Feb 20, 2026

What if you could lose weight on semaglutide without ever stepping foot in a gym? What if the medication handled everything, the appetite, the cravings, the metabolic machinery, and all you had to do was take your weekly injection? That question haunts thousands of people considering semaglutide for weight loss but struggling with physical limitations, packed schedules, or a genuine hatred of treadmills. And the short answer might surprise you.
Yes. You can lose weight on semaglutide without exercise.
But that simple answer hides enormous complexity. How much weight? What kind of weight? Fat or muscle? And what happens six months, twelve months, two years down the road when the body starts fighting back? The clinical trials tell one story. Real-world data tells another. And the gap between them is where most people get stuck, losing some weight but not enough, or losing weight in ways that leave them weaker, slower, and more likely to regain everything. This guide breaks down exactly what happens when you take semaglutide without exercise, what the research shows about outcomes with and without physical activity, how to protect your muscle mass even if you never lift a weight, and the specific strategies that maximize results for people who cannot or choose not to exercise. Whether you are dealing with a physical limitation, a demanding schedule, or just looking for honest answers about what semaglutide can do on its own, the data is here. All of it. Every relevant study, every practical strategy, every honest caveat. Understanding how peptides work at a fundamental level makes everything that follows much clearer.
How semaglutide produces weight loss without you lifting a finger
Before evaluating whether exercise matters, you need to understand what semaglutide is already doing inside your body. The medication works through multiple simultaneous mechanisms, and none of them require you to be physically active. Not one. This is why the medication produces results even in completely sedentary populations. The question is not whether it works without exercise. The question is how well it works, and what trade-offs emerge when physical activity is absent.
Appetite suppression at the neurological level
Semaglutide is a GLP-1 receptor agonist. It mimics a hormone your gut naturally produces after eating, glucagon-like peptide-1, but in a much more potent and long-lasting form. When it binds to GLP-1 receptors in the hypothalamus, the brain region controlling hunger and satiety, it fundamentally changes how your brain perceives food. Hunger signals diminish. Cravings quiet down. The constant mental chatter about snacking, about what to eat next, about whether to order dessert, all of it fades into background noise. People describe it as food becoming less interesting. Not repulsive. Just neutral. The timeline for appetite suppression varies widely between individuals, but most people notice some reduction within the first two weeks, with full effects appearing at therapeutic doses around 1.7 to 2.4 mg.
This mechanism alone accounts for most of the weight loss. When you eat less because you genuinely want less, the caloric deficit happens almost automatically. No meal planning. No willpower battles. No exercise required.
Delayed gastric emptying
Semaglutide slows how quickly food leaves your stomach. A meal that normally passes through in two to three hours might linger for four to five. The result is prolonged physical fullness after eating. A small lunch keeps you satisfied well into the evening. This mechanism is separate from the neurological appetite suppression, meaning you get a double effect. Your brain wants less food AND your stomach feels full longer. The downside is that this same mechanism causes the most common side effects, including constipation, nausea, bloating, and excessive burping. Food sits in the digestive tract longer than the body expects. For most people, these effects are mild and temporary. For some, they are the main reason results happen, because eating large meals becomes physically uncomfortable.
Blood sugar regulation and insulin dynamics
Originally developed for type 2 diabetes, semaglutide regulates blood sugar through dual action. It stimulates insulin release when glucose is elevated and suppresses glucagon, the hormone that tells your liver to dump stored sugar into the bloodstream. The net effect is stable blood sugar throughout the day. Why does this matter for weight loss without exercise? Because unstable blood sugar drives cravings. The crash-and-binge cycle, where blood sugar spikes after a carbohydrate-heavy meal then plummets an hour later, triggering urgent hunger, is one of the most powerful drivers of overeating. Semaglutide flattens that cycle. Fewer crashes mean fewer cravings. Fewer cravings mean easier adherence to a caloric deficit, even without the additional calorie burn that exercise provides. Understanding this relationship between hormonal balance and peptide therapies provides critical context for managing weight.
What semaglutide does NOT do
This is where expectations need recalibrating. Semaglutide does not increase your metabolic rate. Research from the STEP trials shows that resting metabolic rate, adjusted for lean body mass, does not meaningfully change between semaglutide users and placebo groups. The medication does not burn fat directly. It does not build muscle. It does not improve cardiovascular fitness, increase bone density, or enhance physical endurance. It creates conditions, reduced appetite, slower digestion, stable blood sugar, that make a caloric deficit easier to achieve. But the deficit itself still has to happen. And exercise, which would normally expand that deficit and improve body composition, is simply not part of the equation when you skip it. The weight loss still occurs. But the nature of that weight loss changes in ways that matter enormously for long-term health.
What the clinical trials actually show about exercise and semaglutide
The research is clear. Semaglutide produces significant weight loss with or without exercise. But the details matter, and most articles covering this topic cherry-pick the convenient data while ignoring the nuances that actually determine outcomes.
The STEP 1 trial: semaglutide with lifestyle intervention
The landmark STEP 1 trial, published in the New England Journal of Medicine, enrolled 1,961 adults with obesity or overweight with at least one weight-related comorbidity. Participants received either semaglutide 2.4 mg weekly or placebo, alongside a lifestyle intervention. That intervention included counseling sessions every four weeks encouraging a reduced-calorie diet and 150 minutes per week of physical activity. At 68 weeks, the semaglutide group lost an average of 14.9% of body weight compared to 2.4% in the placebo group. 86.4% of semaglutide users achieved at least 5% weight loss, and roughly one-third lost 20% or more.
Here is the critical detail most articles miss. The 150 minutes of weekly exercise was encouraged, not enforced. Adherence to the physical activity recommendation varied enormously. Some participants exercised regularly. Many did not. The trial measured outcomes across the entire group, not stratified by exercise adherence. This means the 14.9% average includes people who barely moved and people who trained consistently. The medication drove the results. Exercise was a bonus, not a requirement. You can use the semaglutide dosage calculator to understand exactly where the therapeutic dose window sits for your specific situation.
The STEP 3 trial: semaglutide with intensive behavioral therapy
STEP 3 took a different approach. Participants received semaglutide 2.4 mg plus intensive behavioral therapy, which included structured exercise programs, detailed diet counseling, and regular accountability sessions. This trial saw even greater weight loss of 16.0% versus 5.7% with placebo plus intensive behavioral therapy. The additional 1.1 percentage points compared to STEP 1 does not sound dramatic. But it represents meaningful additional fat loss, better body composition, and improved metabolic markers. The exercise component made a measurable difference, even if semaglutide was doing most of the heavy lifting. For people interested in how quickly semaglutide produces results, both trials show that the most significant weight loss occurs between months three and twelve.
The SELECT trial: cardiovascular outcomes without intensive exercise requirements
The SELECT trial focused on cardiovascular outcomes rather than weight loss as the primary endpoint. It enrolled 17,604 adults with established cardiovascular disease and overweight or obesity, but without diabetes. Participants received semaglutide 2.4 mg or placebo. The lifestyle intervention was minimal compared to STEP trials, just standard care. Weight loss averaged approximately 9.4% at week 104, lower than STEP 1 numbers but still substantial. More importantly for our question, these participants were not in structured exercise programs. They were receiving standard cardiovascular care and semaglutide. The medication still produced clinically significant weight loss, confirming that exercise is not required for the medication to work. The full timeline from first dose to peak results helps set realistic expectations regardless of exercise status.
Real-world data versus clinical trial outcomes
Clinical trials represent ideal conditions. Participants are screened, monitored, counseled, and supported in ways that real-world patients rarely experience. So what happens in actual clinical practice? A real-world retrospective study found that weight loss outcomes tend to be lower than clinical trial results. However, the key finding for our topic is striking. Sedentary behavior was not independently associated with reduced weight loss response to GLP-1 therapy. In other words, people who did not exercise still lost weight at similar rates to those who did, after controlling for other variables. This does not mean exercise is worthless. Far from it. But it does mean that semaglutide works in sedentary populations, which is enormously reassuring for people who cannot exercise due to physical limitations, chronic pain, or other barriers. Exploring realistic timelines for peptide-based results helps calibrate expectations for both active and sedentary users.
How much weight can you lose on semaglutide without exercise
Numbers. Specific numbers. That is what you want, and that is what the research provides.
Average weight loss numbers without structured exercise
Based on combined data from clinical trials and real-world studies, here is what you can realistically expect from semaglutide without a structured exercise program:
At one month (typically at 0.5 mg dose): 2 to 4% of body weight. For someone at 200 pounds, that is 4 to 8 pounds. Many people see even less during this early phase, and some see the scale move upward due to water retention or dietary changes. The first month on semaglutide is about building tolerance, not seeing dramatic results. If you are at four weeks with no weight loss, that is more common than you think.
At three months (approaching therapeutic dose): 5 to 8% of body weight. Now the appetite suppression is kicking in at full strength. A 200-pound person might be down 10 to 16 pounds. The deficit is happening naturally because hunger is genuinely reduced. No gym required.
At six months (full therapeutic dose for several months): 10 to 14% of body weight. This is where the medication hits its stride. A 200-pound person could be 20 to 28 pounds lighter. The plateau zone often starts somewhere in this window.
At twelve months: 12 to 16% of body weight in the best cases. Some people see continued loss. Others plateau and maintain. The average from STEP 1, remember, was 14.9% at 68 weeks with lifestyle intervention.
Without exercise, expect the lower end of these ranges. But the lower end is still significant. A 10% weight loss without exercise is a legitimate medical achievement. It improves blood pressure, blood sugar, cholesterol, liver fat, and cardiovascular risk markers. You do not need to hit 15% to benefit.
Medication-only versus medication-plus-exercise comparison
Research using the similar GLP-1 medication liraglutide showed that patients who took the medication with exercise lost approximately 21 pounds more than placebo, while those who took the medication without exercise lost approximately 15 pounds more than placebo. That is a meaningful gap, about 6 pounds difference, but not a disqualifying one. The medication alone still produced substantial weight loss. Another way to look at it: exercise added roughly 28% more weight loss on top of what the medication achieved alone. Significant, but the medication was responsible for the vast majority of results either way.
For people exploring the best peptides for weight loss, understanding this exercise-independence is valuable. Many peptide-based weight loss approaches share similar characteristics, producing results through metabolic and appetite mechanisms rather than requiring physical exertion.
Timeline expectations without exercise
Without exercise, weight loss follows a predictable pattern, but it is not a straight line down.
Weeks 1 to 4: Minimal visible change. The dose is sub-therapeutic. You might notice slightly reduced appetite. The scale might barely move. This is normal. Do not panic. Do not conclude the medication is not working.
Weeks 5 to 12: Gradual acceleration. As the dose increases toward 1.7 to 2.4 mg, appetite suppression becomes more noticeable. Weight loss of 1 to 2 pounds per week is typical.
Weeks 13 to 26: Peak loss period. This is where the most dramatic changes occur. The medication is at full strength, habits have adjusted, and the caloric deficit is consistent. Without exercise, expect the lower end of the 1 to 2 pounds per week range.
Weeks 27 to 52: Plateau zone. Metabolic adaptation begins fighting back. Weight loss slows or stops temporarily. This happens to everyone, exercisers and non-exercisers alike, but exercise provides additional tools for breaking plateaus that sedentary users lack. The semaglutide plateau guide covers specific strategies for pushing through this phase.
Weeks 53 and beyond: Maintenance and slow continued loss. The STEP 5 trial showed weight loss continued through 104 weeks, but at a much slower rate. Without exercise, maintaining the loss becomes the primary challenge. Understanding how long to stay on semaglutide helps frame these longer-term expectations.
The body composition problem nobody talks about
Here is where the story gets complicated. And honest.
Weight loss and fat loss are not the same thing. The scale does not distinguish between fat, muscle, water, bone, and the food sitting in your digestive tract. When you lose 30 pounds, the critical question is: what exactly did you lose? And this is where skipping exercise creates a real, measurable problem.
What happens to muscle mass on semaglutide without exercise
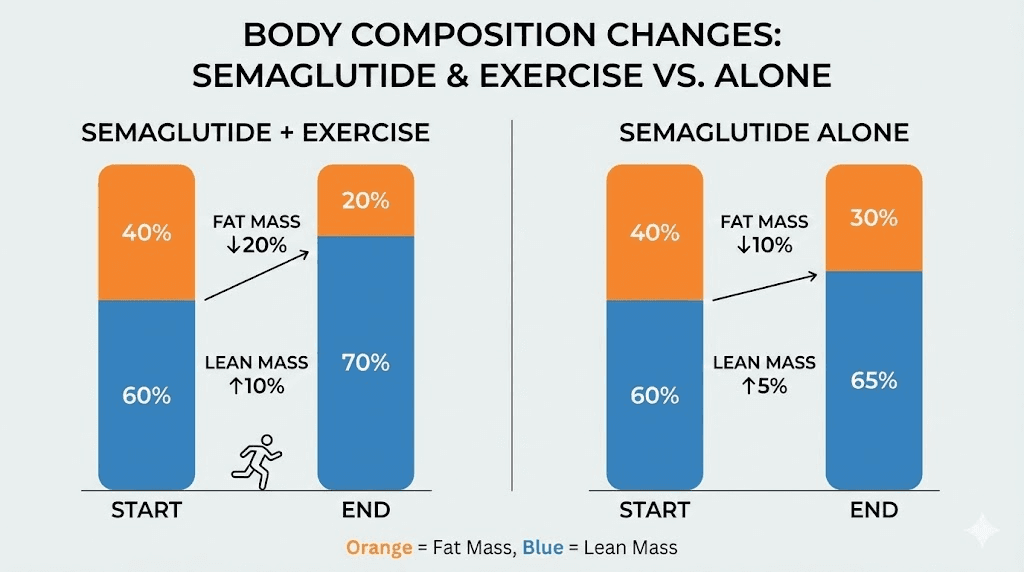
An exploratory analysis of the STEP 1 trial revealed the body composition details that the headline numbers hide. Participants on semaglutide experienced a 19.3% reduction in total fat mass and a 27.4% reduction in visceral fat mass, the dangerous fat around organs. But they also lost 9.7% of total lean body mass. And some analyses suggest that approximately 40% of the weight lost from semaglutide comes from lean mass, including muscle.
Forty percent. That is not a rounding error. That is nearly half the weight you lose coming from the tissue that keeps your metabolism running, your bones supported, and your body functional.
Without exercise, this ratio gets worse. A systematic review of semaglutide and lean mass noted that concerns arise from notable reductions in lean mass, especially in larger trials with longer durations. Another study found that GLP-1 treatment led to a 13.9% loss of lean muscle mass, equivalent to approximately 15 pounds of muscle tissue. In inactive patients, that muscle loss accelerates. The body, receiving fewer calories and no stimulus to maintain muscle, cannibalizes its own tissue for energy. This is not a semaglutide-specific problem. It happens with any weight loss method that does not include resistance training. But semaglutide makes it more concerning because the appetite suppression can be so powerful that people eat significantly less protein, further accelerating muscle breakdown. The protein shake guide for GLP-1 users addresses this specific challenge with practical solutions.
Lean mass versus fat mass ratio explained
The news is not all bad. Despite the absolute decrease in lean mass, the STEP 1 body composition analysis showed that the proportion of lean body mass relative to total body weight actually increased by 3 percentage points. The lean-to-fat mass ratio improved, and this improvement was greater in participants who lost more weight.
What does this mean practically? If you started at 200 pounds with 30% body fat (60 pounds of fat, 140 pounds of lean mass), and you lost 30 pounds, your new weight of 170 pounds might break down to roughly 42 pounds of fat and 128 pounds of lean mass. You lost 18 pounds of fat and 12 pounds of lean mass. Your body fat percentage dropped from 30% to about 24.7%. You are leaner despite losing muscle.
That sounds acceptable until you consider what happens next. Those 12 pounds of lost muscle mean your resting metabolic rate has dropped. You burn fewer calories at rest. And when you eventually stop semaglutide, as most people do at some point, you will regain weight. But the weight you regain tends to be predominantly fat, not muscle. So you end up at the same weight but with worse body composition than when you started. This is the weight cycling trap that exercise helps prevent.
Why body composition matters more than the scale
Two people can weigh exactly the same and have completely different health profiles. Person A at 170 pounds with 25% body fat has a different metabolic rate, different cardiovascular risk, different functional capacity, and different long-term prognosis than Person B at 170 pounds with 35% body fat.
When you lose weight on semaglutide without exercise, you are improving your body composition, but not as much as you could be. The fat loss is real and medically significant. The improvement in metabolic markers is genuine. But the simultaneous muscle loss creates a fragility that becomes apparent when you try to maintain the weight loss long-term, return to normal eating patterns, or handle the physical demands of daily life. Muscle recovery strategies become increasingly important as weight loss progresses, especially for people not engaging in regular resistance training. Those studying peptides for muscle growth understand how valuable preserved lean mass is during any weight loss protocol.
Why exercise still matters even if you skip the gym
This section is not meant to guilt you into exercising. It is meant to give you honest data so you can make informed decisions about your health.
Muscle preservation and metabolic rate
Resistance training sends a signal to your body: this muscle is being used, do not break it down for energy. Without that signal, your body has no reason to preserve expensive, metabolically active tissue during a caloric deficit. Each pound of muscle burns approximately 6 to 7 calories per day at rest. Lose 15 pounds of muscle and your resting metabolic rate drops by roughly 90 to 105 calories daily. That does not sound like much until you realize it compounds. Over a year, that is 33,000 to 38,000 fewer calories burned. Roughly 9 to 11 pounds of fat that would have been burned but was not, simply because of lost muscle.
Research from the Endocrine Society found that combining a high-protein diet with consistent exercise during GLP-1 treatment produced the greatest benefit in preserving bone and muscle mass, compared to diet alone or high protein alone. Exercise is the single most effective tool for preventing the metabolic slowdown that accompanies weight loss. Without it, you need other strategies to compensate, and while those strategies help, they do not fully replace what exercise provides. Understanding how GLP-1 medications interact with metabolism provides additional context for these dynamics.
Cardiovascular health benefits
Semaglutide reduces cardiovascular risk through weight loss, blood sugar regulation, and anti-inflammatory effects. The SELECT trial demonstrated a 20% reduction in major adverse cardiovascular events. But exercise provides cardiovascular benefits that semaglutide cannot replicate. Improved cardiac output, stronger heart muscle, better blood vessel elasticity, enhanced oxygen delivery to tissues, and reduced resting heart rate all require physical activity. You cannot get these benefits from a pill or injection. If cardiovascular health is a priority, and for anyone with overweight or obesity it absolutely should be, exercise adds a dimension of protection that the medication alone cannot provide. The athletic performance resources cover how physical activity integrates with various peptide protocols.
Long-term weight maintenance
This is the strongest argument for exercise alongside semaglutide. Study after study shows that weight regain after stopping GLP-1 medications is substantial. The STEP 1 extension trial found that participants regained approximately two-thirds of their lost weight within one year of stopping semaglutide. Exercise is the single best predictor of long-term weight maintenance. Not because it burns massive calories, though it helps, but because it preserves the metabolic machinery (muscle) that allows your body to maintain a lower weight without constant hunger and cravings. People who exercise regularly are far more likely to maintain weight loss after stopping any intervention, pharmaceutical or otherwise. If you plan to take semaglutide indefinitely, the exercise argument is less urgent. But if you plan to eventually stop, building an exercise habit while on the medication, when appetite is suppressed and energy levels are stable, is one of the smartest long-term investments you can make. The semaglutide withdrawal guide covers what happens when you discontinue.
Mental health and stress reduction
Exercise reduces cortisol, the stress hormone that promotes visceral fat storage. It boosts serotonin and endorphins, improving mood and reducing emotional eating. It improves sleep quality, which directly impacts hunger hormones. And it builds self-efficacy, the belief that you can influence your own health outcomes. None of these benefits come from semaglutide. The medication handles appetite. Exercise handles everything else. For people dealing with semaglutide-related fatigue, light exercise can actually help improve energy levels. The mental health dimensions of peptide protocols further illuminate this connection between physical activity and psychological well-being.
Practical strategies to maximize results without traditional exercise
If you cannot exercise, will not exercise, or are building up to exercise, these strategies help maximize your semaglutide results while mitigating the downsides of a sedentary approach. None of them fully replace exercise. But they collectively reduce the gap between exercising and non-exercising outcomes.
Protein intake: the non-negotiable foundation
If you do nothing else from this guide, do this. Eat more protein.
Research from the Endocrine Society presented at ENDO 2025 found that higher protein intake significantly protected against muscle loss in semaglutide users. Being older, female, or eating less protein was linked to greater muscle loss. The protective effect of protein was independent of exercise status, meaning even sedentary people who ate enough protein preserved more muscle than those who did not.
How much is enough? Aim for 1.2 to 1.6 grams of protein per kilogram of body weight daily. For a 180-pound person (82 kg), that is 98 to 131 grams per day. At the higher end, if you are doing any physical activity at all, target 1.6 to 2.2 grams per kilogram. This is challenging on semaglutide because appetite is suppressed. When you are eating less overall, every bite matters more. Prioritize protein at every meal. Start with the protein source, then add vegetables, then fill in with carbohydrates and fats as appetite allows.
Practical sources include lean meats, fish, eggs, Greek yogurt, cottage cheese, legumes, and protein supplements. The GLP-1 protein shake guide provides specific formulations optimized for people on appetite-suppressing medications. The semaglutide diet plan and list of foods to eat on semaglutide offer comprehensive nutritional frameworks built around adequate protein intake.
Walking: the exercise that does not feel like exercise
Walking is the most underrated tool in weight management. It burns calories without triggering the hunger response that intense exercise can cause. It improves insulin sensitivity. It reduces cortisol. And almost everyone can do it, regardless of fitness level, joint problems, or physical limitations. Ten thousand steps per day burns roughly 300 to 500 additional calories depending on body weight and pace. That is meaningful. Over a week, it adds up to 2,100 to 3,500 extra calories burned, equivalent to about half a pound to one pound of additional fat loss. More importantly, walking preserves more muscle than pure rest because it signals to the body that the legs, the largest muscle group, are still in use.
If 10,000 steps feels overwhelming, start with 3,000. Then add 500 per week. The goal is consistency, not intensity. A daily 20-minute walk after dinner is infinitely better than a gym membership you never use. For those exploring peptides for energy, improved activity levels often follow naturally from better energy management.
NEAT: non-exercise activity thermogenesis
NEAT encompasses all the calories you burn through daily movement that is not structured exercise. Fidgeting. Standing instead of sitting. Taking stairs instead of elevators. Cooking instead of ordering delivery. Gardening. Cleaning. Playing with your kids. These activities collectively burn 200 to 900 calories per day depending on your lifestyle, and the variation between sedentary and active people is enormous.
Increasing NEAT is one of the most effective strategies for people who do not exercise formally. Small changes compound. Standing at your desk for two hours instead of sitting burns 100 extra calories. Parking farther from the entrance and walking adds steps. Taking phone calls while pacing adds more. None of these feel like exercise. But they add up to meaningful calorie expenditure that supports the deficit semaglutide creates.
Sleep optimization
Poor sleep increases ghrelin (hunger hormone), decreases leptin (satiety hormone), impairs insulin sensitivity, elevates cortisol, and shifts food preferences toward high-calorie options. One study found that sleep-deprived individuals consumed an average of 385 additional calories per day. That single variable can erase your entire semaglutide-created caloric deficit.
Without exercise to help regulate sleep naturally, sleep hygiene becomes even more important. Consistent bedtime and wake time, even on weekends. Dark, cool bedroom. No screens for at least 30 minutes before bed. No caffeine after early afternoon. If you snore or experience daytime fatigue despite adequate sleep duration, get evaluated for sleep apnea. Treating sleep apnea can transform not just your energy levels but your entire metabolic response to semaglutide. The connection between GLP-1 medications and sleep disruption deserves attention, as some users report difficulty sleeping during dose escalation.
Stress management
Cortisol promotes visceral fat storage, increases insulin resistance, triggers comfort-food cravings, and breaks down muscle tissue. Chronic stress creates a hormonal environment that actively resists weight loss regardless of medication. Without exercise as a natural stress outlet, you need alternative strategies. Mindfulness meditation, even five minutes daily, has demonstrated cortisol-reducing effects in clinical studies. Deep breathing exercises, time in nature, social connection, and boundary-setting around stressors all contribute to lower baseline cortisol. The stress management guide covers additional strategies, and peptide approaches to anxiety and depression provide further context for the psychological dimensions of weight management.
Hydration and fiber
Dehydration mimics hunger. If you are not drinking enough water, your body may interpret thirst signals as hunger signals, leading to unnecessary eating that undermines the appetite suppression semaglutide provides. Aim for at least 8 cups daily, more if you are in a warm climate or are larger-bodied.
Fiber supports satiety, blood sugar stability, and gut health. Combined with the delayed gastric emptying from semaglutide, high-fiber foods create powerful and sustained fullness. Aim for 25 to 35 grams daily from vegetables, legumes, whole grains, and fruits. This dual focus on hydration and fiber maximizes the appetite-suppressing effects of semaglutide without requiring any physical activity.
Who should definitely add exercise to their semaglutide protocol
While semaglutide works without exercise, certain populations face significantly worse outcomes without it. If you fall into one of these categories, the argument for adding even minimal exercise becomes much stronger.
People with significant muscle loss concerns
Adults over 50 are already losing muscle at a rate of 1 to 2% per year through a process called sarcopenia. Adding semaglutide-related muscle loss on top of age-related loss creates a compounding problem. Research identified that being older and female was linked to greater muscle loss during semaglutide treatment. If you are over 50, especially if you are female, resistance training is not optional for preserving functional capacity. Even two sessions per week of bodyweight exercises, squats, wall push-ups, resistance band work, can dramatically reduce muscle loss. Exploring peptide approaches to muscle building provides additional strategies for this vulnerable population.
Those planning to discontinue semaglutide eventually
If your plan is to use semaglutide for a defined period and then stop, exercise becomes critical for long-term success. The muscle you preserve during treatment is the metabolic engine that helps you maintain your weight loss afterward. Without it, the regain trajectory is steeper and faster. Building exercise habits while appetite is suppressed and energy is available is strategically brilliant. You are essentially using the medication-created window to establish the behaviors that will sustain your results after discontinuation. The withdrawal and discontinuation guide explains why preserved muscle mass is the single most protective factor against weight regain.
People with insulin resistance or type 2 diabetes
The STEP 2 trial, which enrolled participants with type 2 diabetes, showed that 26.8% of diabetic participants on semaglutide lost less than 5% body weight, compared to just 7.6% of non-diabetic participants in STEP 1. Insulin resistance blunts semaglutide effectiveness. Exercise is one of the most potent interventions for improving insulin sensitivity, independent of weight loss. For people with significant insulin resistance, exercise does not just add calorie burn, it fundamentally improves the metabolic environment in which semaglutide operates, making the medication more effective. Understanding the broader hormonal interactions helps frame why exercise amplifies semaglutide effects in insulin-resistant populations.
What type of exercise works best with semaglutide
If you decide to add exercise, even minimal amounts, here is what produces the best results based on current evidence.
Resistance training for muscle preservation
This is the single most impactful type of exercise you can add to a semaglutide protocol. Resistance training, whether using free weights, machines, resistance bands, or bodyweight, directly signals muscles to resist breakdown during weight loss. Research shows that people who combine GLP-1 treatment with resistance training preserve significantly more lean mass than those who do diet alone or even diet plus cardio.
You do not need to become a powerlifter. Two to three sessions per week, 30 to 45 minutes each, focusing on major muscle groups (legs, back, chest, shoulders) is sufficient. If you are new to resistance training, bodyweight exercises like squats, lunges, push-ups, and rows are excellent starting points. The exercise recovery guide can help you manage any soreness from new training routines.
Walking and low-impact cardio
For cardiovascular health and additional calorie burn, walking remains the gold standard for semaglutide users. It is low-impact, accessible, and sustainable. Swimming, cycling, and elliptical machines offer similar benefits for people with joint issues. The key is choosing something you will actually do consistently. A brisk 30-minute walk five days per week provides substantial cardiovascular benefits while burning an additional 150 to 250 calories per session. Combined with semaglutide appetite suppression, this creates a meaningful expansion of the daily caloric deficit.
The minimum effective dose approach
If time and motivation are barriers, focus on the absolute minimum that produces measurable benefits. Research suggests that even one resistance training session per week preserves significantly more muscle than zero. Even 10 minutes of daily walking is meaningfully better than complete inactivity. The minimum effective dose for health benefits from exercise is surprisingly low. The key is doing something, anything, consistently rather than planning elaborate programs you never follow through on. Start absurdly small. Five minutes of bodyweight exercises. A walk around the block. Then build gradually. The appetite suppression from semaglutide means you have more energy available for movement, since you are not spending it on digestion and craving management. Use that energy advantage. For those interested in how other peptide-based fat loss approaches complement exercise, the principles are remarkably similar.
Common mistakes people make when relying on semaglutide alone
Knowing what not to do is just as important as knowing what to do. These mistakes derail results for people who rely solely on medication without exercise.
Ignoring protein requirements
This is the most damaging mistake. When appetite drops, people naturally gravitate toward whatever sounds appealing, which is often carbohydrate-heavy comfort foods or small snacks. Protein, which requires more effort to prepare and is less palatable in small quantities, gets pushed aside. The result is accelerated muscle loss on top of already-suboptimal body composition from not exercising. Every meal should start with a protein source. If you eat nothing else, eat protein. This single habit can mean the difference between losing primarily fat and losing a concerning amount of muscle. The supplement guide for GLP-1 users includes protein supplementation strategies for people struggling with appetite.
Expecting linear results
Weight loss is never a straight line. Never. The scale reflects total body weight, which fluctuates daily based on water retention, sodium intake, hormonal cycles, digestive contents, and dozens of other variables. Without the steady reinforcement of exercise progress (lifting more weight, running farther), people who rely solely on the scale become extremely vulnerable to discouragement during normal fluctuations. Track additional metrics. Waist circumference. How clothes fit. Progress photos every two to four weeks. Energy levels. Sleep quality. Lab values. These collectively paint a far more accurate picture than the scale alone. The semaglutide before and after guide shows what realistic timelines look like for different starting points.
Not tracking food intake
Semaglutide reduces appetite but does not eliminate it. Without exercise to expand the caloric deficit, the margin for error is thinner. Research consistently shows that people underestimate caloric intake by 30 to 50%. A few extra tablespoons of olive oil, a handful of nuts, a generous pour of salad dressing, these can easily add 300 to 500 untracked calories that erase the deficit semaglutide created. Even temporary tracking, two to three weeks of honest logging in an app, recalibrates your understanding of portions. The same precision that matters when using a peptide calculator applies to tracking nutritional intake. You do not have to track forever. But the data it provides is invaluable for making adjustments.
Skipping medical follow-ups
Without exercise providing its own health benefits, regular medical monitoring becomes more important. Blood work every three to six months should track thyroid function, liver enzymes, kidney function, vitamin and mineral levels (especially B12 and iron), blood sugar, and lipid panel. These markers reveal problems that the scale cannot show. Hair loss, nutritional deficiencies, and persistent fatigue are all warning signs that something in your protocol needs adjustment. The peptide safety guide covers the broader monitoring framework that applies to any weight loss intervention.
When semaglutide without exercise is not enough
Sometimes the medication alone, even with perfect dietary adherence, does not produce adequate results. Here is what to consider when you hit a wall.
Plateau strategies for non-exercisers
Plateaus are universal. They happen because your body adapts to the new caloric intake, reducing metabolic rate and adjusting hormone levels to defend against further weight loss. For people who exercise, breaking a plateau involves increasing workout intensity or volume. For non-exercisers, the options are different but still effective.
Diet breaks work by temporarily eating at maintenance calories for one to two weeks, which can partially reset some of the hormonal adaptations driving the plateau. Macronutrient shifting, moving from a higher carbohydrate diet to a higher protein and fat approach, changes the metabolic demands on your body. Meal timing adjustments, such as implementing a 16:8 intermittent fasting window, can create new metabolic stimuli without changing total intake. And sometimes, the answer is patience. Weight loss is not linear, and the scale may stall for weeks before dropping suddenly as water retention patterns shift. The comprehensive plateau-breaking guide provides step-by-step strategies.
Dose adjustments
If you have been at 2.4 mg for several months without adequate response, discuss higher doses with your healthcare provider. Some clinicians use off-label doses above 2.4 mg for patients who tolerate the medication well. The STEP UP trial evaluated semaglutide 7.2 mg and showed superior weight loss compared to 2.4 mg. Extended titration, staying at each dose for six to eight weeks instead of four, sometimes allows the body more time to respond before escalating. Use the semaglutide dosage calculator to understand where you are in the titration schedule and discuss adjustment options with your prescriber.
Alternative and combination approaches
For true non-responders, switching to tirzepatide, a dual GIP and GLP-1 receptor agonist, may produce different results. The SURMOUNT trials showed higher average weight loss (20.9% at the highest dose) compared to semaglutide STEP trials. The dual agonist mechanism provides additional metabolic pathways that some people respond to more strongly. The semaglutide vs tirzepatide comparison breaks down the differences in detail.
Combination therapy, adding phentermine, naltrexone-bupropion, or other medications alongside semaglutide, is emerging as a strategy for patients who need enhanced results. These approaches are not yet standard of care but are increasingly used in obesity medicine practices. For broader context on combining approaches, the peptide stacking guide explores how different compounds work together for optimized weight loss outcomes. Understanding how peptides compare to other interventions provides helpful context for evaluating all your options.
Making the most of semaglutide when exercise is truly not possible
Some people have legitimate reasons why exercise is not possible. Severe joint disease. Chronic fatigue conditions. Post-surgical recovery. Disability. Mental health conditions that make physical activity overwhelming. These are real barriers, not excuses, and they deserve practical solutions rather than lectures about the importance of exercise.
Optimize every variable within your control
When exercise is off the table, the remaining variables become more important, not less. Protein intake should be at the upper end of recommendations, 1.4 to 1.6 grams per kilogram minimum. Sleep should be treated as a non-negotiable priority, seven to nine hours of quality rest. Stress management requires daily attention, whether through meditation, breathing exercises, or other techniques. Meal composition should prioritize protein first, then fiber-rich vegetables, then healthy fats, then carbohydrates. Every food choice carries more weight when you lack the caloric buffer that exercise provides.
Hydration matters more. Vitamin and mineral intake matters more. The timing of meals, the quality of food, the consistency of your routine, all of it becomes proportionally more important. Think of it as compensating for a missing tool by sharpening every other tool in your toolkit. The guide to maximizing peptide results applies these same principles across all protocols.
Use every available tool for monitoring
Without exercise-based metrics (strength progress, endurance improvements) to track, you need other data points. Body composition scales, while imperfect, provide trend data on lean mass versus fat mass over time. Regular blood work catches nutritional deficiencies and metabolic changes early. Waist-to-hip ratio is a better health predictor than BMI or total weight. Grip strength, measured with an inexpensive dynamometer, is a surprisingly powerful predictor of overall health and functional capacity. The common mistakes guide covers monitoring blind spots that many people miss.
Consider physical therapy or adaptive movement
Even when traditional exercise is not possible, working with a physical therapist to identify safe movements can preserve some muscle function. Chair-based exercises, water therapy, resistance bands, and adaptive movement programs provide muscle stimulation without the joint stress or physical demands of conventional exercise. Many insurance plans cover physical therapy for obesity-related conditions. The investment, even a few sessions to learn safe movements, can significantly improve body composition outcomes on semaglutide. For people gradually building activity capacity, recovery protocols help manage the transition from sedentary to active.
The honest bottom line
Can you lose weight on semaglutide without exercise? Yes. The clinical evidence is unambiguous. The medication works through mechanisms that do not require physical activity. Most people will lose meaningful weight, enough to produce genuine health improvements, without ever entering a gym.
But can you achieve the best possible outcome without exercise? No. The data is equally clear on this point. Exercise preserves muscle mass, improves body composition, enhances cardiovascular health, supports long-term weight maintenance, and provides mental health benefits that semaglutide cannot replicate. Without exercise, you lose more muscle, regain weight faster after stopping the medication, and miss out on cardiovascular and psychological benefits that exercise uniquely provides.
The good news is that the exercise threshold for meaningful benefit is lower than most people think. Walking counts. Bodyweight exercises count. Even standing more often throughout the day counts. You do not need to train like an athlete. You need to move your body enough to signal that your muscles are still needed. SeekPeptides members access detailed protocols for optimizing GLP-1 therapy including nutrition frameworks, body composition tracking tools, and expert guidance tailored to individual situations, whether you are fully active, building up gradually, or managing physical limitations that prevent traditional exercise.
If exercise is truly not possible right now, focus on protein, sleep, stress management, and consistent dietary habits. These will not fully replace exercise, but they will get you significantly closer to optimal outcomes than ignoring them. And remember that semaglutide creates a window of reduced appetite and improved energy that many people find makes starting to move easier than it has ever been. Maybe today is not the day you start exercising. But three months from now, 20 pounds lighter and with more energy than you have had in years, it might be.
For researchers and individuals serious about optimizing their weight management protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions about exercise, muscle preservation, and long-term success on GLP-1 therapy.
Frequently asked questions
How much less weight will I lose without exercise compared to exercising?
Research suggests exercise adds approximately 28% more weight loss on top of what semaglutide achieves alone. In practical terms, a person who loses 20 pounds on semaglutide without exercise might lose roughly 25 to 26 pounds with consistent exercise. The gap is meaningful but not enormous. More importantly, the exercise group preserves significantly more muscle mass, which affects long-term maintenance and body composition in ways that the scale cannot capture. The semaglutide results timeline provides week-by-week expectations for both scenarios.
Will walking alone be enough exercise with semaglutide?
Walking is excellent for calorie burn and cardiovascular health, but it does not provide the muscle-preserving stimulus of resistance training. Ideally, combine walking with at least one to two sessions per week of bodyweight exercises or resistance band work. If walking is all you can manage, it is still infinitely better than complete inactivity. A daily 30-minute walk burns 150 to 250 extra calories and provides substantial health benefits. The dosing timing guide can help you schedule walks around your injection to minimize nausea.
How do I know if I am losing too much muscle on semaglutide?
Warning signs of excessive muscle loss include weakness during daily activities, difficulty climbing stairs or getting up from chairs, unusual fatigue unrelated to caloric deficit, loss of grip strength, and feeling physically fragile despite weight loss. If your waist circumference is decreasing but your arms and legs look significantly thinner, you may be losing disproportionate muscle. A body composition scan (DEXA) provides the most accurate measurement. Ask your healthcare provider about baseline and follow-up scans if muscle preservation concerns you. The GLP-1 fatigue guide helps distinguish between normal energy changes and concerning muscle loss symptoms.
Can I build muscle while taking semaglutide and losing weight?
Building new muscle while in a caloric deficit is extremely difficult, though not impossible for beginners or people returning to exercise after a long break. More realistically, the goal during semaglutide treatment is preserving existing muscle mass rather than building new tissue. Once you reach your target weight and transition to maintenance calories, building muscle becomes significantly easier. Resistance training during the weight loss phase sets the foundation for muscle growth in the maintenance phase. Understanding recovery optimization helps maximize whatever muscle-preserving stimulus you provide.
Is it safe to exercise while on semaglutide?
Yes, exercise is safe and encouraged while taking semaglutide. However, some people experience nausea, especially during dose escalation, which can make intense exercise uncomfortable. If nausea is an issue, schedule workouts for times when nausea is lowest, often several days after injection rather than the day of injection. Stay well hydrated, especially during exercise, as semaglutide can contribute to dehydration. Start slowly and build gradually. The injection site guide and timing recommendations can help you coordinate injection and exercise schedules.
What happens to my weight loss if I start exercising after months of semaglutide without exercise?
Adding exercise at any point during semaglutide treatment will likely provide additional benefits. You may see the scale temporarily stall or increase slightly due to water retention from new exercise (muscle inflammation) and glycogen storage. This is normal and temporary. Within two to four weeks, the additional calorie burn and improved body composition will show in both the scale and other metrics. Starting exercise later is always better than not starting at all. The results maximization guide covers how to introduce exercise during an ongoing protocol without disrupting progress.
Do I need to eat more if I add exercise to semaglutide?
Not necessarily, but you may need to adjust what you eat. If exercise increases your caloric burn significantly, eating slightly more, particularly more protein, supports recovery and muscle preservation without undermining weight loss. The goal is to maintain a moderate caloric deficit, not a severe one. Severe deficits combined with exercise accelerate muscle loss. Aim for a deficit of 500 to 750 calories per day including exercise. If your appetite is extremely suppressed, prioritize calorie-dense protein sources like nuts, cheese, protein shakes, and fatty fish to meet protein targets without forcing large volumes of food.
Can I drink alcohol on semaglutide if I am not exercising?
You can, but it is less advisable when exercise is absent from your routine. Without the additional caloric buffer that exercise provides, every unnecessary calorie matters more. Alcohol adds 7 calories per gram with zero nutritional value and disrupts sleep, impairs judgment around food choices, and temporarily halts fat metabolism. If you choose to drink, limit consumption and account for the calories. The complete guide to alcohol and semaglutide covers specific risks and recommendations in detail.
External resources
STEP 1 Trial (New England Journal of Medicine) - The landmark clinical trial demonstrating 14.9% average weight loss with semaglutide 2.4 mg over 68 weeks, including details on the lifestyle intervention component.
Impact of Semaglutide on Body Composition (STEP 1 Exploratory Analysis) - Detailed body composition data showing fat mass, lean mass, and visceral fat changes during semaglutide treatment.
Semaglutide Efficacy Without Diabetes: Systematic Review and Meta-Analysis - Comprehensive analysis of semaglutide weight loss outcomes in populations without diabetes.
Long-term Weight Loss Effects of Semaglutide (SELECT Trial, Nature Medicine) - Real-world cardiovascular outcomes and long-term weight loss data from the largest semaglutide trial.
Protein Intake and Muscle Preservation on Anti-Obesity Medications (Endocrine Society) - Research on how higher protein intake protects against muscle loss in semaglutide users.
The real power of semaglutide lies in its ability to create conditions for weight loss that do not depend on willpower, gym memberships, or athletic ability. It works without exercise. But understanding the trade-offs, the muscle loss, the body composition concerns, the long-term maintenance challenges, allows you to make informed decisions about what additional steps, if any, make sense for your situation.
For ongoing support, personalized protocols, and evidence-based guidance on optimizing GLP-1 therapy, SeekPeptides members access everything needed to navigate these decisions with confidence.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay manageable, your muscle mass stay protected, and your results stay permanent.