Feb 27, 2026

Your mouth feels like sandpaper. You woke up at 3 AM with your tongue stuck to the roof of your mouth, reached for water, and realized this is the fourth night in a row. Nobody warned you about this when you started tirzepatide. The nausea warnings were everywhere. The constipation advice was abundant. But dry mouth? That one caught you off guard.
You are not imagining it. And you are not alone. While gastrointestinal side effects dominate the clinical trial headlines, dry mouth quietly affects a meaningful number of people taking GLP-1 medications. The medical term is xerostomia, and it ranges from mildly annoying to genuinely disruptive. Some people notice a subtle dryness that comes and goes. Others wake up unable to swallow, deal with cracked lips throughout the day, or find that food tastes different because their saliva has all but disappeared.
Here is what makes this side effect tricky. It is not officially listed among the most common adverse events in tirzepatide clinical trials. That does not mean it is not happening. Post-marketing surveillance data, pharmacovigilance reports, and thousands of patient accounts tell a different story. A study published in Biology analyzing GLP-1 receptor signaling found elevated reporting odds ratios for dry mouth across the entire drug class, with tirzepatide showing a ratio of 1.35. That means people taking tirzepatide report dry mouth 35% more often than expected compared to other medications.
This guide covers everything you need to know. Why tirzepatide causes dry mouth in the first place. The biological mechanisms at work. How to tell if your dry mouth is medication-related or something else entirely. And most importantly, 15 proven strategies to get relief, from simple hydration adjustments to prescription-grade solutions that your doctor may not have mentioned. Whether you are on your starting dose or well into your dosing protocol, understanding this side effect can save your teeth, your comfort, and your willingness to stick with treatment.

What dry mouth actually means (and why it matters more than you think)
Dry mouth sounds trivial. It is not.
Saliva does far more than keep your mouth comfortable. It contains enzymes that begin the digestion process before food even reaches your stomach. It maintains a neutral pH that protects tooth enamel from acid erosion. It carries antimicrobial proteins that fight bacteria, fungi, and viruses in your oral cavity. It lubricates tissues so you can speak, chew, and swallow without pain. When saliva production drops, every single one of these protective functions declines.
The clinical definition of xerostomia is the subjective sensation of oral dryness. Hyposalivation, a related but distinct condition, refers to objectively reduced salivary flow, typically measured at less than 0.1 mL per minute for unstimulated whole saliva. You can have xerostomia without measurable hyposalivation, meaning your mouth feels dry even though your salivary glands are technically producing adequate fluid. This distinction matters because it affects which remedies and supplements will actually help.
In the general population, xerostomia prevalence ranges from 5.5% to 46%, depending on the population studied and the definition used. It becomes more common with age, affects women more than men, and is strongly associated with medication use. Over 500 commonly prescribed medications list dry mouth as a potential side effect. Now add GLP-1 medications to that list.
The consequences of ignoring dry mouth
Left unmanaged, chronic dry mouth creates a cascade of oral health problems. Without adequate saliva to buffer acids and remineralize enamel, tooth decay accelerates dramatically. Dentists call this "rampant caries," and it can develop in as little as three months of persistent dry mouth. Gum disease progresses faster without saliva's antimicrobial properties. Oral thrush, a fungal infection caused by candida overgrowth, becomes more likely because saliva normally keeps fungal populations in check.
Then there are the quality-of-life impacts. Difficulty speaking for extended periods. Pain while eating, particularly dry or acidic foods. Persistent bad breath that no amount of brushing resolves. Cracked, bleeding lips. A burning sensation on the tongue. Sleep disruption from nighttime dryness. These are not minor inconveniences. They are the kinds of problems that make people consider stopping their medication entirely, which is exactly why managing dry mouth proactively matters so much.
Why tirzepatide causes dry mouth: the complete science
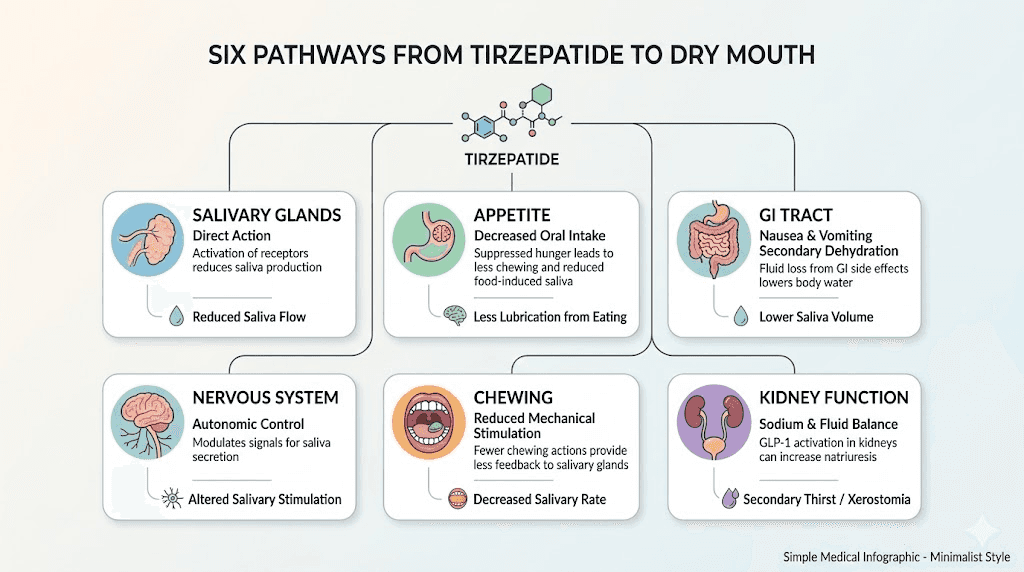
There is no single reason tirzepatide leads to dry mouth. Multiple mechanisms work together, and understanding each one helps you target the right solution. Let me break down every pathway researchers have identified.
Mechanism 1: Direct GLP-1 receptor activation in salivary glands
This is the most recently discovered and possibly the most important mechanism. GLP-1 receptors are not limited to the pancreas and brain. They are expressed in salivary gland tissue. When tirzepatide activates these receptors, it may directly alter how your salivary glands produce and secrete saliva.
A narrative review published in Biology (MDPI, analyzing data from 78 studies) examined the mechanistic basis of GLP-1 receptor agonist-related oral adverse effects. The researchers identified five distinct mechanistic domains linking GLP-1 receptor activation to changes in salivary function. This represents a genuine pharmacological effect, not just a side effect of dehydration or reduced eating.
Tirzepatide is a dual GIP/GLP-1 receptor agonist, meaning it activates both glucose-dependent insulinotropic polypeptide receptors and GLP-1 receptors simultaneously. This dual mechanism, which makes it uniquely effective for weight loss, may also explain why some people experience more pronounced oral dryness compared to pure GLP-1 agonists like semaglutide.
Mechanism 2: Reduced fluid intake from appetite suppression
Tirzepatide powerfully suppresses appetite. When you eat less, you also tend to drink less. Many people do not realize how much of their daily fluid intake comes bundled with meals. That glass of water at dinner. The coffee with breakfast. The soup at lunch. When tirzepatide shrinks your appetite and you skip meals or eat smaller portions, your total fluid intake drops without you noticing.
The math is straightforward. About 20% of daily water intake comes from food. If tirzepatide reduces your food consumption by 30-40%, which is typical based on clinical trial data, you are losing a significant chunk of water intake before you even consider whether you are drinking enough between meals. And most people were not drinking enough to begin with.
Mechanism 3: Gastrointestinal fluid losses
Nausea, vomiting, and diarrhea are among the most commonly reported side effects of tirzepatide, particularly during dose escalation. Each of these depletes body water. Vomiting can cause significant acute fluid loss. Diarrhea pulls water from the intestinal lining. Even persistent nausea, without vomiting, often reduces the desire to drink fluids.
A case series published in Medicine (Baltimore) documented three patients who developed clinically significant hyposalivation while taking a GLP-1 receptor agonist. The researchers specifically investigated and ruled out dehydration from GI side effects as the sole cause, but acknowledged it as a contributing factor. One patient saw salivary flow drop from 30 mL (normal) to just 8 mL at three minutes on the modified Schirmer test. That is a 73% reduction in saliva production.
Mechanism 4: Autonomic nervous system changes
Saliva production is controlled by the autonomic nervous system, specifically the parasympathetic branch. GLP-1 receptor activation can influence autonomic signaling, potentially shifting the balance in ways that reduce the neural drive to salivary glands. This is the same system that controls your heart rate, digestion, and pupil dilation. Small changes in autonomic tone can have widespread effects, and reduced salivary stimulation is one of them.
This mechanism may explain why some people experience dry mouth that does not fully resolve with increased water intake. You can be perfectly hydrated and still have reduced salivary flow if the neural signals driving production are dampened.
Mechanism 5: Reduced chewing and mechanical stimulation
Chewing is one of the most powerful stimulants of saliva production. When you eat less food, eat softer foods because of nausea, or chew less thoroughly because of food aversions, your salivary glands receive less mechanical stimulation. It is a use-it-or-lose-it system. Glands that are not regularly stimulated produce less saliva over time, creating a negative feedback loop where eating less leads to less saliva, which makes eating more uncomfortable, which makes you eat even less.
This is particularly relevant during the early weeks of treatment when appetite suppression is most dramatic and many people dramatically reduce their food intake. The foods you choose during this period can significantly influence how much mechanical stimulation your salivary glands receive.
Mechanism 6: Diuretic and natriuretic effects
GLP-1 receptor agonists have documented diuretic and natriuretic properties. They increase sodium excretion through the kidneys, which pulls water along with it. This mild but persistent fluid loss contributes to overall dehydration if not compensated with adequate water intake. The case series in Medicine specifically highlighted this mechanism, noting that the body water loss associated with GLP-1 agonists may be more significant than commonly appreciated.
Think of it this way. Your body is losing slightly more water through your kidneys than it did before you started tirzepatide. Your appetite is reduced, so you are taking in less water from food and drinks. And your salivary glands may be receiving less stimulation from both neural signals and mechanical chewing. Multiple small deficits compound into noticeable dryness.
When dry mouth typically starts (and the dose connection)
Timing matters. Understanding when dry mouth is most likely to appear helps you prepare and respond effectively.
The dose escalation pattern
Most people who develop dry mouth from tirzepatide notice it during one of two windows. The first is within the initial two to four weeks of starting treatment, when the body is adjusting to GLP-1 receptor activation for the first time. The second is after a dose increase, when receptor stimulation intensifies.
The standard tirzepatide dosing protocol starts at 2.5 mg weekly and escalates in 2.5 mg increments every four weeks, potentially reaching 15 mg. Each step up brings a temporary intensification of side effects as your body adapts to the higher receptor activation. Dry mouth often follows this staircase pattern, appearing or worsening for one to two weeks after each dose increase before gradually improving.
In the case series from Medicine, symptom onset varied considerably. One patient developed symptoms at two weeks. Another at eight weeks. A third at twelve weeks. This variability suggests individual differences in GLP-1 receptor expression in salivary glands, baseline hydration status, and overall sensitivity to the medication.
Does it get better with time?
For many people, yes. The body adapts to GLP-1 receptor activation over time, a process called tachyphylaxis. Side effects that are pronounced during the first months of treatment often diminish as receptors downregulate and the body finds a new equilibrium. Community reports consistently describe dry mouth as most severe during the first few days after each injection, tapering as the week progresses.
But not everyone adapts equally. Some people experience persistent dry mouth throughout treatment, particularly at higher doses. The dose-response relationship is important here. If your dry mouth is manageable at 5 mg but unbearable at 10 mg, that information is clinically useful and worth discussing with your healthcare provider. Microdosing approaches or split dosing strategies may help maintain efficacy while reducing oral dryness.
How to tell if your dry mouth is from tirzepatide
Not all dry mouth is medication-related. Before attributing your symptoms entirely to tirzepatide, consider these differential factors.
Medication timing correlation
The strongest indicator is temporal correlation with your injection schedule. If your dry mouth is worst in the 24-72 hours after your weekly tirzepatide injection and improves toward the end of the week, the medication is almost certainly a factor. Track this pattern over two to three injection cycles to confirm.
Other medications
Over 500 medications can cause dry mouth. Antihistamines, antidepressants, blood pressure medications, decongestants, pain medications, and muscle relaxants are among the most common culprits. If you started tirzepatide around the same time as another new medication, the dry mouth might be coming from the other drug, or from the combination.
Medical conditions to rule out
Certain conditions cause dry mouth independently of medication. Sjogren syndrome is an autoimmune condition that attacks salivary and tear glands. Diabetes, particularly when blood sugar is poorly controlled, causes dehydration-related dry mouth. Thyroid disorders, anxiety, depression, and mouth breathing during sleep can all contribute. If your dry mouth is severe and does not respond to hydration, your healthcare provider may want to run some basic tests to rule out underlying conditions.
The hydration test
Here is a simple way to gauge whether dehydration is the primary driver. For three consecutive days, drink at least 3 liters of water spread evenly throughout the day. Monitor your urine color, aiming for pale yellow. If your dry mouth improves significantly, dehydration from reduced intake is likely the main issue. If it persists despite excellent hydration, the mechanism is more likely direct GLP-1 receptor effects on salivary glands.
15 proven remedies for tirzepatide dry mouth
These strategies range from simple behavioral changes to prescription interventions. Start with the first tier and add more aggressive approaches as needed.
Tier 1: Hydration and behavioral changes
1. Strategic water intake throughout the day
This is the foundation. Not just "drink more water" but a structured approach. Set a baseline of 2.5 to 3 liters daily, which is higher than the standard recommendation because tirzepatide increases your fluid needs through multiple mechanisms. Spread intake evenly rather than drinking large amounts at once. Your body can only absorb about 200-300 mL of water per 15-minute period, so chugging a liter will just send most of it to your bladder. Sip consistently. Set hourly reminders on your phone if needed.
Here is the critical point many people miss. Tirzepatide can suppress thirst along with appetite. You may not feel thirsty even when you are significantly dehydrated. Do not rely on thirst as your hydration guide. Drink on a schedule, not on demand.
2. Electrolyte-enhanced hydration
Plain water is not always enough. Electrolytes, particularly sodium, potassium, and magnesium, help your body retain and distribute water effectively. Tirzepatide's natriuretic effects mean you are losing more sodium through your kidneys, which can impair water retention even when you are drinking adequate fluid. Adding an electrolyte supplement to one or two of your daily water servings can make a measurable difference.
Look for electrolyte mixes without added sugar. Sugar-free options with sodium (300-500 mg per serving), potassium (100-200 mg), and magnesium (50-100 mg) are ideal. Many supplement protocols for tirzepatide users now include electrolytes as a standard recommendation, not just for dry mouth but for overall hydration support.
3. Water-rich foods
Even though your appetite is reduced, prioritizing high-water-content foods serves double duty. They contribute to hydration and provide mechanical stimulation for salivary glands. Cucumbers contain about 95% water. Watermelon sits around 92%. Celery, strawberries, lettuce, and tomatoes all exceed 90% water content. Including these in your tirzepatide diet plan helps compensate for reduced fluid intake from eating less overall.
Broths and soups are particularly effective because they combine hydration, electrolytes, and warmth. A warm broth is often more palatable than cold water when nausea is present, and the sodium content supports fluid retention.
4. Avoid dehydrating beverages and substances
Caffeine is a mild diuretic. Alcohol is a stronger one. Both reduce saliva production and increase fluid loss. If dry mouth is a significant problem, limiting coffee to one to two cups daily and reducing alcohol consumption can make a noticeable difference. Smoking and vaping also contribute to oral dryness by irritating and dehydrating mucosal tissues. If you needed another reason to quit, dry mouth management is one.
Tier 2: Saliva stimulation techniques
5. Sugar-free xylitol gum
Chewing gum is one of the most effective saliva stimulants available without a prescription. The chewing motion mechanically stimulates salivary glands, and xylitol provides additional benefits. It inhibits the growth of Streptococcus mutans, the primary bacterium responsible for tooth decay. This is particularly important when dry mouth has already compromised your natural defenses.
Chew xylitol gum for 10-15 minutes after meals and whenever dryness becomes uncomfortable. Johns Hopkins Medicine and the Mayo Clinic both recommend sugar-free gum as a first-line intervention for xerostomia.
6. Sugar-free lozenges and hard candies
For times when chewing gum is not practical, sugar-free lozenges provide sustained saliva stimulation. The slow dissolution keeps salivary glands active for an extended period. Look for products containing xylitol or citric acid, both of which stimulate salivary flow. Avoid anything with sugar, which would accelerate the tooth decay that dry mouth already predisposes you to.
7. Sour or tart flavors
Sour and tart flavors are the most potent gustatory stimulants of saliva production. A small piece of lemon in your water, a few drops of lemon juice on your tongue, or sugar-free sour candies can trigger a powerful salivary response. This approach works by activating taste receptors that send neural signals directly to salivary glands, bypassing the mechanisms that tirzepatide may be dampening.
Use this strategically before meals. A burst of sour flavor one to two minutes before eating primes your salivary glands and makes the meal more comfortable.
8. Ginger
Ginger is a well-documented herbal sialagogue, meaning it naturally stimulates saliva production. Fresh ginger root, ginger tea, or ginger candies can help. This is a convenient solution because ginger also helps with nausea management, addressing two common tirzepatide side effects simultaneously. Brew fresh ginger slices in hot water for a tea that both soothes the stomach and moistens the mouth.
Tier 3: Over-the-counter products
9. Biotene products (rinse, gel, spray)
Biotene is the most widely recommended over-the-counter product line for dry mouth. Their formulations contain enzymes that mimic the natural protective properties of saliva, including lysozyme, lactoferrin, and lactoperoxidase. The moisturizing gel can be applied directly to oral tissues and provides relief for several hours. The mouth rinse offers a gentler clean than alcohol-based mouthwashes, which actually worsen dry mouth.
Use the rinse twice daily in place of conventional mouthwash. Apply the gel to the roof of your mouth and tongue before bed for nighttime relief. Keep the spray bottle with you for on-the-go relief throughout the day.
10. Saliva substitute sprays
Prescription and over-the-counter saliva substitutes like Aquoral contain ingredients that replicate the lubricating and protective properties of natural saliva. These are particularly useful for people whose dry mouth stems from reduced salivary gland function rather than simple dehydration. They coat oral tissues with a protective film that retains moisture for extended periods.
Aquoral specifically has positioned itself for GLP-1 medication users, recognizing the growing need in this population. Their spray formulation is convenient and provides rapid relief when dryness becomes uncomfortable.
11. Alcohol-free mouthwash
If you are using a conventional mouthwash containing alcohol, stop immediately. Alcohol is a potent desiccant that strips moisture from oral tissues and worsens dry mouth significantly. Switch to an alcohol-free formulation. Look for mouthwashes containing fluoride to provide the cavity protection that your reduced saliva can no longer fully deliver.
12. Fluoride toothpaste and treatments
With dry mouth, your teeth lose their primary defense against decay. Compensate with enhanced fluoride protection. Use a high-fluoride prescription toothpaste if your dentist recommends one. Apply fluoride gel trays at night. Consider adding a fluoride rinse to your routine. This does not fix the dry mouth itself, but it protects against the most serious long-term consequence.
Tier 4: Environmental and nighttime strategies
13. Bedroom humidifier
Dry mouth is almost always worst at night. During sleep, saliva production naturally decreases, and many people unconsciously breathe through their mouth, which accelerates oral drying. Running a humidifier in your bedroom adds moisture to the air and significantly reduces nighttime dryness. Aim for 40-50% relative humidity. Too much moisture encourages mold growth, so a hygrometer to monitor levels is a worthwhile investment.
Cool-mist humidifiers are generally recommended over warm-mist types for safety reasons, particularly if you have children or pets. Clean the unit weekly to prevent bacterial and fungal growth.
14. Nasal breathing during sleep
Mouth breathing dramatically worsens dry mouth by allowing air to flow directly over oral tissues, evaporating moisture. If you snore or wake with an extremely dry mouth, you are likely a mouth breather during sleep. Nasal strips, which physically open the nasal passages, can help redirect breathing through the nose. Some people use mouth tape (specifically designed medical tape, not household tape) to gently encourage nasal breathing during sleep. Consult with a sleep specialist if you suspect obstructive sleep apnea, which commonly causes mouth breathing.
GLP-1 receptor agonists have a documented association with nasopharyngitis (inflammation of the nasal passages), which can further promote mouth breathing. If you develop nasal congestion alongside dry mouth, treating the congestion with saline spray may help both symptoms.
15. Nighttime moisture routine
Before bed, apply a generous amount of Biotene moisturizing gel or similar product to the roof of your mouth, inner cheeks, and tongue. Apply a hydrating lip balm to prevent cracked lips. Keep water on your nightstand for inevitable middle-of-the-night dryness. Some people find that a light coating of coconut oil on the lips before sleep prevents the worst of the nighttime cracking.
Tier 5: Prescription and medical interventions
When over-the-counter solutions are not enough
If Tiers 1 through 4 do not provide adequate relief, prescription options exist. In the published case series, one patient was successfully treated with pilocarpine 5 mg daily. Pilocarpine is a cholinergic agonist that directly stimulates salivary gland secretion. It is FDA-approved for treating dry mouth caused by Sjogren syndrome and radiation therapy, and healthcare providers can prescribe it off-label for medication-induced xerostomia.
Cevimeline is another prescription sialagogue that works through a similar mechanism but with potentially fewer cardiovascular side effects than pilocarpine. Both medications typically produce noticeable improvement within one to two weeks.
In the case series, the patient treated with pilocarpine while continuing her GLP-1 agonist saw salivary flow recover from 9 mL to 25 mL on the modified Schirmer test within four weeks. That is nearly a threefold improvement without having to stop the weight loss medication. Another patient who discontinued the GLP-1 agonist saw complete recovery to 30 mL within four weeks. And a third patient who continued the medication with conservative management (hydration and saliva substitutes) saw gradual recovery over 16 weeks.
Talk to your healthcare provider if your dry mouth is severe, persistent despite basic measures, or causing dental problems. The conversation should include your current tirzepatide dose, whether dose adjustment or split dosing might help, and whether a prescription sialagogue is appropriate.
The dental emergency most people do not see coming
Dentists are sounding alarms about a pattern they are calling "Ozempic teeth." Patients on GLP-1 medications are showing up with rapid-onset dental decay, enamel erosion, and gum disease at rates their dentists have not seen before. The common denominator is dry mouth.
Saliva is your teeth's first line of defense. It neutralizes acids produced by oral bacteria. It delivers calcium, phosphate, and fluoride ions that actively repair early enamel damage in a process called remineralization. It physically washes away food particles and bacteria. When saliva disappears, you lose all three of these protective mechanisms simultaneously.
How fast dental damage can happen
Rampant caries can develop in as little as three months of persistent dry mouth. That is not a typo. Three months. The acid produced by oral bacteria in the absence of saliva's buffering capacity can demineralize enamel at an alarming rate, creating cavities in locations where you have never had them before, including the root surfaces of teeth and the smooth surfaces between teeth.
Gum disease also accelerates. Without saliva's antimicrobial proteins, bacterial biofilms (plaque) accumulate more rapidly and trigger a stronger inflammatory response. Gingivitis can progress to periodontitis, with bone loss around teeth, in a fraction of the time it would take with normal saliva flow.
Protecting your teeth during tirzepatide treatment
Whether your dry mouth is mild or severe, proactive dental care during tirzepatide treatment is essential.
Schedule dental checkups every three to four months instead of the standard six months. Tell your dentist you are taking a GLP-1 medication. Ask about prescription-strength fluoride toothpaste (5000 ppm). Consider professional fluoride varnish applications at each visit. Use an electric toothbrush with a two-minute timer. Floss daily without exception. Rinse with fluoride mouthwash at a separate time from brushing for maximum fluoride exposure.
Acid erosion from vomiting is another concern. If tirzepatide causes nausea-related vomiting, stomach acid contacting your teeth accelerates enamel wear. Do not brush immediately after vomiting. This sounds counterintuitive but brushing softened enamel actually removes it. Instead, rinse with plain water or a baking soda solution (one teaspoon in a glass of water) to neutralize the acid, then wait 30 minutes before brushing.
The nutritional dimension matters too. Rapid weight loss from tirzepatide can affect calcium, vitamin D, and other nutrient levels that are critical for tooth and bone health. Ensuring adequate intake of these nutrients through supplementation and diet supports both your skeletal and dental health during treatment.

Dry mouth by dose: what to expect at each level
Tirzepatide dosing follows a predictable escalation pattern. Here is how dry mouth typically correlates with each dose tier.
Dose | Dry mouth likelihood | Typical severity | Duration of peak symptoms |
|---|---|---|---|
2.5 mg (starting) | Low to moderate | Mild, intermittent | 1-2 weeks after initiation |
5 mg | Moderate | Mild to moderate | 1-2 weeks after increase |
7.5 mg | Moderate | Moderate | 1-2 weeks after increase |
10 mg | Moderate to high | Moderate to significant | 2-3 weeks after increase |
12.5 mg | High | Moderate to significant | 2-3 weeks after increase |
15 mg (maximum) | Highest | Can be significant | 3-4 weeks, may persist |
This table reflects general patterns from patient reports and is not a guarantee. Some people at 15 mg never experience dry mouth. Others develop it at 2.5 mg. Individual variation is significant. The key takeaway is that dose increases typically bring temporary worsening, and the body generally adapts over time.
If you are tracking your side effects alongside your dosing protocol, use a dosage calculator to ensure your measurements are accurate and your dose changes are properly timed. The unit-to-milligram conversion matters here because under- or overdosing could exacerbate side effects unnecessarily.
Tirzepatide dry mouth versus semaglutide dry mouth
If you are considering switching medications to escape dry mouth, the data may surprise you.
Pharmacovigilance data shows elevated reporting odds ratios for dry mouth across all GLP-1 receptor agonists. Semaglutide shows a ratio of 1.34. Tirzepatide shows 1.35. Exenatide shows 1.26. The differences are small and may not be clinically meaningful. Switching from tirzepatide to semaglutide or vice versa is unlikely to resolve dry mouth if the mechanism is direct GLP-1 receptor activation in salivary glands.
That said, the severity and pattern may differ. Tirzepatide's dual GIP/GLP-1 mechanism produces different side effect profiles than pure GLP-1 agonists. Some people tolerate one medication's side effects better than another's, even when the overall incidence is similar. If dry mouth is genuinely intolerable and significantly impacting your quality of life, conversion to a different GLP-1 agent is worth discussing with your provider.
Comparing the full side effect profiles of both medications can help you and your provider make an informed decision. Dry mouth should be weighed against other factors like fatigue, constipation, dizziness, and insomnia when evaluating which medication works best for your body.
Special situations and compounded formulations
Compounded tirzepatide and dry mouth
Many people use compounded tirzepatide rather than brand-name Mounjaro or Zepbound. The dry mouth risk is likely the same because the active ingredient is identical. However, compounded formulations sometimes include additional ingredients that may influence oral dryness.
Tirzepatide compounded with glycine and B12 is a common formulation. Glycine may offer some protective benefits through its role in hydration and cellular function. B12 supports nerve function, which could theoretically influence the autonomic signaling that controls salivary glands. Tirzepatide with niacinamide is another formulation that may have slightly different side effect profiles.
If you are using a compounded formulation and experiencing dry mouth, the strategies in this guide apply equally. The underlying mechanisms are the same regardless of whether your tirzepatide comes in a branded pen or a compounded vial.
Oral tirzepatide formulations
Oral tirzepatide is an emerging option that may have different implications for dry mouth. The oral route means the medication passes through the GI tract rather than being injected subcutaneously, which could alter the pharmacokinetic profile and potentially influence which side effects are more or less prominent. Early data on oral versus injectable tirzepatide is still limited, but it is worth monitoring as more results become available.
Sublingual tirzepatide drops present an interesting consideration. Because they are placed under the tongue and absorbed through oral mucosa, they have direct contact with oral tissues. Whether this increases or decreases oral dryness compared to injections is not yet well studied.
Combination supplements
Many tirzepatide supplement protocols now address dry mouth as part of a comprehensive side effect management approach. Electrolyte supplements for hydration. B vitamins for nerve function. Magnesium for muscle relaxation and hydration support. A well-designed supplement regimen may reduce the severity of multiple side effects simultaneously, including dry mouth, fatigue, body aches, and insomnia.
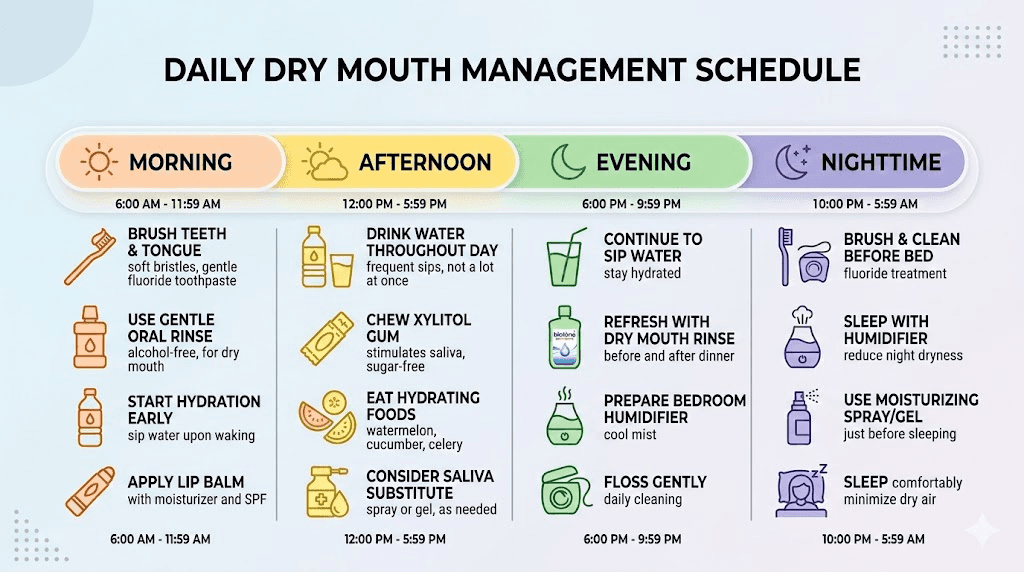
A complete daily protocol for dry mouth management
Here is a practical, time-based protocol that combines the most effective strategies into a manageable routine.
Morning routine
Start with 500 mL of water with electrolytes within 30 minutes of waking. This replenishes the fluid lost during sleep and addresses the overnight depletion of saliva. Use alcohol-free mouthwash or Biotene rinse. Brush with fluoride toothpaste using an electric toothbrush for two minutes. Have a piece of xylitol gum after breakfast if dryness persists.
Throughout the day
Sip water consistently, targeting 250-300 mL per hour. Carry a water bottle everywhere. Add a second electrolyte serving to your midday water. Use xylitol gum or lozenges between meals when dryness is noticeable. Prioritize water-rich foods at meals. Limit coffee to one to two cups before noon. Avoid alcohol or keep it minimal.
Evening routine
Complete your third liter of water by dinner time. Have ginger tea in the evening for saliva stimulation and digestive comfort. Turn on your bedroom humidifier 30 minutes before sleep. Apply Biotene gel to oral tissues. Apply lip balm. Place water on your nightstand. Use nasal strips if you tend toward mouth breathing.
Injection day protocol
On the day of your weekly tirzepatide injection, be extra vigilant. Increase water intake by 500 mL above your baseline. Have electrolytes ready. Keep xylitol gum and lozenges accessible. The 24-72 hours following injection tend to be the peak period for side effects, so front-loading your hydration and saliva stimulation efforts during this window pays dividends.
When dry mouth signals something more serious
In most cases, tirzepatide-related dry mouth is uncomfortable but manageable. Occasionally, it signals something that requires medical attention.
Signs of severe dehydration
Dry mouth combined with dark urine, dizziness when standing, rapid heartbeat, confusion, or significantly reduced urine output suggests dehydration that goes beyond simple dry mouth. The UK Medicines and Healthcare products Regulatory Agency (MHRA) has issued warnings about severe dehydration in GLP-1 users. If you experience these symptoms, increase fluids immediately and contact your healthcare provider. Severe dehydration can be dangerous and may require IV fluid replacement.
Signs of significant hyposalivation
If you notice a thick, ropy quality to your saliva, difficulty swallowing without water, food sticking to your teeth and cheeks, persistent burning on your tongue, or rapidly worsening dental problems, your salivary flow may be significantly impaired. Request a salivary flow rate test from your dentist or an oral medicine specialist. This simple test quantifies whether your production is in the normal range or clinically reduced.
Oral infections
White patches on your tongue, inner cheeks, or palate may indicate oral thrush (candidal infection), which becomes more common with dry mouth. Red, painful patches can signal other infections or inflammatory conditions. Do not ignore these symptoms. They require treatment and may need antifungal medication.
Sleep disruption
If dry mouth is causing significant sleep disruption, waking you multiple times per night, or causing you to avoid lying down, it is affecting your overall health beyond just oral comfort. Sleep deprivation compounds other tirzepatide side effects like fatigue and headaches, creating a negative spiral. Address nighttime dry mouth aggressively using humidifiers, moisture products, and nasal breathing techniques.
What the research says about long-term outcomes
The long-term trajectory of tirzepatide-related dry mouth is an area where research is still catching up to clinical experience.
From the published case series, we know that hyposalivation can resolve. One patient recovered fully within four weeks of stopping the medication. Another recovered with pilocarpine while continuing the GLP-1 agonist. A third showed gradual improvement over 16 weeks with conservative management. These outcomes suggest that the salivary gland effects are generally reversible, which is reassuring.
Longer-term data from the SURPASS and SURMOUNT clinical trial programs, which studied tirzepatide over 40-72 weeks, do not highlight dry mouth as a persistent concern. This may mean it resolves with adaptation or it may mean it was not specifically tracked as a primary endpoint. The distinction matters because adverse events that are not systematically measured often go underreported in clinical trials.
What we can say with confidence is that dry mouth appears to be dose-dependent, generally improves with time as the body adapts, responds to hydration and saliva stimulation measures in most people, and is reversible if the medication is discontinued. For the relatively small percentage of people who experience persistent, severe dry mouth despite all interventions, dose reduction or medication change remains an option.
Frequently asked questions
Does tirzepatide cause dry mouth?
Yes, though it is not listed among the most common clinical trial side effects. Post-marketing data shows a reporting odds ratio of 1.35 for dry mouth with tirzepatide, meaning it is reported more frequently than expected. The mechanisms include direct GLP-1 receptor activation in salivary glands, reduced fluid intake from appetite suppression, GI-related fluid losses, autonomic nervous system changes, reduced chewing stimulation, and mild diuretic effects.
How long does tirzepatide dry mouth last?
For most people, dry mouth is worst during the first two to four weeks of starting treatment and for one to two weeks after each dose escalation. Many people find it gradually improves as their body adapts. Some experience persistent mild dryness throughout treatment. In published case reports, salivary flow recovered within 4-16 weeks with appropriate management.
Should I stop tirzepatide because of dry mouth?
In most cases, no. Dry mouth is manageable with the strategies outlined in this guide. However, if dry mouth is severe, causing significant dental damage, not responding to interventions, or seriously affecting your quality of life, discuss dose adjustment or medication alternatives with your healthcare provider. Do not stop tirzepatide without medical guidance.
Is dry mouth worse with tirzepatide than semaglutide?
Pharmacovigilance data shows very similar reporting odds ratios: 1.35 for tirzepatide versus 1.34 for semaglutide. The difference is negligible. Switching between GLP-1 agents specifically to resolve dry mouth is unlikely to help, though individual responses vary.
Can dry mouth from tirzepatide damage my teeth?
Yes. Persistent dry mouth significantly increases the risk of tooth decay, gum disease, and enamel erosion. Without saliva's protective buffering and remineralization functions, dental damage can develop in as little as three months. Increase dental checkups to every three to four months, use fluoride products aggressively, and maintain excellent oral hygiene throughout treatment.
What is the best product for tirzepatide dry mouth?
No single product works best for everyone. Biotene moisturizing gel and rinse are the most widely recommended starting point. Xylitol gum provides excellent mechanical and chemical saliva stimulation. Electrolyte supplements address the hydration component. Most people benefit from a combination approach rather than relying on any single product.
Does dry mouth mean I am dehydrated?
Not necessarily. You can be well-hydrated and still have dry mouth from direct GLP-1 receptor effects on salivary glands. However, dehydration from reduced fluid intake and GI losses is a common contributing factor. The hydration test described earlier in this guide can help distinguish between the two causes.
Will changing my tirzepatide injection site help with dry mouth?
No. Injection site does not influence systemic side effects like dry mouth. Whether you inject in your abdomen, thigh, or upper arm, the medication reaches the same blood levels and activates the same receptors throughout your body. Injection site reactions are local effects, while dry mouth is a systemic one.
External resources
For researchers serious about optimizing their peptide protocols and managing side effects effectively, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members get access to detailed side effect management protocols, interaction databases, and personalized support from experienced researchers who understand the real-world challenges of GLP-1 therapy.
In case I do not see you, good afternoon, good evening, and good night. May your saliva stay flowing, your teeth stay protected, and your hydration stay consistent.