Feb 28, 2026
Everything you have read about semaglutide and kidney stones is probably half right. That is the frustrating part. Some sources insist this medication will wreck your kidneys. Others wave the concern away entirely, telling you there is nothing to worry about. The truth sits somewhere between those extremes, and it matters more than either camp wants to admit.
Here is what the clinical data actually shows. Large randomized trials have not identified kidney stones as a direct side effect of semaglutide. The FDA prescribing information does not list nephrolithiasis as an adverse event. But that does not make this a closed case. Not even close.
The real risk comes from a side door. The gastrointestinal effects that nearly every semaglutide user experiences, the nausea, the vomiting, the diarrhea, can drain fluid from your body faster than most people realize. And dehydration is one of the most well-established risk factors for kidney stone formation in all of medicine. So while semaglutide does not directly build stones inside your kidneys, it can quietly create the conditions where stones become far more likely to form.
This guide breaks down every piece of evidence connecting semaglutide to kidney stone risk. You will learn exactly how stones form, why GLP-1 side effects change the equation, what the FLOW trial revealed about semaglutide and kidney health, and the specific prevention strategies that keep your kidneys safe throughout treatment. Whether you are just starting your first week on semaglutide or managing side effects months into your protocol, this is the comprehensive reference you need.
What the clinical evidence says about semaglutide and kidney stones
Start with the hard data. It paints a more nuanced picture than either side of the debate acknowledges.
The major semaglutide clinical trials, including SUSTAIN, PIONEER, and STEP, enrolled thousands of participants across multiple years of follow-up. None of these trials identified kidney stones as a statistically significant adverse event. That is not nothing. When you track thousands of patients taking a medication for years and do not see a spike in stone formation, it carries real weight.
But here is where it gets interesting. A retrospective study examining GLP-1 receptor agonist users found that longer duration on semaglutide and higher comorbidity burden correlated with kidney stone development. Patients with a history of diabetes and elevated serum creatinine showed higher stone incidence while on the medication. These correlations do not prove causation, but they highlight that patient-specific factors change the risk calculation dramatically.
Then there is the research that flips the narrative entirely. Studies published in the Journal of Urology and Kidney360 found that semaglutide was associated with a decreased risk of stone growth compared to other GLP-1 receptor agonists. Patients on semaglutide showed a slight decrease in urinary calcium excretion, a factor that could theoretically reduce calcium oxalate stone formation. A study examining 24-hour urine chemistry in patients on GLP-1 based therapy found significant increases in urine citrate and reductions in uric acid stone formation, suggesting a lithoprotective effect independent of weight or diabetes control.
The FDA position on kidney complications
The FDA prescribing information for semaglutide does include a kidney-related warning. But it is about acute kidney injury, not stones.
Postmarketing reports have documented cases where patients experienced rapid worsening of kidney function after starting semaglutide. In the FDA adverse event database from January 2022 to September 2025, acute kidney injury appeared in roughly 1.07% of semaglutide cases. Nearly all of these cases, around 95%, occurred in patients who already had renal risk factors. The pattern is consistent. Severe gastrointestinal symptoms cause volume depletion, which stresses the kidneys.
The distinction matters. Semaglutide side effects do not build stones the way some medications do. They do not alter urinary mineral composition in a way that promotes crystal formation. Instead, the medication creates conditions, specifically dehydration from GI distress, that allow the normal stone-forming process to accelerate. Understanding that difference changes your entire prevention strategy.
Research that suggests kidney protection
The FLOW trial, published in the New England Journal of Medicine, provided landmark data on semaglutide and kidney outcomes. This randomized controlled trial enrolled 3,533 participants with type 2 diabetes and chronic kidney disease. The results were striking enough that the trial was stopped early at a prespecified interim analysis.
Semaglutide reduced the risk of major kidney disease events by 24% compared to placebo, with a hazard ratio of 0.76. The mean annual decline in kidney filtration rate was 1.16 mL per minute per 1.73 m2 slower in the semaglutide group. Cardiovascular death risk dropped by 29%. These are not marginal improvements. For patients with kidney disease, semaglutide appears to slow the disease trajectory meaningfully.
A separate analysis from Mass General Brigham found a consistent, independent association between GLP-1 agonist use and reduced kidney stone risk, regardless of prior stone history. The mechanism likely involves weight reduction, improved metabolic parameters, and favorable changes in urinary chemistry.
So the research presents a paradox. Semaglutide may protect kidneys at the cellular and disease-progression level while simultaneously creating dehydration risk that can trigger stones. Both things can be true at the same time.
How kidney stones actually form
Before diving into how semaglutide interacts with stone formation, you need to understand the process itself. Kidney stones are not random. They follow predictable biochemistry.
Your kidneys filter roughly 200 liters of blood every day. They remove waste products, excess minerals, and toxins, concentrating them into about 1 to 2 liters of urine. That urine contains dissolved substances including calcium, oxalate, phosphate, and uric acid. Under normal conditions, these substances stay dissolved. But when concentrations get too high, or when the urine lacks enough natural inhibitors, crystals begin to form.
Small crystals. Tiny. Most of the time your body flushes them out before you notice anything. But under the right conditions, those crystals attach to one another. They accumulate. They grow into a small mass, a stone, that can block the flow of urine and cause extraordinary pain.
The four main types of kidney stones
Not all kidney stones are created equal. The type matters because it dictates your prevention strategy, your dietary approach, and how aggressively you need to manage hydration on semaglutide.
Calcium oxalate stones account for approximately 80% of all kidney stones. They form when calcium and oxalate, a compound found in many foods, combine in the urine. High concentrations of either substance increase risk. Paradoxically, eating adequate dietary calcium actually reduces calcium oxalate stone risk because calcium binds oxalate in the gut before it reaches the kidneys.
Uric acid stones make up about 9% of cases. They form when urine becomes too acidic, with a pH below 5.5. People with gout, those eating high-purine diets, and anyone experiencing chronic dehydration face elevated risk. This stone type is particularly relevant for semaglutide users because dehydration concentrates uric acid and lowers urine pH simultaneously.
Struvite stones account for roughly 10% and typically form in response to urinary tract infections. They can grow quickly and become quite large. These are less relevant to the semaglutide discussion but worth knowing about.
Cystine stones are rare, about 1% of cases, and result from a genetic condition called cystinuria that causes the kidneys to excrete too much of a specific amino acid.
The concentration equation
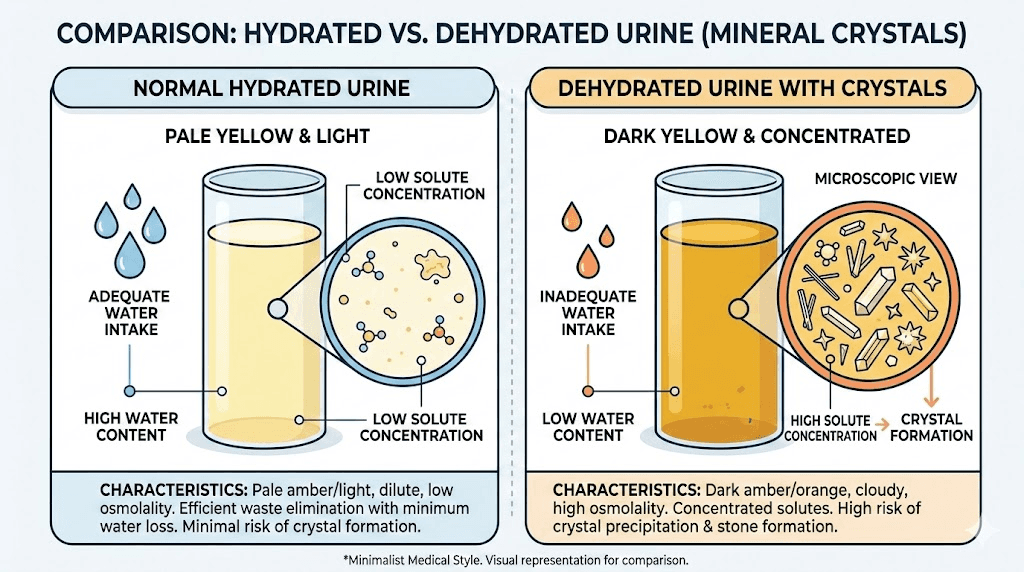
Here is the critical concept. Kidney stones are fundamentally about concentration.
Imagine dissolving sugar in water. A spoonful dissolves easily in a full glass. But try dissolving that same spoonful in a tablespoon of water and you get a saturated mess. Crystals form because there is not enough liquid to keep the solute dissolved.
Your kidneys work the same way. When urine volume drops, the concentration of stone-forming substances rises. Calcium, oxalate, uric acid, phosphate, all of them become more concentrated in a smaller volume of urine. At some threshold, the solution becomes supersaturated. Crystals nucleate. Stones begin.
This is exactly why dehydration, from any cause, dramatically increases kidney stone risk. And this is exactly why semaglutide users who experience significant GI side effects face a real concern, even though the medication itself does not directly promote stone formation.
The dehydration connection: how semaglutide side effects create stone risk
This is the mechanism that matters most. Not some obscure pharmacological pathway. Simple fluid loss.
Semaglutide gastrointestinal side effects are among the most common reasons people struggle with the medication. In clinical trials, nausea affected 20 to 44% of participants depending on the dose. Vomiting occurred in 5 to 24%. Diarrhea hit 8 to 30%. These are not rare events. They are the expected experience for a significant portion of users, especially during the first weeks of treatment and after dose escalations.
Each episode of vomiting or diarrhea pulls fluid from your body. Not just water. Electrolytes too. Sodium, potassium, bicarbonate. The body loses all of these when GI distress strikes. And here is the part most guides skip over: many people on semaglutide also experience significant appetite suppression that makes drinking adequate fluids harder. When you feel nauseated, the last thing you want to do is force down water. So people drink less at the exact moment their bodies are losing more.
The math becomes brutal. You are losing fluid through GI symptoms. You are taking in less fluid because of appetite suppression and nausea. Your urine becomes concentrated. The substances that form stones, calcium, oxalate, uric acid, reach higher concentrations. Crystals form more readily. And if this pattern repeats day after day, week after week, the risk compounds.
The rapid weight loss factor
There is another angle that receives almost no attention. Rapid weight loss itself is a known risk factor for kidney stone formation.
When the body breaks down fat tissue quickly, it releases purines and other metabolic byproducts. Purine metabolism produces uric acid. More uric acid in the bloodstream means more uric acid filtered through the kidneys and concentrated in urine. Studies on bariatric surgery patients have documented significantly elevated kidney stone rates in the months following rapid weight loss, even when hydration appears adequate.
Semaglutide can produce substantial weight loss. Clinical trials document reductions of 10 to 15% of body weight at higher doses. While this weight loss is generally gradual and spread over months, individual responses vary. Some people lose weight quickly, especially early in treatment when appetite suppression is most dramatic and dietary intake drops sharply. Those individuals face a compounded risk from both dehydration and the metabolic consequences of rapid weight reduction.
Medications that compound the risk
Certain medications taken alongside semaglutide increase kidney stone risk further. This is a critical consideration that many prescribers overlook.
Topiramate (Topamax), sometimes prescribed for migraine prevention or weight loss, increases kidney stone risk by promoting urinary calcium excretion and raising urine pH. Combining it with semaglutide, where dehydration risk is already elevated, creates a concerning overlap.
Acetazolamide, a carbonic anhydrase inhibitor used for altitude sickness and certain eye conditions, alkalinizes urine in ways that promote calcium phosphate stones.
High-dose vitamin C supplements, exceeding 1,000 mg daily, convert to oxalate in the body and increase urinary oxalate excretion. If you are already on semaglutide and taking supplements, this is worth reviewing with your provider.
Certain diuretics (loop diuretics in particular) increase calcium excretion and reduce urine volume, both of which promote stones. Thiazide diuretics, interestingly, have the opposite effect and are sometimes prescribed specifically to prevent calcium stones.
Who faces the highest risk
Not every semaglutide user faces equal kidney stone risk. Some people can take this medication for years without any renal concerns. Others carry risk factors that demand vigilant prevention from day one.
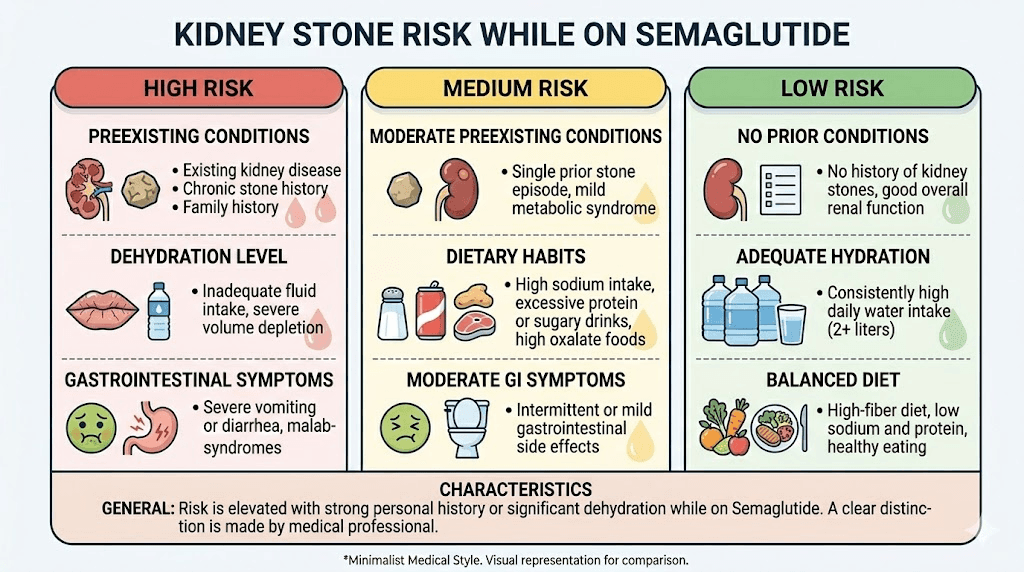
High-risk categories
If you fall into any of these categories, your prevention strategy needs to be aggressive, not casual.
Personal or family history of kidney stones. This is the single biggest predictor. If you have passed a stone before, your recurrence risk is approximately 50% within 5 to 10 years without intervention. Adding semaglutide, with its dehydration potential, to that baseline risk demands proactive management. If first-degree relatives have a stone history, your own risk is elevated even if you have never had one yourself.
Chronic dehydration or low baseline fluid intake. Many people arrive at semaglutide already under-hydrated. They drink coffee, maybe some soda, and not nearly enough water. Starting a medication that can cause nausea, vomiting, and diarrhea on top of already-low fluid intake puts them at immediate risk.
Type 2 diabetes. The FLOW trial population was specifically patients with diabetes and CKD. Research shows that a history of diabetes and elevated serum creatinine correlate with stone incidence in semaglutide users. Diabetic patients on semaglutide need kidney function monitored regularly.
Metabolic conditions. Hyperparathyroidism, gout, and inflammatory bowel disease all alter urinary chemistry in ways that promote stone formation. Gout is particularly relevant because it directly increases uric acid levels, and semaglutide-related dehydration concentrates that uric acid further.
Chronic kidney disease. Patients with reduced kidney function have less reserve capacity to handle dehydration episodes. Even brief periods of volume depletion can cause disproportionate harm.
Lower-risk profiles
You face lower risk if you have no personal or family history of stones, maintain good baseline hydration, tolerate semaglutide with minimal GI symptoms, and have normal kidney function. But lower risk does not mean no risk. The prevention strategies outlined later in this guide apply to everyone.
Semaglutide dosing and kidney stone risk: does the dose matter
Higher doses of semaglutide cause more GI side effects. That connection is well established across every clinical trial. And more GI side effects mean more dehydration risk. So yes, dose matters.
At starting doses of 0.25 mg weekly, GI symptoms tend to be mild and manageable for most people. Nausea might last a day or two. Vomiting is uncommon. Fluid losses are minimal. But as the dose escalates to 0.5 mg, 1.0 mg, 1.7 mg, and eventually 2.4 mg weekly, the intensity and duration of GI symptoms increase substantially.
This is why the standard semaglutide dosing protocol uses gradual escalation over 16 to 20 weeks. The slow ramp gives your GI system time to adapt. When people skip steps, jump doses, or escalate too quickly, GI symptoms hit harder and last longer. Those are the periods of greatest dehydration risk and, by extension, greatest stone risk.
The compounded semaglutide variable
Compounded semaglutide adds another layer of complexity. Compounded formulations may contain additional ingredients like vitamin B12, glycine, or L-carnitine. These additions generally do not affect kidney stone risk directly. However, the accuracy of dosing in compounded preparations can vary between pharmacies, and inconsistent dosing may lead to unexpected spikes in GI symptoms if a particular batch is more concentrated than expected.
If you are using compounded semaglutide, the reconstitution process becomes particularly important. Incorrect dilution ratios mean incorrect doses, which can mean unexpected GI distress and unexpected fluid loss. Use the semaglutide dosage calculator to verify your calculations before every injection.
Timing and injection considerations
When you take semaglutide can influence GI symptom severity. Some users report fewer side effects when injecting in the morning versus evening, or vice versa. Finding the best time of day to take semaglutide that minimizes your personal GI response reduces dehydration risk indirectly.
Similarly, injection site selection can influence absorption rate and GI impact. While the evidence on site-specific absorption differences is limited, some users report better tolerance with abdominal versus thigh injections, or vice versa. The point is not that one site is universally better. The point is that optimizing your personal protocol to minimize GI distress has downstream kidney benefits.
Acute kidney injury versus kidney stones: understanding the difference
These are two distinct kidney problems that get conflated constantly in the semaglutide discussion. Understanding the difference is critical for knowing when you face an emergency versus a manageable risk.
Acute kidney injury
Acute kidney injury, or AKI, is a rapid decline in kidney function that develops over hours to days. It is the condition the FDA specifically warns about in semaglutide prescribing information. AKI from semaglutide almost always stems from severe dehydration caused by intense, prolonged GI symptoms.
In the FDA adverse event database, AKI appeared in roughly 1.07% of semaglutide cases. But context matters. Nearly all cases occurred in patients with pre-existing renal risk factors, such as concurrent use of nephrotoxic medications, hypertension, heart failure, or baseline kidney impairment. In otherwise healthy patients with normal kidneys, semaglutide-related AKI is rare.
Warning signs of AKI include sudden decrease in urine output, swelling in the legs or ankles, persistent fatigue, confusion, and nausea that does not resolve. This is a medical emergency requiring immediate attention.
Kidney stones
Kidney stones develop over weeks to months, not hours. They form gradually as mineral deposits accumulate in the kidney. Symptoms appear when a stone moves from the kidney into the ureter, the narrow tube connecting kidney to bladder. The classic presentation includes severe flank pain that radiates to the groin, blood in the urine, nausea and vomiting (which can worsen dehydration in a vicious cycle), and urgent or frequent urination.
Most small stones pass on their own with adequate hydration and pain management. Larger stones may require medical intervention including shock wave lithotripsy, ureteroscopy, or surgical removal.
The key difference for semaglutide users: AKI is an acute emergency caused by rapid fluid loss. Kidney stones are a chronic risk from sustained dehydration patterns. Both demand prevention through hydration, but AKI requires immediate medical care while stone prevention is an ongoing daily practice.
Prevention strategies that actually work
This is the section that matters most. Research debates aside, there are concrete actions that dramatically reduce your kidney stone risk while on semaglutide. Every single one of them is evidence-based.
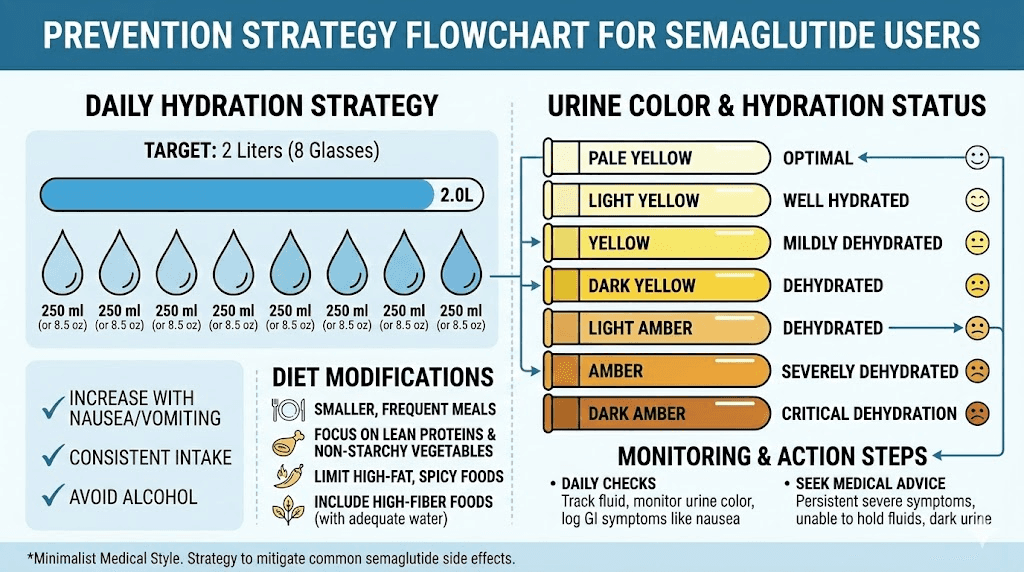
Hydration: the single most important factor
Fluid intake is not a suggestion. It is the cornerstone of kidney stone prevention, and it becomes non-negotiable when taking a medication that can cause dehydration.
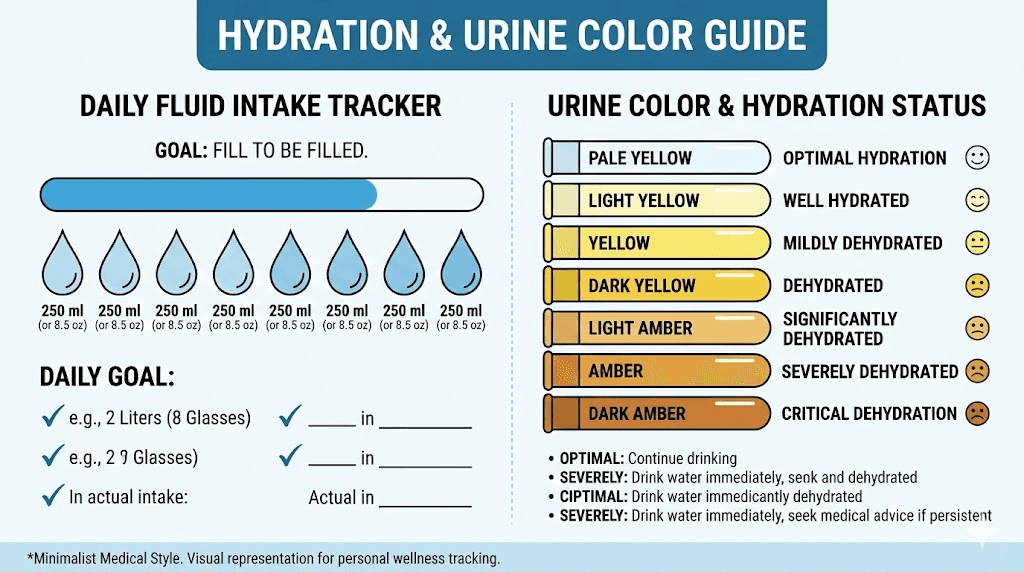
The target is clear. Drink enough fluid to produce at least 2.5 liters of urine daily. For most people, that means consuming roughly 3 to 3.5 liters of fluid throughout the day. The specific number varies based on body size, activity level, climate, and how much fluid you are losing through GI symptoms.
How to know if you are hydrated enough. Check your urine color. Pale yellow, like light straw, indicates adequate hydration. Dark yellow or amber means you need more fluid immediately. Clear urine is fine but not necessary. The pale yellow sweet spot is your target.
Practical hydration strategies for semaglutide users:
Keep a water bottle with you at all times and set hourly reminders to drink
Take small, frequent sips rather than large volumes at once, especially when nauseated
Add a squeeze of lemon to water for flavor and the added benefit of citrate, a natural stone inhibitor
Count all fluids toward your daily total, including tea, coffee, broth, and water-rich foods
Front-load hydration in the morning when nausea is often less severe
If vomiting or diarrhea is persistent, consider an oral rehydration solution that replaces electrolytes
Track daily fluid intake using an app or simple tally marks until it becomes habit
What about specific beverages? Almost all non-sugary beverages count toward hydration. Coffee and tea in moderate amounts are acceptable despite mild diuretic effects, because the fluid they provide outweighs what they cause you to lose. One exception: avoid sugary drinks, as high sugar intake may increase stone risk through elevated urinary calcium. Also avoid excess grapefruit juice and cranberry juice, both of which are high in oxalate.
Dietary changes that reduce stone risk
What you eat on semaglutide matters for more than just weight loss. Your dietary choices directly influence urinary chemistry and stone formation risk.
Sodium: keep it under 2,300 mg daily. This is roughly one teaspoon of table salt. Excess sodium causes your kidneys to excrete more calcium into the urine. Sodium and calcium share the same transport mechanism in the kidney, so high sodium intake directly increases urinary calcium concentration. Since many semaglutide users eat smaller quantities of food overall, this target may be easier to hit, but pay attention to processed foods and restaurant meals that can spike sodium intake quickly.
Calcium: get 1,000 to 1,200 mg daily from food. This seems counterintuitive if you know calcium oxalate stones are the most common type. But dietary calcium actually prevents stones. When you eat calcium-rich foods with meals, the calcium binds to oxalate in your digestive tract. That oxalate-calcium complex gets excreted through feces instead of being absorbed into the bloodstream and filtered through your kidneys. Less oxalate reaching the kidneys means fewer calcium oxalate crystals forming.
The important distinction: dietary calcium is protective, but calcium supplements taken between meals may increase risk. If you need to supplement, take calcium with food.
Oxalate: manage, do not eliminate. High-oxalate foods include spinach, rhubarb, beets, nuts, chocolate, tea, and sweet potatoes. You do not need to eliminate these entirely. Just eat them alongside calcium-rich foods so the oxalate binds in the gut. If you have a history of calcium oxalate stones, moderation with the highest-oxalate foods (spinach and rhubarb in particular) is reasonable.
Animal protein: moderate intake. High animal protein consumption increases urinary calcium and uric acid while decreasing citrate levels and lowering urine pH. All four of those changes promote stone formation. This is especially relevant for people on semaglutide who prioritize high-protein meals to preserve muscle mass during weight loss. Balancing protein with plant-based foods and adequate hydration helps offset these effects.
Citrate: your natural defense. Citrate inhibits stone formation by binding calcium in the urine and preventing crystal aggregation. Lemon juice is an excellent source. Four fluid ounces of fresh lemon juice diluted in water daily provides meaningful citrate supplementation. Avoid sweetened lemonade, as the sugar counteracts the benefit.
Monitoring your kidney function
If you are in a high-risk category, regular monitoring is not optional.
Baseline labs before starting semaglutide should include a basic metabolic panel with creatinine and estimated GFR, a urinalysis, and ideally a uric acid level. These give you a reference point to compare against as treatment continues.
During treatment, kidney function should be checked if you experience significant or prolonged GI symptoms (more than a few days of vomiting or diarrhea), notice changes in urine output or color, develop flank pain or blood in urine, or are escalating doses.
For known stone formers, a 24-hour urine collection provides the most detailed picture. This test measures exactly how much calcium, oxalate, citrate, uric acid, sodium, and other stone-relevant substances your kidneys are excreting. Metabolic evaluation with targeted treatment based on 24-hour urine results is estimated to reduce stone recurrence by up to 90%. That is an extraordinary risk reduction for a single test.
Managing GI side effects to protect your kidneys
Since the kidney stone risk from semaglutide flows through GI side effects and dehydration, managing those side effects is effectively kidney stone prevention. Here are the strategies that work.
Gradual dose escalation
This is the most important protective measure. The standard semaglutide escalation protocol exists for a reason. Starting at 0.25 mg and increasing by 0.25 mg every four weeks gives your body time to adjust to the GI effects. Jumping doses or escalating too quickly produces worse nausea, more vomiting, and greater dehydration risk.
If you experience significant GI distress at any dose, staying at your current level for additional weeks before escalating is a legitimate strategy. The weight loss benefit of higher doses is meaningless if dehydration sends you to the ER with kidney stones or acute kidney injury.
Eating patterns that reduce nausea
Your eating strategy directly influences GI tolerance and, by extension, kidney health.
Eat smaller, more frequent meals rather than large ones. Large meals stretch the stomach and trigger more nausea with semaglutide. Four to six small meals work better than three large ones.
Avoid high-fat and greasy foods, especially in the first few days after each injection. Fat delays gastric emptying, which semaglutide already slows. The combination produces significantly more nausea.
Cold or room-temperature foods often provoke less nausea than hot foods, which have stronger aromas that can trigger the nausea response.
Ginger tea, ginger chews, or ginger supplements can reduce semaglutide-related nausea. The evidence for ginger as an antiemetic is solid, and unlike pharmaceutical options, it carries no kidney-relevant side effects.
When to contact your healthcare provider
Not all GI symptoms require medical attention. Mild nausea that resolves within a few days of each injection is expected and manageable. But certain situations demand professional evaluation.
Contact your provider if:
Vomiting or diarrhea persists for more than 48 hours
You cannot keep any fluids down for more than 24 hours
Urine output drops noticeably or urine becomes very dark
You develop flank or back pain, especially if it radiates to the groin
You see blood in your urine (pink, red, or brown discoloration)
You experience sudden severe fatigue, confusion, or leg swelling
You have a history of kidney stones and GI symptoms are not resolving
Early intervention prevents the escalation from dehydration to acute kidney injury or stone formation. Do not wait until you are in crisis.
Semaglutide versus other GLP-1 medications: kidney stone risk comparison
If kidney stone risk is a significant concern for you, comparing semaglutide against other weight loss peptides and GLP-1 medications matters.
Semaglutide versus tirzepatide
Tirzepatide (the active ingredient in Mounjaro and Zepbound) is a dual GIP/GLP-1 receptor agonist. It also causes GI side effects, though some studies suggest slightly different GI profiles compared to semaglutide. In the FDA adverse event database, AKI appeared in 0.47% of tirzepatide cases compared to 1.07% for semaglutide. However, these numbers reflect reporting patterns rather than head-to-head trial data, so direct comparison requires caution.
Both medications carry similar dehydration-mediated kidney stone risk. If you switch from one to the other specifically to reduce kidney concerns, the fundamental prevention strategy remains identical: stay hydrated, manage GI symptoms, monitor kidney function.
Semaglutide versus retatrutide
Retatrutide, a triple agonist targeting GIP, GLP-1, and glucagon receptors, is still in clinical trials. Early data suggests potent GI effects similar to or potentially stronger than semaglutide at higher doses. If retatrutide moves to market, kidney stone prevention during treatment will likely follow the same hydration-focused framework.
The broader GLP-1 class picture
The Journal of Urology published research specifically examining kidney stone episodes across different GLP-1 receptor agonist medications. The finding was noteworthy: semaglutide showed a significantly lower risk of stone growth compared to other medications in the class. While the mechanism behind this relative advantage is not fully understood, it may relate to semaglutide-specific effects on urinary calcium excretion or weight loss patterns.
This does not mean semaglutide is kidney-stone-proof. It means that among your GLP-1 options, the evidence does not suggest semaglutide is worse than alternatives, and it may actually be somewhat protective relative to the class.
Long-term kidney health on semaglutide
Some people take semaglutide for months. Others stay on it for years. Long-term use changes the risk calculation in important ways.
GI side effects typically improve over time
Good news first. Most semaglutide users report that GI side effects diminish as their bodies adapt to the medication. The worst nausea and vomiting typically occur in the first 4 to 8 weeks and during dose escalations. By the time most people reach their maintenance dose, the severe GI distress has settled considerably. This means the highest kidney stone risk period is usually early in treatment.
But not everyone adapts equally. Some individuals continue to experience significant GI symptoms months into treatment, especially at higher doses. If you are in that category, long-term hydration vigilance becomes a permanent part of your protocol.
Weight loss benefits for kidney health
Here is the other side of the equation. Obesity itself is a major risk factor for kidney stones. Excess body weight is associated with higher urinary excretion of calcium, oxalate, and uric acid, all stone-promoting substances. Insulin resistance, common in obesity, promotes acidic urine that favors uric acid stone formation.
Successful weight loss on semaglutide can actually reduce long-term kidney stone risk by improving metabolic parameters, normalizing urinary chemistry, reducing insulin resistance, and lowering uric acid levels. The challenge is navigating the short-term dehydration risk during the weight loss phase to reach the long-term kidney benefits of a healthier weight.
The metabolic improvement arc
Semaglutide does more than cause weight loss. It improves insulin sensitivity, reduces inflammation, lowers blood sugar, and favorably modifies lipid profiles. Several of these metabolic improvements have downstream kidney benefits. Reduced inflammation protects nephrons. Improved insulin sensitivity normalizes urine pH. Better glucose control reduces the kidney damage that comes with chronically elevated blood sugar.
For patients who respond well to semaglutide and maintain adequate hydration, the net effect on kidney health may actually be positive over time, especially for those with metabolic syndrome, prediabetes, or type 2 diabetes.
Special populations and unique considerations
Semaglutide users with prior kidney stones
If you have a history of kidney stones, semaglutide is not automatically contraindicated. But it demands a more aggressive prevention approach. Before starting, get a 24-hour urine collection to establish your current stone risk profile. Know your stone type from prior episodes if possible, as this dictates specific dietary adjustments.
During treatment, maintain fluid intake sufficient to produce well over 2.5 liters of urine daily. Err on the side of overhydration rather than under. Consider prophylactic potassium citrate supplementation if your provider recommends it based on urinary chemistry. And have a lower threshold for contacting your provider if GI symptoms become moderate to severe.
Semaglutide users with diabetes
Diabetic patients on semaglutide face a nuanced risk profile. On one hand, the FLOW trial demonstrated clear kidney protection from semaglutide in this population. On the other hand, diabetes itself increases kidney stone risk through altered urinary chemistry, and diabetic patients often take multiple medications that can affect kidney function.
If you have diabetes and are taking semaglutide, regular kidney function monitoring (at minimum, annual eGFR and urinalysis, more frequent if GI symptoms are significant) is essential. Coordinate care between your endocrinologist, primary care provider, and a nephrologist if kidney function shows any decline.
Semaglutide users on other peptides
For researchers using semaglutide alongside other peptides, hydration needs increase further. Peptide stacking can compound fluid requirements. If you are running a stack that includes semaglutide plus other compounds, account for the additive fluid demands of each component.
Use the peptide calculator to verify dosing and the reconstitution calculator to ensure accurate preparation. Incorrect reconstitution leading to unexpected dose spikes is a preventable cause of severe GI symptoms.
The electrolyte factor most guides ignore
Hydration is not just about water volume. The electrolyte composition of your fluids matters enormously for kidney stone prevention, and semaglutide-related GI symptoms deplete electrolytes in specific patterns that affect stone risk.
Potassium and citrate
Vomiting and diarrhea deplete potassium rapidly. Low potassium levels reduce urinary citrate excretion, and citrate is one of the most important natural inhibitors of kidney stone formation. Without adequate citrate, calcium crystals aggregate more freely and stones form more readily.
Foods rich in potassium and citrate include bananas, oranges, lemons, limes, potatoes, and tomatoes. If severe GI symptoms make eating difficult, a potassium citrate supplement (with provider approval) can help maintain protective urinary citrate levels.
Magnesium
Magnesium inhibits calcium oxalate crystal formation in the urine. Chronic diarrhea from semaglutide depletes magnesium stores. Low magnesium levels also worsen nausea, creating a cycle where depletion worsens the very symptom causing the depletion.
Magnesium glycinate or magnesium citrate supplementation can address deficiency while also contributing citrate to the urine. This dual benefit makes it a particularly useful supplement for semaglutide users concerned about kidney stones.
Bicarbonate
Both vomiting and diarrhea can disrupt acid-base balance, though in opposite directions. Severe vomiting tends to cause metabolic alkalosis (overly alkaline blood) while severe diarrhea causes metabolic acidosis (overly acidic blood). Acidic conditions favor uric acid stone formation. Alkaline conditions can promote calcium phosphate stones, though this is less common.
For most semaglutide users, the primary concern is diarrhea-induced acidosis promoting uric acid stones. Maintaining adequate citrate intake helps buffer this effect.
Semaglutide, alcohol, and kidney stone risk
Alcohol and semaglutide is already a complicated topic. Add kidney stone risk to the equation and the calculus becomes even more unfavorable for drinking.
Alcohol is a diuretic. It increases urine output while reducing total body water, effectively concentrating urine. For someone already at risk of dehydration from semaglutide GI effects, adding alcohol creates a compounding dehydration effect. Beyond dehydration, beer and wine contain purines that increase uric acid production. Spirits with sugary mixers add fructose, which increases urinary uric acid excretion.
This does not mean absolute abstinence is required. But if you choose to drink while on semaglutide, match every alcoholic beverage with at least an equal volume of water. Drink slowly. Avoid binge episodes that cause rapid dehydration. And if you have any kidney stone risk factors, consider whether the kidney risk is worth it.
Exercise, sweating, and the hidden dehydration trap
Here is a scenario that catches people off guard. You are on semaglutide. Your GI symptoms are manageable. You are drinking what feels like enough water. Then you add intense exercise to your routine to accelerate weight loss results.
Exercise causes fluid loss through sweat. In hot environments or during intense sessions, sweat losses can exceed 1 to 2 liters per hour. If your baseline hydration is already compromised by mild GI symptoms from semaglutide, adding heavy exercise without compensating fluid intake can tip the balance toward stone-forming concentrations quickly.
The solution is straightforward. Weigh yourself before and after exercise. Every pound lost represents roughly 500 mL of fluid that needs replacing. Drink before, during, and after exercise. Consider electrolyte drinks during prolonged sessions. And on days when GI symptoms are worse, reduce exercise intensity or at minimum increase fluid intake to compensate.
Recognizing kidney stones early
Early detection means smaller stones, easier passage, and less risk of complications. Know what to look for.
The classic symptoms
Pain. The hallmark of a kidney stone is sudden, severe pain in the side or back, below the ribs. This pain often radiates to the lower abdomen and groin as the stone moves through the ureter. It comes in waves as the ureter contracts around the stone, with periods of intense pain followed by relative relief. Many describe it as the worst pain they have ever experienced.
Urinary changes. Blood in the urine (hematuria) appears in most kidney stone cases. The urine may look pink, red, or brown. You might also experience increased urgency, frequency, or pain during urination, especially as the stone approaches the bladder.
Nausea and vomiting. This is where it gets tricky for semaglutide users. Stone-related nausea can be difficult to distinguish from medication-related nausea. If your typical semaglutide nausea pattern suddenly changes in character, intensity, or timing, especially if accompanied by flank pain or urinary changes, consider the possibility of a stone.
Fever and chills. If stone symptoms occur alongside fever, this suggests infection. An infected obstructing stone is a urological emergency requiring immediate care. Do not delay.
Subtle early warning signs
Before a stone becomes symptomatic, you might notice mild, intermittent flank discomfort that you dismiss as muscle soreness or GI-related pain. Urine that consistently appears darker than expected despite what you believe is adequate fluid intake. A vague sense of urinary urgency without clear cause. These subtle signs warrant attention, especially if you have risk factors.
Working with your healthcare team
Prevention is most effective when your healthcare providers understand both your semaglutide use and your kidney stone risk factors. Here is how to optimize that relationship.
Information to share with your prescriber
Tell your semaglutide prescriber about any history of kidney stones, including stone type if known. Inform them about all current medications, especially those that affect kidney function or stone risk. Report the severity and frequency of GI side effects honestly. Many patients downplay nausea or diarrhea because they want to stay on the medication or escalate doses. Your provider cannot help you prevent kidney problems if they do not know the full picture.
Lab work to request
At minimum, ask for basic metabolic panel with creatinine and eGFR at baseline and periodically during treatment. If you have stone risk factors, request uric acid levels and a 24-hour urine collection for stone risk assessment. A urinalysis can detect microscopic blood that might indicate early stone formation before symptoms appear.
When to ask for a nephrology referral
Consider seeing a nephrologist if you have a history of recurrent kidney stones and are starting or already on semaglutide, if kidney function declines during treatment (even mildly), if you have diabetes with any kidney involvement, or if you develop a kidney stone while on semaglutide. Nephrologists can perform targeted metabolic evaluations that identify your specific stone-forming risk factors and design personalized prevention plans.
Comparing semaglutide kidney concerns to other weight loss approaches
For perspective, kidney stone risk is not unique to semaglutide. Many weight loss approaches carry similar or greater risk.
Phentermine, a widely prescribed weight loss medication, can cause dehydration through decreased fluid intake and increased metabolic rate. Topiramate, often combined with phentermine in Qsymia, directly increases kidney stone risk through altered urinary chemistry. The combination of phentermine and topiramate carries a higher stone risk than semaglutide alone.
Bariatric surgery patients face significantly elevated kidney stone rates. Procedures that cause malabsorption (like Roux-en-Y gastric bypass) increase oxalate absorption and urinary oxalate excretion dramatically. Stone rates of 7 to 10% within two years of surgery are documented, substantially higher than anything reported with semaglutide.
Crash diets and very-low-calorie diets cause rapid weight loss, dehydration, and metabolic acidosis, all of which promote stone formation. Paradoxically, some people who resist medication-based weight loss in favor of extreme dieting may face greater kidney stone risk than they would on semaglutide with proper hydration.
Ketogenic diets produce metabolic acidosis and increase urinary uric acid, both of which promote stones. Studies report elevated stone rates in patients on long-term ketogenic diets.
The point is not that semaglutide has zero kidney stone risk. It is that the risk is manageable and likely lower than many alternative weight loss approaches, especially when you follow the prevention strategies outlined in this guide.
Building your personal kidney stone prevention protocol
Generic advice is fine. A personalized protocol is better. Here is how to build yours based on your specific risk profile.
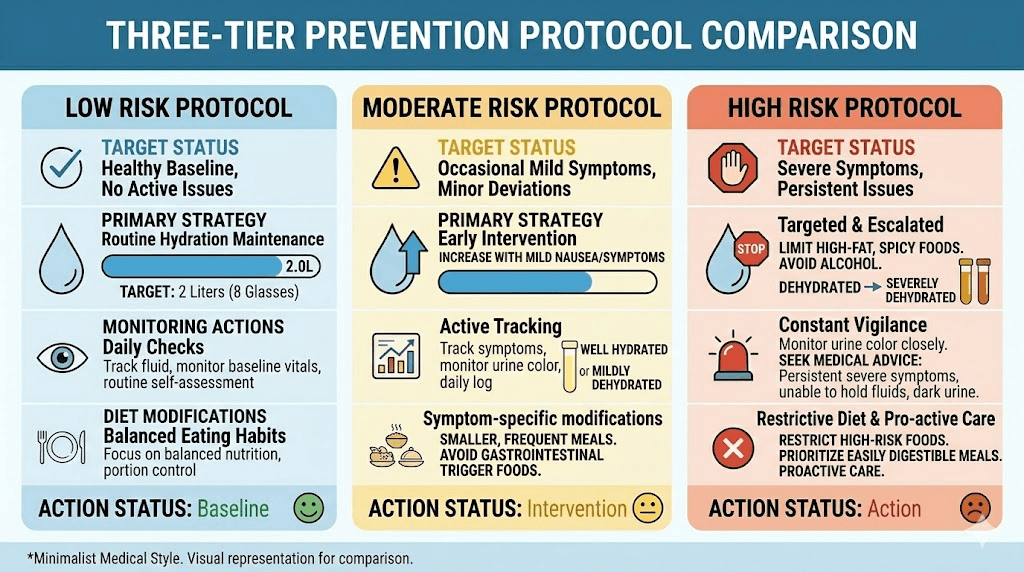
For low-risk semaglutide users
If you have no personal or family stone history, normal kidney function, and tolerate semaglutide well:
Aim for 2.5 to 3 liters of fluid daily
Monitor urine color, keeping it pale yellow
Follow a balanced diet with adequate calcium from food sources
Limit sodium to under 2,300 mg daily
Get baseline kidney labs and repeat annually
Increase fluid intake during dose escalations when GI symptoms may worsen
For moderate-risk semaglutide users
If you have a family history of stones, mild metabolic risk factors, or experience moderate GI symptoms:
Aim for 3 to 3.5 liters of fluid daily
Add daily lemon juice (4 oz fresh lemon juice in water) for citrate
Consider magnesium supplementation (discuss with provider)
Track fluid intake and urine output formally for the first 2 to 3 months
Get kidney labs every 3 to 6 months during active dose escalation
Limit animal protein to moderate portions and increase plant-based foods
Avoid high-dose vitamin C supplements
For high-risk semaglutide users
If you have a personal history of kidney stones, known kidney disease, severe GI symptoms, or multiple metabolic risk factors:
Aim for 3.5+ liters of fluid daily, producing over 2.5 liters of urine
Get a 24-hour urine collection before starting semaglutide and repeat every 6 months
Consider prophylactic potassium citrate (provider-prescribed)
Take magnesium citrate daily (provider-approved)
Get kidney function labs monthly during dose escalation, quarterly at maintenance
Have a low threshold for pausing dose escalation if GI symptoms are significant
Establish care with a nephrologist before starting or early in treatment
Keep an oral rehydration solution available at home for episodes of vomiting or diarrhea
Consider splitting doses or alternative delivery methods if GI tolerance is poor
Frequently asked questions
Does semaglutide directly cause kidney stones?
No. Clinical trials and FDA labeling have not identified kidney stones as a direct side effect of semaglutide. The concern is indirect: GI side effects like nausea and vomiting can cause dehydration, which is a well-established risk factor for stone formation. Maintaining adequate hydration effectively addresses this risk.
Should I stop semaglutide if I have a history of kidney stones?
Not necessarily. A stone history is not a contraindication to semaglutide. However, it does require a more aggressive prevention approach including higher fluid targets, dietary modifications, regular lab monitoring, and possibly a 24-hour urine collection. Discuss your specific situation with your prescriber and consider a nephrology consultation.
How much water should I drink while on semaglutide to prevent kidney stones?
Enough to produce at least 2.5 liters of urine daily, which typically means consuming 3 to 3.5 liters of total fluid. Use urine color as your guide: pale yellow indicates adequate hydration. During episodes of GI distress, increase intake further to compensate for fluid losses.
Can the FLOW trial results reassure me about semaglutide and my kidneys?
The FLOW trial showed semaglutide reduced major kidney disease events by 24% in patients with type 2 diabetes and CKD. This is encouraging for overall kidney health. However, the trial examined kidney disease progression, not kidney stone formation specifically. The stone risk from dehydration remains a separate concern that requires its own prevention measures.
Are kidney stones more likely during dose escalation?
Dose escalation phases carry higher risk because GI side effects tend to be more severe when doses increase. This is when dehydration is most likely. Follow the standard escalation schedule without rushing, increase fluid intake proactively during transitions, and do not hesitate to stay at a dose longer if GI symptoms are not manageable.
Is tirzepatide better than semaglutide for kidney stone risk?
There is no strong evidence that tirzepatide carries lower kidney stone risk than semaglutide. Both medications cause GI side effects that can lead to dehydration. Some data suggests semaglutide may actually have a slight advantage in stone risk compared to other GLP-1 agonists, but this needs further study. The prevention strategy is identical for both medications.
What should I do if I think I am passing a kidney stone while on semaglutide?
Increase fluid intake immediately to help move the stone. Over-the-counter pain management (NSAIDs like ibuprofen are often recommended for stone pain, but verify with your provider as they can affect kidney function). Contact your healthcare provider the same day. If you develop fever, inability to urinate, or uncontrollable pain, go to the emergency department. Consider temporarily holding semaglutide if severe vomiting from the stone event would compound dehydration.
Does compounded semaglutide carry different kidney stone risk than brand-name versions?
Compounded semaglutide carries the same fundamental dehydration-mediated risk as brand-name versions. The primary additional concern with compounded formulations is dosing accuracy. Use the semaglutide dosage calculator and follow precise reconstitution protocols to avoid unexpected dose spikes that could trigger more severe GI symptoms and greater dehydration.
For researchers serious about optimizing their peptide protocols while protecting kidney health, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed safety protocols, interaction databases, and expert guidance that covers every angle of safe peptide research, from reconstitution to long-term health monitoring.
External resources
National Kidney Foundation: Kidney stone diet plan and prevention
NEJM: Effects of semaglutide on chronic kidney disease (FLOW trial)
In case I do not see you, good afternoon, good evening, and good night. May your hydration stay consistent, your kidneys stay clear, and your protocols stay safe.