Feb 25, 2026

Day one, you uncap the pen. You take a breath. You pinch the skin on your abdomen and press the needle in, and for a moment you wonder if anything happened at all. The injection site looks fine. You feel fine. You go about your evening like nothing changed, because honestly, nothing seems different yet. Day two brings a subtle shift, a quiet whisper from somewhere deep in your gut that says you are not quite as hungry as usual. By day three, you sit down to dinner and push your plate away with food still on it, something you have not done in years. By the end of day seven, you step on the scale and see a number that makes you blink twice.
That is the first week on semaglutide for many people. Not dramatic. Not miserable. Just a slow, steady introduction to a medication that works quietly in the background while your brain and body begin recalibrating their relationship with food. But the experience is not identical for everyone. Some people feel nausea within hours. Others notice nothing for days. A few lose several pounds of water weight almost immediately, while others see the scale barely budge.
This guide walks you through every single day of that first week. You will learn exactly what semaglutide does inside your body from the moment it enters your system, what side effects to expect (and which ones should concern you), what to eat, how to handle your injection, and what realistic results actually look like after seven days. Whether you are using a brand name pen or compounded semaglutide, the pharmacology is the same. The molecule does not care about the label. It cares about the receptors it binds to, and those receptors start responding within hours of your very first dose. If you want to understand how fast semaglutide works, you are in the right place. If you want to know whether the discomfort is normal or a red flag, keep reading. And if you simply want a clear, honest picture of what the next seven days will look like, this is the most comprehensive resource you will find.
What happens in your body during the first week on semaglutide
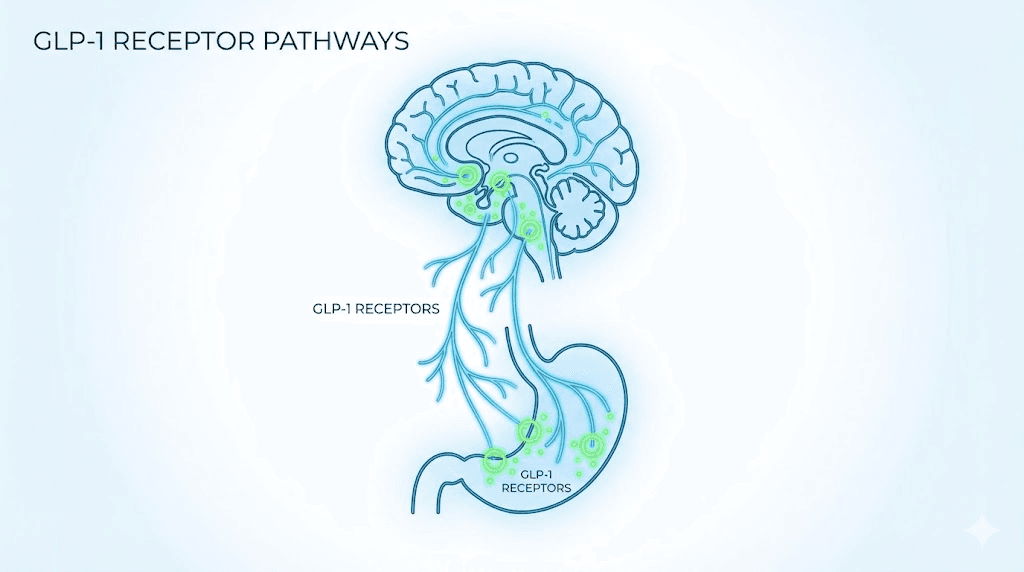
Semaglutide is a GLP-1 receptor agonist. That phrase gets thrown around constantly, but understanding what it actually means changes how you experience your first week. GLP-1 stands for glucagon-like peptide-1, a hormone your gut naturally produces after you eat. It tells your pancreas to release insulin, tells your liver to stop dumping glucose into your blood, and tells your brain that you have had enough food. Semaglutide mimics this hormone, but it does so with a potency and duration that your natural GLP-1 cannot match.
Your body produces GLP-1 in short bursts that last only a few minutes. Semaglutide, by contrast, has a half-life of approximately one week, roughly 168 hours. That means a single injection keeps working for days. The medication reaches peak plasma concentration between one and three days after injection, which explains why most people notice the strongest effects on days two and three rather than immediately after the shot.
Here is what the molecule does once it enters your system. It binds to GLP-1 receptors in the hypothalamus, the region of your brain responsible for hunger signaling, satiety, and food reward.
This is not a stimulant effect. It is not suppressing your appetite through adrenaline or caffeine-like mechanisms. Instead, it fundamentally alters how your brain perceives hunger and fullness. Food still tastes good. You simply do not think about it as often, and when you do eat, you feel satisfied sooner.
Simultaneously, semaglutide slows gastric emptying. Your stomach takes longer to push food into the small intestine, which means you feel physically full for extended periods after meals. This gastric slowing is responsible for many of the digestive side effects people experience during their first week, including nausea, bloating, and constipation. If you are curious about how long it takes semaglutide to suppress appetite, the answer lies in this dual mechanism. The brain effects begin within hours. The gastric effects build over the first few days.
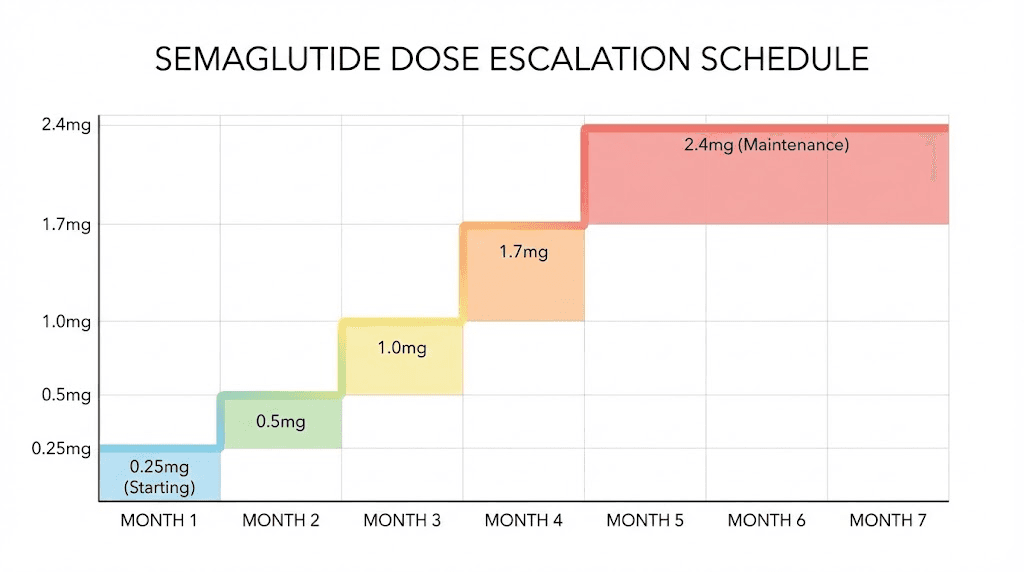
The starting dose of 0.25mg is deliberately low. It is not a therapeutic weight loss dose. It exists solely to let your body acclimate to the medication. Think of it as an introduction, a handshake between the drug and your GLP-1 receptors. At this dose, some people feel pronounced appetite suppression while others notice almost nothing. Both responses are normal.
The standard escalation protocol moves to 0.5mg after four weeks, then to 1mg, 1.7mg, and eventually 2.4mg for weight management.
You can review the full semaglutide dosage in units to understand how these milligram amounts translate to the markings on your syringe. The semaglutide dosage calculator on SeekPeptides can also help you understand your specific concentration and dosing.
One thing to understand about week one specifically: you will not reach steady state. Steady state, where the amount of drug entering your system equals the amount leaving it, takes approximately four to five weeks of consistent weekly dosing. During your first week, you are building from zero. The drug is accumulating in your body for the very first time. This is why week one often feels different from subsequent weeks, and why the side effects can sometimes be more noticeable relative to the benefits.
Your first week on semaglutide day by day
Every person responds to semaglutide on a slightly different timeline. Genetics, body composition, metabolic health, food intake, and even hydration levels all influence how you experience the drug. That said, clinical data and thousands of patient reports reveal consistent patterns across the first seven days. Here is what you can realistically expect.
Day 1 (injection day)
You administer your first injection. If you have never given yourself a shot before, the anticipation is usually worse than the reality. The needle is thin. The injection volume is tiny. Most people describe the sensation as a brief pinch followed by nothing. You can learn the full process in our guide on how to give a semaglutide injection with a syringe.
For the first several hours after your injection, you will likely feel completely normal. This is because semaglutide takes time to absorb from the subcutaneous tissue into your bloodstream. Unlike intravenous medications that hit your system immediately, subcutaneous injections create a slow, sustained release. The medication is working its way into circulation, but it has not yet reached the concentration needed to activate GLP-1 receptors in your brain and gut.
Some people report mild injection site reactions: a small red mark, slight tenderness, or a tiny bump under the skin. These are harmless and typically resolve within a day. Choosing the best injection site for semaglutide can minimize these reactions. The abdomen, thigh, and upper arm are all approved sites, though many providers recommend the abdomen for the most consistent absorption.
Eat normally on day one. Do not preemptively restrict your food intake because you expect the medication to suppress your appetite. It has not had time to do that yet. Drink plenty of water, aim for at least 64 ounces, and eat balanced meals with adequate protein. The question of best time of day to take semaglutide matters here. Many providers suggest morning injections so that if any nausea develops, it occurs during waking hours when you can manage it. Others prefer evening injections so you sleep through any initial discomfort. Either approach works.
Days 2 and 3 (peak concentration)
This is where things get interesting.
Semaglutide reaches peak plasma concentration between 24 and 72 hours after injection. For most people, days two and three represent the window where the medication effects become noticeable for the first time. The most common early sign is a quiet reduction in appetite. You might not feel dramatically different, but you realize at lunch that you forgot to eat breakfast, or you find yourself satisfied after half a sandwich instead of the whole thing.
If nausea is going to appear, it typically shows up during this window. At the 0.25mg starting dose, nausea affects roughly 16% to 20% of users. That means the majority of people do not experience it at all during week one. When it does occur, it tends to be mild, a background queasiness rather than active vomiting. The feeling often worsens if your stomach is completely empty or completely full. Eating small, frequent meals rather than large ones helps considerably. Our detailed guide on whether semaglutide suppresses appetite immediately explains why the timing varies so much between individuals.
You might also notice that certain foods sound unappealing. Greasy, heavy, or very sweet foods are the most common aversions. This is not a conscious choice. Your brain is literally processing food cues differently because of the GLP-1 receptor activation. Many people describe it as a shift in food noise, that constant background chatter about what to eat next, which suddenly gets quieter. Some people notice this shift is dramatic. Others barely perceive it at the starting dose.
Hydration becomes critically important during this window. Semaglutide slows gastric emptying, which can reduce your natural thirst cues. If you are not intentionally drinking water, you may become mildly dehydrated without realizing it. Dehydration amplifies every side effect: nausea feels worse, headaches are more likely, and fatigue deepens. Keep a water bottle with you and sip consistently throughout the day.
Days 4 and 5 (settling in)
By the middle of the week, the initial peak has passed and semaglutide levels begin their slow decline. This does not mean the drug stops working. Remember, the half-life is approximately one week. You still have significant amounts of active medication in your system. But the intensity of side effects often lessens as your body begins adjusting to the presence of the drug.
Many people report that days four and five feel like a new normal. The appetite suppression is present but less dramatic than on days two and three. If you experienced nausea early in the week, it has likely improved or resolved entirely by now. Energy levels, which may have dipped slightly during peak concentration, often stabilize. Some users actually report feeling more energetic than baseline, though this is more common at higher doses. If you are wondering whether semaglutide gives you energy, the answer is complicated. The drug itself is not a stimulant, but the metabolic improvements it triggers can translate to better overall vitality over time.
Digestive patterns may shift during these days. Constipation is common because of the slower gastric transit time. If you are not already eating plenty of fiber and drinking adequate water, now is the time to start. The guide on semaglutide constipation treatment offers specific strategies that work. Some people experience the opposite, loose stools or increased gas, particularly if their diet is high in fat or processed foods.
This is also when you should establish the habits that will carry you through the entire treatment course. Weigh yourself at the same time each day, ideally first thing in the morning after using the bathroom. Track what you eat, not obsessively, but consistently enough to notice patterns. Pay attention to which foods sit well and which ones cause discomfort. These observations become invaluable as your dose increases in the coming weeks.
Days 6 and 7 (approaching your next dose)
The final days before your next injection often reveal how your body processes the medication. Some people notice that appetite begins creeping back as semaglutide levels decline. Others feel no change whatsoever. Both experiences are normal at the starting dose.
If you find that hunger returns strongly on days six and seven, this is useful information. It suggests your body metabolizes the medication relatively quickly, which your provider might consider when adjusting future doses. The duration of effect varies between individuals because of differences in metabolism, body composition, and injection site absorption rates.
Day seven is typically your next injection day if you are following a weekly schedule. Try to inject at approximately the same time each week, though the window is flexible. If you normally inject on Monday mornings but need to shift to Monday evening or even Tuesday morning, that is perfectly acceptable. Consistency matters more than rigid precision. The question of how long it takes semaglutide to work really depends on this accumulation effect. Each weekly dose builds on the last, and the true weight loss benefits typically become apparent over weeks and months, not days.
Common side effects during your first week
Side effects during week one are almost always related to your gastrointestinal system. This makes sense when you understand the mechanism. Semaglutide slows your stomach, changes how your brain processes hunger signals, and alters the speed at which food moves through your digestive tract. Your body needs time to recalibrate. The good news is that most first-week side effects are mild and temporary, resolving as your system adapts to the medication.
Nausea and how to manage it
Nausea is the most discussed side effect of semaglutide, and understandably so. Clinical trials report nausea in 16% to 44% of participants, with the wide range reflecting different doses and study populations. At the 0.25mg starting dose, the incidence sits at the lower end of that range. Most people who experience nausea describe it as mild to moderate, more of an unpleasant awareness than active retching.
The timing matters. Nausea typically peaks when plasma concentrations are highest, roughly 24 to 72 hours after injection. If you inject on a Monday morning, expect the nausea window to fall somewhere between Tuesday morning and Wednesday evening. By Thursday, it has usually improved significantly.
Here are specific strategies that work:
Eat smaller meals more frequently. Five small meals beats three large ones during the first week.
Avoid lying down immediately after eating. Stay upright for at least 30 minutes.
Ginger tea, ginger chews, or ginger capsules can reduce nausea without medication interactions.
Bland foods are your friend. Rice, toast, bananas, and broth sit well in a sensitive stomach.
Avoid cooking strong-smelling foods if odors trigger your nausea.
Stay hydrated. Dehydration makes nausea dramatically worse.
Cold foods (yogurt, smoothies, chilled fruit) tend to be better tolerated than hot meals.
If nausea is severe, your provider may recommend over-the-counter anti-nausea medications.
One pattern that catches people off guard is nausea triggered by eating too fast. Before semaglutide, you could finish a meal in ten minutes. Now your stomach processes food more slowly, and eating at your old pace overwhelms the system. Slow down. Chew thoroughly. Put your fork down between bites. This single habit change eliminates nausea for many first-week users.
Fatigue and low energy
Fatigue during the first week is real, and it has multiple causes. The most obvious one is caloric reduction. If semaglutide suppresses your appetite and you eat significantly less than usual, your body notices the energy deficit. This is especially true if you were consuming 2,500 or more calories daily and suddenly drop to 1,500 without planning for the transition.
But caloric restriction is only part of the picture. Semaglutide itself can cause fatigue through its effects on blood sugar regulation. If your fasting glucose drops lower than your body is accustomed to (even if it drops into a perfectly healthy range), you may feel sluggish until your system adjusts. This is particularly common in people with insulin resistance or prediabetes whose baseline blood sugar ran chronically high. Our comprehensive guide on semaglutide fatigue covers this topic in depth, including strategies for maintaining energy during dose escalation.
The fix is straightforward. Do not skip meals, even if you are not hungry. Eat at least three times per day, focusing on protein and complex carbohydrates that provide sustained energy. If you feel a noticeable energy crash in the afternoon, add a small protein-rich snack. The GLP-1 fatigue complete guide provides additional context on why this medication class can affect energy levels and what you can do about it.
Sleep quality sometimes changes during the first week as well. Some users report difficulty falling asleep or staying asleep, though this is less common than daytime fatigue. If you are curious about whether semaglutide causes insomnia, the research suggests it affects a small percentage of users, typically during dose changes. Maintaining good sleep hygiene, consistent bedtime, cool room, no screens before bed, becomes more important during the adjustment period.
Digestive changes
Your digestive system will notice semaglutide before anything else does.
Constipation affects a significant percentage of users during the first week. The mechanism is simple: semaglutide slows gastric emptying and intestinal transit time, which means food and waste move through your system more slowly. This gives the colon more time to absorb water from stool, resulting in harder, less frequent bowel movements. Increasing fiber intake gradually (not suddenly, which can worsen bloating), drinking more water, and staying physically active all help keep things moving.
Bloating and gas are also common. Your stomach is processing food more slowly, and any food that sits longer in the digestive tract produces more gas. Carbonated beverages make this worse. So do sugar alcohols, which are found in many protein bars and sugar-free products. If bloating bothers you, consider taking a daily walk after meals. The gentle movement stimulates intestinal motility without stressing your system.
Some users experience semaglutide burping, a phenomenon called eructation in medical literature. This sulfur-like burping can be unpleasant but is generally harmless. It results from slowed gastric emptying and can be minimized by eating slowly, avoiding carbonation, and not talking while eating (which causes you to swallow air). The condition typically improves as your body adjusts to the medication over two to four weeks.
Headaches and dizziness
Headaches during the first week almost always trace back to one of two causes: dehydration or blood sugar changes. Both are easily addressed once you know what to look for.
If you are eating less because of appetite suppression but have not increased your water intake, dehydration is the likely culprit. Semaglutide does not directly cause fluid loss, but reduced food intake means you are getting less water from food (which normally contributes 20% to 30% of daily hydration). The solution is simple but requires conscious effort: drink more water than you think you need during week one. You can learn more about the connection between GLP-1 medications and headaches in the GLP-1 headache complete guide.
Semaglutide dizziness tends to occur when standing up quickly, especially if you are slightly dehydrated or have eaten less than usual. This is a form of orthostatic hypotension, where blood pressure drops temporarily when you change positions. Moving slowly when standing, especially first thing in the morning, helps prevent these episodes. If dizziness is persistent or severe, contact your healthcare provider, as it may indicate a more significant blood pressure or blood sugar issue.
Appetite changes
This is the side effect you actually want.
At 0.25mg, appetite suppression ranges from barely noticeable to quite significant, depending on the individual. The most common description is not that hunger disappears entirely, but that it becomes quieter. Food noise, that constant mental loop of thinking about snacks, planning meals, craving specific tastes, fades into the background. You can still eat. Food still tastes good. You just do not feel the same urgency around it.
Some people notice this shift within 24 hours. Others take the full week to perceive any change. And a small percentage notice nothing at all at the starting dose, which is perfectly normal and does not mean the medication will not work for them. The 0.25mg dose is subtherapeutic for weight loss. Its purpose is acclimation, not results. If you are among those who feel little appetite change during week one, the 4 weeks on semaglutide no weight loss article provides reassurance and context. The appetite-suppressing effects become more pronounced at 0.5mg and continue strengthening through higher doses.
One important note: do not interpret reduced appetite as permission to stop eating. Your body still needs nutrients, especially protein. Undereating during the first week sets a dangerous precedent that leads to muscle loss, nutrient deficiencies, and metabolic slowdown over time. Aim for at least 1,200 to 1,500 calories daily as an absolute floor, with most healthcare providers recommending higher targets based on your starting weight and activity level.
What to eat during your first week on semaglutide
Nutrition during week one is not about restriction. It is about adaptation. Your digestive system is adjusting to a new reality, one where food moves through it more slowly and appetite signals have shifted. The foods you choose can either ease this transition or make it significantly more uncomfortable. Many people who report severe nausea or digestive distress during their first week are eating foods that conflict with the medication mechanism, not foods that support it.
Best foods for week one
Protein is your single most important macronutrient during semaglutide treatment, and that priority starts in week one. When you eat less overall (which most people do, even at the starting dose), you need to make every calorie count. Protein preserves lean muscle mass, supports satiety, and prevents the metabolic slowdown that accompanies aggressive calorie restriction. Aim for at least 60 to 80 grams of protein daily, ideally more if your body weight supports it.
Good protein sources for week one include:
Grilled or baked chicken breast (easy to digest, high protein density)
Fish, especially mild varieties like cod, tilapia, or salmon
Eggs, scrambled or hard-boiled for easy digestion
Greek yogurt (also provides probiotics for digestive health)
Cottage cheese
Lean turkey or ground chicken
Protein shakes using whey or plant-based protein, which the protein shakes for GLP-1 guide covers in detail
Complex carbohydrates provide steady energy without spiking blood sugar. Sweet potatoes, brown rice, oatmeal, quinoa, and whole grain bread are all good choices. These foods digest slowly, which complements the gastric slowing effect of semaglutide rather than fighting against it. Avoid refined carbohydrates like white bread, pastries, and sugary cereals, which can cause blood sugar spikes followed by crashes that worsen fatigue.
Vegetables should make up a significant portion of your plate, but choose them wisely during week one. Cooked vegetables are easier to digest than raw ones. Zucchini, spinach, carrots, and green beans sit well in most stomachs. Cruciferous vegetables like broccoli, cauliflower, and Brussels sprouts can increase gas and bloating, so introduce them cautiously. Fruits like bananas, berries, and melon are generally well-tolerated and provide vitamins along with natural sweetness that can satisfy residual cravings.
The best foods to eat on semaglutide guide offers a comprehensive list with specific recommendations for every stage of treatment. For a broader view of meal planning, the list of foods to eat while on semaglutide provides a printable reference you can keep in your kitchen.
Foods to avoid
Certain foods will make your first week considerably more unpleasant. This is not about willpower or discipline. It is about chemistry. Semaglutide changes how your stomach processes food, and some foods simply do not mix well with that new processing speed.
High-fat foods are the biggest offenders. Fried foods, fatty cuts of meat, creamy sauces, and buttery dishes all take longer to digest. When your stomach is already emptying slowly because of semaglutide, adding foods that inherently slow digestion further creates a bottleneck. The result is nausea, bloating, and a heavy, uncomfortable feeling that can last for hours. This does not mean you need to eliminate fat entirely. Healthy fats from avocado, olive oil, nuts, and fatty fish are fine in moderate amounts. The issue is large quantities of saturated or fried fats consumed in a single meal.
Very sugary foods and drinks cause rapid blood sugar spikes that interact poorly with semaglutide effects on insulin secretion. Candy, soda, juice, pastries, and ice cream can trigger nausea and energy crashes. This is especially relevant because many people experience altered taste preferences on semaglutide, finding that foods they previously enjoyed now taste overwhelmingly sweet.
Alcohol deserves special mention. You can read the full analysis in can you drink on semaglutide, but the short answer is that alcohol tolerance often decreases during semaglutide treatment. Drinks hit harder. Hangovers feel worse. And alcohol provides empty calories that work against your goals. During week one specifically, while your body is adjusting to the medication, avoiding alcohol entirely is the safest approach.
Carbonated beverages, including sparkling water, can worsen bloating and burping. Spicy foods may aggravate nausea. Extremely large portions of any food, even healthy food, will overwhelm your slowed digestive system. The foods to avoid on semaglutide article provides a detailed breakdown of every category with alternatives you can substitute.

Sample meal framework for injection day
Injection day matters because you want nutrients in your system before the medication peaks, but you also want to avoid overeating in case nausea develops. Here is a practical framework, not a rigid plan, that works well for most people.
Morning (pre-injection if you inject in the morning):
Light breakfast: scrambled eggs with spinach, or Greek yogurt with berries
8 to 16 ounces of water
Administer injection 30 to 60 minutes after eating
Midday:
Moderate lunch: grilled chicken over rice with cooked vegetables
Keep portions smaller than your pre-semaglutide baseline
Eat slowly over 20 to 30 minutes
Afternoon snack:
Cottage cheese with fruit, or a small protein shake
Continue hydrating throughout the day
Evening:
Light dinner: baked fish with sweet potato and green beans
Finish eating at least 2 to 3 hours before bedtime
Avoid heavy, fatty, or spicy foods at dinner
This framework prioritizes protein at every meal, keeps portions moderate, and avoids the foods most likely to trigger discomfort. If your appetite is significantly reduced and you cannot eat all four meals, prioritize protein-containing meals and skip the snack rather than skipping a meal entirely. The semaglutide diet plan article expands on this framework with multiple meal plan options for different calorie targets and dietary preferences.
Your first semaglutide injection step by step
The first injection is the moment that separates thinking about semaglutide from actually using it. For many people, this is the most anxiety-inducing part of the entire process. The good news is that the injection itself is genuinely simple. The needle is small. The volume is tiny. And the discomfort, if any, is brief.
Choosing and preparing your injection site
You have three approved injection sites for subcutaneous semaglutide administration: the abdomen, the front of the thigh, and the upper arm. Each has advantages and considerations.
The abdomen is the most popular choice. It offers a large, accessible area with consistent subcutaneous fat depth. Inject at least two inches away from your navel, avoiding any area with scars, bruises, or irritation. The abdomen tends to provide the most consistent absorption rates and is the easiest site for self-injection since you can see exactly what you are doing.
The thigh works well for people who prefer not to inject into their midsection. Use the front or outer area of the thigh, avoiding the inner thigh and the area directly above the knee. The thigh has ample subcutaneous tissue in most people and is easy to access.
The upper arm is viable but harder to self-inject because of the angle. Some people have a partner administer injections in this location. If you choose the arm, use the fatty area on the back of the upper arm, between the shoulder and elbow.
Regardless of which site you choose, rotate locations within that area each week. Do not inject into the exact same spot repeatedly. Rotation prevents lipodystrophy, a condition where fat tissue at the injection site becomes hardened or dimpled from repeated needle trauma. The best injection site for semaglutide guide includes diagrams showing specific rotation patterns for each location. For broader context on peptide injection technique, our guide on what is a peptide injection covers the fundamentals and also the guide on where to inject GLP-1.
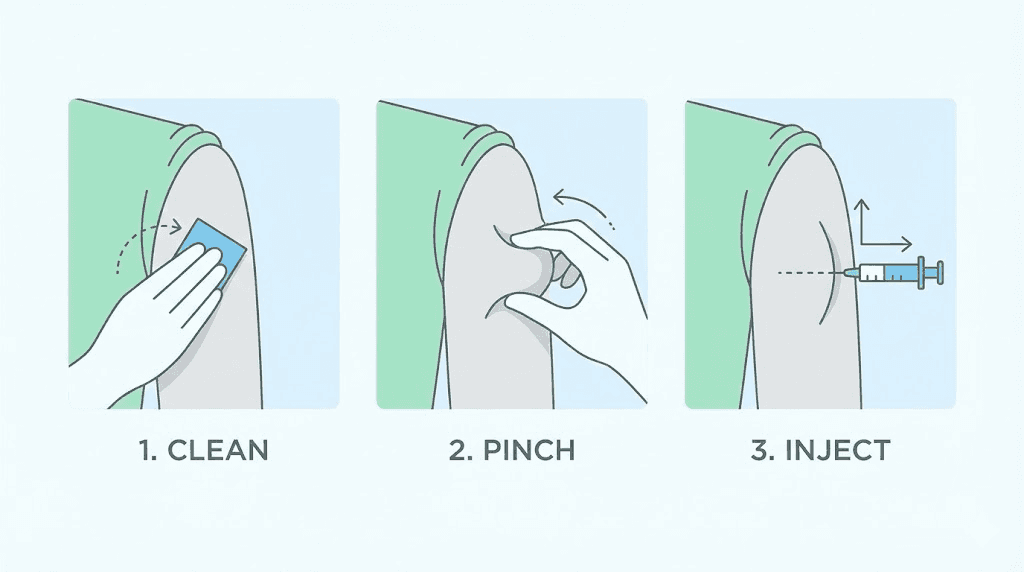
Injection technique
Clean your injection site with an alcohol swab and let it air dry completely. This takes about 30 seconds. Do not blow on it or fan it dry, as this can introduce bacteria.
If you are using a compounded semaglutide vial rather than a pre-filled pen, you will need to draw the medication into an insulin syringe. The how to reconstitute semaglutide guide walks you through the mixing process if your vial requires reconstitution. Understanding semaglutide units to mg conversion is essential for drawing the correct dose. For a 5mg vial specifically, the how to reconstitute 5mg semaglutide article provides step-by-step calculations. The semaglutide reconstitution chart offers a quick visual reference for common vial sizes and water volumes.
Pinch the skin at your injection site between your thumb and forefinger, creating a fold of subcutaneous tissue. Insert the needle at a 90-degree angle (straight in, perpendicular to the skin surface). Push the needle in fully, then depress the plunger slowly and steadily. Hold for 5 to 10 seconds after the plunger reaches the bottom to ensure full delivery of the dose. Remove the needle and release the skin pinch. You may see a tiny drop of blood or medication at the injection site. This is normal.
Do not rub the injection site afterward. Rubbing can increase irritation and potentially affect absorption rates. If there is bleeding, apply gentle pressure with a clean cotton ball or gauze pad for a few seconds. The complete technique is detailed in the how to inject GLP-1 article with photographs and troubleshooting tips.
After the injection
Dispose of your needle properly in a sharps container. Never reuse needles, even for your own injections. Used needles become dull after a single use, which increases pain and infection risk with subsequent injections.
Note the date, time, injection site, and any immediate reactions in a log. This information becomes valuable over the following weeks as you establish patterns. Some people use a simple notebook. Others prefer apps. The method does not matter as long as you track consistently.
Resume normal activities immediately. There are no restrictions on exercise, bathing, or daily tasks after a semaglutide injection. You can shower, swim, or go to the gym right away. The injection site may be slightly tender for a few hours, but this should not limit any activity.
Realistic weight loss expectations for your first week
Let us set honest expectations.
Most people lose between 1 and 5 pounds during their first week on semaglutide. Some lose nothing. A rare few lose more. The number on the scale after seven days tells you almost nothing about how well the medication will work for you long-term, because nearly all first-week weight loss comes from water and reduced food volume rather than fat loss.
Here is why. When you eat less, your body stores less glycogen (the stored form of carbohydrates in your muscles and liver). Each gram of glycogen binds to approximately 3 grams of water. Reduce food intake for a few days, and glycogen stores deplete, releasing bound water. This shows up on the scale as weight loss, but it is water, not fat. It comes back the moment you eat normally for a day or two, which is why people sometimes see a small weight "bounce" early in treatment.
True fat loss at 0.25mg is minimal during week one. The dose is too low and the duration too short for significant fat oxidation to occur. The real fat loss begins as you titrate to higher doses and maintain a consistent caloric deficit over weeks and months. The semaglutide one month results article gives you a more meaningful timeframe for evaluating progress, and the before and after semaglutide guide shows realistic transformation timelines.
What matters more than the scale during week one is how you feel. Are you noticing any appetite changes? Are side effects manageable? Are you able to eat enough protein and stay hydrated? Are you sleeping adequately? These qualitative markers are far more predictive of long-term success than the number on your bathroom scale after seven days.
If you step on the scale after week one and see no change, do not panic. And do not increase your dose without your provider instruction. The article on why you are not losing weight on semaglutide addresses this exact scenario, including what to do about it. Patience during the titration phase pays off. The starting dose is about tolerability, not results.
A useful perspective: clinical trials of semaglutide for weight management show average losses of 15% to 17% of body weight over 68 weeks. That is the trajectory that matters. Week one is a single data point in a months-long journey. Treat it as a baseline measurement, not a verdict on the medication effectiveness.
Exercise and movement during week one
You can and should exercise during your first week on semaglutide. But the intensity and type of exercise may need adjustment based on how you feel.
If you currently have an established exercise routine, continue it with one modification: listen to your body more carefully than usual. If you normally run five miles and feel nauseated at mile two, walk the rest. If you usually lift heavy weights and feel lightheaded between sets, reduce the weight and increase rest periods. The medication is not a contraindication for exercise, but it does change your energy availability and sometimes your blood sugar response during physical activity.
Walking is the single best exercise during week one. It is low-intensity enough to be tolerable even if you feel nauseous, it stimulates intestinal motility (helping with constipation), it improves insulin sensitivity (complementing the medication mechanism), and it burns calories without creating significant stress on your body. Aim for 20 to 30 minutes of walking daily. After meals is an ideal time, as it helps with digestion and blood sugar management.
Resistance training remains important throughout semaglutide treatment. When you lose weight, some portion inevitably comes from muscle mass unless you actively work to prevent it. Strength training two to three times per week signals your body to preserve lean tissue even in a caloric deficit. You do not need to start a new intense program during week one, but if you already lift weights, maintain your routine. If you are new to resistance training, week one is not the time to start a demanding program. Wait until you are comfortable with the medication before adding new physical stressors.
There is growing interest in whether you can lose weight on semaglutide without exercise. The short answer is yes, you can. The medication creates a caloric deficit primarily through appetite suppression. But exercise improves every outcome, from body composition to metabolic health to long-term weight maintenance, and skipping it means leaving results on the table.
Stay hydrated during exercise. This is important normally, and it is critical during semaglutide treatment. Drink water before, during, and after physical activity. If you exercise intensely enough to sweat significantly, consider adding electrolytes to your water. Sodium, potassium, and magnesium all become more important when your overall food intake decreases.
Storage and handling during your first week
Proper storage of semaglutide is not optional. This is a biologic medication, a modified protein that degrades if exposed to improper temperatures, light, or contamination. Getting the storage wrong can render your medication ineffective or unsafe, and you may not realize it until you notice the drug simply is not working.
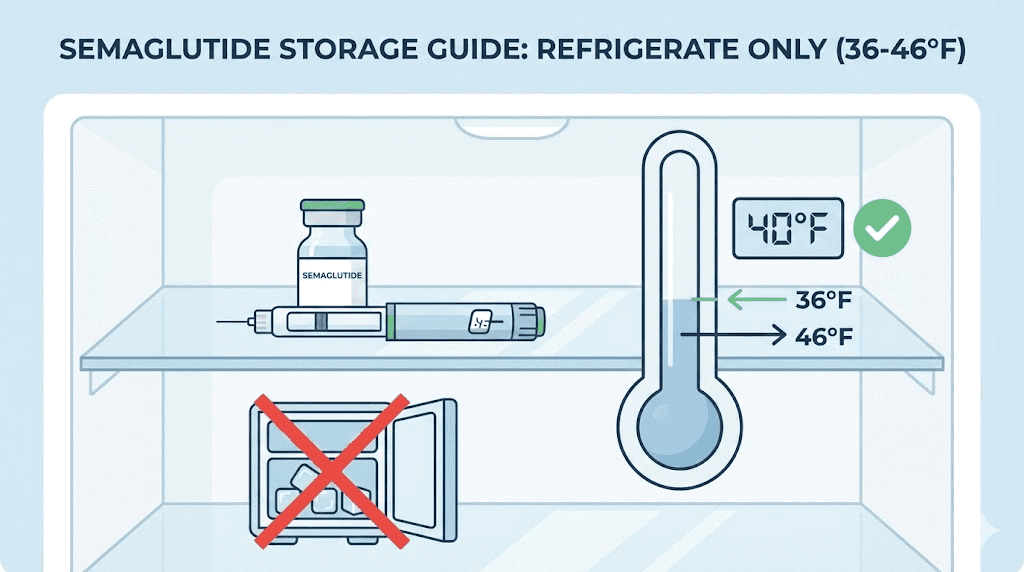
Unopened semaglutide should be stored in a refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). This is the standard refrigerator temperature range. Store the medication in the main body of the fridge, not in the door (where temperature fluctuates with opening and closing) and not against the back wall (where it may freeze). Frozen semaglutide should not be used. Freezing damages the protein structure and can render the medication inactive.
Once you open your vial or pen, it remains usable for a specific period depending on the formulation. Brand name semaglutide pens can be kept at room temperature or refrigerated for up to 56 days after first use. Compounded semaglutide has different stability profiles that vary by pharmacy and formulation, so you should check the labeling from your specific compounder. The articles on how long semaglutide is good for and how long semaglutide lasts in the fridge cover shelf life in detail. For compounded versions specifically, the compounded semaglutide fridge life article addresses common questions about stability.
Does compounded semaglutide need refrigeration? Yes. The compounded semaglutide refrigeration guide explains why temperature control matters even more for compounded formulations, which may not have the same stabilizers as brand name products. The compounded semaglutide expiration article covers what happens when you use product beyond its labeled date.
What if you accidentally leave your semaglutide out overnight? This happens more often than you might think. The accidentally left semaglutide out overnight article provides guidance on whether your medication is still safe to use based on the duration and temperature of exposure. Similarly, if you are curious about what happens if semaglutide gets warm, the answer depends on how warm and for how long.
Visual inspection matters. Before each injection, look at your semaglutide solution. It should be clear and colorless. If you notice cloudiness, particles, discoloration, or any change from its normal appearance, do not use it. The article on what color semaglutide should be helps you identify normal versus abnormal appearances. If your solution appears reddish or pinkish, the why is my semaglutide red article explains possible causes and whether the medication is still safe.
If you need to travel during your first week, planning ahead for medication storage is essential. The travel with semaglutide complete guide covers everything from TSA rules to keeping your medication cold during flights and road trips. A medical-grade cooling case with ice packs is the standard solution for maintaining proper temperature during transport.
For those using compounded semaglutide that requires reconstitution, the mixing process needs to happen before your first injection. Refer to the how to mix peptides with bacteriostatic water guide for general technique, and the specific articles on how much bacteriostatic water to mix with 5mg semaglutide or how much bacteriostatic water to mix with 10mg semaglutide for exact volumes. The semaglutide mixing chart provides a quick reference for common concentrations. Once reconstituted, follow the guidance on how to store peptides after reconstitution to maintain potency.
Common first week mistakes and how to avoid them
Thousands of people start semaglutide every week, and the same mistakes show up over and over again. Avoiding these pitfalls does not just improve your first week experience. It sets the foundation for months of successful treatment.
Mistake 1: Not eating enough. This is the most common and most damaging first-week error. Appetite suppression feels exciting when you have struggled with overeating for years, and the temptation to lean into it aggressively is real. But eating too little during week one leads to fatigue, muscle loss, nutrient deficiencies, and metabolic adaptation that slows weight loss later. Your body needs fuel. Eat at least three meals per day with adequate protein, even if you do not feel hungry. Use the peptide calculator on SeekPeptides to help plan your dosing, and check the semaglutide diet plan for structured meal guidance.
Mistake 2: Expecting dramatic results immediately. The 0.25mg starting dose is not designed for weight loss. It is designed for tolerability. Setting your expectations at this dose means accepting that changes will be subtle, gradual, and primarily focused on acclimation rather than transformation. The real results begin at higher doses and compound over months.
Mistake 3: Taking the wrong dose. This is especially relevant for people using compounded semaglutide with insulin syringes. Confusing units with milligrams is a common and potentially dangerous mistake. The articles on how many units is 0.25mg of semaglutide and the semaglutide dosage chart in units help you convert correctly. For your specific vial concentration, the semaglutide 5mg/ml dosage chart provides the exact syringe markings. Double-check your math before every injection. The compounded semaglutide dose chart also provides visual references for common formulations. If you want to verify your conversion, check whether 20 units of semaglutide equals the mg you expect, or refer to similar conversion guides for 10 units, 40 units, or 50 units.
Mistake 4: Skipping hydration. We have mentioned this multiple times because it is that important. Dehydration amplifies nausea, headaches, fatigue, constipation, and dizziness. It is the single most preventable cause of first-week misery. Carry a water bottle everywhere. Set reminders on your phone if you have to. Aim for at least 80 ounces daily, more if you exercise or live in a warm climate.
Mistake 5: Eating large meals. Your stomach empties more slowly on semaglutide. Eating a large meal on top of a slowly emptying stomach creates a traffic jam. The result is nausea, bloating, and significant discomfort. Shift to smaller, more frequent meals during week one. You will likely find that this pattern feels more natural anyway as your appetite adjusts.
Mistake 6: Not tracking anything. Week one is full of information if you pay attention. Which foods make you nauseous? What time of day do you feel most energetic? How does your appetite change across the week? When do side effects peak? This data shapes your approach for months to come. Track food intake, symptoms, energy levels, and weight in whatever format works for you. The people who have the best long-term results on semaglutide are almost always the ones who tracked carefully during the early weeks.
Mistake 7: Comparing your experience to social media. Someone on the internet lost 10 pounds in their first week. Someone else had zero side effects and felt amazing from day one. Someone else had such severe nausea they could not eat for three days. None of these experiences are your experience. Your body, your dose, your diet, your starting weight, and your metabolism are all unique. Compare yourself to your own baseline, not to strangers online.
When to contact your healthcare provider
Most first-week side effects are mild, expected, and self-limiting. But some symptoms warrant immediate medical attention. Knowing the difference between normal discomfort and a genuine warning sign gives you peace of mind and keeps you safe.
Contact your provider if you experience:
Severe, persistent vomiting that prevents you from keeping down any food or water for more than 24 hours. Mild nausea is normal. Inability to hydrate is not.
Severe abdominal pain that is sharp, stabbing, or localized to one area rather than a general uncomfortable fullness. This could indicate pancreatitis, a rare but serious side effect.
Signs of allergic reaction including hives, facial swelling, difficulty breathing, or rapid heartbeat. Stop taking the medication and seek emergency care immediately.
Significant and persistent dizziness that does not resolve with hydration and eating, especially if accompanied by fainting or near-fainting episodes.
Vision changes that develop after starting the medication, particularly in people with diabetic retinopathy.
Signs of hypoglycemia if you take other diabetes medications, including shakiness, confusion, sweating, and rapid heartbeat. Semaglutide alone rarely causes low blood sugar, but in combination with insulin or sulfonylureas, the risk increases.
Severe injection site reactions with spreading redness, warmth, swelling, or signs of infection.
For symptoms that are uncomfortable but not dangerous, keep a log and discuss them at your next appointment. Your provider can adjust your management strategy, change your injection timing, or offer supportive medications to make the transition easier. Most providers prefer a quick message about concerning symptoms over a patient who suffers in silence.
If you are using compounded semaglutide and notice that your medication looks different from what you expected, reference the can you use expired semaglutide article to assess whether your medication is still viable, or the accidentally took expired semaglutide guide if you realize after the fact that your medication may have been past its use date.
What comes after week one
Week one is the beginning, not the destination. Understanding what lies ahead helps you stay motivated and set appropriate expectations for the coming months.
For the next three weeks, you will remain at the 0.25mg dose. Each weekly injection builds on the last, gradually increasing the amount of semaglutide in your system as you move toward steady state. By week three or four, you will have a much better sense of how the medication affects your appetite, energy, and digestion at this dose level. Side effects that appeared during week one typically diminish over weeks two through four as your body acclimates.
After four weeks at 0.25mg, the standard protocol increases your dose to 0.5mg. This is where many people begin to experience more noticeable appetite suppression and the beginning of meaningful fat loss. The dose escalation continues every four weeks through 1mg, 1.7mg, and potentially up to 2.4mg for weight management. Not everyone needs the highest dose. Your provider will help determine the right maintenance dose based on your response, side effects, and goals. The semaglutide dosing chart in units maps out the full escalation schedule so you know what is coming.
Each dose increase may bring a temporary return of side effects as your body adjusts to the higher concentration. This is normal and follows the same pattern you experienced in week one: symptoms peak during the first few days after the increase and then gradually improve. The semaglutide plateau article addresses what to do if weight loss stalls at any point during your treatment, which is a common and temporary phenomenon that does not necessarily mean the medication has stopped working. Understanding how long you stay on semaglutide for weight loss helps you think about the bigger picture beyond just the first weeks.
Some people explore combination approaches to enhance their results. Adding B12 to semaglutide is a popular option that the semaglutide with B12 complete guide covers thoroughly, and the semaglutide B12 dosage chart provides specific protocols. The semaglutide methylcobalamin guide examines the methylated form of B12 that some providers prefer. Others have looked into semaglutide with glycine for its potential benefits on metabolic health. Some patients also ask about combining phentermine and semaglutide, or want to understand the phentermine vs semaglutide comparison before deciding on a treatment approach.
The question of alternatives often comes up early in treatment. The semaglutide vs tirzepatide comparison is the most common, as tirzepatide offers a dual-agonist mechanism that some people respond to differently. The semaglutide vs tirzepatide side effects article breaks down how the two medications compare in terms of tolerability. For a broader view, the semaglutide vs tirzepatide vs retatrutide guide compares all three major GLP-1 based weight loss medications. If you are considering a switch, the switching from tirzepatide to semaglutide article provides protocol guidance.
Understanding what comes next also means understanding the long game. Semaglutide is not a short-term fix. Research consistently shows that stopping the medication leads to weight regain in the majority of cases, especially if the lifestyle changes made during treatment are not maintained. Think of week one as the beginning of a relationship with a medication that will work alongside your diet, exercise, and behavioral changes to create sustainable results. The semaglutide withdrawal symptoms article covers what to expect if and when you eventually discontinue the medication.
Frequently asked questions
How much weight should I expect to lose in my first week on semaglutide?
Most people lose between 1 and 5 pounds during week one, though some lose nothing. Nearly all first-week weight loss comes from water and reduced food volume rather than actual fat loss. The 0.25mg starting dose is subtherapeutic for weight loss, meaning it is designed for acclimation rather than results. True fat loss begins at higher doses over subsequent weeks. For a broader picture, check out the semaglutide one month results article for a more meaningful evaluation timeline.
Is it normal to feel nothing during the first week?
Absolutely. The 0.25mg starting dose is low enough that many people experience minimal appetite changes and few to no side effects. This does not mean the medication is not working or that it will not work for you at higher doses. Your GLP-1 receptors are being gradually exposed to the drug, and the effects become more pronounced as you titrate upward. The question of how long it takes for GLP-1 to start working is relevant here, as full effects develop over weeks, not days.
What should I do if nausea is severe during week one?
Severe nausea at 0.25mg is uncommon but possible. Switch to smaller, more frequent meals. Avoid fatty, greasy, and spicy foods entirely. Try ginger supplements or ginger tea. Stay hydrated with small, frequent sips of water rather than large gulps. If nausea prevents you from eating or drinking for more than 24 hours, contact your healthcare provider. They may recommend anti-nausea medication or adjustments to your injection timing. The best time to take your GLP-1 shot can influence when nausea peaks.
Can I drink alcohol during my first week on semaglutide?
Technically, there is no absolute contraindication between alcohol and semaglutide. However, most providers recommend avoiding alcohol during the first week while your body adjusts to the medication. Alcohol tolerance often decreases on semaglutide, and drinking can worsen nausea, dehydration, and blood sugar fluctuations. The complete guide to drinking on semaglutide provides a detailed risk assessment.
Does semaglutide affect my period?
Some women report changes to their menstrual cycle after starting semaglutide, including earlier or later periods, changes in flow, or increased cramping. Weight loss itself can affect hormonal balance, and rapid shifts in caloric intake can influence cycle regularity. The semaglutide and menstrual cycle article examines the research and patient reports in detail.
How should I choose between different semaglutide formulations?
Semaglutide is available as brand name injectable pens, compounded injectable formulations, sublingual drops, and oral drops. The choice depends on cost, availability, provider recommendation, and personal preference. The injectable vs oral peptides comparison on SeekPeptides helps you understand the bioavailability differences between delivery methods. If you are exploring compounded options, provider guides like the Empower Pharmacy semaglutide guide, the Olympia semaglutide guide, and the Elevate Health semaglutide guide compare popular compounding pharmacies. The Direct Meds guide and BPI Labs guide offer additional options to consider. For understanding costs across different sources, the how much do peptides cost article provides a broad pricing overview, and the peptide cost calculator helps you compare specific pricing.
Is the starting dose of 0.25mg the same thing as 25 units on my syringe?
Not necessarily. Units and milligrams are different measurements, and the conversion depends entirely on the concentration of your specific semaglutide solution. A 5mg/mL concentration requires a very different number of units to draw 0.25mg than a 2mg/mL concentration. The how many units is 0.25mg of semaglutide article provides conversion tables for common concentrations. Always verify your specific concentration before drawing a dose, and use the semaglutide dosage calculator if you need help with the math. Related conversion guides for other doses include how many units is 1mg, how many units is 1.7mg, and how many units is 2.4mg. You may also want to know whether 20 units of semaglutide is too much or whether 50 units is a lot, which depends entirely on your concentration.
What if I need surgery during my first week?
If you have a scheduled surgery approaching, inform your surgeon and anesthesiologist that you have started semaglutide. The medication slows gastric emptying, which poses aspiration risks during anesthesia. Many surgical guidelines now recommend pausing GLP-1 medications before procedures that require general anesthesia. The when to resume semaglutide after surgery article provides timelines for safely restarting the medication.
External resources
FDA: Medications Containing Semaglutide - Official safety information and approved indications for semaglutide from the U.S. Food and Drug Administration.
STEP 1 Trial (New England Journal of Medicine) - The landmark clinical trial demonstrating semaglutide 2.4mg efficacy for weight management with detailed side effect data.
CDC: Prediabetes and Metabolic Health - Background on metabolic health conditions that semaglutide addresses, including insulin resistance and blood sugar regulation.
Semaglutide Pharmacokinetics (PubMed) - Peer-reviewed pharmacokinetic data on semaglutide absorption, distribution, and half-life relevant to understanding first-week effects.
NIH: Weight Management Resources - Evidence-based weight management information from the National Institute of Diabetes and Digestive and Kidney Diseases.
The first week on semaglutide is a starting point. It is not the finish line, not the dramatic transformation you see on social media, and not a reason to celebrate or despair based on what the scale says after seven days. It is seven days of your body learning to work with a new molecule, seven days of subtle shifts in how you think about food and respond to hunger. The real journey unfolds over weeks and months as you titrate through higher doses and build the habits that support long-term success.
SeekPeptides members access detailed dosing protocols, reconstitution guides, diet plans, and community support designed specifically for people navigating GLP-1 medications. Whether you are figuring out how to convert 100 units of semaglutide to milligrams, looking for the right dosage chart for your concentration, or trying to understand the differences between peptides for fat loss, having accurate information is the difference between a successful treatment course and a frustrating one. Use the peptide reconstitution calculator and peptide stack calculator to support your planning. Learn more about peptides and semaglutide or explore bioactive precision peptides for weight loss to broaden your understanding of the category. The GLP-1 and Ozempic comparison and BMI requirements for GLP-1 articles can help clarify whether this medication class is right for your situation. Your first week is behind you. The progress that matters starts now.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay manageable, your nausea stay mild, and your first week stay the beginning of something remarkable.