Feb 18, 2026

Muscle loss is the quiet problem nobody warned you about.
You started tirzepatide expecting fat to disappear. And it did. The scale moved. Your clothes felt different. But something else was changing too, something you could not see on the scale and might not notice for months. Up to 40% of the weight lost on GLP-1 medications can come from lean tissue. Not fat. Muscle.
That number stopped researchers in their tracks. It stopped clinicians too. Because losing muscle during a weight loss protocol does not just mean looking less toned. It means a slower metabolism going forward. It means reduced strength, impaired mobility, and a higher likelihood of regaining the weight once the medication ends. For older adults, the consequences reach even further, with sarcopenia and falls becoming genuine medical concerns rather than distant possibilities.
This is why glycine entered the conversation. Compounding pharmacies began adding this amino acid to tirzepatide formulations not as a marketing gimmick, not as filler, but as a targeted strategy to address one of the most significant limitations of GLP-1 therapy. Glycine plays a role in collagen production, glutathione synthesis, and the mTOR signaling pathway that tells your body to build and preserve muscle. The question is whether adding it to a compounded injection actually delivers those benefits in meaningful concentrations, or whether the science is still catching up to the clinical hype. SeekPeptides has analyzed the available research, the clinical rationale, and the practical considerations to give you a complete picture. This guide covers everything from the biochemistry of why glycine matters to the specific formulations available, the dosages used, the evidence that exists, and the gaps that remain.
Why muscle loss on tirzepatide matters more than you think
The tirzepatide before and after transformation photos flooding social media tell half the story. The weight comes off. Sometimes dramatically. Clinical trials in the SURPASS series documented average weight reductions of 15-22% of body weight depending on the dose and duration. Those are extraordinary numbers for any weight loss intervention.
But the body composition data tells a different story.
Research published in The Lancet Diabetes and Endocrinology examined what actually happens inside the body during tirzepatide treatment. Approximately 75% of weight lost was fat mass. The remaining 25% was lean mass. That sounds acceptable until you realize what lean mass includes: skeletal muscle, organ tissue, bone mineral content, and water bound to protein structures.
For someone losing 40 pounds, that means roughly 10 pounds of lean tissue. Gone. And while some of that lean mass is water weight that fluctuates naturally, a substantial portion is genuine muscle loss. The implications cascade outward. Resting metabolic rate drops by approximately 15-20 calories per day for every pound of muscle lost. Lose 5 pounds of actual muscle tissue, and your daily caloric needs decrease by 75-100 calories. Over a year, that deficit makes weight regain almost inevitable without permanent dietary restriction or increased activity.
There is a nuance here that deserves attention. Recent imaging studies showed that tirzepatide actually improves muscle quality even as total muscle volume decreases. Fat deposits that infiltrate muscle tissue, a condition called myosteatosis, are reduced significantly. So the muscle that remains is cleaner and more functional than before treatment. That is genuinely encouraging.
Still, the absolute reduction in muscle mass concerns researchers studying long-term outcomes. For someone in their 30s with plenty of muscle reserve, losing some lean tissue during aggressive weight loss might be manageable. For someone in their 50s or 60s already dealing with age-related muscle decline, the math changes entirely.
This is the problem glycine is meant to solve.
What glycine actually does in your body
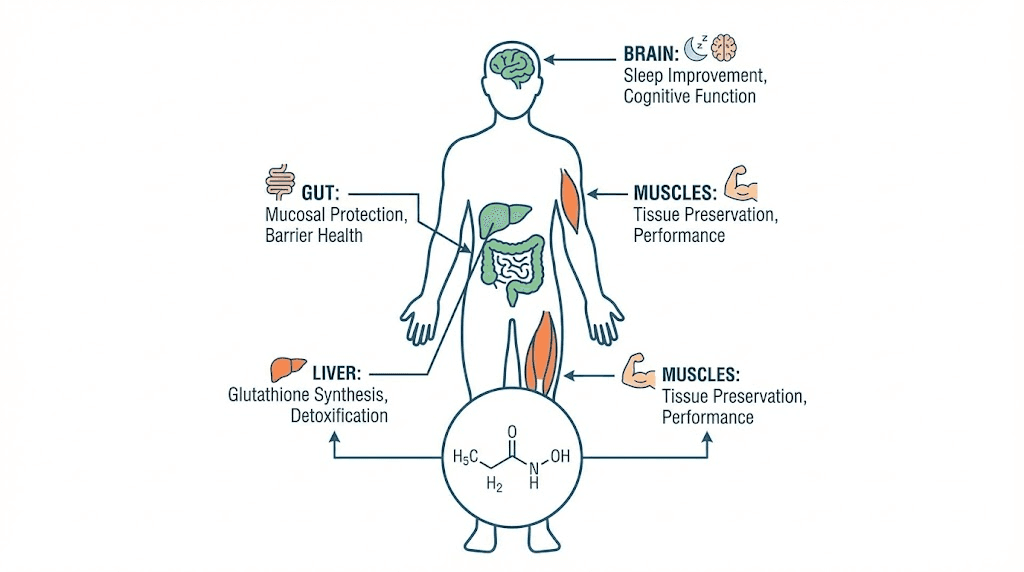
Glycine is the simplest amino acid. It has no side chain, just a hydrogen atom where other amino acids carry complex chemical groups. That simplicity is deceptive. Glycine participates in more metabolic pathways than almost any other amino acid, and its roles are not minor footnotes in biochemistry textbooks. They are central to human physiology.
Three functions matter most when discussing tirzepatide combinations.
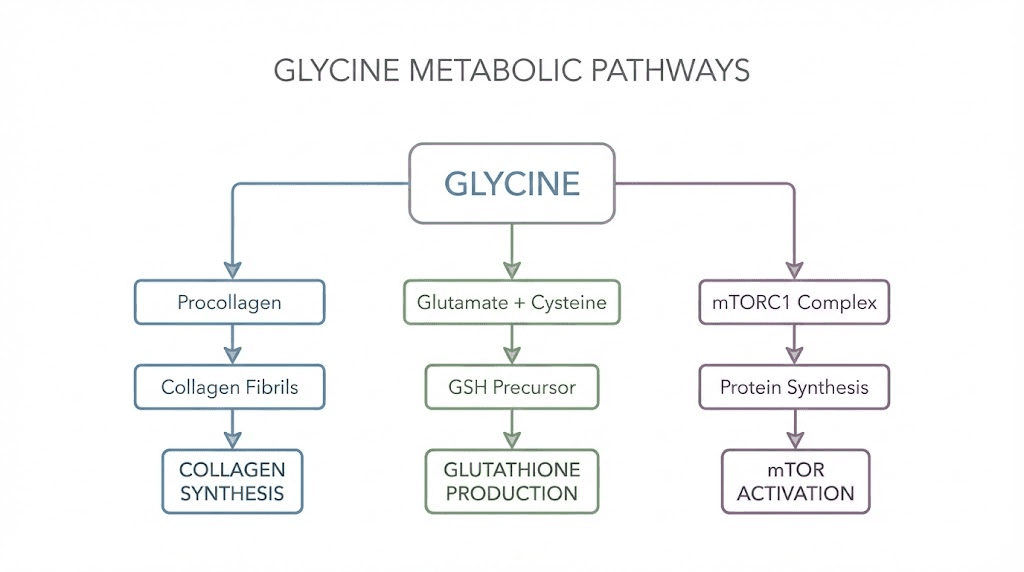
Collagen synthesis and structural support
Roughly one-third of all collagen in the human body is glycine. Every third position in the collagen triple helix must be glycine because it is the only amino acid small enough to fit in the interior of the helix. Without adequate glycine, collagen production falters. Tendons weaken. Cartilage degrades faster. Skin loses elasticity. And critically for our discussion, the extracellular matrix surrounding muscle fibers becomes compromised.
Muscle does not exist in isolation. Each muscle fiber sits within a scaffold of connective tissue that transmits force, provides structural integrity, and facilitates repair after damage. Glycine is essential to maintaining that scaffold. When you lose weight rapidly, and caloric restriction is severe, collagen turnover accelerates while collagen synthesis may lag behind. Supplementing glycine during this period provides the raw material to maintain connective tissue integrity even as the body catabolizes stored energy.
Glutathione production and oxidative defense
Glycine is one of three amino acids required to produce glutathione, your body's master antioxidant. The other two are cysteine and glutamic acid. Research from Baylor College of Medicine demonstrated that glycine supplementation combined with N-acetyl cysteine restored glutathione levels in older adults to levels comparable with young, healthy subjects.
Why does this matter for tirzepatide users? Rapid weight loss generates oxidative stress. Fat cells releasing their stored contents flood the bloodstream with lipid metabolites and inflammatory mediators. The liver works harder to process these compounds. Fatigue increases. Cellular damage accumulates if antioxidant defenses cannot keep pace.
Glutathione is the body's primary defense against this oxidative cascade. And glycine is often the rate-limiting factor in glutathione synthesis, meaning your body has enough cysteine and glutamic acid but not enough glycine to produce all the glutathione it needs. Supplementing glycine removes that bottleneck.
mTOR signaling and muscle protein synthesis
The mechanistic target of rapamycin, mTOR, is the master switch for muscle building. When mTOR is activated, the body synthesizes new muscle protein. When it is suppressed, muscle breakdown predominates. Caloric restriction suppresses mTOR. That is one reason why dieting without resistance training almost always leads to muscle loss.
Glycine activates mTOR signaling through a pathway separate from leucine and other branched-chain amino acids. This means glycine can stimulate muscle protein synthesis through a mechanism that complements, rather than duplicates, the effects of dietary protein. For someone on tirzepatide who struggles to consume adequate protein because of appetite suppression, this alternative pathway for muscle preservation becomes increasingly important.
Animal studies paint a compelling picture. Mice given glycine during caloric restriction lost 14% more fat mass and 27% less lean mass compared to controls. Their quadriceps muscle mass was preserved to a significantly greater degree. These are rodent studies, and translation to humans always requires caution. But the mechanisms are conserved across species, and the effect sizes are large enough to warrant serious attention.
How compounding pharmacies formulate tirzepatide with glycine
Compounding pharmacies do not simply mix glycine into a tirzepatide vial and call it done. The formulation process requires careful consideration of stability, pH, sterility, and bioavailability. Understanding how these formulations are created helps you evaluate what you are actually getting.
The formulation rationale
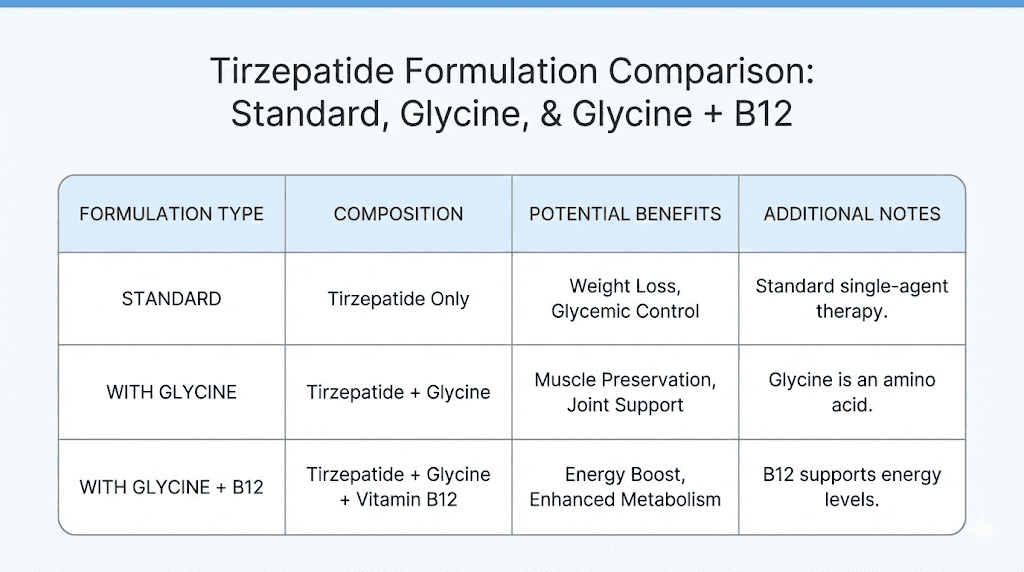
Standard brand-name tirzepatide, sold as Mounjaro and Zepbound, contains tirzepatide as the active ingredient along with excipients like sodium phosphate dibasic heptahydrate, sodium chloride, and hydrochloric acid for pH adjustment. There is no glycine in the commercial formulation.
Compounded tirzepatide formulations differ from manufacturer to manufacturer, but the glycine-containing versions typically include tirzepatide at various concentrations, glycine at doses ranging from 5mg to 30mg per injection, and sometimes vitamin B12 (cyanocobalamin) at 1,000-2,000mcg. Some pharmacies offer tirzepatide with glycine alone. Others combine all three into a tirzepatide, glycine, and B12 triple compound.
The glycine serves multiple purposes in the formulation beyond its metabolic benefits. As a buffer, glycine helps stabilize the pH of the solution, which can extend shelf life and reduce degradation of the peptide. As an osmolality adjuster, it makes the injection more comfortable by bringing the solution closer to physiological tonicity. And as an active ingredient, it delivers glycine directly into the subcutaneous tissue where it can be absorbed systemically.
Available formulation types
Three primary formulation approaches exist in the compounding space:
Tirzepatide with glycine (injectable): The most common formulation. Tirzepatide is reconstituted or prepared as a solution with glycine dissolved in the same vehicle. This is administered as a single subcutaneous injection. Concentrations vary, but typical ranges include 5-60mg of tirzepatide per vial with 5-30mg of glycine.
Tirzepatide with glycine and B12 (injectable): This adds cyanocobalamin or methylcobalamin to the glycine formulation. The B12 component is included primarily to address nausea, a common side effect of GLP-1 medications, and to support energy levels during caloric restriction. This is the most popular compounded formulation for weight management protocols.
Tirzepatide with glycine (sublingual or oral): Less common but emerging. Sublingual formulations dissolve under the tongue and bypass first-pass liver metabolism to some degree. The glycine in these preparations may serve both as a stabilizer and as a bioavailability enhancer, though evidence for improved oral bioavailability of tirzepatide through glycine co-administration is limited.
Quality considerations
Not all compounded formulations are equal. Reputable compounding pharmacies conduct potency testing, sterility testing, and endotoxin testing on each batch. They use pharmaceutical-grade glycine rather than food-grade supplements. They maintain beyond-use dating based on actual stability studies rather than arbitrary timelines.
When evaluating a compounded tirzepatide with glycine formulation, the questions worth asking include: Is the pharmacy 503A or 503B registered? What testing does each batch undergo? What is the beyond-use date, and what stability data supports it? Is the glycine pharmaceutical grade? What is the actual glycine content per injection in milligrams?
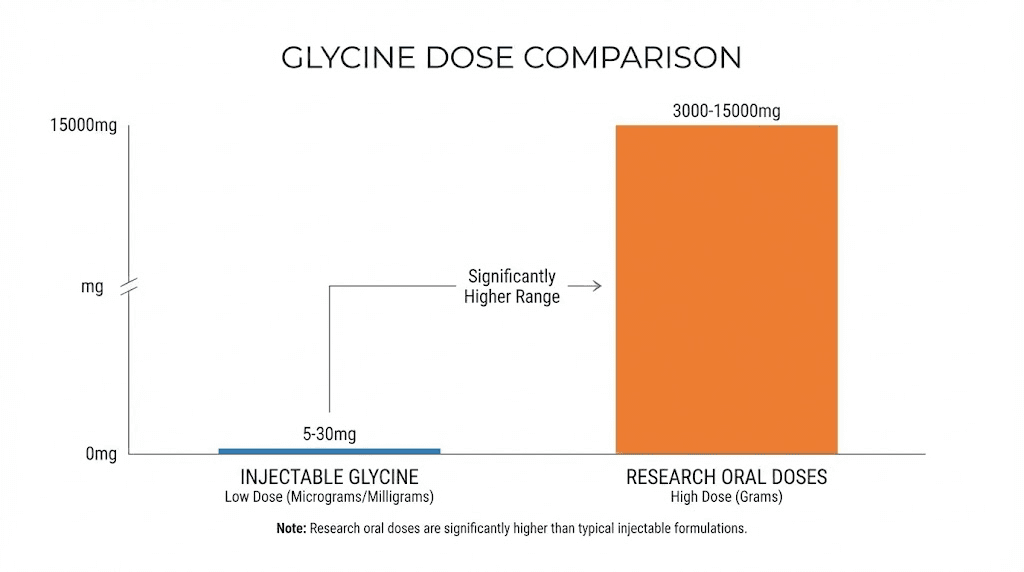
These questions matter because the glycine dose in most compounded injections is relatively small, often 5-30mg per dose. Compare that to the oral glycine doses used in clinical research, which typically range from 3,000-5,000mg (3-5 grams) per day. The gap between what is in the injection and what research suggests is therapeutically meaningful is substantial. We will address this discrepancy in detail later.
Tirzepatide with glycine versus tirzepatide with niacinamide
Glycine is not the only additive compounding pharmacies use. Niacinamide (vitamin B3) is the other major option, particularly from pharmacies like Empower Pharmacy. Understanding the differences helps you determine which formulation aligns with your priorities.
Different mechanisms, different goals
Glycine targets muscle preservation, collagen support, and antioxidant defense. Its primary value proposition in a tirzepatide formulation is protecting lean tissue during aggressive weight loss.
Niacinamide targets cellular energy production, NAD+ biosynthesis, and skin health. Its primary value proposition is supporting metabolic function and potentially reducing the fatigue and skin changes that some tirzepatide users experience.
Neither additive has robust clinical trial data specifically validating its inclusion in tirzepatide formulations. Both have extensive standalone research supporting their individual benefits. The question of which is better depends entirely on what you are trying to optimize.
Head-to-head comparison
Factor | Tirzepatide with glycine | Tirzepatide with niacinamide |
|---|---|---|
Primary benefit | Muscle preservation during weight loss | Cellular energy and NAD+ support |
Secondary benefits | Collagen support, glutathione production, injection comfort | Skin health, metabolic function, DNA repair |
Evidence strength | Moderate (glycine research strong, combination data limited) | Moderate (niacinamide research strong, combination data limited) |
Common dose per injection | 5-30mg glycine | 10-50mg niacinamide |
Best for | Those concerned about muscle loss, older adults, active individuals | Those experiencing fatigue, skin changes, or energy decline |
Side effect profile | Generally well-tolerated | May cause flushing at higher doses |
For individuals prioritizing body composition, particularly those engaged in resistance training alongside weight loss, the glycine formulation makes more theoretical sense. For individuals whose primary concerns are energy levels and overall metabolic support, niacinamide may be more relevant.
Some clinicians recommend oral glycine supplementation (3-5 grams daily) alongside a tirzepatide-niacinamide injection to capture the benefits of both additives. This approach separates the delivery of glycine from the injection, allowing for therapeutically meaningful doses that cannot be achieved in a small-volume subcutaneous injection.
The dosage question: is there enough glycine in the injection?
This is the question that separates marketing from science. And it deserves a blunt, honest answer.
Most compounded tirzepatide with glycine injections contain between 5 and 30 milligrams of glycine per dose. The clinical research on glycine supplementation for muscle preservation, insulin sensitivity, and glutathione production uses doses of 3,000 to 15,000 milligrams per day. That is a difference of 100-fold to 3,000-fold.
Let that sink in.
The mouse study showing preserved muscle mass during caloric restriction used glycine at 1 gram per kilogram of body weight per day. Scaled to a 75kg human (and rodent-to-human scaling is imperfect), that would suggest doses in the multi-gram range. The sleep studies showing improved sleep quality used 3 grams before bed. The glutathione restoration studies used 1.33 millimoles per kilogram per day, which translates to approximately 7-8 grams daily for an average adult.
Five to thirty milligrams is not in the same universe as these research doses.
Does this mean the glycine in compounded injections is useless? Not necessarily. There are arguments on both sides.
The case for injectable glycine at low doses
Subcutaneous injection bypasses the digestive system entirely. When you swallow glycine, it must survive stomach acid, get absorbed through the intestinal wall, pass through the liver (first-pass metabolism), and reach systemic circulation. Bioavailability after oral administration is roughly 30-40% for amino acids. A 3-gram oral dose might deliver 1-1.2 grams to the bloodstream.
A 30mg subcutaneous injection delivers 30mg directly to the tissue with near-100% bioavailability. That 30mg bypasses all the losses associated with oral administration. Is 30mg with 100% bioavailability equivalent to a much larger oral dose in terms of local tissue effects? Possibly, at the injection site and surrounding tissue. But for systemic effects like muscle preservation throughout the body or glutathione production in the liver? Almost certainly not.
The case against injectable glycine at low doses
Glycine is not a drug with nanogram-level potency. It is a common dietary amino acid that your body produces endogenously (roughly 3 grams per day) and that you consume through food (roughly 2-5 grams per day through normal dietary protein). Your body already has grams of glycine in circulation. Adding 5-30 milligrams via injection is like adding a teaspoon of water to a swimming pool.
For glycine to meaningfully shift the balance toward muscle preservation, glutathione production, or improved body composition, the available evidence strongly suggests you need gram-level doses. The injection amount is too small to achieve the systemic effects that the marketing materials imply.
The practical conclusion
The glycine in compounded tirzepatide injections likely provides formulation benefits: pH buffering, improved stability, and possibly reduced injection site discomfort. These are legitimate pharmaceutical benefits. But if your goal is muscle preservation during weight loss, relying solely on the glycine in your injection is not a sound strategy.
Oral glycine supplementation at 3-5 grams per day, taken separately from the injection, is the evidence-based approach to achieving the muscle-preserving, glutathione-boosting, insulin-sensitizing effects that glycine research supports. Think of the injectable glycine as a formulation enhancer and the oral glycine as the therapeutic dose.
Research on glycine for muscle preservation during weight loss
The scientific literature on glycine and muscle preservation is more developed than most people realize. While no randomized controlled trial has specifically tested tirzepatide combined with glycine against tirzepatide alone, the individual components have meaningful evidence behind them.
Animal studies on glycine during caloric restriction
A study published in Clinical Nutrition examined the effects of glycine supplementation during caloric restriction in obese mice. The researchers placed mice on a 40% caloric deficit for 20 days, with one group receiving glycine supplementation and the other receiving alanine as a control amino acid.
The results were striking. Glycine-supplemented mice lost significantly more whole-body fat mass (14% more than controls) while losing significantly less lean mass (27% less than controls). Quadriceps muscle mass was preserved to a statistically significant degree (4% better preservation, p less than 0.01). The glycine group also showed better insulin sensitivity markers and reduced inflammatory markers compared to controls.
These findings are particularly relevant for tirzepatide users because the study modeled exactly the scenario they face: aggressive caloric restriction (since tirzepatide dramatically reduces food intake through appetite suppression) with the risk of concurrent muscle loss.
Human studies on glycine and metabolic function
Human research on glycine supplementation paints a more complex picture. A study published in Scientific Reports in early 2025 examined glycine supplementation in individuals with severe obesity and found that glycine did not significantly change HbA1c, fasting glucose, fasting insulin, or measures of insulin resistance. This contradicts earlier studies suggesting glycine improves insulin sensitivity in healthy individuals and those at risk for diabetes.
The discrepancy may relate to dosing, duration, or the metabolic complexity of severe obesity compared to milder metabolic dysfunction. It does, however, inject important nuance into the conversation. Glycine is not a metabolic magic bullet, and its effects may depend heavily on the population being studied.
What the human research does consistently show is that glycine supplementation at 3-5 grams daily:
Improves sleep quality, which supports recovery and hormonal balance during weight loss. Restores glutathione levels, particularly in older adults with depleted antioxidant reserves. Reduces markers of systemic inflammation. Supports collagen synthesis and connective tissue health. Is exceptionally well-tolerated with minimal side effects even at doses up to 15 grams per day.
The gap in the evidence
The gap is obvious and important: no human clinical trial has specifically examined whether adding glycine to a tirzepatide regimen improves body composition outcomes compared to tirzepatide alone. The mechanistic rationale is strong. The animal data is encouraging. The individual human glycine studies are generally positive. But the specific combination has not been tested in a rigorous, controlled manner.
This does not mean the combination is ineffective. It means the evidence is preliminary. It means we are extrapolating from multiple lines of evidence rather than relying on direct proof. That is a common situation in medicine, particularly with compounded formulations, and it requires honest communication about what we know and what we are still learning.
Glycine and tirzepatide side effect management
Side effects from tirzepatide are common, particularly during dose escalation. Nausea affects roughly 20-30% of users. Vomiting, constipation, diarrhea, and abdominal discomfort are also frequently reported. The question of whether glycine helps manage these side effects has practical significance.
Glycine and gastrointestinal comfort
Glycine has cytoprotective properties in the gastrointestinal tract. It reduces gastric acid secretion, protects against mucosal damage, and has anti-inflammatory effects in the gut lining. These properties are well-established in gastroenterology research, separate from any tirzepatide context.
Whether the small amounts of glycine in compounded injections provide meaningful GI protection is debatable. But oral glycine supplementation, particularly at 3 grams taken with meals, has shown benefit for various forms of digestive discomfort. For tirzepatide users struggling with GI side effects, this represents a low-risk intervention worth trying.
Some clinicians report that patients using glycine-containing tirzepatide formulations report less nausea than those on standard formulations. However, this is anecdotal and could reflect placebo effects, differences in pharmacy quality, or the confounding effect of B12 (which is frequently included alongside glycine and has its own anti-nausea properties).
Glycine and injection site reactions
Injection site pain, redness, and swelling are occasional complaints with tirzepatide. Glycine, as a buffering agent in the formulation, can reduce the pH-related irritation that causes some of these reactions. This is a formulation benefit rather than a therapeutic one, but it matters for patient comfort and adherence.
A solution buffered with glycine tends to be closer to physiological pH (7.35-7.45) than an unbuffered peptide solution, which can be more acidic. Less acidity at the injection site means less tissue irritation, less pain during injection, and potentially less post-injection redness.
Glycine and sleep quality during tirzepatide therapy
Sleep disruption is an underreported issue during GLP-1 therapy. Some users report difficulty sleeping, changes in sleep architecture, or increased wakefulness during the night. The mechanisms are not fully understood but may relate to changes in blood sugar regulation during sleep, altered energy metabolism, or the direct effects of GLP-1 receptor activation on brain regions involved in sleep.
Glycine at 3 grams before bedtime has been shown in multiple human studies to improve subjective sleep quality, reduce time to fall asleep, and improve next-day cognitive performance. The mechanism involves glycine lowering core body temperature through peripheral vasodilation and acting on NMDA receptors in the suprachiasmatic nucleus, the brain's master clock.
For tirzepatide users experiencing sleep issues, oral glycine supplementation before bed is one of the most evidence-based, low-risk interventions available. This benefit alone may justify adding glycine to the protocol, regardless of the muscle preservation question.
How to optimize glycine intake alongside tirzepatide
If you are using tirzepatide and want to maximize glycine's potential benefits, the strategy involves more than just choosing a glycine-containing formulation. It requires a comprehensive approach to amino acid intake that accounts for the reduced food consumption typical of GLP-1 therapy.
Oral supplementation protocol
The research supports 3-5 grams of glycine daily for general health benefits. For individuals on tirzepatide specifically targeting muscle preservation, some clinicians recommend up to 10 grams daily, split into two or three doses.
Morning dose (3 grams): Taken with breakfast or your first meal. Glycine absorbs rapidly on an empty stomach but can also be taken with food. This dose supports daytime collagen synthesis, glutathione production, and insulin sensitivity.
Evening dose (3 grams): Taken 30-60 minutes before bed. This targets the sleep-improving effects documented in clinical research. Better sleep means better recovery, improved growth hormone secretion during deep sleep phases, and reduced cortisol, all of which support muscle preservation.
Optional post-workout dose (2-3 grams): For individuals engaging in resistance training (which all tirzepatide users should be doing to preserve muscle), an additional dose after training may support recovery by providing substrate for collagen repair and activating mTOR signaling.
Glycine powder is inexpensive, mixes easily in water, and has a mildly sweet taste. Most people find it palatable without any flavoring.
Dietary sources of glycine
When appetite is suppressed on tirzepatide, making every calorie and every gram of protein count becomes essential. Certain protein sources are particularly rich in glycine:
Bone broth: One of the richest natural sources, providing 2-3 grams of glycine per cup depending on preparation. For tirzepatide users who struggle with solid food but can tolerate warm liquids, bone broth serves double duty as a glycine source and a hydration strategy.
Collagen peptides: A 10-gram serving of collagen peptides provides approximately 2-3 grams of glycine. These dissolve in hot or cold beverages and are tasteless, making them easy to incorporate even when appetite is low.
Gelatin: Similar glycine content to collagen peptides but requires dissolving in hot liquid. Can be used to make protein-rich gummies or jellies, which some tirzepatide users find easier to consume than traditional protein sources.
Protein-rich foods: Skin-on poultry, pork, and fish provide more glycine than lean cuts. The connective tissue in these foods is rich in collagen and therefore glycine.
What to eat on tirzepatide to maximize glycine benefits
When your appetite allows only 1,200-1,500 calories per day, as is common during active tirzepatide therapy, prioritizing protein intake is critical. Aiming for 0.7-1.0 grams of protein per pound of body weight becomes difficult when you simply cannot eat enough food. This is where strategic supplementation with glycine and collagen bridges the gap.
A practical daily plan might look like this:
Breakfast: High-protein meal (eggs, Greek yogurt, or protein shake) with 3 grams of glycine powder mixed in. Lunch: Protein-focused meal with emphasis on collagen-rich sources when possible. Dinner: Small protein-rich meal or bone broth if appetite is low. Before bed: 3 grams of glycine powder in water.
This approach ensures 6+ grams of supplemental glycine daily plus whatever glycine comes from dietary protein. Combined with the glycine in a compounded tirzepatide injection (however small), total daily glycine intake reaches the range supported by research.
Tirzepatide with glycine versus tirzepatide alone: what actually changes
Setting aside the marketing and focusing strictly on what we can reasonably expect, here is an honest assessment of what tirzepatide with glycine offers compared to tirzepatide alone.
What the glycine in the injection likely does
Improves formulation stability, potentially extending shelf life. Buffers the injection pH, reducing injection site discomfort. Provides a small amount of additional glycine to the subcutaneous tissue. May slightly improve the tolerability profile of the injection itself.
What the glycine in the injection probably does not do
Meaningfully preserve muscle mass at 5-30mg per dose. Significantly boost glutathione levels systemically. Improve insulin sensitivity at injection-level doses. Replace the need for dietary protein or oral glycine supplementation.
What comprehensive glycine supplementation (oral plus injectable) may do
Reduce lean mass loss during aggressive caloric restriction. Improve sleep quality, supporting recovery and hormonal balance. Maintain or restore glutathione levels, reducing oxidative stress. Support collagen and connective tissue integrity during rapid weight change. Provide cytoprotective effects in the GI tract, potentially reducing some side effects. Activate mTOR signaling to support muscle protein synthesis through non-leucine pathways.
The honest summary: tirzepatide with glycine in the injection is a marginally better formulation than tirzepatide without glycine, but the real glycine benefits require oral supplementation at research-supported doses. The injection is not a substitute for a comprehensive glycine strategy.
Combining glycine with other muscle preservation strategies
Glycine does not work in isolation, and it should not be your only strategy for preserving muscle on tirzepatide. The most effective approach combines multiple evidence-based interventions.
Resistance training is non-negotiable
No supplement, amino acid, or compounding additive can replace the muscle-preserving signal sent by resistance training. When you lift weights, you tell your body that muscle is needed. Without that signal, your body will catabolize muscle tissue whenever calories are restricted, regardless of how much glycine you consume.
Two to three resistance training sessions per week, focusing on compound movements (squats, deadlifts, presses, rows), provides the stimulus necessary to maintain muscle mass during GLP-1-mediated weight loss. The training does not need to be extreme. Moderate loads performed consistently send a stronger preservation signal than occasional intense sessions.
Protein intake targets
Aim for 0.7-1.0 grams of protein per pound of target body weight daily. This is challenging on tirzepatide because appetite suppression makes eating difficult. Strategies include front-loading protein at the first meal when appetite is strongest, using liquid protein sources (shakes, bone broth), and prioritizing protein at every eating occasion.
Supplementing with essential amino acids or leucine specifically can also help. Leucine is the primary trigger for mTOR activation through the branched-chain amino acid pathway. Combined with glycine activating mTOR through a separate pathway, the two amino acids may have complementary effects on muscle protein synthesis.
Creatine monohydrate
Creatine at 3-5 grams daily is the most researched and most effective supplement for preserving muscle and strength during caloric restriction. It works through completely different mechanisms than glycine (phosphocreatine energy system, cell hydration, gene expression) and the two can be used together without interaction concerns.
For tirzepatide users, creatine plus glycine plus adequate protein plus resistance training represents the most comprehensive evidence-based muscle preservation stack available.
Gradual dose titration
Rapid dose escalation of tirzepatide leads to more dramatic appetite suppression, more severe caloric restriction, and potentially more muscle loss. Starting at the lowest dose (2.5mg) and increasing gradually every 4 weeks allows the body to adapt, gives you time to establish protein intake habits, and reduces the severity of GI side effects that further interfere with eating.
The compounded formulations from pharmacies like Strive Pharmacy, Wells Pharmacy Network, and others offer microdosing options that allow even more gradual titration than the standard 2.5mg starting dose. Some protocols begin at 1mg or even 0.5mg and increase weekly, giving the body maximal time to adjust.
Understanding the regulatory landscape
Any discussion of compounded tirzepatide must address the regulatory reality. The landscape has shifted significantly, and understanding where things stand helps you make informed decisions.
The FDA resolved the tirzepatide shortage in late 2024, which triggered regulatory changes affecting compounding pharmacies. Under federal law, compounding pharmacies can produce copies of commercially available drugs only under specific circumstances. When a drug is in shortage, Section 503A and 503B of the Federal Food, Drug, and Cosmetic Act permit compounding. When the shortage is resolved, that permission narrows considerably.
However, compounding pharmacies can still produce formulations that are "essentially a copy" exceptions or that represent meaningfully different formulations from the commercial product. This is where additives like glycine and niacinamide become relevant not just therapeutically but legally. A tirzepatide-glycine-B12 formulation is arguably a different product from brand-name Mounjaro, which contains tirzepatide alone.
The legal and regulatory details continue to evolve. What matters for you as someone considering tirzepatide with glycine is that you work with a licensed provider who prescribes from a licensed, inspected compounding pharmacy that maintains appropriate quality controls regardless of the regulatory environment.
Who benefits most from tirzepatide with glycine
Not everyone using tirzepatide needs to worry equally about muscle loss or glycine supplementation. Risk factors help identify who benefits most from this combination approach.
Higher-risk groups for muscle loss
Adults over 50: Age-related muscle loss (sarcopenia) is already occurring at a rate of 1-2% per year after age 30. Adding aggressive weight loss on top of this baseline decline creates compounding risk. Glycine supplementation, resistance training, and high protein intake are all more important for this group.
Sedentary individuals: Without the muscle-preservation signal from exercise, the body preferentially catabolizes muscle during caloric restriction. Sedentary tirzepatide users lose proportionally more lean mass than active users.
Those with low starting muscle mass: If you begin tirzepatide with already-low muscle mass (perhaps from a previous period of weight loss, illness, or sedentary lifestyle), you have less buffer before muscle loss becomes clinically significant.
Higher-dose protocols: Patients on 10mg or 15mg tirzepatide doses experience more aggressive appetite suppression and therefore more severe caloric restriction. The muscle loss risk increases in proportion to the caloric deficit.
Lower-risk groups
Active individuals with robust muscle mass: If you train regularly and start tirzepatide with above-average muscle mass, you have more reserve and are less likely to experience clinically meaningful muscle loss, especially at lower doses.
Those consuming adequate protein: Protein intake above 0.7g per pound of body weight provides substantial protection against lean tissue loss regardless of supplementation.
Younger adults: Anabolic hormone levels and muscle protein synthesis rates are higher in younger adults, providing some natural protection against muscle catabolism during caloric restriction.
Switching to or from tirzepatide with glycine
If you are currently using standard tirzepatide (Mounjaro, Zepbound) and considering switching to a compounded glycine formulation, or vice versa, several considerations apply.
Switching from brand-name to compounded tirzepatide with glycine
The tirzepatide dose should remain the same during the switch. A compounded 5mg tirzepatide with glycine should produce similar GLP-1 and GIP effects as 5mg brand-name tirzepatide. However, differences in formulation, delivery device (syringe versus autoinjector), and excipients may cause subtle differences in absorption kinetics and side effect profiles.
The transition period is typically straightforward. Continue your existing dose schedule, begin oral glycine supplementation if you are not already doing so, and monitor your response over the first 2-4 weeks.
Switching from compounded to brand-name
If transitioning to brand-name tirzepatide (perhaps due to insurance coverage changes or regulatory developments), the loss of injectable glycine is minimal given the low doses involved. Continue oral glycine supplementation at 3-5 grams daily to maintain the therapeutic benefits.
Adding glycine to an existing semaglutide protocol
Everything discussed here about glycine and tirzepatide applies equally to semaglutide with glycine. The muscle loss concern, the glycine mechanisms, and the supplementation strategies are the same across GLP-1 and GLP-1/GIP medications. If you are on semaglutide and want glycine benefits, oral supplementation is the most straightforward and evidence-based approach.
What the future holds for tirzepatide and glycine research
Several developments may clarify the tirzepatide-glycine question in the coming years.
Clinical trials examining body composition outcomes with GLP-1 medications are increasingly including lean mass preservation as a primary or secondary endpoint. As these trials mature, we will have better data on how much muscle loss is typical and which interventions most effectively prevent it.
Research into amino acid supplementation during pharmacological weight loss is growing. Studies on glycine specifically, as well as other amino acids like leucine, HMB (beta-hydroxy beta-methylbutyrate), and creatine, will eventually provide the kind of controlled data needed to make definitive recommendations.
Next-generation GLP-1 medications, including retatrutide (a triple agonist) and CagriSema (cagrilintide plus semaglutide), may have different lean mass preservation profiles. Some early evidence suggests that certain next-generation compounds may be somewhat more muscle-sparing than current options, though this remains to be confirmed in large-scale studies.
Combination approaches pairing GLP-1 medications with muscle-building agents like bimagrumab (a myostatin pathway inhibitor) are in clinical trials. These represent a pharmaceutical approach to the muscle loss problem that could eventually replace or complement nutritional strategies like glycine supplementation.
Until those studies report, the current evidence supports glycine supplementation as a reasonable, low-risk, low-cost addition to a comprehensive tirzepatide protocol that includes resistance training, adequate protein, and mindful dose titration.
Frequently asked questions
Does the glycine in compounded tirzepatide actually preserve muscle?
At the doses typically included in compounded injections (5-30mg), the glycine is unlikely to meaningfully preserve muscle on its own. The research supporting glycine for muscle preservation uses doses of 3,000-15,000mg daily. However, glycine does improve the formulation by buffering pH and stabilizing the peptide. For actual muscle preservation benefits, add oral glycine supplementation at 3-5 grams per day alongside your compounded injection.
Can I take glycine separately instead of using a compounded formulation?
Yes. Taking 3-5 grams of glycine powder daily provides significantly more glycine than any compounded injection. This is actually the most evidence-based approach because it delivers research-level doses. You can use standard tirzepatide (brand or compounded without glycine) and supplement glycine orally to achieve the same or better results than a glycine-containing formulation alone.
Is tirzepatide with glycine safer than tirzepatide alone?
Glycine is extremely safe at supplemental doses. It is a normal dietary amino acid with no known toxicity at doses up to 15 grams per day in research settings. Adding glycine to tirzepatide does not introduce meaningful safety concerns. The side effect profile remains dominated by tirzepatide's known GI effects (nausea, constipation, diarrhea) rather than anything glycine-related.
How much glycine should I take per day on tirzepatide?
Most research supports 3-5 grams daily for general health benefits. For individuals specifically targeting muscle preservation during weight loss, doses up to 10 grams daily (split into 2-3 doses) have been used in clinical settings. A common protocol is 3 grams in the morning and 3 grams before bed. The before-bed dose also supports better sleep.
Does glycine interact with tirzepatide or other medications?
There are no known pharmacological interactions between glycine and tirzepatide. Glycine is also compatible with most common medications. However, because glycine can theoretically affect blood sugar levels and insulin sensitivity, individuals taking insulin or sulfonylureas alongside tirzepatide should discuss glycine supplementation with their prescriber to ensure appropriate monitoring.
What is the difference between tirzepatide with glycine and tirzepatide with glycine and B12?
The triple compound (tirzepatide plus glycine plus B12) adds cyanocobalamin or methylcobalamin to the formulation. B12 is included primarily to address nausea and support energy levels during caloric restriction. Some clinicians prefer the triple compound because B12 deficiency risk increases during prolonged reduced food intake, and the combination addresses multiple supportive needs in a single injection.
Should I choose glycine or niacinamide in my compounded tirzepatide?
Choose glycine if your primary concern is muscle preservation, sleep quality, or connective tissue health. Choose niacinamide if your primary concern is energy levels, skin health, or cellular metabolism. Both have limited direct evidence for their inclusion in tirzepatide specifically, and both have strong standalone research. Some clinicians recommend one formulation while supplementing the other additive orally.
How long should I continue glycine supplementation while on tirzepatide?
Continue glycine supplementation for the entire duration of your tirzepatide protocol and for at least 4-8 weeks after discontinuing the medication. The post-treatment period carries its own muscle loss risk as the body transitions back to normal appetite and caloric intake patterns. Maintaining glycine, protein intake, and resistance training during this transition helps preserve the body composition improvements achieved during treatment.
External resources
Glycine supplementation for physical performance and recovery (PMC)
Dietary glycine as rate-limiting for glutathione synthesis (PMC)
Effects of tirzepatide on skeletal muscle mass: systematic review (PMC)
Tirzepatide and muscle composition changes SURPASS-3 MRI (The Lancet)
New GLP-1 therapies and muscle preservation (American Diabetes Association)
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, detailed compound comparisons, personalized protocol builders, and a community of thousands who have navigated these exact questions about compounded tirzepatide formulations and muscle preservation strategies.
In case I do not see you, good afternoon, good evening, and good night. May your muscle mass stay preserved, your glycine levels stay optimal, and your tirzepatide results stay exactly what you hoped for.