Feb 20, 2026

Experienced researchers who have been administering semaglutide for months know something that most beginners miss entirely. The injection site matters. Not in the way most people think, not as a make-or-break factor that determines whether the medication works, but as a practical detail that affects comfort, consistency, and long-term results. Where you place that needle shapes your experience with every single dose.
Most guides on this topic offer the same surface-level advice. Abdomen, thigh, or arm. Pick one. Rotate. Done.
That is not enough.
The reality is more nuanced than a three-word answer. Different injection sites absorb semaglutide at slightly different rates. Your body composition influences which site works best for you specifically. The technique you use at each site varies in ways that affect both comfort and medication delivery. And the rotation strategy you follow determines whether you develop skin problems, pain, or reduced absorption over weeks and months of treatment. This guide covers everything about semaglutide injection placement, from the science of absorption to the practical techniques that make each injection as effective and painless as possible. Whether you are using a brand-name pen injector or a compounded semaglutide vial with an insulin syringe, SeekPeptides has built this resource to be the only injection site guide you will ever need.
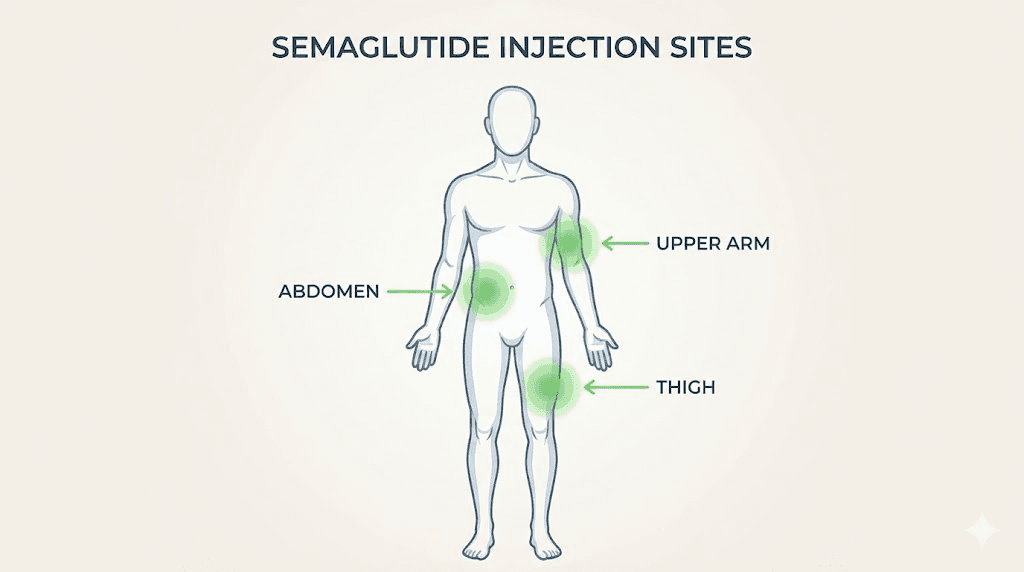
The three approved injection sites for semaglutide
Semaglutide is a subcutaneous injection. That means it goes into the fatty tissue layer just beneath the skin, not into muscle and not into a vein. The subcutaneous injection method requires specific body areas where there is enough fatty tissue to allow proper absorption. Three areas meet this requirement.
Each one has distinct advantages and trade-offs depending on your body type, comfort preferences, and whether you are self-injecting or receiving assistance.
The abdomen: most popular and most accessible
The abdomen is the most commonly recommended semaglutide injection site, and for good reason. It offers the largest surface area of any approved site, which makes rotation easier and gives you more options for finding comfortable spots. The abdominal area also tends to have a consistent subcutaneous fat layer in most people, regardless of overall body composition.
There are rules. Stay at least two inches away from the belly button in every direction. That area contains denser tissue and more nerve endings, which makes injections more painful and less effective. Avoid the waistband zone where clothing presses against the skin, as friction can irritate a fresh injection site and cause redness or discomfort.
The ideal injection zone forms a wide U-shape around the navel. Start about two inches below the belly button and extend outward to the sides, then curve upward to the areas above and beside the navel. This gives you a large zone that you can divide into quadrants for systematic rotation.
Research shows that the abdomen provides the most consistent semaglutide absorption. The subcutaneous fat layer in this area tends to be uniform in thickness, which means the medication disperses predictably. For people tracking their semaglutide dosage carefully and wanting consistent results week to week, the abdomen is typically the best starting point.
The front of the thigh: a solid alternative
The front of the thigh, specifically the upper outer quadrant, serves as an excellent alternative injection site. This area is easy to reach without assistance, and most people have adequate subcutaneous tissue here for proper medication delivery.
Use the middle third of the outer thigh. Avoid the inner thigh entirely. That area contains more nerve endings and blood vessels, which increases the risk of pain and bruising. The kneecap area and the top of the thigh near the groin should also be avoided.
One practical consideration with thigh injections is clothing friction. Pants, especially tight-fitting ones, can rub against a fresh injection site throughout the day. Some people find this more irritating than abdominal injections where loose-fitting shirts provide a buffer. If you choose the thigh, consider injecting in the evening when you will be changing into more comfortable clothing soon after.
The thigh works particularly well for people who find abdominal injections uncomfortable or who have limited subcutaneous fat in the abdominal area. It also provides a useful rotation option to give the abdomen a break between injections. Understanding where to inject GLP-1 medications properly means having multiple sites in your rotation plan.
The back of the upper arm: best with assistance
The back of the upper arm, in the area between the shoulder and the elbow, is the third approved injection site. This location has a consistent fat layer in most people and can be very comfortable for injections.
There is a catch. Self-injecting in the upper arm is difficult. You cannot easily see what you are doing, and the angle required to reach the back of your own arm makes proper technique nearly impossible for most people. This site works best when a partner, family member, or healthcare provider administers the injection.
If you do have someone to help, the upper arm is often the least painful option. The skin here tends to be less sensitive than the abdomen or thigh, and the area is less likely to be irritated by clothing. For people who are new to peptide injections and feel anxious about self-administration, having a partner use the upper arm site can reduce the psychological barrier to starting treatment.
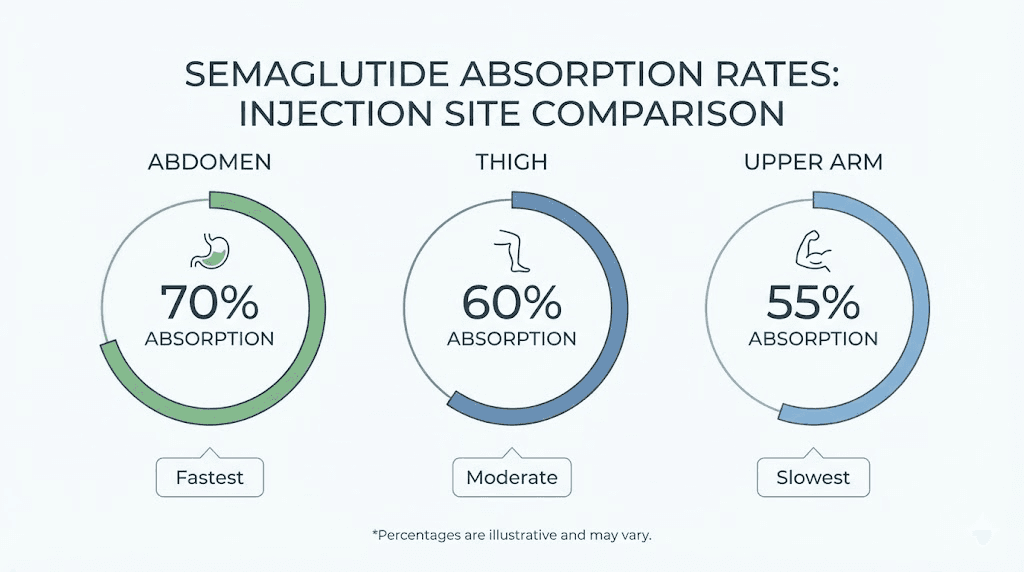
Which injection site absorbs semaglutide best
This is the question everyone asks. Does it actually matter where you inject? Will one site give you better results than another? The answer involves some nuance.
What the research shows about absorption differences
Clinical pharmacokinetic studies have examined whether injection site affects how much semaglutide enters the bloodstream and how quickly it reaches peak concentration. The data shows measurable differences. But here is the important part: those differences are small enough that they do not change clinical outcomes.
The overall subcutaneous bioavailability of semaglutide is approximately 89%. That means about 89% of the injected dose reaches the bloodstream, regardless of which of the three approved sites you choose. This is a high bioavailability for a subcutaneous injection, and it remains consistent across injection sites.
Population pharmacokinetic analyses published in Diabetes Therapy found that the injection site has a minor effect on semaglutide clearance. The researchers characterized this effect as not clinically relevant. In practical terms, your semaglutide results timeline and overall weight loss outcomes should not change based on injection site alone.
The 12% bioavailability difference between abdomen and thigh
One finding that gets cited frequently is a 12% difference in bioavailability between the abdomen and the thigh. Specifically, studies found that thigh injections resulted in approximately 12% lower bioavailability compared to abdominal injections (95% confidence interval: 0.84 to 0.92).
That sounds significant. Twelve percent is not nothing.
But context matters. This 12% difference falls within the normal range of variability that occurs between any two injections, even at the same site. Individual factors like hydration status, skin temperature, activity level, and the exact depth of the injection all create variability in absorption. The site-related difference is real but sits alongside these other sources of variability without meaningfully changing outcomes.
The FDA prescribing information for both Ozempic and Wegovy states that similar exposure to semaglutide is achieved regardless of injection site. This determination was made after reviewing the complete pharmacokinetic data. If the 12% difference were clinically meaningful, the labeling would restrict injection to the abdomen only. It does not, because the difference does not affect how well the medication works for weight loss or appetite suppression.
Why consistency matters more than location
The takeaway from the absorption research is straightforward. Pick a site that works for you and use proper technique every time. Consistency in technique, not consistency in location, drives reliable results. A well-executed injection in the thigh will outperform a poorly executed injection in the abdomen every time.
Factors that affect absorption more than injection site include injection depth (too shallow sits in the dermis, too deep hits muscle), injection speed (rushing can cause the medication to pool rather than disperse), and whether the area has scar tissue or lipodystrophy from repeated use. Mastering these injection fundamentals matters far more than which body part you choose.
How to choose the right injection site for your body
The best injection site is not universal. It depends on your specific body composition, your lifestyle, and whether you are injecting alone or with help. Here is how to think through the decision.
Body composition factors
Subcutaneous injections require a layer of fat between the skin and the underlying muscle. The minimum thickness needed is roughly half an inch, though more provides easier and more comfortable injections. Where you carry your body fat determines which sites will work best.
People with higher body fat percentages typically have the most flexibility. All three sites will have adequate subcutaneous tissue, and the abdomen in particular will offer a large, comfortable injection zone. If you are using a semaglutide dosage calculator to determine your dose, remember that body weight affects dosing but does not change the injection site recommendations.
For leaner individuals, the abdomen may still be the best option as it tends to retain subcutaneous fat even at lower body fat percentages. The thigh can be challenging for very lean people, especially those with muscular legs and minimal subcutaneous fat. In these cases, a skin pinch technique becomes essential. If you can pinch at least half an inch of skin and fat at a potential injection site, it is suitable for subcutaneous injection.
As you lose weight on semaglutide, your body composition changes. An injection site that worked well at the start of treatment might become less ideal as subcutaneous fat decreases. Plan to reassess your preferred sites periodically, especially if you are experiencing significant early results.
Activity level and clothing considerations
Think about what you do after injecting. If you exercise in the morning and inject in the morning, a thigh injection might be irritated by running or cycling. Abdominal injections can be aggravated by core exercises or tight waistbands. Upper arm sites may be uncomfortable if you lift weights or wear compression sleeves.
The simplest solution is timing. Inject at a time of day when you will not be physically stressing the injection area for at least two to three hours. Many people find that evening injections work well because the body is at rest overnight, giving the injection site time to settle. Our guide on the best time of day to take semaglutide covers this in more detail.
Self-injection versus assisted injection
If you are injecting yourself, the abdomen and thigh are your practical options. Both are easily visible and accessible, allowing you to control the angle, depth, and speed of injection. The abdomen is slightly easier for most people because you can see the full injection zone while seated or standing.
If you have a partner or caregiver who can help, the upper arm becomes viable and may even be preferable. Having someone else inject allows for better angle control and more consistent technique, especially for people who experience anxiety around self-injection. For couples managing weight loss together, alternating who administers the other person injections can make the process feel more manageable.
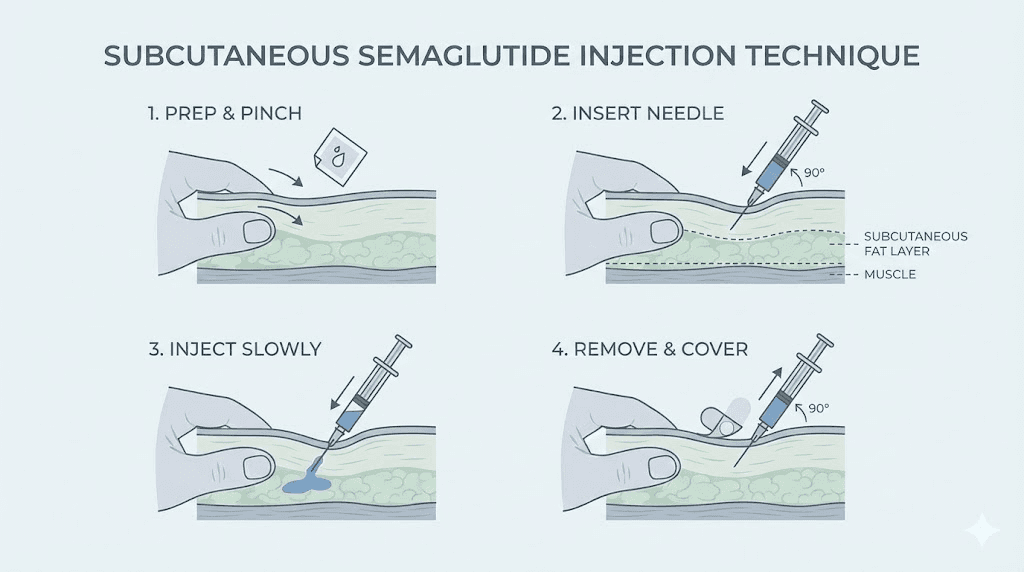
Complete injection technique step by step
Proper technique matters more than injection site selection. A perfectly placed injection done with poor technique will be less effective and more uncomfortable than an imperfect location with excellent technique. This section covers the complete process for both pen injectors and insulin syringes used with compounded semaglutide.
Preparing for your injection
Start by gathering everything you need. For pen injectors, that means the semaglutide pen, a new needle, an alcohol swab, and a sharps container. For compounded semaglutide in a vial, you will need the vial, an insulin syringe (typically 100-unit), an alcohol swab, and a sharps container. Understanding semaglutide syringe dosage charts helps ensure accurate dosing with insulin syringes.
Wash your hands thoroughly with soap and water. This is not optional. Injection site infections are rare but entirely preventable with basic hygiene.
If your semaglutide has been refrigerated, allow it to reach room temperature before injecting. Cold medication stings more upon injection and may absorb less predictably. Remove the pen or vial from the refrigerator 15 to 30 minutes before your scheduled injection time. Check our guide on semaglutide refrigeration requirements for proper storage between injections.
Inspect the medication visually. Semaglutide solution should be clear and colorless. If it looks cloudy, contains particles, or has changed color, do not use it. Understanding how long semaglutide stays good helps you avoid using expired or degraded medication.
Pen injector technique
Brand-name semaglutide pens like Ozempic and Wegovy come pre-loaded with medication and use built-in dose selectors. The technique is standardized and relatively straightforward.
Attach a new needle to the pen. Never reuse needles. Pen needles are typically 31-gauge or 32-gauge, which are extremely thin. Most are 4mm in length, designed specifically for subcutaneous injection without needing to pinch the skin in areas with adequate fat tissue.
Select your prescribed dose using the pen dial. Clean your chosen injection site with an alcohol swab, moving in a circular motion from center outward. Allow the alcohol to dry completely, as injecting through wet alcohol can cause stinging.
If your injection site has adequate fatty tissue, you can insert the needle straight in at a 90-degree angle without pinching. If you are lean or injecting in an area with less subcutaneous fat, pinch a fold of skin between your thumb and forefinger, then insert the needle into the raised fold at a 90-degree angle.
Press the injection button firmly and hold it down. Keep the needle in place for at least 6 seconds after the dose counter shows zero. This pause is critical. It allows the full dose to be delivered and prevents medication from leaking back out of the injection site. For Wegovy pens, you will hear two clicks. The first click starts the injection, and the second confirms the dose is complete. Wait a few seconds after the second click before removing the needle.
Remove the needle in the same straight line you inserted it. Do not twist or angle the needle during removal. Press a clean cotton ball or gauze pad against the site for a few seconds. Do not rub.
Insulin syringe technique for compounded semaglutide
Compounded semaglutide comes in multi-dose vials and requires measuring each dose with an insulin syringe. This process demands more precision than pen injectors but follows the same basic injection principles. Our semaglutide syringe dosage conversion chart helps you determine exactly how many units to draw.
Use a 100-unit insulin syringe with a 31-gauge needle. These are thin enough for minimal pain while being precise enough for accurate dosing. Clean the vial stopper with an alcohol swab before inserting the needle.
Draw air into the syringe equal to the volume of medication you plan to withdraw. Insert the needle through the vial stopper and push the air in. This creates positive pressure that makes drawing the medication easier. Invert the vial with the syringe still inserted and pull the plunger back slowly to your required dose. Check for air bubbles. If present, tap the syringe gently to move them to the top and push them back into the vial, then redraw to your exact dose. Understanding semaglutide units to mg conversions is essential when working with compounded formulations.
The injection technique itself is identical to pen injection. Clean the site, pinch if needed, insert at 90 degrees (or 45 degrees for very lean injection sites), and depress the plunger slowly and steadily. Hold for 5 to 10 seconds after the plunger is fully depressed, then remove the needle smoothly.
If you are reconstituting semaglutide yourself, make sure you have followed the correct mixing ratios. Using the wrong amount of bacteriostatic water changes the concentration, which changes how many units equal your target dose. Our semaglutide reconstitution chart provides precise mixing ratios for common vial sizes.
Needle angles and depth
The goal is to deposit semaglutide into the subcutaneous fat layer. Too shallow and the medication sits in the dermis, where it absorbs poorly and can cause skin irritation. Too deep and it enters the muscle, where it absorbs too quickly and can cause pain.
For most people at most injection sites, a 90-degree angle (straight in, perpendicular to the skin surface) is correct. The standard 4mm pen needles and short insulin syringe needles are designed to reach the subcutaneous layer at this angle without overshooting into muscle.
A 45-degree angle is appropriate in specific situations. Very lean individuals with minimal subcutaneous fat may need the shallower angle to avoid hitting muscle. The same applies when injecting in areas where the fat layer is naturally thinner, such as the thigh in lean people. If you use a 45-degree angle, always pinch the skin first to lift the subcutaneous layer away from the muscle beneath.
Never inject at a very shallow angle (less than 30 degrees). This causes intradermal injection, where the medication pools within the skin layers rather than beneath them. Intradermal semaglutide injection can cause visible welts, intense stinging, and unreliable absorption.
How long to hold the needle after injection
This step gets skipped or rushed more than any other. It should not be.
After pressing the pen button or fully depressing the syringe plunger, the medication needs time to disperse from the needle tip into the surrounding tissue. Removing the needle immediately creates a channel for the medication to leak back out, resulting in an incomplete dose.
For Ozempic pens, hold for at least 6 seconds. For Wegovy autoinjectors, wait until the second click plus a few additional seconds. For insulin syringes with compounded semaglutide, hold for 5 to 10 seconds. Count slowly. Many people count too fast when they are anxious about the needle being in their skin.
After removing the needle, press gently on the site without rubbing. Rubbing can push medication toward the skin surface and increase bruising. A gentle press for 10 to 15 seconds is sufficient.
Injection site rotation: the strategy most people get wrong
Rotation is not optional. It is one of the most important aspects of long-term semaglutide use, and getting it wrong can lead to real problems that affect both comfort and medication effectiveness.
Why rotation matters
Every injection creates microscopic trauma to the tissue at the injection site. The body heals this trauma naturally, but healing takes time. Injecting into the same spot repeatedly before it has fully recovered causes cumulative tissue damage.
The most common consequence is lipodystrophy, a condition where the subcutaneous fat layer changes structure at frequently used injection sites. This can manifest as lipohypertrophy (fatty lumps under the skin) or lipoatrophy (indentations where fat tissue has broken down). Research suggests that as many as two-thirds of people who use regular injections develop some degree of lipohypertrophy over time.
Lipodystrophy does not just look and feel unpleasant. It also affects medication absorption. Scar tissue and altered fat deposits absorb medication inconsistently, which can lead to unpredictable blood levels and variable results. If you are not losing weight on semaglutide despite following your protocol, checking for injection site issues should be one of your first troubleshooting steps.
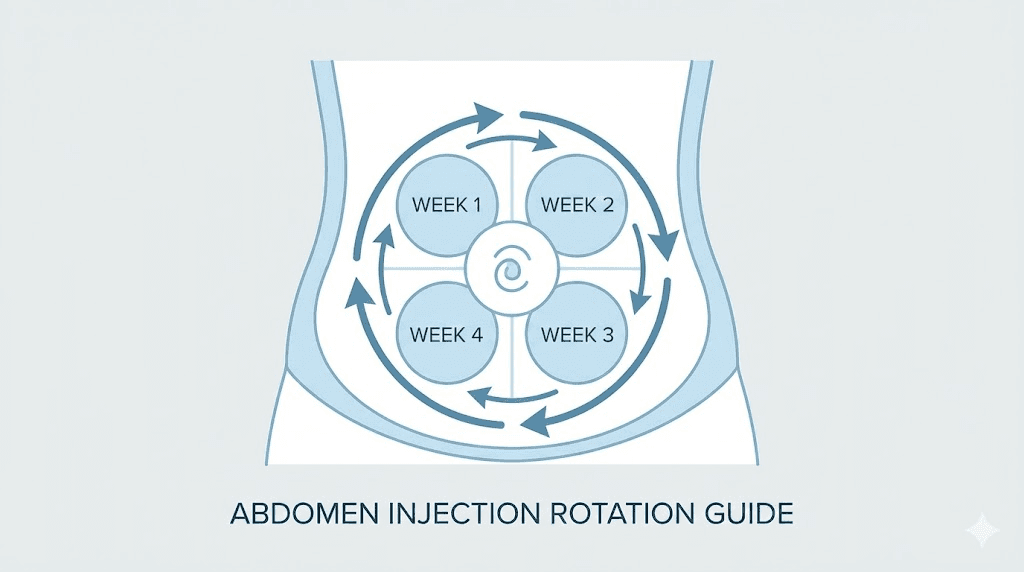
The quadrant method for abdominal rotation
The most effective rotation strategy for abdominal injections divides the injection zone into four quadrants. Picture a cross centered on your belly button (but remember, no injections within two inches of the navel itself).
Upper left. Upper right. Lower left. Lower right.
Each week, use a different quadrant. Move clockwise. Week one, upper left. Week two, upper right. Week three, lower left. Week four, lower right. Then start the cycle again. This gives each quadrant a full three weeks to recover between injections.
Within each quadrant, vary the exact spot slightly. Move at least one inch from any previous injection site. Over the course of a month, no two injections should be closer than an inch apart, and no spot should be reused within four weeks.
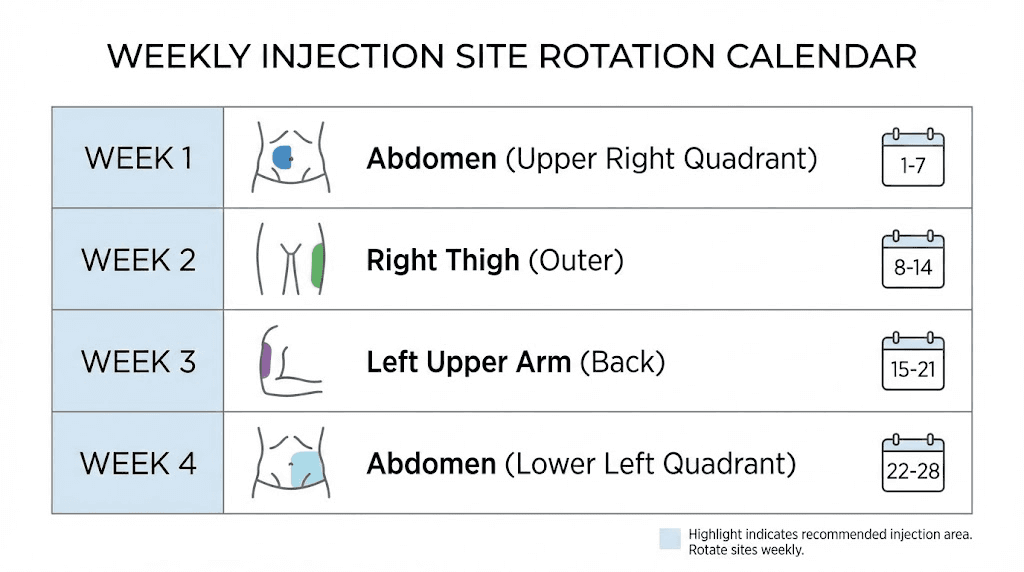
Weekly rotation between body areas
For maximum site recovery, rotate between different body areas rather than staying on the abdomen permanently. A simple three-week rotation might look like this: week one abdomen, week two right thigh, week three left thigh, then back to abdomen. If you have a partner who can help, add upper arms into the rotation for a four or five-week cycle.
This between-area rotation provides the longest recovery time for each site. It reduces the risk of developing localized skin changes, and many people report less discomfort because each area gets several weeks of rest. For people managing long-term semaglutide protocols who want to understand how long they will stay on semaglutide, building good rotation habits early prevents problems later.
Tracking your injection sites
Memory is unreliable for tracking injection sites, especially when you inject only once per week. By the time your next injection comes around, you may not remember exactly where you injected last time.
Simple solutions work best. Keep a small journal or note on your phone. Record the date, the body area (left abdomen, right thigh, etc.), and any notes about comfort or reactions. Some people mark the injection site with a small dot from a washable marker right after injecting, which creates a visible reminder when choosing the next site.
The GLP-1 plotter tool can help you visualize your injection schedule alongside your dosing plan. Keeping organized records becomes especially important as you progress through semaglutide dose escalation, where both the dose and the injection site need careful tracking.
Common injection site problems and how to fix them
Even with perfect technique, injection site issues occur. Understanding what is normal, what requires attention, and what demands medical consultation helps you manage these situations confidently.
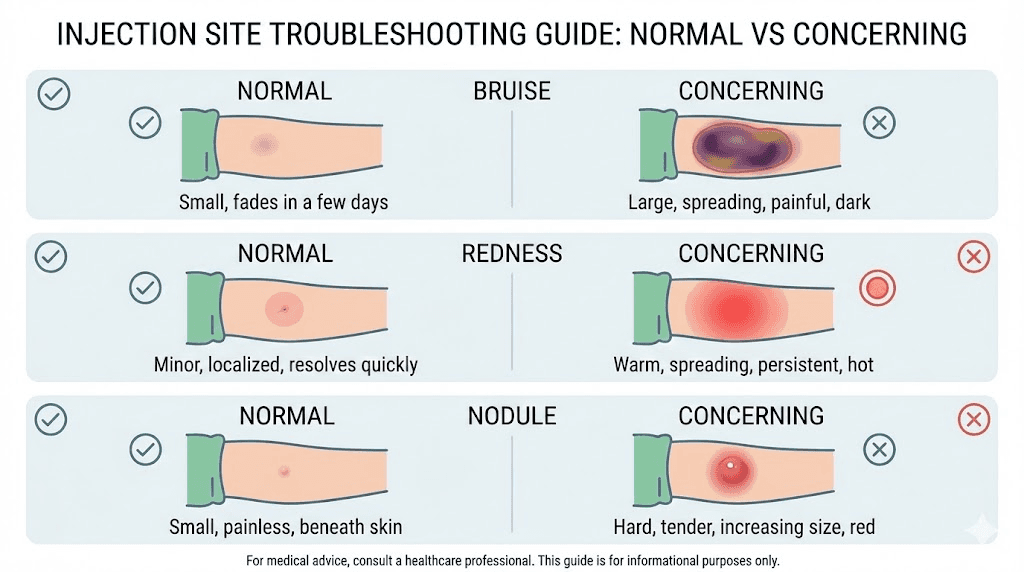
Bruising at the injection site
Bruising is the most common injection site issue. It happens when the needle punctures small capillaries beneath the skin, allowing blood to leak into surrounding tissue. About half of all semaglutide users experience some degree of bruising, particularly when starting treatment.
Small bruises that are quarter-sized or smaller are normal. They typically appear within hours of injection and resolve within a few days to two weeks. The bruise may change colors as it heals, moving from red or purple to green, yellow, and then fading completely.
Reduce bruising by injecting slowly, holding the needle in place for the full recommended time, and pressing gently (without rubbing) after removal. Ice the area for 5 to 10 minutes before injection to constrict blood vessels. Avoid taking blood-thinning medications or supplements like aspirin, ibuprofen, fish oil, or vitamin E before injection if medically appropriate to do so.
Large bruises, bruises that spread significantly, or bruising accompanied by severe pain may indicate that the needle hit a larger blood vessel or went too deep into muscle tissue. Adjust your technique and choose a different spot within the same area for your next injection. If severe bruising persists, consult your healthcare provider.
Pain and stinging during injection
Some discomfort is expected with any injection. The needle itself causes brief, sharp pain as it penetrates the skin, and the medication can create a mild stinging or burning sensation as it enters the tissue. This should be brief. Lasting only seconds.
Pain that persists for more than a few minutes, or pain that is sharp and deep, suggests a technique issue. The most common causes are injecting too quickly (forcing medication into tissue faster than it can disperse), injecting into an area with insufficient subcutaneous fat (hitting muscle or nerve), and using a dull or damaged needle.
Cold medication stings more than room-temperature medication. This is one of the most impactful and simplest adjustments you can make. Taking your semaglutide out of the refrigerator 15 to 30 minutes before injection dramatically reduces the sting. Just do not leave it at room temperature for extended periods, as storage conditions affect medication stability.
Redness and swelling
Mild redness at the injection site is a normal immune response to the needle puncture. It should be small (around the size of a dime), appear shortly after injection, and resolve within 24 to 48 hours. Swelling that is slight and localized falls into the same category.
Redness that spreads beyond a few inches, increases over time rather than fading, or is accompanied by warmth, pus, or fever could indicate an infection. This is rare but requires medical attention. Proper hand washing and alcohol swabbing before injection virtually eliminates infection risk when done consistently.
Allergic-type reactions at the injection site, characterized by raised, itchy welts or hives, are uncommon with semaglutide. If you experience these consistently across multiple injection sites and multiple doses, report it to your prescriber. These reactions may indicate sensitivity to the medication or to an inactive ingredient in the formulation. People using semaglutide with B12 or other combination compounds should consider whether the added ingredients might be contributing to site reactions.
Injection site nodules
Nodules are hard, raised lumps that form at the injection site. They are uncommon with semaglutide but have been documented in medical literature. A published case study in Diabetes Spectrum described a 75-year-old patient who developed quarter-sized, hard, erythematous, pruritic, and raised nodules within minutes of injection after reaching the maximum 1 mg dose.
The key details from that case are instructive. At the 0.5 mg dose, nodules subsided within 24 hours. At the 1 mg dose, they took 2 to 4 days to resolve. The reaction appeared dose-dependent, worsening as the dose increased. Using the Naranjo Adverse Drug Reaction Probability Scale, researchers scored the relationship between semaglutide and the nodules as "definite."
Importantly, injection site nodules are not a class-wide adverse effect across all GLP-1 receptor agonists. They are most commonly associated with exenatide extended-release. If you develop persistent nodules with semaglutide, your healthcare provider may recommend switching to a different GLP-1 medication or adjusting your injection technique.
Lipodystrophy from repeated injections
Lipodystrophy develops slowly over weeks or months of injecting in the same area without adequate rotation. The tissue changes are gradual and often go unnoticed until they become significant.
Lipohypertrophy presents as soft, sometimes rubbery lumps under the skin. They may feel like gentle swelling at first. Many people unconsciously prefer injecting into these areas because the altered tissue has fewer nerve endings, making injections less painful. This creates a cycle: the area feels comfortable, so it gets used more often, which makes the lipohypertrophy worse.
Break the cycle by following strict rotation protocols. If you notice any lumps or changes in skin texture at your injection sites, avoid that area completely for at least 8 to 12 weeks. The tissue can often recover if given enough time. Mark affected areas on your tracking chart so you do not accidentally use them.
Lipoatrophy, where fat tissue actually diminishes, is less common with semaglutide but can occur. It presents as visible dents or depressions in the skin. This is more difficult to reverse than lipohypertrophy. Prevention through proper rotation remains the best approach. If you are concerned about tissue changes, our guide on peptide safety and risks covers broader safety considerations.
Pain reduction strategies that actually work
Nobody enjoys injections. But the discomfort of semaglutide injections can be minimized to the point where most people describe the experience as a mild pinch lasting one to two seconds. Here are the strategies that make the biggest difference.
Temperature management
This is the single most effective pain reduction technique, and it involves no special equipment or products.
Remove semaglutide from the refrigerator 15 to 30 minutes before injection. The medication should feel close to room temperature when you inject it. Cold medication causes a noticeable stinging sensation that room-temperature medication does not. The difference is significant enough that most healthcare providers include this instruction as their first piece of injection advice.
You can also ice the injection site before inserting the needle. Apply an ice cube or cold pack wrapped in a thin cloth for 30 to 60 seconds. This numbs the skin surface without affecting the subcutaneous tissue where the medication needs to go. Remove the ice, clean the site with alcohol, and inject while the area is still slightly numb. The combination of warm medication and a numbed injection site makes the process remarkably painless for most people.
Technique adjustments for less pain
Speed matters, but not in the way most beginners assume. Insert the needle with a quick, confident motion. Hesitating or pushing slowly through the skin surface causes more pain than a swift insertion. Think of it like removing a bandage. Fast is better than slow.
Once the needle is in, switch to slow. Depress the plunger or press the pen button slowly and steadily. Injecting medication too quickly forces it into tissue faster than the tissue can accommodate, causing pressure and pain at the injection site. A slow, steady injection over 5 to 10 seconds is far more comfortable than a rapid push.
Keep the needle perfectly still while injecting. Any movement, tilting, or wobbling of the needle creates additional tissue trauma and increases pain. Brace your hand against your body if needed to maintain stability. If you are using a pen injector, hold the pen firmly against the skin surface rather than hovering.
Topical numbing options
Over-the-counter lidocaine creams or sprays can numb the injection site effectively. Apply the numbing product 20 to 30 minutes before injection, following the product instructions. These products work by temporarily blocking nerve signals from the skin surface.
Some people find that a simple vibration technique provides sufficient distraction from the injection pain. Tap the skin rapidly near (not at) the injection site while inserting the needle. This activates sensory nerve fibers that partially block pain signals, a principle called the gate control theory of pain. It sounds unusual, but many people find it genuinely helpful.
Needle selection for compounded semaglutide
If you are using compounded semaglutide with an insulin syringe, you have control over needle selection that pen users do not. Choose the thinnest, shortest needle that works for your body type.
31-gauge and 32-gauge needles are the standard recommendation. These are extremely thin and cause minimal pain upon insertion. The difference between a 29-gauge and a 31-gauge needle is noticeable to most people, so opting for the thinner option is worthwhile.
Needle length of 4mm to 6mm is appropriate for most people. Shorter needles (4mm) work well for leaner individuals and those using the skin pinch technique. Slightly longer needles (6mm) provide a bit more margin for reaching the subcutaneous layer in areas with more tissue. Check our guide on mixing compounded semaglutide for proper preparation before injection.
Never reuse needles. Used needles develop microscopic burrs on the tip that increase pain and tissue damage with each reuse. A fresh needle every injection is not a luxury. It is a basic requirement for safe, comfortable injection practice.
Injection site mistakes to avoid
Some injection mistakes are obvious. Others are subtle habits that develop over time and gradually undermine your results. These are the most common errors, ranked by how frequently they occur and how significantly they affect outcomes.
Injecting too close to the belly button
The two-inch rule exists for good reason. The area immediately surrounding the navel has denser connective tissue, more nerve endings, and less uniform subcutaneous fat. Injections here hurt more, absorb less consistently, and are more likely to cause bruising.
Use the width of two fingers as a quick measurement. Place your index and middle fingers side by side next to your belly button. The edge of your furthest finger marks the minimum distance. This simple visual check prevents one of the most common injection mistakes. People who have been following common peptide mistakes to avoid will recognize this pattern.
Reusing the same spot repeatedly
Comfort creates bad habits. Once you find a spot that does not hurt, the temptation to use it every time is strong. Resist it. Using the same spot repeatedly, even within the same body area, leads to tissue damage, lipodystrophy, and eventually unreliable absorption.
The minimum distance between consecutive injection sites is one inch. The minimum time before returning to a previously used spot is four weeks. Both rules matter, and following only one of them is not enough.
Injecting into muscle
Intramuscular injection of semaglutide is not dangerous, but it changes how the medication works. Muscle tissue has a richer blood supply than subcutaneous fat, which means the medication absorbs faster and reaches peak concentration sooner. This can increase side effects like nausea and gastrointestinal discomfort while potentially reducing the duration of appetite suppression between doses.
Signs that you are injecting too deep include sharp, deep pain during injection (subcutaneous injections feel like a pinch, not a deep ache), blood flowing into the syringe when you pull back slightly on the plunger, and significant bruising that appears deep under the skin rather than at the surface.
Fix this by using shorter needles, injecting at a 45-degree angle instead of 90 degrees, and always pinching the skin at lean injection sites. If you consistently experience signs of intramuscular injection at one site, switch to a different body area with more subcutaneous tissue.
Not pinching the skin when needed
The skin pinch technique is not always necessary, but knowing when to use it is important. Pinching lifts the subcutaneous fat layer away from the underlying muscle, creating a clear target for the needle tip. It is essential for lean individuals, at thigh injection sites where the fat layer may be thin, and when using needles longer than 4mm.
Pinch firmly with your thumb and forefinger, creating a fold of skin and fat approximately one inch wide. Insert the needle into the center of the fold at a 90-degree angle (or 45 degrees for very thin folds). Maintain the pinch throughout the injection and for a few seconds after removing the needle.
The mistake people make is pinching too tightly or too close to the injection site. A white-knuckle pinch compresses the tissue excessively and can force the needle into muscle despite the pinch. A gentle, firm pinch is all that is needed.
Removing the needle too quickly
This mistake causes medication waste. Every time you remove the needle before the full dose has dispersed from the tip into surrounding tissue, a small amount of medication leaks back through the needle track. Over weeks and months, these small losses add up.
The fix is simple patience. Count to six slowly for pen injectors. Count to ten for insulin syringes. Then remove the needle straight out, in the same angle it went in, without twisting or angling. Apply gentle pressure immediately after withdrawal.
Injection timing and site selection
When you inject and where you inject interact in ways that most guides overlook. Timing can influence comfort, absorption, and even side effect management.
Best time of day to inject semaglutide
Semaglutide can be injected at any time of day. The medication has a half-life of approximately one week, so the exact hour of injection does not significantly affect blood levels between doses. However, the time of day can affect your injection experience.
Morning injections work well for people who want to establish a routine tied to their waking schedule. The downside is that daytime activity can irritate the injection site, especially if clothing rubs against it or if you exercise.
Evening injections are popular because they allow the injection site to rest overnight without friction or physical stress. Some people also prefer evening injections because any nausea or fatigue from the injection can be managed by going to sleep. Our detailed guide on optimal semaglutide timing explores this topic comprehensively.
Choose a time that works with your schedule and stick with it. Consistency in timing makes it easier to remember your weekly injection and helps you build injection into a routine rather than treating it as an event.
Does timing affect which site to use
Yes, indirectly. If you inject in the morning and then go to the gym, an abdominal injection before core work or a thigh injection before leg day will be more uncomfortable than it needs to be. Match your injection site to your schedule.
Planning to sit at a desk all day? The abdomen works fine. Going for a long walk or run? The upper arm (with assistance) or a spot on the abdomen away from your waistband might be more comfortable. The key is thinking one step ahead about what your body will be doing in the hours after injection.
Weekly injection scheduling
Semaglutide is administered once weekly. Try to inject on the same day each week, though the exact day can be changed if needed. If you change your injection day, make sure there are at least two days between the old schedule and the new one.
Many people choose a day with a predictable schedule, like Saturday or Sunday morning, when they are not rushed and can take their time with proper technique. Whatever day you choose, pair it with your rotation tracking to ensure you are using a different site each week.
If you miss your scheduled injection day, take the dose as soon as you remember, as long as your next scheduled dose is at least two days away. If it is less than two days until your next dose, skip the missed dose and resume your regular schedule. Never double up doses to compensate for a missed injection. Understanding semaglutide dosage measurements helps prevent dosing errors during schedule disruptions.
Special considerations for different situations
Standard injection site advice covers most situations. But certain circumstances require adjustments that generic guides rarely address.
Injection sites when losing weight
Semaglutide works. For many people, it works well enough that their body composition changes significantly over weeks and months of treatment. This creates a practical challenge with injection sites.
As you lose subcutaneous fat, areas that previously had ample tissue for comfortable injection may become too lean. The abdomen often changes the most dramatically, especially in people who carry weight primarily in their midsection. A site that worked perfectly at week one might cause pain or intramuscular injection at week twelve.
Reassess your injection sites periodically. Every four to six weeks, check each of your rotation sites by pinching the skin. If you can no longer pinch at least half an inch of tissue, that site has become too lean for comfortable subcutaneous injection. Move to an area with more remaining subcutaneous fat.
For people tracking their semaglutide results month by month, noting any injection site changes alongside weight and measurement data helps you anticipate when site adjustments will be needed. Some people find that what started as an abdomen-only rotation evolves into a thigh-dominant rotation as they lose abdominal fat. This is normal and expected.
Injection sites with scar tissue
Never inject into scar tissue. Scars consist of dense fibrous tissue that lacks the normal subcutaneous fat structure needed for proper medication absorption. Injecting into scar tissue is painful, absorbs poorly, and can cause medication to pool inappropriately.
Surgical scars, stretch marks (while technically not scars, the tissue structure is altered), tattoos (the ink sits in the dermal layer and injection through tattooed skin should be avoided), and any areas of previous injury should be excluded from your injection rotation.
Map these exclusion zones when you first start treatment. If you have abdominal surgical scars from a previous procedure, for example, identify which parts of the abdominal injection zone remain viable and adjust your quadrant rotation accordingly. Most people have enough usable tissue even with some areas excluded.
Injection sites for people with less body fat
People with lower body fat percentages face unique challenges with subcutaneous injections. The standard advice assumes a moderate level of subcutaneous fat, and it does not always translate directly to lean individuals.
For lean people, the lower abdomen and love handle area often retain the most subcutaneous fat and serve as the most reliable injection sites. The thighs may work if there is adequate fat on the outer aspect. The upper arms are often the leanest area and may not be viable without assistance and careful technique.
Always use the pinch technique. Always use a 45-degree angle if the tissue fold is less than one inch. Consider using 4mm needles exclusively to minimize the risk of intramuscular injection. And track your sites carefully, because with fewer viable sites, rotation becomes more challenging and more important.
Traveling with semaglutide and injection sites
Travel does not change which injection sites you can use, but it changes the practical considerations around injection. Our complete guide to traveling with semaglutide covers storage, transport, and timing across time zones.
The key travel-specific injection tip is to plan your injection for a time and place where you can maintain proper hygiene and technique. A hotel room with a bathroom sink works fine. An airplane lavatory does not. If your travel day falls on your injection day, consider shifting your injection by a day to accommodate a more controlled environment.
Injection site comparison: which is right for you
This table summarizes the key differences between injection sites to help you make an informed decision based on your specific situation.
Factor | Abdomen | Thigh | Upper arm |
|---|---|---|---|
Absorption consistency | Most consistent | Slightly lower (12%) | Similar to abdomen |
Self-injection ease | Excellent | Good | Difficult |
Surface area for rotation | Largest | Moderate | Smallest |
Pain level (average) | Low to moderate | Moderate | Low |
Clothing interference | Waistband risk | Pant leg friction | Minimal |
Subcutaneous fat (typical) | Most ample | Variable | Moderate |
Bruising frequency | Moderate | Higher | Lower |
Best for | Most people, self-injection | Rotation alternative | Assisted injection |
Most people do best starting with the abdomen as their primary site and adding the thigh (or upper arm with assistance) as a rotation alternative. This gives you the most consistent absorption at your primary site while providing enough variety to prevent tissue damage from overuse.
The comparison becomes especially relevant when people are deciding between semaglutide and tirzepatide, as both medications use the same injection sites but may have different injection volumes. Understanding the site selection fundamentals covered here applies equally to both medications.
Building your complete injection routine
A good injection routine turns a weekly task into an autopilot habit. Here is a template that incorporates everything covered in this guide.
Pre-injection checklist (2 to 3 minutes)
Remove semaglutide from the refrigerator 15 to 30 minutes before your planned injection time. Check your rotation log to determine which site to use this week. Gather supplies: pen or syringe, alcohol swab, cotton ball, and sharps container. Wash hands thoroughly with soap and water.
Injection process (1 to 2 minutes)
Clean the injection site with alcohol and allow to dry. If using a pen, attach a new needle and dial your dose. If using a syringe, draw your dose carefully following your semaglutide conversion chart. Pinch skin if needed. Insert needle at the appropriate angle with a quick, confident motion. Inject slowly and steadily. Hold for the recommended count. Remove needle smoothly. Press gently with cotton. Dispose of needle in sharps container immediately.
Post-injection steps (30 seconds)
Record the injection in your tracking log: date, site location, dose, and any notes about comfort or reactions. Return semaglutide to the refrigerator if using a multi-dose vial. Check your remaining supply and reorder if you are within two weeks of running out.
That entire process takes less than five minutes once you have practiced it a few times. Most of that time is preparation and recording. The actual injection takes under 30 seconds. People who treat it as a quick, routine task rather than a medical event tend to have the most consistent, comfortable experiences.
SeekPeptides members access comprehensive protocol guides, dosage calculators, and injection tracking tools designed specifically for GLP-1 medication management. The platform provides everything you need to optimize your injection routine from day one through long-term maintenance.
Frequently asked questions about semaglutide injection sites
Can I inject semaglutide in the same spot every week?
No. Injecting in the same spot repeatedly causes lipodystrophy, which creates lumps or dents under the skin and reduces medication absorption. Rotate sites weekly, keeping at least one inch between injection spots and avoiding any specific location for at least four weeks before reusing it. Follow a structured dosing and rotation plan for best results.
Does the injection site affect how well semaglutide works for weight loss?
Research shows a minor absorption difference between sites (the thigh absorbs approximately 12% less than the abdomen), but this difference is not clinically significant. All three approved sites, abdomen, thigh, and upper arm, deliver effective medication levels for weight loss. Proper technique and consistent dosing matter far more than site selection.
Why does my semaglutide injection bruise sometimes but not always?
Bruising depends on whether the needle hits a small blood vessel beneath the skin. Blood vessel distribution varies across your injection sites, so some spots bruise while others do not, even in the same general area. Cold medication, fast injection speed, and blood-thinning medications or supplements increase bruising risk.
Is it normal for semaglutide injections to sting?
Mild stinging during injection is normal, especially with cold medication. Letting semaglutide reach room temperature before injection significantly reduces stinging. If the sting is severe, persistent, or accompanied by significant swelling, the needle may have been placed too shallow in the dermal layer rather than the subcutaneous layer. Adjust your injection technique accordingly.
Can I inject semaglutide in my buttocks?
The buttocks are not an FDA-approved injection site for semaglutide. While the area has adequate subcutaneous fat in most people, it is difficult to access for self-injection and has not been studied in clinical trials for this medication. Stick to the three approved sites: abdomen, thigh, and upper arm.
What should I do if I see a lump at my injection site?
Small, temporary lumps immediately after injection are usually just the medication forming a depot in the subcutaneous tissue. These resolve within hours. Persistent lumps lasting days or weeks could indicate a nodule reaction or early lipohypertrophy. Avoid that site for at least 8 weeks and consult your healthcare provider if the lump does not resolve.
Should I use a different injection site for different doses during titration?
Site selection does not need to change based on dose. The same rotation strategy works whether you are on the starting semaglutide dose of 0.25 mg or the maximum dose of 2.4 mg. Higher doses mean more fluid volume, which may create slightly more pressure at the injection site, so injecting slowly becomes even more important at higher doses.
Can I switch injection sites if one area becomes uncomfortable?
Absolutely. If an injection site develops persistent discomfort, visible skin changes, or bruising that does not resolve between weekly injections, switch to a different body area and let the affected site rest. This is one reason why maintaining multiple sites in your rotation is so important. People switching between GLP-1 medications should maintain the same rotation practices regardless of which medication they are using.
Semaglutide injection site resources by dose and formulation
Different semaglutide formulations and doses may have specific considerations that affect your injection experience. Here are resources organized by the most common scenarios.
For people using semaglutide 5mg/mL formulations, the injection volume is relatively small, which means site selection is flexible and pain is minimal. The 5mg vial dosage chart helps you determine exact volumes for each dose level.
Those working with 10mg vials benefit from even smaller injection volumes per dose, as the higher concentration means less fluid per injection. This can make the injection faster and reduce site reactions. Check the 10mg reconstitution chart for mixing instructions specific to this concentration.
For people using semaglutide combined with methylcobalamin or glycine, the injection volume may be slightly larger than standalone semaglutide. This does not change the recommended injection sites, but it does mean injecting more slowly is even more important to allow the larger volume to disperse comfortably.
People who are tracking their doses in different measurement systems can use our conversion guides: 20 units to mg, 40 units to mg, 50 units to mg, and 100 units to mg. Accurate dosing ensures you are injecting the correct amount at your chosen site every week.
How injection sites relate to semaglutide side effects
The relationship between injection site and systemic side effects is frequently misunderstood. Some people believe that injecting in the abdomen causes more nausea because the medication is closer to the stomach. This is not accurate.
Semaglutide works systemically. Once absorbed from the subcutaneous tissue into the bloodstream, it circulates throughout the body and acts on GLP-1 receptors in the brain, pancreas, and digestive tract. The injection site determines where the medication enters the bloodstream, not where it acts. Abdominal injection does not increase gastrointestinal side effects compared to thigh or arm injection.
That said, local side effects at the injection site are directly related to site selection and technique. Choosing sites with adequate subcutaneous fat reduces local pain and bruising. Proper rotation prevents tissue damage that could affect absorption over time. And correct needle depth prevents the muscle-related discomfort that can make the injection experience unnecessarily unpleasant.
If you are experiencing semaglutide side effects that seem to vary from week to week, consider whether your injection technique varies alongside them. Inconsistent technique can produce inconsistent absorption, which can cause variable side effect profiles. For managing specific side effects, resources on semaglutide constipation, fatigue, and dietary adjustments provide targeted guidance.
Comparing semaglutide injection sites with other GLP-1 medications
If you are considering or have used other GLP-1 medications, you might wonder whether injection site recommendations differ between them. They largely do not.
All subcutaneous GLP-1 receptor agonists use the same three approved injection sites: abdomen, thigh, and upper arm. The injection technique is identical. The rotation principles are the same. Whether you are using semaglutide, tirzepatide, or another GLP-1 medication, the fundamentals covered in this guide apply.
The differences between medications lie in injection volume (some require more fluid per dose), injection frequency (semaglutide is weekly, some are daily), and the specific pen injector design. For people switching between medications, the good news is that your injection site knowledge transfers completely.
Tirzepatide users can find specific guidance in our tirzepatide stomach injection guide and tirzepatide injection dosage chart. Retatrutide users should review our guide on where to inject retatrutide. The underlying principles remain consistent across all these GLP-1 medications, but each has nuances worth understanding.
Beyond injection sites: optimizing your complete semaglutide protocol
Injection site selection is one piece of a larger optimization puzzle. The best results come from combining proper injection technique with the right dose, appropriate timing, dietary adjustments, and consistent monitoring.
Start with understanding your semaglutide dosing schedule and how dose escalation works. Most protocols begin at 0.25 mg for four weeks, then increase to 0.5 mg, then 1 mg, and potentially higher depending on response and tolerability. Each dose increase may slightly change your injection experience because of the different medication volume, so be prepared to adjust your technique as needed.
Nutrition plays a significant role in how well semaglutide works alongside proper injection technique. Following a semaglutide-optimized diet plan and knowing which foods to eat on semaglutide maximizes the medication benefit you receive from each properly placed injection.
Storage also matters. Semaglutide that has been improperly stored may degrade, reducing its effectiveness regardless of how well you inject it. Understanding how long semaglutide lasts in the fridge and whether expired semaglutide is still effective helps you avoid wasting injections on degraded medication.
If you are not seeing expected results despite proper injection technique and consistent dosing, our guides on why you might not be losing weight on semaglutide and troubleshooting early weight loss stalls address the most common reasons and solutions.
For people who are considering alternatives or additions to their semaglutide protocol, comparing semaglutide with phentermine or exploring whether these medications can be combined requires understanding how each one works independently first. Proper injection technique for semaglutide remains the foundation regardless of what other interventions you add.
Monitoring your progress systematically makes all the difference. Track your weight, measurements, appetite changes, energy levels, and injection experiences weekly. This data helps you and your healthcare provider make informed decisions about dose adjustments, site rotation changes, and protocol modifications. SeekPeptides provides comprehensive tracking tools and evidence-based protocol guidance for members who want to optimize every aspect of their GLP-1 treatment.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
External resources
Injection-Site Nodules Associated With Semaglutide (Diabetes Spectrum)
Population Pharmacokinetics of Semaglutide (Diabetes Therapy)
In case I do not see you, good afternoon, good evening, and good night. May your injection sites stay comfortable, your rotation stay consistent, and your results stay on track.