Feb 11, 2026
You have got a 5mg vial of semaglutide sitting in front of you, 2ml of bacteriostatic water in a syringe, and a dosage chart that looks like it was written for someone with a chemistry degree. The numbers do not add up. The units make no sense. And every website you check gives you a slightly different answer.
You are not alone. This specific combination, 5mg of semaglutide reconstituted with 2ml of bacteriostatic water, creates a concentration that does not match the standard charts floating around online. Most guides assume you are using pre-filled pens or different reconstitution volumes. That leaves you doing math at your kitchen table, second-guessing every calculation, and wondering if you are about to inject way too much or barely enough.
The good news is that the math is actually simple once you understand one number: 2.5mg/ml. That is your concentration when you mix 5mg of semaglutide powder with 2ml of bacteriostatic water. Every dosing decision flows from that single figure. From there, converting milligrams to units on an insulin syringe becomes straightforward. No guessing. No ambiguity. Just clean numbers you can trust.
This guide breaks down everything you need for the 5mg/2ml configuration specifically. You will find complete semaglutide 5mg dosage charts, unit-by-unit conversion tables, a week-by-week titration schedule, injection technique guidance, and troubleshooting for common problems. Whether you are starting your first dose or adjusting mid-protocol, every number here applies to your exact setup. SeekPeptides built this resource because getting the concentration wrong is the single most common mistake we see, and it is the one that derails results before they even start.
Understanding the 5mg/2ml concentration
Before you draw a single unit into a syringe, you need to understand exactly what you are working with. When you add 2ml of bacteriostatic water to a 5mg vial of semaglutide, you create a solution with a concentration of 2.5mg per milliliter. This is different from other common configurations. A 5mg vial mixed with 1ml gives you 5mg/ml. The same vial mixed with 3ml gives you approximately 1.67mg/ml. Each concentration changes every number on your dosage chart.
Why does this matter so much?
Because concentration determines how many units you draw on your insulin syringe for each dose. Get the concentration wrong, and you could double your intended dose or take half of what you need. Neither scenario is acceptable when you are working with a GLP-1 receptor agonist that requires careful semaglutide dosing in units for both safety and effectiveness.
The math works like this. You have 5mg of semaglutide dissolved in 2ml of liquid. Divide 5 by 2 and you get 2.5. So every milliliter of your reconstituted solution contains 2.5mg of semaglutide. A standard U-100 insulin syringe holds 1ml and is marked with 100 units. That means each unit on your syringe contains 0.025mg (25 micrograms) of semaglutide.
Write that number down. Tattoo it on your brain. Every calculation in this guide starts from 0.025mg per unit.
How the 5mg/2ml differs from other configurations
You will find semaglutide reconstituted at many different concentrations depending on the source and the volume of water used. Understanding how yours compares helps you avoid accidentally following the wrong chart. A semaglutide 5mg/ml dosage chart uses completely different unit counts than yours because that concentration is twice as strong.
Vial Size | Water Added | Concentration | Units per 0.25mg |
|---|---|---|---|
5mg | 2ml | 2.5mg/ml | 10 units |
5mg | 1ml | 5mg/ml | 5 units |
5mg | 3ml | 1.67mg/ml | 15 units |
10mg | 2ml | 5mg/ml | 5 units |
10mg | 3ml | 3.33mg/ml | 7.5 units |
Notice how the same 0.25mg dose requires different unit counts depending on your concentration. This is exactly why using the wrong chart is dangerous. If you are reconstituting 5mg in 2ml and accidentally follow a chart designed for 5mg in 1ml, you would draw half the units you actually need. If you follow a chart for a more dilute solution, you could overdose. Always verify your concentration before drawing any dose. The peptide reconstitution calculator can help you double-check your numbers.
Why 2ml is a popular reconstitution volume
There are practical reasons people choose 2ml as their reconstitution volume for a 5mg vial. The resulting 2.5mg/ml concentration creates unit counts that are easy to read on standard insulin syringes. Doses fall on clean numbers rather than awkward fractions. A 0.25mg starting dose equals exactly 10 units. A 0.5mg dose equals exactly 20 units. No splitting hairs between syringe markings.
The 2ml volume also provides enough liquid to work with comfortably. Too little water and the solution becomes extremely concentrated, making tiny measurement errors more impactful. Too much water and you burn through syringe volume quickly, especially at higher doses. Two milliliters hits the sweet spot for the 5mg vial.
Researchers who want to explore different semaglutide mixing approaches sometimes experiment with alternative volumes, but 2ml remains the most practical for this vial size. If you are working with a larger vial, check the semaglutide mixing chart for 10mg vials instead.
Complete semaglutide 5mg/2ml dosage chart
This is the chart you came for. Every number below assumes you have reconstituted 5mg of semaglutide with exactly 2ml of bacteriostatic water, giving you a 2.5mg/ml concentration. Use a U-100 insulin syringe for all measurements.
Dose (mg) | Dose (mcg) | Volume (ml) | Units on U-100 Syringe |
|---|---|---|---|
0.125 | 125 | 0.05 | 5 |
0.25 | 250 | 0.10 | 10 |
0.375 | 375 | 0.15 | 15 |
0.5 | 500 | 0.20 | 20 |
0.625 | 625 | 0.25 | 25 |
0.75 | 750 | 0.30 | 30 |
0.875 | 875 | 0.35 | 35 |
1.0 | 1000 | 0.40 | 40 |
1.25 | 1250 | 0.50 | 50 |
1.5 | 1500 | 0.60 | 60 |
1.7 | 1700 | 0.68 | 68 |
2.0 | 2000 | 0.80 | 80 |
2.4 | 2400 | 0.96 | 96 |
2.5 | 2500 | 1.00 | 100 |
A few things stand out from this chart. The maximum dose of 2.4mg (the highest FDA-approved weekly dose for weight management) requires 96 units, which is nearly a full syringe. And the entire vial contains exactly 5mg, meaning a single vial at the lowest starting dose of 0.25mg per week lasts 20 weeks. At the highest dose of 2.4mg per week, one vial lasts just over 2 weeks.
Understanding how many doses your vial provides at each level helps you plan ahead. Many researchers find the peptide cost calculator useful for budgeting their protocols.
Quick reference: common starting doses
Most protocols begin at either 0.125mg or 0.25mg per week. Here is a quick reference for those critical first doses that eliminates any confusion about your semaglutide dosage conversion in units.
Starting Dose | Units to Draw | Syringe Marking | Doses per Vial |
|---|---|---|---|
0.125mg (microdose) | 5 units | 5 on U-100 | 40 doses |
0.25mg (standard start) | 10 units | 10 on U-100 | 20 doses |
0.5mg (first escalation) | 20 units | 20 on U-100 | 10 doses |
At the standard starting dose of 0.25mg weekly, your 5mg vial will last nearly 5 months. That is significant value and one reason this particular vial size and reconstitution volume combination is popular among researchers working with compounded semaglutide dosing protocols.
Step-by-step reconstitution process
Getting the reconstitution right is non-negotiable. If you make a mistake here, every dose you draw afterward will be wrong. Take your time. Follow each step exactly.
What you need
Gather everything before you start. You do not want to pause mid-process to hunt for supplies. The complete reconstitution guide covers general principles, but here is what you need specifically for the 5mg/2ml setup.
1 vial of lyophilized semaglutide (5mg)
1 vial of bacteriostatic water
1 sterile syringe with needle (3ml or 5ml for drawing water)
Alcohol swabs
U-100 insulin syringes (29-31 gauge, 0.5ml or 1ml) for dosing
Sharps container
The reconstitution steps
Step one. Clean the rubber stoppers on both the semaglutide vial and the bacteriostatic water vial with alcohol swabs. Let them air dry for 10 seconds. Do not blow on them. Do not wipe them.
Step two. Draw exactly 2ml of bacteriostatic water into your larger syringe. Be precise here. Every fraction of a milliliter matters because it changes your final concentration. Understanding how bacteriostatic water volume affects peptide concentration is fundamental to accurate dosing.
Step three. Insert the needle through the rubber stopper of the semaglutide vial. Angle the needle so it points at the glass wall of the vial, not directly at the powder. This is critical.
Step four. Slowly depress the plunger to release the water down the inside wall of the vial. Do not spray it directly onto the powder. Do not push it in quickly. A slow, steady stream down the wall prevents foaming and preserves the peptide structure. This is the same principle used when mixing any peptide with bacteriostatic water.
Step five. Remove the syringe. Gently swirl the vial with a slow circular motion. Do not shake it. Shaking creates bubbles and can damage the peptide chains. Swirl for 30 to 60 seconds until the powder is fully dissolved. The solution should be clear and colorless. If you see particles or cloudiness, continue swirling gently.
Step six. Label the vial with today's date and the concentration: 2.5mg/ml. Store it in the refrigerator at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit). Use within 28 days.
That is it. Six steps. No complicated equipment. No special skills. Just precision and patience. Proper peptide storage after reconstitution is just as important as the mixing itself.
Common reconstitution mistakes
Three mistakes show up over and over again. The first is spraying water directly onto the powder. This creates foam, traps air bubbles in the solution, and can damage the peptide. Always direct the stream at the vial wall.
The second is shaking the vial. The instinct makes sense. You want to mix it quickly. But semaglutide molecules are fragile. Aggressive agitation breaks peptide bonds and reduces potency. Gentle swirling accomplishes the same mixing without the damage.
The third is using the wrong volume of water. Adding 1.5ml instead of 2ml changes your concentration from 2.5mg/ml to 3.33mg/ml. That means every unit on your syringe now contains 33% more semaglutide than your chart says. At higher doses, that kind of error creates real problems. Always measure your water volume precisely and consider using the free peptide reconstitution calculator to verify your math before injecting.
Week-by-week titration schedule
Semaglutide requires gradual dose escalation. You do not start at your target dose and ride it out. The titration process gives your body time to adjust, minimizes side effects (especially nausea), and helps you find the dose that works best for your specific goals. This schedule follows established clinical protocols adapted for the 5mg/2ml (2.5mg/ml) concentration.
Standard titration protocol
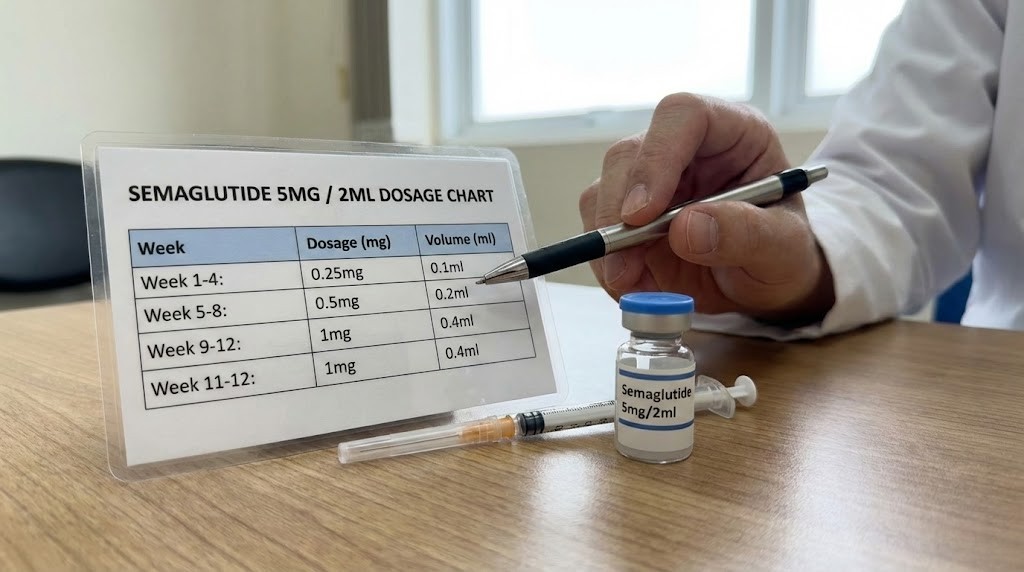
Weeks | Weekly Dose | Units to Draw | Volume (ml) | Purpose |
|---|---|---|---|---|
1-4 | 0.25mg | 10 units | 0.10 | Initiation, GI adjustment |
5-8 | 0.5mg | 20 units | 0.20 | Building tolerance |
9-12 | 1.0mg | 40 units | 0.40 | Therapeutic range entry |
13-16 | 1.7mg | 68 units | 0.68 | Enhanced effect |
17+ | 2.4mg | 96 units | 0.96 | Maximum therapeutic dose |
Each phase lasts a minimum of four weeks. Some researchers stay at a given dose longer if they experience significant side effects or if the current dose is producing satisfactory results. There is no rule that says you must reach the maximum dose. Many people find their sweet spot at 1.0mg or 1.7mg per week. The semaglutide results timeline varies considerably between individuals.
One vial of 5mg semaglutide reconstituted with 2ml of water will last you through the first 10 weeks of this protocol if you follow the standard schedule. Here is the breakdown.
Weeks 1 through 4: 0.25mg per week for 4 weeks = 1.0mg used
Weeks 5 through 8: 0.5mg per week for 4 weeks = 2.0mg used
Weeks 9 and 10: 1.0mg per week for 2 weeks = 2.0mg used
Total: 5.0mg (one full vial)
So you will need your second vial starting around week 9 or 10, depending on how closely you follow the schedule. Planning ahead ensures you do not have gaps in your protocol. Understanding how long semaglutide protocols typically last helps with long-term planning.
Conservative titration protocol (slower escalation)
Some people are more sensitive to GLP-1 receptor agonists. If you have a history of GI sensitivity, are starting at a lower body weight, or simply prefer a cautious approach, this slower schedule reduces the chance of significant nausea and other digestive issues.
Weeks | Weekly Dose | Units to Draw | Volume (ml) |
|---|---|---|---|
1-4 | 0.125mg | 5 units | 0.05 |
5-8 | 0.25mg | 10 units | 0.10 |
9-12 | 0.375mg | 15 units | 0.15 |
13-16 | 0.5mg | 20 units | 0.20 |
17-20 | 0.75mg | 30 units | 0.30 |
21-24 | 1.0mg | 40 units | 0.40 |
25-28 | 1.5mg | 60 units | 0.60 |
29+ | 2.0-2.4mg | 80-96 units | 0.80-0.96 |
This protocol takes nearly twice as long to reach therapeutic doses, but the trade-off is significantly fewer side effects along the way. Many experienced researchers prefer this approach because it allows more precise assessment of how each dose level affects appetite, energy, and body composition. The conservative approach aligns with how semaglutide works over time to gradually shift metabolic patterns.
How to read your insulin syringe for this concentration
Insulin syringes can be confusing if you have never used one before. The markings seem arbitrary. The numbers do not correspond to milligrams. And different syringe sizes have different graduation marks. This section eliminates the confusion for your specific 2.5mg/ml concentration.
Understanding U-100 syringes
A U-100 insulin syringe is designed for insulin dosed at 100 units per milliliter. You are not using insulin, but the syringe works the same way. It divides 1ml into 100 equal units. Each unit equals 0.01ml of liquid. Since your semaglutide concentration is 2.5mg/ml, each unit contains 0.025mg (or 25mcg) of semaglutide.
Common syringe sizes you will encounter include 0.3ml (30 units), 0.5ml (50 units), and 1.0ml (100 units). For the lower doses in your titration schedule (0.25mg to 0.5mg), a 0.3ml or 0.5ml syringe offers better precision because the graduation marks are spaced further apart and easier to read. For higher doses above 0.5mg, you will need a 0.5ml or 1.0ml syringe. Checking the semaglutide syringe dosage conversion chart can help with choosing the right syringe size.
Syringe markings for each dose tier
Here is exactly where to draw to for each dose level at the 2.5mg/ml concentration.
0.25mg dose = 10 units. On a 0.3ml syringe, draw to the first major marking after the 5-unit line. On a 0.5ml syringe, this is the second small marking from the bottom. On a 1.0ml syringe, this is the first major marking.
0.5mg dose = 20 units. On a 0.3ml syringe, draw to the 20-unit line. On a 0.5ml or 1.0ml syringe, find the 20-unit marking.
1.0mg dose = 40 units. On a 0.5ml syringe, draw to the 40-unit line, which is near the top. On a 1.0ml syringe, this is slightly below the halfway mark. Do not attempt this dose with a 0.3ml syringe.
1.7mg dose = 68 units. This falls between the 65 and 70-unit markings on a 1.0ml syringe. Be as precise as you can, aiming for the third small graduation mark above 65. Always use a 1.0ml syringe for this dose.
2.4mg dose = 96 units. Nearly a full 1.0ml syringe. Draw to just below the 100-unit mark, leaving roughly one small graduation of space. Only a 1.0ml syringe can accommodate this dose. For those working with unit-to-mg conversions for semaglutide, understanding your specific concentration is everything.
Tips for accurate drawing
Hold the syringe at eye level when reading the measurement. Looking from above or below creates parallax error. Read at the bottom of the meniscus (the curved surface of the liquid). Pull the plunger back slightly past your target mark, then push forward slowly to the exact line. This eliminates air bubbles and gives you more precise control.
If you see air bubbles in the syringe after drawing, flick the barrel gently with your finger to move bubbles to the top. Then push the plunger up just enough to expel the air without losing liquid. Re-check your volume at the target line. These same principles apply whether you are measuring semaglutide or working with any peptide dosage calculation.
Injection technique and site rotation
Knowing how much to inject is only half the equation. Where and how you inject matters for absorption, comfort, and long-term site health. Proper technique ensures consistent drug delivery and minimizes injection site reactions. This applies whether you are using semaglutide or any other injectable peptide.
Recommended injection sites
Semaglutide is administered subcutaneously, meaning the needle goes into the fat layer just beneath the skin. Three areas work well.
Abdomen. The most popular choice. Use the area at least two inches away from your belly button in any direction. Avoid the belt line and any areas with scars, moles, or skin irritation. The abdomen offers consistent absorption and is easy to reach. Many researchers find it the most comfortable site for subcutaneous peptide injections.
Front of the thigh. Use the middle third of the front of your thigh. Avoid the inner thigh and the area near your knee. The thigh provides a good fat layer for most people, though absorption may be slightly slower than the abdomen.
Back of the upper arm. This site works well but can be difficult to reach without help. If you have someone who can assist, the outer back area of the upper arm provides good results.
Site rotation protocol
Never inject in the same spot twice in a row. Repeated injections in one location can cause lipohypertrophy (lumpy fat deposits) or lipoatrophy (tissue loss), both of which affect absorption and create cosmetic concerns.
A simple rotation system works best. Use the abdomen for week one. Switch to the right thigh for week two. Move to the left thigh for week three. Return to the abdomen for week four, but use a different spot within the abdominal area. Some researchers divide the abdomen into four quadrants (upper right, upper left, lower right, lower left) and rotate through all six sites on a six-week cycle.
Keep a simple log. Write down the date and injection location after each dose. Over time, this prevents accidentally overusing one site. Consistent rotation is a basic principle covered in most peptide beginner guides.
Step-by-step injection process
Step one. Wash your hands thoroughly with soap and water.
Step two. Clean the injection site with an alcohol swab using a circular motion, starting from the center and moving outward. Let it air dry completely.
Step three. Draw your dose into the insulin syringe as described in the syringe reading section above. Remove any air bubbles.
Step four. Pinch a fold of skin at the injection site with your non-dominant hand. This lifts the subcutaneous fat away from the muscle layer beneath.
Step five. Insert the needle at a 90-degree angle (straight in) if using a short needle (4mm to 6mm). Use a 45-degree angle for longer needles (8mm or more). The goal is to place the medication in the fat layer, not the muscle.
Step six. Release the skin pinch. Slowly depress the plunger to inject the full dose. Take 5 to 10 seconds for larger doses to reduce discomfort.
Step seven. Hold the needle in place for 5 to 10 seconds after the plunger is fully depressed. This prevents medication from leaking back out.
Step eight. Withdraw the needle straight out. Do not rub the injection site. A small amount of bleeding is normal and nothing to worry about.
Step nine. Dispose of the used syringe in a sharps container immediately. Never recap needles.
How long your 5mg vial lasts at each dose
Budget planning matters. Knowing exactly how many weeks of coverage each vial provides helps you order refills on time and avoid protocol interruptions. Here is a complete breakdown for the 5mg/2ml reconstitution.
Weekly Dose | mg per Week | Doses per Vial | Weeks of Coverage |
|---|---|---|---|
0.125mg | 0.125 | 40 | 40 weeks |
0.25mg | 0.25 | 20 | 20 weeks |
0.5mg | 0.5 | 10 | 10 weeks |
1.0mg | 1.0 | 5 | 5 weeks |
1.7mg | 1.7 | 2.9 | ~3 weeks |
2.4mg | 2.4 | 2.08 | ~2 weeks |
The economics shift dramatically as you increase your dose. At the starting dose, one vial could theoretically last nearly five months. At the maximum dose, you need a new vial every two weeks. Remember that reconstituted semaglutide should be used within 28 days, so at lower doses you may need to discard unused portions before the vial is empty. Understanding how long compounded semaglutide lasts in the fridge helps prevent waste.
This creates an important planning consideration. If you are at the 0.25mg dose, you will use only 1mg of the 5mg vial in four weeks (the recommended refrigerated shelf life). The remaining 4mg goes to waste unless you can use it within the 28-day window. Some researchers solve this by using smaller vial sizes at lower doses and switching to the 5mg vial once their weekly dose increases past 0.5mg.
Others share vials with a partner or family member who is also on a semaglutide protocol. Just make sure each person uses their own syringe and never shares needles. The cost of peptides is a real factor in protocol planning.
Managing side effects during dose escalation
Side effects are the number one reason people abandon their semaglutide protocol early. Most of these effects are predictable, manageable, and temporary. Knowing what to expect and how to respond keeps you on track during the critical dose escalation phase.
Common side effects by frequency
Clinical data from the STEP trials provides clear numbers on what to expect. Nausea affects approximately 44% of people at the 2.4mg dose, making it the most common side effect by far. But it is important to note that nausea tends to peak during dose increases and subside within 1 to 2 weeks at each new dose level.
The full breakdown from clinical trials shows that gastrointestinal effects dominate the side effect profile. Nausea occurs most often, followed by diarrhea, vomiting, and constipation. Less common effects include headache, fatigue, and dizziness. Serious side effects are rare but include pancreatitis and gallbladder problems.
Understanding semaglutide-related symptoms helps you distinguish between normal adjustment effects and signals that require medical attention.
Nausea management strategies
Nausea is almost always worse during the first two weeks at a new dose. Here is what works.
Eat smaller, more frequent meals. Five or six small meals spread throughout the day instead of three large ones. This keeps your stomach from becoming either too empty or too full, both of which trigger nausea with semaglutide.
Avoid high-fat and fried foods. Fat slows gastric emptying, and semaglutide already slows it significantly. Combining the two creates a double delay that makes nausea much worse. Stick to lean proteins, vegetables, and complex carbohydrates during the adjustment period.
Stay hydrated. Sip water throughout the day. Dehydration worsens nausea and other GI symptoms. Aim for at least 64 ounces per day, more if you are active or in a warm climate.
Ginger is your ally. Ginger tea, ginger chews, and ginger supplements have well-documented anti-nausea properties. Keep some on hand during each dose escalation phase. It is a simple, natural intervention that genuinely helps.
Timing matters. Many people find that injecting in the evening rather than the morning reduces nausea because the initial peak effect occurs while they sleep. Experiment with injection timing to find what works best for you.
Stay upright after eating. Do not lie down for at least 30 minutes after a meal. Gravity helps keep food moving in the right direction when your stomach is emptying more slowly than usual.
When to slow down your titration
Not everyone needs to follow the four-week escalation schedule rigidly. If you experience persistent nausea, vomiting, or diarrhea that does not improve after two weeks at a new dose, consider these options.
Stay at your current dose for an additional two to four weeks before attempting the next increase. Drop back to the previous dose for one to two weeks, then try the increase again. Split the increase in half by using an intermediate dose (for example, 0.375mg between 0.25mg and 0.5mg, which is easily achievable with your 2.5mg/ml concentration at 15 units).
The flexibility of the 5mg/2ml setup is one of its advantages. Because each unit equals 0.025mg, you can make very fine adjustments that pre-filled pens do not allow. This granularity lets you create custom titration schedules that match your tolerance perfectly. Many common peptide mistakes come from escalating too quickly when a slower approach would produce better long-term results.
Comparing 5mg/2ml to other semaglutide configurations
Your 5mg/2ml setup is one of several options. Understanding how it compares helps you make informed decisions if you ever need to switch configurations or if you are helping someone else set up their protocol. The general semaglutide 5mg dosage chart covers other water volumes for this vial size.
Configuration | Concentration | Units for 0.25mg | Units for 1.0mg | Precision | Ease of Use |
|---|---|---|---|---|---|
5mg/2ml | 2.5mg/ml | 10 units | 40 units | High | Excellent |
5mg/1ml | 5mg/ml | 5 units | 20 units | Moderate | Good |
5mg/3ml | 1.67mg/ml | 15 units | 60 units | High | Good |
10mg/2ml | 5mg/ml | 5 units | 20 units | Moderate | Good |
10mg/3ml | 3.33mg/ml | 7.5 units | 30 units | Moderate | Good |
The 5mg/2ml configuration scores well on both precision and ease of use. Doses fall on clean unit markings, making measurement simple. The concentration is moderate, meaning small drawing errors have less impact than with higher concentrations like 5mg/ml. And the overall syringe volume needed for most doses fits comfortably in standard insulin syringes.
The main limitation appears at the highest doses. A 2.4mg dose requires 96 units, which is nearly a full 1.0ml syringe. Some people find drawing this volume challenging. In that situation, a higher concentration (like 5mg/ml) that requires only 48 units for the same dose might be more practical. If you are working with a 10mg vial, check the 10mg vial dosage chart and the 10mg mixing chart for those specific numbers.
When to consider switching configurations
Several scenarios might prompt you to change your reconstitution volume or vial size.
If you reach the maximum dose and find drawing 96 units uncomfortable or imprecise, switching to a 10mg vial with 2ml of water (5mg/ml concentration) cuts your drawing volume in half while maintaining the same dose.
If you are on a low dose for an extended period and wasting medication due to the 28-day expiration of reconstituted solution, consider a smaller vial or a more concentrated solution that uses less volume per dose.
If you are transitioning from semaglutide to tirzepatide, you will need an entirely different dosage chart because the medications have different potencies and dosing schedules. The semaglutide versus tirzepatide comparison covers the differences in depth.
Storage and stability after reconstitution
Your reconstituted semaglutide is a fragile solution. Proper storage preserves potency. Improper storage degrades it, sometimes invisibly, giving you full-volume injections with reduced or zero effectiveness.
Temperature requirements
Store reconstituted semaglutide at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit). This means the main compartment of your refrigerator, not the door (which fluctuates in temperature with opening and closing) and not the back wall (where items can freeze). The middle shelf is ideal.
Never freeze reconstituted semaglutide. Freezing creates ice crystals that physically damage the peptide structure. Thawed semaglutide may appear clear and normal but can have significantly reduced potency. If your vial freezes accidentally, discard it. The peptide storage after reconstitution guide covers optimal conditions in detail.
Brief temperature excursions (leaving the vial on the counter for a few minutes while drawing a dose) are fine. Extended exposure to room temperature degrades the peptide. Try to minimize the time your vial spends outside the refrigerator. Pull it out, draw your dose, and put it back. Understanding peptide expiration and stability helps you make informed decisions about when to discard a vial.
Light protection
Semaglutide is sensitive to light, particularly UV light. Store your vial in its original box or wrap it in aluminum foil if the box is not available. A dedicated small box in the refrigerator works well for keeping all your peptide supplies organized and protected.
The 28-day rule
Once reconstituted, semaglutide should be used within 28 days. After that point, bacterial growth (despite the bacteriostatic water) and natural peptide degradation reduce both safety and effectiveness. Write the reconstitution date and the discard date on the vial label. Some researchers also set a phone reminder for day 25 to ensure they plan their last doses accordingly.
At the 0.25mg weekly dose, you use only 1mg in 28 days, leaving 4mg unused. At the 1.0mg weekly dose, you use 4mg in 28 days, with only 1mg wasted. At the 2.4mg dose, you exhaust the vial before the 28 days are up. Planning your purchases around your current dose level prevents unnecessary waste and saves money. The peptide refrigerator shelf life guide provides more detail on maximizing vial life.
What to expect at each dose level
Knowing what happens at each stage of the titration helps you set realistic expectations and recognize both progress and potential problems. The effects of semaglutide build gradually, and each dose increase introduces new dynamics. This section draws from clinical trial data and the real-world experiences of thousands of researchers.
At 0.25mg per week (10 units)
This is the initiation dose. Most people notice subtle appetite changes within the first few days. Food cravings may diminish slightly. You might feel satisfied with smaller portions at meals without consciously trying to eat less. Some people notice nothing at all during this phase.
Weight loss at this dose is typically minimal, perhaps 1 to 3 pounds over the four-week period. The purpose is not aggressive weight loss but rather allowing your GI system to adjust to the medication. Do not be discouraged by slow initial results. The real changes come at higher doses.
Side effects at 0.25mg are generally mild. Some people experience mild nausea for the first two to three days after injection. Others report slight constipation or a feeling of fullness that is unfamiliar. These effects usually resolve within a week. If you are concerned about any symptoms, reviewing the comprehensive peptide safety guide provides useful context.
At 0.5mg per week (20 units)
Appetite suppression becomes more noticeable. Most people report a significant reduction in hunger between meals. Cravings for high-calorie foods often decrease. Portion sizes naturally shrink without deliberate restriction.
Weight loss typically accelerates to 1 to 2 pounds per week. Over the four-week period at this dose, a loss of 4 to 8 pounds is common. Some people see more dramatic results, especially those with higher starting weights.
Nausea may return when you first increase from 0.25mg to 0.5mg. It follows the same pattern as before. Worst in the first three to five days, then gradually improving. The nausea management strategies from earlier in this guide become particularly important during this phase.
At 1.0mg per week (40 units)
This is where most people enter what researchers call the therapeutic range. Appetite suppression is strong. Many people describe forgetting to eat or needing conscious reminders to have meals. The concept of food noise, that constant background mental chatter about eating, often goes quiet.
Weight loss at 1.0mg typically runs 2 to 3 pounds per week. Cumulative loss by this point often reaches 10 to 15 pounds from baseline. Body composition changes become visible. Clothes fit differently. Energy levels often improve as excess weight decreases.
Some people plateau at this dose and never need to increase further. If your goals are moderate weight loss or improved metabolic markers, 1.0mg may be your maintenance dose. The troubleshooting guide for semaglutide plateaus covers what to do if results stall.
At 1.7mg per week (68 units)
Enhanced appetite suppression compared to 1.0mg. Most people eating at this level have dramatically reduced caloric intake without feeling deprived. The body begins utilizing stored fat more aggressively as the GLP-1 receptor activation intensifies.
Weight loss continues at approximately 2 to 4 pounds per week for many individuals. Some people experience their most dramatic results at this dose level. Others find that the incremental improvement over 1.0mg is modest.
Side effects may re-emerge when transitioning from 1.0mg to 1.7mg. GI symptoms are the most common. Follow the management strategies outlined above and give your body two to three weeks to adjust before assessing whether the dose is tolerable.
At 2.4mg per week (96 units)
The maximum studied dose for weight management. Appetite suppression reaches its peak. Clinical trials showed an average body weight reduction of approximately 15% from baseline over 68 weeks at this dose.
Not everyone needs or tolerates this dose. If you are achieving your goals at a lower level, there is no benefit to escalating further. Higher doses carry higher rates of side effects without proportionally greater weight loss for all individuals.
At 96 units per injection, you are drawing nearly a full syringe. Precision becomes more challenging at this volume. Take extra care with your measurement and consider whether a higher-concentration solution might be more practical for long-term use at this dose. SeekPeptides members access detailed protocols and guidance for optimizing their research at every dose level.
Semaglutide with B12 and other combinations
Some compounded semaglutide formulations include additional ingredients, most commonly vitamin B12 (cyanocobalamin). This combination addresses a practical concern: GLP-1 receptor agonists can reduce appetite to the point where nutritional intake drops below optimal levels. B12 supplementation helps maintain energy levels and supports metabolic function during aggressive caloric reduction.
How B12 affects your dosage chart
If your 5mg vial contains only semaglutide and you reconstitute with 2ml of bacteriostatic water, the charts in this guide apply exactly. However, if you are using a compounded formulation that already includes B12 or other ingredients, the total volume and concentration may differ. Always check the label of your specific product. The semaglutide with B12 dosage chart covers those specific formulations.
For researchers who add B12 separately, the small volume of a B12 injection does not significantly change the semaglutide concentration if they are administered separately. Do not mix B12 into your reconstituted semaglutide vial unless the formulation specifically calls for it. The complete semaglutide with B12 guide covers the nuances of this combination in detail.
If you are using a pre-mixed compounded formulation like those documented in the compounded semaglutide with B12 dosage chart, the concentration on your label supersedes everything in this guide. Always dose according to the concentration stated on your specific product.
Other common additions
Some compounding pharmacies include L-carnitine, lipo-B complexes, or other ingredients in their semaglutide formulations. Each addition potentially changes the concentration, volume, and dosing calculations. This guide specifically covers plain semaglutide 5mg reconstituted with 2ml of bacteriostatic water. If your product contains additional ingredients, consult the compounding pharmacy for a dosage chart specific to your formulation. Understanding the broader landscape of peptides for weight loss can help you evaluate different options.
Troubleshooting common dosing problems
Even with a clear chart and careful technique, problems arise. Here are the most common issues researchers encounter with the 5mg/2ml setup and how to resolve them.
Air bubbles in the syringe
Small air bubbles are the most frequent complaint. They look alarming but are generally harmless in subcutaneous injections. However, they do reduce the volume of medication you actually inject, effectively lowering your dose.
To eliminate them, draw your dose, then hold the syringe with the needle pointing up. Flick the barrel gently with your fingernail until all bubbles rise to the top. Push the plunger up slowly until the bubbles are expelled and a tiny drop of liquid appears at the needle tip. Re-check that your dose volume is correct.
If bubbles keep forming, the problem is usually either cold solution (let the vial warm for 2 to 3 minutes on the counter before drawing) or inserting the needle too aggressively into the vial stopper (which pushes air into the vial). Gentle technique prevents both issues.
Difficulty drawing small volumes
At the 0.125mg dose (5 units), you are working with a tiny amount of liquid. Standard 1.0ml syringes have graduation marks spaced far apart, making 5 units hard to see and measure precisely.
The solution is to use a 0.3ml (30-unit) insulin syringe for low doses. These syringes have larger markings for the same number of units, making small volumes much easier to read. Some researchers prefer 0.5ml (50-unit) syringes as a compromise between visibility and range. This is one of many beginner mistakes that is easily avoided with the right equipment.
Cloudy or discolored solution
A properly reconstituted semaglutide solution should be clear and colorless. If you see cloudiness, particles, or discoloration, do not use it. These signs indicate contamination, improper storage, or peptide degradation.
Possible causes include using non-sterile water, contaminating the vial during reconstitution (touching the needle or stopper with bare fingers), storing at incorrect temperatures, or the vial exceeding its 28-day shelf life. Discard the vial and start fresh with a new one. The cost of wasted medication is far less than the risk of injecting a compromised solution. Understanding how long reconstituted peptides last helps prevent this situation.
Injection site reactions
Redness, swelling, or itching at the injection site occurs occasionally. These reactions are usually mild and resolve within 24 to 48 hours. Ice applied for 5 to 10 minutes after injection can reduce local inflammation. Rotating injection sites (as described earlier) minimizes recurrence.
If injection site reactions are severe, persistent, or spreading, consult a healthcare professional. Allergic reactions to semaglutide are rare but possible. A thorough understanding of peptide safety and risk management helps you distinguish between normal reactions and warning signs.
Missing a dose
If you forget your weekly injection, take it as soon as you remember if there are at least two days before your next scheduled dose. If there are fewer than two days until your next dose, skip the missed dose and resume your regular schedule. Do not double up on doses to compensate. Two doses within 48 hours can cause significant GI distress.
To prevent missed doses, set a recurring weekly alarm on your phone. Pick a consistent day and time. Many people choose Sunday evenings, associating the injection with the start of a new week. Consistency in timing helps maintain steady drug levels.
Tracking your progress
Data drives decisions. Without tracking, you are guessing at whether your protocol is working, whether dose adjustments are needed, and whether side effects are improving or worsening over time.
What to track weekly
Weight is the obvious metric, but it is not the only one that matters. Body composition changes, measurements, and subjective indicators provide a more complete picture of how your semaglutide protocol is performing.
Body weight. Weigh yourself at the same time each week, ideally first thing in the morning after using the bathroom and before eating. Weight fluctuates by 2 to 4 pounds daily due to water, food, and hormonal cycles. Consistent timing reduces noise in the data.
Waist circumference. Measure at the narrowest point of your waist or at the level of your navel. Use the same reference point each time. Waist measurements often change before the scale does, especially in the early weeks.
Appetite rating. On a scale of 1 to 10, rate your hunger level throughout the day. This subjective score helps you identify patterns and assess whether dose increases are producing meaningful appetite suppression beyond what the previous dose achieved.
Side effects. Log any nausea, GI issues, headaches, or other effects. Note severity (mild, moderate, severe) and duration. This log becomes invaluable when deciding whether to escalate, maintain, or reduce your dose.
Energy and mood. Brief daily notes on energy levels and general mood capture improvements that the scale misses. Many people report improved energy and mental clarity within weeks of starting semaglutide, often before significant weight loss occurs.
When to adjust your dose
Use your tracking data to make informed decisions about dose changes. If you are losing 1 to 2 pounds per week with minimal side effects, your current dose is likely appropriate. If weight loss has stalled for three or more weeks despite consistent adherence, consider the next dose escalation.
If side effects are severe and not improving after two to three weeks, consider dropping back to a lower dose. If appetite is fully controlled and weight loss is on track, there is no reason to increase just because the schedule says to.
The tracking approach is similar to what SeekPeptides recommends across all peptide protocols. Data-driven adjustments produce better outcomes than rigid schedule adherence. The comprehensive peptide dosing guide covers these principles in broader context.
Understanding semaglutide mechanism and weight loss
Knowing how semaglutide actually works gives you a deeper appreciation for why the dosage chart matters, why titration is necessary, and why individual responses vary so dramatically.
GLP-1 receptor activation
Semaglutide is a GLP-1 receptor agonist. GLP-1 stands for glucagon-like peptide-1, a hormone your body naturally produces in the gut after eating. This hormone signals your brain to feel full, slows stomach emptying, and improves insulin sensitivity. Semaglutide mimics this natural hormone, but with modifications that make it last much longer in the body.
Natural GLP-1 has a half-life of about 2 minutes. Your body breaks it down almost immediately. Semaglutide has been engineered to resist this breakdown. Its half-life is approximately 7 days, which is why you only need one injection per week. Each injection creates a sustained elevation of GLP-1 receptor activity that persists until your next dose. Understanding the general mechanisms of how peptides work provides helpful background here.
Three pathways to weight loss
Semaglutide produces weight loss through three complementary mechanisms.
Appetite suppression. The primary driver. By activating GLP-1 receptors in the hypothalamus, semaglutide reduces hunger signals and increases satiety. Most people eating less is not a conscious choice. They simply feel full sooner and think about food less often.
Delayed gastric emptying. Semaglutide slows the rate at which food leaves your stomach. This extends the feeling of fullness after meals and reduces the desire to snack between meals. It also explains why high-fat foods cause more nausea on semaglutide. Fat already delays gastric emptying, and adding semaglutide on top creates excessive delay.
Improved insulin sensitivity. By improving how your body processes glucose, semaglutide reduces insulin spikes after meals. Lower insulin levels facilitate fat burning and reduce the storage of new fat. This metabolic shift contributes to weight loss beyond the direct caloric reduction from eating less.
These mechanisms work together and build with increasing doses, which is why the titration schedule exists. Starting at the full dose would overwhelm all three systems simultaneously, causing severe nausea and GI distress. Gradual escalation allows your body to adapt to each level of receptor activation before increasing further. The best peptides for weight loss resource covers how semaglutide compares to other options in this category.
Why individual responses vary
Not everyone loses the same amount of weight at the same dose. Several factors explain the variation.
Genetics influence how many GLP-1 receptors you have, how sensitive they are, and how your body metabolizes the drug. Body composition matters because people with more excess weight tend to lose a higher percentage of body weight initially. Lifestyle factors like diet quality, exercise, sleep, and stress all modulate the response. Even injection site and technique can slightly affect absorption rates.
This variability is exactly why tracking your personal response matters more than following a generic chart rigidly. Your optimal dose is the one that produces meaningful results with tolerable side effects for your body. Exploring the complete guide to peptides for fat loss gives you context for how semaglutide fits into the broader landscape of metabolic optimization.
Transitioning between protocols
Life changes. Goals change. Sometimes you need to switch from one semaglutide protocol to another, from semaglutide to a different medication, or from compounded to pharmaceutical-grade products. Each transition requires careful planning to avoid disruption.
Switching vial sizes
If you switch from a 5mg vial to a 10mg vial (or vice versa) while keeping the same water volume, your concentration changes. This means every unit count on your dosage chart changes too. The semaglutide reconstitution chart provides numbers for multiple vial sizes.
Before drawing your first dose from a new vial, recalculate your concentration. Write the new concentration on the vial label. Cross-reference with the appropriate chart. Drawing the wrong number of units because you forgot to account for a concentration change is a common and potentially serious error. The semaglutide dosage calculator eliminates the guesswork by doing the math for you.
Switching from pre-filled pens to vials
Pre-filled pens like Ozempic and Wegovy deliver precise, predetermined doses. Switching to reconstituted vials introduces the variable of manual measurement. The actual semaglutide dose should remain the same. What changes is how you measure it.
If you were on 1.0mg per week via a pre-filled pen and switch to a 5mg/2ml reconstituted vial, you draw 40 units. The dose is identical. The delivery method is different. Give yourself a week or two to become comfortable with the manual drawing process before making any dose changes.
Transitioning to tirzepatide
Some researchers switch from semaglutide to tirzepatide for various reasons, including plateus, side effects, or a desire for the dual GIP/GLP-1 mechanism. This is not a simple 1:1 dose conversion because the two medications have different potencies and dosing scales.
The semaglutide to tirzepatide dose conversion chart provides specific guidance. Generally, researchers starting tirzepatide after semaglutide begin at the standard tirzepatide starting dose (2.5mg per week) regardless of their semaglutide dose. The tirzepatide versus semaglutide dosage chart offers side-by-side comparisons.
Do not switch directly from a high dose of semaglutide to a high dose of tirzepatide. The mechanisms are different, the receptor profiles are different, and your body needs time to adjust. Even experienced researchers follow the conservative tirzepatide dosing guide when transitioning between medications.
Diet and lifestyle optimization on semaglutide
Semaglutide is powerful, but it is not magic. The medication works best when combined with intentional dietary choices and consistent physical activity. Ignoring these factors limits your results and can create nutritional deficiencies as your appetite decreases.
Protein prioritization
This is the single most important dietary adjustment on semaglutide. When you eat less food overall (which you will), you must ensure adequate protein intake to prevent muscle loss. Research consistently shows that weight loss without sufficient protein disproportionately reduces lean muscle mass, which lowers your metabolic rate and makes long-term weight maintenance harder.
Aim for a minimum of 0.7 grams of protein per pound of body weight daily. For a 200-pound person, that is 140 grams of protein per day. This target does not change as your caloric intake drops. If anything, it becomes more important at lower calorie levels.
High-quality protein sources include chicken breast, fish, lean beef, eggs, Greek yogurt, cottage cheese, and protein supplements. Plan meals around protein first, then add vegetables and complex carbohydrates. This approach ensures you hit your protein target even on days when appetite is extremely low.
Hydration strategy
Semaglutide-related nausea, reduced food intake, and increased metabolic activity all increase the risk of dehydration. Drink at least 64 to 80 ounces of water daily. More if you exercise or live in a warm climate.
Signs of dehydration on semaglutide include headache, fatigue, dizziness, and concentrated urine. These symptoms overlap with medication side effects, making it easy to blame semaglutide when the real culprit is insufficient water intake. Stay ahead of hydration rather than trying to catch up after symptoms appear.
Exercise considerations
Regular physical activity amplifies the weight loss effects of semaglutide and, critically, helps preserve lean muscle mass during weight loss. A combination of resistance training (2 to 3 sessions per week) and moderate cardiovascular exercise (150 minutes per week) produces optimal body composition outcomes.
Start conservatively if you are not currently active. Semaglutide can reduce energy in the first few weeks of each dose increase as your body adjusts. Low-intensity walking is perfectly fine during titration phases. Increase exercise intensity gradually as you stabilize at each dose level. The peptides for weight loss and muscle gain guide covers how to optimize body composition during peptide protocols.
Nutrient supplementation
Reduced food intake means reduced micronutrient intake. A quality multivitamin covers the basics. Beyond that, pay special attention to several key nutrients.
Vitamin B12 supports energy metabolism and can become depleted with reduced dietary intake. This is one reason compounded semaglutide with B12 is popular. Vitamin D is important for bone health and immune function, especially if you are losing significant weight. Magnesium supports muscle function and sleep quality, both of which can be affected during weight loss. Omega-3 fatty acids provide anti-inflammatory support and help maintain healthy cell membranes.
These recommendations apply broadly to anyone eating in a significant caloric deficit, whether from semaglutide-induced appetite suppression or intentional dieting. For researchers interested in additional support, the best peptides for energy and energy and focus optimization guide cover complementary approaches.
Safety considerations and contraindications
Semaglutide is a potent medication with a generally favorable safety profile when used correctly. However, certain conditions and circumstances require extra caution or are absolute contraindications.
Who should not use semaglutide
People with a personal or family history of medullary thyroid carcinoma (MTC) should not use semaglutide. Animal studies showed increased thyroid tumor incidence at clinically relevant exposures, and while human risk is uncertain, the contraindication exists as a precaution.
People with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) should avoid semaglutide due to the associated thyroid cancer risk.
Semaglutide is not recommended during pregnancy or while breastfeeding. If you are planning to become pregnant, discontinue semaglutide at least two months before conception to allow the drug to clear your system. For women navigating hormonal changes, the peptides for menopause weight loss guide discusses alternative and complementary approaches.
Interactions with other medications
Semaglutide slows gastric emptying, which can affect the absorption of oral medications taken at the same time. If you take oral medications (particularly those with narrow therapeutic windows like warfarin, levothyroxine, or oral contraceptives), discuss timing with your healthcare provider.
Combining semaglutide with other diabetes medications, particularly insulin or sulfonylureas, increases the risk of hypoglycemia (dangerously low blood sugar). Dose adjustments of those medications are typically needed.
Using semaglutide alongside other GLP-1 receptor agonists is not recommended. Do not stack semaglutide with tirzepatide, liraglutide, or other drugs in the same class. If you are considering switching between these medications, use the conversion charts and transition properly rather than overlapping.
Warning signs that require medical attention
Seek immediate medical attention if you experience severe, persistent abdominal pain (potential pancreatitis), vision changes (potential diabetic retinopathy progression), signs of allergic reaction (swelling, difficulty breathing, severe rash), or signs of hypoglycemia (confusion, trembling, sweating, rapid heartbeat) if you are also taking diabetes medications.
Monitor for gallbladder symptoms including upper right abdominal pain, especially after meals, nausea with fever, or yellowing of the skin. Rapid weight loss is a known risk factor for gallstones, and semaglutide-associated weight loss is no exception. Understanding the complete safety profile of peptide-based medications helps you make informed decisions about your protocol.
Frequently asked questions
Can I use a different volume of water with a 5mg vial?
Yes. You can reconstitute with 1ml (giving 5mg/ml) or 3ml (giving approximately 1.67mg/ml) or other volumes. However, the dosage charts in this guide ONLY apply to the 2ml reconstitution (2.5mg/ml concentration). If you use a different volume, you need a different chart. The semaglutide 5mg mixing chart covers alternative volumes.
How do I know if my semaglutide has gone bad?
Clear and colorless solution indicates a good product. Cloudiness, particles, discoloration, or an unusual odor means the vial should be discarded. Also discard any vial that has been reconstituted for more than 28 days, has been frozen, or has been left at room temperature for extended periods. More details in the expired semaglutide guide.
What if I accidentally inject too much?
Contact a healthcare provider immediately. Overdose symptoms typically include severe nausea, vomiting, and potential hypoglycemia. Do not attempt to "compensate" by skipping your next dose. Medical guidance is essential for managing an overdose situation safely.
Can I travel with reconstituted semaglutide?
Yes, but it must remain refrigerated. Use an insulated travel case with ice packs for transport. At your destination, store it in a refrigerator immediately. Avoid checking it in luggage on flights where the cargo hold may freeze. Carry a prescription or letter from your provider to avoid issues at security checkpoints.
Is the 5mg/2ml concentration suitable for microdosing?
Yes. The 2.5mg/ml concentration allows microdoses as low as 0.025mg (1 unit). However, accuracy at single-unit measurements is challenging with standard syringes. For consistent microdosing, consider reconstituting with a larger volume of water (3ml or 4ml) to increase the volume per dose and improve measurement precision. The peptide calculator can help you determine the optimal reconstitution volume for your target dose.
How does the 5mg/2ml chart differ from a pre-mixed 2.5mg/ml compounded solution?
Functionally, they are the same concentration and the dosage chart applies to both. The difference is that pre-mixed compounded solutions arrive ready to use, while a lyophilized vial requires reconstitution. Some compounded solutions include additional ingredients (B12, L-carnitine) that do not change the semaglutide concentration but may affect the total volume. Always verify the semaglutide concentration on your product label and check the pharmacy-specific dosage charts if available.
What is the best injection day and time?
Choose any day that works for your schedule and stick with it consistently. The best time of day varies by individual. Evening injections may reduce nausea because the initial peak effect occurs during sleep. Morning injections work well for people who do not experience significant nausea. The most important factor is consistency, not the specific day or time chosen.
Should I split my weekly dose into two injections?
Standard protocol is one injection per week. Some researchers experiment with splitting the dose (for example, 0.5mg twice per week instead of 1.0mg once) to reduce peak-related side effects. While there is limited clinical data on this approach, anecdotal reports suggest it can help people who experience severe nausea at peak drug levels. Discuss this approach with your healthcare provider before implementing it.
External resources
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, personalized protocol builders, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night.