Feb 27, 2026

You are doing everything right. You got the prescription. You started the injections. You stuck with the schedule, marked the calendar, rotated the injection sites, and waited. But the hunger is still there. That gnawing, persistent feeling that was supposed to disappear weeks ago refuses to leave. And the frustration is starting to outweigh the optimism.
You are not imagining it. And you are not alone.
Thousands of people starting tirzepatide experience the same confusion. The clinical trials promised dramatic weight loss and powerful appetite suppression. Friends or forum posts paint pictures of food becoming an afterthought. Yet here you are, staring at an empty plate and wanting more. The disconnect between expectations and reality can feel isolating, even defeating. But persistent hunger on tirzepatide does not mean the medication has failed you or that your body is broken. In the vast majority of cases, it means something specific and fixable is going on behind the scenes. Maybe your dose has not reached the therapeutic window yet. Maybe your diet composition is working against the medication rather than with it. Maybe the timing, the hydration, or even the sleep patterns are quietly undermining every injection.
This guide breaks down the nine most common reasons people stay hungry on tirzepatide, what the research actually says about appetite suppression timelines, and the specific changes that turn the medication from disappointing into transformative. No vague advice. No generic "eat less" platitudes. Just the mechanisms, the data, and the practical fixes.
How tirzepatide actually controls your appetite
Before troubleshooting why hunger persists, you need to understand what tirzepatide is supposed to do and how it does it. The mechanism matters because it reveals exactly where the process can break down.
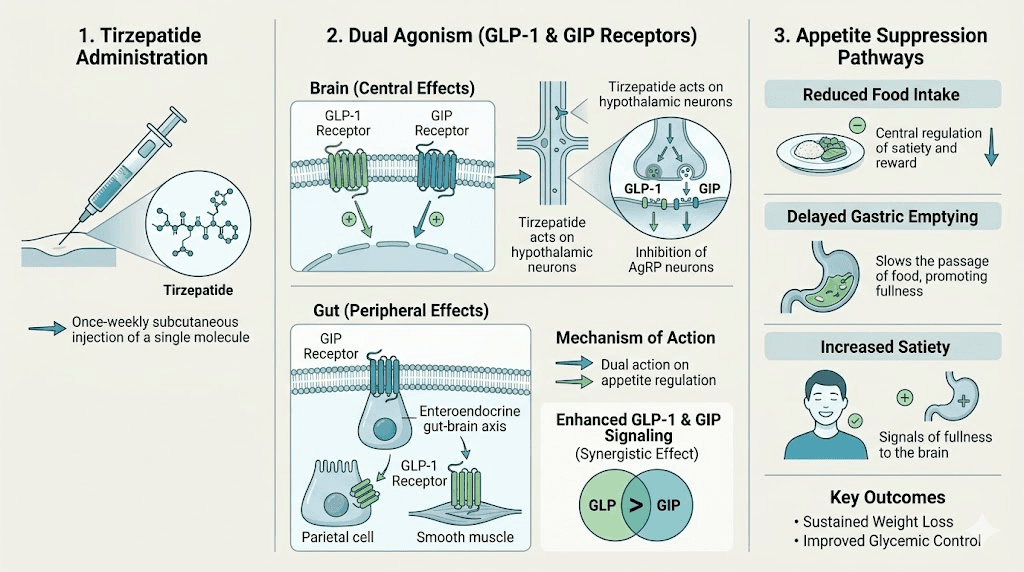
Tirzepatide is a dual agonist. That means it activates two different receptor systems simultaneously: GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide). Most weight loss peptides only target one of these. Tirzepatide targets both, and that dual action is precisely why it outperforms single-target medications in clinical trials.
Here is what happens after each injection.
GLP-1 receptor activation slows gastric emptying. Food sits in your stomach longer, which sends prolonged fullness signals to your brain. Simultaneously, GLP-1 acts directly on the hypothalamus, the brain region that regulates hunger and satiety. It turns down the volume on ghrelin (your hunger hormone) and amplifies signals from peptide YY and other satiety messengers. The result, when everything works properly, is that you simply do not think about food as often.
GIP receptor activation adds another layer. Research published in Diabetes journals shows that GIP agonism in the central nervous system independently suppresses appetite while also reducing the nausea that pure GLP-1 agonists sometimes cause. This is why many people tolerate tirzepatide better than semaglutide from a side effect standpoint, even though tirzepatide produces greater weight loss results.
The SURMOUNT-1 trial, published in the New England Journal of Medicine, found that tirzepatide reduced daily caloric intake by approximately 350 to 600 calories compared to placebo. Participants reported meaningful decreases in hunger, food cravings, and the anticipation of eating. These were not subtle changes. At the 15mg maintenance dose, participants lost an average of 22.5% of their body weight over 72 weeks.
But here is the part nobody emphasizes enough: those results came at maintenance doses, after a full 20-week escalation period. The starting dose of 2.5mg is not a therapeutic dose for appetite suppression. It is a tolerability dose designed to let your gut and brain adjust to the medication. If you are in the first 8 to 12 weeks, the appetite suppression machinery may not have fully engaged yet.
The 9 reasons you are still hungry on tirzepatide
Not all hunger on tirzepatide comes from the same place. Some causes are medication-related. Others are dietary. A few are psychological. Understanding which category your hunger falls into changes the solution entirely.
1. Your dose has not reached therapeutic levels yet
This is the most common reason, and it is the one that catches people off guard the most.
Tirzepatide follows a strict dose escalation schedule. You start at 2.5mg for four weeks. Then you move to 5mg for four weeks. Then 7.5mg. Then 10mg. Then 12.5mg. Then 15mg. The full escalation takes approximately 20 weeks if you increase on schedule at each step.
At 2.5mg and even 5mg, many people feel little to no appetite change. This is normal. The receptors need a certain level of activation before appetite suppression becomes consistent and reliable. Think of it like adjusting the volume dial slowly rather than flipping a switch. At lower doses, the signal is there but faint. At higher doses, it becomes impossible to ignore.
The SURMOUNT trials used maintenance doses of 5mg, 10mg, and 15mg. The most dramatic appetite suppression and weight loss occurred at 10mg and 15mg. If you are currently at 2.5mg or 5mg and feeling frustrated, the medication is working exactly as designed. Your body is acclimating. The appetite changes are coming.
What to do: Be patient through the escalation. Track your dosage in units carefully, follow the schedule your prescriber set, and do not expect dramatic appetite changes until you reach at least 7.5mg to 10mg. If your provider uses compounded tirzepatide, make sure you understand the exact concentration and dosing chart for your specific vial.
2. You have not given it enough time
Even at an adequate dose, tirzepatide does not flip a switch overnight.
The medication has a half-life of approximately 5 days, which means it takes several weeks at any given dose for blood levels to reach steady state. Clinical data suggests that appetite suppression typically becomes noticeable between weeks 4 and 8 at a stable dose, with full effects potentially taking 12 or more weeks to manifest.
This timeline surprises people. Social media is filled with "Week 1 on tirzepatide" posts from early responders who lost their appetite immediately. These are real experiences, but they represent one end of the response spectrum. The other end includes people who do not notice significant appetite changes until they have been at their target dose for two to three months.
Research from the SURMOUNT-3 trial showed that weight loss continued to accelerate between weeks 12 and 36, suggesting that the metabolic and appetite-related effects deepen well beyond the initial dose escalation period. How fast tirzepatide works varies enormously from person to person.
What to do: Give each dose at least 4 full weeks before evaluating its effect on your appetite. Keep a simple hunger journal, rating your hunger from 1 to 10 at meals, so you can spot subtle trends that your memory might miss. Sometimes appetite is decreasing gradually without you realizing it because the change is so incremental.
3. Your protein intake is falling short
This one is enormous. And it is the factor most people underestimate.
Tirzepatide slows gastric emptying and reduces appetite hormones, but it cannot override the satiety impact of what you actually eat. If your meals are heavy on refined carbohydrates and light on protein, you will feel hungry again sooner, regardless of what dose you are taking.
Protein is the most satiating macronutrient. It triggers the release of peptide YY and GLP-1 from your gut (yes, the same hormone tirzepatide mimics), which means high-protein meals amplify the medication effect. Studies show that high-protein diets produce approximately 50% greater feelings of fullness compared to standard diets. One clinical trial found that participants consuming 1.2 grams of protein per kilogram of body weight daily reported significantly less hunger and better weight loss outcomes than those eating 0.8 grams per kilogram.
For someone weighing 200 pounds (90kg), that means aiming for 90 to 108 grams of protein daily. Most people on tirzepatide are eating far less than that, especially as their overall food intake decreases.
What to do: Track your protein for one week. Use a simple app or even a notebook. Aim for protein at every meal, targeting 25 to 35 grams per sitting. Good sources include eggs, Greek yogurt, chicken breast, fish, cottage cheese, and whey protein. Check our guide on what to eat on tirzepatide for specific meal ideas that maximize satiety while keeping portions manageable. The tirzepatide diet plan we have created can serve as a starting framework.
4. You are not eating enough fiber
Fiber works differently from protein, but the satiety effect is equally powerful.
Soluble fiber absorbs water in your digestive tract and forms a gel-like substance that slows digestion further. This complements the gastric emptying delay that tirzepatide already provides. Together, they create a prolonged feeling of fullness that pure calorie restriction alone cannot match.
The recommended daily fiber intake is 25 to 30 grams. Most adults eat between 10 and 15 grams. That gap is significant. Without adequate fiber, food moves through your system faster, blood sugar spikes and crashes more dramatically, and hunger returns sooner after meals.
Foods rich in soluble fiber include oats, lentils, beans, flaxseeds, Brussels sprouts, avocados, and sweet potatoes. Including one or two of these at each meal can meaningfully extend the window between hunger episodes.
What to do: Add fiber gradually. A sudden increase can cause constipation or digestive discomfort, which is already a concern with tirzepatide. Start with an extra serving of vegetables at lunch and dinner, then add legumes or whole grains over the following weeks. Pair fiber increases with adequate water intake, which leads to the next point.
5. You are dehydrated and confusing thirst for hunger
This sounds too simple to be a real factor. It is not.
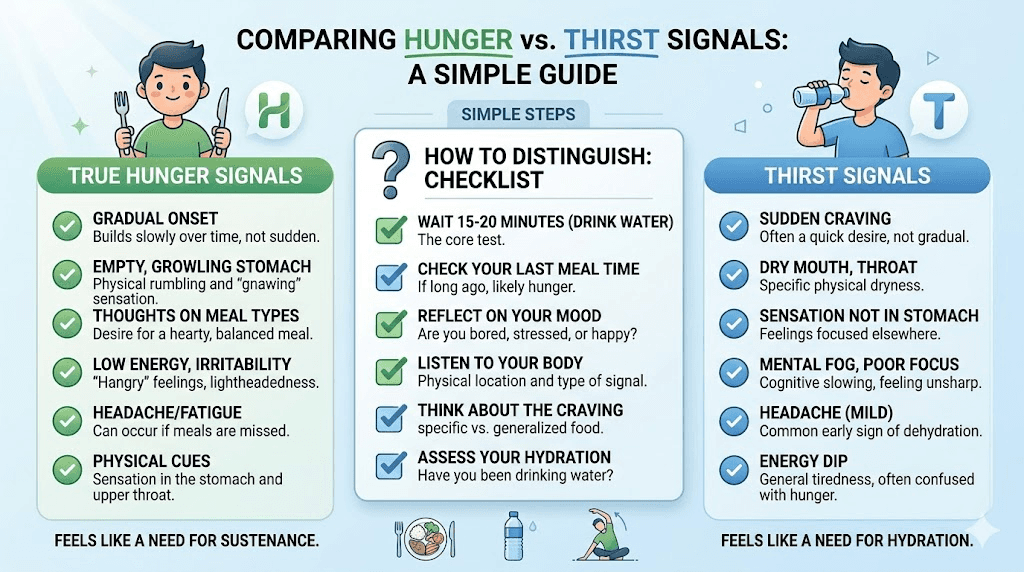
The human brain processes thirst and hunger signals through overlapping neural pathways in the hypothalamus. When you are mildly dehydrated, your body can send signals that feel exactly like hunger. You eat when you actually need water. The food temporarily satisfies the signal, but the underlying dehydration persists, and the false hunger returns within an hour.
Tirzepatide makes this worse. The medication can reduce thirst perception in some people, and the gastrointestinal side effects (nausea, constipation) can further decrease fluid intake. If you are not consciously drinking water throughout the day, you may be chronically mildly dehydrated without realizing it.
General hydration guidelines suggest approximately 91 ounces (2.7 liters) of total daily water intake for women and 125 ounces (3.7 liters) for men. These numbers include water from food, but if you are eating less food due to tirzepatide, your dietary water intake drops and your drinking water needs increase.
What to do: Before reaching for food between meals, drink 16 ounces of water and wait 15 minutes. If the hunger fades, it was thirst. Track your water intake for a few days to see where you actually stand. Aim for at least 8 to 10 glasses of plain water daily, more if you exercise or live in a warm climate. Electrolyte supplementation can also help with hydration quality, not just quantity.
6. Poor sleep is sabotaging your appetite signals
Sleep deprivation is one of the most powerful appetite stimulators known to science. And it has nothing to do with willpower.
When you sleep fewer than 7 hours, your body increases ghrelin production (the hunger hormone) by approximately 15% and decreases leptin production (the satiety hormone) by a similar amount. This hormonal shift creates genuine, biological hunger that even tirzepatide may not fully counteract. One night of poor sleep increases caloric intake by an average of 385 calories the following day, according to a meta-analysis published in the European Journal of Clinical Nutrition.
Tirzepatide itself can sometimes contribute to sleep disruption. Some users report insomnia or restless sleep, particularly during dose escalation. If the medication is affecting your sleep quality, it could be indirectly fueling the very hunger it is supposed to suppress.
What to do: Prioritize 7 to 9 hours of sleep per night. This is not a luxury. It is a metabolic requirement. If tirzepatide is disrupting your sleep, discuss timing adjustments with your prescriber. Some people find that switching their injection day or time of day improves sleep quality. Also consider basic sleep hygiene: consistent bedtime, cool room temperature, no screens for 30 minutes before bed, and limiting caffeine after noon.
7. Stress and emotional eating are overriding the medication
Tirzepatide addresses physical hunger signals. It reduces ghrelin. It slows gastric emptying. It tells your hypothalamus that you are full.
It does not address emotional hunger.
Emotional eating operates through entirely different brain pathways, primarily the dopamine reward system and the amygdala stress response. When you reach for food because you are anxious, bored, lonely, or stressed, those cravings come from a place that tirzepatide was never designed to reach. The medication may reduce the intensity of these cravings slightly (some dual agonist research suggests modest effects on food reward pathways), but it cannot eliminate decades of learned behavioral patterns.
If you have historically used food as comfort, stress relief, or boredom management, those patterns will persist even as physical hunger decreases. You might find yourself eating without being physically hungry, then wondering why tirzepatide is not working. It is working. The hunger you are experiencing is not the kind it treats.
What to do: Start noticing when you eat and why. Before reaching for food, pause and ask: Am I physically hungry, or am I reacting to an emotion? Physical hunger builds gradually, is satisfied by any food, and resolves with eating. Emotional hunger appears suddenly, craves specific comfort foods, and does not go away after eating. If emotional eating is a significant pattern, consider working with a therapist who specializes in cognitive behavioral therapy for eating behaviors. This is not weakness. It is addressing a different part of the problem that medication alone cannot solve.
8. Your body has adapted to weight loss
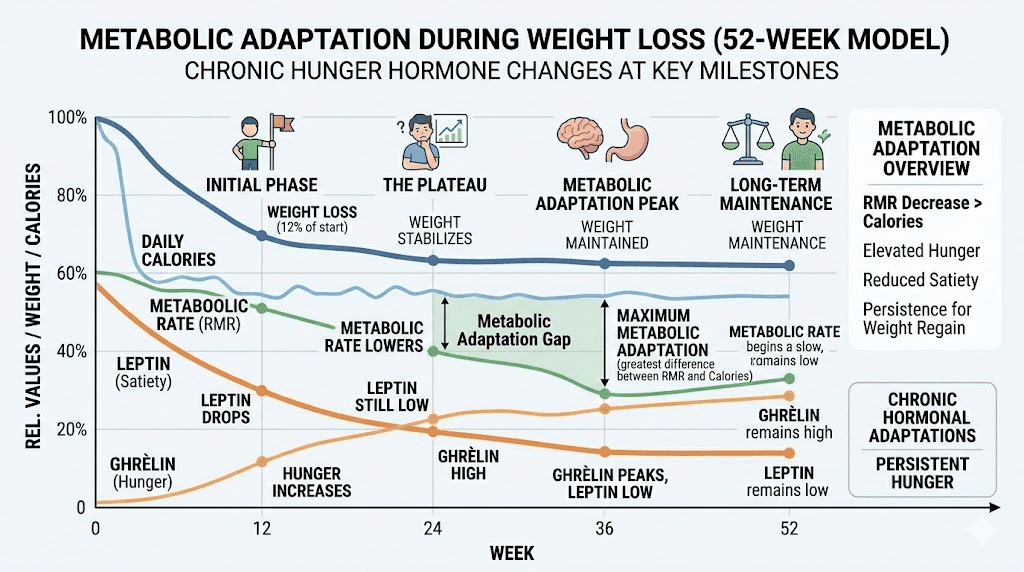
Metabolic adaptation is real, predictable, and completely normal.
As you lose weight, your body responds by increasing hunger hormones and decreasing metabolic rate. This is an evolutionary survival mechanism. Your body does not know you are intentionally losing weight. It interprets the calorie deficit as potential starvation and fights back by making you hungrier and more efficient at storing energy.
Research shows that for every kilogram of weight lost, ghrelin increases by approximately 50 to 100 picograms per milliliter and leptin decreases proportionally. This means someone who has lost 20 pounds will experience significantly more baseline hunger than they did before the weight loss, even if nothing else has changed.
Tirzepatide partially counteracts this adaptation, which is why the SURMOUNT-4 trial showed that stopping the medication after significant weight loss led to substantial weight regain. The medication is actively fighting your metabolic adaptation the entire time you are taking it. But if the adaptation is strong enough, particularly after substantial weight loss, you may notice increased hunger even at a stable dose.
This does not mean the medication stopped working. It means your body metabolic defense systems are escalating, and the medication is holding the line rather than pushing further. Your prescriber may recommend a dose increase at this point, or you may need to focus on the strategies for maintaining weight loss while the medication continues its work.
What to do: If hunger increases after a period of good appetite control and significant weight loss, discuss dose optimization with your prescriber. Also focus on supporting your metabolism through resistance training, adequate protein intake, and quality sleep. These three factors partially offset the metabolic adaptation that accompanies weight loss.
9. Inconsistent injection timing or technique
Tirzepatide has a half-life of about 5 days. That means blood levels peak roughly 24 to 48 hours after injection and gradually decline over the following days. If your injection schedule is inconsistent, you create peaks and valleys in the medication concentration that directly affect appetite control.
Injecting on Monday one week and Thursday the next creates a 3-day gap followed by a 10-day gap. During that longer gap, blood levels drop low enough that hunger signals break through. You then associate those hungry days with the medication "not working," when the real issue is timing inconsistency.
Injection technique also matters. Subcutaneous injections need to reach the fatty tissue layer beneath the skin. If the injection goes too shallow (into the dermis) or too deep (into muscle), absorption rates change, which affects how consistently the medication reaches therapeutic levels. Injection site reactions can also be a clue that technique needs adjustment.
What to do: Pick the same day each week and stick to it. Set a phone alarm. If you need to change your injection day, shift by no more than 2 days in either direction. For technique, review our guide on how to inject tirzepatide properly. Rotate between three sites: abdomen (2 inches from the navel), outer thigh, and upper arm. Consistent depth and rotation promote steady absorption and reduce injection site reactions.
What to eat on tirzepatide to stay full longer
Diet composition is not just a supporting factor. It is a multiplier. The right foods amplify tirzepatide appetite suppression. The wrong foods work against it.
Here is what the research says about building meals that keep hunger at bay.
The satiety priority framework
Not all calories are created equal when it comes to fullness. Protein, fiber, and healthy fats produce significantly longer satiety than refined carbohydrates, even at the same calorie count. A 400-calorie meal of grilled salmon, roasted vegetables, and quinoa will keep you full for 4 to 5 hours. A 400-calorie bowl of pasta with marinara sauce might last 2 hours.
The order in which you eat also matters. Research published in Diabetes Care found that eating protein and vegetables before carbohydrates at the same meal reduced post-meal blood sugar spikes by 29% and increased satiety. On tirzepatide, this eating order strategy can extend fullness by an additional 30 to 60 minutes per meal.
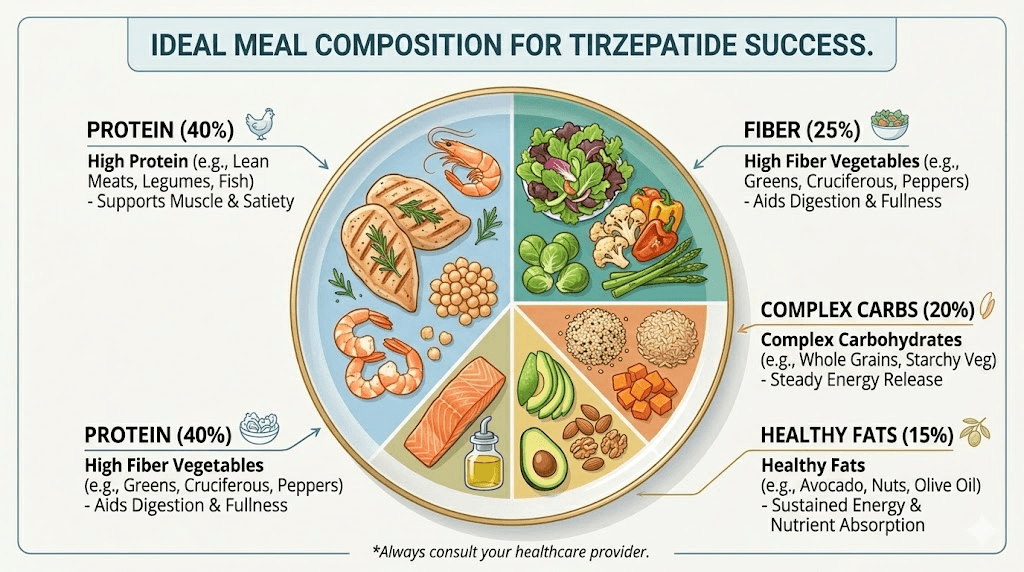
Build every meal around this structure:
Protein first (25 to 35 grams): chicken, fish, eggs, Greek yogurt, cottage cheese, tofu, or a protein shake
Fiber-rich vegetables second: broccoli, spinach, Brussels sprouts, bell peppers, zucchini, or leafy greens
Complex carbohydrates last: sweet potatoes, brown rice, quinoa, lentils, or whole grain bread
Healthy fats throughout: avocado, olive oil, nuts, seeds, or fatty fish
For a detailed breakdown, check our comprehensive guide on foods to avoid on tirzepatide and the corresponding meal plan that maximizes satiety without overcomplicating your daily routine.
Sample high-satiety meal ideas
Breakfast options:
3 eggs scrambled with spinach and feta, half an avocado on the side (32g protein, 12g fiber)
Greek yogurt parfait with berries, walnuts, and chia seeds (28g protein, 8g fiber)
Protein smoothie with whey, frozen berries, spinach, flaxseed, and almond butter (35g protein, 10g fiber)
Lunch options:
Grilled chicken salad with mixed greens, chickpeas, cucumber, olive oil, and feta (38g protein, 10g fiber)
Lentil soup with a side of grilled chicken and whole grain bread (34g protein, 14g fiber)
Tuna salad lettuce wraps with avocado and a side of mixed vegetables (30g protein, 8g fiber)
Dinner options:
Baked salmon with roasted broccoli and sweet potato (35g protein, 9g fiber)
Ground turkey stir-fry with peppers, onions, and brown rice (32g protein, 7g fiber)
Grilled chicken thighs with roasted Brussels sprouts and quinoa (36g protein, 11g fiber)
These meals align with what research calls the "protein leverage hypothesis," the concept that humans continue eating until protein needs are met. When protein is prioritized at each meal, total caloric intake naturally decreases because the protein satiety signal arrives before excess calories accumulate.
Our guide on foods to eat while on GLP-1 medications provides even more options. While written for semaglutide users, the nutritional principles apply equally to tirzepatide.
The complete tirzepatide dose escalation timeline
Understanding the dose schedule removes a massive amount of anxiety. Here is exactly what to expect at each stage, including when appetite changes typically appear.
Dose | Weeks | Purpose | Typical appetite effect |
|---|---|---|---|
2.5mg | Weeks 1-4 | Tolerability assessment | Minimal to no appetite change for most people |
5mg | Weeks 5-8 | First therapeutic dose | Some notice mild appetite reduction, many do not |
7.5mg | Weeks 9-12 | Moderate therapeutic dose | Most people begin noticing meaningful appetite decrease |
10mg | Weeks 13-16 | Standard maintenance dose | Significant appetite suppression for majority of users |
12.5mg | Weeks 17-20 | Higher maintenance dose | Strong appetite suppression, reduced food cravings |
15mg | Week 20+ | Maximum dose | Maximum appetite suppression achieved in trials |
Not everyone needs to reach 15mg. Many people find excellent appetite control at 7.5mg or 10mg. Your prescriber will help determine the right maintenance dose based on your response, side effect tolerance, and weight loss trajectory.
If you are using compounded tirzepatide, the concentration may differ from brand-name Mounjaro or Zepbound. Use our compounded tirzepatide dosage calculator to ensure accurate dosing. Some people also explore microdosing tirzepatide as a way to manage side effects during escalation while still progressing toward therapeutic levels.
The key takeaway: if you are in weeks 1 through 12 and still feeling hungry, you are likely still in the building phase. The appetite suppression will come. It just takes time to get there.
For detailed unit-by-unit breakdowns at each dose level, review our tirzepatide dosing chart in units or the injection dosage chart that matches your specific vial concentration.
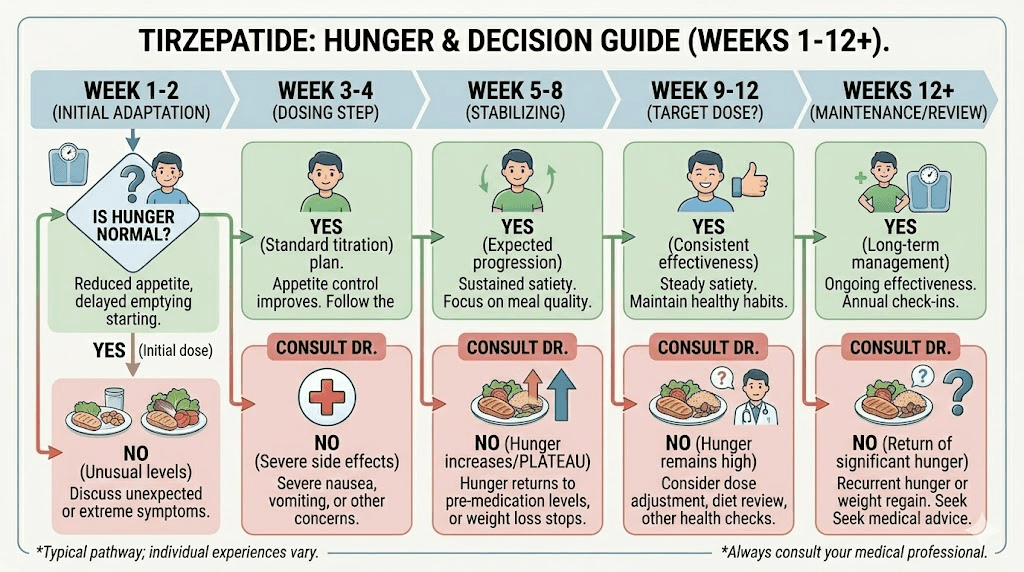
When to talk to your doctor about persistent hunger
There is a clear line between normal dose-escalation hunger and hunger that warrants medical attention. Knowing where that line falls prevents both unnecessary panic and dangerous complacency.
Normal scenarios (keep going)
You are in the first 8 weeks and at 2.5mg or 5mg
Your appetite has decreased slightly but not dramatically
You feel hungrier on days 5 to 7 after injection compared to days 1 to 3
Your hunger is manageable with proper meals and hydration
Your weight is slowly trending down even if hunger persists
Contact your prescriber if
Significant hunger persists after 12 or more weeks at a stable maintenance dose (7.5mg or higher)
Appetite suddenly increases after a period of good control (possible medication storage issue, check refrigeration requirements and temperature exposure)
Hunger is accompanied by excessive thirst, frequent urination, or unexplained fatigue (screen for blood sugar issues)
You are experiencing severe headaches, anxiety, or other symptoms alongside persistent hunger
Weight has completely stalled for 6 or more weeks despite dietary adherence (your provider may consider troubleshooting the protocol)
Your prescriber has several options when hunger persists at higher doses. They may increase to the next dose tier if you are not yet at maximum. They may add a complementary medication like phentermine for short-term appetite support. They may investigate whether a compounded formulation has expired or been improperly stored, affecting potency.
Never adjust your own dose without medical guidance. Increasing tirzepatide too quickly raises the risk of gastrointestinal side effects and does not necessarily improve outcomes. The dose escalation schedule exists for safety reasons.
Supplements and strategies that support appetite control
Beyond food composition and medication timing, several evidence-based strategies can meaningfully reduce hunger while on tirzepatide.
Supplements worth considering
Fiber supplements: Psyllium husk (Metamucil) or glucomannan taken with water before meals can add bulk to your stomach and slow digestion further. Start with half doses and increase gradually. These are particularly helpful if you struggle to get enough fiber from food alone. Check our detailed guide on supplements to take with tirzepatide for dosing guidance.
B12 and methylcobalamin: GLP-1 agonists can reduce B12 absorption over time. Low B12 levels contribute to fatigue, which some people interpret as hunger. Many compounded formulations now include B12 directly in the tirzepatide blend. If yours does not, a separate B12 supplement is worth discussing with your provider.
Glycine: This amino acid has shown appetite-modulating properties in preliminary research. Some compounded tirzepatide formulations include glycine or glycine and B12 together. Glycine may also improve sleep quality, which indirectly supports appetite regulation.
Niacinamide: Some compounded blends add niacinamide to tirzepatide. Research suggests potential synergistic effects on metabolic health, though more studies are needed on direct appetite impacts.
L-carnitine: Another common addition to compounded blends, levocarnitine with tirzepatide may support fat metabolism and energy levels, reducing the fatigue-related hunger that some people experience during calorie restriction.
Behavioral strategies
Slow eating: One study found that people who ate slowly consumed approximately 70 fewer calories per meal. This works because the satiety signals from your gut take about 20 minutes to reach your brain. If you finish a meal in 5 minutes, you miss that feedback loop entirely. Aim for a 20-minute meal window. Put your fork down between bites.
Meal timing consistency: Eating at roughly the same times each day helps regulate circadian hunger signals. Erratic meal timing disrupts ghrelin rhythms and can increase overall hunger. You do not need to follow a strict schedule, but general consistency within a 1-hour window helps.
Mindful eating practices: Eating while distracted (phone, TV, computer) increases caloric intake by 25% or more, according to research from the American Journal of Clinical Nutrition. When you eat, just eat. Notice the food. Chew thoroughly. This is not woo. It is neuroscience. Your brain needs attention directed at eating to properly process satiety signals.
Resistance training: This seems counterintuitive, but resistance training can improve appetite regulation over time. It increases insulin sensitivity, supports lean mass (which raises metabolic rate), and improves the hormonal profile associated with hunger regulation. Aim for at least 150 minutes of moderate exercise per week, including 2 to 3 sessions of resistance training. Peptides for muscle growth is a related topic worth exploring if you are concerned about lean mass preservation during weight loss.
How tirzepatide hunger compares to semaglutide
If you have tried semaglutide before tirzepatide, or you are deciding between the two, understanding the appetite differences helps set realistic expectations.
Semaglutide (Ozempic, Wegovy) is a pure GLP-1 receptor agonist. Tirzepatide is a dual GLP-1 and GIP receptor agonist. This difference matters for appetite in several ways.
In head-to-head comparisons from the SURMOUNT-5 trial, tirzepatide produced approximately 47% more weight loss than semaglutide at maximum doses over 72 weeks. Much of that additional weight loss comes from greater appetite suppression and better tolerability.
Semaglutide users commonly report that appetite suppression is strong but accompanied by more nausea, which can make the experience unpleasant even when it works. Tirzepatide users tend to report appetite suppression with less nausea, thanks to the GIP component. However, some tirzepatide users note that the appetite suppression feels less "dramatic" than semaglutide, even though the weight loss outcomes are better.
If you switched from semaglutide to tirzepatide, read our guide on switching between the two medications and the dose conversion chart to make sure your tirzepatide dose is equivalent to or higher than your previous semaglutide dose. Underdosing during a switch is a common reason for returning hunger.
For semaglutide users wondering about appetite timelines, we have a separate guide on how long semaglutide takes to suppress appetite and what to do if appetite suppression does not happen immediately.
The bottom line: tirzepatide produces better weight loss results with generally better tolerability, but the subjective experience of appetite suppression varies. Some people feel it less intensely with tirzepatide, even though the objective outcomes are superior. Trust the scale and your body composition changes over the subjective feeling of hunger.
Building habits that outlast the medication
Here is the uncomfortable truth that most tirzepatide articles avoid: the medication is not forever for most people.
Whether you eventually wean off tirzepatide, switch to a maintenance dose, or continue long-term, the habits you build while on the medication determine whether the results stick. The SURMOUNT-4 trial showed that participants who stopped tirzepatide after 36 weeks regained approximately two-thirds of their lost weight over the following year. Participants who continued the medication maintained their results.
The lesson is not that you need to take tirzepatide forever. The lesson is that the medication creates a window of opportunity, a period where hunger is reduced and behavior change is easier, and what you do with that window matters enormously.
Use the appetite suppression period to establish:
Protein-forward eating habits that become automatic, not something you have to think about
Regular meal timing that regulates your hunger hormones naturally
Movement patterns that support metabolic rate and muscle mass
Sleep routines that protect hormonal balance
Stress management techniques that do not involve food
These habits become the safety net that catches you if and when medication support changes. SeekPeptides members access detailed protocol guides that cover exactly this, building sustainable frameworks around peptide use so that the results last beyond the injection.
The researchers who see the best long-term outcomes are not the ones with the strongest initial appetite suppression. They are the ones who used the low-hunger window to rewire their relationship with food, exercise, and self-care. The medication bought them time. They invested it wisely.
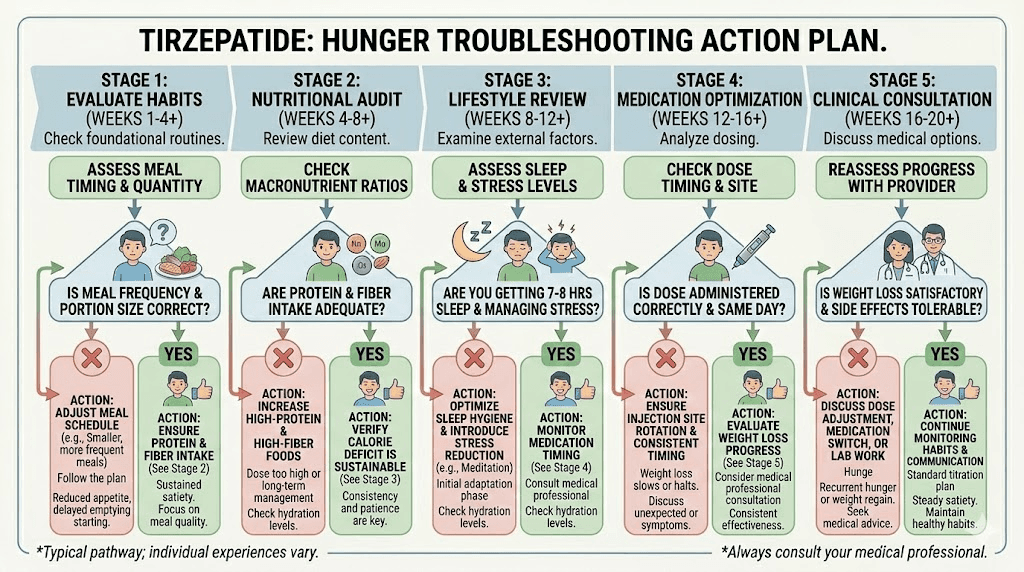
Putting it all together: your action plan
If you are still hungry on tirzepatide right now, here is the decision tree.
Step 1: Check your dose and timeline. Are you below 7.5mg? Have you been at your current dose for fewer than 4 weeks? If yes, patience is the primary prescription. Review the dose chart and confirm you are on track.
Step 2: Audit your diet for 3 days. Track protein, fiber, and water. If protein is below 0.8 grams per kilogram of body weight, if fiber is under 20 grams, or if water intake is under 64 ounces, these are your immediate fixes. Use the tirzepatide diet plan as a starting template.
Step 3: Evaluate sleep and stress. If you are sleeping under 7 hours or experiencing chronic stress, these are undermining the medication. Address them in parallel with any dietary changes.
Step 4: Confirm injection consistency. Same day each week. Proper technique. Correct depth. Good rotation. Review injection site options and stomach injection technique if needed.
Step 5: Distinguish physical from emotional hunger. If you are eating when not physically hungry, the solution is behavioral, not pharmaceutical. Consider professional support.
Step 6: If all factors are optimized and hunger persists at a maintenance dose for 12+ weeks, contact your prescriber. There may be a medication adjustment, storage issue, or underlying factor that needs clinical evaluation.
For researchers navigating these decisions, SeekPeptides provides comprehensive protocol guides, dosing tools, and community support from people who have walked this exact path. The compounded tirzepatide dosage calculator and general peptide calculator can help ensure your dosing is precise, while the compound dosage charts provide visual references for each concentration.
Frequently asked questions
How long does it take for tirzepatide to suppress appetite?
Most people begin noticing meaningful appetite suppression between weeks 4 and 8 at a stable dose, with full effects potentially taking 12 or more weeks. At the starting dose of 2.5mg, appetite changes are minimal for most users. Significant suppression typically begins at 7.5mg or higher. Read our detailed tirzepatide timeline guide for week-by-week expectations.
Why am I hungry on 7.5mg of tirzepatide?
At 7.5mg, many people are still in the building phase. Give it at least 4 full weeks at this dose before evaluating. If hunger persists, check your protein intake (aim for 1.0 to 1.2 grams per kilogram of body weight), hydration, and sleep quality. Your prescriber may also consider increasing to 10mg if 7.5mg proves insufficient after an adequate trial period.
Does tirzepatide completely eliminate hunger?
No. Tirzepatide modulates hunger signals rather than eliminating them entirely. The goal is a meaningful reduction in appetite, food cravings, and the preoccupation with eating, not the complete absence of hunger. Most people on therapeutic doses report that they can eat smaller portions and feel satisfied, that they think about food less often, and that cravings for high-calorie foods decrease substantially. Some physical hunger will always remain, which is normal and healthy.
Can I eat more protein to help with hunger on tirzepatide?
Yes. Increasing protein intake is one of the most effective strategies for managing hunger on tirzepatide. Aim for 25 to 35 grams of protein per meal, prioritizing lean sources like chicken, fish, eggs, and Greek yogurt. Our guide on what to eat on tirzepatide provides specific meal ideas. Protein triggers additional satiety hormones that complement the medication mechanism.
Should I split my tirzepatide dose if I am hungry between injections?
Some prescribers do recommend splitting the dose into two smaller injections per week to maintain more consistent blood levels. This approach can smooth out the peaks and valleys that cause end-of-week hunger. However, this should only be done under medical supervision. Do not split your dose without consulting your prescriber first.
Is it normal to feel more hungry right before my next injection?
Yes. This is called end-of-dose hunger and happens because tirzepatide blood levels are at their lowest point 6 to 7 days after injection. It is one of the most commonly reported patterns. Some people manage this by scheduling their injection for the day they feel hungriest, creating a natural rhythm. Others find that injecting a day early helps, though consistency is more important than any single adjustment.
Will the hunger come back if I stop tirzepatide?
Research from the SURMOUNT-4 trial confirms that hunger does increase after stopping tirzepatide. Most participants who discontinued the medication experienced a return of appetite and significant weight regain over the following 12 months. This is why maintaining weight loss after tirzepatide requires a structured plan and why many prescribers recommend long-term use or a gradual weaning protocol.
Does alcohol affect appetite on tirzepatide?
Yes. Alcohol can increase appetite through multiple mechanisms: it lowers inhibitions around food choices, stimulates ghrelin production, and provides empty calories that do not trigger satiety. Many tirzepatide users also report reduced alcohol tolerance, which changes the risk-reward calculation. If hunger management is a priority, minimizing alcohol intake will help.
External resources
Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1) - New England Journal of Medicine
Tirzepatide Reduces Appetite, Energy Intake, and Fat Mass - PubMed Central
Tirzepatide Reduces Appetite, Energy Intake, and Fat Mass - Diabetes Care
SURMOUNT-4: Continued Treatment With Tirzepatide for Weight Maintenance - PubMed Central
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay balanced, your doses stay consistent, and your results stay everything you hoped for.