere, no breathing difficulty)
Resolves within 3 to 7 days
Does not typically worsen after the first 24 to 48 hours
Systemic allergic reaction characteristics:
Symptoms extend beyond the injection site
Hives, rash, or flushing on areas distant from the injection site
Respiratory symptoms (coughing, wheezing, throat tightness)
Cardiovascular symptoms (rapid pulse, low blood pressure, dizziness)
Gastrointestinal symptoms (nausea, vomiting, cramping) beyond typical GI side effects
Local reactions almost never require discontinuation of tirzepatide. Systemic reactions always require medical evaluation before continuing. If you are uncertain which type of reaction you are experiencing, err on the side of caution and contact a healthcare provider. Managing uncertainty about side effects is part of navigating any medication protocol, and our guides on tirzepatide fatigue, GI side effects, and menstrual changes cover other common concerns.
Signs of infection
True injection site infections are rare with proper technique but do occur. They are caused by bacteria introduced during the injection process and require antibiotic treatment.
Infection warning signs:
Timing: Symptoms appear or worsen 2 to 5 days after injection (delayed compared to reaction symptoms)
Redness: Progressively expanding, bright red, with distinct borders
Pain: Increasing rather than decreasing over time
Warmth: Injection site feels significantly warmer than surrounding skin
Drainage: Yellow or green pus, cloudy fluid, or foul odor
Systemic: Fever, chills, general malaise
If you suspect infection, do not attempt to treat it at home with warm compresses or over-the-counter antibiotics. See a healthcare provider for evaluation and appropriate antibiotic therapy. Prevention through proper skin preparation, using new needles for each injection, and maintaining sterile technique during peptide mixing and handling is far easier than treating an established infection.
Alternative administration options
For users whose injection site reactions persist despite optimal technique and treatment, alternative administration routes eliminate the subcutaneous injection entirely. These options are not available to everyone and come with their own trade-offs, but they deserve consideration when injection site reactions significantly impact quality of life.
Oral tirzepatide
Oral tirzepatide bypasses the subcutaneous injection route entirely, eliminating injection site reactions as a concern. The oral vs injection comparison shows that efficacy appears similar in clinical studies, though oral formulations have their own considerations including specific fasting requirements and potentially different GI side effect profiles.
Oral tirzepatide is available in some markets and may become more widely available as regulatory approvals expand. For users experiencing persistent injection site reactions that do not respond to the treatment strategies in this guide, oral administration represents a legitimate alternative worth discussing with a healthcare provider. Tirzepatide tablets versus injections each have distinct advantages depending on individual circumstances.
Sublingual options
Sublingual tirzepatide involves placing a formulation under the tongue for absorption through the oral mucosa. This route also avoids subcutaneous injection. Tirzepatide drops and orally disintegrating tablets represent different approaches to non-injection delivery.
Sublingual absorption rates and bioavailability differ from subcutaneous injection, meaning doses may need adjustment. These formulations are typically available through compounding pharmacies rather than as brand-name products. If injection site reactions are driving you to consider a switch, have an honest conversation with your provider about the available options and their relative effectiveness for your specific situation.
Switching to semaglutide
Some users who experience persistent injection site reactions with tirzepatide find that switching to semaglutide resolves the issue. Since semaglutide is a different molecule, antibodies against tirzepatide do not cross-react with it, and the formulation differences mean the local immune response may be entirely different.
The side effect profiles of semaglutide vs tirzepatide differ in several ways, and injection site reactions are one area where individual response varies significantly between the two medications. The conversion between semaglutide and tirzepatide requires careful dose adjustment, so this is not a switch to make without medical guidance.
Switching is not giving up. It is strategic adaptation. If one medication causes intolerable side effects while another achieves similar results without them, the practical choice is clear. Our guide on switching between GLP-1 medications provides the dosage equivalency information you need for an informed conversation with your provider.
Long-term management strategies
Injection site reactions are not a one-time problem for many users. They recur with each injection, sometimes for weeks or months before improving. Long-term management requires a systematic approach rather than treating each reaction as an isolated event.
Tracking your reactions
Keeping a simple injection log transforms your understanding of your reactions from vague impressions into actionable data. Track the following with each injection:
Date and time of injection
Injection site (specific location, e.g., left abdomen, 3 inches from navel)
Dose
Medication temperature (did you warm it to room temperature?)
Reaction type (redness, itch, swelling, bruise, lump, pain)
Reaction severity (1 to 10 scale)
Reaction duration (hours or days until resolution)
Treatment used
Treatment effectiveness
After several weeks of tracking, patterns emerge. You might discover that thigh injections cause less reaction than abdominal injections. Or that reactions are worse on weeks when you forgot to warm the medication. Or that pre-injection antihistamines cut your reaction severity in half. These insights allow you to optimize your injection protocol based on your own data rather than generic recommendations.
Users who track diligently alongside their tirzepatide weight loss timeline often find that injection site reactions become a minor inconvenience rather than a major concern once they identify and address their specific triggers.
Building tolerance over time
The immune system adapts. For many users, injection site reactions that were significant during the first few weeks diminish substantially by month 2 or 3. The body gradually develops tolerance to the medication, reducing the intensity of the local immune response with each exposure.
This tolerance-building process is analogous to allergy immunotherapy, where repeated exposure to an allergen gradually desensitizes the immune system. The key is consistent, regular injection. Skipping doses or taking extended breaks can reset the tolerance process, potentially causing reactions to return at previous intensity when you resume.
If your reactions are tolerable but annoying, treating them and continuing the protocol often leads to natural resolution over time. The published case literature supports this, showing that most patients who continued tirzepatide through mild to moderate injection site reactions experienced gradual improvement without needing to discontinue.
For users concerned about whether their reactions indicate a deeper problem, or for those who want to optimize every aspect of their protocol, SeekPeptides offers comprehensive resources including troubleshooting guides for tirzepatide, detailed diet plans, meal planning resources, and information on foods to avoid while on tirzepatide that can help maximize your results while minimizing side effects.
The complete injection day protocol
Putting it all together, here is the optimal injection day protocol that incorporates every prevention strategy and treatment preparedness measure discussed in this guide.
Before injection (preparation phase)
30 minutes before: Remove tirzepatide from the refrigerator to reach room temperature
15 minutes before: Gather supplies: alcohol swabs, cold pack, hydrocortisone cream, clean needle
1 hour before: Take oral antihistamine (cetirizine 10mg) if you have a history of reactions
Choose injection site: Check your log for the last site used. Select a different region. Inspect the skin for any bruising, scarring, or irritation from previous injections.
During injection
Clean: Alcohol swab in circular motion. Wait for complete drying (15 to 30 seconds).
Optional ice: Apply cold pack to injection site for 30 to 60 seconds if you are prone to reactions
Pinch: If lean, pinch a fold of skin at the injection site
Insert: Quick, dart-like insertion at 90 degrees
Inject: Slow, steady depression of plunger or pen button. Count slowly to 10 or 15.
Hold: Keep needle in place for 5 to 10 seconds after full dose delivery
Withdraw: Straight out, same angle as insertion
Pressure: Press a cotton ball or gauze pad to the site for 30 to 60 seconds. Do not rub.
After injection (monitoring phase)
Immediately: Apply cold compress for 10 to 15 minutes
First hour: Monitor for any unusual symptoms beyond the injection site
First 24 hours: Repeat cold compress every 2 to 3 hours if a reaction develops
First 48 hours: Apply hydrocortisone 1% twice daily if redness or itching persists
Day 3 to 7: Switch to warm compress if swelling or lumps remain. Continue hydrocortisone if needed.
Log: Record all details in your injection tracker
This protocol represents the cumulative wisdom of clinical evidence and experienced user practice. It addresses prevention, immediate treatment, and ongoing management in a single systematic approach. Users following their tirzepatide dosage schedule with this level of preparation rarely experience reactions that disrupt their daily lives.
For researchers serious about optimizing every aspect of their peptide protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, proven protocols, detailed peptide calculators, and a community of thousands who have navigated these exact questions. Whether you are calculating doses with the tirzepatide dosage calculator, exploring how fast tirzepatide works, reviewing before and after results, or managing side effects like constipation and fatigue, the resources are there to support every step of your journey.
Frequently asked questions
How long do tirzepatide injection site reactions last?
Most mild reactions resolve within 24 to 48 hours without treatment. Moderate reactions with significant redness and itching typically clear within 3 to 5 days with appropriate treatment. Severe reactions like the one documented in published case reports can take up to a month to fully resolve, though these are uncommon. Using the treatment protocols in this guide, most users see significant improvement within 1 to 2 days. Our overview of tirzepatide timelines covers broader expectations.
Can I still take tirzepatide if I have injection site reactions?
Yes, in the vast majority of cases. Local injection site reactions are not a medical reason to discontinue tirzepatide. They are uncomfortable but not dangerous. The exception is if you experience signs of a systemic allergic reaction (hives spreading beyond the injection site, breathing difficulty, facial swelling), which requires immediate medical evaluation before continuing. Discuss persistent reactions with your healthcare provider to develop a personalized management plan.
Will injection site reactions get better over time?
For most users, yes. The immune system gradually develops tolerance to the medication with repeated exposure. Many users report that reactions that were significant during the first month become barely noticeable by months 2 to 3. Consistent injection technique and regular dosing schedule support this tolerance-building process. Tracking your reactions over time with a simple log provides objective evidence of improvement that can be reassuring during the adjustment period.
Do injection site reactions mean I am allergic to tirzepatide?
Not necessarily. Local injection site reactions are a normal immune response to a foreign substance entering the skin and do not indicate true allergy. True allergic reactions involve systemic symptoms, including hives beyond the injection site, respiratory symptoms, and cardiovascular symptoms. If you are uncertain, a healthcare provider can help distinguish between local reactions and true allergic responses. In clinical trials, the rate of serious allergic reactions to tirzepatide was very low.
Does the injection site affect how well tirzepatide works?
The injection site can affect absorption rate slightly but does not significantly impact overall effectiveness. Abdominal injections tend to absorb somewhat faster than thigh injections, and timing your injection consistently helps maintain steady medication levels. The most important factor for effectiveness is consistent weekly dosing at the prescribed amount, regardless of injection site. Use the tirzepatide dosage guide to ensure accurate dosing.
Should I use ice before or after tirzepatide injection?
Both. Ice before injection (30 to 60 seconds) numbs the area and constricts blood vessels, reducing pain and bruising risk. Ice after injection (10 to 15 minutes) reduces the inflammatory response, limiting redness, swelling, and itching. For users with a history of reactions, the before-and-after ice protocol provides the most comprehensive prevention. Just make sure to let the alcohol swab dry completely before applying ice, and always wrap the ice pack in a thin cloth to prevent skin damage.
Are compounded tirzepatide injection site reactions worse than brand name?
This varies by individual and formulation. Some users report more reactions with compounded formulations due to preservatives (benzyl alcohol) and additives (niacinamide, B12). Others find no difference. If you suspect your compounded formulation is causing reactions, ask your pharmacy about a formulation without additives. Comparing experiences across different pharmacies like Empower or Priority Meds can help identify whether the formulation is the issue.
Can I take Benadryl before tirzepatide injection?
Yes, diphenhydramine (Benadryl) can be taken before injection to reduce reactions. However, it causes significant drowsiness, so most providers recommend non-drowsy alternatives like cetirizine (Zyrtec) or loratadine (Claritin) as the first-line preventive option. If non-drowsy antihistamines are not effective enough, taking diphenhydramine 25mg about 30 to 60 minutes before your injection, preferably in the evening, provides stronger histamine blockade.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your injection sites stay calm, your reactions stay mild, and your protocols stay on track.