Feb 26, 2026
Of the participants who stopped tirzepatide in the landmark SURMOUNT-4 trial, 82.5% regained at least a quarter of the weight they had lost within one year. Read that again. More than four out of five people watched their progress reverse after discontinuing the medication that had transformed their relationship with food and hunger.
That statistic terrifies people. It should.
But it also tells an incomplete story. The 17.5% who maintained most of their weight loss did something different. They did not simply stop tirzepatide and hope for the best. They prepared. They built systems. They understood exactly what would happen inside their bodies once the medication cleared, and they had strategies ready for every challenge that followed. This guide is the playbook they used. Whether you are planning to stop tirzepatide in the coming weeks, actively tapering your dose, or already feeling the pull of returning hunger, everything you need is here. From the specific exercise protocols that research shows prevent regain, to the protein targets that preserve muscle mass, to the tapering schedules that give your body time to adapt, this is not vague advice about eating well and moving more. These are specific, actionable strategies backed by clinical trial data and real-world experience from thousands of researchers who have navigated this exact transition.
The tirzepatide weight loss timeline is well documented. The before and after results speak for themselves. But what happens after tirzepatide? That conversation matters just as much, and it does not get nearly enough attention. SeekPeptides has compiled the most comprehensive evidence available on post-tirzepatide weight maintenance. From understanding how tirzepatide works to mastering the dosing protocols, the foundation matters. But the exit strategy might matter even more. The researchers who maintain their results after stopping tirzepatide share one thing in common. They treat the post-medication phase not as a return to normal, but as the beginning of an entirely new protocol, one that requires the same discipline, tracking, and strategic thinking that made their treatment phase successful. The medication did part of the heavy lifting. Now you do all of it. But you do it with knowledge, preparation, and a proven framework.
Why weight regain happens after stopping tirzepatide
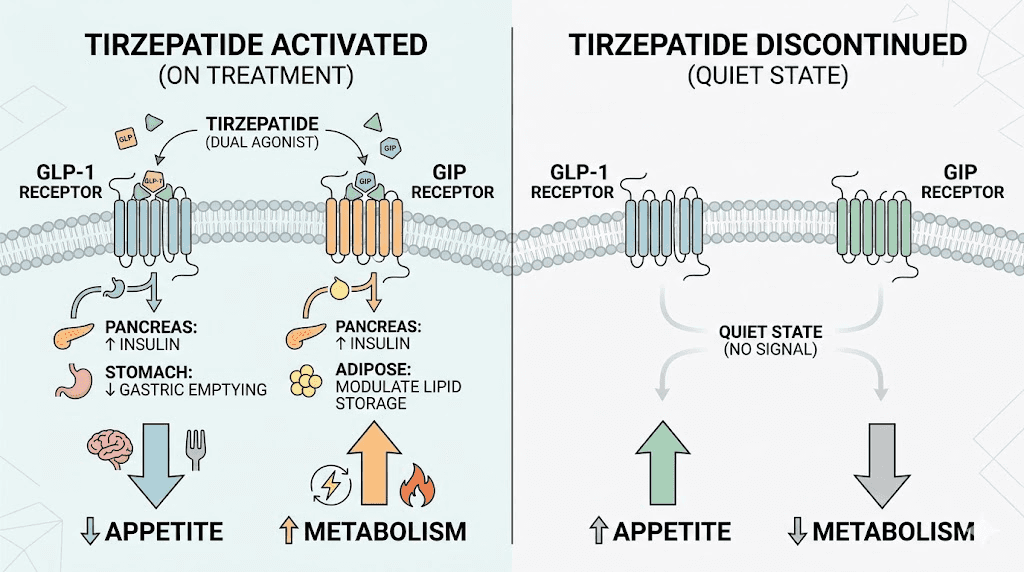
The biology is unforgiving. Tirzepatide works by activating two receptor systems simultaneously, GLP-1 and GIP, that control hunger, satiety, gastric emptying, and metabolic rate. When the medication leaves your system, those receptors go quiet. The consequences are immediate and predictable.
Appetite returns first. The appetite suppression that tirzepatide provides is one of its most powerful effects. Within days of discontinuation, hunger signals begin resurging. Within two to three weeks, most people report appetite levels comparable to pre-treatment baseline. That is not a failure of willpower. It is biochemistry.
Gastric emptying accelerates. On tirzepatide, food moves through the stomach more slowly, creating prolonged feelings of fullness. Remove the medication, and gastric transit returns to normal speed. Meals that used to keep you satisfied for hours now leave you hungry within 90 minutes. The mechanisms behind GLP-1 appetite suppression involve direct signaling to the brain, not just stomach mechanics, which explains why the effect reverses so completely once the drug clears.
Then comes the metabolic adaptation. Your body lost weight on tirzepatide, which means it now requires fewer calories than before. But the returning appetite drives you toward the same caloric intake that maintained your higher pre-treatment weight. This mismatch is the fundamental driver of regain. It is the same mechanism that undermines every weight loss approach, from calorie restriction to bariatric surgery. The body defends against weight loss with remarkable persistence.
Hormonal changes compound the problem. Leptin levels drop proportionally with fat loss, signaling to the brain that energy stores are depleted. Ghrelin, the hunger hormone, increases. These hormonal shifts were partially masked by tirzepatide dual receptor activity. Without the medication, the full force of these compensatory mechanisms activates. Understanding how tirzepatide affects metabolism helps explain why the transition is so challenging. The medication does not just reduce appetite. It fundamentally alters energy balance through multiple pathways simultaneously.
The withdrawal experience from GLP-1 medications varies significantly between individuals. Some people notice dramatic hunger increases within the first week. Others experience a more gradual return over three to four weeks. The fatigue that accompanies GLP-1 medication changes can make the transition even more difficult, sapping the energy needed for exercise and meal preparation at exactly the moment those habits matter most.
What makes this particularly frustrating is that the speed of regain does not match the speed of initial loss. The rapid results that tirzepatide delivers took weeks to months to achieve. Regain can erase months of progress in a fraction of that time. Research suggests that most regain occurs in the first six months after discontinuation, with the rate highest in the initial 8 to 12 weeks.
None of this means maintaining weight loss is impossible. It means you need a plan that accounts for these specific biological realities. The differences between GLP-1 medications matter here too. Tirzepatide, as a dual GIP/GLP-1 agonist, creates a different metabolic environment than single-receptor medications like semaglutide. The transition from tirzepatide may differ from semaglutide discontinuation because two receptor systems are deactivating simultaneously rather than one, potentially making the adjustment period more intense.
There is also a psychological dimension that compounds the biological challenge. During treatment, many people develop a new relationship with food. Meals become fuel rather than comfort. Portions shrink naturally. The constant background noise of food thoughts goes quiet. When tirzepatide stops, that noise returns, and it can feel like losing a superpower you had grown to depend on. The emotional impact of returning hunger should not be underestimated. It is real, it is difficult, and it requires its own set of coping strategies beyond just diet and exercise.
The key insight is this: weight regain after stopping tirzepatide is not a personal failure. It is a predictable biological response to removing a medication that fundamentally altered multiple metabolic pathways. Knowing this changes the entire approach from guilt-based willpower struggles to evidence-based strategic preparation.
What the SURMOUNT-4 trial actually shows
The SURMOUNT-4 trial provides the clearest picture of what happens when tirzepatide stops. Understanding this data is essential for setting realistic expectations and planning accordingly.
Here is what happened. Adults with obesity received tirzepatide for 36 weeks during an open-label period, achieving significant weight loss on maximum tolerated doses of 10 or 15 mg weekly. At week 36, 670 participants were randomly split into two groups. Half continued receiving tirzepatide. Half switched to placebo. The results after 52 additional weeks were striking.
Among those who continued tirzepatide, approximately 9 in 10 maintained at least 80% of the weight they had lost during the initial phase. The medication kept working. No surprise there. The standard tirzepatide dose protocols deliver reliable, sustained weight reduction when maintained consistently.
Among those switched to placebo, the outcomes broke down into four distinct groups. Fifty-four participants regained less than 25% of their lost weight. Seventy-seven regained between 25% and 50%. One hundred and three regained between 50% and 75%. And seventy-four regained 75% or more of their initial weight loss.
Those numbers tell a nuanced story.
Yes, 82.5% regained at least a quarter of what they lost. But nearly 18% kept the vast majority of their progress. And the distribution reveals important patterns. The participants who regained the least shared common characteristics. They tended to have established exercise routines during the treatment phase. They maintained higher protein intake. They had structured monitoring systems in place. They did not simply stop the medication and return to pre-treatment habits.
What matters for your planning is this: the degree of regain directly correlated with the reversal of health improvements. Those who regained less than 25% of body weight showed no significant changes in waist circumference, triglycerides, non-HDL cholesterol, fasting insulin, or insulin resistance measures. Their carefully managed dosing history had built a metabolic foundation that partially held even without the medication.
Those who regained 75% or more saw nearly complete reversal of all cardiometabolic improvements. Blood pressure, cholesterol, blood sugar markers, and inflammatory indicators all returned toward baseline levels. The question of treatment duration is central to this discussion. The SURMOUNT-4 data suggests that longer treatment periods before discontinuation may provide some protective effect, though this needs further investigation.
One critical takeaway from SURMOUNT-4 that often gets overlooked: the participants who maintained the most weight did not have superhuman willpower. They had preparation. They entered the post-medication phase with established habits, monitoring systems, and support structures already in place. They treated the end of medication as the beginning of a new protocol, not the end of a journey. That mindset shift, from passive medication recipient to active maintenance strategist, appears to be the most significant predictor of long-term success.
The real-world tirzepatide transformations demonstrate what is possible during treatment. The question this guide answers is how to preserve those results for the months and years that follow. The early results from GLP-1 medications are inspiring, but the long-term maintenance story is where lasting health outcomes are determined.
For context, similar patterns appear across all GLP-1 receptor agonist studies. The early weeks of any GLP-1 medication set the trajectory for long-term outcomes. And the challenges of optimizing weight loss on these medications parallel the challenges of maintaining it afterward. In both cases, the details of the protocol matter enormously.
The SURMOUNT-MAINTAIN trial is currently investigating dedicated maintenance strategies after tirzepatide weight loss. Until those results are available, the strategies in this guide represent the best available evidence for keeping weight off after discontinuation.
The tapering approach: how to step down gradually
The FDA prescribing information for tirzepatide does not require a taper. Pharmacologically, you can stop the medication at any dose without dangerous withdrawal effects. But "medically safe to stop" and "optimal for weight maintenance" are two very different things.
Research presented at the European Congress on Obesity found that people who gradually reduced their dose over an average of nine weeks maintained stable body weight for the first 26 weeks after complete cessation. Those who stopped abruptly saw weight increases beginning almost immediately. The difference was significant enough to change clinical practice recommendations.
Tapering works for a practical reason. It gives your appetite-regulating systems time to partially recalibrate at each lower dose level. Rather than experiencing the full force of appetite return all at once, you face incremental increases that are easier to manage with behavioral strategies. Think of it as training wheels for your metabolism.
There is also an important psychological benefit to tapering. Stopping abruptly can feel like jumping off a cliff. The sudden return of hunger creates panic. The panic leads to reactive overeating. The overeating creates guilt. The guilt creates a shame cycle that undermines every maintenance strategy you planned. Tapering converts that cliff into a gradual slope. Each step gives you time to prove to yourself that you can manage at the new level before taking on more. That confidence compounds over the entire tapering period and carries forward into the medication-free maintenance phase.
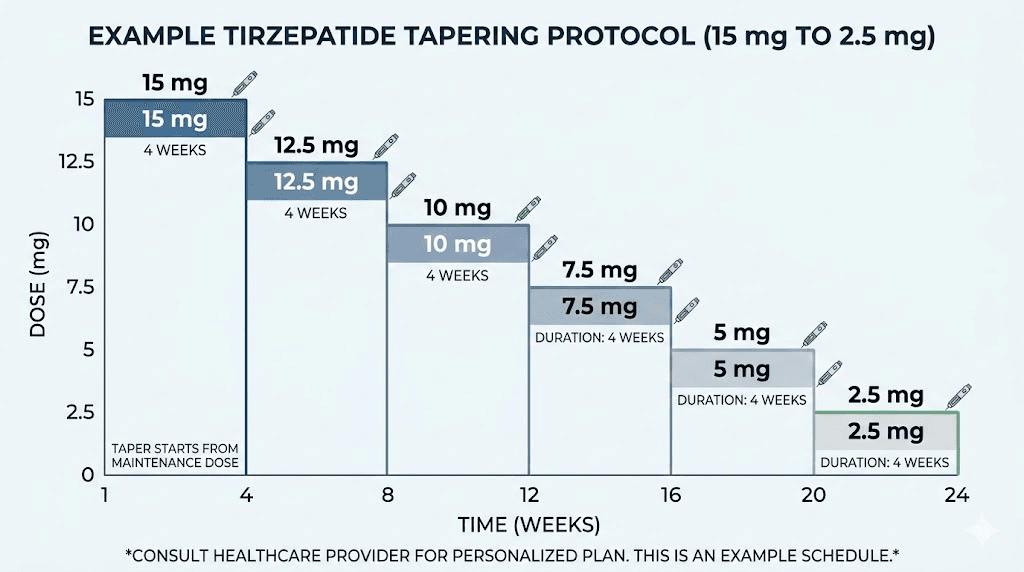
A reasonable tapering protocol looks like this.
If you are currently on 15 mg weekly, reduce to 12.5 mg and hold for four to six weeks. Monitor your hunger levels, energy, and weight stability at this dose. The detailed dosage charts for higher tirzepatide doses can help you understand the conversion if you are using compounded formulations that differ from standard pharmaceutical concentrations.
Once stable at 12.5 mg, step down to 10 mg for another four to six weeks. Again, monitor closely. The 10 mg dosage chart will guide the injection volume for your specific concentration.
From 10 mg, reduce to 7.5 mg. Then to 5 mg. Then to 2.5 mg. Each step lasting four to six weeks depending on how your body responds. This patience is not optional. Rushing through dose reductions undermines the entire purpose of tapering.
At the 2.5 mg level, you might consider an additional micro-tapering phase. The microdosing tirzepatide approach has gained significant interest for this exact purpose. A microdose schedule might involve 1.25 mg weekly, or even 2.5 mg every other week, before full discontinuation. The tirzepatide microdose chart provides detailed guidance on sub-therapeutic dosing levels that can ease the final transition.
Use the compounded tirzepatide dosage calculator to determine exact injection volumes for each tapering step. Getting the math right matters. Underdosing by accident can create unpredictable hunger patterns. Overdosing wastes medication during a phase where cost efficiency matters more than ever.
During the taper, certain monitoring points deserve attention.
Weekly weigh-ins provide objective data. Use the same scale, same time of day, same conditions. Weight fluctuations of one to three pounds between measurements are normal and do not indicate failed maintenance. Look at four-week trends, not daily numbers. Hunger tracking helps identify your personal threshold. Rate your hunger on a simple 1-to-10 scale three times daily. When hunger ratings consistently exceed 7 at a new dose level, consider holding at that dose for an additional two weeks before stepping down further.
The split dosing approach, where you divide your weekly dose into two smaller injections, can help smooth out the peaks and valleys of medication levels during tapering. This keeps blood concentration more stable and may reduce the hunger spikes that occur in the days before your next scheduled injection.
Energy levels matter during tapering. The compound dosage charts can help you fine-tune amounts if you are working with compounded formulations that allow more flexible dosing increments than the standard manufactured tiers.
Blood glucose monitoring is particularly important for anyone with prediabetes or type 2 diabetes. As tirzepatide dose decreases, glucose regulation may shift. Check fasting glucose at each dose level and discuss any significant increases with your prescribing provider. The dosing chart in units and a dosage calculator both help ensure accuracy at every step of the taper.
The total tapering timeline typically ranges from 16 to 30 weeks, depending on your starting dose and how many intermediate steps you include. This is not wasted time. It is an investment in sustainable maintenance that pays dividends for months and years after complete discontinuation.
One common mistake during tapering: reducing the dose and simultaneously relaxing dietary discipline, assuming the medication will still provide sufficient appetite control at the lower level. It will provide some control, but less than before. Each dose reduction requires a corresponding increase in behavioral effort to compensate.
Maintenance dosing: staying on a lower dose
Not everyone needs to stop tirzepatide completely. For many people, the most effective long-term strategy is transitioning from a weight loss dose to a maintenance dose, a lower amount that provides just enough appetite regulation to prevent regain without the full therapeutic intensity.
The concept is straightforward. Instead of stepping down to zero, you find the minimum effective dose that keeps your weight stable and stay there. This approach mirrors how most chronic conditions are managed. Blood pressure medications are not stopped once blood pressure normalizes. The medication continues at whatever dose maintains the target. Obesity treatment is no different.
Research supports this. The SURMOUNT-4 trial demonstrated that continuing tirzepatide after initial weight loss preserved 80% or more of weight reduction in approximately 90% of participants. But that was at full therapeutic doses. Emerging clinical experience suggests that lower doses may provide significant maintenance benefits at substantially reduced cost.
Typical maintenance doses range from 2.5 mg to 7.5 mg weekly, though the optimal level varies between individuals. Someone who achieved their target weight on 15 mg might maintain beautifully at 5 mg. Another person might need 7.5 mg. A third might get by at 2.5 mg. The injection dosage chart helps determine the correct volume for your target maintenance dose.
Finding your maintenance dose requires experimentation. Start by reducing your current dose by one level and observe for four weeks. If weight remains stable and hunger is manageable, reduce again. Continue stepping down until you find the dose where weight begins to creep upward or hunger becomes difficult to manage. Then step back up one level. That is your maintenance dose.
Cost is a legitimate factor in this decision. Lower doses mean fewer milligrams per week, which can substantially reduce monthly expenses. The affordable tirzepatide options and compounded tirzepatide pricing become even more accessible at maintenance dose levels. A 2.5 mg weekly dose costs a fraction of a 15 mg dose from the same source.
Compounded formulations offer particular advantages for maintenance dosing because they allow more flexible dose adjustments. Rather than being locked into manufactured dose tiers, compounded tirzepatide from pharmacies like Empower Pharmacy can be precisely calibrated to your maintenance requirements.
Some people consider switching medication forms during the maintenance phase. Oral tirzepatide is emerging as an alternative to injections, and the comparison between tablets and injections is worth evaluating for long-term convenience. The oral versus injection analysis suggests that bioavailability differs between delivery methods, which affects dosing calculations.
The maintenance approach is not for everyone. Insurance coverage complications, supply issues, personal preference for medication-free living, or pregnancy planning (the tirzepatide and breastfeeding considerations are important here) may all argue for complete discontinuation. But for those who can maintain a low dose indefinitely, the evidence strongly favors continued use over abrupt cessation.
The exercise protocol for weight maintenance
Exercise is the single most powerful tool for maintaining weight loss after stopping tirzepatide. Not casual walking. Not occasional movement. Structured, consistent, progressive exercise that builds and preserves metabolically active tissue.
The S-LiTE trial provides the strongest evidence. In this randomized controlled study, adults who completed a weight loss phase were assigned to one year of either supervised exercise, GLP-1 medication, both combined, or placebo for weight maintenance. One year after all treatments stopped, the exercise group showed the best long-term weight maintenance outcomes.
That finding deserves emphasis.
Exercise outperformed continued GLP-1 medication for sustained weight maintenance after treatment ended. The reason is that exercise creates lasting metabolic adaptations, including increased muscle mass, improved insulin sensitivity, and enhanced mitochondrial function, that persist even without the training stimulus. Medication effects vanish when the medication stops. Exercise effects have longer residual benefits.
The research points to a specific volume. You need 200 to 300 minutes per week of moderate-intensity exercise for weight maintenance. That is 30 to 45 minutes daily. Less than this, and the metabolic protection is insufficient to counteract the biological drive toward regain. But not all exercise is equal for this purpose.
Resistance training is non-negotiable. Weight loss, whether from medication or any other method, inevitably causes some muscle loss along with fat loss. The relationship between weight loss and muscle preservation is one of the most important factors in long-term maintenance. Muscle tissue burns more calories at rest than fat tissue. Every pound of muscle you preserve or build increases your daily energy expenditure without additional effort. A basic resistance training protocol for weight maintenance includes three to four sessions per week targeting all major muscle groups. Compound movements like squats, deadlifts, presses, and rows provide the most metabolic benefit per minute of training. Progressive overload, gradually increasing weight or volume over time, ensures continued adaptation rather than stagnation.
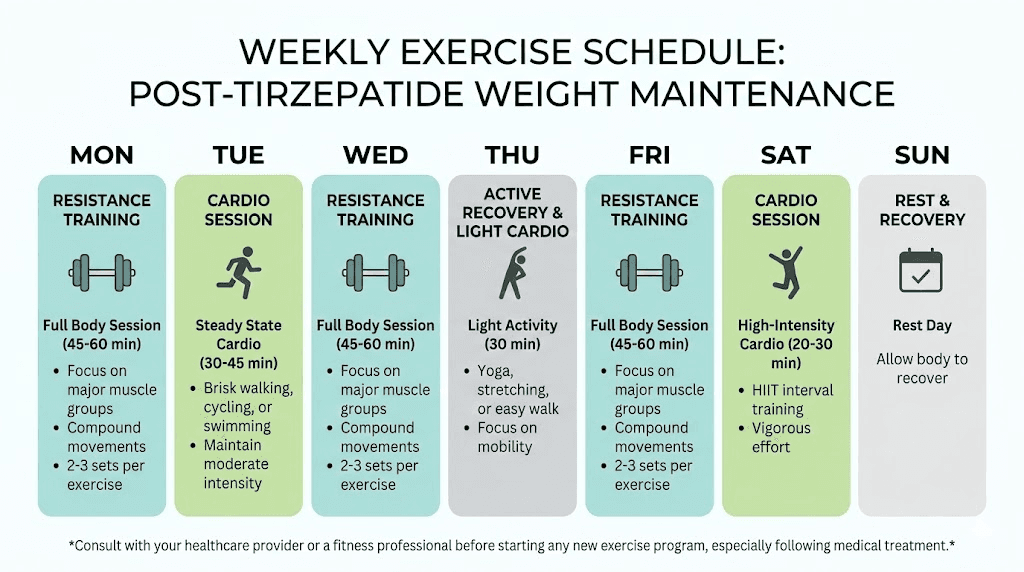
Cardiovascular exercise complements resistance training but does not replace it. The best approaches for sustained fat loss combine both modalities. Two to three cardio sessions per week at moderate intensity, brisk walking, cycling, or swimming at a conversational pace, improve insulin sensitivity and cardiovascular health while burning additional calories.
Here is a practical weekly schedule. Monday: full body resistance training, 45 minutes. Tuesday: moderate cardio such as brisk walking or cycling, 30 to 40 minutes. Wednesday: upper body resistance training, 40 minutes. Thursday: moderate cardio, 30 to 40 minutes. Friday: lower body resistance training, 45 minutes. Saturday: active recreation like hiking, sports, or a longer walk, 60 minutes. Sunday: rest or light stretching. This provides approximately 250 to 300 minutes of total activity with a strong emphasis on muscle preservation.
The timing of exercise initiation matters enormously. Ideally, establish your exercise routine while still on tirzepatide, not after you stop. Building the habit with appetite suppression in place makes it dramatically easier to maintain once hunger returns. The relationship between GLP-1 medications and exercise is synergistic. The medication provides the appetite control while exercise builds the metabolic infrastructure for maintenance.
One critical note: the strategies for targeting visceral fat are particularly relevant during post-tirzepatide maintenance. Visceral fat, the metabolically dangerous fat surrounding organs, tends to return fastest after weight loss. High-intensity interval training and heavy resistance training are the most effective exercise modalities for preventing visceral fat accumulation. The comprehensive guide to fat loss strategies and muscle growth approaches provide additional context for those building a complete post-medication exercise program.
For those concerned about muscle loss specifically, the data is clear. People who lose weight without resistance training lose approximately 25 to 30 percent of their total weight as lean mass. Those who incorporate resistance training reduce that to 10 to 15 percent. Over a 40-pound weight loss, that is the difference between losing 10 to 12 pounds of muscle versus 4 to 6 pounds. The metabolic consequences of that difference compound over months and years, making resistance training arguably the single most important habit for post-medication maintenance.
The fat burning strategies for men and weight management approaches for women both emphasize the critical role of exercise in any sustainable protocol. The athletic performance optimization guide provides additional frameworks for those ready to take their training beyond basic maintenance into performance territory.
Do not skip exercise. It is the foundation upon which every other maintenance strategy builds. Without it, the other strategies in this guide become significantly less effective.
Nutrition strategies that prevent regain
When tirzepatide stops suppressing your appetite, your nutrition strategy becomes the front line of defense. The specific choices you make about what, when, and how much you eat will determine whether you maintain your progress or watch it slip away over the following months.
Protein intake is the single most important nutritional variable. Full stop.
Research shows that higher protein intake, between 1.2 and 1.6 grams per kilogram of body weight per day, provides measurably better weight maintenance outcomes. A landmark study found that increasing protein from 15% to 18% of total energy intake resulted in 50% less weight regain, with the regained weight consisting entirely of fat-free mass rather than body fat. That is a massive difference from a relatively small dietary shift.
For a 175-pound person (approximately 80 kg), this translates to 96 to 128 grams of protein daily. The protein strategies for GLP-1 medication users apply directly to the post-medication maintenance phase as well, and possibly matter even more once the appetite suppression of the medication is gone.
Distribute protein across all meals. Each meal should contain 25 to 40 grams. This maximizes muscle protein synthesis throughout the day and provides sustained satiety between meals. Front-loading protein at each meal, eating it before carbohydrates and fats, further enhances the satiating effect. Specific protein sources matter. Lean meats, fish, eggs, Greek yogurt, cottage cheese, and legumes provide high protein density with manageable calorie loads. The foods recommended during tirzepatide treatment remain excellent choices during the maintenance phase because they are already optimized for satiety and nutritional density.
Fiber is your second nutritional ally. High-fiber foods slow gastric emptying naturally, partially mimicking one of the mechanisms tirzepatide provided pharmacologically. Aim for 25 to 35 grams of fiber daily from vegetables, fruits, whole grains, and legumes. The tirzepatide diet plan provides a solid foundation that you can adapt for the maintenance phase with minor modifications.
Meal structure requires deliberate attention. Without tirzepatide reducing your appetite, the temptation to eat larger portions or add snacks between meals is powerful and constant. Structured eating, with planned meals at consistent times, prevents the gradual caloric creep that drives regain. Three meals and one to two planned snacks per day works well for most people. Each meal should include protein, fiber, and healthy fats. This combination provides the most sustained satiety per calorie consumed. The tirzepatide meal plan can serve as a template that you modify based on your increased appetite.
The foods to avoid on tirzepatide deserve continued avoidance during maintenance. Ultra-processed foods, high-sugar beverages, and calorie-dense snack foods are engineered to override satiety signals. Without the pharmaceutical assistance of tirzepatide, these foods become even more problematic than they were during treatment.
Similarly, the semaglutide diet plan and the recommended food lists for GLP-1 medications provide excellent nutritional frameworks that remain valid after discontinuation. The best foods for GLP-1 users and the foods to avoid during GLP-1 treatment were chosen for their effects on satiety, blood sugar stability, and nutritional density, exactly the qualities that matter for maintenance.
Hydration matters more than most people realize. Dehydration mimics hunger. Drinking 16 ounces of water before each meal reduces caloric intake by 75 to 90 calories per meal according to multiple studies. Over the course of a day, that is 225 to 270 fewer calories without any dietary restriction or deprivation.
Supplements that support tirzepatide users remain relevant during maintenance. A high-quality multivitamin, vitamin D, and omega-3 fatty acids address the most common nutritional gaps. The B12 supplementation guidance is particularly important because GLP-1 medications can affect B12 absorption, and levels may need monitoring even after discontinuation.
The glycine supplementation research is worth noting here as well. Glycine supports sleep quality, which directly affects appetite regulation, and may have independent metabolic benefits during the transition period. Similarly, B12 in its various forms and glycine combinations continue to support metabolic health as your body adjusts to functioning without pharmaceutical support.
Watch for digestive changes during the transition. Constipation during tirzepatide use often improves after discontinuation as gastric motility normalizes. But some people experience a period of looser stools as the gut readjusts to normal transit speed. These changes are temporary and typically resolve within two to four weeks.
A sample day of maintenance eating might look like this. Breakfast: three eggs scrambled with spinach and bell peppers, one slice of whole grain toast, and half an avocado. That delivers approximately 35 grams of protein and 8 grams of fiber. Mid-morning snack: Greek yogurt with a handful of almonds and berries, adding another 20 grams of protein. Lunch: grilled chicken salad with mixed greens, chickpeas, cucumber, tomatoes, olive oil dressing, and a side of quinoa. That is another 40 grams of protein with substantial fiber. Afternoon snack: cottage cheese with celery sticks, adding 15 grams of protein. Dinner: salmon with roasted broccoli, sweet potato, and a side salad. Another 35 grams of protein. Total daily protein: approximately 145 grams. Total fiber: approximately 30 grams. This template keeps you full, fueled, and within a caloric range that supports weight maintenance for most people.
Meal preparation is your secret weapon during the transition period. Without tirzepatide suppressing appetite, the moment you feel hungry and have no prepared food available is the moment poor choices happen. Spending two to three hours on a weekend preparing proteins, vegetables, and grain bases for the week eliminates the decision fatigue that leads to fast food and convenience eating. This is not optional for serious maintenance. It is essential infrastructure.
The fundamental nutrition principle is this: eat as though you are still on a structured weight management protocol, even though the medication is no longer doing part of the work for you. The habits you built during treatment need to become permanent lifestyle practices, not temporary measures that end when the medication does.
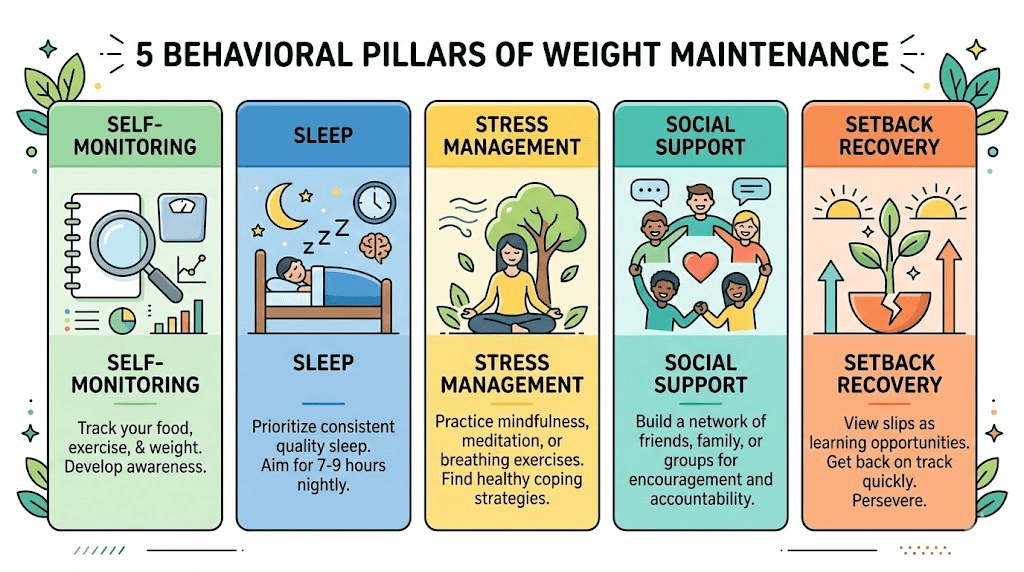
The behavioral toolkit
Biology sets the challenge. Behavior determines the outcome.
The strategies in this section address the psychological and behavioral factors that predict successful long-term weight maintenance after medication discontinuation. These are not soft suggestions. They are evidence-based practices with measurable impact on maintenance success rates.
Self-monitoring is the most consistently validated predictor of weight maintenance success. People who weigh themselves regularly, track food intake, and monitor activity levels maintain significantly more weight loss than those who do not. This is not about obsession. It is about early detection. Weigh yourself two to three times per week under consistent conditions. Morning, after using the bathroom, before eating. Record the numbers. Look at weekly averages, not individual readings. A trend upward of more than two to three pounds sustained over two weeks signals that adjustments are needed, before small gains become large ones.
Food logging does not need to be permanent, but it should be active during the first three to six months after stopping tirzepatide. This is the highest-risk period for regain. Apps that track protein and calorie intake make this manageable without becoming burdensome. After six months, many people develop enough intuitive awareness to maintain without logging, but should resume if weight begins trending upward.
Sleep is a non-negotiable component of your maintenance toolkit. Research consistently shows that inadequate sleep, fewer than seven hours, increases hunger hormones, decreases insulin sensitivity, and impairs decision-making around food choices. Sleep disruptions during tirzepatide use sometimes improve after discontinuation, but the transition itself can temporarily affect sleep quality as neurotransmitter systems readjust.
Target seven to nine hours nightly. Consistent sleep and wake times improve sleep quality more than total duration alone. Avoid screens for 60 minutes before bed. Keep the bedroom cool and dark. These are not minor lifestyle suggestions. Poor sleep actively undermines every other maintenance strategy you implement.
Stress management requires intentional practice. Cortisol, the primary stress hormone, directly promotes fat storage, particularly visceral fat, and increases appetite for calorie-dense foods. Without tirzepatide dampening appetite signals, stress-driven eating becomes a more potent threat than it was during treatment. Find one or two stress management practices that work for you and practice them consistently. Options include meditation, progressive muscle relaxation, time in nature, journaling, or structured breathing exercises. Ten to fifteen minutes daily provides measurable cortisol reduction.
Alcohol deserves specific attention during the maintenance phase. The relationship between tirzepatide and alcohol changes after discontinuation. Many people report that tirzepatide significantly reduced their desire to drink. When the medication stops, alcohol cravings may return. Alcohol provides empty calories, impairs food decision-making, disrupts sleep, and increases cortisol. During the maintenance phase, minimizing alcohol consumption provides outsized benefits relative to the sacrifice. The same applies to those transitioning from other GLP-1 medications, as the alcohol considerations for semaglutide users follow similar patterns.
Social support structures significantly influence maintenance success. Research shows that people with structured support, whether from healthcare providers, support groups, or informed partners, maintain substantially more weight loss than those working alone. SeekPeptides provides community access where members share strategies, track progress, and support each other through transitions like medication discontinuation.
Build accountability into your routine. Regular check-ins with a healthcare provider, a nutritionist, a training partner, or a supportive community keep you engaged and honest about your progress. The fatigue patterns that affect GLP-1 users and the timing strategies that optimize medication effectiveness are just two examples of the detailed, practical knowledge that community support can provide.
Environmental design is an underrated but powerful behavioral tool. Remove trigger foods from your home entirely. Stock your kitchen with the protein-rich, fiber-dense foods that support maintenance. Keep pre-portioned snacks visible and accessible. Place your workout clothes where you see them first thing in the morning. These small environmental modifications reduce the number of decisions you need to make each day, and every decision you eliminate is one less opportunity for the returning appetite to override your intentions.
Plan for setbacks. They will happen. A week of poor eating, a missed exercise period, a stressful life event that disrupts routines, these are inevitable parts of life. The difference between people who maintain long-term and those who regain is not the absence of setbacks. It is the speed of recovery. Having a concrete recovery plan, a specific set of actions you take immediately after a setback, prevents temporary slips from becoming permanent reversals.
Metabolic health monitoring after discontinuation
Stopping tirzepatide does not just affect your weight. It alters multiple metabolic parameters that require monitoring, particularly in the first three to six months after discontinuation.
Blood glucose monitoring is the most urgent priority, especially for anyone with type 2 diabetes, prediabetes, or insulin resistance. Tirzepatide provides powerful glycemic control through both GLP-1 and GIP receptor activation. Removing this control can cause rapid glucose increases that need immediate attention. Check fasting blood glucose at least weekly during the first month after discontinuation. If you were using tirzepatide for type 2 diabetes management, daily monitoring may be necessary. Discuss target ranges and medication adjustments with your prescribing provider before beginning your taper.
Blood pressure often improves during tirzepatide treatment, partly from weight loss and partly from direct vascular effects of the medication. After discontinuation, blood pressure may rise as weight returns and the direct medication effects fade. Monitor blood pressure at least monthly using a home blood pressure monitor for convenient, consistent readings.
Lipid profiles, particularly triglycerides and non-HDL cholesterol, tend to improve substantially during tirzepatide treatment. The SURMOUNT-4 post-hoc analysis showed that these improvements reversed proportionally with weight regain. Get a lipid panel at three months and six months after discontinuation to track any changes that might require intervention.
Hair loss associated with GLP-1 medications is a concern some people experience during rapid weight loss phases. Interestingly, hair shedding sometimes occurs or worsens temporarily after stopping the medication as the body readjusts to a new metabolic state. This is typically telogen effluvium, a reversible condition that resolves within three to six months. Adequate protein intake and appropriate supplementation can minimize this effect.
Gastrointestinal changes are common during the transition period. Constipation that occurred during treatment typically resolves as gastric motility normalizes. But some people experience a temporary period of increased gastrointestinal motility as the gut recalibrates to functioning without GLP-1 receptor stimulation. Dizziness and body aches during the transition are occasionally reported, though these tend to resolve within two to three weeks.
The muscle pain some experience on tirzepatide often improves after discontinuation. Anxiety symptoms and headaches may temporarily increase or decrease depending on individual response, as multiple neurotransmitter systems readjust to functioning without pharmaceutical influence.
Mental health monitoring deserves attention alongside physical metrics. The transition off tirzepatide can affect mood, motivation, and self-image in ways that catch people off guard. The confidence built during successful weight loss can erode quickly when appetite returns and the scale begins moving in the wrong direction. If you notice persistent low mood, loss of motivation, or increasing anxiety about weight and food, these are signals to seek professional support. A therapist experienced in weight management can provide coping strategies that complement your physical health protocols.
Keep a symptom journal during the first eight weeks after discontinuation or dose reduction. Tracking what you experience helps your healthcare provider make informed decisions about whether to restart medication, adjust other treatments, or simply wait for the transition to complete naturally.
The monitoring schedule should look like this: weekly blood glucose and weight checks for the first month, biweekly for months two and three, then monthly thereafter. Blood pressure monthly. Lipid panel at three and six months. Review all results with your healthcare provider at each check-in to catch problems early and adjust strategies as needed.
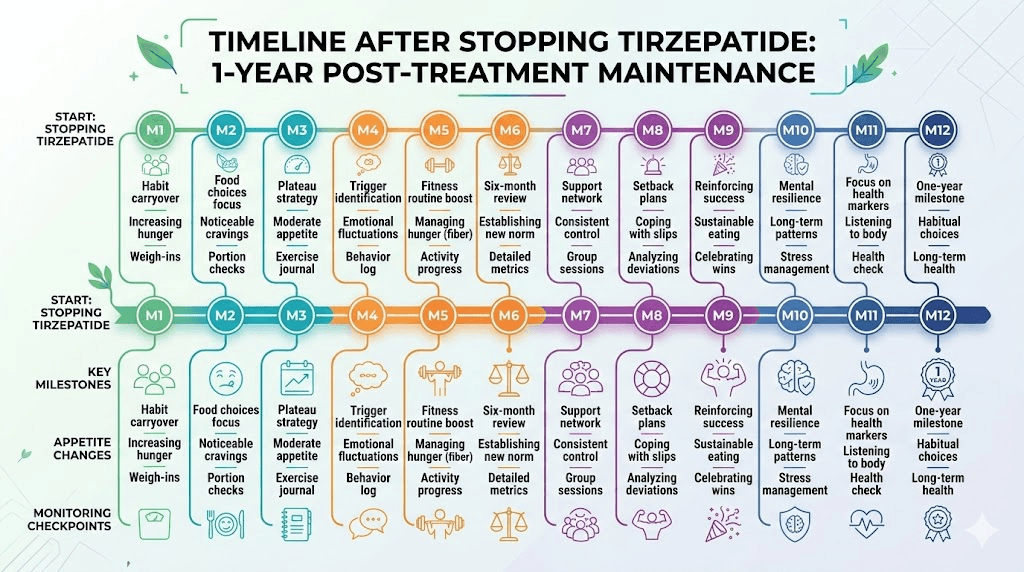
Week-by-week timeline after stopping tirzepatide
Knowing exactly what to expect removes the anxiety and lets you prepare for each phase of the transition. Uncertainty is one of the biggest psychological barriers to successful maintenance. When you do not know whether what you are experiencing is normal, every change feels like failure. This timeline, based on clinical data and reported patient experiences, eliminates that uncertainty and lets you focus on execution rather than worry.
Week 1 to 2: The medication is clearing your system. Tirzepatide has a half-life of approximately five days, meaning it takes roughly 25 days for the drug to be essentially eliminated. During the first two weeks, you still have meaningful medication levels circulating. Appetite may begin increasing slightly, but most people notice relatively little change during this period. This is the time to finalize your exercise, nutrition, and monitoring systems. Use this window wisely.
Week 3 to 4: The transition intensifies. By the end of week three, medication levels have dropped significantly. Most people notice a clear increase in appetite. Meals that previously felt satisfying may leave you wanting more. Food thoughts, the mental preoccupation with eating that tirzepatide suppressed, begin returning. This is normal and expected. It does not mean your plan is failing.
Energy changes are common during this phase. Some people feel more energized as the mild fatigue associated with GLP-1 medications lifts. Others feel less energized as appetite disruption affects meal timing and composition. The energy effects of tirzepatide vary between individuals, and the reversal of those effects is equally variable. Maintaining your exercise routine during this period is critical, even when motivation dips.
Month 2 to 3: The new normal begins forming. Appetite has returned to approximately pre-treatment levels. Gastric emptying has normalized. The metabolic adaptations from weight loss are fully manifesting, meaning your body requires fewer calories than it did at your original weight but your appetite is pushing toward the original intake level. This mismatch creates the pressure that drives regain.
This is the highest-risk period for significant regain. The plateau experiences common with GLP-1 medications have a parallel here. Just as plateaus during treatment require protocol adjustments, the period between stopping medication and finding sustainable equilibrium requires active management and willingness to adjust strategies.
Weight changes of two to five pounds during this period are typical and not necessarily cause for alarm. The body retains water differently as GLP-1 effects diminish, which can cause weight fluctuations that do not reflect actual fat gain. Track the trend over weeks, not days. Any injection site reactions from previous doses have fully resolved by this point.
Month 3 to 6: The critical maintenance window. Research indicates that weight trajectory during this period strongly predicts long-term outcomes. If you have maintained within five to eight percent of your lowest weight by month six, your probability of sustained maintenance increases significantly.
Continue all monitoring. Adjust calorie targets if needed. Increase exercise volume if weight is trending upward. This is where the behavioral toolkit earns its value, because the biological pressure to regain is constant and requires consistent behavioral counterforce that does not waver.
Month 6 to 12: Stabilization or decision point. By this stage, your weight has either stabilized at a sustainable level or the trend toward regain has become clear enough to require a strategic reassessment. If weight has increased by more than 10 to 15 percent of your total loss, this is the time to reassess with your healthcare provider. Options include restarting medication, trying a different medication, adjusting lifestyle strategies, or accepting a new set point that, while higher than your lowest weight, may still represent significant improvement from your starting point. The timeline for GLP-1 medications to take effect when starting is measured in weeks. The timeline for the body to fully adjust to their absence is measured in months. Give yourself that time.
Alternative medications for weight maintenance
If lifestyle strategies alone prove insufficient, several medication options can support weight maintenance after tirzepatide without returning to full therapeutic dosing.
Metformin is the most studied alternative for post-GLP-1 weight maintenance. Originally developed for type 2 diabetes, metformin provides modest weight management benefits through improved insulin sensitivity and reduced hepatic glucose output. At doses of 1500 to 2000 mg daily, it supports weight stability without the appetite suppression of GLP-1 medications. It is inexpensive, widely available, and has decades of safety data supporting long-term use.
Some providers recommend starting metformin during the tirzepatide tapering phase, allowing its effects to establish before GLP-1 activity fully clears. This bridging approach can smooth the metabolic transition and reduce the magnitude of appetite rebound.
Phentermine is another option, though its use is more controversial for maintenance purposes. Compared to GLP-1 medications, phentermine provides appetite suppression through a different mechanism involving norepinephrine release and is typically intended for short-term use. However, some providers prescribe it intermittently during the high-risk post-GLP-1 period. Understanding how phentermine differs from GLP-1 medications is important for informed decision-making about this approach.
The combination of phentermine with tirzepatide has been explored during tapering periods, though evidence remains limited. Similar combinations with semaglutide have been used clinically with mixed results.
Switching between GLP-1 medications is another strategy worth considering. Some people find that transitioning from tirzepatide to semaglutide at a lower equivalent dose provides enough appetite regulation for maintenance at reduced cost. The dose conversion charts and the conversion calculators help determine equivalent dosing between the two medications so you do not lose ground during the transition.
This approach takes advantage of the fact that semaglutide, as a GLP-1 only agonist, may be available at lower cost than tirzepatide while still providing meaningful appetite regulation. The three-way comparison between major GLP-1 options provides detailed analysis of how these medications differ in mechanism, efficacy, side effect profiles, and cost.
Looking ahead, several next-generation medications are in development specifically for weight maintenance scenarios. CagriSema, which combines cagrilintide and semaglutide, is being studied for long-term weight management. Mazdutide and survodutide offer different receptor profiles that may be better suited for maintenance at lower doses. Orforglipron, an oral GLP-1 agonist, could eliminate the need for injections entirely during long-term maintenance.
The retatrutide protocol represents another frontier. As a triple agonist targeting GLP-1, GIP, and glucagon receptors, retatrutide may offer unique metabolic benefits that could be leveraged at maintenance doses for sustained weight control.
Naltrexone-bupropion (brand name Contrave) represents another pharmaceutical option for maintenance. It works through different mechanisms than GLP-1 medications, targeting the reward and motivation circuits of the brain rather than appetite directly. For some people, this complementary mechanism addresses the emotional and reward-driven aspects of eating that resurface after stopping tirzepatide, even if it does not provide the same magnitude of appetite suppression.
The concept of medication cycling is gaining clinical interest as well. Rather than staying on one medication indefinitely, some providers rotate between different weight management medications to reduce tolerance effects and manage costs. This approach lacks formal clinical trial support but reflects a practical reality for patients managing a chronic condition with limited resources and evolving needs.
Whatever medication strategy you consider, discuss it thoroughly with your healthcare provider. The goal is finding the minimum pharmaceutical intervention that, combined with lifestyle strategies, keeps your weight stable and your metabolic health preserved for the long term.
Common mistakes that lead to rapid regain
Understanding what not to do is as valuable as knowing what to do. These are the most common errors that accelerate weight regain after tirzepatide discontinuation.
Mistake 1: Stopping all structure simultaneously. Some people stop tirzepatide and simultaneously abandon the dietary discipline, exercise routine, and monitoring habits they maintained during treatment. This creates a perfect storm of returning appetite plus no behavioral guardrails. The fix is straightforward. Maintain every non-medication strategy you had during treatment. Change one variable at a time, and the variable you are removing is the medication.
Mistake 2: Ignoring early weight increases. A gain of two to three pounds feels insignificant after losing 30 or 40 pounds on tirzepatide. So it gets dismissed. Then it becomes five pounds. Then eight. By the time alarm sets in, reversing the trend requires significant effort. The fix: respond to the first sustained increase. Tighten dietary control, increase exercise, and resume food logging immediately. Early intervention prevents small gains from becoming large ones.
Mistake 3: Relying on motivation instead of systems. Motivation is temporary. It fluctuates with mood, stress, sleep quality, and life circumstances. Systems, including automated habits, environmental design, and scheduled accountability, operate regardless of how you feel on any given day. The troubleshooting approaches for GLP-1 medications emphasize system-based thinking over motivation-based approaches, and the same principle applies with even greater force to maintenance.
Mistake 4: Inadequate protein intake. Without deliberate effort, protein intake naturally decreases as appetite increases and carbohydrate-rich foods become more appealing. This accelerates muscle loss, reduces metabolic rate, and undermines the benefits of exercise. Track protein for the first six months at minimum.
Mistake 5: Skipping resistance training. Cardiovascular exercise gets prioritized because it burns more calories per session. But resistance training preserves the muscle that determines your resting metabolic rate. Losing muscle during the post-medication period creates a metabolic environment that practically guarantees regain regardless of dietary discipline.
Mistake 6: Using food for emotional regulation. Tirzepatide reduces the neurological reward response from eating. When that suppression lifts, the emotional comfort of food returns in full force. Developing alternative coping mechanisms before stopping the medication is essential. If emotional eating was a pattern before tirzepatide, it will be a pattern after unless actively addressed through therapy, mindfulness practices, or other behavioral interventions.
Mistake 7: Poor medication storage during tapering. If you are tapering over months, proper medication storage matters. Understanding reconstitution protocols, refrigeration requirements, and temperature sensitivity ensures you get full potency from every dose during the taper. Using degraded medication means you are getting less appetite suppression than expected, which can throw off your entire tapering timeline and create unpredictable results.
Mistake 8: Comparing yourself to your lowest weight. Your lowest weight on tirzepatide may not be your sustainable weight off tirzepatide. A maintenance weight that is five to ten percent above your lowest medicated weight can still represent a dramatically healthier state than your pre-treatment weight. Setting unrealistic expectations leads to discouragement, which leads to abandoning maintenance efforts entirely. Define success realistically.
Mistake 9: Neglecting the social environment. The people around you influence your eating patterns more than most people realize. If your social circle regularly involves high-calorie restaurant meals, alcohol-centered gatherings, or food-as-entertainment activities, maintaining weight loss becomes exponentially harder without the pharmacological buffer of tirzepatide. This does not mean isolating yourself. It means developing strategies for social situations, like eating protein before events, choosing restaurants with menu transparency, and having non-food social activities in your regular rotation.
Mistake 10: Assuming the transition is temporary. Many people approach post-tirzepatide maintenance as a temporary phase that eventually resolves. They believe appetite will naturally decrease, metabolism will reset, or the body will find a new equilibrium without effort. The research is clear that this is not the case for most people. The metabolic drive to regain weight persists for years after weight loss. Maintenance is not a phase. It is a permanent lifestyle commitment that requires ongoing attention, even if the intensity of effort decreases somewhat over time as habits become more automatic. The troubleshooting guide for when tirzepatide stops working addresses a related mindset issue, the expectation that results should be effortless, that applies equally to the maintenance phase.
When to consider restarting tirzepatide
Sometimes the best strategy is accepting that tirzepatide may need to be a longer-term part of your health management plan. There is no shame in this recognition. Obesity is increasingly understood as a chronic metabolic condition, similar to hypertension or type 2 diabetes, that often requires ongoing pharmaceutical management to maintain remission.
The medical community increasingly supports the idea of long-term pharmacotherapy for obesity management. Just as someone with hypertension would not be expected to maintain normal blood pressure through lifestyle alone after stopping medication, expecting permanent weight maintenance after stopping anti-obesity medication is often unrealistic for patients with significant metabolic dysfunction. This reframing removes stigma and allows for more honest, productive conversations about treatment duration.
Consider restarting tirzepatide if weight has increased by more than 10 to 15 percent of your total loss despite consistent adherence to exercise and nutrition strategies. Consider it if metabolic markers like blood glucose, blood pressure, or lipids have deteriorated to clinically concerning levels. Consider it if quality of life has significantly decreased due to returning symptoms like joint pain, reduced mobility, or sleep apnea. And consider it if the mental and emotional toll of constant hunger management has become unsustainable despite your best behavioral efforts.
Restarting does not mean starting from scratch. Most people regain responsiveness to tirzepatide quickly upon reinitiation, though beginning at the original high dose is not recommended. A gradual re-escalation from 2.5 mg helps minimize gastrointestinal side effects and allows dose optimization. The starting dose guidance applies whether you are new to the medication or returning after a break.
The shelf life and expiration considerations are relevant if you stored medication in anticipation of a potential restart. Check expiration dates and storage conditions before using any previously purchased tirzepatide. The detailed shelf life information can help you determine whether stored medication remains viable.
Future treatment options may make long-term maintenance more accessible and affordable. The pipeline of anti-obesity medications is expanding rapidly. Next-generation combination therapies may offer better maintenance profiles, lower cost oral alternatives like orforglipron could make long-term use more convenient, and maintenance-specific formulations are actively being developed and studied.
SeekPeptides members stay informed about emerging treatments, clinical trial updates, and new strategies as this rapidly evolving field continues to advance. For those navigating the complex decisions around medication continuation, dosing adjustments, and lifestyle optimization, access to current, evidence-based information makes all the difference between informed choices and guesswork.
The decision to restart, continue at a maintenance dose, switch medications, or pursue lifestyle-only maintenance is deeply personal. It depends on your health status, financial resources, quality of life priorities, and risk tolerance. Work with a knowledgeable healthcare provider who understands the full spectrum of available options and can guide you toward the approach that fits your specific situation.
Frequently asked questions
How quickly does appetite return after stopping tirzepatide?
Most people notice significant appetite increases within two to three weeks of their last injection. Tirzepatide has a half-life of approximately five days, so meaningful medication levels persist for about 20 to 25 days. The appetite suppression timeline reverses in roughly the same pattern it originally developed, though the return of hunger often feels more abrupt than the gradual onset of suppression.
Can I combine exercise with other peptides for better maintenance?
Some researchers explore complementary peptides alongside exercise for body composition management during the post-medication period. The AOD-9604 combination research and peptides for weight loss and muscle gain provide detailed context on available options. Always discuss any supplementation with your healthcare provider before beginning a new protocol.
Is there a minimum BMI required to restart tirzepatide?
Clinical guidelines generally recommend GLP-1 medications for adults with a BMI of 30 or greater, or 27 or greater with weight-related complications. The BMI requirements for GLP-1 medications provide detailed information about eligibility criteria and how they apply to medication restarts versus initial prescriptions.
Should I take supplements after stopping tirzepatide?
A high-quality multivitamin, vitamin D, B12, omega-3 fatty acids, and potentially glycine are commonly recommended during the post-medication transition period. The glycine and B12 combination guide and the complete supplements guide provide specific recommendations based on current research.
Can berberine help with weight maintenance after tirzepatide?
Berberine has demonstrated modest effects on blood glucose regulation and lipid metabolism in clinical studies. Some researchers call it a natural metformin. The berberine and GLP-1 interaction research provides relevant information, though evidence for berberine as a standalone weight maintenance tool remains limited compared to pharmaceutical options.
What if I only regain a small amount of weight?
Some weight regain after stopping tirzepatide is expected and clinically acceptable. Research suggests that maintaining at least 75% of your total weight loss represents an excellent long-term outcome. A regain of 5 to 10 percent of your lowest medicated weight may actually be sustainable and healthy, especially if it includes some muscle mass recovery from resistance training.
How does tirzepatide discontinuation differ from stopping semaglutide?
Tirzepatide activates both GLP-1 and GIP receptors, while semaglutide targets only GLP-1. This means tirzepatide discontinuation involves two receptor systems deactivating rather than one. Some clinicians believe this makes the transition more abrupt, though head-to-head discontinuation comparison studies are still limited in the published literature.
Where should I inject during the tapering phase?
Injection site rotation remains important during tapering to ensure consistent absorption. The injection site options for tirzepatide and the GLP-1 injection guide provide detailed instruction on proper technique. Consistent injection technique ensures predictable absorption, which matters significantly when you are managing smaller doses during a taper.
External resources
SURMOUNT-4 Trial: Continued Treatment With Tirzepatide for Maintenance of Weight Reduction (JAMA)
S-LiTE Trial: Healthy Weight Loss Maintenance With Exercise and GLP-1 (PMC)
The Role of Protein in Weight Loss and Maintenance (American Journal of Clinical Nutrition)
NIH National Institute of Diabetes and Digestive and Kidney Diseases: Weight Management
For researchers serious about optimizing their post-tirzepatide maintenance strategy, SeekPeptides offers the most comprehensive resource available. Members access detailed protocol guides, dosing calculators, community support from thousands of experienced researchers, and up-to-date information on emerging maintenance strategies, everything needed to protect the progress you have worked so hard to achieve.
In case I do not see you, good afternoon, good evening, and good night. May your weight stay stable, your appetite stay manageable, and your progress stay permanent.