Feb 28, 2026

Your doctor just prescribed tirzepatide. You are already taking metformin. And now one question keeps circling through your mind, refusing to settle: can these two medications work together safely, or are you about to create a problem that did not exist five minutes ago?
It is a fair concern. Both medications target blood sugar. Both affect the gut. Both come with their own list of potential side effects that could, in theory, stack on top of each other in ways nobody warned you about. The internet offers contradictory answers, forum posts filled with personal anecdotes that may or may not apply to your situation, and clinical jargon that requires a medical degree to decode.
Here is the straightforward answer: yes, metformin and tirzepatide can be taken together. In fact, the largest clinical trials studying tirzepatide, the SURPASS program, specifically enrolled patients who were already taking metformin. The combination is not only safe for most people, it is one of the most studied medication pairings in modern diabetes and weight loss research. But the details matter. Timing matters. How you manage the shared side effects matters. And understanding why these two medications complement each other, rather than compete, could be the difference between a smooth experience and weeks of unnecessary digestive misery.
This guide covers everything: the clinical evidence behind the combination, exactly how each medication works at the cellular level, practical protocols for taking both, strategies for managing overlapping side effects, and the specific situations where your prescriber might adjust one or both medications. Whether you are adding tirzepatide to an existing metformin regimen or considering both from scratch, the research points clearly in one direction. These medications were practically designed to work together.
How metformin and tirzepatide work through different pathways
Understanding why these two medications pair so well starts with understanding how each one works independently. They target blood sugar and body weight through completely separate mechanisms. Think of it like attacking a problem from two different directions simultaneously.
Metformin has been around since the 1950s. It remains the most widely prescribed diabetes medication on the planet, and for good reason. Its primary mechanism involves reducing hepatic glucose production, which means it tells the liver to stop releasing so much stored sugar into the bloodstream. At the molecular level, metformin inhibits mitochondrial complex I in liver cells, which activates an enzyme called AMP-activated protein kinase (AMPK). This enzyme acts as a master energy sensor, and when activated, it shifts the liver from glucose production mode into glucose conservation mode.
But that is only part of what metformin does.
It also improves insulin sensitivity in muscle tissue, helping cells absorb glucose more effectively. It reduces intestinal glucose absorption, meaning less sugar from food enters the bloodstream. And here is something most people do not know: metformin actually increases natural GLP-1 secretion in the gut. Research published in the Journal of Clinical Investigation found that metformin has a direct, AMPK-dependent effect on GLP-1-secreting L cells, boosting the body's own production of the very hormone that tirzepatide mimics.
Now look at tirzepatide. It works through an entirely different door. Tirzepatide is a dual GIP/GLP-1 receptor agonist, meaning it activates two incretin receptors simultaneously. When you inject tirzepatide, it mimics two gut hormones that your body naturally produces after eating. GLP-1 stimulates insulin release when blood sugar is high, slows gastric emptying so food moves through the stomach more gradually, and signals the brain to reduce appetite. GIP (glucose-dependent insulinotropic polypeptide) enhances insulin secretion even further and may help the body burn fat more efficiently.
The result is a one-two punch that no single medication can achieve alone.
Metformin reduces basal hyperglycemia, the elevated fasting blood sugar that occurs between meals, through its liver-focused mechanism. Tirzepatide targets postprandial glucose elevations, the blood sugar spikes that happen after eating, through its incretin-based approach. Metformin works on insulin sensitivity and glucose production. Tirzepatide works on insulin secretion, appetite regulation, and gastric emptying. Together, they cover virtually every pathway involved in blood sugar control and weight management.
What the SURPASS clinical trials tell us about this combination
The strongest evidence for combining metformin and tirzepatide comes from the SURPASS clinical trial program, a series of large, randomized trials that studied tirzepatide across thousands of patients. What makes this evidence particularly relevant is that most participants in these trials were already taking metformin when they started tirzepatide. The combination was not an afterthought. It was the primary study design.
SURPASS-2: the landmark trial
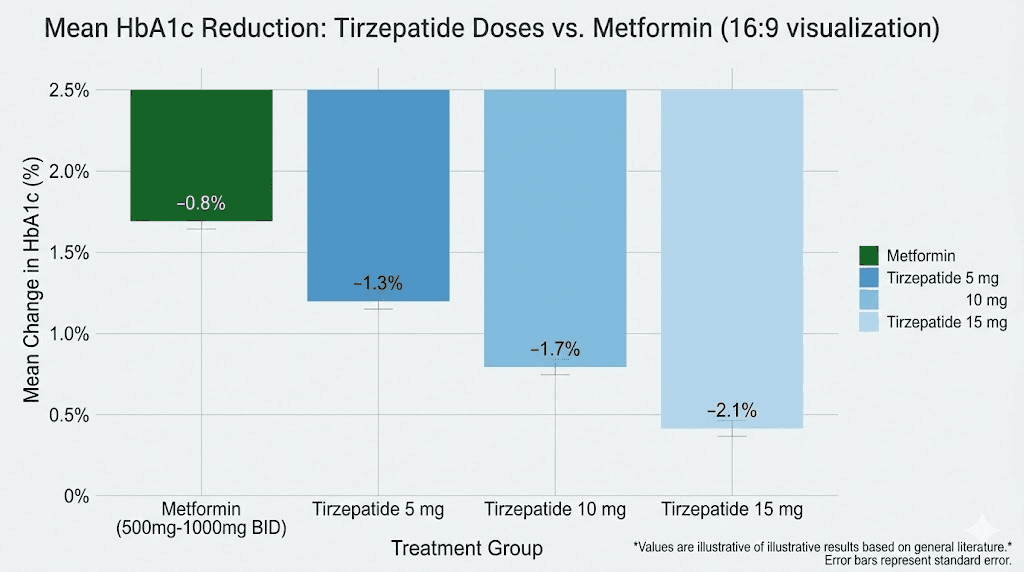
SURPASS-2 enrolled 1,879 adults with type 2 diabetes who had inadequate blood sugar control on metformin alone, at doses of 1,500 mg or higher per day. These patients were randomized to receive tirzepatide at 5 mg, 10 mg, or 15 mg weekly, or semaglutide 1 mg weekly, while continuing their existing metformin regimen. The trial ran for 40 weeks.
The results were striking.
Participants had a mean baseline HbA1c of 8.28% and a mean baseline weight of 93.7 kg. By the end of the study, the tirzepatide groups achieved HbA1c reductions of 2.01 percentage points (5 mg dose), 2.24 percentage points (10 mg dose), and 2.30 percentage points (15 mg dose). For context, a 2.0+ percentage point reduction in HbA1c is exceptional. Many patients went from poorly controlled diabetes to normal or near-normal blood sugar levels within 40 weeks, all while continuing metformin.
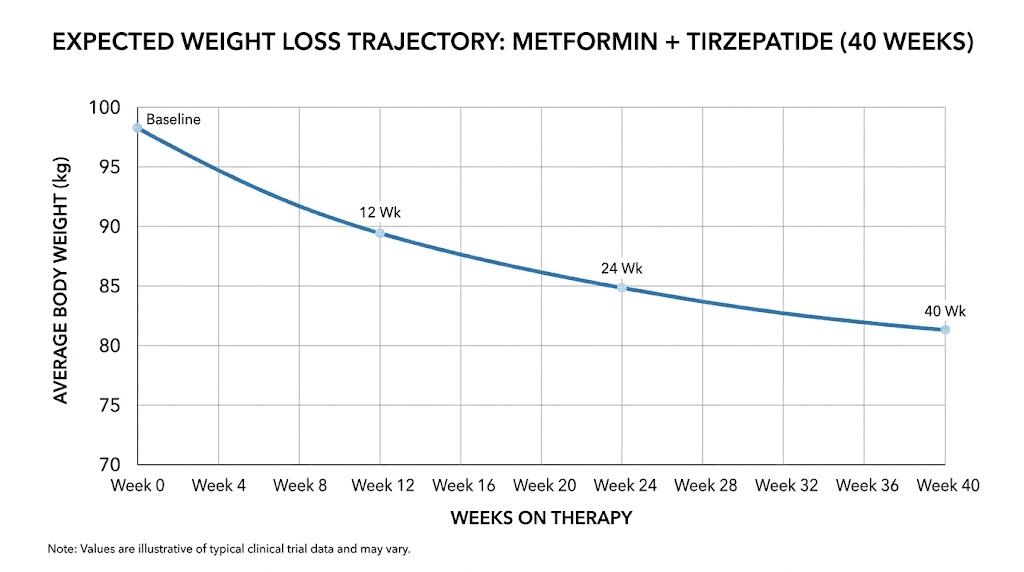
Weight loss told an equally compelling story. Patients on metformin plus tirzepatide experienced mean weight losses ranging from 7.6 kg at the 5 mg dose to 12.9 kg at the 15 mg dose. The 15 mg tirzepatide group achieved 5.5 kg more weight loss than the semaglutide group, a statistically significant and clinically meaningful difference.
Perhaps the most impressive finding involved a composite endpoint: achieving HbA1c at or below 6.5% with at least 10% body weight loss and no hypoglycemic episodes. Among the tirzepatide groups, 32% (5 mg), 51% (10 mg), and 60% (15 mg) of participants hit this triple target. Only 22% of semaglutide patients achieved the same.
SURPASS-4: long-term safety data
SURPASS-4 extended the evidence to 104 weeks, two full years, in patients with type 2 diabetes inadequately controlled on metformin and/or sulfonylureas. This post-hoc analysis specifically evaluated the long-term efficacy and safety of tirzepatide when added to existing metformin therapy. The findings confirmed that the benefits seen at 40 weeks were sustained, with consistent HbA1c reductions and weight loss maintained through the two-year mark. No new safety signals emerged from the longer observation period.
This matters because combination therapy is not a short-term strategy. Most people who benefit from both medications will take them for years. Knowing the combination remains effective and well-tolerated over 104 weeks provides the kind of reassurance that 40-week data alone cannot.
What about other SURPASS trials?
The SURPASS program included five major trials, and metformin was a permitted or required background medication in most of them. Across the program, the consistency of results was remarkable. Whether patients were on metformin alone, metformin plus a sulfonylurea, or metformin plus insulin, adding tirzepatide produced significant improvements in both blood sugar control and weight loss. No trial identified a safety concern specific to the metformin-tirzepatide combination.
Drug interactions: what happens when both medications are in your system
One of the most common concerns about taking two medications together is drug interactions. Will one medication change how the other is absorbed? Will they compete for the same metabolic pathways? Could the combination produce unexpected effects that neither medication causes alone?
With metformin and tirzepatide, the pharmacokinetic picture is reassuringly clean.
There are no significant pharmacokinetic interactions between these two medications. They do not affect each other's absorption, distribution, metabolism, or elimination. Metformin is not metabolized by the liver's cytochrome P450 enzymes. It is absorbed in the small intestine and excreted unchanged by the kidneys. Tirzepatide, being a peptide-based medication, is broken down through proteolysis (protein degradation) rather than hepatic metabolism. These completely separate metabolic pathways mean neither medication alters the blood levels of the other.
However, one interaction deserves attention, and it is indirect.
Tirzepatide delays gastric emptying. This is actually one of its therapeutic mechanisms, slowing how quickly food leaves the stomach helps reduce post-meal blood sugar spikes and promotes feelings of fullness. But this same mechanism can theoretically slow the absorption of oral medications taken at the same time, including metformin. In practice, this effect appears to be clinically minor for metformin because metformin is primarily absorbed in the small intestine rather than the stomach. The delay in gastric emptying may shift the timing of metformin absorption slightly but does not reduce the total amount absorbed.
This gastric emptying effect is more relevant for other oral medications. The prescribing information for tirzepatide specifically warns about oral contraceptives, advising patients who use oral birth control to consider a non-oral method or add a barrier method for four weeks after starting tirzepatide and after each dose increase. For metformin, however, no dose adjustment is recommended when tirzepatide is added.
The clinical trials confirm this. In the SURPASS studies, metformin doses were not changed when tirzepatide was initiated. Patients continued their existing metformin regimen without modification, and the combination worked as expected.
Dosing protocols when combining both medications
Getting the dosing right for both medications simultaneously requires understanding each one's titration schedule and how they overlap in practice.
Metformin dosing basics
Most prescribers start metformin at 500 mg once daily, taken with a meal. The dose increases by 500 mg every one to two weeks, depending on tolerance, until reaching the target dose. Standard maintenance doses range from 1,500 to 2,000 mg daily, typically split into two or three doses taken with meals. Extended-release (ER) formulations allow once-daily dosing, usually 1,500-2,000 mg with dinner.
If you are already on a stable metformin dose before starting tirzepatide, there is generally no reason to change it. The clinical evidence supports continuing your existing metformin regimen exactly as prescribed.
Tirzepatide dosing protocol
Tirzepatide starts at 2.5 mg injected subcutaneously once weekly for a minimum of four weeks. This starting dose is not primarily therapeutic. It exists to let your body adjust to the medication and minimize gastrointestinal side effects. After the initial four weeks, the dose increases to 5 mg weekly. From there, your prescriber may increase the dose by 2.5 mg increments, no more frequently than every four weeks, up to a maximum of 15 mg weekly.
The starting dose and escalation schedule remain identical whether you are on metformin or not. There is no need to adjust the tirzepatide titration based on concurrent metformin use.
Practical combination protocol
Here is what a typical combination looks like in practice:
If you are already on metformin and adding tirzepatide:
Continue your current metformin dose without changes
Begin tirzepatide at 2.5 mg weekly
Choose a consistent injection day each week
Take metformin with meals as usual
After 4 weeks, increase tirzepatide to 5 mg if tolerated
Subsequent increases every 4+ weeks as directed by your prescriber
If starting both medications simultaneously:
Begin metformin at 500 mg once daily with a meal
Wait 1-2 weeks for GI tolerance before adding tirzepatide
Start tirzepatide at 2.5 mg weekly
Titrate metformin upward by 500 mg weekly to target dose
Titrate tirzepatide upward per standard schedule
Some prescribers prefer to stagger the initiation of both medications by two to four weeks. This approach has practical value: if you start both on the same day and develop nausea, you will not know which medication is causing it. Starting them separately makes it easier to identify and manage side effects from each medication individually.
For detailed unit-based dosing guidance, check out the tirzepatide dosing chart and the compounded tirzepatide dosage calculator on SeekPeptides.
Managing overlapping gastrointestinal side effects
Here is the honest truth about combining these medications: both can cause GI issues, and when taken together, those issues can sometimes amplify each other. This section is arguably the most practically important part of this entire guide, because GI side effects are the primary reason people discontinue either medication.
The shared side effect profile
Metformin commonly causes diarrhea, nausea, flatulence, indigestion, vomiting, and abdominal discomfort. Diarrhea and nausea are the most frequent complaints, affecting roughly 10-25% of patients depending on the dose and formulation.
Tirzepatide commonly causes nausea, diarrhea, decreased appetite, vomiting, constipation, and abdominal pain. Nausea is the most reported side effect, occurring in 12-18% of patients in clinical trials, with higher rates at larger doses.
Notice the overlap. Both medications can cause nausea. Both can cause diarrhea. Both can cause abdominal discomfort. When you combine them, you are not doubling the side effects, but you are increasing the likelihood of experiencing them, particularly during the adjustment period when your body is getting used to both.
The good news about timing
GI side effects from both medications are typically worst during the first few weeks and during dose escalation. They tend to diminish as your body adapts. For metformin, most patients find that GI symptoms settle within two to four weeks of reaching a stable dose. For tirzepatide, nausea and other GI effects usually peak in the first one to two weeks after each dose increase and then gradually fade.
If you are already established on metformin and your GI system has adapted, adding tirzepatide at the 2.5 mg starting dose may produce minimal additional GI effects. Your gut has already adjusted to one medication, and the low starting dose of tirzepatide gives it time to adjust to the second.
Practical strategies for minimizing GI issues
Dietary adjustments make a real difference. Eating smaller, more frequent meals throughout the day, five or six instead of three, prevents the stomach from becoming overly full. This is especially important with tirzepatide because it slows gastric emptying. A large meal that would normally leave the stomach in two hours might sit there for three or four, creating that uncomfortable fullness and nausea that many people report.
Choose easily digestible foods during the adjustment period. High-fat meals take longer to digest and can worsen nausea. Heavily processed foods and fried items tend to cause the most discomfort. Lean proteins, cooked vegetables, and simple carbohydrates are generally better tolerated. For a comprehensive food guide, review our article on foods to avoid on tirzepatide and the best foods to eat on GLP-1 medications.
Hydration matters more than most people realize. Sip fluids consistently throughout the day rather than gulping large volumes. Room temperature beverages tend to be better tolerated than very hot or very cold drinks. Ginger tea and peppermint tea have mild anti-nausea properties that some people find helpful. If nausea is significant, over-the-counter ondansetron (Zofran) is effective, and your prescriber can provide a prescription if needed.
Timing your metformin dose with food is critical. Never take metformin on an empty stomach, as this dramatically increases the chance of GI side effects. The extended-release formulation of metformin produces significantly fewer GI symptoms than the immediate-release version. If you are experiencing persistent diarrhea or stomach upset from metformin, ask your prescriber about switching to metformin ER.
Eat your last meal at least two to three hours before bedtime. Lying down shortly after eating amplifies the uncomfortable fullness caused by tirzepatide's gastric emptying delay. Late-night eating on this combination is a recipe for overnight nausea.
When to contact your prescriber
Most GI side effects are uncomfortable but not dangerous. However, certain symptoms warrant a call to your healthcare provider:
Nausea severe enough to prevent eating or drinking for more than 24 hours
Persistent vomiting, especially if it continues beyond 24 hours
Signs of dehydration (dark urine, dizziness when standing, dry mouth)
Severe abdominal pain that does not resolve
Diarrhea that continues for more than three days
In rare cases, your prescriber may temporarily reduce the tirzepatide dose or pause the dose escalation until GI symptoms resolve. They may also reduce the metformin dose temporarily. This is not a failure. It is smart, individualized medicine.
Why these medications are better together than alone
The rationale for combining metformin and tirzepatide goes beyond simply adding the effects of two medications. There are genuine synergistic interactions between these medications that produce outcomes neither can achieve independently.
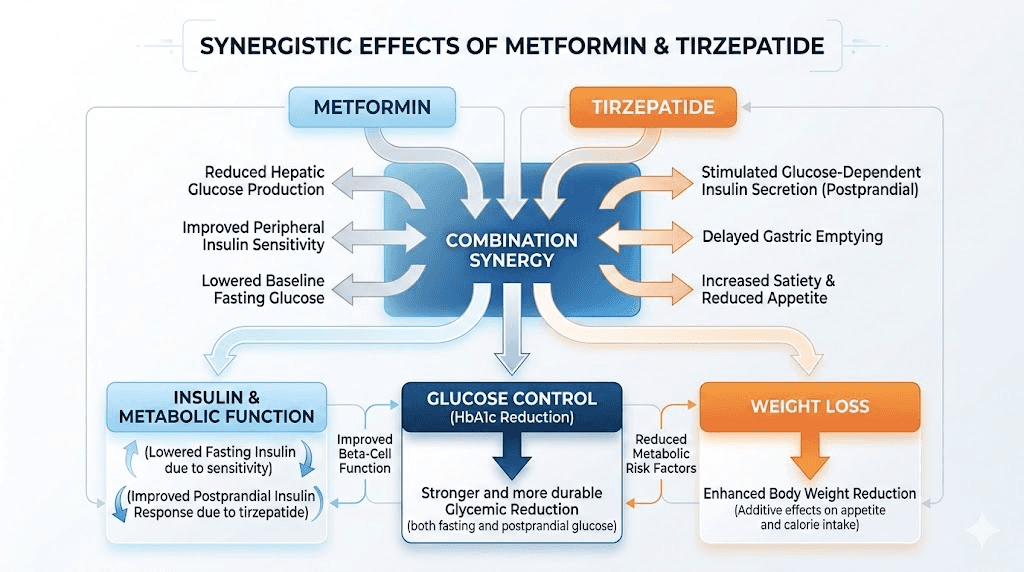
Complementary metabolic pathways
Metformin primarily targets fasting glucose by reducing hepatic glucose production. Tirzepatide primarily targets post-meal glucose through insulin secretion and gastric emptying. When you combine them, you are covering the full 24-hour glucose cycle. Fasting levels stay lower because of metformin. Post-meal spikes are blunted because of tirzepatide. The result is smoother, more stable blood sugar throughout the day.
The SURPASS-2 data illustrates this perfectly. Patients on metformin alone had a mean HbA1c of 8.28%, despite being on at least 1,500 mg daily. Adding tirzepatide dropped that by over two percentage points. Many participants achieved an HbA1c below 5.7%, which is technically in the normal, non-diabetic range. Metformin alone rarely achieves this. Tirzepatide alone rarely achieves this for patients with long-standing diabetes. Together, the combination accomplished what each medication could not do on its own.
The hidden GLP-1 connection
Here is something fascinating that most articles about this combination miss entirely. Metformin actually increases natural GLP-1 secretion from L cells in the gut. Research in the journal Diabetologia demonstrated that metformin has a direct, AMPK-dependent effect on these GLP-1-producing cells, boosting the body's own GLP-1 output.
Why does this matter? Because tirzepatide is a synthetic GLP-1 (and GIP) receptor agonist. When you take metformin, your body produces more natural GLP-1. When you add tirzepatide, you get even more GLP-1 receptor activation from the synthetic version. The combination creates a more robust GLP-1 signal than either approach alone, which translates to better appetite control, better insulin secretion, and better blood sugar management.
Think of it this way: metformin turns up the volume on your body's natural GLP-1 production, and tirzepatide adds a powerful external speaker. The combined signal is louder and clearer than either source alone.
Enhanced insulin sensitivity
Metformin improves how cells respond to insulin, a property called insulin sensitization. It does this partly through AMPK activation and partly by reducing fat accumulation in the liver and muscle, two conditions (hepatic steatosis and intramyocellular lipid accumulation) that drive insulin resistance. Tirzepatide also improves insulin sensitivity, but primarily through weight loss and direct metabolic effects on fat tissue.
The combination attacks insulin resistance from multiple angles simultaneously. Metformin works at the cellular level to make tissues respond better to insulin. Tirzepatide reduces body fat, which removes one of the primary causes of insulin resistance in the first place. The result is greater improvement in insulin sensitivity than either medication provides alone.
Weight loss synergy
Metformin produces modest weight loss, typically 2-3 kg over several months, through mechanisms that include reduced appetite (via increased GLP-1), decreased hepatic fat, and possibly altered gut microbiome composition. It is not primarily a weight loss drug, but it helps.
Tirzepatide produces substantial weight loss, 7-13 kg in clinical trials, through potent appetite suppression, delayed gastric emptying, and direct effects on fat metabolism through GIP receptor activation. It is one of the most effective weight loss medications ever studied.
When combined, the total weight loss tends to exceed what tirzepatide alone achieves. Metformin's contribution to weight stability, insulin sensitivity improvement, and background GLP-1 enhancement creates a metabolic environment where tirzepatide can work more effectively. The combination also appears to help maintain weight loss over time, a critical consideration since weight regain after stopping GLP-1 medications is a well-documented concern. Our guide on maintaining weight loss after tirzepatide covers this in detail.
Who benefits most from the combination
Not everyone needs both medications. Understanding who benefits most from the metformin-tirzepatide combination helps set realistic expectations and guides treatment decisions.
Type 2 diabetes with inadequate control on metformin
This is the classic scenario supported by the strongest evidence. If you have type 2 diabetes and your HbA1c remains above target (typically above 7.0%) despite being on a full dose of metformin (1,500-2,000 mg daily), adding tirzepatide is one of the most effective next steps available. The SURPASS trials enrolled exactly this population and demonstrated consistent, robust results.
Type 2 diabetes with obesity
For patients who have both type 2 diabetes and obesity (BMI 30 or higher), the combination is particularly compelling. You get the blood sugar control benefits from both medications plus the significant weight loss that tirzepatide provides. Losing 10-15% of body weight often produces dramatic improvements in insulin sensitivity, sometimes allowing patients to reduce other diabetes medications.
Insulin resistance without diabetes
Some prescribers use the combination for patients with significant insulin resistance (sometimes called pre-diabetes or metabolic syndrome) who have not yet progressed to type 2 diabetes. Metformin is commonly used off-label in this population, and adding tirzepatide (marketed as Zepbound for weight management in non-diabetic patients) can address both the insulin resistance and the excess weight that drives it. This represents a more aggressive approach to metabolic health that aims to prevent diabetes rather than treat it.
PCOS (polycystic ovary syndrome)
Metformin has been used for decades in PCOS management due to its effects on insulin resistance, which drives many PCOS symptoms. Some prescribers are now combining it with tirzepatide for PCOS patients who also struggle with weight management. The weight loss from tirzepatide can improve hormonal balance, menstrual regularity, and fertility in PCOS, while metformin addresses the underlying insulin resistance.
Weight regain prevention
Some prescribers continue metformin even when a patient achieves their weight loss goals on tirzepatide, using it as a maintenance strategy. The rationale is that metformin's insulin-sensitizing effects and modest appetite-suppressing properties may help prevent weight regain if the tirzepatide dose is reduced or eventually discontinued. The evidence for this specific approach is limited but the theoretical basis is sound.
Situations where the combination requires extra caution
While the metformin-tirzepatide combination is safe for most people, certain situations demand additional monitoring or dose adjustments.
Kidney function concerns
Metformin is cleared by the kidneys. If kidney function declines, metformin can accumulate in the body and increase the risk of a rare but serious condition called lactic acidosis. Your prescriber should check kidney function (eGFR) before starting metformin and periodically thereafter. Metformin is generally safe when eGFR is above 30, used with caution between 30-45, and contraindicated below 30. Tirzepatide does not significantly affect kidney function, but the combination means kidney monitoring becomes even more important.
Hypoglycemia risk
Neither metformin nor tirzepatide commonly causes hypoglycemia (dangerously low blood sugar) when used alone or together. Both medications are "glucose-dependent," meaning they primarily work when blood sugar is elevated and back off when it drops to normal levels. However, if you are also taking a sulfonylurea (like glipizide or glyburide) or insulin, the addition of tirzepatide can increase hypoglycemia risk. Your prescriber may need to reduce the dose of these other medications when adding tirzepatide.
Dehydration risk
Both medications can contribute to fluid loss. Metformin through GI effects (diarrhea). Tirzepatide through reduced food and fluid intake (from appetite suppression) and GI effects (nausea, vomiting). Dehydration is particularly concerning because it can impair kidney function, which then affects metformin clearance. Maintaining adequate hydration is not optional when on this combination. It is essential.
Pancreatitis history
GLP-1 receptor agonists, including tirzepatide, carry a theoretical risk of pancreatitis, though the actual risk in clinical trials has been very low. Metformin is not associated with pancreatitis risk. If you have a history of pancreatitis, your prescriber will weigh this risk carefully and monitor for symptoms (severe abdominal pain radiating to the back, nausea, vomiting).
Contrast dye procedures
If you need a CT scan or other imaging procedure with iodinated contrast dye, your prescriber will typically hold metformin for 48 hours before and after the procedure. This has nothing to do with tirzepatide and everything to do with the temporary effect contrast dye can have on kidney function, which could impair metformin clearance. Tirzepatide can usually be continued through these procedures without interruption.
Metformin and tirzepatide for weight loss specifically
An increasing number of people are using or considering this combination specifically for weight management rather than diabetes treatment. The evidence supports this approach, though the context differs slightly from diabetes management.
How much weight can you expect to lose?
In the SURPASS-2 trial (patients with type 2 diabetes on metformin), weight loss with tirzepatide ranged from 7.6 kg to 12.9 kg over 40 weeks, depending on the tirzepatide dose. In the SURMOUNT trials (non-diabetic patients with obesity, some on metformin), weight loss was even more dramatic, with the 15 mg dose producing approximately 22.5% total body weight loss over 72 weeks.
Adding metformin to tirzepatide for weight loss provides several advantages beyond the modest additional weight loss metformin itself produces:
Improved insulin sensitivity may help the body metabolize fat more efficiently
Reduced hepatic fat can improve metabolic health markers independent of total weight loss
Increased natural GLP-1 production amplifies tirzepatide's appetite-suppressing effects
Better blood sugar stability reduces cravings and energy crashes
The lean mass concern
One valid concern with significant weight loss from GLP-1 medications is the loss of lean muscle mass along with fat. Both tirzepatide and semaglutide produce weight loss that includes roughly 25-40% lean mass. Metformin may modestly help preserve lean mass through its effects on AMPK activation in muscle tissue, though the evidence for this is preliminary.
Regardless of medication, the most important strategies for preserving lean mass during weight loss are adequate protein intake (1.2-1.6 g/kg body weight daily) and resistance training (at least 2-3 sessions per week). These interventions matter far more than any medication adjustment for lean mass preservation.
Building an effective weight loss protocol
For weight loss optimization with this combination, consider these evidence-based strategies:
Nutrition: Prioritize protein at every meal. Follow a tirzepatide-friendly diet plan that emphasizes nutrient-dense, easily digestible foods. Track protein intake to ensure you are hitting minimums. Eat slowly and stop at comfortable fullness, which will come sooner due to tirzepatide's appetite effects.
Exercise: Focus on resistance training to preserve muscle. Add moderate cardio (walking, cycling, swimming) for cardiovascular health and additional calorie expenditure. Do not overdo cardio early in the process when appetite is most suppressed, as this can lead to excessive calorie deficit.
Supplements: Consider a quality multivitamin during significant calorie restriction. Vitamin D, magnesium, and omega-3 fatty acids are commonly needed. Our guide on supplements to take with tirzepatide covers the specifics.
Monitoring: Track weight weekly (same day, same time, same conditions). Use body measurements or body composition scans rather than relying solely on the scale. Monitor energy levels, sleep quality, and mood as indicators of overall metabolic health.
Comparing metformin plus tirzepatide to other combinations
Metformin plus tirzepatide is not the only combination therapy available. Understanding how it compares to alternatives helps put its benefits in perspective.
Metformin plus tirzepatide vs. metformin plus semaglutide
The SURPASS-2 trial directly compared these two combinations. At equivalent doses, tirzepatide produced greater HbA1c reductions and greater weight loss than semaglutide when added to metformin. The 15 mg tirzepatide dose achieved 5.5 kg more weight loss than semaglutide 1 mg. The advantage appears to come from tirzepatide's dual mechanism (GIP plus GLP-1) versus semaglutide's single mechanism (GLP-1 only). For a detailed comparison, see our semaglutide vs tirzepatide breakdown.
That said, semaglutide 2.4 mg (Wegovy dose for weight management) was not directly compared to tirzepatide in the SURPASS trials, so the comparison against the highest semaglutide dose is less clear. Both are excellent options. Tirzepatide appears to have an edge in total efficacy, but individual response varies considerably.
Metformin plus tirzepatide vs. metformin plus insulin
Adding insulin to metformin is the traditional approach for type 2 diabetes that is not controlled by metformin alone. Insulin is highly effective at lowering blood sugar but typically causes weight gain (4-8 kg in the first year) and carries significant hypoglycemia risk. Tirzepatide produces comparable or superior blood sugar control while causing weight loss rather than weight gain and much lower hypoglycemia risk. For most patients, metformin plus tirzepatide is now preferred over metformin plus insulin, unless insulin is specifically needed (very high HbA1c, type 1 diabetes features, etc.).
Metformin plus tirzepatide vs. metformin plus phentermine
For weight loss specifically, some providers combine metformin with phentermine as a lower-cost alternative. Phentermine is a stimulant-based appetite suppressant that works through completely different mechanisms (norepinephrine release in the CNS). While this combination can be effective for short-term weight loss, phentermine has significant limitations: it is typically only approved for short-term use (12 weeks), it can raise blood pressure and heart rate, it carries abuse potential, and it does not improve blood sugar or insulin sensitivity. Tirzepatide is a more comprehensive and sustainable option, though it costs more. See our phentermine vs GLP-1 comparison for more context.
Combination | HbA1c Reduction | Weight Loss | Hypo Risk | Duration | Key Advantage |
|---|---|---|---|---|---|
Metformin + tirzepatide | 2.0–2.3% | 7.6–12.9 kg (40 wks) | Very low | Long-term | Best overall efficacy |
Metformin + semaglutide | 1.8–1.9% | 5.7–6.2 kg (40 wks) | Very low | Long-term | Established track record |
Metformin + insulin | 1.5–2.0% | +4–8 kg (gain) | Moderate–high | Long-term | Reliable glucose control |
Metformin + phentermine | Minimal | 5–8 kg (12 wks) | None | Short-term only | Lower cost |
Metformin + sulfonylurea | 1.0–1.5% | +1–3 kg (gain) | Moderate | Long-term | Very low cost |
Practical tips from clinical experience
Beyond the clinical trial data, certain practical considerations make a real difference in how well this combination works in daily life.
Timing your medications
Metformin should always be taken with food. If you are on twice-daily dosing, take it with breakfast and dinner. If you are on extended-release, take it with your largest meal (usually dinner). Tirzepatide can be injected at any time of day, with or without food. Many people find it most convenient to inject on the same day each week, often in the morning. The best time to take your GLP-1 shot is whenever you will consistently remember it.
Some patients report that injecting tirzepatide on Friday evening works well because any GI side effects (most common in the 24-48 hours after injection) occur over the weekend when they can rest at home. Others prefer Monday morning so the injection's appetite-suppressing effects peak during the workweek when healthy eating is most challenging. There is no medically superior timing. Choose whatever fits your schedule.
What to do when you plateau
Weight loss and blood sugar improvements often slow after several months on any medication. If you hit a plateau on the metformin-tirzepatide combination, consider these steps before assuming the medications have stopped working:
First, review your diet honestly. Tirzepatide's appetite suppression can wane slightly as your body adjusts, and old eating habits may creep back. Tracking food intake for a week or two often reveals the issue. Our guide on tirzepatide not working anymore covers common plateau causes and solutions.
Second, check if you are at an appropriate tirzepatide dose. Many patients see renewed progress when increasing from 5 mg to 10 mg, or from 10 mg to 15 mg. The dose escalation exists precisely for this reason.
Third, verify your metformin dose. If you are on less than 2,000 mg daily and tolerating it well, there may be room to increase. Extended-release metformin at 2,000 mg daily provides the maximum therapeutic effect.
Fourth, evaluate your exercise routine. Adding or increasing resistance training often breaks plateaus by improving insulin sensitivity and increasing metabolic rate through muscle preservation. If your weight loss has stalled, the issue is rarely the medication alone.
Monitoring and lab work
When on both medications, your prescriber will typically monitor:
HbA1c every 3 months until stable, then every 6 months
Fasting glucose as needed for dose adjustments
Kidney function (eGFR, creatinine) at least annually, more often if impaired
Liver function tests periodically (metformin is generally safe for the liver, but baseline and periodic monitoring is good practice)
Vitamin B12 levels annually (metformin can reduce B12 absorption over time, see our guide on B12 supplementation with GLP-1 medications)
Lipid panel annually (both medications can improve lipid profiles)
Complete blood count periodically
Vitamin B12 monitoring deserves special attention. Metformin is known to reduce B12 absorption in the small intestine, and long-term use (years) can lead to B12 deficiency if not monitored. Symptoms of B12 deficiency include fatigue, numbness or tingling in the hands and feet, cognitive changes, and anemia. A simple blood test catches this early, and supplementation is straightforward.
Alcohol and this combination
Both medications have implications for alcohol consumption. Metformin can increase the risk of lactic acidosis in the setting of excessive alcohol intake, as alcohol impairs the liver's ability to clear lactate. Tirzepatide slows gastric emptying, which can alter how quickly alcohol is absorbed and increase its effects. Heavy or binge drinking is not recommended with either medication, and the combination amplifies this advice. Moderate, occasional alcohol consumption is generally considered acceptable, but discuss your specific situation with your prescriber. For more detail, see can you drink on tirzepatide.
Switching between or adding medications
Several common scenarios involve transitions between medications while maintaining the metformin foundation.
Switching from semaglutide to tirzepatide (while staying on metformin)
If you are on metformin plus semaglutide and switching to tirzepatide, the transition is relatively straightforward. Most prescribers recommend starting tirzepatide at 2.5 mg on the week following your last semaglutide injection. Continue metformin unchanged throughout the transition. Our semaglutide to tirzepatide conversion chart provides detailed dose mapping guidance.
Expect some adjustment period during the switch. Even though both are GLP-1 receptor agonists, tirzepatide's additional GIP activity means your body needs time to adapt to the dual mechanism. GI side effects may temporarily return during this transition.
Adding metformin to an existing tirzepatide regimen
If you are already on tirzepatide and your prescriber wants to add metformin, the standard approach is to start metformin at 500 mg once daily with food and titrate upward by 500 mg every one to two weeks until reaching the target dose. Extended-release metformin is often preferred in this scenario to minimize additional GI burden on top of existing tirzepatide GI effects. No tirzepatide dose adjustment is needed.
Considering retatrutide or other next-generation options
For people interested in the latest developments, retatrutide is a triple-receptor agonist (GLP-1, GIP, and glucagon) currently in clinical trials. While not yet approved, early data suggests even greater weight loss potential than tirzepatide. The retatrutide vs tirzepatide comparison is an area of active research. Metformin will likely remain a valuable combination partner for these next-generation medications as well, given its complementary mechanism and excellent safety profile.
The cost and access question
Practical considerations around cost and insurance coverage significantly affect medication decisions.
Metformin is one of the least expensive prescription medications available. Generic metformin costs roughly $4-15 per month at most pharmacies, even without insurance. It has been available as a generic for decades, and cost is rarely a barrier to access.
Tirzepatide is significantly more expensive. Brand-name versions (Mounjaro for diabetes, Zepbound for weight management) can cost $1,000+ per month without insurance. Insurance coverage varies widely. Many commercial insurance plans cover Mounjaro for type 2 diabetes but may restrict or deny coverage for weight management (Zepbound). Prior authorization requirements are common.
Compounded tirzepatide has emerged as a lower-cost alternative. Our guides on affordable tirzepatide and cheap compounded tirzepatide options cover the landscape. For those using compounded formulations, the reconstitution process and proper storage become important practical skills. SeekPeptides provides detailed reconstitution guides and calculators to help with this process.
From a cost-effectiveness perspective, the metformin-tirzepatide combination makes strong economic sense. Adding a $10/month medication (metformin) to enhance the effectiveness of a $1,000/month medication (tirzepatide) is arguably the best return on investment in all of metabolic medicine. If metformin helps you achieve your goals at a lower tirzepatide dose, or reach your goals faster, the savings dwarf the modest cost of metformin.
The role of lifestyle alongside medication
No medication combination replaces the fundamentals of healthy eating, regular physical activity, adequate sleep, and stress management. Metformin and tirzepatide create a powerful metabolic foundation, but the lifestyle choices you make on top of that foundation determine your overall outcomes.
Patients who combine these medications with structured nutrition and exercise programs consistently achieve better results than those who rely on medication alone. The medications reduce appetite and improve metabolic function, making healthy behaviors easier to maintain. Take advantage of this window. When tirzepatide reduces your appetite, use that opportunity to establish healthy eating patterns that you can sustain long-term. When metformin improves your insulin sensitivity, complement it with regular exercise that further enhances glucose uptake in muscle tissue.
For practical meal planning guidance while on these medications, explore the tirzepatide meal plan, the semaglutide diet plan, and our comprehensive guide on what to eat on tirzepatide. For understanding how the medications fit into a broader weight loss strategy, SeekPeptides members access detailed protocols, tracking tools, and a community of researchers navigating these same decisions.
Frequently asked questions
Do I need to adjust my metformin dose when starting tirzepatide?
No. In clinical trials (SURPASS program), metformin doses were not changed when tirzepatide was added. Continue your existing metformin regimen as prescribed. Your prescriber may only adjust metformin if you experience significant GI side effects that necessitate temporary dose reduction.
Can I take metformin and tirzepatide at the same time of day?
Yes. Metformin is taken orally with meals, while tirzepatide is injected subcutaneously once weekly. There is no interaction requiring separation of doses. Take metformin with your meals as usual and inject tirzepatide at whatever time is convenient on your chosen day.
Will the nausea be worse if I take both medications?
It can be, particularly during the initial adjustment period or dose escalations. However, if you are already established on metformin and your GI system has adapted, adding low-dose tirzepatide (2.5 mg) typically produces manageable symptoms. Staggering the start of each medication by 2-4 weeks can help identify which medication is causing any GI issues. Using extended-release metformin also significantly reduces GI side effects.
Is it safe to stop metformin once I start tirzepatide?
This decision should be made by your prescriber based on your individual situation. For type 2 diabetes, most guidelines recommend continuing metformin as foundational therapy. For weight management without diabetes, the role of metformin is less established and stopping it may be appropriate if tirzepatide alone is achieving your goals. Do not stop metformin without discussing it with your healthcare provider.
How much additional weight loss does adding metformin to tirzepatide provide?
Metformin alone typically produces 2-3 kg of weight loss. When added to tirzepatide, the additional weight loss is modest but the metabolic benefits (improved insulin sensitivity, enhanced GLP-1 signaling, reduced hepatic fat) contribute to better overall outcomes and potentially more sustainable long-term weight maintenance.
Can I take metformin, tirzepatide, and other medications together?
Many patients take additional medications alongside metformin and tirzepatide, including blood pressure medications, statins, and thyroid medications. Tirzepatide's gastric emptying delay can theoretically affect the absorption timing of oral medications, so discuss your complete medication list with your prescriber. Some adjustments may be needed, particularly for medications with narrow therapeutic windows.
Does the combination affect fertility or pregnancy?
Both tirzepatide and metformin can improve hormonal balance and ovulation in women with PCOS or insulin resistance, potentially increasing fertility. If pregnancy is possible, this is an important discussion to have with your prescriber before starting the combination. Tirzepatide should be stopped at least two months before planned conception. Metformin's safety in pregnancy is better established but still requires prescriber guidance. See our article on pregnancy and tirzepatide for more information.
How long does it take to see results from the combination?
Most people notice appetite changes within the first week or two of starting tirzepatide. Measurable weight loss typically begins within 4-6 weeks. Blood sugar improvements can be detected within 2-4 weeks. Full steady-state effects of tirzepatide develop over 4-5 weeks at each dose level. For detailed timelines, see our guide on how long tirzepatide takes to work.
External resources
For researchers serious about understanding peptide-based therapies and optimizing their protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your blood sugar stay stable, your side effects stay manageable, and your protocols stay effective.