Feb 12, 2026

Before you skip your next dose because of that throbbing behind your eyes, read this. Because the headache you are blaming on tirzepatide might not actually be caused by tirzepatide at all. And even if it is, stopping the medication is almost certainly the wrong move.
Headaches are one of the most commonly reported complaints among people starting tirzepatide therapy, yet they barely appear in the prescribing information. Clinical trial data shows headache rates between 4% and 10.71% depending on dose, compared to 7.5% in the placebo group. That gap is smaller than most people expect. But when you are the one dealing with a pounding head three days after your injection, statistics offer little comfort.
Here is what matters. The overwhelming majority of tirzepatide headaches are not caused by the peptide itself. They are caused by what the peptide does to your eating patterns, your hydration habits, and your blood sugar regulation. That distinction changes everything about how you treat them, how long they last, and whether they come back.
This guide breaks down the complete picture. You will learn exactly why headaches happen during tirzepatide dosing, which types of headaches signal a real problem versus a temporary adjustment, the specific protocols that eliminate them for most people within days, and when a headache means you need medical attention. SeekPeptides has compiled the clinical data, real-world reports, and practical management strategies into one comprehensive resource so you never have to guess whether that headache is something to worry about.
What the clinical trials actually show about tirzepatide and headaches
Let us start with the numbers. Because the internet is full of vague claims about tirzepatide headaches, and vague claims do not help you make decisions about your protocol.
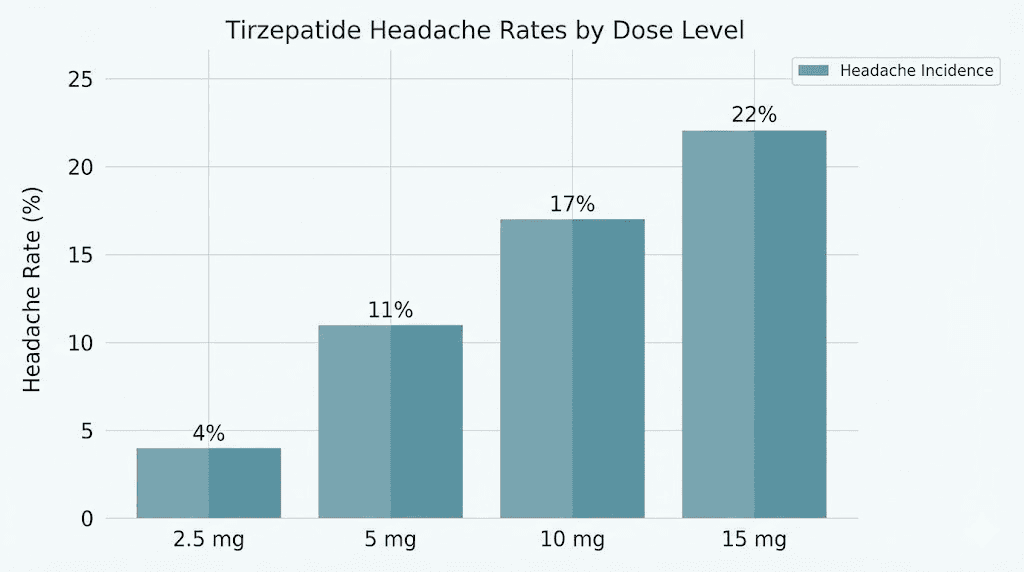
A meta-analysis of ten clinical trials involving 6,836 participants published between 2018 and 2022 found clear dose-dependent headache rates for tirzepatide. At the 5mg dose, 4.00% of participants reported headaches. At 10mg, the rate climbed to 5.16%. And at the 15mg dose, headaches affected 10.71% of participants.
Those numbers tell a clear story. Higher doses produce more headaches.
But context matters enormously here. In the same trials, the placebo group reported headaches at a rate of 7.5%. Read that again. People taking absolutely nothing still reported headaches at 7.5%. This means the difference between tirzepatide and placebo was much smaller than most people assume, especially at lower doses where the tirzepatide group actually had fewer headaches than the sugar pill group.
The SURMOUNT trials, the largest tirzepatide clinical studies to date, confirmed this pattern. A systematic review found the odds ratio for headache was 1.08 with a 95% confidence interval of 0.80 to 1.46. In plain language, there was no statistically significant difference in headache rates between tirzepatide and placebo when accounting for all variables.
So what does this mean for you? It means tirzepatide probably does not cause headaches directly in most people. Instead, the lifestyle changes that accompany tirzepatide therapy, eating less, drinking less water, experiencing blood sugar shifts, those are the actual culprits. And those are things you can control.
How headache rates compare across GLP-1 medications
Tirzepatide is not unique in this regard. Semaglutide produces similar headache rates in clinical trials, and the same underlying mechanisms apply. If you have experienced headaches on semaglutide and are considering switching to tirzepatide specifically to avoid them, the headache profile is comparable between both medications.
Where tirzepatide differs is in its dual mechanism. As both a GLP-1 and GIP receptor agonist, tirzepatide affects appetite suppression more aggressively than GLP-1-only medications in many patients. Stronger appetite suppression means more dramatic changes to eating and hydration patterns, which can increase headache risk indirectly.
The newer triple agonists like retatrutide show similar headache patterns in early trials. The common thread across all these medications is not the peptide itself causing headaches. It is the rapid metabolic changes that follow.
Dose-specific headache data you should know
Here is a breakdown of headache incidence by tirzepatide dose from the meta-analysis:
Dose | Headache rate | 95% confidence interval | Compared to placebo (7.5%) |
|---|---|---|---|
5 mg | 4.00% | 1.92% to 6.80% | Lower than placebo |
10 mg | 5.16% | 1.10% to 11.96% | Comparable to placebo |
15 mg | 10.71% | 4.84% to 18.54% | Higher than placebo |
The pattern is unmistakable. At the starting dose, headaches are actually less common than in people taking nothing. As doses increase, headache rates climb. This dose-response relationship supports the theory that headaches come from the metabolic effects of stronger appetite suppression and greater blood sugar regulation, not from the tirzepatide molecule itself.
Most tirzepatide protocols start at 2.5mg and titrate up every four weeks. This gradual approach gives your body time to adapt, and it is one reason why the real-world headache rate during early treatment tends to be lower than what clinical trials report at higher doses.
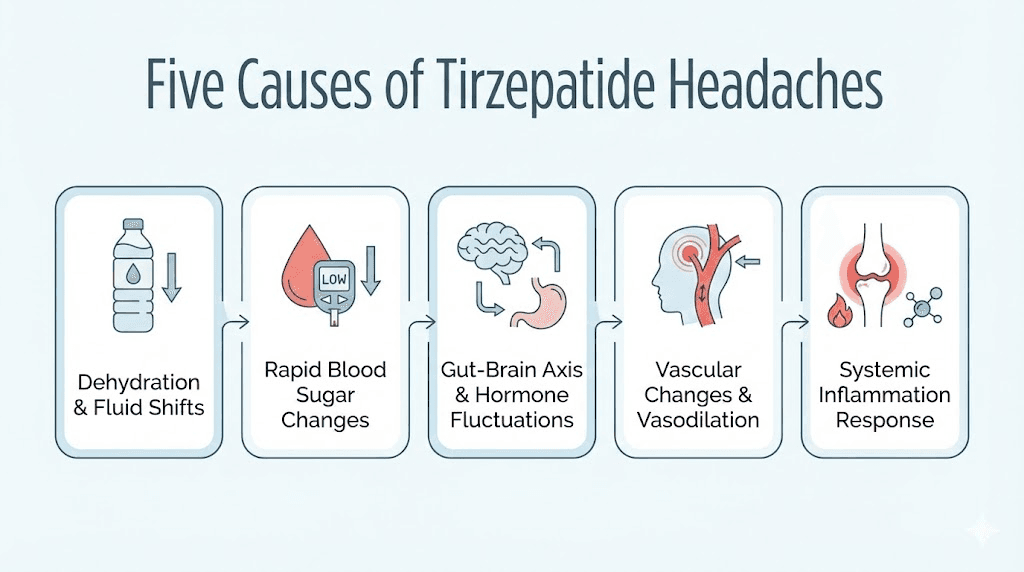
Why tirzepatide causes headaches: the five mechanisms
Understanding why headaches happen is the first step to preventing them. There are five distinct mechanisms that explain virtually every tirzepatide-related headache. Most people experience headaches from the first two causes. Rarely does the medication itself play a direct role.
Mechanism 1: dehydration
This is the number one cause. Not close. Not arguably. Dehydration causes the majority of headaches reported during tirzepatide therapy.
Here is how it happens. Tirzepatide suppresses appetite powerfully, which means you eat less. Many people do not realize that approximately 20% of daily water intake comes from food. Eat less food, get less water. Simple math, brutal consequence.
But it gets worse. Common GI side effects like nausea, vomiting, and diarrhea accelerate fluid loss. When you feel nauseous, the last thing you want to do is drink water. So you eat less (less water from food), you experience GI symptoms (more water lost), and you drink less (because nausea kills your desire to drink). The result is a dehydration triple threat that produces throbbing, persistent headaches.
Dehydration headaches have a specific character. They tend to worsen with movement, concentrate around the forehead or temples, and improve noticeably within 30 to 60 minutes of drinking water. If your headache gets better when you hydrate, you have your answer.
Mechanism 2: blood sugar fluctuations
Tirzepatide works by enhancing insulin secretion and slowing gastric emptying. Both actions lower blood sugar. For most people, this is the desired therapeutic effect. But rapid or excessive blood sugar drops trigger headaches through changes in cerebral blood vessel dilation.
The clinical data shows mild hypoglycemia rates of 17 to 22% across tirzepatide doses in patients with type 2 diabetes. Even in non-diabetic patients using tirzepatide for weight loss, blood sugar fluctuations occur, especially when meals are skipped or significantly reduced due to appetite suppression.
Blood sugar headaches feel different from dehydration headaches. They often come with lightheadedness, irritability, shakiness, or difficulty concentrating. They tend to hit hardest in the morning if you have not eaten enough the day before, or in the late afternoon when blood sugar naturally dips.
The fix is straightforward. Eat consistent, protein-rich meals even when your appetite is reduced. You do not need to eat large volumes of food. But you do need to eat regularly. Our tirzepatide diet plan provides specific meal timing and composition guidance designed to prevent blood sugar crashes.
Mechanism 3: dose escalation response
Headaches cluster around dose increases. This pattern appears clearly in the clinical trial data, where adverse events including headaches were most common during the titration period.
When you increase your tirzepatide dose, your body experiences a sudden intensification of appetite suppression, delayed gastric emptying, and metabolic regulation. This adjustment period typically lasts one to two weeks after each dose increase. During this window, headaches are most likely.
Think of it like altitude adjustment. When you move from sea level to a mountain town, you might get headaches for a few days while your body adapts. The same principle applies to dose escalation with tirzepatide. Your body is adjusting to a new metabolic baseline, and headaches are part of that adjustment for some people.
Most dose escalation headaches resolve within 7 to 14 days. If they persist beyond two weeks at a stable dose, the cause is more likely dehydration or blood sugar issues rather than the dose change itself.
Mechanism 4: hormonal and vascular changes
This mechanism is less common but worth understanding. Tirzepatide stimulates GLP-1 and GIP receptor activity throughout the body, not just in the gut and pancreas. GLP-1 receptors exist in the central nervous system, and activation of these receptors can influence vascular tone, the tension and diameter of blood vessels.
Changes in vascular tone can trigger headaches, particularly in people who are prone to migraines or vascular headaches. The good news is that this mechanism appears to affect a small minority of users. The research literature documents it primarily in case reports rather than large-scale studies.
Interestingly, GLP-1 receptor agonists have also shown promise in reducing migraine frequency in obese patients, likely through anti-inflammatory effects. GLP-1 medications reduce proinflammatory cytokines like interleukin-6 and tumor necrosis factor alpha, both of which are elevated in neuroinflammatory conditions including migraine. So while tirzepatide might trigger headaches initially through vascular adjustment, it could actually improve headache conditions long-term.
Mechanism 5: caffeine and medication interactions
This one surprises people. When tirzepatide dramatically reduces your food intake, it often reduces your beverage habits too. Many people who normally drink 2 to 3 cups of coffee daily start drinking less without thinking about it. The resulting caffeine withdrawal causes headaches, and it has nothing to do with tirzepatide pharmacologically.
Caffeine withdrawal headaches typically start 12 to 24 hours after your last caffeine intake, peak at 20 to 51 hours, and can last up to nine days. They feel like a dull, persistent pressure that wraps around the head. If your headache started around the same time you reduced your coffee intake, caffeine withdrawal is the likely explanation.
Similarly, changes in meal timing and composition can alter the absorption of other medications you may be taking, potentially affecting blood pressure medications, thyroid medications, or other drugs that influence headache susceptibility.
Types of headaches on tirzepatide and what each one means
Not all headaches are the same. Identifying your specific headache type helps you choose the right treatment and determine whether you need to adjust your protocol or see a doctor.
Tension headaches
These are the most common type reported with tirzepatide. They feel like a band of pressure around the head, typically mild to moderate in intensity. Tension headaches on tirzepatide usually result from dehydration, stress, poor sleep, or muscle tension from reduced caloric intake.
Duration: 30 minutes to several hours. Frequency: intermittent during the first 2 to 4 weeks of treatment or dose changes. Responds well to hydration, rest, and over-the-counter pain relief.
Dehydration headaches
More intense than typical tension headaches, dehydration headaches throb. They worsen when you bend over, move quickly, or stand up. They concentrate around the temples and forehead.
The telltale sign is dramatic improvement within 15 to 30 minutes of drinking 16 to 20 ounces of water. If you drink a tall glass of water and your headache starts fading within half an hour, dehydration was the cause. No further investigation needed.
Hypoglycemic headaches
These headaches come with friends. If your headache is accompanied by shakiness, brain fog, irritability, sweating, or a feeling of weakness, low blood sugar is likely the trigger. They hit hardest after long periods without eating, particularly in the morning or late afternoon.
Hypoglycemic headaches respond quickly to eating something with both sugar and protein. A small handful of nuts with a piece of fruit, or a glass of milk, can resolve the headache within 15 to 20 minutes. If you are tracking your tirzepatide dosage and experiencing these regularly, your eating schedule needs adjustment.
Migraine episodes
For people with a history of migraines, tirzepatide can occasionally trigger episodes during the initial adjustment period. Migraine headaches are different from tension or dehydration headaches. They typically affect one side of the head, pulse or throb, cause sensitivity to light and sound, and may include nausea (making it hard to distinguish from tirzepatide GI side effects).
If you have a migraine history and notice increased frequency after starting tirzepatide, document the pattern and discuss it with your healthcare provider. One case study documented a patient with hemiplegic migraines experiencing daily episodes during 60 days of GLP-1 agonist treatment. This is rare but warrants attention.
However, here is the flip side. A real-world study on tirzepatide in patients with idiopathic intracranial hypertension showed significant headache improvement with weight loss. So the same medication that might trigger migraines short-term could reduce them long-term by addressing underlying inflammatory and metabolic factors.
Caffeine withdrawal headaches
Dull, constant, bilateral pressure. Often starts in the morning. Gets better after coffee. Lasts 2 to 9 days if you do not resume caffeine. If you reduced your coffee intake around the same time you started tirzepatide, this is probably your culprit.
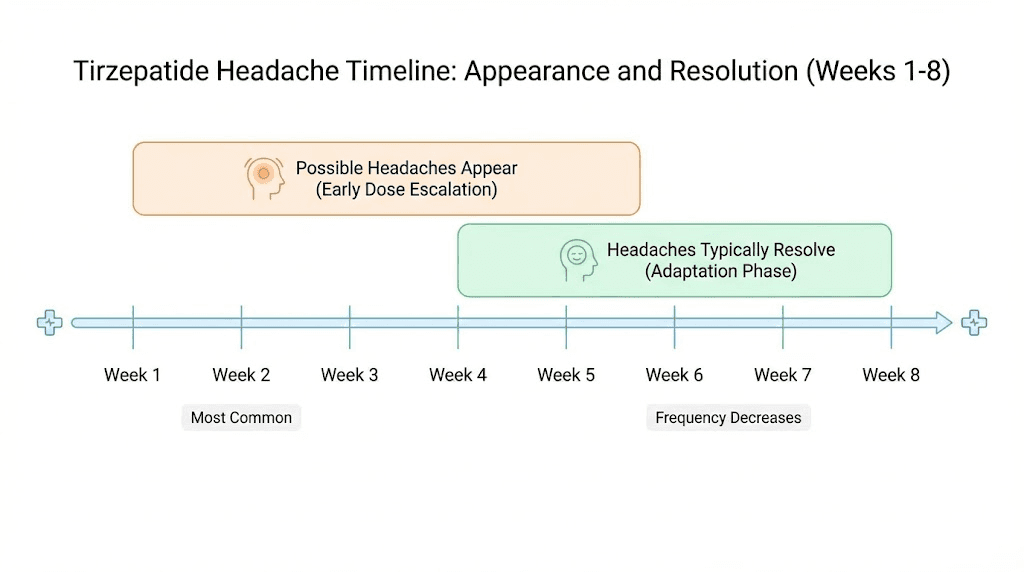
Timeline: when tirzepatide headaches start, peak, and resolve
Understanding the typical timeline helps you plan your protocol and know when to worry versus when to wait.
Week 1 to 2: the adjustment window
Most headaches appear within the first one to two weeks of starting tirzepatide or increasing a dose. This is when your body is making the biggest metabolic adjustments. Appetite drops suddenly, eating patterns change, and hydration habits have not caught up yet.
During this window, headaches are most likely caused by dehydration and blood sugar changes. They are typically mild to moderate and respond well to hydration and regular eating.
Week 2 to 4: the plateau phase
For most people, headaches either resolve or significantly improve by week two to four. Your body has adapted to the new dose, your eating patterns have stabilized, and you have hopefully adjusted your water intake upward.
If headaches persist beyond four weeks at a stable dose, something else is going on. Chronic dehydration, consistently inadequate nutrition, medication interactions, or an unrelated headache condition needs evaluation.
Dose escalation restarts the clock
Every time you increase your dose, expect a brief adjustment period. The standard tirzepatide escalation schedule moves from 2.5mg to 5mg, then to 7.5mg, 10mg, 12.5mg, and finally 15mg, with each step lasting at least four weeks. Each increase can trigger 3 to 7 days of mild headaches as your body readjusts.
This is normal. This is temporary. And it does not mean tirzepatide is wrong for you.
The long-term picture
After the initial titration phase, headaches become uncommon for the vast majority of users. Long-term studies show that adverse event rates, including headaches, decrease substantially after the first 12 to 16 weeks of therapy. People who maintain adequate hydration and consistent nutrition rarely report ongoing headaches beyond the adjustment period.
How to prevent tirzepatide headaches before they start
Prevention is dramatically more effective than treatment. These strategies reduce headache risk by 80% or more when followed consistently.
Hydration protocol
This is the single most important thing you can do. Drink more water than you think you need.
Minimum target: 8 to 10 glasses (64 to 80 ounces) of water daily. But that is the floor, not the ceiling. People on tirzepatide who are active, live in warm climates, or experience GI side effects should aim for 100 or more ounces daily.
Practical approach:
Drink 16 ounces immediately upon waking, before coffee, before food
Keep a water bottle visible at all times as a physical reminder
Set phone reminders every 2 hours to drink 8 ounces
Add electrolytes to one or two glasses daily (sodium, potassium, magnesium)
Track your intake for the first two weeks until the habit is automatic
Electrolytes matter more than most people realize. Pure water alone does not prevent dehydration headaches if your electrolyte balance is off. A pinch of salt in your water, an electrolyte packet, or coconut water can make a meaningful difference. This is particularly important if you are experiencing tirzepatide fatigue alongside headaches, as both symptoms share dehydration as a root cause.
Blood sugar management
Even if you are not hungry, eat. This is the hardest adjustment for people on tirzepatide, because the whole point of the medication is to reduce appetite. But your brain still needs glucose, and skipping meals entirely is the fastest route to hypoglycemic headaches.
Follow this eating schedule:
Eat something within 1 hour of waking
Include 20 to 30 grams of protein at each meal
Eat every 3 to 4 hours even if you are not hungry
Keep emergency snacks available (nuts, cheese, protein bars)
Avoid going more than 5 hours without food during waking hours
Protein is essential. It stabilizes blood sugar more effectively than carbohydrates alone, sustains energy longer, and preserves muscle mass during weight loss. Our tirzepatide food guide covers exactly which foods to prioritize and which to avoid during therapy.
Caffeine consistency
If you drink coffee, keep drinking coffee. Seriously. Do not let tirzepatide-induced appetite changes alter your caffeine routine. If you normally have two cups in the morning, maintain two cups in the morning. Caffeine withdrawal headaches are entirely preventable by simply maintaining your existing caffeine habits.
If you want to reduce caffeine intake, do it slowly and deliberately. Reduce by half a cup every 3 to 4 days. Do not let it happen accidentally because your appetite decreased.
Sleep optimization
Poor sleep increases headache susceptibility by 36% according to headache research. Tirzepatide can affect sleep quality indirectly, especially if nausea or appetite changes disrupt your normal evening eating patterns.
Aim for 7 to 9 hours nightly. Maintain consistent wake and sleep times. Eat a small protein-rich snack before bed if you tend to wake up with morning headaches, as overnight blood sugar drops are common during tirzepatide therapy.
Injection timing optimization
Some people find that headaches correlate with injection timing. While there is no large-scale data on this, anecdotal reports suggest that injecting in the evening rather than the morning may reduce next-day headaches for some users. The theory is that sleeping through the initial peak absorption period reduces the conscious experience of side effects.
Experiment with your injection timing and track whether headaches correlate with specific days post-injection. Many people report headaches are worst on days 1 to 3 after injection and resolve by day 4 to 5.
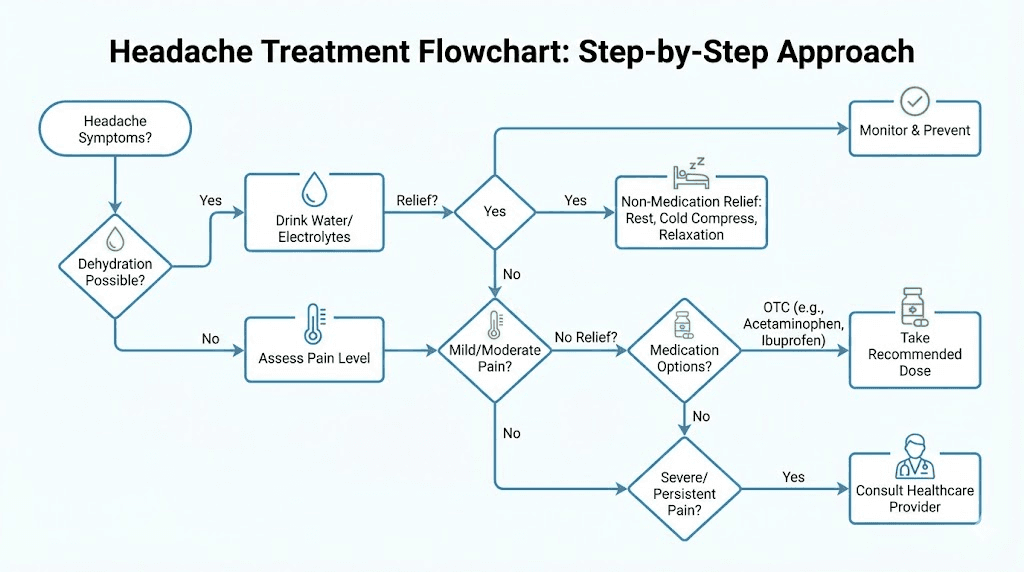
How to treat tirzepatide headaches when they happen
Prevention does not work 100% of the time. When a headache breaks through, here is exactly what to do.
First response: hydrate immediately
Before you reach for any medication, drink 16 to 20 ounces of water. Wait 20 to 30 minutes. In at least half of all tirzepatide headache cases, this alone resolves the issue.
Add electrolytes if available. A glass of water with a quarter teaspoon of salt and a squeeze of lemon delivers sodium quickly. Commercial electrolyte drinks or packets work too. Avoid sugary sports drinks, as the sugar spike and subsequent crash can make things worse.
Second response: eat something
If hydration alone does not work within 30 minutes, eat a small meal or snack containing both protein and carbohydrates. This addresses potential blood sugar issues. Good options include:
Apple slices with almond butter
Greek yogurt with berries
A handful of nuts and a banana
Cheese and crackers
A protein shake
If eating triggers nausea, try bland, easy-to-digest options. A few saltine crackers, a piece of toast, or a small cup of broth can stabilize blood sugar without overwhelming your stomach.
Third response: over-the-counter medication
If hydration and food have not resolved the headache within an hour, over-the-counter pain relief is appropriate.
Acetaminophen (Tylenol): 650 to 1000mg. This is generally the safest first choice. Acetaminophen does not interact with tirzepatide and does not irritate the stomach, which is important when GI side effects are already present. Do not exceed 3000mg in 24 hours.
Ibuprofen (Advil): 400 to 600mg. Effective for inflammatory and vascular headaches. Take with food to reduce stomach irritation. Avoid if you have existing GI issues from tirzepatide, as NSAIDs can worsen nausea and stomach discomfort. Do not exceed 1200mg in 24 hours without medical guidance.
Aspirin: 500 to 1000mg. Similar profile to ibuprofen. Take with food. Avoid if you have GI sensitivity.
Avoid combination headache medications containing caffeine (Excedrin) if you are not a regular caffeine consumer, as they can create rebound headache cycles.
For persistent headaches
If headaches persist despite hydration, nutrition, and OTC medication, try these additional approaches:
Cold compress on the forehead or back of the neck for 15 to 20 minutes
Dark, quiet room for 20 to 30 minutes (especially effective for vascular headaches)
Gentle neck stretches to relieve tension that accumulates during nausea episodes
Peppermint oil applied to the temples (some evidence for tension headache relief)
The dehydration problem: why it is worse on tirzepatide than you think
Dehydration deserves its own section because it is massively underestimated by tirzepatide users. Most people think they drink enough water. Most people are wrong, even before starting a medication that dramatically changes fluid balance.
The triple dehydration effect
Tirzepatide creates a perfect storm of dehydration through three simultaneous mechanisms:
Reduced food intake. The average person gets 20 to 30% of their daily water from food. Fruits, vegetables, soups, and even meat contain significant water. When tirzepatide cuts your food intake by 30 to 50%, you lose a major water source that most people never account for.
GI fluid losses. Nausea affects up to 29% of tirzepatide users. Diarrhea affects up to 23%. Vomiting affects up to 14%. Each of these symptoms drains fluid rapidly. A single episode of vomiting can deplete 200 to 500ml of fluid. Diarrhea can cause even greater losses.
Reduced thirst drive. This is the sneaky one. When you eat less, you think about food less, and you often think about drinking less too. The natural cues that prompt hydration, meals, snack breaks, lunchtime routine, fade when appetite disappears. You simply forget to drink.
Signs you are dehydrated beyond headaches
Headaches are an early warning sign of dehydration, but they are not the only sign. Watch for:
Dark yellow or amber urine (should be pale yellow to clear)
Dry mouth or lips
Fatigue and low energy
Dizziness when standing up
Decreased urine frequency (fewer than 4 bathroom trips daily)
Dry skin that tents when pinched
If you are experiencing fatigue on tirzepatide, check your hydration before assuming it is a medication side effect. Dehydration causes fatigue, headaches, brain fog, and low energy, all symptoms that people commonly attribute to the medication itself rather than their fluid intake.
Electrolyte balance matters
Drinking plain water is necessary but not sufficient. When you lose fluids through GI symptoms, you lose electrolytes too. Sodium, potassium, and magnesium all decrease. These minerals regulate nerve function, muscle contraction, and fluid balance in the brain. Their depletion causes headaches independent of total water intake.
Consider adding an electrolyte supplement to your daily routine, especially during the first month of treatment or after any dose increase. Look for products containing sodium (300 to 500mg), potassium (150 to 300mg), and magnesium (50 to 100mg) per serving. Avoid products with large amounts of added sugar.
Blood sugar and headaches: the connection most guides ignore
Blood sugar management is the second most important factor in preventing tirzepatide headaches, and most guides barely mention it beyond saying eat regular meals. Let us go deeper.
How tirzepatide affects blood sugar
Tirzepatide enhances glucose-dependent insulin secretion. When blood sugar rises after a meal, tirzepatide amplifies the insulin response to bring it down faster. It also slows gastric emptying, which means food takes longer to digest and blood sugar rises more gradually after eating.
Both of these mechanisms are therapeutically beneficial. But they can also create blood sugar dips that trigger headaches, particularly in three situations:
Situation 1: Skipping meals. When you skip a meal on tirzepatide, your blood sugar drops because the medication is still enhancing insulin sensitivity. Without incoming food to maintain glucose levels, the drop can trigger a headache. This is the most common blood-sugar-related headache scenario.
Situation 2: High-carb meals followed by crashes. Eating a high-sugar or high-carbohydrate meal causes a rapid blood sugar spike, which tirzepatide helps bring down aggressively. The resulting crash below your normal baseline can trigger a headache 1 to 3 hours after eating. This is why avoiding certain foods on tirzepatide matters.
Situation 3: Overnight fasting. The longest gap between meals is overnight. If you eat dinner at 6pm and do not eat breakfast until 8am, that is 14 hours without food. On tirzepatide, which is still working to regulate blood sugar during this period, morning headaches become more likely. Eating a small protein-rich snack before bed can prevent this.
The protein solution
Protein is your best tool for preventing blood sugar headaches on tirzepatide. Here is why.
Protein stabilizes blood sugar because it converts to glucose slowly, without the spike-and-crash pattern of simple carbohydrates. It also triggers glucagon release, which prevents blood sugar from dropping too low. And it provides satiety, making it easier to eat enough despite reduced appetite.
Target 20 to 30 grams of protein per meal, three times daily. If you can only manage two meals, aim for 30 to 40 grams each. Use our dosage calculators and dietary planning resources to build a nutrition strategy that prevents blood sugar headaches while supporting your weight loss goals.
When tirzepatide headaches signal something serious
The vast majority of tirzepatide headaches are harmless and temporary. But certain headache patterns require immediate medical attention. Knowing the difference could save your life.
Red flags: seek medical help immediately
Thunderclap headache: sudden, severe headache reaching maximum intensity within 60 seconds. This can indicate subarachnoid hemorrhage or other vascular emergencies.
Headache with neurological symptoms: confusion, difficulty speaking, vision changes, weakness on one side of the body, or numbness. These could indicate stroke or other serious neurological events.
Worst headache of your life: any headache that is dramatically more severe than anything you have experienced before warrants emergency evaluation.
Headache with fever and stiff neck: this combination suggests possible meningitis or other infection.
Progressive worsening: a headache that gets steadily worse over days or weeks without responding to any treatment needs imaging studies to rule out structural causes.
Yellow flags: schedule a doctor appointment
Headaches persisting beyond 4 to 6 weeks at a stable dose despite adequate hydration and nutrition
Headaches that do not respond to any over-the-counter treatment
New-onset migraine patterns in someone without migraine history
Headaches accompanied by significant vision changes, especially visual field loss or papilledema symptoms
Headaches that consistently wake you from sleep
Important safety note about pancreatitis
Acute pancreatitis occurs in approximately 0.32 to 0.39% of tirzepatide users in clinical trials. Pancreatitis can cause severe headaches alongside its primary symptom of intense abdominal pain that radiates to the back. If you experience a severe headache combined with upper abdominal pain, nausea, and vomiting that seems different from typical GI side effects, seek medical evaluation promptly.
This is not meant to alarm you. The risk is very low. But being aware of the connection between abdominal symptoms and headaches on tirzepatide helps you recognize unusual patterns early.
Tirzepatide headaches versus other side effects: the full context
Headaches are one of many potential side effects of tirzepatide. Understanding how they compare to other adverse events helps you put the headache risk in perspective.
Side effect comparison table
Side effect | Incidence rate | Severity | Duration | Treatability |
|---|---|---|---|---|
Nausea | 13 to 29% | Mild to moderate | 2 to 4 weeks | Highly treatable |
Diarrhea | 13 to 23% | Mild to moderate | 1 to 3 weeks | Highly treatable |
Headache | 4 to 11% | Mild to moderate | 1 to 4 weeks | Very treatable |
Vomiting | 5 to 14% | Mild to moderate | 1 to 2 weeks | Treatable |
Constipation | 6 to 9% | Mild | Variable | Treatable |
Fatigue | 5 to 8% | Mild | 2 to 6 weeks | Treatable |
Injection site reactions | 3 to 5% | Mild | 1 to 2 days | Self-resolving |
Notice where headaches fall on this list. They are less common than GI side effects and generally milder. They are also among the most treatable side effects because their primary causes (dehydration and blood sugar) are modifiable behaviors rather than pharmacological effects.
Compared to other tirzepatide side effects like anxiety, headaches are more straightforward in both their causes and their solutions. The anxiety connection is more complex and involves neurotransmitter changes that are harder to address with simple lifestyle modifications.
Why headaches should not make you stop tirzepatide
The discontinuation rate due to adverse events in tirzepatide trials ranged from 3.3% at 10mg to 4.3% at 15mg, compared to 0.5% for placebo. Headaches alone almost never justify stopping the medication, especially when the underlying causes are addressable.
Consider the risk-benefit calculation. Tirzepatide produces 16 to 22.5% body weight reduction in clinical trials. The health benefits of that weight loss, reduced cardiovascular risk, improved blood sugar control, decreased joint pain, better sleep, vastly outweigh the temporary inconvenience of manageable headaches.
If headaches are making you consider stopping tirzepatide, try the prevention and treatment protocols in this guide first. Give them two full weeks of consistent implementation before making any decisions about your medication. In the overwhelming majority of cases, the headaches resolve completely.
Special populations: who is more likely to get tirzepatide headaches
While anyone on tirzepatide can experience headaches, certain groups face higher risk. Knowing whether you fall into a higher-risk category allows you to implement prevention strategies proactively.
People with migraine history
If you have existing migraines, tirzepatide can temporarily increase their frequency during the adjustment period. This is likely related to blood sugar fluctuations and hormonal changes rather than a direct pharmacological effect. However, research also suggests that GLP-1 receptor agonists may reduce migraine frequency long-term through anti-inflammatory pathways, so the initial worsening may be temporary.
Strategy: maintain a migraine diary, keep rescue medications available, and discuss preventive migraine therapy with your neurologist before starting tirzepatide.
People on blood pressure medications
Tirzepatide causes weight loss, which naturally lowers blood pressure. If you are already taking antihypertensives, the combination can cause blood pressure to drop too low, triggering headaches, dizziness, and lightheadedness.
Strategy: monitor blood pressure regularly during the first 8 to 12 weeks. Discuss potential dose adjustments with your prescriber. Headaches in this population may require medication adjustment rather than just hydration.
People with diabetes on insulin or sulfonylureas
Adding tirzepatide to existing diabetes medications that lower blood sugar creates a higher risk of hypoglycemia. The meta-analysis showed mild hypoglycemia rates up to 22.6% in the 10mg group. Hypoglycemic headaches in this population are more common and potentially more severe.
Strategy: work closely with your endocrinologist to adjust existing diabetes medications when starting tirzepatide. Blood sugar monitoring is essential during the titration period.
People who exercise heavily
Athletes and fitness enthusiasts on tirzepatide face compounded dehydration risk. Exercise increases fluid losses through sweat, while tirzepatide reduces fluid intake through appetite suppression. The combination creates substantial dehydration risk, especially during intense training sessions.
Strategy: increase water intake by an additional 16 to 24 ounces for every 30 minutes of exercise. Replenish electrolytes during and after training. Consider timing your training sessions around meals to maintain blood sugar stability.
People starting at higher doses
The clinical data clearly shows a dose-response relationship for headaches. Starting at higher doses or escalating too quickly increases headache risk proportionally. People who skip the standard titration schedule, whether by choice or prescriber recommendation, face the highest headache rates.
Strategy: follow the recommended escalation schedule. Start at 2.5mg for four weeks before moving to 5mg. Patience during titration prevents not only headaches but also the GI side effects that compound dehydration.
Compounded tirzepatide and headaches: does the formulation matter
Many people obtain tirzepatide from compounding pharmacies rather than brand-name Mounjaro or Zepbound. Does the formulation affect headache risk?
The short answer is: the active peptide is the same. Compounded tirzepatide contains the identical amino acid sequence as brand-name versions. The headache risk from the peptide itself does not change based on the source.
However, compounded formulations often include additional ingredients. Tirzepatide with glycine is a common compounded formulation. Tirzepatide with niacinamide is another. Tirzepatide with B12 is increasingly popular.
Niacinamide specifically can cause flushing and headaches in some people, particularly at higher doses. If you are using a compounded formulation containing niacinamide and experiencing headaches that seem disproportionate to what clinical data would predict, the additional ingredient might be contributing.
B12 additions are less likely to cause headaches and may actually help. B12 deficiency can cause headaches, and many people on calorie-restricted diets become deficient over time.
If you suspect your compounded formulation is contributing to headaches, ask your compounding pharmacy about the specific inactive ingredients and discuss alternatives with your prescriber. You might benefit from a formulation adjustment, such as switching from one compounded tirzepatide product to another with different additives.
Tracking your headaches: the data-driven approach
Guessing does not work. If you want to eliminate tirzepatide headaches permanently, you need data. A simple tracking system takes 60 seconds per day and provides the insights needed to identify your specific triggers.
What to track daily
Water intake (in ounces or glasses)
Meals consumed (timing and approximate protein content)
Caffeine intake (cups of coffee or tea)
Headache occurrence (yes or no)
Headache severity (1 to 10 scale)
Headache timing (morning, afternoon, evening)
What helped (water, food, medication, rest)
Days since last injection
Current tirzepatide dose
Patterns to look for
After tracking for one to two weeks, look for these patterns:
Injection day correlation. Do headaches consistently appear on specific days relative to your injection? Many people report headaches on days 1 to 3 post-injection, which aligns with peak absorption and metabolic effects.
Hydration correlation. Do headaches appear on days when water intake drops below a certain threshold? Most people find a clear cutoff where anything below 60 to 70 ounces triggers headaches.
Meal timing correlation. Do headaches follow long gaps without eating? Morning headaches often indicate inadequate evening nutrition or overnight blood sugar drops.
Dose correlation. Did headaches start or worsen after a dose increase? Dose escalation headaches follow a predictable pattern of appearing within days of the increase and resolving within one to two weeks.
This data gives you and your healthcare provider actionable information instead of vague complaints. Rather than saying I get headaches on tirzepatide, you can say I get headaches on days when I drink less than 64 ounces of water, specifically on days 2 to 3 after injection. That level of specificity leads to targeted solutions.
Frequently asked questions
Can I take Tylenol with tirzepatide?
Yes. Acetaminophen (Tylenol) does not interact with tirzepatide and is generally considered the safest first-line pain reliever during GLP-1 therapy. Take 650 to 1000mg as needed, not exceeding 3000mg in 24 hours. If you are taking other medications that contain acetaminophen, account for those doses in your daily total. Always take Tylenol with a small amount of food to reduce the chance of stomach upset, especially since tirzepatide already affects your GI system.
How long do tirzepatide headaches last?
Individual headache episodes typically last 30 minutes to several hours and respond well to hydration, food, and over-the-counter medication. The overall pattern of recurring headaches usually resolves within 2 to 4 weeks of starting treatment or adjusting the dose. For 15mg doses, headaches may persist slightly longer, up to 4 to 6 weeks, before resolving. If headaches continue beyond 6 weeks at a stable dose with adequate hydration and nutrition, consult your healthcare provider for further evaluation.
Should I stop tirzepatide if I get headaches?
No, not unless your healthcare provider specifically advises it. Headaches alone are not a medical reason to discontinue tirzepatide in the vast majority of cases. The weight loss benefits of tirzepatide significantly outweigh the temporary inconvenience of manageable headaches. Try the prevention and treatment strategies in this guide for at least two weeks before considering any medication changes. If headaches are severe, persistent, or accompanied by neurological symptoms, discuss them with your doctor promptly.
Do headaches get worse at higher tirzepatide doses?
Clinical data shows a dose-dependent increase. At 5mg, headache rates are 4%. At 10mg, rates are 5.16%. At 15mg, rates climb to 10.71%. However, each dose increase triggers a temporary adjustment period, and headaches at any given dose typically resolve within 2 to 4 weeks. The standard tirzepatide titration schedule of four weeks at each dose level gives your body adequate time to adjust and minimizes headache risk at each step.
Can dehydration from tirzepatide cause severe headaches?
Yes. Dehydration is the most common cause of tirzepatide headaches and can cause severe, throbbing headaches that mimic migraines in intensity. Severe dehydration headaches worsen with movement, concentrate around the temples, and can be accompanied by dizziness and fatigue. Prevention through adequate fluid intake (minimum 64 to 80 ounces daily, more if experiencing GI symptoms) is significantly more effective than treatment after the headache starts.
Is it normal to get a headache the day after a tirzepatide injection?
Yes, this is one of the most commonly reported patterns. Headaches on days 1 to 3 post-injection correspond with peak peptide absorption and the most significant metabolic changes. These headaches are typically mild to moderate and respond well to hydration and food. If day-after headaches are consistent, try increasing your water intake by 20 to 30% on injection day and the following day. Some people also find that evening injections reduce next-day headaches compared to morning injections.
Will tirzepatide headaches go away permanently?
For the vast majority of users, yes. Long-term studies show that adverse event rates decrease substantially after the initial 12 to 16 weeks of therapy. Once your body has fully adapted to the medication and you have established consistent hydration and eating patterns, headaches become rare. Some users experience brief headache recurrences with each dose increase, but these follow the same 1 to 2 week resolution pattern and become progressively milder with successive increases.
Does the type of tirzepatide matter for headaches?
Brand-name tirzepatide (Mounjaro, Zepbound) and compounded tirzepatide contain the same active peptide. The headache risk from the peptide is identical. However, compounded formulations with niacinamide may slightly increase headache risk due to the additional ingredient. If you suspect your compounded formulation is contributing to headaches, discuss alternative formulations with your provider.
External resources
Adverse Events Related to Tirzepatide - Meta-analysis (PubMed Central)
Tirzepatide and Idiopathic Intracranial Hypertension Study (PubMed Central)
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed side effect management guides, interaction databases, and direct support from experienced researchers who understand what you are going through.
In case I do not see you, good afternoon, good evening, and good night. May your headaches stay brief, your hydration stay consistent, and your tirzepatide results stay worth every adjustment.