Feb 22, 2026

Some people notice changes within days. Others wait weeks and wonder if anything is happening at all. The gap between those two experiences is not random, and it is not about willpower or luck. It comes down to pharmacokinetics, individual biology, the specific medication being used, and a handful of factors that most providers never explain in detail.
That uncertainty drives people to search for answers at 2 a.m., scrolling through forums, comparing notes with strangers, and questioning whether their medication is even working. It is a legitimate concern. GLP-1 receptor agonists do not flip a switch the moment they enter your body. They build. They accumulate. They gradually shift the signaling pathways in your brain and gut until, one day, you realize that the constant background noise of hunger has gone quiet.
This guide walks through exactly what happens from the moment a GLP-1 medication enters your system, hour by hour, week by week, month by month. It covers why semaglutide and tirzepatide work on different timelines, why appetite suppression arrives before weight loss does, why your neighbor lost ten pounds in month one while you lost three, and what the clinical trial data actually says about realistic expectations. Whether you are considering your first injection or sitting at week six wondering when results will show up, every answer you need is here.
What happens in your body after the first GLP-1 dose
The moment a GLP-1 receptor agonist enters your bloodstream, a cascade begins. Not a dramatic one. Not something you can feel immediately. But at the molecular level, things start shifting within hours.
GLP-1 receptor agonists are synthetic versions of a hormone your body already produces. Natural GLP-1 gets released from your gut after eating, but it degrades within minutes. The pharmaceutical versions are engineered to resist that breakdown, which is why a single injection of semaglutide can keep working for an entire week.
Here is what happens in sequence.
The first 24 hours
After subcutaneous injection, the medication begins absorbing from the injection site into your bloodstream. Absorption is gradual, not instant. For semaglutide, peak plasma concentration occurs roughly 24 to 72 hours after injection. Tirzepatide follows a similar pattern with peak levels around 8 to 72 hours. During this window, the drug molecules are finding and binding to GLP-1 receptors scattered throughout your body.
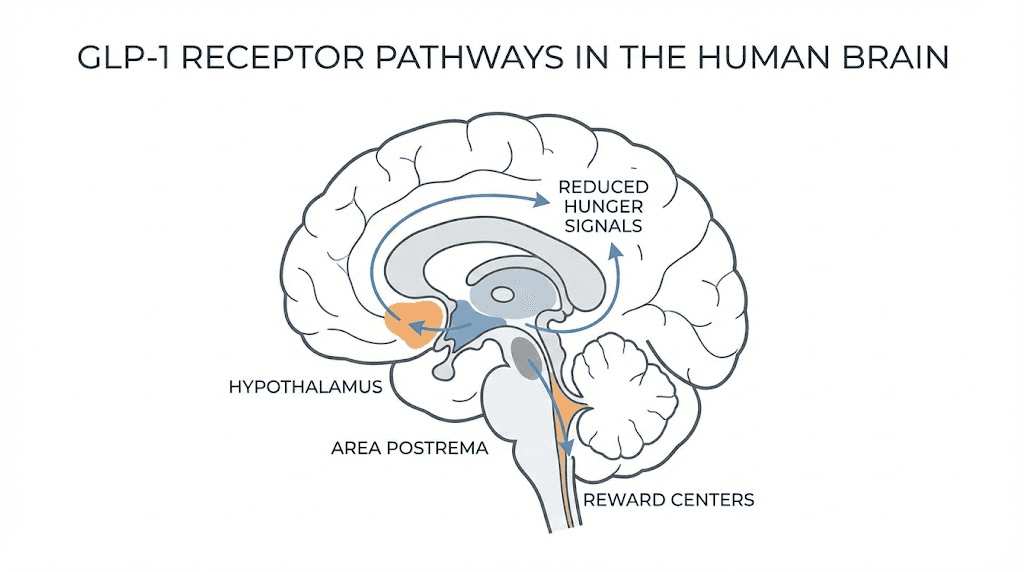
Those receptors are not just in your pancreas. They sit in the hypothalamus, the area postrema in your brainstem, the ventral tegmental area, and the nucleus accumbens. Each location produces a different effect. The hypothalamus controls hunger signals. The area postrema, which lacks a blood-brain barrier, detects circulating signals and can trigger nausea. The reward centers reduce the dopamine response to food, making that slice of pizza feel less compelling. Understanding where to inject GLP-1 matters because injection site affects absorption speed and consistency.
The brain response
GLP-1 crosses the blood-brain barrier through passive diffusion and receptor-mediated transcytosis. Once inside, it activates anorexigenic pathways. Specifically, it increases POMC and CART expression in the hypothalamus, the peptides that tell your brain you are full. Simultaneously, it decreases NPY and AgRP expression, the peptides that drive hunger and food-seeking behavior.
This is not a subtle effect. It is a fundamental rewiring of the hunger signaling system. But it takes time to build because receptor sensitivity needs to adjust and the medication needs to reach steady-state concentrations.
Some people feel mild appetite reduction within the first day or two. Most do not notice anything dramatic until the end of week one or the beginning of week two. Choosing the best time to take your GLP-1 shot can influence how quickly you notice these initial effects.
Gastric emptying changes
One of the fastest observable effects of GLP-1 therapy is delayed gastric emptying. Food sits in your stomach longer. You feel full sooner and stay full longer. This effect begins with the very first dose, though it strengthens over subsequent weeks as drug levels accumulate. The slowed gastric emptying is also responsible for much of the nausea that people experience early on, and understanding whether GLP-1 is the same as Ozempic helps clarify why different brand names produce similar gastrointestinal effects.
The complete GLP-1 timeline week by week
Clinical trials provide averages. Your experience will not match those averages exactly, and that is normal. But knowing the general trajectory helps set expectations and prevents premature frustration. Below is a comprehensive timeline based on published data from the STEP trials for semaglutide, the SURMOUNT trials for tirzepatide, and thousands of documented patient experiences.
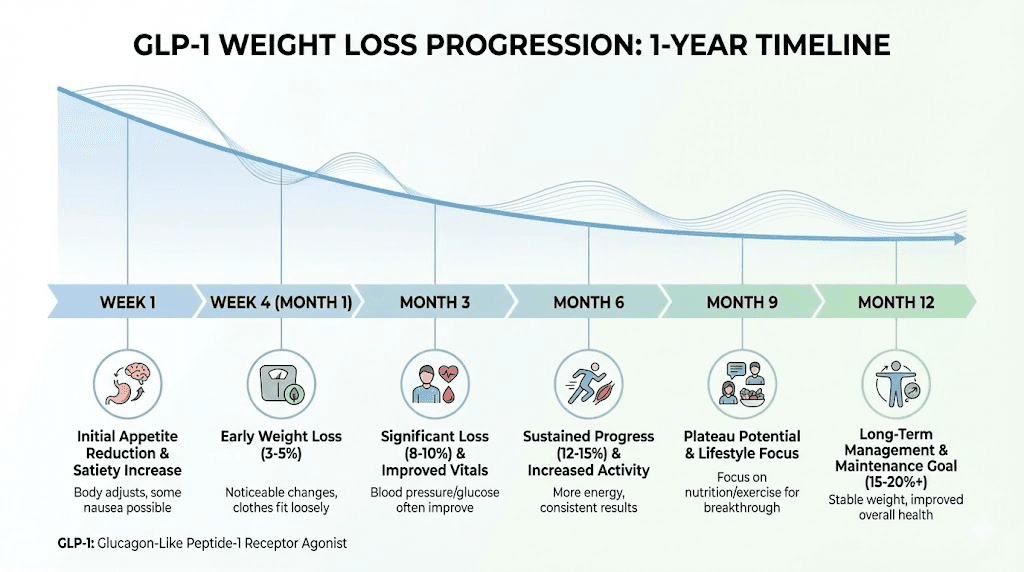
Week 1: first impressions
The first week is mostly about your body adjusting. You are on the lowest starting dose, which is intentionally subtherapeutic for weight loss. Semaglutide starts at 0.25 mg weekly. Tirzepatide starts at 2.5 mg weekly. These doses exist to let your gastrointestinal system adapt.
What you might notice:
Mild appetite reduction, particularly in the 24 to 72 hours after injection
Slight nausea, especially after eating large or fatty meals
A subtle sense of fullness that arrives sooner than expected
Some people notice absolutely nothing at this stage
Weight change in week one is typically minimal, zero to two pounds. Any significant weight loss at this point is usually water weight or reduced food intake from nausea, not fat loss. Do not read too much into week one results. The medication has barely begun accumulating in your system.
If you want to understand what realistic early outcomes look like, semaglutide one month results provides a clearer picture of where most people land after those initial weeks.
Weeks 2 to 4: building momentum
By week two, the medication is building toward meaningful blood levels. You are still on the starting dose, but with two to four injections behind you, cumulative drug exposure is increasing. Semaglutide has a seven-day half-life, which means it takes approximately four to five weeks to reach steady state at any given dose. Tirzepatide has a roughly five-day half-life, reaching steady state slightly faster.
This is where appetite suppression typically becomes noticeable for most people. The internal conversation around food starts changing. You might find yourself forgetting about lunch. Or eating half a meal and feeling genuinely satisfied. Or noticing that the 3 p.m. snack craving that used to be automatic simply does not show up.
Weight loss during weeks two through four typically ranges from two to five pounds total from baseline. The variation is enormous. Some individuals following a structured semaglutide diet plan see faster results, while others on a comparable tirzepatide diet plan experience a different trajectory entirely. Understanding which foods to eat while on semaglutide or what to eat on tirzepatide can meaningfully influence how quickly your body responds during this critical building phase.
Blood sugar improvements often appear before weight loss does. If you have type 2 diabetes or prediabetes, fasting glucose and post-meal spikes may start declining within the first one to two weeks. A1c changes will not show up on labs this early since A1c reflects a three-month average, but the underlying glucose dynamics are already shifting.
Weeks 5 to 8: the dose escalation phase
Most GLP-1 protocols involve dose escalation every four weeks. At week five, you typically move up to the next dose tier. For semaglutide, that means jumping from 0.25 mg to 0.5 mg. For tirzepatide, from 2.5 mg to 5 mg.
This is where things get interesting. And sometimes uncomfortable.
The higher dose amplifies appetite suppression significantly. Many people describe this as the moment when the medication "kicks in" for real. Food thoughts decrease further. Portions shrink naturally. The effort required to eat less disappears because the desire to eat more simply is not there.
But dose escalation can also bring back side effects. Nausea that had faded may return. Gastrointestinal symptoms like constipation or loose stools can reappear or intensify. These effects typically resolve within one to two weeks of adjusting to the new dose, following the same adaptation pattern you experienced initially. People who experience four weeks on semaglutide with no weight loss often find that the dose increase is what finally triggers meaningful changes.
Weight loss during weeks five through eight typically accelerates. Total weight loss from baseline reaches four to eight pounds for most individuals, with some outliers on both ends. The rate of loss increases compared to the first month because you are now at a pharmacologically active dose.
Weeks 9 to 12: approaching steady state
By weeks nine through twelve, the medication is reaching or has reached steady state at your current dose. This means drug levels are consistent from injection to injection, and the effects become more predictable and stable. The appetite suppression that fluctuated in earlier weeks now feels more like a constant baseline.
This is also the window where you can genuinely assess whether the medication is working for you. Clinical trials suggest that patients who achieve at least 5% body weight loss by months three to four are likely to be long-term responders. If you have not lost at least 5% by this point, it is worth discussing dose adjustment with your provider.
Total weight loss by week 12 typically ranges from 5% to 8% of starting body weight, depending on the medication and dose. The tirzepatide weight loss timeline tends to show slightly faster results at comparable time points due to its dual mechanism of action.
For visual context, before and after semaglutide results at the three-month mark typically show noticeable but not dramatic changes. The real transformation comes later.
Months 3 to 6: full therapeutic effect emerging
This is where the results become hard to ignore.
By month three, you are typically at or approaching the maintenance dose. For semaglutide, the target dose for weight management is 2.4 mg weekly. For tirzepatide, it ranges from 5 mg to 15 mg weekly depending on individual response and tolerance. Each dose escalation restarts the four-to-five-week steady-state clock, which is why the full therapeutic effect takes several months to emerge.
Weight loss during this period is often linear and consistent, roughly one to two pounds per week at the maintenance dose. Total weight loss from baseline reaches 10% to 15% of starting body weight for many patients. This is the phase where clothes start fitting differently, friends start commenting, and the scale reflects a number you might not have seen in years.
A1c improvements are now measurable on lab work. Semaglutide at therapeutic doses reduces A1c by 1.0 to 1.5 percentage points on average. Tirzepatide achieves even larger reductions, up to 2.0 to 2.3 percentage points in clinical trials. These are clinically significant improvements that can move people from diabetic to prediabetic ranges, or from prediabetic to normal. The before and after tirzepatide weight loss results at this stage often show striking transformations.
Beyond weight and blood sugar, many patients report improvements in energy levels, sleep quality, joint pain from reduced weight bearing, and even mental clarity. Some of these benefits relate directly to whether semaglutide gives you energy through metabolic improvements, while tirzepatide users often ask whether tirzepatide provides an energy boost as well.
Months 6 to 12 and beyond: maximum results and maintenance
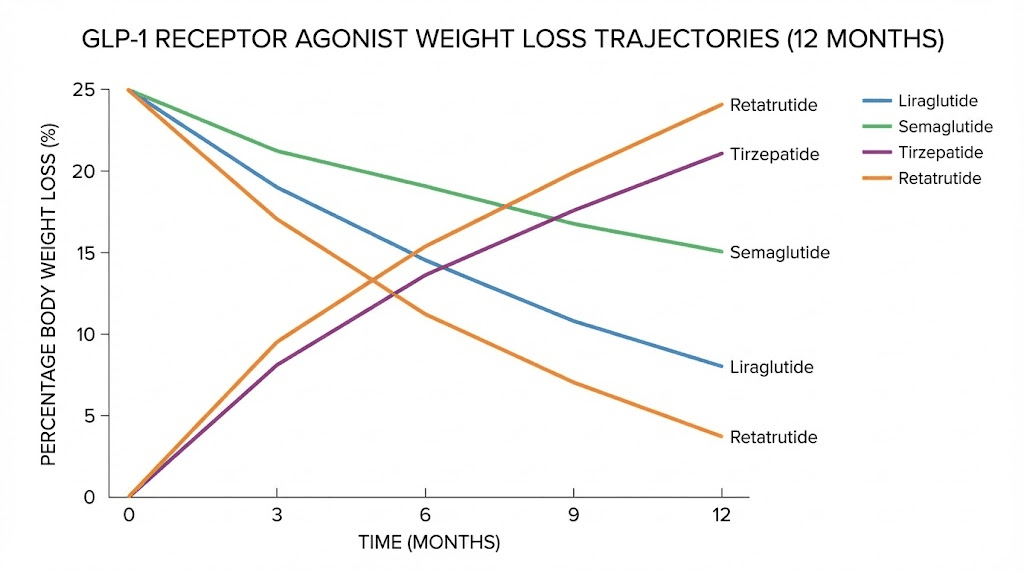
The STEP trials showed that semaglutide 2.4 mg produces an average of approximately 15% body weight loss by week 68, roughly 16 months. The SURMOUNT trials demonstrated tirzepatide at 15 mg achieving 15% to 21% body weight loss by week 72, about 17 months. These are averages, meaning some individuals exceed them substantially.
Weight loss typically plateaus somewhere between months 12 and 18. This is not the medication failing. It is your body reaching a new equilibrium where energy expenditure matches your reduced caloric intake at the lower body weight. The medication continues working to maintain that new set point, which is why discontinuation often leads to weight regain.
For those curious about the visual impact over time, men before and after tirzepatide results at the six-to-twelve month mark can be remarkable, and tirzepatide before and after documentation across genders consistently shows that the most dramatic visual changes occur between months four and ten.
Understanding how long to stay on semaglutide for weight loss is an important part of long-term planning, since premature discontinuation is one of the most common mistakes people make once results feel stable.
How fast each GLP-1 medication works
Not all GLP-1 medications are created equal. Their chemical structures, receptor binding profiles, half-lives, and dosing schedules create meaningfully different timelines. Here is what the data shows for each major option.
Semaglutide: the weekly standard
Semaglutide remains the most widely prescribed GLP-1 receptor agonist for weight management. Its seven-day half-life enables once-weekly dosing, and it reaches steady state at any given dose in approximately four to five weeks.
The dose escalation schedule spans 16 to 20 weeks: 0.25 mg for four weeks, 0.5 mg for four weeks, 1.0 mg for four weeks, 1.7 mg for four weeks, and finally 2.4 mg as the maintenance dose. This means you do not reach the full therapeutic dose until roughly month four or five.
In the STEP 1 trial, patients on semaglutide 2.4 mg lost an average of 14.9% of their body weight by week 68. At week 12, the average loss was approximately 6%. By week 28, it reached about 10%. The weight loss curve follows a pattern of rapid initial loss that gradually decelerates over time.
For a detailed look at how quickly effects manifest, the dedicated guide on how fast semaglutide works breaks down the pharmacokinetics in detail, while how long it takes semaglutide to work addresses the specific question of onset timing. Understanding the semaglutide dosage chart in units helps track exactly where you are in the escalation process, and our semaglutide dosage calculator can help you determine precise dosing.
Tirzepatide: the dual agonist advantage
Tirzepatide is not simply another GLP-1 agonist. It is a dual GIP and GLP-1 receptor agonist, meaning it activates two incretin pathways simultaneously. This dual mechanism appears to produce faster and more pronounced appetite suppression for many patients, along with greater total weight loss.
Tirzepatide has a half-life of approximately five days, slightly shorter than semaglutide. Despite this, its dual receptor activity creates a more potent appetite-suppressing effect at comparable time points. Many users report stronger appetite reduction within the first two weeks compared to semaglutide.
The SURMOUNT-1 trial showed tirzepatide at 5 mg producing 7.6 kg of weight loss at 40 weeks. The 10 mg dose achieved 9.3 kg. The 15 mg dose reached 11.2 kg at the same time point. For comparison, semaglutide 2.4 mg achieved 5.7 kg at 40 weeks in the head-to-head SURMOUNT-2 crossover data. That is a meaningful difference.
To understand tirzepatide-specific timing, how fast tirzepatide works covers the pharmacokinetic details, and how long it takes for tirzepatide to work addresses onset expectations. The tirzepatide dosage chart in units helps track your escalation progress, and whether tirzepatide increases metabolism explores the metabolic advantages of the dual agonist approach.
Liraglutide: the daily option
Liraglutide was the first GLP-1 receptor agonist approved specifically for weight management under the brand name Saxenda. It requires daily injections because its half-life is only 13 hours, reaching steady state within two to three days.
The shorter half-life means liraglutide reaches stable blood levels much faster than semaglutide or tirzepatide. Some patients notice appetite suppression within the first few days. However, the trade-off is less total weight loss. The SCALE trials showed liraglutide 3.0 mg producing approximately 8% body weight loss over 56 weeks, roughly half of what semaglutide achieves.
The dose escalation for liraglutide spans about five weeks: 0.6 mg for one week, 1.2 mg for one week, 1.8 mg for one week, 2.4 mg for one week, and then 3.0 mg as the maintenance dose. Because of the rapid steady state, you are at the full therapeutic dose and experiencing maximum effects much sooner than with weekly injectables.
Retatrutide: the triple agonist frontier
Retatrutide represents the next evolution, a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. The addition of glucagon receptor activation increases energy expenditure directly, theoretically producing faster fat loss.
Phase 2 trial data showed remarkable results, with participants losing up to 24% of body weight over 48 weeks at the highest dose. That exceeds anything achieved by semaglutide or tirzepatide in comparable time frames. Early reports suggest appetite suppression onset is similar to tirzepatide, with meaningful effects within the first two to four weeks. For a detailed comparison, retatrutide versus semaglutide breaks down the differences, while the retatrutide dosage chart for weight loss and retatrutide dose complete guide provide dosing specifics.
Emerging options worth knowing about
The GLP-1 landscape is expanding rapidly. Mazdutide versus tirzepatide comparisons are emerging as mazdutide enters late-stage trials. Survodutide versus tirzepatide data is also becoming available for the GLP-1/glucagon dual agonist. The oral GLP-1 space is advancing too, with orforglipron versus tirzepatide representing a potential future where daily pills replace weekly injections. And for those comparing across the triple agonist space, mazdutide versus retatrutide and Ozempic versus retatrutide provide helpful context.
The head-to-head semaglutide versus tirzepatide dosage chart remains the most useful comparison tool for the two medications that are currently most accessible, and our broader semaglutide versus tirzepatide comparison page provides a full breakdown.
Appetite suppression vs weight loss vs blood sugar: three different timelines
One of the biggest sources of confusion is that GLP-1 medications produce multiple effects, and each one operates on its own timeline. Appetite suppression, weight loss, and blood sugar improvement do not arrive at the same time. Understanding this prevents the frustration of expecting one outcome while experiencing another.
Appetite suppression: the first signal
Appetite reduction is typically the first noticeable effect. It can begin within days of the first injection, though it is often subtle at starting doses. By weeks two through four, most people on semaglutide or tirzepatide report meaningful appetite changes. Peak appetite suppression, the strongest reduction in hunger and food-related thinking, typically occurs around weeks 12 to 14 at therapeutic doses.
The nature of the suppression is worth describing because it differs from what most people expect. It is not that food becomes repulsive. It is that the urgency around eating diminishes. The background hum of "what should I eat next" goes quiet. You can still enjoy food. You simply do not obsess over it.
For timing specifics, how long it takes for semaglutide to suppress appetite covers the semaglutide timeline in detail, while how long it takes for tirzepatide to suppress appetite addresses the tirzepatide-specific experience. If you are wondering whether the effect is instant, whether semaglutide suppresses appetite immediately answers that directly.
Blood sugar improvements: faster than you think
Glucose metabolism responds to GLP-1 therapy faster than body weight does. GLP-1 receptor agonists enhance glucose-dependent insulin secretion, meaning they help your pancreas release more insulin when blood sugar rises after meals. This effect begins working within the first week.
Fasting glucose levels often show improvement within one to two weeks. Post-meal glucose spikes start blunting within days. However, A1c, which reflects your average blood sugar over roughly three months, will not show meaningful changes on lab work until you have been on the medication for at least eight to twelve weeks.
Optimal A1c reduction typically takes 12 to 16 weeks at therapeutic doses. Semaglutide reduces A1c by 1.0 to 1.5 percentage points on average. Tirzepatide achieves reductions of up to 2.0 to 2.3 percentage points, which is among the largest A1c improvements seen with any diabetes medication.
Weight loss: the slowest but most visible outcome
Weight loss is the outcome everyone focuses on, but it is the slowest to manifest in meaningful amounts. While the scale might show a pound or two in the first week, clinically significant weight loss, defined as 5% or more of starting body weight, typically requires four to twelve weeks depending on the medication and dose.
The math is straightforward. A pound of fat contains roughly 3,500 calories. Even with significant appetite suppression reducing intake by 500 to 700 calories per day, actual fat loss accumulates at one to two pounds per week. Any larger drops in the first few weeks are predominantly water, glycogen depletion, and reduced food volume in the digestive tract.
Most of the total weight loss occurs in the first four to five months of treatment. After that, the rate of loss decelerates, eventually reaching a plateau where the body reaches a new energy balance.
Energy and mood: the bonus timeline
Many people notice improvements in energy, mood, and mental clarity as secondary benefits. These changes follow a variable timeline but often emerge between weeks four and twelve. Part of this is physiological, better blood sugar stability means fewer energy crashes and less brain fog. Part is psychological, losing weight and feeling in control of eating habits naturally improves mood. The question of whether semaglutide gives you energy and whether tirzepatide provides an energy boost both have nuanced answers that depend on individual starting points.
Why some people respond faster than others
Two people can start the same medication on the same day at the same dose and have completely different experiences by week four. This is not a flaw in the medication. It reflects the reality that individual biology creates enormous variation in drug response. Here are the major factors that determine your personal timeline.
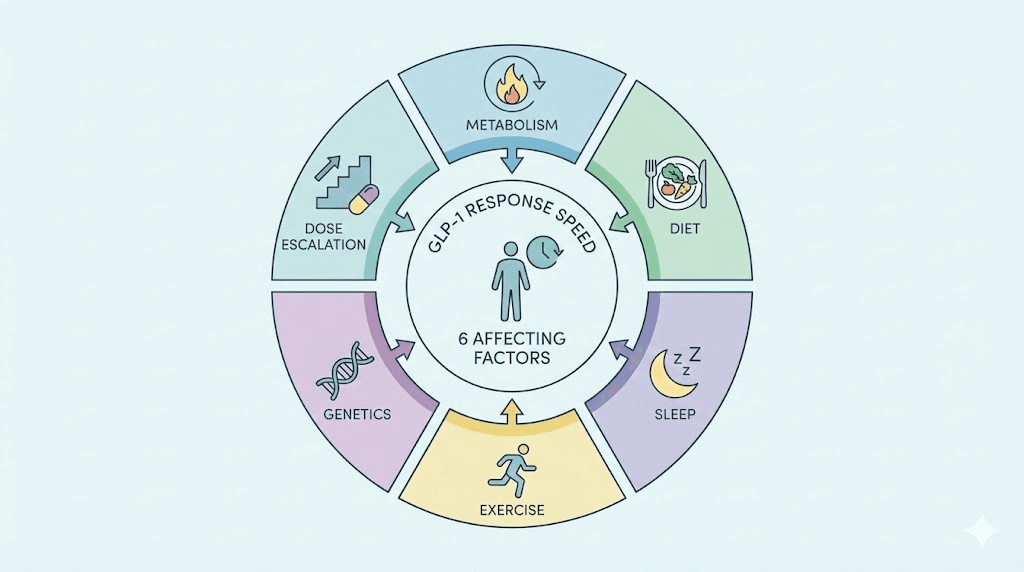
Starting weight and metabolic health
People with higher starting weights often lose more absolute weight in the early weeks, partly because their higher caloric needs create a larger deficit when appetite decreases. However, percentage weight loss tends to be relatively similar across starting weights, meaning someone starting at 200 pounds and someone starting at 300 pounds may both lose roughly 15% by 68 weeks, even though the absolute numbers differ dramatically.
Metabolic health matters too. Individuals with insulin resistance or type 2 diabetes sometimes respond more slowly in terms of weight loss, though their blood sugar improvements are often faster and more pronounced. The medication is addressing their metabolic dysfunction first, and weight loss follows as insulin sensitivity improves.
Dose escalation speed
How quickly you move through the dose escalation schedule directly impacts your timeline. Standard protocols increase doses every four weeks. Some providers are more conservative, holding at lower doses for six to eight weeks before escalating. Others move faster in some cases. Slower escalation means fewer side effects but a longer wait for full therapeutic effects. Faster escalation means reaching the effective dose sooner but potentially dealing with more intense gastrointestinal side effects.
Diet quality and protein intake
What you eat while on a GLP-1 medication matters enormously. The medication reduces appetite, but if you continue eating calorie-dense, processed foods in smaller amounts, weight loss will be slower than if you shift toward protein-rich, nutrient-dense options.
Protein is particularly important. GLP-1-induced weight loss can include lean mass loss if protein intake is insufficient. Adequate protein, generally 0.7 to 1.0 grams per pound of body weight daily, helps preserve muscle while losing fat. It also enhances satiety, working synergistically with the medication. Following a structured approach using foods recommended while on semaglutide or understanding what to eat on tirzepatide makes a measurable difference. Equally important is knowing which foods to avoid on semaglutide and which foods to avoid on tirzepatide, since certain food choices can worsen side effects and slow progress.
Sleep and stress
Cortisol, the primary stress hormone, promotes fat storage and increases appetite. Chronic stress and poor sleep elevate cortisol chronically, which can partially counteract the appetite-suppressing effects of GLP-1 therapy. Sleep deprivation also disrupts ghrelin and leptin signaling, the hunger and satiety hormones that GLP-1 medications are designed to modulate.
People who prioritize seven to nine hours of quality sleep and manage stress effectively tend to see faster and more consistent results. This is not a "nice to have." It is a pharmacologically relevant factor that directly impacts how well your medication works.
Exercise habits
Exercise does not drive the majority of weight loss, but it significantly influences the quality of weight loss and the speed of visible changes. Resistance training preserves lean muscle mass, which keeps metabolic rate higher and improves body composition even when the scale moves slowly. Cardiovascular exercise creates additional caloric deficit and improves insulin sensitivity.
That said, some people who struggle with exercise find that GLP-1 therapy creates an indirect exercise benefit. As weight decreases and energy improves, physical activity becomes easier and more appealing, creating a positive feedback loop. For those wondering about results without exercise, losing weight on semaglutide without exercise is possible, though outcomes tend to be better with at least some physical activity.
Genetics and receptor sensitivity
Individual variation in GLP-1 receptor expression, density, and sensitivity creates a genetic component to treatment response. Some people have receptor variants that make them more or less responsive to GLP-1 agonists. This is not something you can control, test for, or change. But it explains why some individuals respond dramatically at low doses while others need maximum doses to achieve similar effects.
Compounded versus pharmaceutical versions
The source of your medication matters. Pharmaceutical-grade semaglutide and tirzepatide from FDA-approved manufacturers have rigorous quality controls, consistent potency, and verified purity. Compounded versions, produced by compounding pharmacies, may vary in quality. A comprehensive look at compounded semaglutide explains the differences, quality considerations, and what to look for.
The supplements recommended alongside tirzepatide can also influence response speed by addressing nutritional deficiencies that may impair metabolic function or worsen side effects.
What to do when your GLP-1 does not seem to be working
You have been on the medication for weeks. The scale has barely moved. You still think about food constantly. You are starting to wonder if you are one of the non-responders. Before reaching that conclusion, there are several factors to evaluate.
The patience factor
First, understand that the timeline described above is based on averages, and averages mask enormous individual variation. Some people simply take longer to respond. If you are in the first four to six weeks on a starting dose, you may not have given the medication enough time or dose to show meaningful effects. Patience sounds like unhelpful advice, but pharmacokinetics do not care about your timeline. The drug needs time to accumulate.
Common mistakes that slow results
Several behavioral patterns can undermine GLP-1 effectiveness:
Eating through the appetite suppression. Some people continue eating their normal portions out of habit despite feeling full sooner. The medication reduces hunger, but it does not prevent you from overriding that signal. Mindful eating, stopping when satisfied rather than when the plate is clean, is essential.
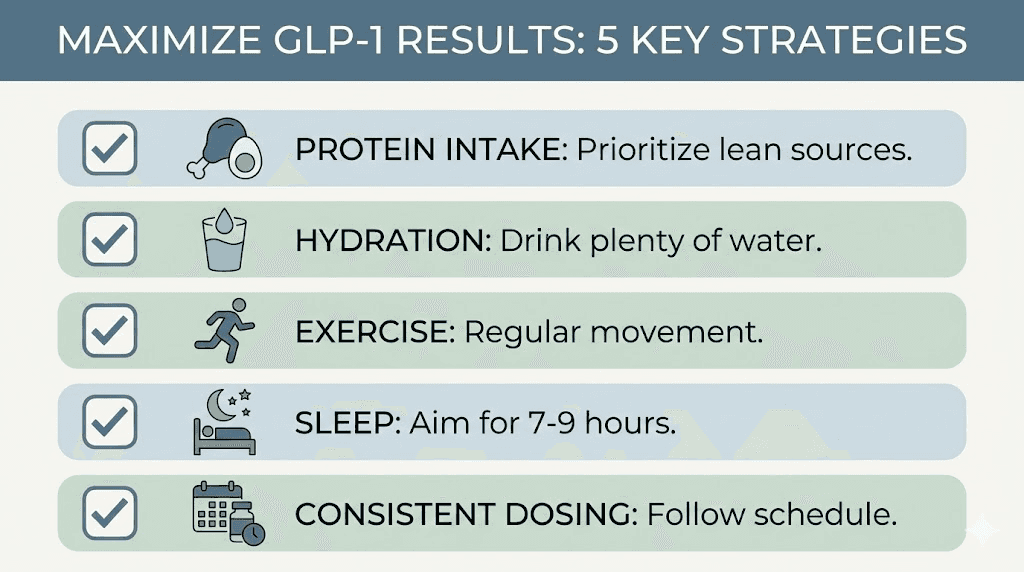
Skipping doses or inconsistent timing. Missing injections disrupts the steady-state concentration that the medication needs to work effectively. Consistent weekly dosing at roughly the same time each week produces the best results.
Compensating with calorie-dense liquids. Smoothies, juices, alcohol, and high-calorie coffee drinks bypass much of the gastric emptying delay that makes you feel full. Liquid calories are the most common hidden saboteur of GLP-1 weight loss. Understanding whether you can drink on semaglutide and whether you can drink on tirzepatide is particularly important for managing caloric intake.
Insufficient protein intake. Low protein leads to muscle loss, which lowers metabolic rate, which slows weight loss. It also reduces satiety between meals.
When to discuss a dose increase
If you have been at your current dose for four or more weeks with minimal appetite suppression or weight change, a dose increase is usually the appropriate next step. Most providers follow the standard escalation schedule, but some patients need to move up sooner, and a few do well staying at intermediate doses longer. The key indicator is whether you are experiencing meaningful appetite reduction. If not, the dose is likely too low.
For deeper guidance on this situation, why you are not losing weight on semaglutide and why you are not losing weight on tirzepatide cover the full spectrum of reasons and solutions. The guide on four weeks on semaglutide with no weight loss specifically addresses early non-response, while tirzepatide not working anymore addresses the scenario where effects diminish over time.
When to talk to your provider
If you have reached the maximum recommended dose and maintained it for 12 to 16 weeks without achieving at least 5% body weight loss, a conversation with your provider is warranted. Options at that point may include switching medications, adding adjunctive therapy, investigating underlying conditions like hypothyroidism or PCOS, or reassessing whether this medication class is right for you.
The GLP-1 plateau and how to push past it
Plateaus are normal. They are frustrating, sometimes demoralizing, but they are a predictable part of the weight loss trajectory with any intervention. Understanding why they happen and how long they last makes them manageable rather than panic-inducing.
Why plateaus happen
As you lose weight, your body adapts. Your metabolic rate decreases because you are now a smaller person requiring fewer calories. Your body also becomes more efficient, extracting more energy from the food you eat. This is metabolic adaptation, and it is not a sign that your medication has stopped working. It is basic thermodynamics meeting evolutionary biology.
Additionally, the appetite-suppressing effects of GLP-1 medications can partially attenuate over time as receptors adjust to sustained stimulation. This does not mean the medication is no longer active. It means the relative impact may be less dramatic than it was during the initial months.
Typical plateau timing and duration
Most patients experience their first significant plateau somewhere between months three and six. These plateaus typically last two to eight weeks before weight loss resumes, either spontaneously or with intervention. Some people experience multiple shorter plateaus throughout their weight loss journey. The semaglutide plateau guide provides detailed strategies for breaking through.
Strategies for breaking through
Dose adjustment is the most direct pharmacological approach. If you have not yet reached the maximum dose, escalation often restarts weight loss. Some providers also use microdosing approaches with tirzepatide or adjust timing to address plateaus.
Beyond dose changes, dietary modifications can help. Reducing carbohydrate intake, increasing protein, cycling caloric intake, or implementing time-restricted eating windows can break through metabolic adaptation. Exercise intensity adjustments, particularly adding or increasing resistance training, can also shift the equation.
Stress and sleep remain underrated plateau contributors. A two-week stretch of poor sleep or high stress can stall weight loss entirely, independent of diet and medication adherence. Addressing these lifestyle factors is sometimes the simplest path through a plateau.
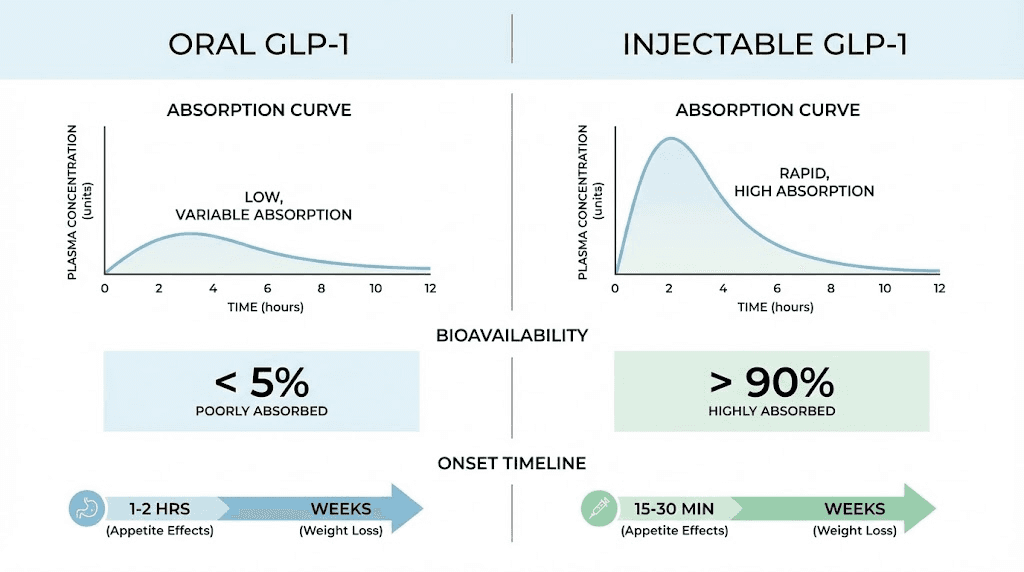
Oral vs injectable GLP-1: does delivery method change the timeline
The GLP-1 space is expanding beyond weekly injections. Oral formulations represent a major shift in accessibility and convenience, but they come with different pharmacokinetic profiles that affect onset and timeline.
Oral semaglutide
Oral semaglutide, marketed as Rybelsus, was the first oral GLP-1 receptor agonist. It uses a formulation technology called SNAC that enhances absorption through the stomach lining. However, oral bioavailability is only about 1%, meaning you need a much higher absolute dose to achieve comparable blood levels to the injectable form.
The clinical implications for timeline are meaningful. Oral semaglutide reaches peak plasma levels in about 60 to 90 minutes, much faster than injectable. But because it must be taken daily on an empty stomach with minimal water, and because absorption varies significantly day to day, achieving consistent steady-state levels takes longer and is less predictable.
Weight loss with oral semaglutide 14 mg, the highest approved dose, is approximately 8% to 10% of body weight over a similar time frame where injectable semaglutide achieves 15%. The oral semaglutide drops complete guide covers the nuances of the sublingual formulation, while the semaglutide sublingual complete guide provides specific administration details.
Oral tirzepatide
Oral tirzepatide is in advanced development and early data suggests it may achieve weight loss results closer to injectable tirzepatide than oral semaglutide achieves relative to its injectable counterpart. The oral tirzepatide complete guide covers what is known so far, and the comparison between tirzepatide oral versus injection helps weigh the pros and cons of each route.
Additional oral and alternative delivery formats are emerging. Tirzepatide drops represent another delivery approach, and the comparison between tirzepatide tablets versus injections addresses how formulation affects onset and efficacy. Some providers offer tirzepatide sublingual dosing, which has its own absorption characteristics. Even transdermal delivery is being explored through GLP-1 patches like Onmorlo.
Timeline differences between delivery methods
In general, injectable GLP-1 medications produce faster, more predictable, and more pronounced effects compared to oral formulations. The timeline for noticeable appetite suppression is similar, within one to four weeks, but the magnitude of appetite reduction and ultimate weight loss tends to be greater with injectables.
The primary advantages of oral formulations are convenience and needle avoidance, not faster onset. If speed of results is your priority, injectable formulations currently offer the most reliable timeline. For those using GLP-1 six in one oral liquid formulations, understanding the absorption differences from injectable forms is particularly important for setting realistic expectations.
Side effects timeline: what to expect and when they fade
Side effects follow their own timeline that is largely predictable but varies by individual. Knowing when to expect what, and when it should resolve, helps distinguish between normal adjustment and something that warrants medical attention.
Nausea: the most common early side effect
Nausea affects 30% to 50% of GLP-1 users at some point during treatment. It typically begins within the first one to three days after an injection, peaks during the first week, and gradually diminishes over the next two to four weeks as your body adjusts to the medication.
Importantly, nausea can reappear with each dose increase. When you escalate from 0.5 mg to 1.0 mg of semaglutide, for example, the nausea pattern may reset. This is normal and expected. The severity is usually less intense than the initial onset, and the duration of adjustment is shorter.
Most people find that nausea resolves completely within the first two months of treatment at a stable dose. If it persists beyond that, medication timing, eating patterns, and hydration should be evaluated.
Gastrointestinal effects
Beyond nausea, the full spectrum of GI side effects includes constipation, diarrhea, bloating, and abdominal discomfort. These typically emerge in the first two to four weeks and improve as the body adapts.
Constipation is particularly common because slowed gastric emptying means everything moves more slowly through the digestive tract. The semaglutide constipation treatment guide and tirzepatide constipation treatment guide provide specific strategies for managing this side effect. For those dealing with the opposite issue, how long tirzepatide diarrhea lasts addresses that concern.
Other gastrointestinal symptoms like semaglutide burping and general digestive discomfort tend to follow a similar pattern of onset and resolution.
Fatigue
Fatigue affects a subset of GLP-1 users, typically during the first four to eight weeks of treatment. It can result from reduced caloric intake, the body adapting to different energy sources, or dehydration from reduced fluid intake alongside reduced food intake.
The GLP-1 fatigue complete guide provides comprehensive strategies for managing tiredness during treatment. The semaglutide fatigue guide and the guide on whether tirzepatide makes you tired address medication-specific considerations.
Headaches
Headaches are reported by approximately 10% to 15% of GLP-1 users, typically in the first few weeks. They are often related to dehydration, reduced caloric intake, or caffeine withdrawal if coffee consumption decreases alongside overall food intake. The GLP-1 headache complete guide covers causes and solutions, while whether tirzepatide causes headaches addresses tirzepatide-specific concerns. Some users also experience semaglutide dizziness, which shares some of the same underlying causes.
Muscle pain and body aches
A less commonly discussed side effect is musculoskeletal discomfort. Tirzepatide side effects including muscle pain can occur during the first few months and may relate to rapid body composition changes or electrolyte shifts. Tirzepatide body aches tend to be transient and manageable with adequate hydration, electrolyte supplementation, and gentle movement.
Anxiety and mood changes
Some individuals report mood changes during GLP-1 therapy. The question of whether tirzepatide can cause anxiety is one that comes up frequently in online communities. While GLP-1 receptors exist in brain regions associated with mood and reward, serious mood disturbances are uncommon and should be reported to a provider if they occur.
Sleep disruption
Tirzepatide insomnia is reported by some users, particularly in the early weeks of treatment or after dose increases. The relationship between GLP-1 agonists and sleep is complex because while some people experience initial sleep disruption, others report improved sleep quality as weight decreases and metabolic health improves.
Hair loss: the delayed side effect
Hair loss related to GLP-1 therapy typically does not appear until months three to six, making it a delayed side effect that catches many users off guard. It is usually related to telogen effluvium, a temporary hair shedding condition triggered by rapid weight loss and nutritional changes rather than by the medication itself.
The GLP-1 hair loss complete guide explains the mechanisms, prevention strategies, and expected regrowth timeline. Adequate protein and micronutrient intake can significantly reduce the risk.
Side effects comparison between medications
A detailed semaglutide versus tirzepatide side effects comparison shows that while both medications share similar side effect profiles, the severity and duration can differ. In general, tirzepatide tends to produce similar rates of nausea but potentially different patterns of gastrointestinal effects due to its additional GIP receptor activity.
Maximizing how fast your GLP-1 works
While you cannot change your genetics or receptor sensitivity, several modifiable factors can meaningfully accelerate your GLP-1 response. These are not magic tricks. They are evidence-based strategies that optimize the environment in which your medication operates.
Protein-first eating
When your appetite is reduced, every bite matters more. Prioritizing protein at each meal serves multiple purposes: it preserves lean mass during weight loss, it enhances the satiety effects of GLP-1 medications, and it supports metabolic rate. Aim for 25 to 40 grams of protein per meal. Start each meal with protein before moving to vegetables and then carbohydrates. Protein shakes designed for GLP-1 users can help when solid food feels challenging during periods of strong appetite suppression.
Hydration
Dehydration is a stealth saboteur of GLP-1 results. When appetite decreases, fluid intake often decreases alongside it because much of our daily hydration comes from food. Dehydration can cause headaches, fatigue, and constipation, all of which mimic or worsen GLP-1 side effects. Aim for a minimum of 64 ounces of water daily, more if you are active or in a warm climate.
Injection timing and consistency
Consistency matters more than the specific day or time. Pick a day of the week and a general time of day, then stick with it. Consistent timing maintains steady drug levels, which produces more consistent appetite suppression. The guide on the best time of day to take semaglutide covers timing considerations in detail. Choosing the best injection site for semaglutide and learning how to give a semaglutide injection with a syringe correctly also ensures optimal absorption.
Exercise: prioritize resistance training
If you can only do one type of exercise while on GLP-1 therapy, choose resistance training. Weight loss inevitably involves some lean mass loss, and resistance training is the most effective countermeasure. It preserves metabolic rate, improves body composition, enhances insulin sensitivity, and creates a better visual result for the same amount of weight lost.
That does not mean cardio has no value. It does. But if time is limited, lifting weights, using resistance bands, or doing bodyweight strength exercises three to four times per week will produce better outcomes than cardio alone.
Sleep optimization
Seven to nine hours of quality sleep per night is not a luxury when you are on GLP-1 therapy. It is a performance enhancer. Sleep deprivation increases ghrelin, the hunger hormone, by up to 15%. It decreases leptin, the satiety hormone, by a similar amount. It elevates cortisol, promotes insulin resistance, and impairs decision-making around food.
Prioritize sleep hygiene: consistent bed and wake times, cool dark room, limited screens before bed, no caffeine after early afternoon. The return on investment for sleep optimization is enormous.
Supplement considerations
Certain supplements may support GLP-1 therapy outcomes. B12 supplementation is common because GLP-1 medications can reduce B12 absorption over time. The guides on semaglutide with B12 and tirzepatide with B12 cover the rationale and dosing. Glycine is another supplement gaining attention for its potential synergistic effects, with semaglutide with glycine and tirzepatide with glycine guides exploring this combination.
For compounded formulations that combine multiple ingredients, the tirzepatide glycine B12 compound guide and semaglutide methylcobalamin guide provide detailed information. The tirzepatide methylcobalamin guide covers the same territory for tirzepatide-based compounds.
SeekPeptides members access detailed supplement protocols, interaction databases, and evidence-based guidance for optimizing their GLP-1 therapy, including which supplements to prioritize and which to avoid.
Switching GLP-1 medications and how it affects your timeline
Switching between GLP-1 medications is increasingly common as patients seek better results, fewer side effects, or respond to availability changes. Each switch resets aspects of your timeline while preserving others.
Semaglutide to tirzepatide
Switching from semaglutide to tirzepatide is the most common transition, typically motivated by a desire for greater weight loss or a plateau on semaglutide. The semaglutide to tirzepatide switching dosage chart provides specific dose conversion guidance.
When making this switch, the GLP-1 receptor activity remains engaged since you are not starting from scratch. However, the addition of GIP receptor activation is new to your system, and some adaptation period is expected. Most people notice increased appetite suppression within one to two weeks of the switch, sometimes with a temporary increase in GI side effects as the body adjusts to the dual agonist.
The semaglutide to tirzepatide conversion chart helps ensure you start tirzepatide at an appropriate dose based on your semaglutide history.
Tirzepatide to semaglutide
The reverse switch, tirzepatide to semaglutide, is less common but occurs due to insurance changes, availability issues, or side effect preferences. The guide on switching from tirzepatide to semaglutide covers the logistics and expectations. The tirzepatide to semaglutide conversion chart provides dose equivalences.
Patients switching from tirzepatide to semaglutide should expect somewhat reduced appetite suppression and potentially slower weight loss, given that they are moving from a dual agonist to a single agonist. The GLP-1 receptor remains engaged, so the transition is typically smooth from a tolerability standpoint.
Moving to retatrutide after tirzepatide
For those exploring the next generation, how long retatrutide takes to kick in after tirzepatide addresses the specific transition timeline. The retatrutide dosage schedule after high-dose tirzepatide provides protocol guidance for this increasingly discussed transition.
Dose conversion considerations
There is no perfect dose equivalence between different GLP-1 medications because they work through different receptor combinations and have different potencies. The conversion charts available through SeekPeptides provide the best available guidance based on clinical data and documented patient experiences, but individual adjustment is always necessary.
When switching medications, expect a two-to-four-week adjustment period where side effects may fluctuate and appetite suppression may vary. This is a temporary reset, not a return to square one.
Reconstitution, storage, and preparation: protecting your timeline
For those using compounded GLP-1 formulations rather than pre-filled brand-name injectors, proper handling directly impacts how well and how consistently the medication works. Degraded peptide means reduced potency, which means a slower, less predictable response timeline.
Proper reconstitution is essential. The guides on how to reconstitute semaglutide and how to reconstitute tirzepatide walk through the process step by step. Getting the dilution right matters because incorrect reconstitution leads to inaccurate dosing, which undermines the entire dose escalation schedule.
Understanding stability and expiration is equally important. Whether semaglutide expires after 28 days, whether tirzepatide expires, and how long semaglutide stays good are practical questions that affect the reliability of each dose.
For dosing precision, the semaglutide dosage in units and tirzepatide dosage in units guides help translate milligram doses into insulin syringe units. The semaglutide mixing chart and the guide on how much bacteriostatic water to mix with 10mg semaglutide ensure accurate preparation. For specific vial concentrations, the semaglutide 10mg dosage chart and tirzepatide 10mg dosage chart provide ready reference.
Additional dosing resources include the compounded semaglutide dose chart, the compounded semaglutide with B12 dosage chart, the compounded tirzepatide starting dose guide, and the tirzepatide compound dosage chart. For milliliter-based dosing, the semaglutide dosage chart in ml and tirzepatide dosage chart in ml convert units to volume measurements.
Our peptide reconstitution calculator and peptide calculator take the guesswork out of preparation math.
Other medications and interactions affecting your GLP-1 timeline
Many GLP-1 users take other medications or supplements concurrently, and some of these interactions can affect how quickly or effectively the GLP-1 medication works.
Phentermine is one of the most commonly discussed combinations. Whether you can take phentermine and semaglutide together and whether you can take phentermine and tirzepatide together are questions that many patients raise. The comparison between phentermine versus semaglutide and the question of whether phentermine is a GLP-1 clarify how these medications differ in mechanism and timeline.
For women, hormonal interactions add another layer of complexity. Whether semaglutide affects your period and whether tirzepatide affects your period are common concerns that can influence perceived side effect timelines. For those who are nursing, whether you can take GLP-1 while breastfeeding is a critical safety consideration.
Some providers explore microdosing GLP-1 for autoimmune conditions, which follows a completely different dosing and timeline protocol than weight management.
Tools for tracking your GLP-1 timeline
Tracking your progress systematically helps you understand your personal response curve and identify what is working. Several tools can help.
The GLP-1 plotter allows you to visualize your medication levels over time based on your dosing schedule. The GLP-1 companion guide provides a comprehensive framework for tracking weight, measurements, side effects, and dietary changes throughout your journey.
Conversion charts are invaluable for understanding dose relationships. The semaglutide dosage conversion chart in units and tirzepatide dosing conversion chart for weight loss help translate between different measurement systems. For specific provider protocols, the IVIM semaglutide dosing chart provides another reference point.
For those interested in lower-dose approaches, the tirzepatide microdose chart outlines protocols for reduced dosing strategies, and the broader compounded tirzepatide dosage calculator helps with precise dose calculations.
Accurate tracking of your dose, timing, side effects, weight, and dietary patterns creates a personal dataset that makes optimizing your protocol dramatically easier. SeekPeptides provides tracking tools, protocol guidance, and a community of people navigating the same journey, so you do not have to figure it all out alone.
The peptide cost calculator can also help you budget your treatment timeline, especially if cost is a factor in how long you plan to remain on therapy. And for comprehensive fat loss context, our peptides for fat loss page covers the full landscape of peptide options beyond GLP-1 alone.
What to expect if you stop your GLP-1 medication
Understanding the discontinuation timeline is just as important as understanding the onset timeline, because many people will eventually stop or pause their medication.
When you stop a GLP-1 medication, the drug clears your system based on its half-life. For semaglutide, it takes about five weeks for the medication to fully clear after the last dose. Appetite gradually returns during this period. Most people notice increasing hunger within two to three weeks of their last injection.
Weight regain is common and well-documented. Studies show that approximately two-thirds of the weight lost on GLP-1 therapy is regained within one year of discontinuation if no other interventions are in place. This is not a failure of willpower. It reflects the biological reality that the medication was managing a chronic condition, and removing it allows the condition to reassert itself.
Understanding semaglutide withdrawal symptoms helps set expectations for what the discontinuation period feels like and how to manage the transition.
Frequently asked questions
Does GLP-1 work immediately after the first injection?
GLP-1 medications begin working at the molecular level within hours, activating receptors in the brain and gut. However, the starting dose is intentionally low, designed for tolerability rather than therapeutic effect. Most people do not notice meaningful appetite suppression until weeks two through four, with full effects emerging over several months as the dose escalates to therapeutic levels. Understanding whether semaglutide suppresses appetite immediately helps set realistic expectations for those first days.
How long until I lose 10 pounds on a GLP-1 medication?
For most people, losing 10 pounds takes approximately six to twelve weeks, depending on starting weight, the specific medication, dose escalation speed, and adherence to dietary changes. People with higher starting weights may reach 10 pounds sooner due to larger caloric deficits. The semaglutide one month results guide provides realistic expectations for early weight loss milestones.
Can I speed up GLP-1 results?
Yes, within limits. Prioritizing protein intake at 0.7 to 1.0 grams per pound of body weight, staying well hydrated, exercising consistently with an emphasis on resistance training, sleeping seven to nine hours nightly, and managing stress all meaningfully accelerate results. What you cannot speed up is the pharmacokinetics, the medication needs time to reach steady state at each dose regardless of your lifestyle choices.
What if my GLP-1 stops working after a few months?
A perceived loss of effectiveness usually indicates a plateau rather than true medication failure. Metabolic adaptation, dose tolerance, and lifestyle drift are common culprits. The semaglutide plateau guide and the tirzepatide not working anymore guide provide specific strategies for breaking through these stalls.
How long should I stay on a GLP-1 medication?
Most clinical guidance suggests treating obesity as a chronic condition requiring ongoing management. The data shows that discontinuing GLP-1 medications leads to significant weight regain in the majority of patients. The guide on how long to stay on semaglutide for weight loss covers the evidence and considerations for long-term versus defined-duration treatment.
Is tirzepatide faster than semaglutide?
In terms of appetite suppression onset, many patients report that tirzepatide produces noticeable effects slightly faster, likely due to its dual GIP/GLP-1 mechanism. In terms of weight loss at comparable time points, tirzepatide consistently outperforms semaglutide in clinical trials. The SURMOUNT trials showed tirzepatide at 15 mg achieving 15% to 21% weight loss by week 72, compared to semaglutide at 2.4 mg achieving approximately 15% by week 68. For a detailed comparison, the semaglutide versus tirzepatide comparison page provides a complete breakdown.
Do oral GLP-1 medications work as fast as injections?
Oral GLP-1 formulations produce similar onset of appetite suppression, within one to four weeks, but achieve less total weight loss compared to injectable formulations. The primary advantage of oral forms is convenience, not speed. The oral semaglutide guide and oral tirzepatide guide cover the practical differences in detail.
Will my GLP-1 side effects go away?
Most GLP-1 side effects are temporary and diminish as your body adapts. Nausea typically resolves within two months at a stable dose. GI symptoms like constipation and bloating usually improve within the first four to six weeks. Side effects may briefly reappear with dose increases but resolve faster each time. If any side effect persists beyond eight weeks at a stable dose, consult your provider.
External resources
FDA information on semaglutide medications for diabetes and obesity
SURMOUNT-1 tirzepatide trial in the New England Journal of Medicine
For those serious about optimizing their GLP-1 journey, SeekPeptides offers comprehensive protocols, dosing tools, tracking resources, and a community of thousands who have navigated these exact questions. Members access personalized guidance, evidence-based protocol adjustments, and expert support that takes the guesswork out of GLP-1 therapy.
In case I do not see you, good afternoon, good evening, and good night. May your GLP-1 timeline stay on track, your appetite signals stay balanced, and your results stay consistent.