Feb 12, 2026

Nobody should pay $1,069 per month for tirzepatide. And yet thousands of people do. They walk into a pharmacy, hand over their credit card, and absorb a cost that adds up to nearly $13,000 per year because they do not know the alternatives exist. Some of them have commercial insurance that would cover the medication for $25 a fill if they activated a free savings card. Others qualify for a manufacturer self-pay program that drops the price to $299. A few are months away from Medicare coverage at $50 per month and do not realize the program is coming.
The tirzepatide affordability landscape has changed faster than almost any medication in recent memory. Eli Lilly slashed prices on Zepbound vials in December of last year. Medicare coverage launches as early as April of this year. The FDA restricted compounding pharmacies, shrinking one affordable pathway while the manufacturer opened several new ones. The result is a confusing web of options where the "cheapest" choice depends entirely on your insurance status, your income, your location, and how comfortable you are navigating pharmaceutical bureaucracy.
This guide maps every legitimate pathway to affordable tirzepatide, ranks them by cost, and helps you identify which one fits your specific situation. No vague advice. No outdated pricing. Just the current numbers, the qualifying criteria, and the steps to access each option.
SeekPeptides has analyzed dozens of access pathways, provider pricing structures, and patient assistance programs to build the most comprehensive affordability guide available.
Why tirzepatide costs what it costs
Before hunting for savings, understanding the pricing structure helps you negotiate from a position of knowledge rather than desperation.
Tirzepatide took over a decade and billions of dollars to develop. The SURMOUNT clinical trial program alone enrolled thousands of participants across multiple countries, producing the most impressive weight loss data ever seen in a randomized trial. Participants on the highest dose lost an average of 22.5% of their body weight over 72 weeks. That translates to roughly 56 pounds for someone starting at 250. The SURMOUNT-4 continuation study pushed total weight reduction past 25% for those who stayed on treatment through 88 weeks.
Those results cost money to produce. And Eli Lilly, like every pharmaceutical company, prices their product to recoup that investment while the patent protection lasts.
The list price for Mounjaro and Zepbound sits at approximately $1,069 per month without any discounts or insurance coverage. That number is the starting point, not the final price. Think of it like the sticker price on a car. Almost nobody actually pays it. The real price depends on your negotiating position, which in pharmaceutical terms means your insurance coverage, your eligibility for assistance programs, and your willingness to explore alternatives.
Here is the critical insight most people miss. Eli Lilly does not want you paying $1,069 per month. They want you on the medication long-term, which means they need the price to be sustainable. That is why they launched LillyDirect, created savings cards, expanded vial options, and negotiated Medicare coverage. Every one of these programs exists because Eli Lilly understands that a $25 per month patient who stays on treatment for three years is more valuable than a $1,069 per month patient who quits after two fills.
The real price range in practice
When you account for all available programs, tirzepatide actually costs anywhere from $25 to $449 per month for most people who do their homework. The $1,069 figure only applies to patients who walk into a retail pharmacy without insurance, without a savings card, without checking any manufacturer programs, and without exploring alternatives.
Access pathway | Monthly cost | Who qualifies |
|---|---|---|
Commercial insurance + savings card | $25 | Anyone with commercial drug coverage for Zepbound/Mounjaro |
Medicare Part D (launching 2026) | $50 | Medicare beneficiaries in participating plans |
Compounded (budget tier) | $166-$229 | Patients with documented medical need for compounding |
LillyDirect self-pay (starting dose) | $299 | Anyone with a prescription, no insurance required |
LillyDirect self-pay (maintenance) | $399-$449 | Anyone with a prescription at higher doses |
Commercial insurance without coverage + savings card | $499 | Insured patients whose plan does not cover Zepbound |
Retail pharmacy (no programs) | $1,069 | Nobody should be paying this |
That table contains the single most important piece of information in this entire article. Your job is to figure out which row applies to you, then follow the steps to access that pathway. The rest of this guide shows you exactly how.
Pathway 1: commercial insurance with savings card ($25 per month)
This is the cheapest legitimate way to get tirzepatide. Period.
If you have commercial health insurance through an employer, the marketplace, or a private plan, and that insurance covers either Zepbound or Mounjaro, you can activate a manufacturer savings card that drops your copay to as little as $25 per fill. That covers up to a three-month supply.
How the Zepbound savings card works
The Zepbound savings card is free to activate. You do not need to apply, qualify based on income, or prove financial hardship. If you have commercial insurance that covers Zepbound, you are eligible. The card provides maximum monthly savings of up to $620 per fill and a separate annual savings cap of $8,060. You can use it for up to 13 prescription fills per calendar year. The card expires at the end of this year.
To activate it, visit the official Zepbound savings page or ask your prescribing provider. Most electronic health record systems can apply the card directly at the point of prescribing. Your pharmacist can also process it at the counter.
The math is straightforward. If your insurance copay for Zepbound is $200 per month, the savings card covers up to $620, bringing your out-of-pocket cost to $0 (since the card covers the full copay). If your copay is $500, the card covers $500, and you pay the remainder. For most commercial plans, the copay lands well under $620, meaning you pay the $25 minimum.
The Mounjaro savings card (for diabetes patients)
Mounjaro is the same active ingredient as Zepbound, tirzepatide, but prescribed for type 2 diabetes rather than weight management. If you have type 2 diabetes and commercial insurance that covers Mounjaro, the savings card terms are nearly identical. Maximum monthly savings up to $150 for a one-month supply or $450 for a three-month supply, with an annual cap of $1,950.
Here is where it gets strategic. If you have both obesity and type 2 diabetes, your provider has flexibility in which brand to prescribe. Insurance formularies sometimes cover Mounjaro but not Zepbound, or vice versa. A conversation with your prescriber about which brand your specific plan covers could be the difference between paying $25 per month and paying $449.
What disqualifies you from savings cards
These programs are not available to everyone. Federal healthcare program recipients, including Medicare, Medicaid, Tricare, and Veterans Affairs beneficiaries, cannot use manufacturer savings cards. This is due to federal anti-kickback statutes, not a Eli Lilly policy decision. If you have government-funded insurance, skip to the Medicare or Medicaid sections below.
Patients without any insurance are also ineligible for the standard savings card terms, though Eli Lilly offers separate self-pay pathways through LillyDirect that we cover later.
Step-by-step: activating your savings card
First, call your insurance company or check your pharmacy benefit portal to confirm whether Zepbound or Mounjaro is on your formulary. If it is covered, ask about your expected copay amount. Then visit the official savings card website for whichever brand your insurance covers. Create an account and download the digital savings card. Provide the card information to your pharmacy or prescriber. Fill your prescription and verify the discount was applied at the register.
This entire process takes under 30 minutes and saves you over $10,000 per year compared to retail pricing. If you do nothing else after reading this article, check whether your insurance covers tirzepatide and activate the savings card.
Pathway 2: Medicare coverage at $50 per month (launching soon)
This is the most significant development in tirzepatide affordability for the 65+ population.
The Centers for Medicare and Medicaid Services announced a program that will allow eligible Medicare Part D beneficiaries to access GLP-1 medications, including Zepbound, for a maximum copay of $50 per month. The program launches as early as April of this year, with broader implementation expected in January of next year when Part D plan years begin.
What we know about Medicare coverage
The initial program operates as a short-term CMS initiative covering eligible beneficiaries for the remainder of the calendar year. Starting in January of next year, standalone prescription plans in original Medicare and Medicare Advantage plans will determine whether they want to participate in the five-year CMS pilot program with the same $50 per month cost-sharing structure.
This represents a fundamental shift. Previously, Medicare explicitly excluded weight loss medications from coverage. The change reflects growing recognition that obesity is a chronic disease with enormous downstream healthcare costs, and that treating it with effective medications like tirzepatide is more cost-effective than managing the complications of untreated obesity.
Who qualifies for Medicare tirzepatide coverage
The specific eligibility criteria are still being finalized, but the general framework requires a Medicare Part D prescription drug plan, a diagnosis of obesity or overweight with related comorbidities, and a prescription from a qualified provider. Individuals with type 2 diabetes may have additional coverage pathways through existing Mounjaro formulary inclusion.
If you are a Medicare beneficiary currently paying out of pocket for tirzepatide, or if you have been avoiding the medication because of cost, this program changes your calculation entirely. At $50 per month ($600 per year), tirzepatide becomes one of the most cost-effective treatments in the Medicare formulary relative to the health outcomes it produces.
What to do right now if you are on Medicare
Contact your Part D plan administrator and ask whether they plan to participate in the CMS GLP-1 coverage pilot. If they do not know yet, ask when they will have that information. Schedule an appointment with your provider to discuss tirzepatide eligibility. Having a prescription ready when coverage launches means you can start immediately rather than waiting weeks for approval.
If your current Part D plan does not participate, you may be able to switch plans during the next open enrollment period to one that does. This is a situation where choosing the right Part D plan could save you $5,000+ per year in medication costs.
Pathway 3: LillyDirect self-pay program ($299-$449 per month)
For patients without insurance coverage for tirzepatide, Eli Lilly created a direct-to-consumer pathway that bypasses pharmacies entirely.
LillyDirect is Eli Lilly manufacturer direct pharmacy. You get a prescription, submit it through their platform, and Zepbound ships to your door. No insurance required. No pharmacy middleman. No uncertainty about whether your order will be filled.
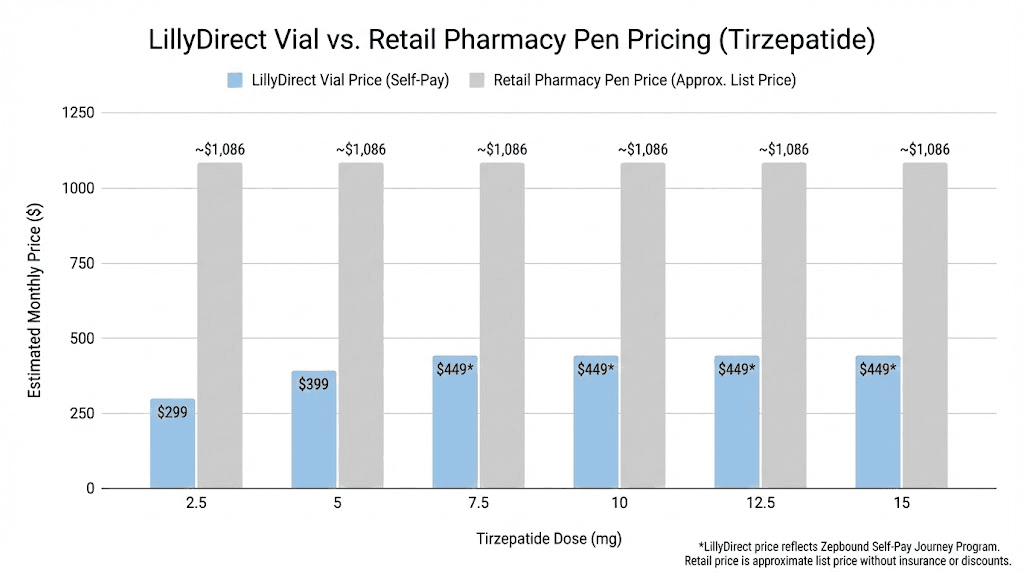
Current LillyDirect pricing (updated December)
Eli Lilly reduced prices on Zepbound single-dose vials in December of last year. The current structure looks like this.
Dose | Monthly price | Format |
|---|---|---|
2.5mg (starting) | $299 | Single-dose vial |
5mg | $399 | Single-dose vial |
7.5mg | $449 | Single-dose vial |
10mg | $449 | Single-dose vial |
12.5mg | $449 | Single-dose vial |
15mg | $449 | Single-dose vial |
These are single-dose vials, not the pre-filled autoinjector pens you might have seen in commercials. The vials require you to draw the medication with a syringe, similar to how you would use compounded tirzepatide. The key difference is that these vials are FDA-approved, manufactured under strict Good Manufacturing Practice standards, and contain the exact same formulation used in the SURMOUNT clinical trials.
Multi-dose pen options are also becoming available through LillyDirect. Pricing starts at $299 for the lowest dose and caps at $449 for higher doses. You must refill within 45 days to maintain program pricing.
Who should choose LillyDirect
This pathway makes the most sense if you do not have insurance that covers tirzepatide, you want FDA-approved medication with verified potency and purity, and your budget can accommodate $299-$449 per month. It also works well for patients who previously used compounded tirzepatide and want to transition to a brand-name product without the regulatory uncertainty.
The LillyDirect pricing is competitive with mid-range compounded providers. When you factor in the convenience of pre-measured single-dose vials (no multi-dose vial math), the FDA approval backing, and the elimination of questions about potency or purity, many patients find the small premium over budget compounded options worthwhile.
How to enroll in LillyDirect
Get a prescription for Zepbound from any licensed prescriber. Your provider sends the prescription electronically to LillyDirect through their EHR system. Create a LillyDirect account. Complete the intake questionnaire. Your medication ships directly to your home with temperature-controlled packaging. Walmart pickup is also available as an alternative to home delivery.
The entire process from prescription to first delivery typically takes 5-10 business days. Subsequent refills ship faster since your account is already established.
Pathway 4: compounded tirzepatide ($166-$399 per month)
This was once the most popular affordable tirzepatide option. The landscape has shifted significantly, but compounded tirzepatide still exists under specific circumstances.
What happened to compounded tirzepatide
During a nationwide shortage of brand-name tirzepatide, the FDA exercised enforcement discretion that allowed compounding pharmacies to produce the medication. This was not a blanket approval. It was a temporary allowance while Eli Lilly could not meet market demand.
In late 2024, the FDA determined the shortage was resolved. Enforcement discretion periods ended in early 2025, with Section 503A pharmacies given until February and Section 503B outsourcing facilities given until March. Courts have upheld the FDA decision against legal challenges from compounding pharmacies.
What is still legally available
Compounded tirzepatide can still be prescribed when a patient has a documented medical need that cannot be met by an FDA-approved formulation. The most common qualifying scenario is a verified allergy or sensitivity to an inactive ingredient in Mounjaro or Zepbound. General reasons like cost savings or personal preference do not meet the legal threshold under Section 503A compounding regulations.
Some providers continue to operate in this space through various legal interpretations and state-level regulatory frameworks. The availability varies significantly by state and by provider. If a telehealth company tells you compounded tirzepatide is freely available with no medical justification required, that is a red flag about their regulatory compliance.
Pricing from current compounded providers
For patients who do qualify for compounded tirzepatide, pricing typically ranges from $166 to $399 per month depending on the provider, dose, and subscription terms. Starting doses (2.5mg) cluster around $166-$229 per month. Maintenance doses (5mg-15mg) run $250-$450 per month. Longer subscription commitments (three to six months) often reduce per-month costs by 10-25%.
The critical consideration is that compounded tirzepatide has not undergone the same FDA review for safety, effectiveness, or quality as brand-name products. Dosing precision, potency, sterility, and stability may vary between compounding pharmacies. For a detailed comparison of compounded versus brand-name options, see our guide on compounded tirzepatide costs and safety.
How to evaluate a compounded provider
If you do pursue compounded tirzepatide, verify these non-negotiable requirements. The pharmacy must be licensed as either a 503A state-licensed pharmacy or an FDA-registered 503B outsourcing facility. A real healthcare provider, not just a questionnaire, must evaluate you before prescribing. The pharmacy should provide certificates of analysis showing third-party testing for potency and sterility. Vials must include clear labeling with concentration, lot number, and beyond-use date. Pricing should be transparent with no hidden fees for consultations, shipping, or dose adjustments.
Red flags that should end your consideration immediately include pricing below $150 per month (the math does not work for legitimate operations), no medical consultation requirement, shipping without temperature control, and guaranteed weight loss claims.
Pathway 5: patient assistance programs (free or reduced cost)
Several programs exist specifically to help patients who cannot afford tirzepatide at any of the price points above.
Lilly Cares patient assistance program
Eli Lilly operates the Lilly Cares Foundation, which provides free medications to eligible patients. The program targets low-income, uninsured, or underinsured individuals who meet specific financial criteria. As of this writing, coverage for Mounjaro and Zepbound specifically is limited, but the program evolves and medications are added over time. Check the current covered medication list directly with Lilly Cares.
To qualify, you typically need to demonstrate household income below a certain threshold of the federal poverty level, lack of adequate prescription drug coverage, United States residency, and an active prescription from a licensed provider.
Patient Advocate Foundation co-pay relief
The Patient Advocate Foundation operates a Co-Pay Relief program that provides direct financial assistance to cover copays, coinsurance, and deductibles for eligible patients. To qualify for tirzepatide assistance, you must be currently insured with coverage for the medication, have a confirmed diagnosis and treatment plan, reside and receive treatment in the United States, and have household income at or below 300-400% of the federal poverty guideline.
This program bridges the gap for patients whose insurance covers tirzepatide but whose copay is still unaffordable even with the manufacturer savings card.
State pharmaceutical assistance programs
Several states operate their own pharmaceutical assistance programs that may cover GLP-1 medications. Eligibility varies by state and typically depends on income, age, and insurance status. Check with your state health department for available programs. These programs are often underutilized because patients do not know they exist.
Clinical trial participation
Eli Lilly and other pharmaceutical companies continue running clinical trials involving tirzepatide and next-generation medications. Trial participants receive the study medication at no cost, along with medical monitoring and follow-up care. ClinicalTrials.gov lists active recruiting studies. This pathway is not a long-term affordability solution, but it can provide free access to tirzepatide for the duration of the trial while contributing to medical research.
Pathway 6: insurance appeal and prior authorization strategies
If your insurance initially denies coverage for tirzepatide, that is not necessarily the final answer. Insurance appeals succeed more often than most patients realize, especially for medications with strong clinical evidence.
Why insurers deny tirzepatide coverage
Most denials fall into three categories. The medication is not on the plan formulary (the insurer has not added it to their approved drug list). The plan excludes weight loss medications as a category. Or the prior authorization requirements were not met because documentation was incomplete.
Each of these barriers has a strategy to overcome it.
Building a successful appeal
For formulary exclusions, your provider can submit a formulary exception request demonstrating medical necessity. This requires documentation of your BMI history, weight-related comorbidities (type 2 diabetes, hypertension, obstructive sleep apnea, cardiovascular disease, joint disease), previous weight loss attempts and their outcomes, and a letter of medical necessity explaining why tirzepatide specifically is needed.
For category exclusions of weight loss medications, the approach shifts to framing the prescription around a covered diagnosis. If you have type 2 diabetes, Mounjaro is prescribed for diabetes management, not weight loss, and is more likely to be covered. If you have obstructive sleep apnea, Zepbound carries an FDA-approved indication for that condition specifically, which may bypass the weight loss exclusion.
For prior authorization failures, simply resubmitting with complete documentation often resolves the issue. Common missing elements include a current BMI measurement, documentation of supervised weight loss attempts, lab work confirming related conditions, and the specific prior authorization form your insurer requires.
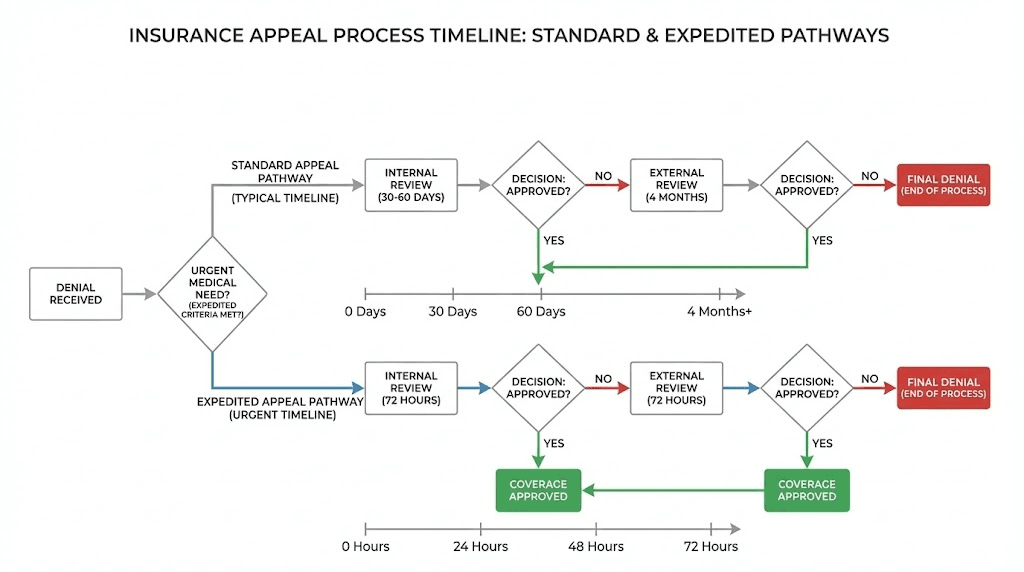
The appeal timeline
Standard appeals typically take 30-60 days for a decision. Expedited appeals, available when delay poses a health risk, must be decided within 72 hours. External review by an independent third party is available if internal appeals fail. Many states require insurers to cover the cost of the medication during the appeal process, preventing gaps in treatment.
A single successful appeal transforms your tirzepatide cost from $449-$1,069 per month to potentially $25 per month with the savings card. The time investment in a thorough appeal is one of the highest-return financial decisions you can make.
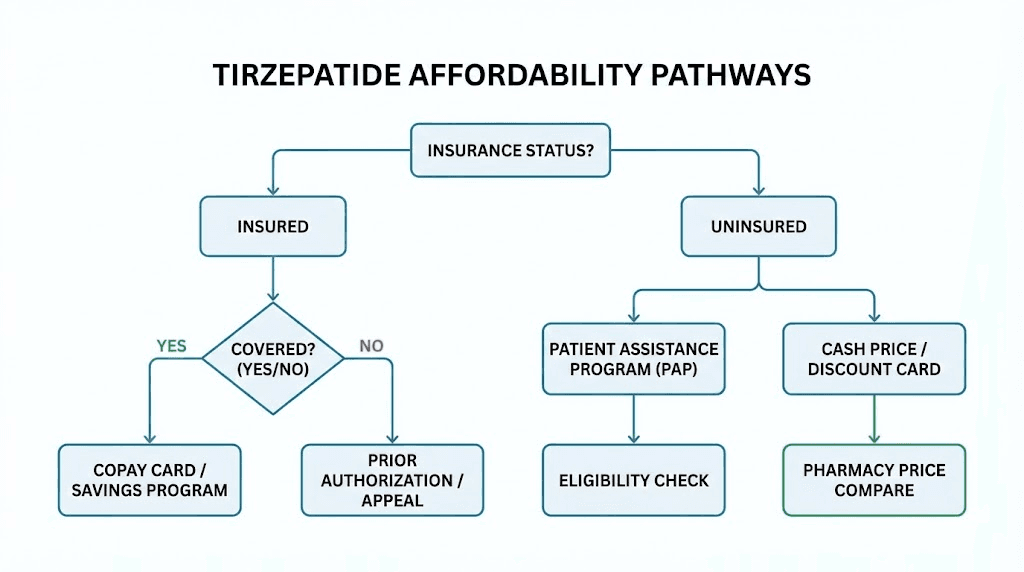
How to pick the right pathway for your situation
With six distinct pathways, the decision tree depends on your specific circumstances. Here is a direct guide based on your starting point.
If you have commercial insurance
Start by calling your insurer to check formulary coverage for both Zepbound and Mounjaro. If either is covered, activate the savings card for $25 per month. If neither is covered, file an appeal or formulary exception request. While the appeal processes, consider LillyDirect at $299-$449 per month as a bridge. If the appeal succeeds, transition to the $25 per month savings card pathway.
If you have Medicare
Contact your Part D plan to ask about GLP-1 coverage participation starting this year. If they are participating, work with your provider to have a prescription ready when coverage launches. Your cost will be $50 per month maximum. If they are not participating, consider switching plans during the next enrollment period or explore LillyDirect as a self-pay option in the interim.
If you have Medicaid
Coverage varies dramatically by state. Thirteen state Medicaid programs currently cover GLP-1 medications for obesity treatment under fee-for-service as of early this year. The BALANCE model, a five-year CMS Innovation Center initiative, aims to expand Medicaid access to obesity drugs starting in May. Contact your state Medicaid office to check current coverage. If tirzepatide is not covered, ask about coverage for the obstructive sleep apnea indication specifically, which may have different formulary rules.
If you are uninsured
LillyDirect is your primary pathway at $299-$449 per month. Check eligibility for the Lilly Cares patient assistance program if your income qualifies. Explore compounded tirzepatide if you have a documented medical need that qualifies under current FDA regulations. Consider whether semaglutide, which remains on the FDA shortage list and is more readily available through compounding, might be a more accessible alternative.
If you are currently on compounded tirzepatide
Verify your provider regulatory compliance status. Compare your current monthly cost against LillyDirect pricing, because the gap may be smaller than you think. If your provider cannot demonstrate a clear legal basis for continued compounding, develop a transition plan to avoid treatment interruption. Have a LillyDirect account ready as a backup. Consider whether your compounded dose could be maintained at a lower level to reduce cost during a transition period. Our guide on microdosing tirzepatide discusses maintenance dosing strategies.
The dosing protocol that affects your total cost
Your tirzepatide dose directly impacts your monthly expense. Understanding the standard dosing schedule helps you budget accurately and avoid unnecessary dose escalation that increases cost without proportional benefit.
Standard escalation and cost implications
Treatment begins at 2.5mg once weekly for four weeks. This is the acclimation phase where your body adjusts to the medication. Side effects are typically mildest at this dose. Cost is lowest at this dose.
After four weeks, the dose increases to 5mg weekly for at least four more weeks. This is where therapeutic effects begin. Most patients start noticing meaningful appetite suppression and early weight loss. The SURMOUNT trials showed 16% body weight reduction even at this moderate dose.
Subsequent escalation proceeds through 7.5mg, 10mg, 12.5mg, and finally 15mg, each step lasting at least four weeks. Not every patient needs the maximum dose. Many achieve their goals at 7.5mg or 10mg. Since LillyDirect prices jump from $299 (2.5mg) to $399 (5mg) to $449 (7.5mg+), finding your optimal dose at the lowest effective level saves real money.
Why dose optimization saves money
Here is a scenario most affordability guides ignore. Patient A escalates to 15mg because that is what the protocol allows. Patient B works with their provider to find that 10mg produces satisfactory results. Both use LillyDirect.
Patient A pays $449 per month from month three onward. Patient B pays $449 per month from month three onward too, because LillyDirect prices are the same for 7.5mg and above. In this case, there is no monthly cost difference at LillyDirect. But Patient B experiences fewer side effects, which means better adherence, fewer treatment interruptions, and potentially a shorter total treatment duration.
With compounded tirzepatide, the cost difference is more direct. Compounding pharmacies often price by vial size, meaning a 10mg monthly supply costs less than a 15mg supply. The savings range from $50-$100 per month, or $600-$1,200 per year.
The broader point is that more medication is not always better. The right dose is the lowest dose that produces clinically meaningful results with tolerable side effects. Finding it requires working with your provider, tracking your response, and resisting the temptation to escalate prematurely.
Cost per pound lost analysis
A useful way to evaluate tirzepatide affordability is cost per pound of weight lost. This accounts for both the medication expense and the actual outcomes achieved.
Access pathway | Annual cost | Expected weight loss (200lb person) | Cost per pound lost |
|---|---|---|---|
Insurance + savings card | $300 | 32-45 lbs | $7-$9 |
Medicare | $600 | 32-45 lbs | $13-$19 |
Compounded (budget) | $2,400 | 32-45 lbs | $53-$75 |
LillyDirect | $4,800 | 32-45 lbs | $107-$150 |
Retail (no programs) | $12,828 | 32-45 lbs | $285-$401 |
At the insurance + savings card pathway, tirzepatide costs roughly $7-9 per pound of weight lost. Compare that to the cost of managing obesity-related conditions like type 2 diabetes ($9,601 average additional annual healthcare cost), cardiovascular disease ($18,953 average annual cost), or joint replacement surgery ($30,000-$50,000 one-time). The medication essentially pays for itself in avoided healthcare expenses at almost every price point except full retail.
Making tirzepatide work while spending less overall
The total cost of tirzepatide treatment is not just the medication price. It includes the duration of treatment, which is influenced by how effectively you support the medication with lifestyle factors. Faster results mean fewer months on medication and lower total spend.
The protein priority
Tirzepatide suppresses appetite aggressively. That is the mechanism. But reduced eating often means reduced protein intake, which means muscle loss alongside fat loss. Losing muscle drops your metabolic rate, making weight regain more likely when you eventually stop the medication, which could mean restarting treatment and paying for another round.
Target 0.7-1.0 grams of protein per pound of your goal body weight daily. This is harder than it sounds when your appetite is suppressed. Protein shakes, Greek yogurt, cottage cheese, lean meats, and egg whites become essential tools. Our tirzepatide nutrition guide covers optimal food choices in detail, and the tirzepatide diet plan provides structured meal frameworks.
Resistance training is not optional
Strength training three to four times per week is the primary defense against muscle loss during rapid weight loss. Compound movements like squats, deadlifts, bench press, and rows preserve lean mass and metabolic rate. You do not need a complicated program. You need consistency. You need progressive overload. And you need to show up even on days when the appetite suppression makes eating, and therefore recovering, more difficult.
Hydration as a medical necessity
GLP-1 medications slow gastric emptying and can cause nausea, vomiting, and diarrhea. All of these deplete fluids. Dehydration on tirzepatide is not just uncomfortable, it is medically dangerous. Acute kidney injury secondary to dehydration is a documented serious adverse event. Drink 80-100 ounces of water daily minimum. Supplement electrolytes. Treat this as a non-negotiable part of your protocol, not a wellness suggestion.
Side effect management saves money
Poorly managed side effects lead to treatment interruption. Treatment interruption leads to weight regain. Weight regain leads to restarting from a higher dose. That cycle is expensive.
Common side effects like nausea respond to simple strategies. Eat smaller meals. Avoid high-fat foods, especially in the first 48 hours after injection. Stay hydrated. Take the injection in the evening so the peak effect coincides with sleep. If nausea persists, discuss anti-nausea medication with your provider before escalating your dose. Escalation before side effects resolve just compounds the problem.
For a comprehensive overview of what to expect, see our guides on tirzepatide fatigue, tirzepatide and anxiety, and dosage optimization strategies.
Comparing tirzepatide to other affordable weight loss options
Tirzepatide is the most effective weight loss medication available, but it is not the only option. If the cost remains prohibitive even after exploring all pathways above, understanding the alternatives helps you make an informed decision.
Semaglutide (Wegovy/Ozempic)
Semaglutide versus tirzepatide is the most common comparison in the GLP-1 weight loss space. Semaglutide is a single GLP-1 receptor agonist, while tirzepatide is a dual GIP/GLP-1 agonist. The clinical data shows tirzepatide produces greater weight loss at comparable treatment durations: 22.5% on tirzepatide versus approximately 15-17% on semaglutide.
However, semaglutide has two significant advantages from an affordability standpoint. First, compounded semaglutide remains more accessible because semaglutide is still on the FDA drug shortage list as of this writing, which means compounding pharmacies can produce it under enforcement discretion. Second, brand-name semaglutide (Wegovy) has been on the market longer, meaning more insurance formularies include it.
If tirzepatide is unaffordable but semaglutide is accessible, the weight loss results are still clinically significant. Getting 15% body weight reduction on an affordable medication is better than getting 0% reduction because the more effective medication is out of reach. Our tirzepatide versus semaglutide dosage comparison breaks down how the two protocols differ.
Oral GLP-1 options
Oral tirzepatide is currently in clinical trials and may eventually provide a non-injectable option. Oral semaglutide is already available in certain formulations. For patients who are needle-averse, oral options may improve adherence and reduce the total treatment cost by eliminating injection-related barriers. Oral versus injectable tirzepatide considerations will become increasingly relevant as these options mature.
Next-generation medications
Retatrutide, a triple GIP/GLP-1/glucagon receptor agonist, showed up to 24.2% body weight reduction in phase 2 trials. It is not yet FDA-approved, but its emergence will increase competitive pressure on tirzepatide pricing. CagriSema, combining cagrilintide with semaglutide, represents another promising dual-mechanism approach. More competition in this space means lower prices for patients across all options.
The broader GLP-1 landscape
The weight loss medication market is expanding rapidly. GLP-1 patches are in development. Tirzepatide sublingual drops offer alternative delivery methods. Every new entrant increases pricing pressure on existing options. The trajectory is clearly toward greater affordability, even if the pace feels slow when you are the one writing the check every month.
Common mistakes that make tirzepatide more expensive than it needs to be
These errors are surprisingly widespread and collectively cost patients thousands of dollars per year.
Not checking insurance coverage at all
An astonishing number of patients assume their insurance does not cover tirzepatide without actually checking. Insurance formularies change frequently. Your employer may have added GLP-1 coverage in the latest benefits cycle. A 15-minute phone call to your insurer or a quick check on your pharmacy benefit portal is the highest-return time investment you can make. If coverage exists and you activate the savings card, you drop from whatever you are currently paying to $25 per month.
Skipping the savings card
The Zepbound and Mounjaro savings cards are free. They take minutes to activate. And yet patients with commercial insurance coverage still pay full copay amounts because they did not know these programs existed. If you have commercial insurance that covers either medication, the savings card is non-negotiable. Activate it before your first fill.
Escalating dose without evaluating response
Your provider should adjust your dose based on your individual response, not simply follow a rigid escalation schedule. If you are losing weight steadily on 5mg, there may be no clinical reason to jump to 7.5mg or 10mg. Higher doses cost more in compounded formulations, cause more side effects, and do not always produce proportionally better results for every patient. The right dose in units is the lowest effective dose for your body.
Neglecting nutrition and exercise
Tirzepatide is not a substitute for basic health behaviors. It is an amplifier. Patients who combine tirzepatide with adequate protein intake, resistance training, and hydration achieve faster results, reach their goals in fewer months, and spend less on medication overall. Patients who rely solely on appetite suppression without supporting their protocol often need longer treatment durations and higher doses, both of which increase cost.
Stopping treatment too early
The SURMOUNT-4 trial showed that patients who stopped tirzepatide after 36 weeks regained roughly half their lost weight. The cheapest-sounding strategy of using tirzepatide briefly and hoping results stick does not work for most people. Budget for at least 12-18 months of treatment, and potentially longer-term maintenance dosing at a reduced dose. Planning for the real duration avoids the expensive cycle of starting, stopping, regaining, and restarting.
Choosing a provider based only on price
The cheapest compounded provider might save you $50 per month. But if their product is underdosed, improperly stored, or inconsistently compounded, your results suffer. Reduced results mean longer treatment. Longer treatment means higher total cost. Sometimes spending slightly more per month on a verified, high-quality option actually reduces your total treatment expenditure by producing faster outcomes.
Long-term affordability planning
Tirzepatide is not a short-term medication for most patients. Understanding the long-term cost trajectory helps you plan realistically.
The maintenance dose question
After reaching your weight loss goal, you face a decision. Continue tirzepatide at a maintenance dose to prevent regain, or discontinue and rely on lifestyle changes alone. The clinical data strongly suggests maintenance treatment produces better long-term outcomes. But maintenance does not necessarily mean the same dose you used during active weight loss.
Some providers are exploring lower maintenance doses, 2.5mg or 5mg weekly, for patients who have reached their goal weight. These doses are less expensive and produce fewer side effects while potentially providing enough GLP-1/GIP receptor activation to prevent the metabolic adaptations that drive weight regain. The duration of GLP-1 treatment is an evolving area of research with significant cost implications.
The improving affordability trajectory
Every trend in the tirzepatide market points toward lower prices over time. Eli Lilly is cutting prices proactively to compete with compounders and expand their market. Medicare coverage is launching. More commercial insurers are adding GLP-1 medications to their formularies as the cost-effectiveness data becomes undeniable. New competitors like retatrutide and CagriSema will increase pricing pressure. Generic tirzepatide will eventually become available when patent protection expires.
If you start tirzepatide today at $449 per month, there is a reasonable probability that your cost will decrease over the next 12-24 months without you doing anything differently. The market dynamics are working in the patient favor for the first time.
Health savings accounts and flexible spending accounts
If you have access to an HSA or FSA through your employer, tirzepatide is an eligible expense. These accounts use pre-tax dollars, effectively reducing your medication cost by your marginal tax rate. For someone in the 24% federal bracket plus state taxes, using HSA/FSA dollars saves roughly 30% on the after-tax cost of medication. On a $449 per month LillyDirect prescription, that is over $130 per month in tax savings, bringing the effective cost to approximately $315.
Maximum HSA contributions for individuals are $4,300 in the current year. For families, the limit is $8,550. If your annual tirzepatide cost fits within these limits, you effectively get a 25-35% discount through tax advantages.
Practical tools that help you save
Several resources can help you navigate the affordability landscape more effectively.
The SeekPeptides cost calculator lets you compare total treatment costs across different access pathways based on your specific dose, duration, and provider. Plug in your numbers and see exactly what each option costs over 6, 12, and 18 months.
The peptide dosage calculator helps verify exact dosing volumes if you are using vials from LillyDirect or a compounding pharmacy. Correct dosing means no wasted medication, which directly impacts your cost per month.
The reconstitution calculator ensures proper preparation if your tirzepatide requires mixing. Improper reconstitution can ruin a vial, wasting an entire month supply.
For researchers navigating the tirzepatide dosing protocol, accurate calculations prevent both underdosing (which reduces effectiveness and extends treatment) and overdosing (which increases side effects and may require dose reduction).
What the future holds for tirzepatide pricing
The tirzepatide affordability landscape will look meaningfully different 12 months from now. Several developments are already in motion.
Medicare coverage expansion will bring millions of new patients into the affordable access pool. As more beneficiaries use the medication and outcomes data accumulates, pressure for permanent coverage inclusion will grow. The CMS pilot program is widely expected to demonstrate cost-effectiveness that justifies ongoing coverage.
Eli Lilly continues aggressive pricing strategies through LillyDirect. Each price reduction they announce puts pressure on remaining compounded providers and signals that the manufacturer intends to own the affordable tirzepatide space rather than cede it to compounders.
New weight loss medications entering the market will create competitive dynamics that benefit patients. When retatrutide reaches FDA approval, Eli Lilly (which also manufactures retatrutide) will need to differentiate its pricing between products. Other manufacturers are developing competing GLP-1 and multi-agonist medications. Competition drives prices down.
State-level legislative action is also accelerating. Multiple states have introduced bills requiring commercial insurers to cover FDA-approved weight loss medications. As these bills pass, the percentage of commercially insured patients with access to the $25 per month savings card pathway will increase substantially.
The direction is clear. Tirzepatide will become more affordable over time. The question is how to minimize your cost today while waiting for that future to arrive.
Frequently asked questions
What is the absolute cheapest way to get tirzepatide right now?
If you have commercial insurance that covers Zepbound or Mounjaro, the savings card brings your cost to $25 per fill. That is the cheapest legitimate pathway. For uninsured patients, LillyDirect starts at $299 per month for the 2.5mg starting dose. For a detailed pricing breakdown of compounded options, see our compounded tirzepatide pricing guide.
Can I still get compounded tirzepatide?
The FDA ended enforcement discretion for tirzepatide compounding in early 2025 after resolving the shortage. Compounded tirzepatide can still be prescribed when a patient has a documented medical need that FDA-approved formulations cannot meet, such as an allergy to inactive ingredients. The legal landscape has narrowed significantly from the open compounding that existed during the shortage.
Is LillyDirect worth it compared to compounded tirzepatide?
LillyDirect provides FDA-approved Zepbound at $299-$449 per month, which overlaps with mid-range compounded pricing ($250-$400). The advantages of LillyDirect include verified potency and purity, pre-measured single-dose vials, no regulatory uncertainty, and the same formulation used in clinical trials. If your budget accommodates LillyDirect pricing, many patients find the certainty worth the potentially small premium over budget compounded options.
When will Medicare cover tirzepatide?
CMS will launch a program allowing eligible Medicare Part D beneficiaries to access GLP-1 medications at $50 per month maximum, potentially starting as early as April of this year. Broader implementation through participating Part D plans is expected in January of next year. Contact your Part D plan administrator to ask about participation.
What if my insurance denies tirzepatide coverage?
Appeal the denial. Gather BMI documentation, records of weight-related comorbidities, evidence of previous weight loss attempts, and a letter of medical necessity from your provider. Many initial denials are overturned on appeal. If your plan excludes weight loss medications categorically, explore whether a prescription for an alternative indication (type 2 diabetes for Mounjaro, obstructive sleep apnea for Zepbound) might succeed.
How much does tirzepatide cost per year at different pathways?
Annual costs range from $300 (insurance + savings card) to $12,828 (full retail). LillyDirect runs $3,588-$5,388 depending on dose. Compounded options range from $1,992-$4,788. Medicare coverage will cost approximately $600 per year. Use our cost calculator to see exact numbers for your specific situation.
Should I wait for prices to drop further before starting?
Prices will likely continue decreasing, but the health costs of delayed treatment are real. Every month carrying excess weight increases cardiovascular risk, joint stress, metabolic dysfunction, and healthcare expenses. Starting at current prices and transitioning to cheaper options as they become available is typically more cost-effective than waiting, especially if your weight-related health conditions are actively worsening.
Can I use an HSA or FSA for tirzepatide?
Yes. Tirzepatide prescribed by a licensed provider is an eligible HSA and FSA expense. Using pre-tax dollars effectively reduces your medication cost by 25-35% depending on your tax bracket. If you have access to these accounts through your employer, this is one of the simplest ways to reduce your effective tirzepatide cost.
External resources
SURMOUNT-1 Clinical Trial Results (New England Journal of Medicine)
Centers for Medicare and Medicaid Services (CMS) Coverage Updates
For researchers serious about optimizing both their protocols and their budgets, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, cost analysis tools, and a community of thousands who have navigated these exact affordability decisions.
May your tirzepatide stay affordable, your protocols stay optimized, and your results stay permanent.