Feb 27, 2026

Hour one. Nothing. Hour six, maybe a faint heaviness in the stomach. Hour twelve, you notice you forgot about the leftover pizza in the fridge. Day three, you eat half a sandwich and push the plate away. Day seven, you step on the scale and squint. Something shifted.
That is the real first-week arc for most people starting tirzepatide, and it looks nothing like the dramatic transformation stories plastered across social media. The reality is quieter. More gradual. And honestly, more confusing than most guides prepare you for, because nobody tells you that the first dose is mostly a waiting game where your body and the medication figure each other out before anything visible happens on the outside.
This guide covers everything that happens after your first tirzepatide injection. Not the idealized version. The actual version, hour by hour, day by day, and week by week, with specific timelines, the side effects to expect (and the ones that mean something is wrong), exactly what changes in your appetite and digestion, and how to handle the adjustment period so you get the best possible start. Whether you are using brand-name Zepbound, Mounjaro, or a compounded tirzepatide formulation, the first-dose experience follows remarkably similar patterns. And understanding those patterns before they happen is the difference between panicking at every new sensation and recognizing exactly what your body is doing.
SeekPeptides has tracked thousands of first-dose experiences through member reports and protocol tracking, and the data tells a clear story. Your first dose matters less for what it does and more for how you respond to it. Here is that complete picture.
How tirzepatide actually works in your body
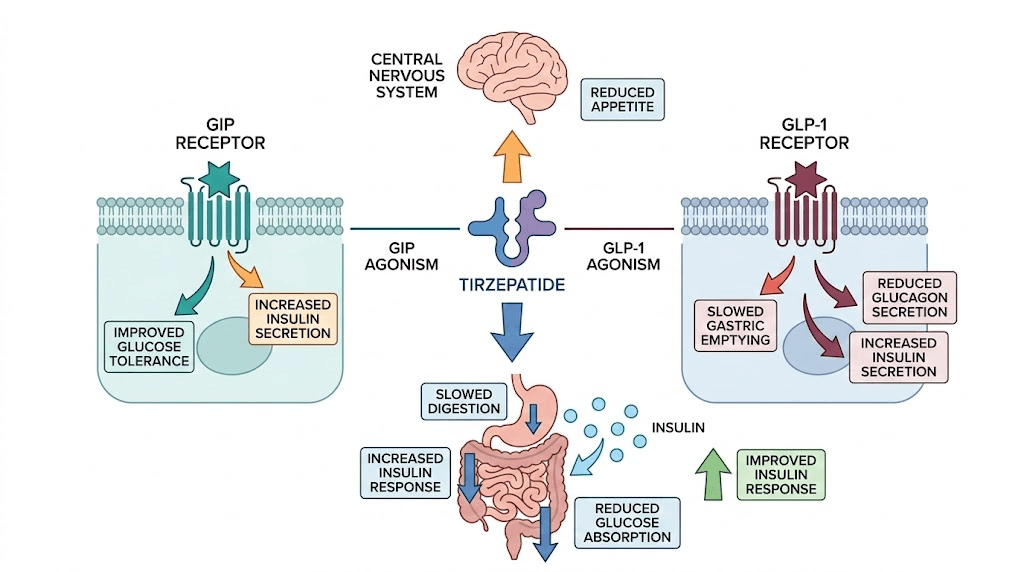
Before diving into timelines, understanding the mechanism helps you interpret every sensation you feel after that first injection. Tirzepatide is not a simple appetite suppressant. It is a dual GIP/GLP-1 receptor agonist, a 39-amino-acid synthetic peptide that activates two separate incretin receptors simultaneously. That dual action is what separates it from semaglutide and other single-receptor GLP-1 medications.
The GLP-1 receptor activation slows gastric emptying. Food sits in your stomach longer. You feel full faster and stay full longer. This is why many people describe their appetite changing before they see any weight on the scale move. The GIP receptor activation adds something semaglutide cannot do alone. It improves insulin sensitivity, enhances fat metabolism, and influences energy balance through pathways that researchers are still mapping.
Here is what matters for your first dose. Tirzepatide has a half-life of approximately five days. That means it takes roughly five days for half the medication to clear your system, and about 20 to 25 days to reach steady-state concentration. Your first injection starts building this baseline. You are not getting the full therapeutic effect on day one. You are laying groundwork.
The dual agonism also explains why tirzepatide produces different side effect profiles than semaglutide and other pure GLP-1 agonists. Some people tolerate it better. Others experience effects that single-agonist medications do not produce. Both responses are normal, and both make sense when you understand that two receptor systems are adjusting simultaneously.
Clinical trials like SURMOUNT-1 showed average weight loss of 15 to 22.5 percent of body weight over 72 weeks depending on dose. But none of that happens from one injection. The complete weight loss timeline builds gradually, and your first dose is the very beginning of a long curve. Knowing this prevents the disappointment that derails many people in week one when the scale barely moves. Tirzepatide also outperforms single-agonist medications in head-to-head comparisons, which is why researchers are so interested in how it compares to both semaglutide and newer triple agonists like retatrutide.
The first 24 hours after your injection
You did it. The needle went in, the plunger went down, and now you are staring at the injection site wondering what happens next. Here is the truth about the first 24 hours, broken into what actually happens at each stage.
Hours 0 to 2: immediately after injection
Most people feel nothing. Literally nothing beyond the injection site itself. If you used a standard insulin syringe technique, you might notice a small red dot, slight tenderness, or mild warmth at the injection site. This is normal and resolves within minutes to hours.
The medication is now being absorbed from the subcutaneous tissue into your bloodstream. Absorption rate depends on your injection site. The abdomen tends to absorb slightly faster than the thigh or upper arm. But we are talking small differences, not clinically meaningful ones for most people.
Do not expect to feel appetite changes yet. Do not expect nausea. Do not expect anything. The medication is entering your system but has not reached concentrations high enough to produce noticeable effects in most people.
Hours 2 to 8: the quiet buildup
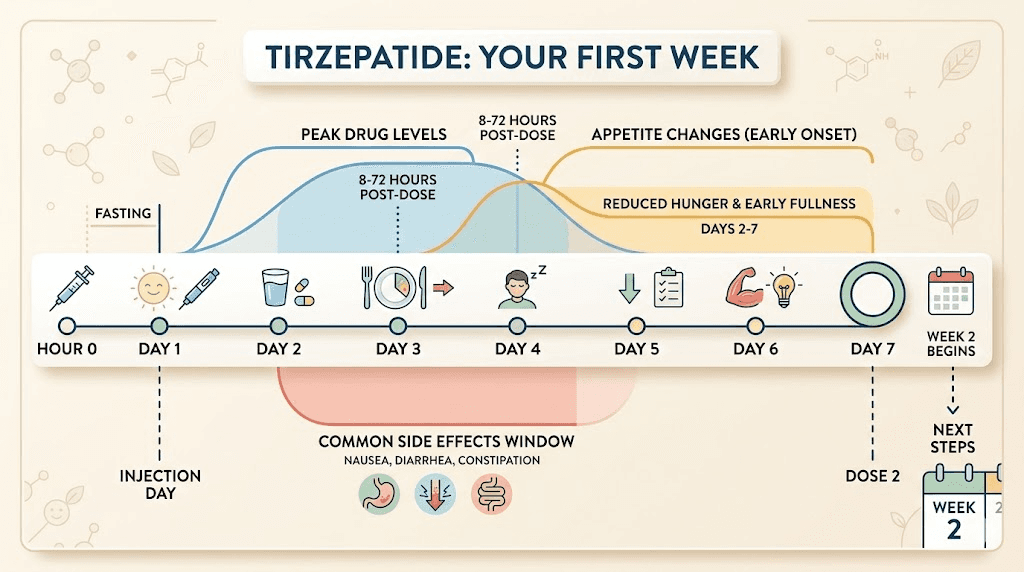
Tirzepatide serum levels are climbing during this window. Peak plasma concentration occurs somewhere between 8 and 72 hours after injection, with most people hitting peak levels around 24 to 48 hours. So during this early window, you are still on the upslope.
Some people, maybe 15 to 20 percent based on clinical data, report very early mild effects during this window. A slight decrease in appetite. A faint feeling of fullness that was not there before. A subtle heaviness in the stomach area. These early responders are not imagining things, but they are also not representative of everyone. If you feel nothing at hour six, that is the majority experience.
This is a good time to eat a normal, balanced meal. Do not skip dinner because you think the medication should be working already. Your starting dose of 2.5 mg is intentionally low. It is a calibration dose, designed to let your body adjust with minimal disruption before titrating up.
Hours 8 to 24: first potential effects
Now things get interesting for some people. As serum levels approach or reach peak concentration, a portion of first-time users start noticing changes. The most commonly reported first-day effects include mild nausea (reported by roughly 12 to 18 percent at the 2.5 mg starting dose), decreased appetite without feeling sick, slight fatigue or drowsiness, and a vague sense of stomach fullness.
Notice what is not on that list. Dramatic weight loss. Profound appetite elimination. Powerful food aversion. Those come later, at higher doses, after steady state. Your first day is subtle.
If you do experience nausea, it typically appears in this 8 to 24 hour window. It tends to be mild at the starting dose. Not the kind where you cannot function. More like background queasiness that comes and goes. Eating small, bland meals helps. Ginger tea helps. Staying hydrated helps. Lying down after eating helps. We will cover specific side effect management strategies in detail later in this guide.
The important thing about the first 24 hours is resetting your expectations. This is not a switch that flips. It is a dial that turns slowly. And on day one, it has barely moved.
Days 2 through 7: your first full week on tirzepatide
The first week is where patterns emerge. Not dramatic ones. Subtle ones that become obvious only in hindsight. Here is what each day typically brings.
Days 2 and 3: side effects peak (if they come at all)
If you are going to experience gastrointestinal side effects from your first dose, days two and three are when they most commonly appear. The medication is at or near peak concentration, and your digestive system is encountering GLP-1 receptor activation for the first time.
The stomach slows down. Gastric emptying rate decreases. Food that normally moved through in 2 to 4 hours might sit for 4 to 6 hours. This is the mechanism behind the nausea, the early fullness, and the general digestive weirdness that some people report.
Common day 2-3 experiences include feeling full after eating much less than usual, mild to moderate nausea especially after fatty or heavy foods, some people report diarrhea while others experience constipation (it can go either direction), fatigue that feels like you did not sleep enough even though you did, and mild headaches that may be related to reduced food intake or dehydration.
Not everyone gets these. Clinical trial data shows that at the 2.5 mg starting dose, gastrointestinal adverse events are significantly lower than at therapeutic doses of 10 or 15 mg. Many first-dose users sail through the entire week without any notable side effects.
Days 4 and 5: the adjustment begins
By day four, your body has been exposed to tirzepatide for long enough that initial adaptation is underway. If you experienced nausea on days two or three, it often improves noticeably by day four. The stomach is still processing food more slowly than baseline, but your digestive system is beginning to calibrate to the new normal.
Appetite effects become more consistent during this window. Instead of the fluctuating "sometimes hungry, sometimes not" pattern of the first few days, many people settle into a more predictable reduced-appetite state. It is not dramatic. You still want to eat. You just notice that you think about food less frequently, and meals feel satisfying sooner.
Fatigue, if present, also tends to improve around this time. The initial energy dip that some people report is likely a combination of reduced caloric intake and the metabolic adjustment to GIP/GLP-1 receptor activation. As your body adapts, energy levels typically stabilize.
This is a good time to pay attention to hydration. The combination of reduced appetite, potentially smaller meals, and the metabolic changes tirzepatide initiates means many people under-drink during their first week. Aim for at least 64 ounces of water daily. More if you are active. Dehydration amplifies every negative side effect, nausea, headaches, fatigue, all of them.
Days 6 and 7: approaching your next dose
As day seven approaches, serum levels of tirzepatide are declining. Remember that five-day half-life. By day seven, roughly 25 to 30 percent of the original dose remains active. Some people notice a slight return of baseline appetite during this window. Others feel consistent. Both patterns are normal.
If you chose your injection day and time strategically, your second dose lands right as the first is waning. Many users find that taking their injection on the same day and time each week creates the most consistent experience, minimizing the "peaks and valleys" of drug levels that can intensify side effects.
By the end of week one, here is what most people report. Weight change is minimal, typically 0 to 3 pounds, and much of that may be water or reduced gut content rather than fat loss. Appetite is noticeably but not dramatically reduced. Side effects, if they occurred, have mostly resolved or significantly improved. Energy levels have returned to baseline. Mood and motivation are largely unchanged from pre-treatment.
This is normal. This is expected. The full timeline for tirzepatide to produce significant results spans months, not days. Week one is about tolerance, not transformation.
Weeks 2 through 4: what changes during your first month
The second, third, and fourth weeks on tirzepatide are where the medication starts to feel less like a foreign substance and more like something your body understands. Depending on your provider protocol, you stay at the 2.5 mg starting dose for 4 weeks before titrating to 5 mg. This gradual approach exists for a reason.
Week 2: the rhythm establishes itself
Your second injection introduces a dose into a system that already has residual tirzepatide from the first week. Drug levels are now building toward a more consistent baseline. This is where most people notice the clearest difference compared to week one.
Appetite suppression becomes more predictable. The "forgetting to eat" phenomenon shows up for the first time. You look at the clock at 2 PM and realize you never had lunch, not because you skipped it intentionally but because the hunger signal simply did not fire. This is GLP-1 receptor activation working as designed, reducing the hormonal hunger signals that drive food-seeking behavior.
Side effects from the first dose have usually resolved entirely by now. The second injection at 2.5 mg tends to produce fewer gastrointestinal effects than the first because your system has already adapted to the receptor activation. Some people report mild symptoms after their second injection, but they are typically milder and shorter-lived than the first round.
If your appetite has not changed noticeably by the end of week two, that does not mean the medication is not working. The timeline for appetite suppression varies significantly between individuals, and some people do not notice clear changes until they titrate to 5 mg or higher. Patience during this phase prevents the frustration that leads many people to abandon treatment prematurely.
Week 3: subtle body changes
Three weeks in, the scale may start to cooperate. Most people report 2 to 5 pounds of total weight loss by week three, though the range is wide. Some see more. Some see less. Body composition changes, like reduced bloating, slightly looser clothing, or feeling less puffy, often appear before the scale reflects significant fat loss.
This is also when food preferences begin shifting for many users. Cravings for highly processed, high-sugar, and high-fat foods often decrease noticeably. This is not willpower. It is neurochemistry. The GLP-1 receptor system directly influences reward pathways in the brain, and tirzepatide modulation of these pathways changes how your brain responds to food cues. Research participants in SURMOUNT trials reported reduced food cravings as one of the earliest and most consistent effects.
Energy levels often improve during week three compared to the initial adjustment period. Some users even report increased energy as reduced caloric intake paradoxically frees up metabolic resources that were previously devoted to processing excess food.
Week 4: preparing for your first dose increase
Week four is the final week at your starting dose. Your body has now had four full doses of 2.5 mg, and steady-state concentration at this dose level has been reached. This is the most adapted you will be at this dose level.
Most providers will increase your dose to 5 mg after completing four weeks at 2.5 mg. Some dose escalation protocols extend the 2.5 mg phase to 6 or even 8 weeks if side effects were significant during the initial month. Others may move to the next dose earlier if tolerance was excellent. Your provider will guide this decision based on your response.
By the end of month one, realistic expectations include total weight loss of 3 to 7 pounds (some more, some less), established appetite reduction at the starting dose level, resolved or minimal gastrointestinal side effects, a sense of how your body responds to the medication, and a baseline from which your provider can adjust dosing going forward.
If you want to see what longer timelines look like, real tirzepatide before and after results show the progressive changes that build over months of treatment. The first month creates the foundation. Months two through six build the visible results.
Common side effects and how to manage each one
Side effects are the part everyone worries about before their first dose. Let us break down each one with specific data, management strategies, and timelines so you know exactly what to expect and what to do about it.
Nausea
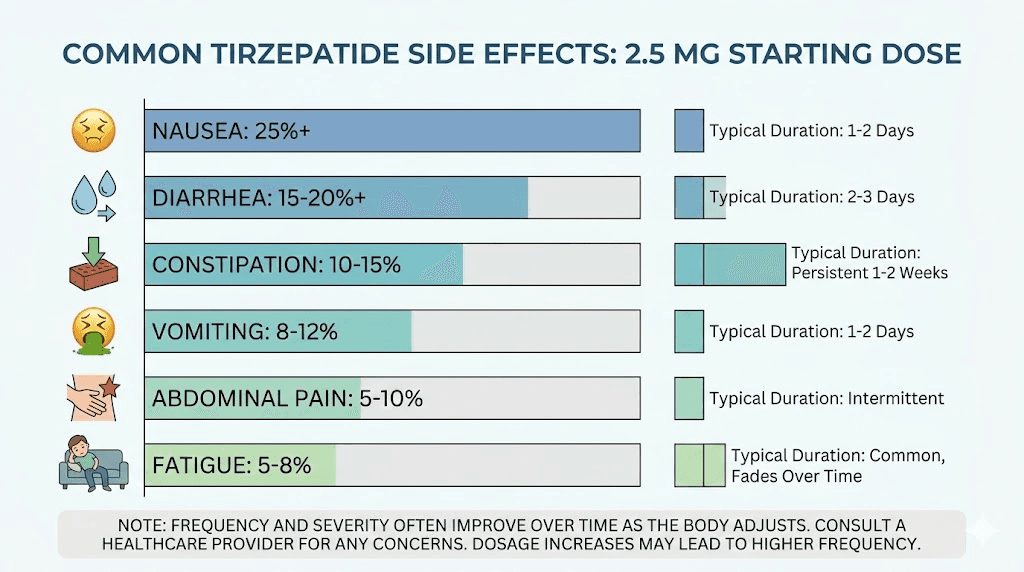
This is the most commonly reported side effect. In clinical trials, nausea affected approximately 12 to 18 percent of participants at the 2.5 mg starting dose, rising to 24 to 29 percent at higher therapeutic doses. At the starting dose, it is usually mild.
When it appears: typically 12 to 48 hours after injection, most intense during the first 2 to 3 days. Duration: 1 to 5 days for most people, resolving as the body adapts. Severity at starting dose: mild to moderate (functional, not debilitating).
Management strategies that work. Eat smaller, more frequent meals rather than three large ones. Choose bland, low-fat foods when nausea is active. Ginger tea, ginger capsules, or ginger chews can reduce symptoms by 20 to 40 percent based on antiemetic research. Avoid lying down immediately after eating; stay upright for at least 30 minutes. Stay aggressively hydrated since dehydration worsens nausea significantly. The foods to avoid on tirzepatide are primarily greasy, fried, and very rich items that sit heavy in a stomach with slowed emptying.
Decreased appetite
This is technically a desired effect, not a side effect. But many people experience it as unsettling during the first week because the change feels involuntary. Your brain simply stops sending hunger signals at the frequency it used to.
Important distinction: decreased appetite is not the same as food aversion. You can still eat. Food still tastes fine. You just do not feel driven to eat as often or as much. This is a critical difference from nausea-driven appetite loss, which feels unpleasant. The GLP-1 mediated appetite reduction should feel more like indifference to food than revulsion.
Still, eating adequately on tirzepatide matters. Undereating leads to muscle loss, nutrient deficiency, and metabolic slowdown. Aim for at least 1,200 calories daily (and often more depending on your size and activity level) even when your appetite is suppressed. Prioritize protein at every meal.
Fatigue and tiredness
Approximately 7 to 12 percent of first-dose users report fatigue that lasts 2 to 5 days. This can stem from reduced caloric intake, the metabolic adjustment to GIP/GLP-1 receptor activation, or disrupted sleep from digestive changes.
Management: maintain adequate calorie intake (undereating is the most common cause), stay hydrated, allow extra rest during the first week if possible, and consider taking your injection on a day where you can have a lighter schedule the following day. Most fatigue resolves by day 4 to 5.
Diarrhea
Affects roughly 12 to 17 percent of tirzepatide users across all doses. At the starting dose, incidence is lower. Diarrhea from tirzepatide typically appears within the first 48 hours and resolves within 3 to 5 days.
Management: avoid high-fiber foods temporarily, stay hydrated with electrolyte-containing fluids, eat binding foods like rice, bananas, and toast, and avoid dairy if it worsens symptoms. If diarrhea persists beyond 5 to 7 days, contact your provider.
Constipation
The opposite problem affects a similar percentage of users. Slowed gastric emptying can slow the entire digestive tract. Constipation treatment strategies include increasing water intake significantly, adding gentle fiber through foods or supplements, moderate physical activity (walking is surprisingly effective), and a stool softener if dietary changes are not enough.
Headaches
Reported by 5 to 10 percent of first-dose users. GLP-1 related headaches are typically mild to moderate and linked to dehydration, blood sugar changes, or reduced caffeine intake (since many people drink less coffee when their appetite decreases).
Quick fix: drink a full glass of water, eat something if you have gone more than 4 hours without food, and take your usual over-the-counter pain reliever if needed. Persistent headaches beyond 3 days warrant a call to your provider.
Injection site reactions
Injection site reactions occur in approximately 2 to 5 percent of tirzepatide users. Symptoms include redness, mild swelling, itching, or tenderness at the injection site. Most reactions are mild and self-limiting, resolving within 24 to 72 hours.
If your injection site becomes red and itchy, cold compresses for 10 to 15 minutes several times daily plus over-the-counter hydrocortisone cream typically resolve it. Rotating injection sites between abdomen, thigh, and upper arm with each weekly dose reduces recurrence. The complete injection site reaction treatment guide covers more severe scenarios.
Less common side effects
These affect smaller percentages of users but are worth knowing about. Dry mouth affects about 3 to 5 percent and responds well to increased hydration and sugar-free hard candies. Anxiety has been reported by some users, though it is difficult to separate from the anxiety of starting a new medication. Joint pain and muscle pain are reported by roughly 3 to 5 percent and typically resolve with standard over-the-counter anti-inflammatory medication. Insomnia or sleep disruption occurs in some users, particularly during the first 2 to 3 days after injection. Menstrual cycle changes have been reported by some women, likely related to hormonal shifts that accompany weight changes and metabolic alterations.
Across all of these, the pattern is the same. Starting dose side effects are milder than therapeutic dose side effects. They peak in the first 48 to 72 hours. They improve with each subsequent dose at the same level. And they are almost always manageable with simple strategies. The starting dose exists specifically to minimize this adjustment period.
What your first injection actually feels like
This section is for the needle-anxious. And there are a lot of you. Injection anxiety is one of the top reasons people delay starting GLP-1 medications, so let us walk through exactly what the experience involves.
The pre-filled pen experience
If you are using brand-name Mounjaro or Zepbound, you have a pre-filled autoinjector pen. You press it against your skin, click the button, and the device does the rest. The needle is hidden. You never see it. The injection takes about 5 to 10 seconds, and most people describe the sensation as a brief pinch or sting that rates about 1 to 2 on a 10-point pain scale. Some people feel nothing at all.
The needle gauge on the autoinjector is 31 gauge, which is among the thinnest available. For reference, that is thinner than the needles used for most blood draws. The pen needle is also very short, typically 4 to 5 mm, meaning it barely penetrates the subcutaneous layer.
The vial and syringe experience
If you are using compounded tirzepatide from a vial, the process requires manually drawing and injecting with a syringe. This sounds more intimidating than it is. With a proper syringe (typically 29 to 31 gauge insulin syringe), the injection itself feels identical to the autoinjector. The only difference is that you handle the drawing and injection yourself.
For compounded formulations, you will need to either reconstitute lyophilized powder with bacteriostatic water or use a pre-mixed liquid formulation. If reconstituting, follow your pharmacist instructions exactly, and our guide on how much bacteriostatic water to mix with tirzepatide walks through the math. Many compounded formulations come as lyophilized (freeze-dried) powder that requires reconstitution before injection.
Where to inject
Three FDA-approved injection sites: abdomen (at least 2 inches from the navel), front of the thigh (middle third), and back of the upper arm. Most people find the abdomen the easiest and least painful option for self-injection. The thigh is a close second. Upper arm is more difficult to self-inject and generally requires help from another person.
Rotate your injection site each week. Do not inject into the same spot repeatedly. This prevents lipodystrophy (tissue changes under the skin) and reduces the risk of injection site reactions. Our complete injection site guide covers the specific techniques for each location, and the general GLP-1 injection guide covers proper technique applicable to all injection-based medications in this class.
Practical first-injection tips
Let the medication reach room temperature for 15 to 30 minutes before injecting if it has been refrigerated. Cold medication stings more than room-temperature medication. Clean the injection site with alcohol and let it dry completely. Pinch the skin gently to create a fold of subcutaneous tissue. Insert the needle at a 90-degree angle for abdomen and thigh sites. Inject slowly and steadily. Hold the needle in place for 5 to 10 seconds after fully depressing the plunger to ensure complete delivery. Apply gentle pressure with a cotton ball or gauze after withdrawing. Do not rub the site.
That is it. The entire process takes under two minutes once you have done it a couple of times. Most people find that the anxiety beforehand is worse than the actual injection. By the third or fourth weekly injection, it becomes routine.
Appetite changes: the timeline from subtle to significant
Appetite suppression is why most people take tirzepatide. Understanding the realistic timeline prevents both premature disappointment and unrealistic expectations.
The first dose appetite effect
At 2.5 mg, appetite suppression ranges from barely noticeable to moderately significant depending on the individual. About 30 to 40 percent of first-dose users report noticeable appetite reduction within the first week. Another 30 percent notice subtle changes that they only recognize in retrospect. And the remaining 30 percent feel essentially no appetite change at the starting dose.
All three responses are normal. The 2.5 mg dose is not designed to produce powerful appetite suppression. It is designed to introduce your body to the medication with minimal disruption. Expecting dramatic hunger elimination at this dose sets you up for disappointment.
That said, even at 2.5 mg, some people experience what researchers call "food noise reduction." The constant background chatter about food, the planning of the next meal, the pull toward the pantry, all of it quiets. Not silences. Quiets. This is often the first sign that the medication is working even before the scale moves.
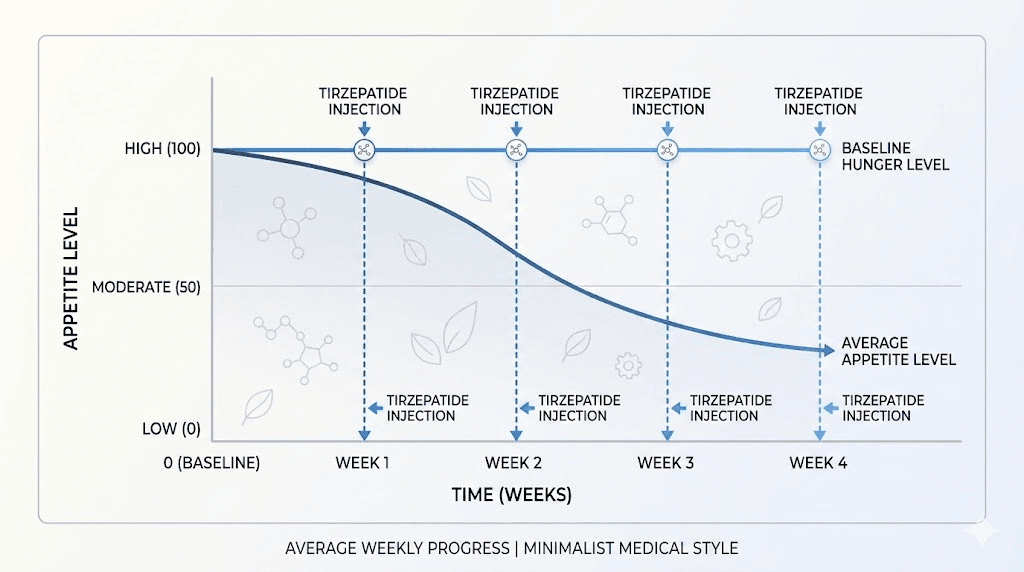
How appetite builds over the first month
With each weekly dose, drug concentration builds. By week two at 2.5 mg, appetite suppression is typically more consistent than week one. By week three, most people have established a new baseline for hunger and satiety. By week four, the starting dose effect has stabilized.
The jump to 5 mg at week five (for most protocols) is where many people experience a significant increase in appetite suppression. This is the dose where "forgetting to eat" becomes common, where portion sizes shrink noticeably, and where the relationship with food begins its most visible shift.
If you followed the experience of someone on semaglutide, the first week pattern is remarkably similar, though tirzepatide dual-receptor activation often produces stronger appetite effects at equivalent dose escalation points. The semaglutide appetite suppression timeline provides an interesting comparison for those who have experience with both medications.
What appetite suppression actually feels like
People describe it differently. "Like I ate a big meal even though I did not." "I just stop thinking about food." "I can take it or leave it." "I see cake and feel nothing." "I eat half my plate and I am done."
The common thread is indifference rather than aversion. The medication does not make food disgusting. It does not make eating unpleasant (nausea aside, which is a separate mechanism). It simply turns down the volume on the hunger signal. You still enjoy food when you eat it. You just do not need as much of it, and you do not think about it between meals.
This distinction matters because some people expect to hate food on tirzepatide. If that happens, it is more likely a nausea response than an appetite response, and the two should be addressed differently. Nausea-driven food avoidance needs management. Appetite-mediated portion reduction is the medication working as designed.
Eating on tirzepatide: what works after your first dose
What you eat in the first few days and weeks can significantly impact how you feel. The medication changes your digestive speed and capacity. Your eating strategy needs to change with it.
First 48 hours eating strategy
Keep it simple. Smaller portions. Bland-ish foods. Nothing deep-fried or heavily processed. Think grilled chicken and vegetables rather than a cheeseburger and fries. Not because you can never eat those foods again, but because your slowed gastric emptying will punish heavy, fatty meals with prolonged discomfort.
Good first-48-hour foods include lean proteins (chicken, fish, turkey), cooked vegetables (easier to digest than raw), rice or potatoes (simple carbs that sit light), broth-based soups (hydrating and easy to digest), and crackers or toast (helpful if nausea is present).
The first week meal framework
As your body adjusts, you can expand your food choices. But the core principles remain consistent throughout tirzepatide treatment. Protein first, always. Aim for 25 to 30 grams of protein per meal. When your appetite is reduced, every calorie matters, and protein protects muscle mass during weight loss. Without adequate protein, your body will break down muscle along with fat, which wrecks your metabolism long-term.
Our complete guide on foods to avoid on tirzepatide covers the specific items most likely to trigger nausea and digestive distress. The short version: fried foods, extremely fatty meals, carbonated beverages, very spicy foods, and large volumes of food eaten quickly.
A structured tirzepatide diet plan or meal plan can be helpful during the adjustment period because it removes decision-making when your appetite signals are confusing. You do not have to follow a strict plan forever. But having one during weeks one through four provides structure while you figure out your new hunger patterns.
Hydration is non-negotiable
This cannot be overstated. Dehydration is the single most common amplifier of tirzepatide side effects. Nausea worse than expected? Probably dehydrated. Headaches? Likely dehydration. Fatigue? Could be dehydration. Constipation? Almost certainly dehydration playing a role.
Minimum 64 ounces of water daily. More if you weigh over 200 pounds or are physically active. Set timers if you have to. Carry a water bottle everywhere. Add electrolytes if plain water feels unsatisfying. This one habit prevents more first-dose misery than any other single intervention.
Supplements worth considering
The supplements to take with tirzepatide discussion comes up frequently among new users. A few evidence-supported options include a high-quality multivitamin (reduced food intake means reduced micronutrient intake), a fiber supplement if constipation develops, a probiotic to support gut health during the digestive adjustment, and ginger supplements for nausea management. Many compounded formulations already include B12, glycine, or other additions designed to support the weight loss process. If your formulation includes glycine and B12, additional supplementation of those specific nutrients may not be necessary.
Alcohol and your first dose
Drinking alcohol on tirzepatide deserves its own mention. The combination is not dangerous, but it is not ideal during the first week. Alcohol is absorbed more slowly when gastric emptying is delayed, which means it hits harder and lasts longer than you might expect. Many people report feeling effects from less alcohol than usual. Additionally, alcohol irritates the stomach lining and can worsen nausea. The reasonable advice is to avoid alcohol for the first week while you figure out how your body responds, then reintroduce it cautiously in small amounts.
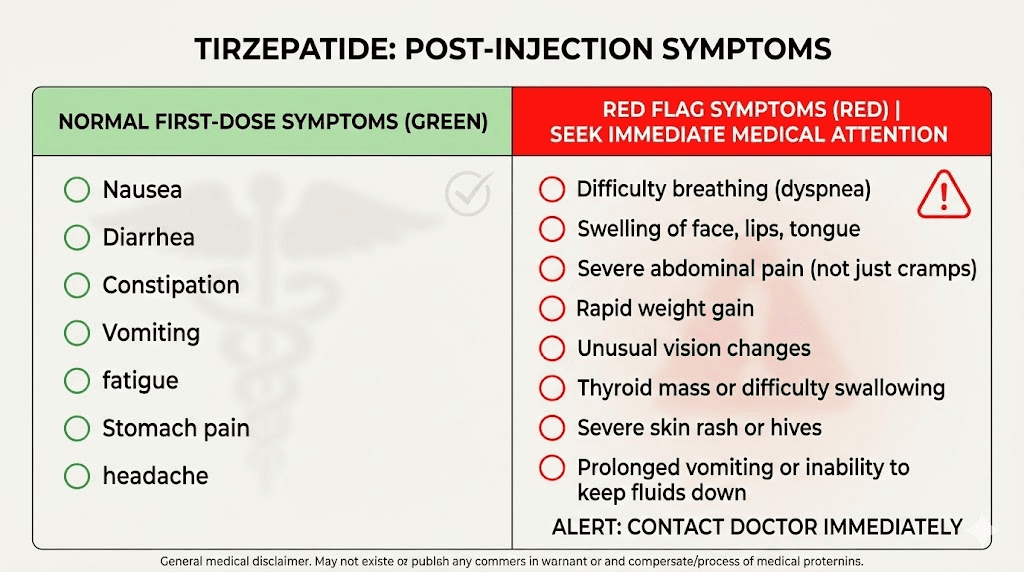
When something feels wrong: red flags vs normal adjustment
The anxiety of starting a new medication makes every sensation feel significant. It helps to know which symptoms are normal adjustment responses and which warrant medical attention.
Normal (do not panic)
Mild to moderate nausea that comes and goes for 1 to 5 days. Reduced appetite that feels unusual but not distressing. Mild fatigue for 2 to 4 days. One or two episodes of loose stool or mild constipation. A mild headache. Slight injection site redness that resolves within 24 hours. Feeling "off" or "different" without specific symptoms. Burping more than usual (slowed gastric emptying produces more gas). Feeling full from small amounts of food.
All of these are within the expected adjustment spectrum and typically resolve without intervention.
Contact your provider
Severe nausea that prevents you from keeping any food or fluids down for more than 24 hours. Vomiting more than 2 to 3 times in a single day. Severe abdominal pain (not just discomfort, actual pain that is hard to ignore). Signs of dehydration: dark urine, dizziness upon standing, dry mouth that does not improve with drinking. Persistent diarrhea lasting more than 5 to 7 days. Injection site reaction that spreads, worsens, or produces warmth/fever. Jaundice (yellowing of skin or eyes, which could indicate a rare pancreatic issue). Signs of allergic reaction: hives, difficulty breathing, facial swelling. Chest pain or heart palpitations.
These are uncommon, especially at the 2.5 mg starting dose, but they warrant prompt medical evaluation.
The pancreatitis question
Many first-dose users worry about pancreatitis because it appears in the tirzepatide safety information. The reality: pancreatitis is rare. In SURMOUNT-1, the incidence was less than 0.2 percent. Symptoms include severe, persistent upper abdominal pain that radiates to the back, accompanied by nausea and vomiting. Mild stomach discomfort after eating is not pancreatitis. The crampy, gassy, "my stomach is adjusting" feeling is not pancreatitis. If you experience severe, unrelenting abdominal pain, seek immediate medical attention. Otherwise, garden-variety digestive adjustment at the starting dose is overwhelmingly more likely.
Special populations
A few groups should approach the first dose with extra awareness. Anyone with a history of thyroid cancer or multiple endocrine neoplasia type 2 should discuss risks with their endocrinologist. People with a history of pancreatitis need closer monitoring. Those with BMI considerations at the lower end of the qualifying range may experience stronger effects at the starting dose. Women who are pregnant or could become pregnant should know that tirzepatide is not recommended during pregnancy, and some women have reported unexpected pregnancies on tirzepatide due to GLP-1 medications potentially increasing fertility. If you are breastfeeding, discuss the risks and benefits with your provider before starting.
What experienced tirzepatide users wish they knew on day one
After tracking member experiences at SeekPeptides, several consistent themes emerge from people looking back at their first dose.
The scale is a liar in week one
Weight fluctuates 2 to 5 pounds daily based on hydration, sodium intake, gut content, and hormonal cycles. Weighing yourself daily in the first week produces anxiety, not data. The recommendation from experienced users: weigh yourself once per week, same day, same time, same conditions (morning, after bathroom, before food). Trend lines over weeks matter. Individual daily readings do not.
Your second dose is not your first dose
Many people expect each subsequent dose to feel like the first. It does not. As drug levels build and your body adapts, the weekly injection pattern becomes smoother. Side effects that appeared after dose one often do not recur at the same dose level. The real adjustment happens at each new dose tier (2.5 to 5 mg, 5 to 7.5 mg, and so on), not every single weekly injection.
Stock your kitchen before day one
Having the right foods on hand when nausea or appetite changes hit makes an enormous difference. Stock up on lean proteins, easy-to-digest carbs, ginger products, electrolyte drinks, and light soups before your first injection. You do not want to be figuring out what to eat when you feel queasy. Have a plan ready.
Take your first dose on a Friday
If possible, time your first injection for a Friday afternoon or evening. This gives you the weekend to experience peak drug levels and any initial side effects without work obligations. If day 2 hits you with fatigue or nausea, you have the flexibility to rest. Many experienced users consider this the single most practical tip for first-dose success.
Protein intake is non-negotiable
The most regretted mistake among experienced users is not eating enough protein during the early weeks. When appetite drops, it is easy to eat whatever sounds tolerable rather than what your body needs. But inadequate protein intake leads to muscle loss, which reduces metabolic rate, which undermines the entire purpose of the medication. Target 0.7 to 1.0 grams of protein per pound of body weight daily. Protein shakes become essential for many people who cannot eat large protein portions.
Storage matters from day one
Whether you are using a pre-filled pen or a compounded vial, proper refrigeration is essential. Tirzepatide should be stored at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Compounded vials have specific shelf life requirements that differ from brand-name products. If your medication gets warm or is left out overnight, you need to know the stability guidelines. And if the color of your medication looks off, do not inject it until you have verified it is safe.
Walking is the best first-week exercise
Intense workouts on day one of tirzepatide are not a great idea. But walking is. Moderate walking (20 to 30 minutes daily) improves digestion, reduces nausea, prevents constipation, supports mood, and gently boosts calorie expenditure without taxing a body that is adjusting to a new medication. Start with walking. Add intensity as your body acclimates.
Track everything
Food intake, water intake, side effects, weight (weekly), injection site, and injection time. This data becomes invaluable at your follow-up appointment and helps your provider optimize your dosing protocol. It also helps you identify patterns, like which foods trigger nausea or which injection site produces the fewest side effects.
Compounded vs brand-name: does it change what you expect?
The first-dose experience varies slightly depending on which formulation you are using. Understanding these differences prevents confusion.
Brand-name (Mounjaro, Zepbound)
Pre-filled autoinjector pens. Exact 2.5 mg starting dose. Consistent formulation. The experience follows the clinical trial data most closely because the clinical trials used this exact formulation. Storage in the refrigerator, but can be kept at room temperature (up to 86 degrees Fahrenheit) for up to 21 days.
Compounded formulations
Compounded tirzepatide comes in various concentrations and formulations. Some include additional ingredients like vitamin B12, glycine and B12, vitamin B6, methylcobalamin, or levocarnitine. These additions can slightly modify the first-dose experience.
B12-containing formulations sometimes produce a mild energy boost that pure tirzepatide does not. Glycine-containing formulations may provide slightly better GI tolerability for some users. Niacinamide formulations offer their own potential benefits. The core tirzepatide effects remain the same regardless of these additions.
Compounded formulations require careful dosage calculation because concentrations vary. A 10 mg/mL vial requires different unit math than a 20 mg/mL vial. Understanding how many units equal your starting dose at your specific concentration is critical. Getting this wrong means getting the wrong dose, which changes everything about what you experience.
Expiration dates for compounded formulations are typically shorter than brand-name products, and shelf life depends on whether the vial is reconstituted or pre-mixed. These details matter for your first dose and every dose after.
Oral and alternative forms
Tirzepatide also exists in oral formulations, including tablets, sublingual drops, and orally disintegrating tablets. The first-dose experience with oral forms differs from injectable in terms of onset timing, bioavailability, and side effect profile. If you are using an oral form, the timelines in this guide may need adjustment since absorption kinetics are different.
How tirzepatide compares to other first-dose experiences
If you have taken other GLP-1 medications before, or are deciding between options, understanding comparative first-dose experiences helps set expectations.
Tirzepatide vs semaglutide first dose
The most common comparison. Semaglutide (Ozempic, Wegovy) is a pure GLP-1 receptor agonist. Tirzepatide activates both GIP and GLP-1 receptors. In practice, this means tirzepatide often produces slightly less nausea at equivalent dose escalation points (thanks to the GIP component), potentially stronger appetite suppression once doses reach therapeutic levels, and additional metabolic benefits that semaglutide does not provide.
People who switch from tirzepatide to semaglutide or vice versa often notice differences in the quality of appetite suppression. The side effect profiles differ subtly, with some people tolerating one better than the other. If you have experience with your first week on semaglutide, expect a broadly similar trajectory with tirzepatide, adjusted for the dual-agonist mechanism.
Tirzepatide vs newer options
For those researching all available options, CagriSema, orforglipron, mazdutide, and retatrutide each represent different approaches to incretin-based weight management. The complete three-way comparison between semaglutide, tirzepatide, and retatrutide covers how these medications differ in mechanism, efficacy, and side effect profiles. Tirzepatide remains one of the most well-studied and widely prescribed options, with the most robust clinical trial data for both diabetes and weight management.
Month two and beyond: what comes next
Your first dose is one step in a longer journey. Understanding what comes after helps you plan and set realistic expectations.
Dose escalation timeline
The standard tirzepatide dose escalation moves from 2.5 mg to 5 mg after 4 weeks, then to 7.5 mg after another 4 weeks, then to 10 mg, potentially up to 15 mg. Each increase brings a mini adjustment period. The complete dosing chart shows the standard escalation schedule, but your provider may customize this based on your response.
Each dose increase typically produces a brief return of mild side effects (1 to 3 days), followed by enhanced appetite suppression. This "mini first-dose experience" at each new level is normal and expected. It is also shorter and milder than your actual first dose because your body already understands GIP/GLP-1 receptor activation.
Some people find that microdosing approaches or splitting doses help smooth out the transition between dose levels. These strategies can reduce the intensity of dose-increase side effects, though they should be discussed with your provider.
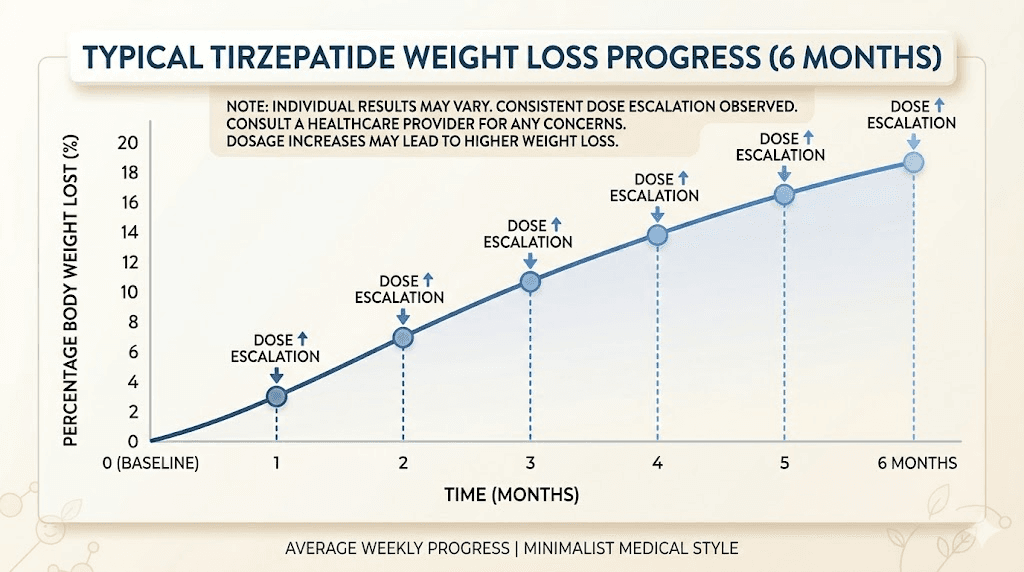
When weight loss becomes visible
Clinical data shows that most people begin seeing noticeable weight loss results between weeks 4 and 12. The week-by-week weight loss timeline shows that the curve accelerates as doses increase. By month three, most people on therapeutic doses have lost 5 to 10 percent of their starting body weight.
Before and after results from real users show the progressive changes that build over months. The transformation is rarely dramatic in any single week. It accumulates. And that accumulation is what makes the first month of patience so important.
What if it does not seem to work?
If you reach week four with no appetite changes and no weight loss, do not panic. The 2.5 mg dose is below the therapeutic range for weight management. It is a starting dose, not a treatment dose. Many people who feel nothing at 2.5 mg experience clear effects at 5 or 7.5 mg. If you are still seeing no response at 10 mg, that warrants a conversation with your provider about dose optimization, formulation changes, or alternative approaches.
Our guides on tirzepatide not working and why you might not be losing weight on tirzepatide cover the full troubleshooting process for each scenario.
Long-term planning
Tirzepatide is not a short-term fix. Research indicates that discontinuing GLP-1 medications after achieving weight loss goals often leads to weight regain. The conversation about maintaining weight loss after tirzepatide and potentially tapering off the medication is one to have with your provider well before you reach your goal weight.
Some people transition to lower maintenance doses. Others switch to different medications based on evolving needs. A few successfully discontinue and maintain results through lifestyle changes alone. There is no one-size-fits-all exit strategy, but having a plan is far better than stopping abruptly and hoping for the best.
Practical first-dose checklist
Before your first injection, have these items ready and these actions completed.
Supplies: Medication (properly stored), alcohol swabs, cotton balls or gauze, sharps container for needle disposal, and if using a vial, syringes and bacteriostatic water if reconstitution is needed.
Kitchen: Lean proteins, plain crackers, ginger products (tea, chews, capsules), electrolyte drinks, broth or soup, bananas, rice, and plenty of water.
Schedule: First injection timed so that days 2 and 3 fall on low-obligation days. Follow-up appointment scheduled for 4 to 6 weeks out. Weekly reminder set for same-day, same-time injections.
Knowledge: You understand that the starting dose is a calibration dose, not a treatment dose. You know the common side effects and have management strategies ready. You know the red flags that require medical attention. You know that weight loss at this dose is minimal and patience is required. And you know that SeekPeptides provides ongoing protocol support, tracking tools, and community insights for every phase of the tirzepatide journey.
Tracking: A simple journal or app to record injection date, time, site, any side effects, food intake, water intake, and weekly weight. This data drives better outcomes. Use the tirzepatide vs semaglutide comparison tools and dosage calculators available on the site to support your calculations and comparisons.
Frequently asked questions
How quickly will I lose weight after my first tirzepatide dose?
Most people lose 0 to 3 pounds in the first week, primarily from reduced food intake and water changes rather than fat loss. Meaningful fat loss typically begins between weeks 4 and 12 as doses increase to therapeutic levels. Clinical trials show average weight loss of 3 to 7 percent of body weight by week 12, with the full timeline extending over months.
Is it normal to feel nothing after my first injection?
Completely normal. The 2.5 mg starting dose produces noticeable effects in roughly 30 to 60 percent of people during the first week. The remaining 40 to 70 percent feel minimal or no changes until the dose increases to 5 mg or higher. The starting dose is intentionally low to build tolerance, not to produce dramatic effects.
Should I eat before or after my injection?
There is no strict requirement either way. Some providers recommend eating a light meal before your injection to reduce the chance of nausea on an empty stomach. Others say it does not matter. What most experienced users recommend: eat a normal meal 1 to 2 hours before your injection so you are neither full nor hungry when the medication enters your system. Check the best time to take your GLP-1 shot for more timing guidance.
Can I exercise after my first dose?
Light to moderate exercise is fine. Intense training is better saved for after you know how the medication affects you. Walking, yoga, and gentle cycling are great first-week activities. Heavy lifting, HIIT, and long runs can wait until you have established how your body responds to the medication, particularly regarding energy levels and digestive comfort.
What if I get severe nausea?
Severe nausea at the 2.5 mg starting dose is uncommon but possible. If it prevents you from eating or drinking for more than 24 hours, contact your provider. They may prescribe anti-nausea medication (ondansetron is commonly used), adjust your dosing schedule, or recommend staying at 2.5 mg for an extended period before increasing.
How long do first-dose side effects last?
The majority of first-dose side effects resolve within 3 to 5 days. Some people experience effects for up to 7 days. If any side effect persists beyond 7 days at the starting dose, discuss it with your provider. The comparative side effect guide provides detailed duration data across different GLP-1 medications.
Can I drink coffee on tirzepatide?
Yes. Coffee is not contraindicated with tirzepatide. However, caffeine on an empty stomach can worsen nausea, and some people find that their coffee tolerance decreases when their appetite is suppressed (less food in the stomach means more caffeine sensitivity). Start with your normal amount and adjust if you notice increased jitteriness or stomach upset.
What should my injection site look like afterward?
Normal: a small red dot that fades within hours, slight tenderness when pressed, no visible mark by the next day. Mildly concerning but usually fine: a small bruise (common with thigh injections), mild redness that lasts 12 to 24 hours, slight itching. Requires attention: spreading redness, significant swelling, warmth radiating from the site, or any reaction that worsens rather than improves over 24 hours. See the complete injection site reaction guide for detailed assessment criteria.
External resources
Mayo Clinic: Tirzepatide (subcutaneous route) - Side effects and dosage
Cleveland Clinic: Tirzepatide (Mounjaro) - How it works and side effects
PMC: The role of tirzepatide in type 2 diabetes management (SURPASS clinical trials)
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed dosing calculators, side effect management databases, and the kind of peer support that turns a confusing first-dose experience into a confident treatment journey.
In case I do not see you, good afternoon, good evening, and good night. May your first dose go smoothly, your side effects stay mild, and your results exceed every expectation.