Feb 13, 2026

Your doctor prescribed phentermine. It worked. Five pounds came off in the first two weeks and the appetite suppression felt like a superpower. Then you heard about semaglutide and the 15% body weight reductions people were reporting. Now you are wondering if combining them could accelerate everything, double the appetite suppression, attack fat from two different angles, and finally reach the number on the scale you have been chasing for years.
It is not a crazy question. Phentermine targets weight loss through the central nervous system by flooding the hypothalamus with norepinephrine. Semaglutide takes a completely different route, mimicking the GLP-1 hormone to slow gastric emptying, regulate insulin, and rewire appetite signaling in the brain. Two separate mechanisms. Two separate pathways. On paper, the combination sounds logical.
But the reality is more complicated than the theory. No large-scale clinical trials have studied phentermine and semaglutide used simultaneously. The FDA has not approved the combination. And the potential side effects of stacking a sympathomimetic stimulant with a GLP-1 receptor agonist raise legitimate cardiovascular and gastrointestinal concerns that every person considering this approach needs to understand before making a decision. This guide covers the mechanisms behind both drugs, what limited evidence exists about combination therapy, the real risks involved, and how to have an informed conversation with your healthcare provider about whether this strategy makes sense for your specific situation.
How phentermine works for weight loss
Before you can understand whether combining these two medications makes sense, you need to understand how each one works independently. They are fundamentally different drugs that happen to share a common goal.
Phentermine is old. It was approved by the FDA in 1959, making it one of the longest-standing prescription weight loss medications in American medicine. It belongs to a class of drugs called sympathomimetic amines, and it is classified as a Schedule IV controlled substance because of its structural similarity to amphetamines.
The mechanism is straightforward.
Phentermine enters your brain and triggers the release of norepinephrine from presynaptic vesicles in the lateral hypothalamus. This is the region of the brain responsible for hunger signaling and energy balance. When norepinephrine floods this area, your brain receives a strong signal that you are not hungry. The drug also shows weaker effects on dopamine release and minimal effects on serotonin, which is why it produces appetite suppression without the serotonergic side effects that plagued earlier weight loss drugs like fenfluramine.
There is more to it than just appetite suppression, though. Phentermine also increases resting energy expenditure and inhibits neuropeptide Y, one of the most powerful hunger-stimulating signals in the human body. The combined effect creates a state where your body simultaneously feels less hungry and burns slightly more calories at rest. Think of it as putting your body into a mild fight-or-flight mode where eating drops lower on the priority list.
The standard dosage ranges from 15 mg to 37.5 mg taken once daily, typically about two hours after breakfast. Most doctors prescribe it for short-term use only, generally 12 weeks or less, because of concerns about tolerance development and its stimulant properties. Clinical studies show an average weight loss of approximately 3.6 kg more than placebo over 2 to 24 weeks, with the best results typically appearing in the first few months of use.
The side effects reflect its stimulant nature. Increased heart rate. Elevated blood pressure. Dry mouth. Insomnia. Restlessness and anxiety. These are the predictable consequences of a drug that increases sympathetic nervous system activity throughout your body. For most healthy adults under medical supervision, these effects are manageable and temporary. For people with existing cardiovascular conditions, hypertension, or anxiety disorders, phentermine can be genuinely dangerous.
Why phentermine stops working over time
One of the biggest frustrations with phentermine is tolerance. Your body adapts to the increased norepinephrine levels. The appetite suppression that felt incredible in week one becomes barely noticeable by week eight. This is not a failure of willpower. It is basic neuropharmacology. Your brain downregulates norepinephrine receptors in response to chronic stimulation, requiring higher doses to achieve the same effect.
This tolerance issue is precisely why many people start looking for something to add to their regimen. If phentermine alone stops producing results after a few months, what happens when you combine it with something that works through an entirely different mechanism?
How semaglutide works for weight loss
Semaglutide represents a fundamentally different approach to weight management. While phentermine brute-forces appetite suppression through sympathetic nervous system stimulation, semaglutide works by mimicking a hormone your body already produces.
GLP-1, or glucagon-like peptide-1, is released by L-cells in your small intestine after you eat. It performs several functions simultaneously. It signals your brain that food has arrived. It tells your pancreas to release insulin. It slows down gastric emptying so food stays in your stomach longer. And it communicates with reward centers in your brain to reduce the hedonic drive to eat.
Semaglutide is a synthetic version of GLP-1 that has been modified to last much longer than the natural hormone. Where natural GLP-1 is broken down within minutes, semaglutide persists for approximately one week. This extended duration allows for once-weekly dosing and provides continuous appetite regulation rather than the peaks and valleys you get with shorter-acting medications.
The weight loss results are substantially more impressive than phentermine.
In the STEP clinical trial program, participants taking semaglutide 2.4 mg weekly lost an average of approximately 15% of their body weight over 68 weeks. Some participants lost more than 20%. These numbers are unprecedented for a non-surgical weight loss intervention and represent roughly three to four times the average weight loss seen with phentermine alone.
Semaglutide achieves this through multiple overlapping mechanisms. In the hypothalamus, it activates anorexigenic POMC/CART neurons while suppressing orexigenic NPY/AgRP neurons. Translation: it simultaneously turns up the fullness signals and turns down the hunger signals. In the brainstem, it enhances satiety signals from the vagus nerve. In the stomach, it slows gastric emptying by 10-20%, which makes you feel physically fuller for longer after eating. And recent research shows it also modulates dopamine reward signaling, making food less psychologically rewarding.
The side effect profile is dominated by gastrointestinal symptoms. Nausea is the most common complaint, affecting roughly 40-45% of users at some point during treatment. Vomiting, diarrhea, and constipation are also frequent. These side effects typically peak during dose escalation and improve as your body adjusts. The standard dosing protocol starts at 0.25 mg weekly and increases gradually over 16-20 weeks to the maintenance dose of 2.4 mg weekly, specifically to minimize these gastrointestinal effects.
The theoretical case for combining phentermine and semaglutide
When you look at these two drugs side by side, the argument for combination therapy writes itself. They attack appetite and weight through completely different biochemical pathways. Phentermine increases norepinephrine in the sympathetic nervous system. Semaglutide mimics GLP-1 in the incretin system. There is essentially zero pharmacological overlap between the two mechanisms.
This concept is called complementary mechanism combination therapy, and it is not unique to weight management. Oncology uses it routinely, combining chemotherapy agents that target different phases of cell division. Cardiology does it with blood pressure medications, stacking an ACE inhibitor with a calcium channel blocker because they lower blood pressure through independent pathways.
In the context of weight loss, the theoretical benefits look like this:
Phentermine provides: rapid appetite suppression through norepinephrine release, increased resting energy expenditure, fast-acting effects within hours of the first dose, and strong short-term motivation from quick initial weight loss.
Semaglutide provides: sustained appetite regulation through GLP-1 receptor activation, delayed gastric emptying for prolonged satiety, modulation of food reward pathways in the brain, improved glycemic control and insulin sensitivity, and long-term weight maintenance potential.
Together, a person would theoretically experience appetite suppression from two independent systems, potentially achieving greater calorie reduction than either drug alone. The phentermine could provide the immediate, noticeable suppression that helps build momentum, while the semaglutide provides the deep, sustained regulation that drives long-term results.
Some clinicians have already started prescribing this combination off-label. A case report published in the Journal of Clinical Endocrinology and Metabolism documented a patient who lost 32.5% of their total body weight using a multi-drug regimen that included both phentermine and semaglutide. That level of weight reduction approaches what is typically only achievable through bariatric surgery.
But a case report is not a clinical trial. And the theoretical logic of combining mechanisms does not automatically translate into safe, effective practice.
What the limited research actually shows
Here is the uncomfortable truth. There are no large randomized controlled trials specifically studying the combination of phentermine and semaglutide. None. The evidence base consists of case reports, clinical observations from off-label prescribing, and extrapolation from related research.
What we do have is a randomized, placebo-controlled pilot study that looked at adding phentermine to liraglutide, another GLP-1 receptor agonist in the same drug class as semaglutide. That study found that adding phentermine to liraglutide did not provide meaningful additional weight loss compared to liraglutide plus placebo. This is an important finding because it challenges the assumption that stacking two appetite-suppressing mechanisms automatically produces additive results.
There is also animal research showing additive effects when liraglutide was combined with phentermine in mice, but animal models do not reliably predict human outcomes in weight management research.
The case reports that do exist are encouraging but limited. Individual patients have shown significant weight loss on combination regimens. But these are selected patients, often with medical supervision and concurrent lifestyle interventions. They do not tell us what would happen in a broader population or over longer time periods.
Network meta-analyses comparing weight loss medications individually show that semaglutide achieves approximately 13.7% average weight loss while phentermine/topiramate achieves approximately 9.1%. But combining individual efficacy numbers does not tell you what happens when you combine the drugs themselves.
Drug interactions between phentermine and semaglutide
This is where people get confused, so let us be precise.
Drugs.com classifies the interaction between phentermine and semaglutide as moderate. Moderate does not mean dangerous. It means there are theoretical concerns that warrant monitoring and physician oversight. There is no absolute pharmacological contraindication prohibiting concurrent use.
The two drugs are metabolized differently and do not compete for the same enzymes or transporters. Semaglutide is broken down through proteolytic degradation, similar to how your body processes other proteins. Phentermine is primarily excreted by the kidneys. They do not interfere with each other at the pharmacokinetic level, meaning one does not change the blood levels or effectiveness of the other.
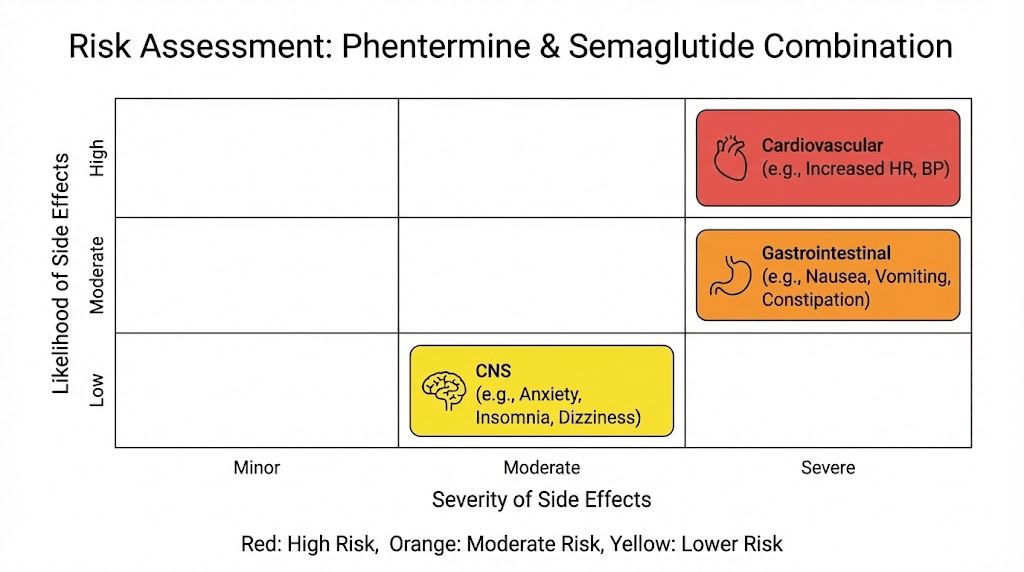
Where the concern lies is in pharmacodynamic interactions, the combined physiological effects of both drugs acting simultaneously on your body. The potential areas of concern include cardiovascular effects, gastrointestinal effects, central nervous system effects, and metabolic effects. We will cover each of these in detail.
Cardiovascular concerns
This is the biggest red flag in the combination.
Phentermine increases heart rate and blood pressure. It is a sympathomimetic stimulant. That is what it does. Average heart rate increases of 3-5 beats per minute and systolic blood pressure increases of 1-3 mmHg are typical and expected.
Semaglutide also increases heart rate, though through a different mechanism. GLP-1 receptor activation in the sinoatrial node produces a mild chronotropic effect. Average heart rate increases of 1-4 beats per minute have been observed in clinical trials.
Individually, these increases are clinically insignificant for most healthy adults. Combined, they could become meaningful, particularly for anyone with underlying cardiovascular conditions, borderline hypertension, or a history of arrhythmias. An additive heart rate increase of 5-9 beats per minute, while still modest, shifts the risk calculation.
It is worth noting that the SUSTAIN-6 and PIONEER-6 trials demonstrated cardiovascular safety for semaglutide, and the SELECT trial actually showed cardiovascular benefit in people with established heart disease. Phentermine data is less reassuring on this front, largely because long-term cardiovascular studies have not been conducted for phentermine as a monotherapy.
Gastrointestinal overlap
Semaglutide slows gastric emptying significantly. That is one of its primary mechanisms for weight loss. Phentermine can also affect gastrointestinal motility through sympathetic nervous system activation, though this is not its primary mechanism.
When you combine both drugs, the gastrointestinal effects can stack. People may experience more severe nausea, more pronounced appetite suppression leading to inadequate caloric intake, increased risk of constipation from reduced gut motility, and potential for nutritional deficiencies if food intake drops too dramatically.
The excessive appetite suppression concern is real and underappreciated. When two drugs simultaneously suppress your desire and ability to eat, some people end up consuming dangerously low calories, below 800-1000 per day, without realizing it. This can lead to muscle loss, nutritional deficiencies, gallstone formation, and metabolic adaptation that makes future weight management even harder.
Central nervous system effects
Phentermine is a stimulant. It increases alertness, can cause insomnia, and produces anxiety in some users. Semaglutide, while not a stimulant, does cross the blood-brain barrier and affects multiple neurotransmitter systems including dopamine signaling.
Some people combining these medications report increased nervousness, difficulty sleeping, mood changes, and difficulty concentrating. The combination may also lower the seizure threshold in susceptible individuals, though this has not been systematically studied.
Who might be a candidate for combination therapy
Not everyone asking about this combination is in the same situation. The risk-benefit calculation varies enormously depending on individual circumstances, and understanding where you fall on that spectrum matters more than any general answer.
Scenario 1: currently on phentermine, considering adding semaglutide
This is perhaps the most common scenario. You started phentermine, lost some weight, but are now hitting a plateau as tolerance develops. You have heard that semaglutide produces better long-term results and want to either add it or transition to it.
Many obesity medicine specialists in this situation recommend transitioning rather than combining. Start tapering the phentermine while initiating the semaglutide dose escalation. By the time you reach therapeutic semaglutide doses, you have discontinued the phentermine entirely. This approach gives you the benefits of semaglutide without the risks of combination therapy.
If a provider does recommend a temporary overlap period, it would typically be during the semaglutide dose escalation phase when semaglutide is not yet at its full appetite-suppressing dose. The phentermine bridges the gap until semaglutide reaches therapeutic levels, then gets discontinued.
Scenario 2: on semaglutide, not losing enough weight
Some people reach the maximum semaglutide dose and still do not achieve their weight loss goals. This is not uncommon. Approximately 15-20% of people on semaglutide are classified as suboptimal responders, losing less than 5% of body weight.
In this scenario, adding phentermine is one option, but it is not the first-line recommendation. Most guidelines suggest first evaluating adherence to the medication and lifestyle modifications, checking for medical conditions that could impair weight loss such as hypothyroidism or Cushing syndrome, considering switching to tirzepatide which targets both GLP-1 and GIP receptors for potentially greater weight loss, and optimizing diet quality and meal planning to maximize the medication effects.
If those steps do not resolve the plateau, short-term phentermine addition might be discussed as an off-label strategy. But it should be presented as what it is: an experimental approach without robust clinical evidence.
Scenario 3: high BMI requiring aggressive intervention
For individuals with severe obesity, defined as BMI 40 or greater, or BMI 35 or greater with obesity-related comorbidities, the risk-benefit calculation tilts more toward aggressive pharmacotherapy. The health risks of remaining severely obese often outweigh the risks of combination medication therapy.
In these cases, some obesity medicine specialists will prescribe combination regimens that may include phentermine and a GLP-1 agonist, along with careful cardiovascular monitoring. The 32.5% body weight reduction documented in the case report mentioned earlier came from a patient in this clinical category.
But even in this scenario, combination therapy should involve regular monitoring of blood pressure, heart rate, basic metabolic panel, and overall nutritional status. It is not a set-it-and-forget-it approach.
Who should absolutely NOT combine these medications
Certain populations should avoid this combination entirely. People with uncontrolled hypertension face compounded cardiovascular risk from the additive heart rate and blood pressure effects. Anyone with a history of cardiovascular disease, heart failure, or arrhythmias should avoid phentermine entirely, regardless of whether semaglutide is involved.
People with a personal or family history of anxiety disorders or panic attacks may find the stimulant effects of phentermine amplified when combined with semaglutide effects on brain signaling. Those with a history of substance abuse should be cautious with phentermine given its Schedule IV classification and structural similarity to amphetamines.
Pregnant or breastfeeding individuals should not use either medication, individually or combined. Anyone with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use semaglutide. And people with severe gastrointestinal conditions like gastroparesis may find the combination intolerable due to stacked effects on gut motility.
Side effects of combining phentermine and semaglutide
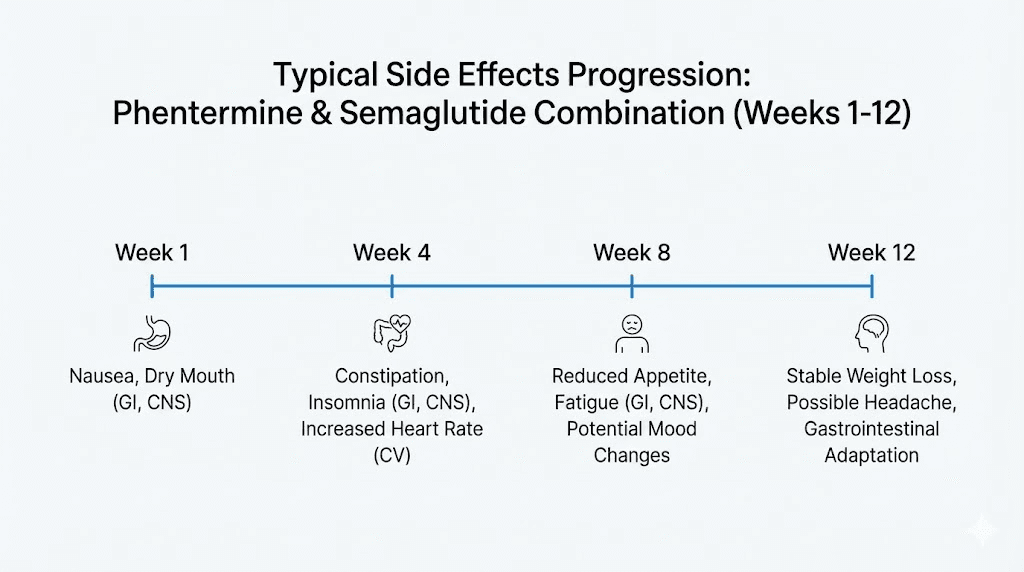
When two medications are used together, side effects do not simply add, they can amplify each other. Understanding the full side effect landscape helps you make an informed decision and know what to watch for if you do proceed with combination therapy under medical supervision.
Gastrointestinal side effects
Nausea is the dominant complaint. Semaglutide alone causes nausea in approximately 40-45% of users during dose escalation. Adding phentermine, which can cause its own gastrointestinal discomfort through sympathetic activation, increases both the likelihood and severity of nausea. Some combination users report nausea severe enough to interfere with daily activities and work.
Constipation affects users from both directions. Semaglutide slows gut motility as part of its mechanism. Phentermine can cause constipation through sympathetic nervous system activation that diverts blood flow away from the digestive tract. Together, constipation can become significant enough to require intervention with fiber supplements, stool softeners, or osmotic laxatives.
Vomiting, diarrhea alternating with constipation, abdominal pain, and bloating are all more likely with the combination than with either drug alone. These are not just comfort issues. Severe vomiting can lead to dehydration and electrolyte imbalances. Chronic diarrhea can cause nutritional malabsorption.
Cardiovascular side effects
The additive effect on heart rate is the most measurable cardiovascular concern. Expect resting heart rate to increase by 5-9 beats per minute on average, with some individuals experiencing larger increases. Heart palpitations may become noticeable, particularly in the hours after taking phentermine when its stimulant effects peak.
Blood pressure increases are usually modest but consistent. If you already have borderline high blood pressure, the combination can push you into the hypertensive range. Regular monitoring is essential, with most physicians recommending blood pressure checks at least every two weeks during the initial combination period.
Neurological and psychological side effects
Insomnia from phentermine is common even when used alone. Combined with semaglutide effects on brain signaling, sleep disruption can become more pronounced. Difficulty falling asleep, staying asleep, or achieving restful sleep can compound over time, leading to fatigue, irritability, and impaired cognitive function.
Some users report heightened anxiety, restlessness, or a feeling of being overstimulated. Mood changes including irritability and depression have been reported with both medications individually, and the combination may increase these risks. Difficulty concentrating and a sense of mental cloudiness are occasionally reported, though these effects are more commonly attributed to inadequate caloric intake than to direct drug effects.
Metabolic and nutritional risks
When appetite is suppressed from two different angles simultaneously, caloric intake can drop below safe levels. This creates several cascading problems.
Muscle loss accelerates when protein intake drops too low, which is common when people are eating less than 1000 calories per day. Losing muscle while losing fat creates a condition sometimes called metabolic starvation where your resting metabolic rate drops faster than your weight, making weight regain almost inevitable once medications are discontinued.
Nutritional deficiencies become likely when food intake is severely restricted. B vitamins, iron, zinc, magnesium, and vitamin D are the most commonly depleted nutrients during aggressive pharmaceutical weight loss. Vitamin B12 deficiency deserves special attention because semaglutide can impair B12 absorption independently, and reduced food intake compounds this effect.
Gallstone formation risk increases with any rapid weight loss, and the combination can produce weight loss rapid enough to significantly elevate this risk. Gallstones form when the liver secretes too much cholesterol relative to bile salts, which happens more frequently when the body is mobilizing fat stores quickly.
Phentermine vs semaglutide: head-to-head comparison
For people trying to decide between these medications rather than combine them, understanding the key differences helps clarify which one might be more appropriate for your situation.
Factor | Phentermine | Semaglutide |
|---|---|---|
Drug class | Sympathomimetic amine (stimulant) | GLP-1 receptor agonist |
FDA approval year | 1959 | 2021 (for weight loss) |
Route | Oral (pill) | Subcutaneous injection (weekly) |
Average weight loss | 5-10% body weight | 15% body weight |
Time to results | Days to weeks | 4-8 weeks to notice, peak at 6-12 months |
Duration of use | Short-term (12 weeks) | Long-term (ongoing) |
Controlled substance | Yes (Schedule IV) | No |
Main mechanism | Norepinephrine release | GLP-1 receptor activation |
Primary side effects | Insomnia, dry mouth, elevated HR/BP | Nausea, vomiting, diarrhea |
Tolerance development | Common (weeks to months) | Uncommon |
Weight regain after stopping | Very common and rapid | Common but more gradual |
Cardiovascular safety data | Limited long-term data | Demonstrated CV benefit (SELECT trial) |
Cost without insurance | $15-75/month (generic) | $900-1300/month (brand) |
The comparison reveals fundamentally different profiles. Phentermine is cheap, fast-acting, and effective for short-term results but limited by tolerance, stimulant side effects, and lack of long-term data. Semaglutide is expensive, slower to produce results, but delivers superior weight loss, has demonstrated cardiovascular benefits, and can be used long-term.
For many people, the question is not really whether to combine them but whether to transition from one to the other. If you have been on phentermine and are hitting a plateau, transitioning to semaglutide rather than adding it on top may be the more evidence-based approach.
What happens when you stop phentermine and continue semaglutide
Many people on the combination end up discontinuing phentermine while maintaining semaglutide. Understanding what to expect during this transition prevents unnecessary anxiety and helps you plan accordingly.
The first thing most people notice is a temporary increase in appetite. Phentermine provides rapid, noticeable appetite suppression. When that layer gets removed, it can feel like your appetite has returned even though semaglutide is still working in the background. This is not semaglutide failing. It is the sudden absence of norepinephrine-mediated suppression creating a relative increase in hunger signals.
This transition period typically lasts 1-3 weeks as your body readjusts. Most people find that their appetite stabilizes once the phentermine is fully out of their system, usually within 5-7 days given its half-life of approximately 20 hours. The semaglutide-mediated appetite suppression, while subtler and more gradual, remains effective.
Some people experience a temporary weight plateau or even a slight weight increase of 1-3 pounds during the transition. This is almost entirely water retention and increased food volume in the gastrointestinal tract as eating normalizes. It is not fat regain. Staying consistent with semaglutide and not panicking during this adjustment period is critical.
Energy levels may shift. If you were relying on phentermine stimulant effects for energy, you might feel more fatigued for a week or two after discontinuation. Semaglutide fatigue is a separate phenomenon that some users experience, and it can be more noticeable once the stimulating effects of phentermine are no longer masking it.
Safe approaches to combination therapy under medical supervision
If after reviewing all the evidence and risks, you and your healthcare provider decide to proceed with combination therapy, certain approaches minimize risk.
The staggered start approach
Rather than starting both medications simultaneously, most physicians who prescribe this combination use a staggered start. Begin one medication first, establish tolerance and baseline side effects, then carefully introduce the second. Most commonly, semaglutide is started first with its standard dose escalation protocol. Phentermine is introduced only if semaglutide alone is not producing adequate results after reaching the therapeutic dose.
This approach lets you distinguish which side effects come from which medication. If you start both at once and develop nausea, you do not know whether semaglutide, phentermine, or their interaction is responsible. That makes management much harder.
The bridge approach
Some clinicians use phentermine as a bridge during semaglutide initiation. Since semaglutide takes 16-20 weeks of dose escalation before reaching its full effect, phentermine provides appetite suppression during those early weeks when semaglutide is not yet fully active. As semaglutide dose increases, phentermine dose decreases, eventually being discontinued entirely once semaglutide reaches therapeutic levels.
This is probably the most conservative and defensible approach to combination use. The overlap period is limited, the phentermine serves a specific purpose (bridging the gap), and the end goal is semaglutide monotherapy.
The intermittent approach
Rather than daily phentermine alongside weekly semaglutide, some providers prescribe phentermine only 2-3 days per week. This intermittent dosing may reduce cardiovascular strain, limit tolerance development, and provide appetite suppression on days when it is most needed, such as weekends or high-social eating situations.
No clinical trials support this specific approach, but it reflects a harm-reduction philosophy. If a patient is going to take both medications regardless, intermittent phentermine dosing is likely safer than daily dosing.
Required monitoring during combination therapy
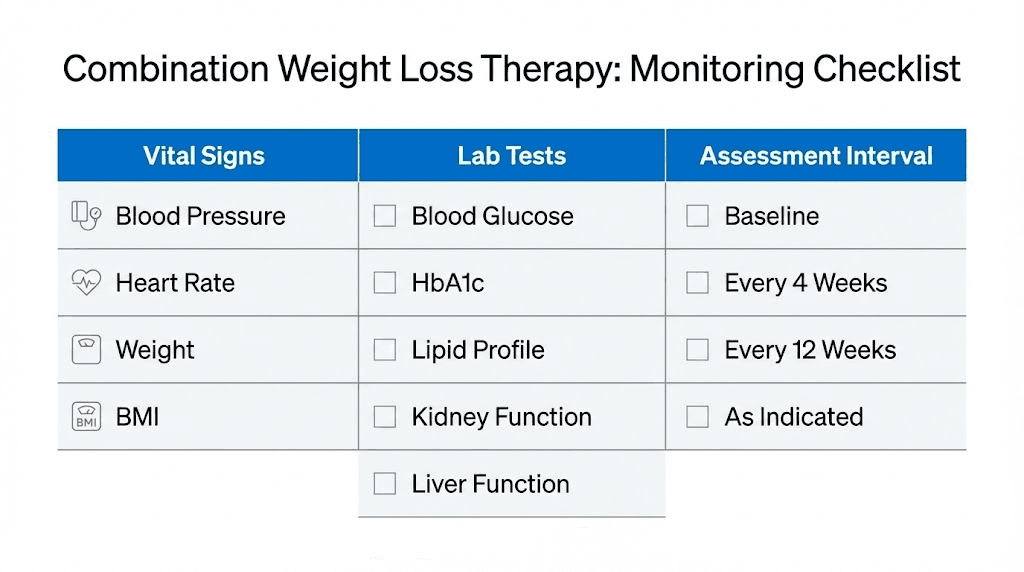
Regardless of which approach is used, combination therapy demands closer medical monitoring than either drug alone. This should include blood pressure and heart rate measurements at every office visit and ideally daily home monitoring, an EKG at baseline and periodically during treatment, regular assessment of caloric intake to prevent dangerously low consumption, basic metabolic panel every 4-8 weeks to check kidney function and electrolytes, complete blood count to screen for nutritional deficiency markers, and regular assessment of mental health status including mood, sleep, and anxiety.
If at any point blood pressure exceeds 140/90, resting heart rate exceeds 100 beats per minute, or severe gastrointestinal symptoms develop, most clinicians would recommend discontinuing the phentermine and maintaining semaglutide alone.
Alternative combinations to consider
If the phentermine-semaglutide combination feels too risky or your provider is not comfortable prescribing it, several alternative approaches may achieve similar goals with better evidence support.
Tirzepatide as monotherapy
Tirzepatide is a dual GIP/GLP-1 receptor agonist that produces even greater weight loss than semaglutide in head-to-head comparisons. The SURMOUNT-1 trial showed average weight loss of approximately 20-22% at the highest dose, which exceeds the theoretical maximum of phentermine plus semaglutide for most people. If you are looking for more aggressive weight loss than semaglutide alone provides, switching to tirzepatide rather than adding phentermine may be a better strategy.
Tirzepatide also appears to have a somewhat different side effect profile than semaglutide, with some patients tolerating it better. The dosing protocol follows a similar escalation pattern to semaglutide, starting at 2.5 mg weekly and increasing to 5, 7.5, 10, 12.5, or 15 mg.
Semaglutide plus metformin
Metformin has been used as an adjunct to GLP-1 agonists for decades in diabetes management, and it has well-established safety data in combination. While metformin alone is a modest weight loss agent, typically producing 2-3% body weight reduction, its combination with semaglutide is supported by extensive clinical experience and does not carry the cardiovascular concerns of adding phentermine.
Semaglutide plus topiramate
Topiramate has independent weight loss properties and is already FDA-approved in combination with phentermine as Qsymia. Some clinicians combine topiramate with semaglutide instead of phentermine, reasoning that topiramate provides appetite suppression through GABAergic mechanisms without the sympathomimetic cardiovascular effects of phentermine. This combination has less evidence than semaglutide monotherapy but avoids the stimulant-related risks.
Semaglutide plus naltrexone/bupropion
Contrave (naltrexone/bupropion) is another FDA-approved weight loss medication that works through different pathways than semaglutide. Bupropion increases norepinephrine and dopamine, while naltrexone blocks opioid receptors involved in food reward. Some obesity medicine specialists combine Contrave with semaglutide for patients who need more aggressive pharmacotherapy. The evidence base for this specific combination is limited but growing.
Lifestyle optimization before adding medications
Before adding any second medication, ensure the first one is working in an optimal environment. Many people on semaglutide underperform because their dietary patterns do not support the medication effects. Adequate protein intake, typically 1.0-1.2 grams per kilogram of body weight, prevents muscle loss and supports satiety. Regular resistance training preserves lean mass during weight loss. Consistent sleep patterns enhance hormonal regulation of appetite. Stress management reduces cortisol-driven eating behaviors.
Optimizing these factors can improve semaglutide response enough to eliminate the perceived need for a second medication.
The FDA and clinical guidelines perspective
It is important to understand where regulatory bodies and professional organizations stand on this combination.
The FDA has not approved the concurrent use of phentermine and semaglutide. Each drug is approved as individual therapy for weight management. Phentermine is approved only for short-term use. Semaglutide (as Wegovy) is approved for chronic weight management. Using them together constitutes off-label prescribing.
Off-label prescribing is legal and common in medicine. Physicians have the right to prescribe medications outside their approved indications when they believe the benefit outweighs the risk for a specific patient. Approximately 20% of all prescriptions in the United States are written off-label.
However, major US obesity treatment guidelines do not specifically recommend the phentermine-semaglutide combination due to insufficient safety and efficacy data. The Obesity Medicine Association and the Endocrine Society acknowledge that combination anti-obesity medication regimens may be appropriate in certain clinical scenarios but stop short of recommending specific drug pairs without adequate trial data.
The American Association of Clinical Endocrinology guidelines are somewhat more progressive, recognizing that patients with severe obesity may benefit from multi-drug approaches and that the absence of evidence is not evidence of harm. But they emphasize the need for careful patient selection and monitoring.
What this means practically: your physician can prescribe this combination if they believe it is appropriate for you, but they should be transparent about the limited evidence, the off-label nature of the approach, and the need for enhanced monitoring.
Practical dosing considerations
For individuals who are prescribed both medications, understanding how they are dosed and timed matters for both efficacy and side effect management.
Timing
Phentermine should be taken in the morning, ideally before 10 AM, to minimize insomnia. Most prescribers recommend taking it about two hours after breakfast. Semaglutide is injected once weekly and can be administered any day of the week at any time, though consistency helps. There is no specific timing interaction between the two that would require taking them at particular intervals relative to each other.
Some clinicians recommend not taking phentermine on the same day as the semaglutide injection to spread out the appetite-suppressing effects more evenly throughout the week. Others prefer to overlap the effects for maximum suppression. There is no evidence favoring either approach.
Dosing when combining
Most providers who prescribe this combination use lower doses of phentermine than would be used in monotherapy. Rather than the standard 37.5 mg, a typical combination dose might be 15 mg or even 8 mg of phentermine, which provides meaningful appetite suppression with less cardiovascular stimulation.
Semaglutide dosing typically follows the standard escalation protocol regardless of whether phentermine is being co-administered. Starting at 0.25 mg weekly and increasing every four weeks through 0.5, 1.0, 1.7, and 2.4 mg.
For people using compounded semaglutide, the dosing principles remain the same, though the specific concentrations and injection volumes will differ based on the compounding pharmacy formulation. Always verify your concentration and use a semaglutide dosage calculator to confirm accurate dosing.
Diet and nutrition during combination therapy
Adequate nutrition becomes even more critical when appetite is suppressed by two mechanisms. Prioritize protein at every meal, aiming for 25-30 grams per sitting. Eat nutrient-dense foods rather than empty calories, since every calorie needs to count when total intake is reduced. Consider a high-quality multivitamin and specific supplementation based on blood work, especially vitamin B12, vitamin D, iron, and magnesium.
Track your caloric intake for at least the first few weeks of combination therapy. If you are consistently eating below 1200 calories per day without intentionally following a very-low-calorie diet under medical supervision, your appetite suppression may be excessive. Report this to your physician.
Hydration is also important. Both medications can contribute to dehydration through different mechanisms, phentermine through increased sweating and metabolic rate, semaglutide through potential nausea and vomiting. Aim for at least 64 ounces of water daily, more if you are experiencing gastrointestinal side effects.
The semaglutide diet plan principles apply to combination therapy as well: high protein, moderate healthy fats, complex carbohydrates, and plenty of fiber to support gut health and regular bowel movements.
Real-world experiences and what people report
While clinical trials are sparse, real-world reports from patients and physicians provide some insight into what combination therapy actually looks like in practice.
The most common positive report is dramatic appetite reduction. People describe barely thinking about food, easily skipping meals without discomfort, and feeling satisfied with much smaller portions. For individuals who have struggled with constant food fixation, this can feel transformative.
Weight loss velocity tends to be faster than with either drug alone, particularly in the first 2-3 months. Some clinicians report their combination patients losing 3-5 pounds per week during the early phase, which is rapid but not unprecedented for pharmaceutical weight loss in people with high starting weights.
The most common negative report is nausea severity. People who tolerated semaglutide reasonably well often find that adding phentermine tips them over into more significant nausea, particularly in the mornings. This usually improves as the body adapts but can be severe enough to prompt discontinuation of the combination in some cases.
Energy and mood reports are mixed. Some people love the stimulant energy from phentermine combined with the steady appetite control of semaglutide. Others find the combination overstimulating, describing a jittery, anxious quality that makes the weight loss feel not worth it.
Weight loss plateaus still happen. Even with both drugs, some people stall after initial success. This usually reflects metabolic adaptation rather than drug failure and may respond to adjustments in caloric intake, exercise, or medication dosing rather than adding yet another drug.
Questions to ask your doctor before starting combination therapy
If you are considering this combination, walking into your appointment prepared with specific questions will lead to a more productive conversation. Here are the questions that matter most.
What is your experience prescribing phentermine and semaglutide together? You want a provider who has managed patients on this combination, not one who is learning on you. Experienced prescribers will have established monitoring protocols and know what warning signs to watch for.
What is the specific rationale for combining rather than switching? Your provider should be able to articulate why combination therapy is better for your specific situation than optimizing semaglutide monotherapy or switching to tirzepatide.
What monitoring schedule will you follow? Blood pressure, heart rate, labs, and clinical assessments should be clearly defined before starting. If your provider says regular monitoring without specifying what and when, press for details.
What are the stopping criteria? At what point would you discontinue one or both medications? Having predefined criteria, such as blood pressure thresholds or heart rate limits, prevents subjective decision-making under pressure.
What is the exit strategy? How long will I take both medications? Is the plan to transition to semaglutide monotherapy eventually? Having a defined timeline and endpoint matters for both safety and insurance coverage.
How will you address nutritional adequacy? Will there be regular assessment of caloric intake, protein consumption, and micronutrient status? Combination therapy demands more nutritional vigilance than monotherapy.
The cost reality
Financial considerations are often the unspoken factor driving combination therapy decisions.
Phentermine is cheap. Generic phentermine costs $15-75 per month depending on the pharmacy and dosage. It is one of the most affordable prescription weight loss medications available.
Brand-name semaglutide (Wegovy) costs $900-1300 per month without insurance. Even with insurance coverage, copays can be substantial. Compounded semaglutide is significantly less expensive, though availability and regulatory status continue to evolve.
Some people start with phentermine because it is accessible and affordable, then add semaglutide later when they can access it. Others use phentermine to bridge the gap while waiting for insurance prior authorization for semaglutide. These are pragmatic decisions driven by healthcare system realities, not ideal clinical strategy.
When factoring in the cost of required monitoring, including more frequent office visits, additional lab work, and potential EKGs, combination therapy is more expensive than monotherapy with either drug. Factor these costs into your decision.
Frequently asked questions
Is it safe to take phentermine and semaglutide at the same time?
There is no absolute contraindication, but the combination has not been studied in clinical trials. A moderate drug interaction exists, primarily related to additive cardiovascular effects. It should only be done under physician supervision with regular monitoring of blood pressure, heart rate, and overall health status. Safety depends heavily on your individual health profile.
How much weight can you lose on phentermine and semaglutide together?
Individual results vary widely. One published case report documented 32.5% total body weight loss on a multi-drug regimen including both medications. Typical results are likely less dramatic but potentially greater than either drug alone. Semaglutide monotherapy produces approximately 15% average weight loss, and the combination may push this higher for some individuals.
Can my primary care doctor prescribe both medications together?
Any licensed physician can prescribe these medications together off-label. However, given the monitoring requirements and limited evidence, many primary care physicians prefer to refer to obesity medicine specialists or endocrinologists for combination therapy management. Ask your doctor directly whether they are comfortable managing both prescriptions.
What should I do if I experience severe nausea on the combination?
Severe nausea may indicate that the combination is producing excessive gastrointestinal effects. Contact your prescribing physician. They may recommend temporarily discontinuing phentermine to determine if semaglutide alone is the cause, reducing the phentermine dose, adjusting the timing of medication administration, or adding anti-nausea medication as a temporary measure.
How long can you safely take phentermine and semaglutide together?
Phentermine is FDA-approved for short-term use only, generally 12 weeks or less. Any longer use is off-label. Semaglutide is approved for chronic use. Most clinicians who prescribe the combination do so for a limited duration, using phentermine as a bridge or boost rather than a permanent addition to the regimen.
Will insurance cover phentermine and semaglutide prescribed together?
Insurance coverage varies dramatically. Many insurers cover semaglutide for weight loss with prior authorization. Phentermine, as a generic medication, is usually covered but may have quantity limits. However, your insurer may flag the combination for review, particularly if they have policies against concurrent appetite suppressant prescriptions. Check with your specific plan before assuming coverage.
Can I take phentermine and compounded semaglutide together?
From a pharmacological standpoint, compounded semaglutide contains the same active ingredient as brand-name Wegovy. The combination considerations are the same. However, ensure your compounded semaglutide comes from a reputable compounding pharmacy and that your physician is aware you are using compounded medication.
Does phentermine help with the semaglutide titration period when doses are still low?
This is one of the more clinically rational uses of the combination. During the 16-20 week semaglutide dose escalation, appetite suppression may be minimal. Phentermine can provide immediate appetite reduction during this period and then be tapered off as semaglutide reaches therapeutic doses. Many providers view this bridge approach as the most defensible combination strategy.
External resources
For researchers serious about optimizing their weight management protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed interaction databases, dosing calculators, and expert guidance that goes far beyond what any single article can cover.
In case I do not see you, good afternoon, good evening, and good night. May your medications stay effective, your side effects stay manageable, and your weight loss goals stay within reach.