Feb 20, 2026

Before you blame your GLP-1 medication for that pounding in your skull, read this. Because the headache you are experiencing might not mean what you think it means.
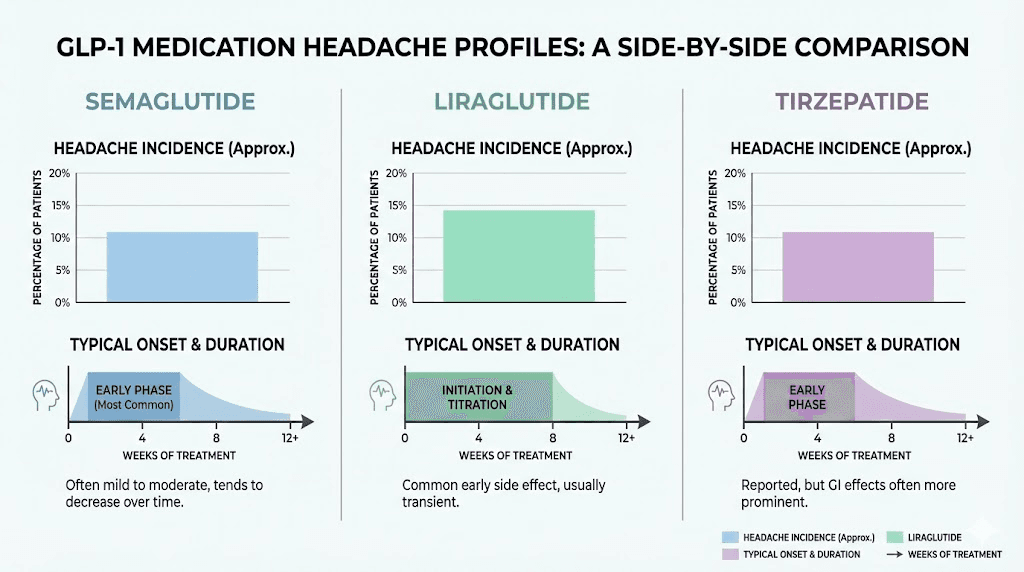
Headaches rank among the most commonly reported side effects of GLP-1 receptor agonists. Somewhere between 4% and 14% of users experience them, depending on the specific medication and dosage. That is a wide range. And it tells you something important. The headache is not random. It is not inevitable. And in most cases, it is entirely manageable once you understand what is actually causing it.
Here is where it gets interesting.
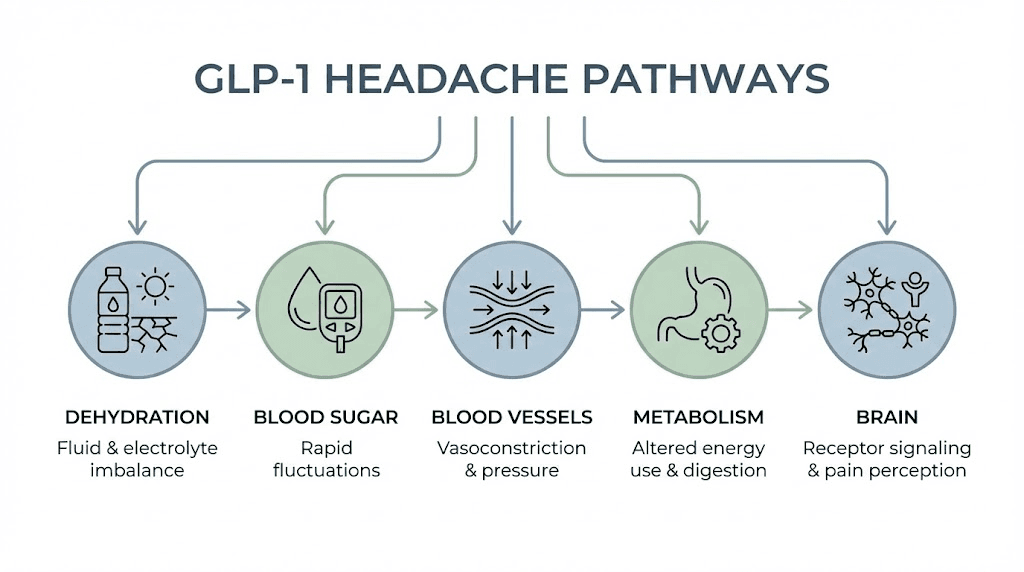
The mechanisms behind GLP-1 headaches are more complex than most guides suggest. Dehydration plays a role, yes. But so do cerebrovascular changes, blood sugar fluctuations, central nervous system pathway activation, and metabolic shifts that occur during rapid weight loss. Each mechanism requires a different response. Treating a dehydration headache the same way you treat a vasodilation headache is like putting a bandage on a broken bone. It misses the point entirely.
This guide breaks down every mechanism behind GLP-1 headaches, covers the real clinical trial numbers for semaglutide, tirzepatide, and liraglutide, and gives you specific protocols for prevention and relief. Whether you just started your first injection or you are dealing with persistent headaches after a dose increase, you will find actionable solutions here. SeekPeptides has compiled the research so you do not have to guess your way through it.
Why GLP-1 medications cause headaches
The question sounds simple. The answer is not.
GLP-1 receptor agonists trigger headaches through at least five distinct pathways. Some are obvious. Some are not. And understanding which pathway is responsible for your specific headache changes everything about how you respond to it. Researchers studying GLP-1 fatigue and other side effects have found that most adverse reactions share overlapping mechanisms, which means addressing the root cause of your headache often improves other symptoms simultaneously.
Dehydration from gastrointestinal side effects
This is the big one. The mechanism most doctors point to first, and for good reason.
GLP-1 medications slow gastric emptying. That is their primary mechanism for reducing appetite. But slowed digestion also triggers nausea, vomiting, and diarrhea in a significant percentage of users. Each of these conditions drains fluid from your body. Nausea reduces your desire to drink. Vomiting expels fluid directly. Diarrhea pulls water from your intestinal lining faster than you can replace it.
The result? A dehydration headache that can range from a dull background pressure to a throbbing, debilitating pain that makes concentration impossible. Studies identify dehydration as the predominant non-neurological contributor to headaches during GLP-1 treatment, which means it is responsible for more headaches than any other single factor.
If you are taking compounded semaglutide or any other GLP-1 formulation, your fluid requirements increase the moment you start treatment. Not by a little. By a lot. Most researchers recommend 2 to 3 liters of water daily while on GLP-1 therapy, compared to the standard 1.5 to 2 liters for the general population. That difference matters.
Blood sugar fluctuations and hypoglycemia
GLP-1 receptor agonists lower blood glucose. That is part of their design, particularly for medications like Ozempic originally developed for type 2 diabetes management. But lower blood sugar can cross the line into hypoglycemia, especially if you are also taking insulin, sulfonylureas, or other glucose-lowering medications.
Hypoglycemic headaches have a distinctive quality. They tend to come with dizziness, shakiness, confusion, and fatigue. The headache itself often feels different from a dehydration headache, more like a heavy pressure behind the eyes accompanied by a general sense of unwellness.
The risk increases significantly when you skip meals. And here is the problem. GLP-1 medications suppress appetite, sometimes dramatically. Users on higher doses of semaglutide or tirzepatide frequently report forgetting to eat entirely. No appetite means no food. No food means dropping blood sugar. Dropping blood sugar means headaches.
The solution is not complicated. But it requires intentional effort.
Cerebrovascular changes and vasodilation
This mechanism is less well known but increasingly documented in research. GLP-1 receptor activation in the central nervous system influences cerebrovascular tone and regional blood flow. In simpler terms, these medications can cause blood vessels in your brain to dilate.
Cerebral vasodilation creates mechanical strain on pain-sensitive structures surrounding blood vessels. That strain registers as a headache. This is actually the same mechanism behind many migraines, which is why some GLP-1 users report headaches that feel distinctly migraine-like, complete with sensitivity to light, nausea that seems separate from the GI effects, and throbbing unilateral pain.
FDA pharmacovigilance data supports this connection. Analysis found a reporting odds ratio of 1.74 for headache onset and 1.28 for migraine among GLP-1 receptor agonist users. Those numbers suggest that vascular-mediated headaches are a real and measurable phenomenon, not just anecdotal reports from online forums.
Metabolic shifts during rapid weight loss
Rapid weight loss changes your body chemistry. Hormones shift. Fat cells release stored compounds as they shrink. Electrolyte balance fluctuates. Your metabolism recalibrates to a new energy expenditure baseline. All of these changes can trigger headaches.
Users who experience significant weight loss on tirzepatide or semaglutide sometimes report headaches that persist beyond the initial adjustment period. These metabolic headaches tend to be more diffuse, less severe, and harder to pin down than dehydration or blood sugar headaches. They feel like a constant low-grade pressure that comes and goes without obvious triggers.
The good news? They typically resolve as your body reaches a new metabolic equilibrium. The bad news? That can take weeks to months, depending on the rate of weight loss.
Central nervous system pathway modulation
GLP-1 receptors exist throughout the brain. When you take a GLP-1 receptor agonist, you are not just affecting your gut and pancreas. You are activating receptors in brain regions involved in appetite regulation, reward processing, and pain perception.
Research has identified GLP-1 mediated modulation of pain pathways through microglial activation in the caudal trigeminal nucleus. Microglia are immune cells in the brain, and when they become activated, they can exacerbate central sensitization and worsen headache symptoms. This mechanism may explain why some users experience headaches that do not respond well to standard OTC painkillers, because the headache originates from neuroinflammatory processes rather than peripheral causes like dehydration.
Understanding these pathways matters for SeekPeptides members tracking their protocols, because the treatment approach differs substantially depending on which mechanism is driving your headache.
How common are GLP-1 headaches (the real numbers)
Numbers matter. When you are deciding whether to start a medication or wondering if your experience is normal, vague reassurances do not help. Specific data does.
Semaglutide headache rates
Clinical trials paint a clear picture. For semaglutide used at diabetes doses (Ozempic, up to 1 mg weekly), headache incidence runs between 4% and 8%. That is roughly 1 in 15 to 1 in 25 users.
Raise the dose to weight management levels (Wegovy, up to 2.4 mg weekly), and the numbers jump. Headache rates climb to 8% to 14% of participants. One clinical trial reported that 15.2% of participants experienced headaches after higher-dose semaglutide, compared to 12.2% receiving placebo. That difference, roughly 3 percentage points above placebo, represents the genuine medication-attributable headache risk.
That matters. It means some headaches on semaglutide would have happened anyway, regardless of the medication. But it also confirms that semaglutide does genuinely increase headache risk above baseline. Users exploring semaglutide dosing charts should factor this into their decision-making.
Tirzepatide headache rates
Tirzepatide operates on two receptors, GLP-1 and GIP, making it a dual agonist. Despite this additional mechanism, headache rates are actually slightly lower than high-dose semaglutide, running approximately 5% to 7% in most clinical trials.
However, one study documented headaches in 13.5% of tirzepatide participants during dose escalation phases. That higher number likely reflects the titration period, when GI side effects peak and dehydration risk is highest. Once users reach stable maintenance doses, headache rates tend to decrease substantially.
If you are researching whether tirzepatide causes headaches, the answer is yes, but typically at lower rates than the highest semaglutide doses. The dual receptor action does not appear to compound headache risk.
Liraglutide and other GLP-1 medications
Liraglutide (Saxenda for weight loss, Victoza for diabetes) shows documented headache events at doses of 1.8 mg daily. The incidence is comparable to semaglutide at equivalent effect levels, generally in the 6% to 10% range.
Exenatide (Byetta, Bydureon) at 2 mg weekly and dulaglutide (Trulicity) at 0.75 to 1.5 mg weekly both show headache as a reported adverse event. Across the entire GLP-1 class, headache remains one of the most frequently reported non-gastrointestinal side effects. The consistency across different medications suggests the mechanism is tied to GLP-1 receptor activation itself rather than any specific drug formulation.
For researchers comparing options, the semaglutide versus tirzepatide comparison page provides detailed head-to-head data on side effect profiles.
Clinical trial data versus real-world experience
Clinical trials control variables. Real life does not.
Trial participants receive standardized doses, regular monitoring, dietary guidance, and hydration reminders. Real-world users often start medications without adequate preparation, skip meals because they have no appetite, forget to increase fluid intake, and push through side effects without adjusting their protocol.
This gap explains why online communities report headache rates that seem higher than clinical trial data. It is not that the studies are wrong. It is that real-world compliance with headache prevention strategies is much lower than clinical trial compliance. The people experiencing the worst headaches are often the ones doing the least to prevent them.
Types of headaches on GLP-1 medications
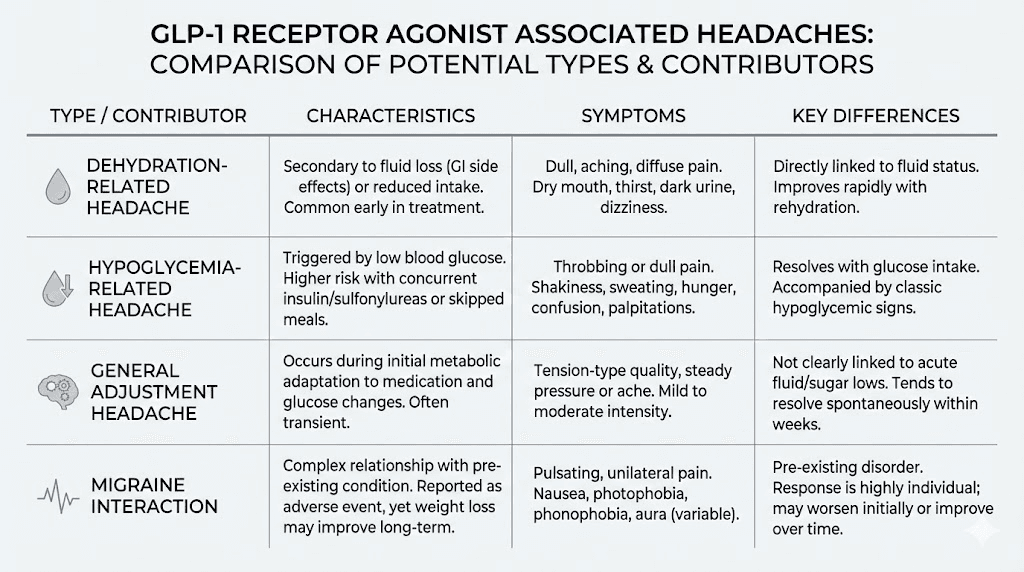
Not all headaches are the same. And treating them all the same way wastes time and prolongs your suffering. Identifying your specific headache type is the first step toward resolving it.
Tension headaches
The most common type. Tension headaches feel like a band of pressure around your forehead and temples. They are bilateral, meaning they affect both sides of your head equally. The pain is steady rather than throbbing, and it typically ranges from mild to moderate.
On GLP-1 medications, tension headaches most often stem from dehydration, stress about new medication side effects, changes in sleep patterns due to altered appetite, or muscle tension from nausea. They respond well to adequate hydration, rest, and standard OTC pain relievers like acetaminophen.
Users who experience semaglutide fatigue alongside tension headaches should recognize that both symptoms often share the same root cause. Address the dehydration and blood sugar instability, and both symptoms tend to improve together.
Migraine headaches
More concerning. Migraines present with throbbing pain, usually on one side of the head. They come with sensitivity to light and sound, nausea that feels separate from GI effects, and sometimes visual disturbances called aura.
FDA pharmacovigilance data shows a reporting odds ratio of 1.28 for migraine among GLP-1 users. That elevated risk is modest but real. Published case reports describe hemiplegic migraines exacerbated by injectable GLP-1 agonists used for weight loss. If you have a personal or family history of migraines, GLP-1 medications may increase your frequency or severity of attacks, particularly during the initial weeks of treatment.
The vascular mechanism discussed earlier, cerebral vasodilation from GLP-1 receptor activation, likely drives these migraine presentations. Unlike tension headaches, migraines may require prescription-level intervention if they persist or worsen.
Dehydration headaches
These have a particular character. The pain worsens when you stand up quickly, bend over, or increase physical activity. It improves when you lie down. You may notice that your urine is darker than usual, your mouth feels dry, and your skin lacks its normal elasticity.
Dehydration headaches from GLP-1 medications often develop gradually over hours rather than striking suddenly. They build as your fluid deficit accumulates throughout the day. By late afternoon or evening, the headache is fully established, and no amount of water in the next hour will resolve it quickly.
The lesson? Prevention beats treatment every time. Proactive hydration throughout the day prevents these headaches far more effectively than reactive water consumption after the headache has already started. Users on compounded semaglutide or compounded tirzepatide should be especially vigilant because compounded formulations may have different concentration profiles that affect GI symptom timing.
Hypoglycemic headaches
These hit differently. Fast onset. Accompanied by shakiness, sweating, confusion, irritability, and sometimes blurred vision. The headache itself feels heavy, oppressive, and distinctly unpleasant in a way that differs from typical tension or dehydration headaches.
Hypoglycemic headaches on GLP-1 medications are more common in people who also take insulin or sulfonylureas. But they can occur in anyone who significantly reduces caloric intake after starting treatment. When your appetite drops dramatically and you cut calories too aggressively, blood sugar can dip below comfortable levels even without additional diabetes medications.
Monitoring your diet becomes essential. The best foods for semaglutide users and tirzepatide dietary recommendations emphasize balanced macronutrients specifically to prevent these blood sugar drops.
When GLP-1 headaches occur (the timeline)
Timing reveals cause. If you know when your headache pattern started, you can often identify why it started.
First injection headaches
Many users report headaches within 24 to 72 hours of their very first GLP-1 injection. This makes sense. Your body has never encountered exogenous GLP-1 receptor activation at these levels before. Every system affected by the medication, appetite, digestion, blood sugar regulation, vascular tone, needs to recalibrate.
First injection headaches are usually mild to moderate and resolve within a few days. They represent the adjustment period, your body learning to function with a new chemical signal operating in the background. Think of it as the onboarding phase. Uncomfortable, but temporary.
For users just starting treatment, understanding proper GLP-1 injection technique and optimal injection sites will not directly prevent headaches, but ensuring proper medication delivery reduces the risk of erratic absorption that can worsen side effect profiles.
Dose escalation headaches
This is the pattern most users notice. You tolerate the starting dose fine. Maybe a mild headache the first day or two. Then you increase your dose, and the headache returns, sometimes worse than before.
Dose escalation headaches occur because each increase amplifies the medication effects. More GLP-1 receptor activation means more appetite suppression, more gastric slowing, more fluid loss risk, and more cerebrovascular influence. Your body adapted to the lower dose. Now it needs to adapt again.
Clinical trials consistently show that gastrointestinal side effects (and their downstream consequences including headaches) tend to occur during dose escalation rather than at stable maintenance doses. For semaglutide, the standard titration starts at 0.25 mg weekly and increases every four weeks. For tirzepatide, titration begins at 2.5 mg weekly with similar escalation schedules.
The slower you titrate, the less likely severe headaches become. Users who rush through dose escalation, skipping intermediate steps or increasing faster than recommended, tend to experience the worst headaches. Patience during titration is not just about tolerability. It is about giving your body time to adjust its fluid regulation, blood sugar management, and vascular responses at each level before adding more stimulation.
Ongoing versus transient headaches
Most GLP-1 headaches are transient. They appear during the first few weeks of treatment or after dose increases, then gradually fade as the body adjusts. Research describes them as generally mild, nondisabling, and most frequently occurring within the first 26 weeks of treatment.
But some users experience persistent headaches. These ongoing headaches, lasting beyond the typical adjustment window, warrant medical evaluation. They may indicate chronic dehydration that the user has not adequately addressed, an underlying headache condition being exacerbated by the medication, or a need for dosage adjustment.
The distinction matters because transient headaches typically respond to hydration and OTC treatment, while persistent headaches may require changes to your overall protocol. SeekPeptides members tracking their progress can use protocol adjustment features to document headache patterns alongside dose changes, making it easier to identify triggers and solutions.
How long do GLP-1 headaches last
Two timeframes matter here. How long each individual headache episode lasts, and how long headaches persist as a recurring side effect.
Individual episodes typically resolve within a few hours to a couple of days. A dehydration headache might clear within 1 to 2 hours of adequate fluid and electrolyte replacement. A post-injection headache might linger for 24 to 48 hours before fading. A dose escalation headache might persist for 3 to 5 days as your body adjusts to the new level.
As a recurring side effect, most users find that headaches improve substantially within 2 to 8 weeks of starting treatment or reaching a new dose. The body adapts. The GI effects diminish. Fluid regulation normalizes. Blood sugar stabilizes. And the headaches fade.
However, every person responds differently. What resolves in days for one user might take weeks for another. Factors that influence duration include your baseline hydration habits, overall health status, the specific medication and dose you are taking, whether you are on concurrent medications, and how aggressively you implement prevention strategies.
Users who experience semaglutide withdrawal symptoms when missing doses should know that headache can also occur during withdrawal, creating a frustrating cycle where headaches appear both when starting and when stopping the medication.
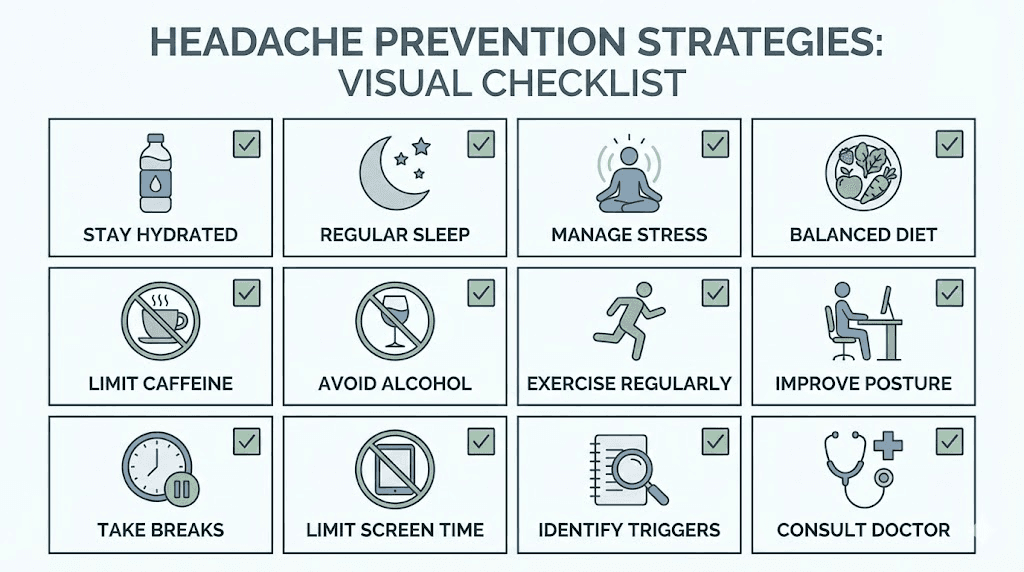
12 proven strategies to prevent GLP-1 headaches
Prevention works better than treatment. These strategies are ranked by impact, from the most effective interventions to supportive measures that enhance overall outcomes.
Strategy 1: aggressive hydration protocol
This is non-negotiable. If you do nothing else on this list, do this.
Standard recommendation is 8 glasses of water daily. On GLP-1 medications, aim for 10 to 12 glasses, or 2 to 3 liters total. But do not try to drink it all at once. Distribute your intake throughout the day. Set reminders every hour. Keep a water bottle visible at all times. Drink before you feel thirsty, because thirst is a late indicator of dehydration.
Morning hydration is especially critical. You wake up already dehydrated from 6 to 8 hours without fluid intake. Start your day with 16 to 20 ounces of water before anything else. Before coffee. Before food. Before your morning routine. This single habit prevents more headaches than any other intervention.
Strategy 2: electrolyte management
Water alone is not enough. When GLP-1 medications cause fluid loss through GI effects, you lose electrolytes too. Sodium, potassium, and magnesium all drop. And electrolyte imbalance triggers headaches independently of dehydration.
Products like LMNT, Nuun tablets, or Liquid IV can help replace lost electrolytes. Bone broth is an excellent natural option that provides sodium along with other minerals. Some users find that adding a pinch of sea salt to their water bottle prevents the electrolyte-related component of their headaches entirely.
The key minerals to watch are sodium (1500 to 2300 mg daily), potassium (2600 to 3400 mg daily), and magnesium (310 to 420 mg daily). If your diet has changed significantly since starting GLP-1 medication, which it likely has given the appetite suppression, you may need to supplement what you are no longer getting from food. Users exploring supplements to take with tirzepatide will find electrolyte supplementation at the top of most recommendation lists.
Strategy 3: blood sugar stabilization through nutrition
Eat something. Even when you do not want to.
GLP-1 medications suppress appetite powerfully. But your brain still needs glucose. Your muscles still need protein. Your cells still need micronutrients. Skipping meals entirely because you have no appetite is one of the fastest routes to a headache.
Focus on smaller, more frequent meals rather than trying to force large ones. Three small meals and two snacks beats two large meals for blood sugar stability. Each meal should include protein, complex carbohydrates, and healthy fats. This macronutrient combination slows glucose absorption and prevents the spikes and crashes that trigger headaches.
The semaglutide diet plan and tirzepatide diet plan resources both emphasize balanced nutrition specifically designed to minimize side effects while maintaining adequate caloric intake for health.
Strategy 4: gradual dose titration
Do not rush your dose increases. The standard titration schedules exist for a reason.
For semaglutide, that means starting at 0.25 mg for four weeks, then 0.5 mg for four weeks, then 1 mg, and so on. For tirzepatide, it means 2.5 mg for four weeks minimum before moving to 5 mg. Some users benefit from extending each step to 6 or even 8 weeks if side effects are significant.
A significantly higher proportion of tirzepatide users (77.6%) achieve guideline-recommended maintenance doses compared to semaglutide users (52.9%), with tirzepatide users also reaching maintenance more quickly, at a median of 32 days versus 143 days. But faster is not always better if headaches are disrupting your quality of life. Discuss extended titration schedules with your healthcare provider if headaches consistently accompany dose increases.
Users tracking their progress through tirzepatide microdosing charts or semaglutide dosing charts can use these resources to plan more gradual escalation strategies.
Strategy 5: injection timing optimization
When you inject matters more than most people realize.
Many users find that injecting in the evening reduces daytime headache severity because the peak of GI side effects occurs while they sleep. Others prefer morning injections so they can actively manage any side effects that arise. There is no universally correct answer, but tracking your headache patterns relative to injection timing can reveal your optimal window.
Explore best time of day to take semaglutide for a detailed breakdown of timing strategies and their effects on side effect profiles.
Strategy 6: pre-injection meal preparation
Eating a balanced meal before your injection creates a buffer against both nausea and blood sugar drops. A meal containing lean protein, complex carbs, and healthy fats, consumed 1 to 2 hours before injection, provides your body with steady fuel to draw from as the medication takes effect.
This is especially important during the first few weeks and after any dose increase. The pre-injection meal does not need to be large. A handful of nuts, some Greek yogurt, or a small chicken breast with rice works perfectly. The goal is steady blood sugar, not a full stomach.
Strategy 7: caffeine management
Caffeine is a vasoconstrictor. In small doses, it can actually help relieve certain types of headaches, which is why many OTC headache medications include caffeine. But excessive caffeine also causes dehydration, which undermines your primary headache prevention strategy.
The sweet spot for most GLP-1 users is moderate caffeine, roughly 200 to 300 mg daily (about 2 to 3 cups of coffee). Stay above that, and the dehydrating effects start outweighing any headache relief benefits. If you typically drink more coffee than this, consider gradual reduction rather than sudden elimination, since caffeine withdrawal itself causes headaches.
Strategy 8: sleep optimization
Poor sleep increases headache frequency regardless of medication status. On GLP-1 medications, the connection strengthens because sleep deprivation impairs your body ability to regulate fluid balance, blood sugar, and inflammation, all of which contribute to headaches.
Aim for 7 to 9 hours of quality sleep. Maintain consistent sleep and wake times. If GLP-1 related nausea disrupts your sleep, consider adjusting your injection timing or discussing anti-nausea strategies with your provider. Users reporting tirzepatide fatigue should evaluate whether their fatigue-headache combination stems from inadequate sleep quality.
Strategy 9: stress and tension management
Starting a new medication is stressful. Monitoring side effects is stressful. Worrying about headaches creates tension that causes headaches. The irony is not lost on anyone who has experienced this cycle.
Progressive muscle relaxation, deep breathing exercises, gentle stretching, and regular walks all reduce the tension component of GLP-1 headaches. These are not "nice to have" additions to your protocol. For tension-type headaches, they are sometimes the most effective intervention available.
Strategy 10: alcohol limitation
Alcohol compounds every headache risk factor on GLP-1 medications. It dehydrates you further. It disrupts blood sugar regulation. It interferes with sleep quality. And it impairs liver function that metabolizes the medication.
If you are experiencing headaches on GLP-1 therapy, eliminating or significantly reducing alcohol consumption is one of the simplest high-impact changes you can make. For more on this topic, the guides on drinking on semaglutide and drinking on tirzepatide cover the specific interactions in detail.
Strategy 11: food quality focus
What you eat matters as much as whether you eat. Processed foods, high-sodium meals, excessive sugar, and foods high in tyramine (aged cheeses, cured meats, fermented foods) are all known headache triggers. When your threshold is already lowered by GLP-1 medication, these dietary triggers can push you over the edge.
Focus on whole foods. Fresh vegetables, lean proteins, complex carbohydrates, and healthy fats. The foods to avoid on tirzepatide and foods to avoid on semaglutide guides provide specific lists tailored to GLP-1 users.
Strategy 12: headache diary
Keep a simple log. Date. Time headache started. Severity (1 to 10). What you ate that day. How much water you drank. Any dose changes. Sleep quality the night before. Activity level.
Patterns emerge quickly. Maybe your headaches always happen on injection day. Maybe they correlate with days when you drank less than a liter of water. Maybe they follow nights of poor sleep. The diary transforms headaches from random events into identifiable, preventable patterns.
How to treat a GLP-1 headache right now
Prevention failed. The headache is here. Now what?
Over-the-counter medication options
Acetaminophen (Tylenol): First-line choice for most GLP-1 headaches. Effective for tension and mild migraine headaches. Maximum dosage is 3000 mg daily, but lower doses often suffice. Does not irritate the stomach, which matters when your GI system is already under stress from GLP-1 medication.
Ibuprofen (Advil, Motrin): Anti-inflammatory properties make it effective for headaches with a vascular or inflammatory component. However, it can worsen GI symptoms including nausea. Use sparingly, no more than 2 to 3 days per week, to avoid medication overuse headaches.
Aspirin: Similar profile to ibuprofen. Can be effective but carries the same GI concerns. Low-dose aspirin (325 mg) is generally better tolerated than standard doses.
Combination products: Excedrin contains acetaminophen, aspirin, and caffeine. The caffeine component provides vasoconstriction that can be particularly helpful for migraine-type GLP-1 headaches. One dose may be more effective than acetaminophen alone.
Important: always consult your healthcare provider before adding any medications to your regimen, even OTC options, to ensure there are no interactions with your specific GLP-1 medication or other drugs you may be taking.
Non-medication approaches
Cold compress on the forehead or back of the neck provides immediate, drug-free relief. Apply for 15 to 20 minutes. The cold constricts blood vessels, which directly addresses the vasodilation mechanism. For tension headaches, a warm compress on the neck and shoulders may work better by relaxing muscle tension.
Darkness and quiet help with migraine-type headaches. If you can, lie down in a cool, dark room for 20 to 30 minutes. Close your eyes. Breathe slowly and deeply. This is not laziness. It is a legitimate treatment intervention.
Gentle neck stretches and massage target tension headaches specifically. Slowly roll your neck in circles. Press your thumbs into the base of your skull where it meets your neck. Apply firm pressure for 30 seconds, release, repeat. These pressure points connect to pain pathways that, when released, can reduce headache intensity significantly.
Peppermint oil applied to the temples has documented effectiveness for tension headaches. The menthol creates a cooling sensation that can distract from pain and may have mild analgesic properties. It is not a cure, but it provides noticeable relief for many users.
Emergency hydration protocol
If you suspect dehydration is driving your headache, implement this protocol immediately.
Drink 16 to 20 ounces of water with electrolytes over 20 minutes. Not plain water, because electrolytes are needed for your body to actually retain and utilize the fluid. Follow with another 8 to 12 ounces over the next hour. Continue sipping regularly for the rest of the day.
You will not feel better immediately. Dehydration headaches take time to resolve even after rehydrating because your brain tissue needs time to rebalance. Expect 1 to 2 hours before significant improvement. If the headache has not improved after 2 to 3 hours of aggressive hydration, another mechanism is likely responsible and you should consider OTC medication or medical consultation.
GLP-1 headaches by medication (detailed comparison)
Different GLP-1 medications have different headache profiles. This section compares the three most commonly used options side by side.
Semaglutide (Ozempic and Wegovy)
Semaglutide is the most widely prescribed GLP-1 receptor agonist. Available in injectable form (Ozempic for diabetes, Wegovy for weight management) and oral form (Rybelsus), it provides weekly dosing convenience that makes it the default choice for many providers.
Headache rates scale with dosage. At the lower diabetes doses (0.25 to 1 mg weekly), headaches affect 4% to 8% of users. At the higher weight management dose (2.4 mg weekly), rates climb to 8% to 14%. The semaglutide dosage calculator can help determine appropriate starting doses based on individual factors.
Semaglutide headaches tend to peak during the first 4 to 8 weeks of treatment and during each dose increase. Most users report resolution within the first 26 weeks. Those taking semaglutide with B12 may experience slightly fewer headaches, as B12 supports neurological function and energy metabolism, though controlled studies on this combination are limited.
Oral semaglutide (Rybelsus) shows similar headache rates to injectable forms, but the daily dosing schedule means the medication level in your body fluctuates more, potentially creating a different headache pattern. Users considering oral semaglutide options should factor this difference into their planning.
Tirzepatide (Mounjaro and Zepbound)
As a dual GIP/GLP-1 receptor agonist, tirzepatide offers a different pharmacological profile. The GIP component adds metabolic benefits that may partially offset some side effects, including headaches.
Clinical trial headache rates for tirzepatide run 5% to 7% at standard doses, with spikes during titration phases. The tirzepatide dose chart shows the recommended escalation schedule designed to minimize side effects.
Tirzepatide users who experience headaches often report that they are less severe than headaches experienced on equivalent semaglutide doses, though head-to-head trials specifically measuring headache outcomes are limited. The semaglutide versus tirzepatide side effects comparison provides a comprehensive look at all adverse event profiles between these two medications.
If headaches are a primary concern, tirzepatide may offer a slight advantage based on available data. However, medication selection should consider the full picture of efficacy, side effects, cost, and individual response rather than any single side effect in isolation.
Liraglutide (Victoza and Saxenda)
Liraglutide requires daily injection rather than weekly dosing. This creates a more stable drug level in your body, which some users find produces fewer peaks and valleys of side effects. However, the daily injection routine is less convenient and requires more consistency.
Headache rates for liraglutide fall in the 6% to 10% range, comparable to mid-dose semaglutide. The daily dosing means headaches, when they occur, tend to be lower intensity but potentially more frequent, a mild background headache rather than a severe episodic one.
Medication comparison table
Factor | Semaglutide | Tirzepatide | Liraglutide |
|---|---|---|---|
Headache rate | 4-14% | 5-7% | 6-10% |
Dosing frequency | Weekly | Weekly | Daily |
Peak headache period | First 4-8 weeks | During titration | First 2-4 weeks |
Headache severity | Mild to moderate | Generally mild | Generally mild |
Resolution timeline | 2-8 weeks | 2-6 weeks | 1-4 weeks |
Dose-dependent | Yes (higher doses = more headaches) | Yes (mainly during titration) | Modest dose relationship |
When GLP-1 headaches signal something serious
Most GLP-1 headaches are benign. Annoying, uncomfortable, disruptive to your day, but not dangerous. However, certain headache patterns require immediate medical attention.
Red flags that demand attention
The "worst headache of my life": Sudden onset of the most severe headache you have ever experienced, especially if it reaches maximum intensity within seconds to minutes, requires emergency evaluation. This pattern can indicate subarachnoid hemorrhage or other vascular emergencies.
Neurological symptoms: Vision changes (blurring, double vision, loss of peripheral vision), weakness on one side of the body, numbness, difficulty speaking, or confusion alongside a headache are never normal side effects of GLP-1 medication. These warrant immediate medical evaluation.
Persistent escalation: A headache that gets progressively worse over days to weeks without responding to any intervention. Normal GLP-1 headaches fluctuate and eventually improve. Headaches that only worsen suggest an underlying issue separate from the medication.
New onset after age 50: New headache patterns starting after age 50 always warrant investigation, regardless of medication status. The differential diagnosis expands significantly with age, and attributing headaches solely to GLP-1 medication without evaluation could miss serious pathology.
When to call your healthcare provider
Contact your provider if your headaches persist beyond the expected adjustment period of 2 to 8 weeks, if they interfere with your ability to work or perform daily activities, if OTC medications provide no relief, or if you notice headaches worsening rather than improving over time.
Also contact your provider if headaches are accompanied by severe nausea and vomiting lasting more than 24 hours, signs of significant dehydration (dark urine, dizziness, rapid heartbeat), or fever. These combinations may indicate complications that require medical management beyond standard headache treatment.
Users monitoring side effects should also review related conditions like tirzepatide and anxiety, tirzepatide muscle pain, and GLP-1 hair loss to understand the broader side effect landscape and identify patterns that might inform your medical conversations.
Never stop medication abruptly
Even if headaches are severe, never discontinue your GLP-1 medication without medical guidance. Abrupt cessation can trigger rebound effects, including weight regain, blood sugar spikes in diabetic patients, and paradoxically, withdrawal headaches. Your provider can help you taper safely if discontinuation is warranted, or they may adjust your dose downward rather than stopping entirely.
The surprising flip side: when GLP-1 medications actually help headaches
Here is something most guides completely miss.
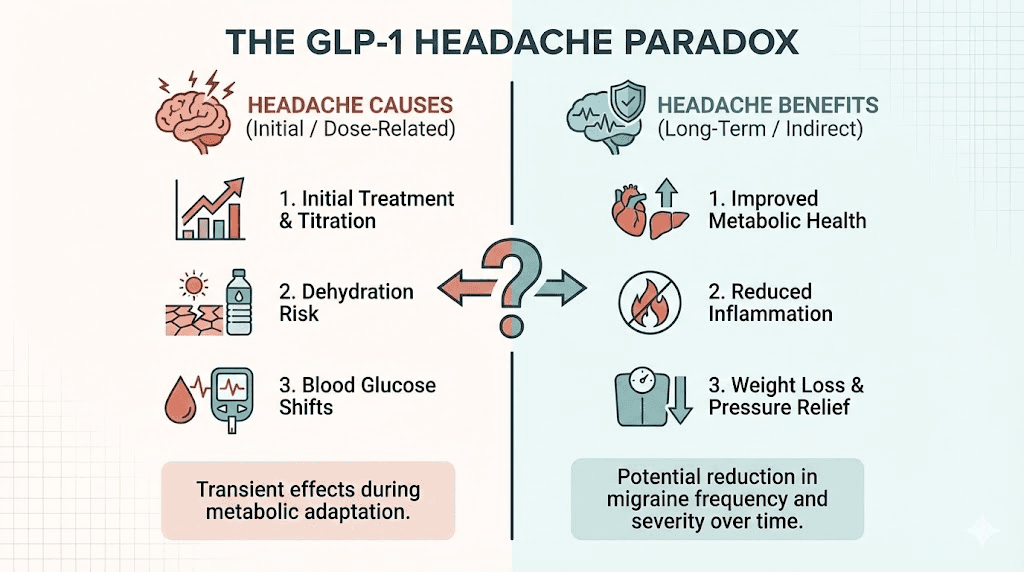
GLP-1 receptor agonists do not just cause headaches. They can also treat certain headache conditions. The science behind this paradox is fascinating and increasingly well documented.
Idiopathic intracranial hypertension improvement
Idiopathic intracranial hypertension (IIH) is a condition characterized by elevated pressure of cerebrospinal fluid around the brain. It causes severe, chronic headaches, often with visual symptoms. IIH is strongly associated with obesity, and weight loss of just 5% to 10% can significantly reduce cerebrospinal fluid pressure and headache severity.
GLP-1 receptor agonists offer a dual benefit for IIH patients. First, they promote weight loss that addresses the root cause. Second, and more interestingly, GLP-1 receptors are present in the choroid plexus, the brain tissue that produces cerebrospinal fluid. Activation of these receptors appears to directly reduce CSF secretion by inhibiting the sodium-potassium ATPase pump, lowering intracranial pressure through a mechanism entirely separate from weight loss.
Research shows that GLP-1 agents significantly reduce monthly headache days in IIH patients at 3 months and at the end of follow-up periods. For patients with IIH who also need weight management, GLP-1 medications may address both conditions simultaneously.
Migraine reduction through weight loss and anti-inflammatory mechanisms
Obesity is a major modifiable risk factor for chronic migraine. It contributes to central sensitization and exacerbates the frequency and severity of migraine attacks. By promoting sustained weight loss, GLP-1 medications can reduce migraine burden in overweight patients.
But the benefits extend beyond weight loss alone. Liraglutide stimulates secretion of IL-10, an anti-inflammatory cytokine, which alleviates migraine-like pain in animal models. GLP-1 receptor activation also suppresses pro-inflammatory cytokines including IL-1 beta and TNF alpha, both of which are upregulated during migraine attacks. Additionally, GLP-1 modulates microglial activity, reducing chronic inflammation that contributes to central sensitization.
The paradox, then, is real. GLP-1 medications can cause headaches through vascular and metabolic mechanisms in the short term while simultaneously reducing headache burden through anti-inflammatory and weight-related mechanisms in the long term. The net effect depends on the individual patient, their headache history, their weight status, and how far along they are in their treatment journey.
No studies have specifically assessed this endpoint in migraine populations yet, which represents a critical gap in the literature. But the biological rationale is compelling enough that researchers consider it a promising area for future investigation.
Connection to other GLP-1 benefits
The anti-inflammatory and neuroprotective properties of GLP-1 receptor agonists connect to broader research on these medications for neurological conditions. Users already experiencing improvements in energy levels on semaglutide may also notice improvements in headache frequency as treatment progresses. The metabolic improvements, including better glucose control, reduced inflammation, and improved cardiovascular function, create an environment where headache triggers gradually diminish even as the direct medication effects that cause headaches also wane.
How to tell if your headache is from GLP-1 medication
Not every headache that happens while you are on a GLP-1 medication is caused by the medication. People get headaches for dozens of reasons. Stress. Weather changes. Eye strain. Hormonal fluctuations. Illness. Poor posture. The challenge is distinguishing a medication-related headache from one that would have happened regardless.
Timing correlation
GLP-1 related headaches follow predictable timing patterns. They tend to appear within 24 to 72 hours of injection, during the first few weeks of a new dose, or on days when fluid intake drops significantly. If your headaches follow these patterns consistently, the medication is likely involved.
Headaches that appear at random intervals with no connection to injection timing, dose changes, or hydration status are less likely to be medication-related. A headache diary (strategy 12 from the prevention section) is the most reliable way to identify these patterns. After 2 to 3 weeks of logging, the data usually tells a clear story.
Response to interventions
GLP-1 related headaches typically respond to hydration, electrolyte replacement, and blood sugar stabilization. If drinking 16 to 20 ounces of electrolyte water relieves your headache within 1 to 2 hours, dehydration was almost certainly the cause. If eating a balanced meal resolves it, blood sugar was the culprit.
Headaches that do not respond to any of these interventions may have a different origin. They could be tension headaches from stress, migraines triggered by weather or hormonal changes, or headaches from other medications or health conditions. These deserve separate evaluation rather than being automatically attributed to your GLP-1 therapy.
Character and location
GLP-1 dehydration headaches usually present as bilateral pressure, felt equally on both sides. Blood sugar headaches tend to concentrate behind the eyes. Vascular headaches from GLP-1 receptor activation may mimic migraines with unilateral throbbing. Knowing these characteristic presentations helps you match your headache to its likely cause and choose the most effective treatment response.
Context clues
Ask yourself these questions when a headache strikes. Did I drink enough water today? When did I last eat? Am I within 48 hours of an injection or dose change? Did I sleep poorly last night? Have I been under unusual stress? The answers will often point directly to the cause, whether medication-related or not.
Users exploring the complete side effect landscape can reference guides on semaglutide appetite suppression timelines and tirzepatide onset of action to understand when medication effects peak and how those peaks might correlate with headache episodes.
Next-generation GLP-1 medications and headache considerations
The GLP-1 medication landscape is evolving rapidly. Newer agents with different receptor profiles are entering clinical trials and approaching market availability. Understanding their headache implications matters for users planning their treatment journey.
Retatrutide (triple receptor agonist)
Retatrutide activates three receptors: GLP-1, GIP, and glucagon. This triple action produces faster weight loss in clinical trials than any dual or single agonist studied to date. But more receptor activation means more potential for side effects, including headaches.
Early trial data shows gastrointestinal side effects are common during retatrutide dose escalation, which suggests headache profiles will likely mirror or exceed those seen with tirzepatide. The glucagon receptor component adds a metabolic dimension that could independently influence blood sugar stability and headache risk.
Users interested in retatrutide should review the retatrutide versus semaglutide comparison for context on how this newer agent stacks up against established options. The retatrutide dosage chart and dose schedule outline the titration approach designed to minimize adverse effects during treatment initiation.
Oral GLP-1 formulations
The shift from injectable to oral delivery represents a major change in how GLP-1 medications are absorbed and distributed. Oral tirzepatide and other oral formulations create different pharmacokinetic profiles than injections. Peak drug levels may be lower but more frequent, potentially producing a different headache pattern.
The tirzepatide oral versus injection comparison and tablets versus injections analysis explore the practical differences between delivery methods, including side effect profiles. Early evidence suggests oral formulations may cause fewer injection-site-related headaches while potentially increasing GI-mediated headaches due to direct gut exposure.
Combination compounds
Compounding pharmacies increasingly offer GLP-1 medications combined with complementary ingredients. Tirzepatide with niacinamide, semaglutide with B12, and tirzepatide with glycine are among the most popular combinations.
Each additive brings its own profile. Niacinamide can cause flushing that some users mistake for headache-related symptoms. B12 supports neurological function and may reduce headache susceptibility. Glycine offers neuroprotective benefits that could dampen pain signaling. Understanding what your specific compound contains helps you predict and manage potential headache patterns.
The tirzepatide B12 combination guide provides detailed information on how these additives interact with the primary medication and influence the overall side effect profile.
Special considerations for different user groups
Users combining GLP-1 medications with other treatments
Combining GLP-1 medications with other therapies can alter headache risk in both directions. Users taking phentermine with semaglutide may experience increased headache frequency because phentermine itself lists headache as a common side effect. The combination creates additive headache risk that requires more aggressive prevention strategies.
Similarly, users taking semaglutide with glycine or tirzepatide with glycine may find that glycine neuroprotective properties help mitigate headache severity. Glycine functions as an inhibitory neurotransmitter that can calm overactive pain signaling pathways.
B12 combinations are particularly relevant. Both semaglutide with methylcobalamin and tirzepatide with glycine and B12 may support neurological function in ways that reduce headache susceptibility. B12 deficiency itself causes headaches, and GLP-1 medications can impair B12 absorption by altering gastric function. Supplementation addresses this potential deficiency before it becomes symptomatic.
Users transitioning between medications
Switching from one GLP-1 to another creates a unique headache risk window. Users switching from tirzepatide to semaglutide or vice versa may experience a temporary increase in headaches during the transition period. Your body adjusted to one receptor activation pattern and now must readjust to a different one.
The conversion chart between semaglutide and tirzepatide provides dosing equivalencies that help smooth transitions. Starting the new medication at a lower equivalent dose and titrating up gradually reduces the likelihood of severe transition headaches.
Users on compounded formulations
Compounded GLP-1 medications may have different excipient profiles, concentrations, and absorption characteristics compared to brand-name products. These differences can affect side effect timing and severity. Users taking compounded semaglutide or compounded tirzepatide should pay extra attention to headache patterns and ensure their compounding pharmacy provides consistent, high-quality product.
Proper storage also matters. Degraded medication can cause unpredictable side effects. Ensure you follow proper storage guidelines, as outlined in resources covering semaglutide refrigeration requirements and tirzepatide storage needs.
Building a complete headache management protocol
Putting it all together. Here is a structured approach that addresses prevention, identification, treatment, and escalation.
Daily prevention routine
Morning: 16 to 20 ounces of water with electrolytes immediately upon waking. Balanced breakfast within 1 hour, even if small. Track hydration start.
Midday: Continue hydration (target 1 liter by noon). Second meal with protein, carbs, and fat. Brief walk or stretching if possible.
Afternoon: Third hydration check (target 1.5 liters by 3 PM). Healthy snack if appetite allows. Note any headache onset or changes.
Evening: Final hydration push (target 2 to 3 liters by bedtime). Dinner with balanced macronutrients. Log the day headache status, water intake, and any notes.
Injection day protocol
Pre-injection: balanced meal 1 to 2 hours before. Extra hydration throughout the day. Have acetaminophen available as needed.
Post-injection: continue aggressive hydration for 48 hours. Eat regular small meals even if appetite drops. Rest if possible. Avoid alcohol for at least 24 to 48 hours.
Users who need guidance on injection technique and timing should review the GLP-1 injection guide and injection site selection resources to ensure proper medication delivery.
Dose increase protocol
Week before increase: establish optimal hydration habits. Stock up on electrolyte supplements. Plan meals for the coming week. Clear your schedule of demanding commitments if possible during the first 3 to 5 days after the increase.
Week of increase: maximum hydration. Frequent small meals. Minimize headache triggers (alcohol, poor sleep, stress, excessive caffeine). Have both acetaminophen and cold compresses ready.
Week after increase: maintain heightened prevention for at least 7 days. If headaches persist beyond 7 to 10 days, consider contacting your provider about a possible temporary dose reduction before trying the increase again.
Escalation pathway
Level 1 (mild headache): hydration, rest, cold compress. No medication needed.
Level 2 (moderate headache): add acetaminophen 500 to 1000 mg. Continue hydration. Rest in dark, quiet room if possible.
Level 3 (severe headache): combination OTC therapy (acetaminophen plus caffeine). Aggressive electrolyte replacement. If no improvement in 2 to 3 hours, consider ibuprofen.
Level 4 (persistent or worsening): contact healthcare provider. Do not continue managing at home if headaches are severe, persistent, or accompanied by neurological symptoms.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, protocol tracking tools, and a community of thousands who have navigated these exact questions. Members access detailed side effect management protocols, dosing calculators like the semaglutide dosage calculator and peptide calculator, and expert guidance for troubleshooting issues just like GLP-1 headaches.
The role of reconstitution and preparation in headache prevention
For users working with compounded or research-grade formulations, proper reconstitution directly affects side effect profiles. Incorrectly reconstituted medication can create concentration variations that lead to inconsistent dosing, which in turn causes unpredictable spikes in side effects including headaches.
Getting the bacteriostatic water ratio right matters. Too little diluent creates a highly concentrated solution where small measurement errors translate to large dose variations. Too much diluent makes accurate dosing difficult with standard syringes. Resources on semaglutide reconstitution, tirzepatide reconstitution, and bacteriostatic water mixing ratios provide the exact calculations needed for consistent preparation.
The peptide reconstitution calculator eliminates guesswork by calculating exact volumes based on your vial concentration and desired dose per injection. Consistent dosing means consistent side effects, which means predictable headache patterns that you can prevent rather than react to.
Understanding the relationship between GLP-1 headaches and other side effects
Headaches do not exist in isolation. They connect to other GLP-1 side effects through shared mechanisms, and addressing one often improves the others.
Headache and fatigue: Both share dehydration and blood sugar instability as common causes. Users experiencing both GLP-1 fatigue and headaches should prioritize hydration and nutrition, as these interventions address both symptoms simultaneously.
Headache and constipation: GLP-1 medications slow GI transit, causing constipation in many users. Dehydration worsens constipation, and constipation can contribute to headaches through toxin accumulation and general malaise. Adequate fiber and fluid intake addresses both. The semaglutide constipation treatment guide and tirzepatide constipation treatment guide provide specific protocols.
Headache and nausea: These two symptoms create a vicious cycle. Nausea reduces fluid and food intake. Reduced intake causes dehydration and blood sugar drops. Both dehydration and blood sugar drops cause headaches. And headaches worsen nausea. Breaking this cycle requires addressing the nausea first, through proper medication timing, anti-nausea strategies, and dietary adjustments.
Headache and weight loss plateaus: Users who hit a weight loss plateau on semaglutide or tirzepatide sometimes request dose increases, which then trigger headaches. Understanding that plateaus are a normal part of the weight loss process can prevent unnecessary dose escalation and the headaches that come with it.
Long-term outlook for GLP-1 headache sufferers
The trajectory is almost always positive. And understanding this trajectory can provide the psychological reassurance that helps you push through the uncomfortable early weeks rather than abandoning treatment prematurely.
Short term (weeks 1 to 8): highest headache risk. Adjustment period. Prevention strategies essential. OTC treatment may be needed regularly.
Medium term (months 2 to 6): headache frequency and severity decrease substantially. Most users report significant improvement. Prevention habits are established and become routine.
Long term (6 months and beyond): headaches are rare for the vast majority of users. The body has fully adapted. The anti-inflammatory and metabolic benefits of treatment may actually reduce baseline headache frequency below pre-treatment levels, especially for users who have lost significant weight.
These adverse effects rarely lead to treatment discontinuation, unlike more severe adverse effects such as pancreatitis or severe GI reactions. Headaches are manageable, temporary, and should not be the primary reason anyone avoids or discontinues GLP-1 therapy. The benefits of treatment, including weight loss, improved metabolic health, cardiovascular protection, and enhanced quality of life, overwhelmingly outweigh the transient headache risk for most users. Every week that passes brings your body closer to full adaptation, and the headaches that felt overwhelming during week one often become a distant memory by month three.
What helps most during the difficult early period is having a clear plan. Know your hydration targets. Know your meal schedule. Know which OTC medication to reach for. Know when to call your provider. When headaches feel unpredictable and uncontrollable, structure restores your sense of agency. And agency, as it turns out, is one of the most effective headache treatments available.
Users on longer-term protocols who want to understand how long to stay on semaglutide should know that headache burden decreases over time and should not factor heavily into decisions about treatment duration.
Frequently asked questions
Do all GLP-1 medications cause headaches?
All GLP-1 receptor agonists list headache as a potential side effect, including semaglutide, tirzepatide, liraglutide, exenatide, and dulaglutide. Headache rates range from 4% to 14% depending on the specific medication and dosage. However, not every user experiences headaches. The majority of users do not report significant headache issues, and those who do typically find them transient and manageable.
Will my GLP-1 headache go away on its own?
In most cases, yes. Research describes GLP-1 headaches as generally mild, nondisabling, and most frequently occurring within the first 26 weeks of treatment. Most users see improvement within 2 to 8 weeks. Individual headache episodes typically resolve within hours to days. If headaches persist beyond 8 weeks or worsen over time, consult your healthcare provider.
Can I take ibuprofen while on semaglutide or tirzepatide?
Ibuprofen is generally safe for occasional use with GLP-1 medications but should be used sparingly, no more than 2 to 3 days per week. Ibuprofen can irritate the stomach lining, and GLP-1 medications already affect gastrointestinal function. Acetaminophen is typically the preferred first-line option because it does not carry the same GI risks. Always check with your healthcare provider before adding any medication to your regimen.
Does the headache mean my GLP-1 medication is working?
Not directly. Headaches indicate your body is responding to the medication, but they are a side effect rather than a marker of efficacy. You can experience full therapeutic benefit from GLP-1 therapy without ever having a headache. Conversely, severe headaches do not mean the medication is working better. They typically mean your hydration, nutrition, or dose titration needs adjustment.
Is a headache after my first GLP-1 injection normal?
Common and expected for a subset of users. First injection headaches occur because your body has never experienced exogenous GLP-1 receptor activation at therapeutic levels. The headache typically resolves within 1 to 3 days. Proactive hydration, balanced meals, and having acetaminophen available can minimize the impact. If the headache is severe or accompanied by neurological symptoms, contact your provider.
Should I reduce my dose if I get headaches every time I increase?
Discuss this with your provider. Some users benefit from extended titration schedules, staying at each dose level for 6 to 8 weeks instead of the standard 4 weeks. Others may find that temporarily reducing the dose and then reattempting the increase with better prevention strategies resolves the issue. Using resources like the tirzepatide dosage calculator can help determine appropriate intermediate doses for more gradual escalation.
Can dehydration from GLP-1 medications cause severe headaches?
Yes. Dehydration is the most common cause of GLP-1 related headaches, and severe dehydration can produce severe headaches. If you are experiencing intense headaches alongside dark urine, dizziness, rapid heartbeat, or dry mouth, you may be significantly dehydrated. Aggressive rehydration with electrolyte-containing fluids is the immediate intervention. If symptoms persist, seek medical attention.
Do GLP-1 headaches get worse with higher doses?
Generally, yes. Higher doses of GLP-1 medications are associated with increased headache rates. Semaglutide at weight management doses (2.4 mg) shows headache rates of 8 to 14%, compared to 4 to 8% at lower diabetes doses. However, this relationship is not linear, and individual response varies. Many users who experience headaches at lower doses do not necessarily experience worse headaches at higher doses, especially if they implement effective prevention strategies.
External resources
Hemiplegic migraines exacerbated using an injectable GLP-1 agonist for weight loss (PMC case report)
In case I do not see you, good afternoon, good evening, and good night. May your hydration stay consistent, your headaches stay brief, and your GLP-1 results stay worth every adjustment along the way.