Feb 17, 2026

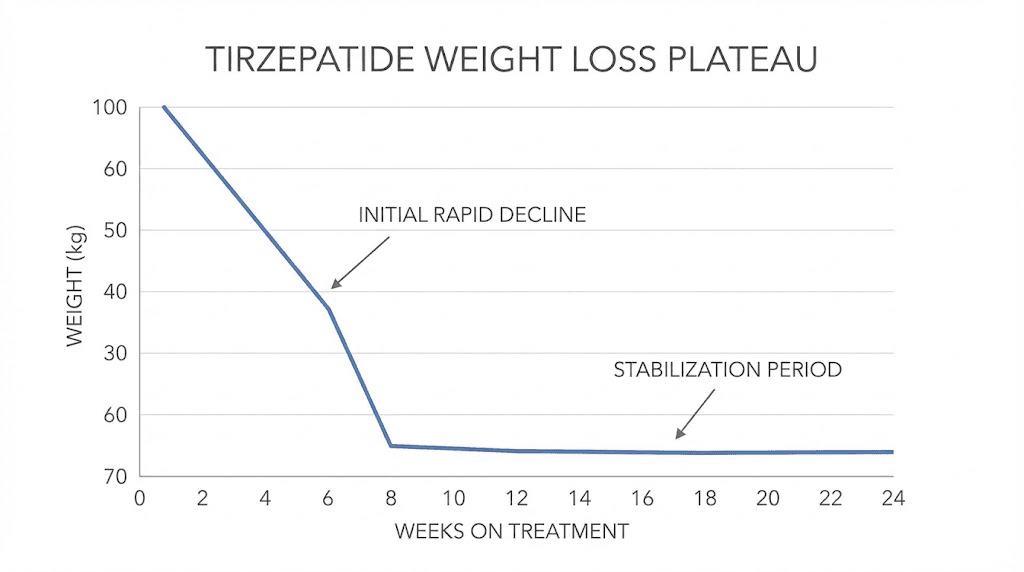
Six months ago, the weight was falling off. Your appetite had quieted. Portions shrank without effort. The scale moved every week, sometimes every few days, and for the first time in years the trajectory felt inevitable. Tirzepatide was working.
Then it stopped.
Not overnight. Not dramatically. More like a slow fade. The scale stuck. Then it bounced. The hunger crept back, not the roaring appetite from before, but enough to notice. Enough to make you wonder whether something had changed, whether your body had adapted, whether the medication had simply run out of magic.
You are not imagining this. And you are not alone. The SURMOUNT-1 clinical trial data shows that approximately 88 to 90 percent of tirzepatide users reach a weight plateau by week 72. That is not a failure rate. That is biology doing exactly what biology does when you lose significant weight. But understanding why it happens and what to do about it makes the difference between someone who pushes through and someone who gives up on a medication that is still working harder than they realize.
This guide breaks down every mechanism behind tirzepatide plateaus. The metabolic adaptation. The hormonal shifts. The receptor changes. The lifestyle factors that quietly sabotage results. More importantly, it gives you a systematic, evidence-based approach to restart weight loss when tirzepatide feels like it has stalled. SeekPeptides has analyzed thousands of protocols and the patterns are unmistakable once you know what to look for.
The biology behind why tirzepatide stops producing visible results
Before you change anything about your protocol, you need to understand what is actually happening inside your body. Because the truth is counterintuitive. In most cases, tirzepatide has not stopped working. Your body has simply become more efficient at defending its new, lower weight.
Metabolic adaptation is not optional
When you lose weight, your body does not celebrate. It panics. From an evolutionary perspective, rapid weight loss signals famine. Your body responds with a coordinated defense strategy designed to stop the loss and regain the weight. This is called metabolic adaptation, and it happens to everyone who loses significant weight, regardless of how they lose it.
Here is what metabolic adaptation looks like in practice. Your resting metabolic rate drops. Not just because you are smaller and require fewer calories to exist, but disproportionately. A person who has lost 50 pounds burns fewer calories at rest than a person who has always weighed that lower amount. The deficit goes beyond what the math predicts. Your body is actively throttling energy expenditure.
A study published in Cell Metabolism examined tirzepatide impact on metabolic adaptation directly. In animal models, tirzepatide attenuated the metabolic adaptation that occurred during calorie restriction. However, in human clinical trials the picture was more nuanced. Tirzepatide did not appear to fully prevent metabolic adaptation, but it did increase fat oxidation, meaning the body preferentially burned fat for fuel even as overall energy expenditure declined. That is a meaningful distinction because it means the medication is still actively working on fat metabolism even when the scale has stopped moving.
Hormonal counterregulation fights back
Weight loss triggers a cascade of hormonal changes designed to make you eat more and move less. Leptin, the hormone that signals satiety, drops as fat stores shrink. Ghrelin, the hunger hormone, rises. These shifts persist for months or even years after weight loss, creating a sustained biological pressure to regain.
Tirzepatide counteracts some of these changes through its dual GLP-1 and GIP receptor activation. It suppresses appetite, slows gastric emptying, and improves insulin sensitivity. But the hormonal counterregulation intensifies as weight loss accumulates. At some point, the medication is fighting harder just to maintain the current weight loss, leaving less pharmacological power available to drive further loss.
This is not tolerance. This is a shift in the battlefield. The medication is working as hard as ever. Your body is simply fighting back harder.
Gastric emptying tachyphylaxis changes the equation
One of tirzepatide fastest-acting mechanisms is delayed gastric emptying. Food sits in your stomach longer, stretch receptors fire satiety signals, and you feel full faster. This effect is strongest after the very first dose.
But research published in the Journal of Clinical Endocrinology and Metabolism shows that tachyphylaxis, a reduction in response to repeated dosing, occurs with the gastric emptying effect. At a fixed dose of 5mg, tachyphylaxis was complete after repeated dosing. However, in dose escalation cohorts, tachyphylaxis was not observed because each dose increase re-intensified the effect.
What this means practically: if you have been on the same dose for months, you have lost some of the gastric emptying benefit. The food moves through your stomach faster than it did initially. You might not feel as dramatically full after meals. This contributes to the sensation that tirzepatide has stopped working, even though the central appetite suppression and metabolic effects remain active.
The set point theory and your body defense system
Your body appears to defend a weight set point, a range it considers normal based on your history, genetics, and hormonal environment. When you move below this set point, every biological system pushes to bring you back. When you move above it, the pressure is less intense, which is why weight gain is easier than weight loss.
GLP-1 receptor agonists like tirzepatide appear to lower this set point through sustained hormonal changes that promote satiety and diminish appetite. But the set point does not drop infinitely. At some point, the medication establishes a new equilibrium, a weight your body defends on tirzepatide. This is your plateau. It is not a failure. It is your body reaching a new defended weight that is significantly lower than where you started.
The question then becomes: can you lower the set point further? In many cases, yes, through dose optimization, lifestyle modification, and time.
How to tell the difference between a plateau and the medication actually failing
Not every stall is a plateau. And not every plateau requires the same response. The first step is accurate diagnosis.
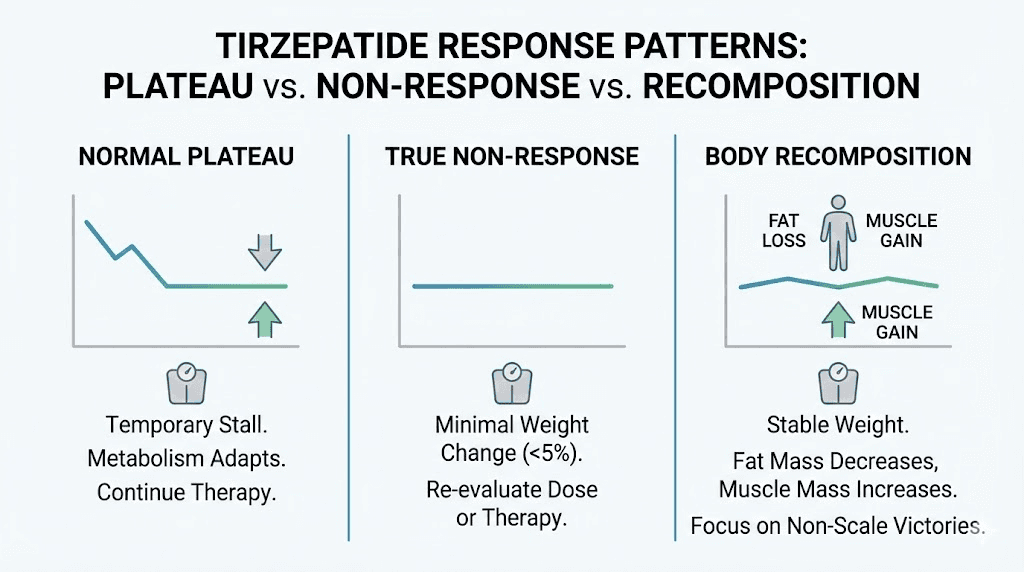
Normal plateau (medication is working)
A normal tirzepatide plateau looks like this. You lost significant weight over months. The rate of loss slowed gradually. You have been within a 3 to 5 pound range for 4 to 8 weeks. Your appetite remains lower than it was before starting tirzepatide. Your clothes still fit differently than they did before treatment. You feel better overall, more energy, better digestion, improved mood.
The SURMOUNT-1 trial defined a weight plateau as less than 5 percent weight change over a 12-week interval and all subsequent 12-week intervals. By this definition, reaching a plateau is the expected outcome, not the exception. The median time to plateau ranged from 24 to 36 weeks depending on BMI category and dose level.
If you match this description, the medication is still working. Your body has found a new equilibrium. The strategies in this guide can help push through to additional loss.
True non-response (medication may not be working)
True non-response looks different. You have been on a therapeutic dose (5mg or higher) for at least 12 weeks with zero weight change. Your appetite has not decreased at all. Your eating patterns are identical to pre-treatment. You have experienced no side effects, not even mild nausea during dose escalation.
Complete non-response to tirzepatide is rare. In the SURMOUNT-1 trial, 82 percent of participants achieved at least 5 percent weight loss by week 12. Of the remaining 18 percent who were slow to respond, 90 percent still achieved clinically meaningful weight loss by week 72. True non-responders are a small minority.
If you genuinely believe you are a non-responder, the next section on medical evaluation is especially important for you.
Pseudo-plateau (body recomposition)
This one catches a lot of people off guard. The scale has not moved in six weeks. You feel frustrated. But your pants are looser. Your face looks thinner. Someone commented that you look like you have lost weight.
This is body recomposition. You are losing fat and gaining lean mass simultaneously, which is common when people add resistance training during tirzepatide treatment. Muscle is denser than fat. You can lose inches while the scale stays flat.
Research shows that up to 39 percent of weight lost on GLP-1 and GIP/GLP-1 medications comes from lean mass, including muscle. If you are actively countering this with strength training and adequate protein, you may be building muscle while losing fat. The scale does not know the difference. Your body does.
Take measurements. Track waist circumference, hip circumference, and how your clothes fit. These metrics often tell a more accurate story than the scale alone.
The SURMOUNT data: what clinical trials reveal about tirzepatide plateaus
Let the data ground the conversation. The emotions around a weight loss stall are real, but the science provides clarity.
Time to plateau by BMI category
A dedicated analysis of the SURMOUNT-1 and SURMOUNT-4 trials examined exactly when participants hit their weight plateau. The findings were specific and revealing.
Participants with overweight (BMI 27 to 30) reached their median plateau at 24.3 weeks. Those with Class I obesity (BMI 30 to 35) plateaued at 26 weeks. Class II obesity (BMI 35 to 40) and Class III obesity (BMI 40 and above) both hit median plateau at 36.1 weeks.
The pattern is clear. People with more weight to lose take longer to plateau. They also achieve greater total weight loss before stabilizing. Higher BMI categories showed significantly greater additional weight loss after week 24 compared to lower BMI categories.
Factors that predict when you will plateau
Three factors consistently predicted a longer time to plateau across both SURMOUNT trials.
Higher medication doses. The 10mg dose extended time to plateau by 4.4 weeks compared to 5mg. The 15mg dose extended it by 6.7 weeks. This is important because it means dose escalation is not just about more weight loss. It is about delaying the plateau itself, giving you more time in the active loss phase.
Younger age. Each 10-year decrease in age was associated with 0.9 additional weeks before reaching plateau. Younger bodies may have more metabolic flexibility and less entrenched hormonal resistance to weight loss.
Female sex. Women experienced approximately 4.2 additional weeks before reaching plateau compared to men. This may relate to differences in body composition, hormonal profiles, or fat distribution patterns.
Factors that predicted earlier plateaus
Baseline prediabetes diagnosis was associated with earlier plateaus. This makes sense because insulin resistance creates metabolic headwinds that blunt weight loss. Asian race was associated with reaching plateau approximately 2.6 weeks earlier than White participants. The presence of comorbidities like hypertension and dyslipidemia also predicted earlier plateaus.
None of these factors meant the medication failed. They simply influenced when the plateau arrived, not whether additional strategies could push through it.
The late responder data is critical
Here is the number that should give everyone hope. Of the 18 percent of participants who had less than 5 percent weight loss at week 12, the so-called late responders, 90 percent still achieved clinically meaningful weight loss by week 72.
Read that again. Nine out of ten people who appeared to be failing at three months were succeeding at eighteen months. The medication works on different timelines for different people. If you are stalled early, the data overwhelmingly supports continuing treatment.
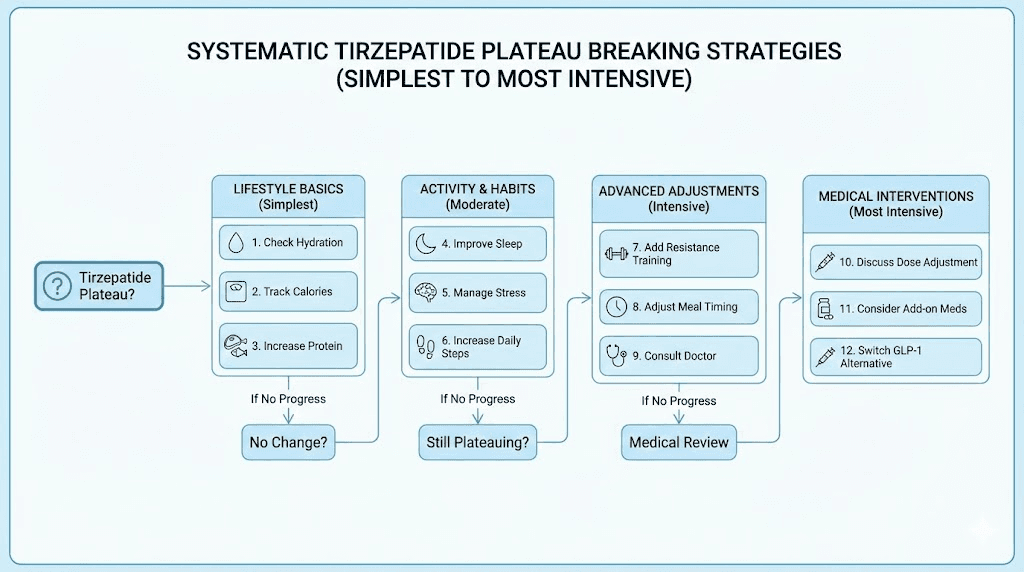
Twelve proven strategies to break through a tirzepatide plateau
Here is the practical part. These strategies are ordered from simplest to most intensive. Start at the top and work down.
Strategy 1: verify you are actually plateaued
Before you change anything, confirm the stall is real. Weight fluctuates daily based on hydration, sodium intake, bowel movements, hormonal cycles, and a dozen other factors. A single week of no change means nothing. Even two weeks can be noise.
Use these criteria. Has your weight been within a 3 to 5 pound range for at least 4 weeks while maintaining your current dose and lifestyle? If yes, you are likely in a genuine plateau. If your stall is less than 4 weeks old, give it more time before intervening.
Weigh yourself consistently. Same time, same conditions, same scale. First thing in the morning after using the bathroom. Track the weekly average, not individual daily readings. The trend matters more than any single data point.
Strategy 2: audit your protein intake
This is the single most impactful dietary change for most people on tirzepatide. Protein does three things simultaneously. It preserves lean muscle mass during weight loss, which maintains metabolic rate. It is the most satiating macronutrient, meaning it keeps you fuller longer per calorie. And it has a higher thermic effect, meaning your body burns more calories digesting protein than carbohydrates or fat.
The research is clear. Recommended protein intake for people on GLP-1 medications ranges from 1.0 to 1.6 grams per kilogram of body weight per day. That is significantly higher than the standard dietary recommendation of 0.8 grams per kilogram. Most tirzepatide users underestimate how much protein they eat because they feel full so quickly on the medication that they stop eating before reaching adequate protein targets.
Calculate your specific target based on your goal body weight. If your goal weight is 160 pounds, aim for at least 73 to 116 grams of protein daily. Distribute it across meals. Prioritize protein at the start of each meal when your appetite is strongest. Consider protein supplements if whole food intake is limited by appetite suppression.
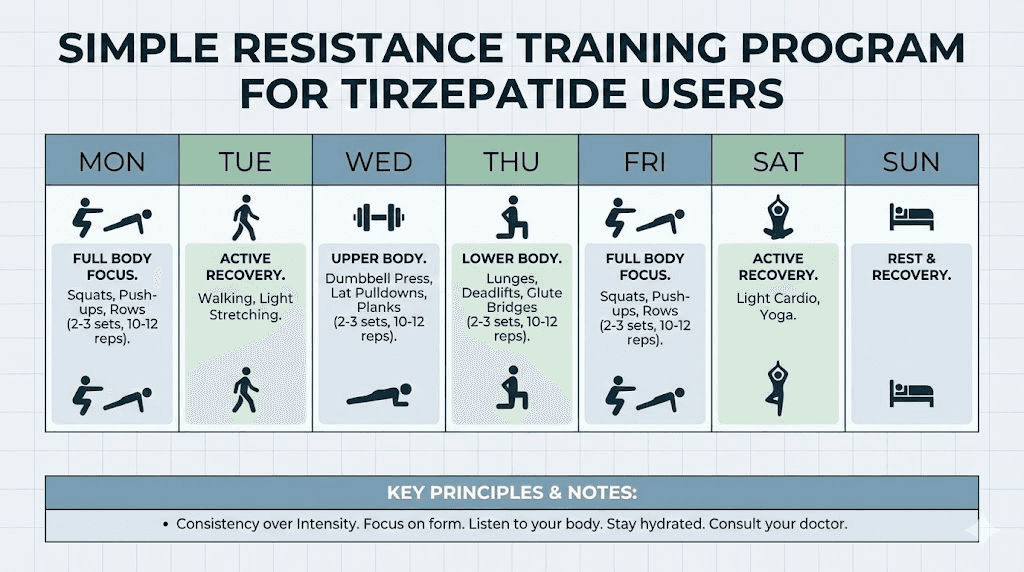
Strategy 3: add or intensify resistance training
Resistance training is the most powerful tool for combating the metabolic slowdown that causes plateaus. When you lift weights, you signal your body to preserve and build muscle even while in a caloric deficit. This directly counters the lean mass loss that drives metabolic adaptation.
Research shows that incorporating resistance training two to three times weekly helps preserve lean muscle mass during weight reduction and can increase resting metabolic rate. Even two sessions per week of resistance exercises signal your body to hold onto or rebuild lean mass.
You do not need to become a bodybuilder. Compound movements like squats, deadlifts, rows, and presses hit multiple muscle groups efficiently. Start with bodyweight exercises if you are new to strength training. Progress to weighted movements as you build capacity. The goal is progressive overload, gradually increasing the challenge to your muscles over time.
The research on muscle preservation during GLP-1 medication use is unambiguous. Concurrent physical activity, especially resistance training, has been shown to effectively minimize loss of muscle mass and function during weight reduction therapy.
Strategy 4: optimize sleep ruthlessly
Poor sleep is a silent plateau perpetuator. Sleep deprivation increases ghrelin and decreases leptin, directly opposing tirzepatide mechanism of action. It increases cortisol, which promotes fat storage, particularly visceral fat. It impairs insulin sensitivity, which blunts tirzepatide metabolic benefits. And it increases reward-center activity in response to food cues, making cravings harder to resist.
Seven to nine hours of quality sleep is not a luxury when you are trying to break through a tirzepatide plateau. It is a force multiplier. Every study on weight loss and sleep reaches the same conclusion: sleep-deprived individuals lose less fat, lose more muscle, and experience stronger hunger than well-rested individuals on identical protocols.
If you are sleeping less than seven hours consistently, fixing this single factor may restart weight loss without any other changes.
Strategy 5: eliminate ultra-processed food
Ultra-processed foods are engineered to override satiety signals. They combine sugar, fat, and salt in ratios that trigger dopamine release in the reward center, the same nucleus accumbens that tirzepatide is trying to quiet. Eating these foods while on tirzepatide is like pressing the gas and brake simultaneously.
A landmark NIH study found that people eating ultra-processed diets consumed approximately 500 more calories per day than those eating unprocessed foods, even when both diets were matched for macronutrients. The ultra-processed foods bypassed normal satiety mechanisms.
You do not need to be perfect. But if your diet is more than 30 percent ultra-processed foods, reducing this significantly can restart the appetite suppression you felt in the early weeks. Focus on whole proteins, vegetables, fruits, nuts, and whole grains. Let tirzepatide work with your diet, not against it.
Strategy 6: discuss dose adjustment with your provider
If you have been on a submaximal dose (below 15mg weekly) for at least four weeks and have tolerated the current dose well, increasing to the next dose level may restore weight loss momentum.
The data supports this approach. The SURMOUNT-1 trial showed that higher doses produced greater weight loss and delayed the plateau. The 15mg group achieved 22.5 percent body weight reduction compared to 16 percent for the 5mg group. Each dose increase re-engages gastric emptying delay through overcoming tachyphylaxis, re-intensifies central appetite suppression, and provides greater metabolic benefit.
The standard dose escalation increases by 2.5mg every four weeks. If you have been sitting at a comfortable 7.5mg or 10mg and your weight has plateaued, moving to the next level is a logical step. Your provider evaluates tolerability, side effects, and clinical need before recommending an increase. Do not adjust your own dose without medical guidance.
Strategy 7: evaluate medication quality
Some people using compounded formulations of tirzepatide report variable results compared to brand-name Mounjaro or Zepbound. Compounded formulations can differ in potency, stability, and absorption characteristics depending on the compounding pharmacy.
If you switched from brand-name to compounded tirzepatide around the same time your plateau started, the correlation is worth investigating. Discuss this with your provider. A switch back to brand-name, or verification of your compounding pharmacy quality standards, may resolve the issue.
Storage matters too. Proper refrigeration is essential for maintaining tirzepatide potency. If your medication has been exposed to high temperatures, left unrefrigerated for extended periods, or stored improperly, the active ingredient may have degraded. Check your storage conditions and expiration dates.
Strategy 8: request comprehensive blood work
Underlying metabolic conditions can significantly blunt tirzepatide effectiveness and contribute to plateaus. Request a comprehensive panel that includes thyroid function (TSH, free T4, free T3), fasting insulin and C-peptide, HbA1c, fasting glucose, cortisol (morning), complete metabolic panel, and sex hormones (testosterone, estrogen, DHEA-S).
Untreated hypothyroidism alone can stall weight loss completely. Even subclinical hypothyroidism, where TSH is elevated but still within the reference range, can slow metabolic rate enough to create a persistent plateau. Cortisol dysregulation from chronic stress creates hormonal conditions that directly oppose weight loss. Insulin resistance, even moderate levels, creates metabolic headwinds that tirzepatide must fight through.
Blood work provides objective data that guides next steps. Treat what is treatable. You cannot overcome undiagnosed hypothyroidism with willpower or a better diet.
Strategy 9: implement strategic calorie cycling
Sustained caloric restriction, even when mediated by appetite suppression, can push your body deeper into metabolic adaptation. One approach to disrupting this pattern is strategic calorie cycling, alternating between periods of moderate deficit and periods of maintenance-level eating.
The concept is straightforward. Spend 5 to 6 days at your typical reduced intake. Then spend 1 to 2 days eating at maintenance calories (not a free-for-all, just more food, primarily protein and complex carbohydrates). The higher-calorie days signal to your body that famine is not occurring, which can partially reverse the metabolic adaptations that cause plateaus.
This approach is not license to binge. The refeed days should still consist of nutritious whole foods. The goal is strategic metabolic signaling, not emotional eating under a pseudoscientific banner.
Strategy 10: address stress and emotional eating
Chronic stress elevates cortisol, which directly stimulates appetite and promotes fat storage. But stress-driven eating is a different beast than physiological hunger. Tirzepatide addresses physiological hunger brilliantly through its dual receptor mechanism. Emotional hunger operates on a different pathway entirely.
If you are eating when you are not physically hungry, when there is no stomach growling or genuine hunger signals, you are likely eating emotionally. Stress, boredom, loneliness, anxiety, and habit can all drive food intake that has nothing to do with the hormones tirzepatide modulates.
Addressing the psychological component is not a weakness. It is a strategic necessity. Cognitive behavioral therapy, mindful eating practices, and support groups have all shown efficacy in improving weight loss outcomes when combined with pharmacological treatment. The medication handles the biology. You need to handle the behavior.
Strategy 11: review timing and injection technique
Tirzepatide has a half-life of approximately five days. Many users report that appetite suppression is strongest in the 1 to 3 days following injection and gradually softens before the next dose. This pattern is more noticeable at lower doses.
Strategic injection timing can help. Some people time their injection to align peak appetite suppression with their most challenging eating days. If weekends are your difficult days, injecting Thursday evening puts peak effects over Saturday and Sunday. If weekday work stress drives overeating, injecting Sunday night covers Monday through Wednesday.
Injection technique matters too. Tirzepatide is a subcutaneous injection. If injected too shallow (intradermal) or too deep (intramuscular), absorption kinetics change, affecting how quickly and consistently the medication reaches therapeutic levels. Inject into the subcutaneous fat of the abdomen, thigh, or upper arm. Rotate sites to prevent lipohypertrophy, which can impair absorption over time.
Strategy 12: consider combination approaches
For plateaus that persist despite optimizing all the above factors, some providers explore combination approaches. These are advanced strategies that should only be pursued under direct medical supervision.
Adding phentermine or other appetite suppressants alongside tirzepatide can provide additional central appetite suppression through different neurochemical pathways. This is an off-label combination but has growing clinical support in obesity medicine circles.
Some researchers explore combining tirzepatide with other peptide protocols that target different metabolic pathways. The emerging research on triple agonists like retatrutide, which adds glucagon receptor activation to the GLP-1 and GIP mechanisms, suggests that engaging additional pathways can overcome plateaus that dual agonists alone cannot.
These are not first-line strategies. They are options to discuss with a knowledgeable provider when simpler approaches have been exhausted.
What the research says about long-term tirzepatide effectiveness
Understanding the long-term trajectory helps calibrate expectations and prevent premature discouragement.
Weight loss phases on tirzepatide
Months 1 to 3: the acceleration phase. This is when weight loss feels effortless. Dose escalation drives progressively stronger appetite suppression. The body has not yet mounted significant metabolic resistance. Average weight loss during this phase is approximately 13 to 14.5 percent in the clinical trials. This is the honeymoon period, and it is genuinely powerful, but it does not last forever.
Months 3 to 6: the peak phase. For most people, this window represents the fastest weight loss and strongest appetite suppression. Doses have typically reached therapeutic levels. Steady-state blood concentrations are established. Both GLP-1 and GIP pathways are fully engaged. Results are dramatic and motivating.
Months 6 to 12: the stabilization phase. The rate of loss slows. Appetite suppression may soften slightly. Not because the medication is weaker, but because metabolic adaptation has intensified. The body has adjusted to the new weight and is defending it. This is when most people perceive that tirzepatide has stopped working. In reality, the medication is working to maintain a significantly lower weight against increasing biological resistance.
Beyond 12 months: the maintenance phase. The SURMOUNT-4 trial demonstrated clearly that ongoing tirzepatide treatment maintains weight loss while discontinuation leads to regain. Participants who continued tirzepatide maintained and extended their results. Those who switched to placebo regained weight. Appetite suppression continues as long as the medication continues, though the intensity may fluctuate.
The discontinuation data is sobering
Among participants who achieved weight reduction with 36-week tirzepatide treatment, withdrawing the medication led to 25 percent or greater weight regain in most participants within one year. The appetite suppression, metabolic benefits, and hormonal modulation all require ongoing pharmacological support.
This is not a short course that permanently resets your metabolism. Tirzepatide is a chronic treatment for a chronic condition. Understanding this prevents the disappointment of expecting a cure and receiving management, which is still profoundly effective management.
The role of lean mass preservation in overcoming plateaus
This topic deserves its own section because it is the most underappreciated factor in tirzepatide plateaus.
Why muscle loss causes plateaus
Every pound of muscle you carry burns approximately 6 to 7 calories per day at rest. That sounds small until you multiply it. Losing 10 pounds of muscle reduces your resting metabolic rate by 60 to 70 calories daily. Over a month, that is 1,800 to 2,100 fewer calories burned. Over six months, it is 10,800 to 12,600 calories, equivalent to approximately 3 to 3.5 pounds of potential weight loss erased.
Research shows that up to 39 percent of weight lost on GLP-1 and GIP/GLP-1 medications can come from lean mass. On a 40-pound weight loss, that could be 15 to 16 pounds of muscle. The metabolic impact is substantial and directly contributes to plateaus.
This is why resistance training and protein intake are not optional accessories to tirzepatide treatment. They are essential components of a protocol designed for sustained results.
The protein leverage hypothesis
Some researchers propose that the body regulates food intake partly based on protein needs. If you are not getting enough protein, your body drives you to eat more overall in an attempt to hit its protein target. This is called the protein leverage hypothesis.
On tirzepatide, where total food intake is reduced, protein becomes even more critical. If 70 percent of your reduced diet is carbohydrates and fat, your body may signal hunger specifically because it needs more protein, even though overall caloric needs are met. Prioritizing protein-rich foods at every meal can reduce this protein-specific hunger signal.
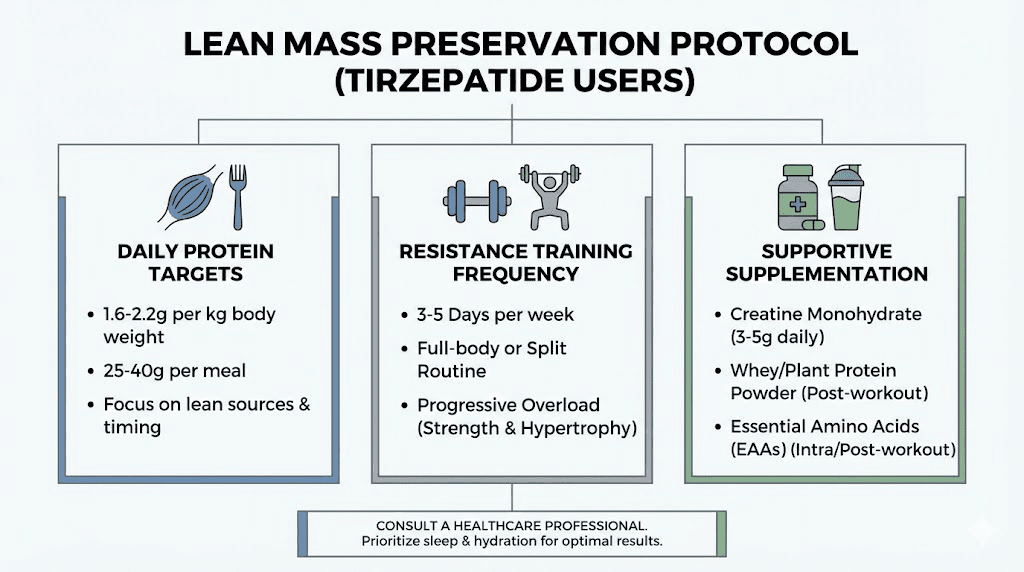
Practical lean mass preservation protocol
Protein target: 1.0 to 1.6 grams per kilogram of body weight daily. Use goal body weight, not current weight, for the calculation. Distribute across 3 to 4 meals.
Resistance training: 2 to 4 sessions per week focusing on compound movements. Progressive overload is key. Track your weights and aim to increase them gradually over time.
Creatine monohydrate: 3 to 5 grams daily. Creatine is the most studied and effective supplement for muscle preservation and performance. It supports strength training efforts directly.
Walking: 7,000 to 10,000 steps daily. This supports fat loss without the muscle-wasting effects of excessive cardio. Walking is metabolically productive without being catabolic.
Adequate recovery: Rest days matter. Muscle growth happens during recovery, not during training. Sleep, nutrition, and rest days between training sessions give your body the resources to build and maintain lean mass.
When to worry and when to wait
Knowing when a plateau requires action versus patience is one of the hardest judgment calls in weight management. Here is a practical framework.
Wait if:
Your plateau is less than 4 weeks old. Your current dose is submaximal and a scheduled increase is coming. You recently changed your exercise routine and may be building muscle. You are in the first 12 weeks of treatment. Your measurements are still changing even if the scale is not. You recently experienced a stressful life event that could be causing temporary cortisol-driven water retention.
Act if:
Your weight has been stable for 8 or more weeks despite consistent medication use. You have optimized lifestyle factors (sleep, protein, exercise, stress) without improvement. You are at maximum dose (15mg) with no further escalation available. You are experiencing symptoms that suggest an underlying condition (fatigue, cold intolerance, hair loss, hormonal irregularities). Your appetite has returned to pre-treatment levels despite continued medication use.
Seek immediate medical attention if:
You are gaining weight rapidly despite continued tirzepatide use, which could indicate an undiagnosed medical condition. You experience new or worsening symptoms alongside the plateau, such as significant fatigue, swelling, or mood changes. You suspect your medication has been compromised due to storage issues or pharmacy errors.
The psychology of a tirzepatide plateau
The emotional impact of a plateau is real and deserves acknowledgment.
The expectations trap
The early weeks of tirzepatide treatment create powerful expectations. Rapid weight loss feels like the new normal. When it slows, the contrast is jarring. You might feel like you are failing even though you have already achieved what many would consider a remarkable transformation.
Perspective matters. If you have lost 30 pounds and plateaued, you are still 30 pounds lighter than when you started. The health benefits of that weight loss, improved insulin sensitivity, lower blood pressure, reduced inflammation, better mobility, persist at the plateau. The plateau does not erase what came before.
The comparison trap
Social media is full of dramatic tirzepatide transformation stories. Someone who lost 80 pounds in six months. Someone whose before and after photos look like two different people. These stories are real, but they are not representative. They are selected for their dramatic impact. The person who lost 25 pounds and plateaued at a healthy weight does not make compelling content, but their outcome may be medically just as successful.
Your journey is your journey. Comparing your month 7 plateau to someone else highlight reel is a recipe for unnecessary distress.
The abandonment trap
The most dangerous response to a plateau is stopping the medication. The SURMOUNT-4 data is clear. Discontinuation leads to weight regain. Most participants who stopped tirzepatide regained 25 percent or more of their lost weight within a year.
If your tirzepatide is not producing further weight loss, it is almost certainly still preventing weight regain. That function alone has enormous health value. Maintaining a 15 percent body weight reduction reduces cardiovascular risk, improves glycemic control, reduces joint stress, and enhances quality of life. Stopping the medication sacrifices these benefits for the hope that something else might work better. That gamble rarely pays off.
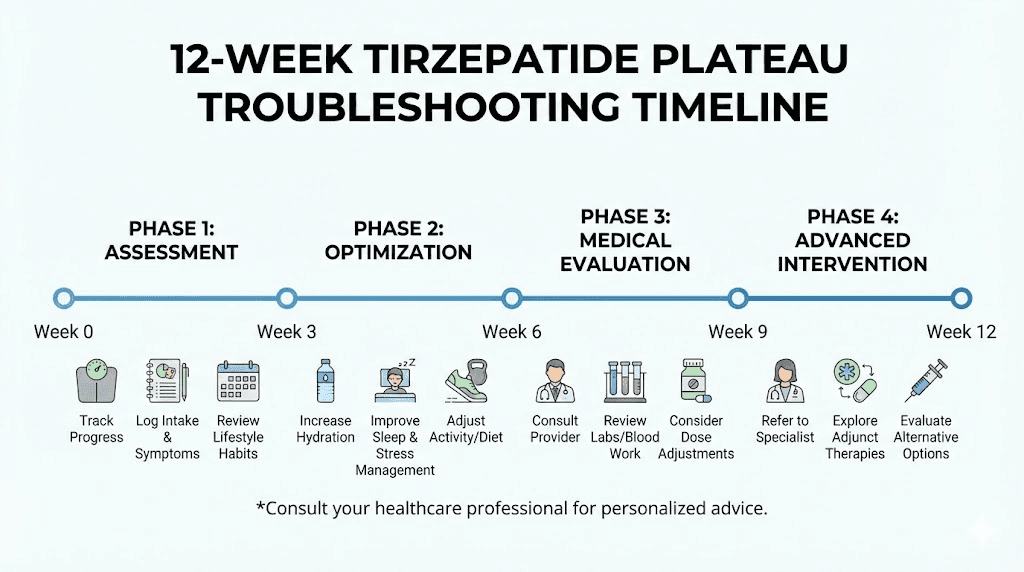
A complete troubleshooting protocol
Here is a systematic approach to diagnosing and addressing a tirzepatide plateau. Follow it step by step.
Week 1 to 2: assessment
Confirm the plateau. Has your weight been within a 3 to 5 pound range for 4 or more weeks? If not, give it more time.
Review your data. Check your food journal, dosing records, exercise log, and sleep tracker. Look for patterns or changes that coincide with the stall.
Take measurements. Waist, hips, chest, arms, thighs. Compare to earlier measurements. Body recomposition may be occurring.
Honest assessment. Have any lifestyle factors slipped? More alcohol? Less sleep? Skipped workouts? Returned to snacking? Increased stress? Be ruthlessly honest.
Week 3 to 4: lifestyle optimization
Protein audit. Track every gram of protein for one week. Are you hitting 1.0 to 1.6 grams per kilogram? If not, increase immediately.
Sleep audit. Are you consistently getting 7 to 9 hours? If not, this is your priority.
Exercise audit. Are you doing resistance training at least twice per week? If not, start now.
Diet quality audit. What percentage of your diet is ultra-processed? Reduce to below 20 percent.
Hydration audit. Are you drinking at least 64 ounces of water daily? Dehydration causes water retention that masks fat loss on the scale.
Week 5 to 8: medical evaluation
If lifestyle optimization does not restart weight loss within 4 weeks, pursue medical evaluation.
Blood work. Thyroid panel, fasting insulin, HbA1c, cortisol, sex hormones. Treat anything abnormal.
Medication review. Are any other medications you take associated with weight gain? Discuss alternatives with your provider.
Dose evaluation. If you are on a submaximal dose, discuss escalation. If you are at maximum dose, discuss combination approaches.
Week 9 to 12: advanced interventions
If medical evaluation and lifestyle optimization have not broken the plateau, discuss advanced strategies with your provider.
Calorie cycling. Implement strategic refeed days at maintenance calories 1 to 2 days per week.
Exercise progression. Increase resistance training intensity or frequency. Consider working with a certified personal trainer.
Combination pharmacotherapy. Discuss adding phentermine or other agents alongside tirzepatide.
Specialist referral. If weight remains stable despite all interventions for 12 or more weeks, referral to an obesity medicine specialist is warranted.
Common mistakes that make tirzepatide plateaus worse
Certain responses to a plateau actively make the situation worse. Avoid these.
Crash dieting during a plateau
The instinct when weight loss stalls is to eat even less. This backfires. Severe caloric restriction deepens metabolic adaptation, accelerates muscle loss, and triggers stronger hormonal counterregulation. Your body interprets the additional restriction as an intensifying famine and doubles down on its defense mechanisms.
If anything, a plateau may require more calories strategically, particularly more protein, not fewer calories overall.
Excessive cardio
Adding hours of cardio to break a plateau seems logical but is often counterproductive. Excessive endurance exercise increases cortisol, depletes glycogen stores that can cause water retention when replenished, and can drive compensatory hunger that exceeds the calories burned. It also promotes muscle loss, which worsens the metabolic slowdown causing the plateau in the first place.
Walking and moderate activity support weight loss. Extreme cardio often hinders it during a plateau.
Obsessive scale watching
Weighing yourself multiple times per day during a plateau is a recipe for despair. Weight fluctuates by 2 to 5 pounds within a single day based on water, food, and waste. These fluctuations mean nothing. They are noise masquerading as signal.
Weigh yourself once daily or even once weekly. Track the trend. Ignore the noise.
Stopping the medication
Worth repeating because it is the most common and most consequential mistake. The SURMOUNT-4 data shows that stopping tirzepatide leads to substantial weight regain. Even if the medication is not producing further loss, it is maintaining your current loss, which has enormous health value. Maintaining is not failing.
Ignoring non-scale victories
Your blood pressure has dropped 15 points. Your HbA1c went from 6.2 to 5.4. Your knee pain is gone. You can walk up stairs without getting winded. You sleep better. Your clothes fit differently. Your energy is higher. Your confidence has improved.
None of these show up on a scale. All of them matter more than the number on it.
When tirzepatide genuinely is not working: rare scenarios
In a small percentage of cases, tirzepatide truly does not produce meaningful results. Understanding these scenarios helps distinguish them from normal plateaus.
True pharmacological non-response
Some individuals have genetic variations in GLP-1 or GIP receptors that reduce their response to tirzepatide. This is rare, but it exists. True non-responders typically show no appetite suppression, no gastrointestinal side effects, and no weight change even at maximum doses over 6 or more months.
If this describes your experience, your provider may recommend switching to a different medication class or exploring other weight management approaches.
Medication absorption issues
Lipohypertrophy, thickened fatty tissue at injection sites from repeated injections in the same area, can impair medication absorption. If you have been injecting in the same spot for months, absorption may be inconsistent. Rotating injection sites between abdomen, thigh, and upper arm prevents this.
Patients with extensive lipodystrophy or certain connective tissue conditions may also have impaired subcutaneous absorption. Alternative delivery methods or injection sites may help.
Competing medical conditions
Certain conditions can completely override tirzepatide effects. Cushing syndrome produces cortisol levels so high that no appetite suppressant can overcome them. Severe untreated hypothyroidism slows metabolism to a degree that creates an insurmountable deficit. Rare hormonal tumors (insulinomas, pheochromocytomas) create metabolic environments incompatible with weight loss.
These are uncommon but important to rule out if you are a true non-responder.
Frequently asked questions
Is tirzepatide not working anymore the same as developing tolerance?
No. Current research shows no evidence that the body develops true pharmacological tolerance to tirzepatide. What people experience as "tolerance" is actually metabolic adaptation, your body biological defense against continued weight loss. The medication is still working, but your body is fighting harder against further loss. Strategies like dose escalation, increased protein intake, and resistance training can help overcome this resistance.
How long do tirzepatide plateaus typically last?
A typical tirzepatide plateau lasts 4 to 8 weeks and is considered a normal part of the weight loss process. Some plateaus resolve spontaneously as the body adjusts to its new weight. Others require intervention through lifestyle optimization or dose adjustment. If your plateau extends beyond 12 weeks despite active intervention, consult your provider for further evaluation.
Should I stop taking tirzepatide if it is not working anymore?
No. The clinical trial data is clear that discontinuing tirzepatide leads to significant weight regain. Even when the medication is not producing further weight loss, it is preventing weight regain and maintaining the metabolic improvements you have already achieved. Stopping should only be considered under medical guidance and with a clear alternative plan.
Can switching from compounded to brand-name tirzepatide help break a plateau?
Possibly. Compounded formulations can vary in potency and consistency depending on the pharmacy. If your plateau coincided with a switch to compounded tirzepatide, the formulation may be a factor. Discuss this with your provider. A trial of brand-name medication (Mounjaro or Zepbound) can help determine whether the formulation is contributing to your stall.
Does exercise matter for breaking a tirzepatide plateau?
Significantly. Research shows that combining tirzepatide with lifestyle modifications including exercise led to an additional 21 percent weight loss in just 12 weeks compared to medication alone. Resistance training specifically preserves muscle mass, increases resting metabolic rate, and improves insulin sensitivity, all of which directly counter the mechanisms causing plateaus.
What blood tests should I get if tirzepatide stopped working?
Request a comprehensive panel including thyroid function (TSH, free T4, free T3), fasting insulin, HbA1c, morning cortisol, sex hormones (testosterone, estrogen, DHEA-S), complete metabolic panel, and vitamin D. Untreated hormonal imbalances and nutritional deficiencies can significantly blunt tirzepatide effectiveness.
Is it normal for appetite to return while still on tirzepatide?
Yes. Appetite suppression fluctuates throughout treatment. Some weeks it feels powerful. Other weeks, hunger creeps back. Hormonal cycles, stress, sleep disruption, illness, and seasonal changes all modulate the degree of appetite suppression on any given day. The medication is still working. The fluctuations happen on top of a baseline that remains lower than your pre-treatment hunger level.
Can tirzepatide work again after a plateau?
Yes. Many people break through plateaus and resume weight loss through dose escalation, lifestyle optimization, or simply time. The SURMOUNT trial data shows that people who continued treatment beyond their initial plateau often achieved additional weight loss. Patience and strategic intervention are key.
External resources
For researchers serious about optimizing their protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Whether you are breaking through a plateau or building a long-term maintenance strategy, SeekPeptides members access detailed protocol builders, dosing calculators, and expert-reviewed guidance that accounts for individual factors most resources ignore.
In case I do not see you, good afternoon, good evening, and good night. May your plateaus stay temporary, your metabolism stay resilient, and your results stay worth the patience.