Feb 12, 2026

What if the reason your semaglutide results are inconsistent has nothing to do with the peptide itself? What if the problem is sitting right there in your reconstitution step, hiding in plain sight, costing you potency every single week?
It happens more often than you would think. A researcher pulls out a 5mg vial of semaglutide, grabs a bottle of bacteriostatic water, and then freezes. How much water goes in? Two milliliters? Three? Five? The wrong answer does not just make math harder. It changes the concentration of every single dose you draw from that vial. Too much water and you are injecting larger volumes for the same dose. Too little and you are working with concentrations so high that tiny measurement errors become magnified into real dosing problems.
This guide exists because that moment of uncertainty should never happen again. We are going to walk through every common reconstitution ratio for a 5mg semaglutide vial, show you the exact concentrations each one produces, explain how to calculate your dose in units on an insulin syringe, and cover the storage rules that keep your reconstituted solution stable for weeks. Whether you are working with semaglutide for the first time or switching from a 10mg vial to a 5mg vial and need to recalibrate your approach, SeekPeptides has built this resource to make the math disappear. No guesswork. No wasted peptide. Just clean, accurate reconstitution every time.
Why the amount of bacteriostatic water matters
Reconstitution is not just about dissolving powder. It is about creating a solution at a specific concentration that makes accurate dosing possible. The amount of bacteriostatic water you add to your 5mg semaglutide vial directly determines three things: the concentration of the final solution in milligrams per milliliter, the volume you need to draw for each dose, and how easy or difficult it is to measure that volume accurately on your syringe.
Think of it this way.
If you add 2mL of bacteriostatic water to a 5mg vial, your concentration is 2.5mg/mL. That means every 0.1mL (10 units on a U-100 insulin syringe) contains 0.25mg of semaglutide. Clean numbers. Easy math. Minimal room for error.
But if you add 1mL to that same vial, the concentration jumps to 5mg/mL. Now every single unit on your syringe represents 0.05mg. A tiny measurement difference of just 2-3 units means you are off by 0.1-0.15mg. For someone on a 0.25mg weekly dose, that is a 40-60% dosing error from a nearly invisible syringe misread. These kinds of mistakes cascade through an entire semaglutide protocol without the researcher ever realizing what went wrong.
The relationship between water volume and dosing accuracy is not linear either. Higher concentrations require smaller injection volumes, which demand more precise syringe technique. Lower concentrations require larger volumes but offer more forgiving measurements. Finding the right balance depends on your specific dosing needs and the syringes you have available.
The four most common reconstitution ratios for 5mg semaglutide
There is no single correct amount of bacteriostatic water for a 5mg vial. Different ratios serve different purposes. Here are the four most practical options, each with its own advantages, and the math that makes them work with standard insulin syringes.
Option 1: 2mL of bacteriostatic water (most popular)
This is the ratio most researchers choose, and for good reason. Adding 2mL of bacteriostatic water to a 5mg vial produces a concentration of 2.5mg/mL. The math works out cleanly on a U-100 insulin syringe.
At this concentration, each unit on your syringe equals 0.025mg of semaglutide. A standard starting dose of 0.25mg requires drawing to the 10-unit mark. A dose of 0.5mg means 20 units. The numbers are round, memorable, and hard to get wrong even when you are half asleep on injection day.
This ratio also gives you exactly 20 doses of 0.25mg from a single vial. That is 20 weeks at the starting dose, or 10 weeks if you have titrated up to 0.5mg. For researchers running a standard titration schedule, 2mL is the sweet spot between concentration and practicality.
Option 2: 1mL of bacteriostatic water (high concentration)
Adding just 1mL creates a concentration of 5mg/mL. This is the most concentrated option and produces the smallest injection volumes. Your 0.25mg dose requires only 5 units on the syringe. Your 0.5mg dose requires 10 units.
The advantage is minimal injection volume. Less liquid under the skin means less chance of irritation at the injection site. Some researchers prefer this when they are injecting multiple peptides in the same session and want to keep total volume low.
The disadvantage is significant. At 5mg/mL, every unit on your syringe represents 0.05mg. If your syringe reading is off by even 2 units, your dose is off by 0.1mg. On a 0.25mg dose, that is a 40% error. This ratio demands exceptional syringe technique and preferably a syringe with half-unit markings. It is not ideal for beginners.
Option 3: 2.5mL of bacteriostatic water (simplest math)
Adding 2.5mL produces a concentration of exactly 2mg/mL. Some researchers love this ratio because the concentration number itself is so clean. Every 0.1mL contains exactly 0.2mg. Every 0.05mL contains exactly 0.1mg.
On a U-100 syringe, your 0.25mg dose falls at 12.5 units. That half-unit can be slightly tricky to measure without a syringe that has half-unit markings, but the overall math remains straightforward. For a 0.5mg dose, you draw 25 units. For the maximum 2.4mg dose, you need 120 units, which actually exceeds a standard 100-unit syringe. This ratio works best for lower doses in the early titration phases.
Option 4: 5mL of bacteriostatic water (most forgiving)
This is the 1:1 ratio, producing a concentration of 1mg/mL. Every 0.1mL on your syringe contains exactly 0.1mg. The math could not be simpler.
A 0.25mg dose requires 25 units. A 0.5mg dose requires 50 units. Even at higher doses like 1mg (100 units), you stay within the range of a standard syringe. The measurement forgiveness at this concentration is excellent since being off by a unit only changes your dose by 0.01mg.
The trade-off is volume. At higher therapeutic doses, you are injecting half a milliliter or more per shot. Some researchers find larger volumes uncomfortable, and the storage duration becomes a consideration since you are pulling more liquid from the vial each week.
Complete concentration and dosing reference chart
This table shows exactly what happens at each reconstitution ratio. Find your water volume on the left, then read across to see what each common dose looks like on your insulin syringe in units.
BAC Water Added | Concentration | 0.25mg Dose | 0.5mg Dose | 1mg Dose | 1.7mg Dose | 2.4mg Dose |
|---|---|---|---|---|---|---|
1mL | 5mg/mL | 5 units | 10 units | 20 units | 34 units | 48 units |
2mL | 2.5mg/mL | 10 units | 20 units | 40 units | 68 units | 96 units |
2.5mL | 2mg/mL | 12.5 units | 25 units | 50 units | 85 units | 120 units |
5mL | 1mg/mL | 25 units | 50 units | 100 units | 170 units | 240 units |
Notice something important about the higher doses. With 2.5mL or 5mL of water, the 1.7mg and 2.4mg doses require drawing volumes that exceed a standard 100-unit (1mL) syringe. This means you would either need a larger syringe or split your dose into two injections. For researchers who plan to titrate to higher doses, the 2mL reconstitution ratio is typically the best choice because it keeps all standard doses within the range of a single syringe draw.
The 2mL option also maximizes the useful life of the vial. At 0.25mg per week, a single 5mg vial lasts 20 weeks. At 0.5mg per week, 10 weeks. At 1mg, 5 weeks. At the maximum 2.4mg dose, just over 2 weeks. Track your dose progression against these numbers to know exactly when you will need your next vial.
Step-by-step reconstitution instructions
Knowing the right ratio is only half the equation. The reconstitution technique itself determines whether your semaglutide maintains full potency or degrades before you even draw your first dose. Follow these steps exactly, every time.
What you need before starting
Gather everything before you begin. You do not want to pause mid-reconstitution to hunt for supplies. Here is the complete list:
One 5mg semaglutide lyophilized vial
One vial of bacteriostatic water (0.9% benzyl alcohol)
One sterile syringe for reconstitution (1mL or 3mL)
Alcohol swabs (at least 2)
Clean, flat work surface
Permanent marker for labeling
Do not use sterile water for injection unless you plan to use the entire vial in a single dose. Sterile water contains no preservative. Once opened, bacteria can colonize the solution within hours. Bacteriostatic water contains benzyl alcohol that inhibits bacterial growth, allowing safe multi-dose use over 28 days.
Step 1: clean both vial tops
Swab the rubber stopper on both the semaglutide vial and the bacteriostatic water vial with separate alcohol pads. Use firm, circular motions. Let the alcohol evaporate completely before proceeding. This takes about 30 seconds. Skipping this step is the fastest way to introduce contamination into your solution.
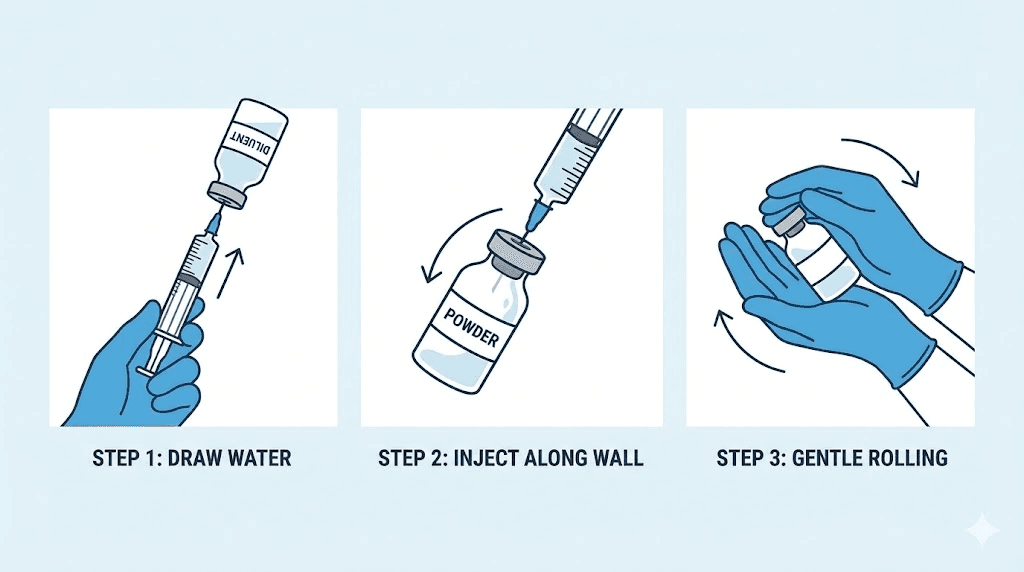
Step 2: draw the bacteriostatic water
Using a sterile syringe with needle attached, draw air equal to the volume of water you plan to add. If you are using the 2mL ratio, draw 2mL of air. Insert the needle into the bacteriostatic water vial and push the air in. This equalizes pressure and makes drawing the water much easier. Now invert the vial and slowly pull back the plunger to your target volume. Remove the syringe and check for air bubbles. Tap the barrel gently to move bubbles to the top and push them out with a tiny plunger press.
Step 3: add water to the semaglutide vial (the critical step)
This is where most reconstitution errors happen. Insert the needle through the rubber stopper of the semaglutide vial. Here is what matters: aim the needle at the glass wall of the vial, not directly at the lyophilized powder cake at the bottom.
Press the plunger slowly. Let the water trickle down the inside wall of the vial. This should take 15-20 seconds for 2mL. Never spray water directly onto the powder. The force of a direct stream can denature the peptide chains, reducing potency before you have even started. This single technique detail separates a properly reconstituted vial from a compromised one.
Step 4: dissolve gently
Do not shake the vial. Ever. Shaking introduces mechanical stress and creates air bubbles, both of which can damage the peptide structure. Instead, hold the vial between your palms and gently roll it back and forth. Or tilt it slowly at a 45-degree angle and rotate. The powder should dissolve completely within 2-5 minutes, creating a clear, colorless solution.
If you see particles floating after 10 minutes of gentle mixing, something went wrong. The powder may have degraded before reconstitution, or the water temperature was too extreme. Do not use a solution that remains cloudy or contains visible particles. For proper reconstitution technique across all peptides, consistent gentle mixing is the universal rule.
Step 5: label and store
Write the following on the vial with a permanent marker: the date of reconstitution, the concentration (for example, 2.5mg/mL), and the total volume added. Store immediately in the refrigerator at 2-8 degrees Celsius (36-46 degrees Fahrenheit). Keep the vial upright and away from light. Reconstituted semaglutide remains stable for up to 28 days when stored properly.
How to calculate your dose in syringe units
Once your vial is reconstituted, you need to convert your prescribed milligram dose into units on your insulin syringe. This is where the reconstitution ratio pays off. The formula is simple, but getting it wrong means getting your dose wrong every single week.
The universal formula
Dose in mL = desired dose in mg divided by concentration in mg/mL.
Then convert mL to units: multiply mL by 100 (on a U-100 syringe).
For example, at 2.5mg/mL concentration (2mL of water added to 5mg vial):
0.25mg dose: 0.25 / 2.5 = 0.1mL = 10 units
0.5mg dose: 0.5 / 2.5 = 0.2mL = 20 units
1.0mg dose: 1.0 / 2.5 = 0.4mL = 40 units
1.7mg dose: 1.7 / 2.5 = 0.68mL = 68 units
2.4mg dose: 2.4 / 2.5 = 0.96mL = 96 units
Save yourself the math each week by using the SeekPeptides semaglutide dosage calculator. Enter your vial size, water volume, and desired dose, and it returns the exact number of units to draw. No mental arithmetic. No conversion errors. Just accurate dosing every time.
What if you are using a 0.5mL syringe?
Some researchers prefer 0.5mL (50-unit) insulin syringes because the graduation marks are closer together, allowing for more precise readings. The conversion is the same. Each unit still represents 0.01mL. But the syringe maxes out at 50 units (0.5mL), which limits the doses you can draw in a single pull.
At 2.5mg/mL, a 0.5mL syringe covers doses up to 1.25mg (50 units). For anything higher, you would need to either switch to a 1mL syringe or draw two separate injections. Many researchers find the precision trade-off worthwhile during the early titration phases when they are working with smaller doses.
Dealing with the standard titration schedule
The standard semaglutide titration follows a step-up protocol designed to minimize gastrointestinal side effects. Starting at 0.25mg weekly for the first four weeks, then increasing to 0.5mg for weeks 5-8, then to 1mg for weeks 9-12, and continuing to step up through 1.7mg and 2.4mg at four-week intervals.
With a 5mg vial reconstituted at 2mL (2.5mg/mL), here is how the math works across the full titration:
Weeks | Dose | Units per Injection | Doses from 5mg Vial |
|---|---|---|---|
1-4 | 0.25mg | 10 units | 20 doses |
5-8 | 0.5mg | 20 units | 10 doses |
9-12 | 1.0mg | 40 units | 5 doses |
13-16 | 1.7mg | 68 units | ~2.9 doses |
17+ | 2.4mg | 96 units | ~2.1 doses |
At the starting dose, a single 5mg vial lasts nearly five months. At the maintenance dose of 2.4mg, it lasts barely two weeks. Planning your vial purchases around your titration schedule prevents interruptions in your protocol. Understanding how semaglutide works over time helps you appreciate why consistent dosing matters through each phase.
Why bacteriostatic water and not sterile water
This distinction matters more than most researchers realize. Both dissolve the lyophilized powder just fine. Both produce a clear, injectable solution. But what happens after reconstitution is where the two diverge dramatically.
The preservative difference
Bacteriostatic water contains 0.9% benzyl alcohol. This preservative actively inhibits bacterial growth within the solution. Every time you puncture the rubber stopper to draw a dose, you introduce a microscopic pathway for potential contamination. The benzyl alcohol suppresses any bacteria that enter through that pathway, keeping the solution safe for repeated use over 28 days.
Sterile water contains no preservative. It is sterile at the moment of manufacture and remains sterile until the seal is broken. Once you puncture the stopper, contamination risk begins immediately. Sterile water is designed for single-use applications only. Using it for a multi-dose vial is asking for bacterial growth in a protein-rich solution. That is not a risk worth taking.
Stability implications
Research indicates that semaglutide reconstituted with bacteriostatic water maintains stability for 28 days when refrigerated at 2-8 degrees Celsius. Some studies suggest the peptide may remain viable beyond that window, but 28 days is the conservative standard most protocols follow. After 28 days, even with proper refrigeration, both the preservative effectiveness and the peptide stability begin declining.
With sterile water, the usable window shrinks to a single session. Any leftover solution should be discarded. For a 5mg vial where you might draw 10-20 individual doses, using sterile water would waste the vast majority of your peptide. The cost calculation is straightforward: a $3 vial of bacteriostatic water saves hundreds of dollars in peptide waste.
What about normal saline?
Normal saline (0.9% sodium chloride) is sometimes suggested as a reconstitution option. While it dissolves the powder effectively, it lacks the antimicrobial properties of bacteriostatic water. The sodium chloride does not prevent bacterial growth. For multi-dose peptide vials, bacteriostatic water remains the clear standard. For detailed guidance on mixing peptides with bacteriostatic water, the principles apply universally across all reconstituted peptides.
Common reconstitution mistakes that destroy potency
Semaglutide is a 31-amino-acid peptide. Its biological activity depends entirely on the integrity of that amino acid chain. Reconstitution mistakes do not just reduce potency. They can eliminate it entirely, leaving you injecting an expensive solution that does nothing.
Mistake 1: spraying water directly onto the powder
The lyophilized powder cake at the bottom of your vial looks sturdy. It is not. The peptide chains within that cake are held in a fragile crystalline structure. Directing a stream of water at them creates hydraulic force that can physically shear the peptide bonds apart. The solution still looks clear. The semaglutide concentration still tests correctly. But a percentage of those broken chains are now biologically inactive fragments that your body cannot use.
Always aim the needle at the vial wall. Let gravity do the work. Patience here costs you 15 extra seconds and saves you the full potency of your vial.
Mistake 2: shaking to dissolve faster
Shaking creates two problems simultaneously. First, the mechanical agitation subjects peptide chains to shear forces at the liquid-air interface. Protein molecules are naturally attracted to these interfaces and can unfold (denature) when forced against them repeatedly. Second, shaking creates foam. Foam dramatically increases the surface area of that liquid-air interface, multiplying the denaturation effect.
Gentle swirling achieves the same dissolution result with none of the damage. If the powder does not dissolve after 5 minutes of gentle rolling, the vial may have been improperly stored before reconstitution. Check whether your peptide storage conditions are correct before attempting to dissolve a stubborn powder cake.
Mistake 3: using water that is too cold or too warm
Bacteriostatic water should be at room temperature when you add it to the vial. Cold water slows dissolution and can cause the powder to clump rather than dissolve evenly. Hot water denatures peptides on contact. Anything above 35 degrees Celsius begins compromising the peptide structure. Room temperature, between 20-25 degrees Celsius, is the target.
If your bacteriostatic water has been refrigerated, let it sit at room temperature for 15-20 minutes before reconstitution. This small wait protects the peptide you paid for.
Mistake 4: skipping alcohol swabs
Every puncture of a rubber stopper is a potential contamination event. The needle passes through air containing bacteria, through the rubber which may have surface contaminants, and into a protein-rich solution that bacteria love to colonize. Swabbing with alcohol before every single puncture is not optional safety theater. It is the primary barrier between a clean solution and a contaminated one.
Some researchers skip the swab after the first few draws, figuring the bacteriostatic water preservative will handle any contamination. The benzyl alcohol is a backup, not a primary defense. It inhibits growth but does not sterilize. A heavy contamination load can overwhelm the preservative capacity. Swab every time. This is basic peptide safety that applies to every reconstituted product.
Mistake 5: incorrect volume measurement
Air bubbles in the syringe barrel displace liquid volume. If you have a large bubble sitting above the water line when you draw from the bacteriostatic water vial, you are adding less water than you think. That means your concentration is higher than calculated. Every dose you draw afterward will be slightly stronger than intended.
Conversely, if you accidentally add extra water, every dose is weaker. For a once-weekly peptide like semaglutide where consistent dosing drives therapeutic response, these errors accumulate over the life of the vial. Take the extra 30 seconds to tap bubbles out and verify your volume before injecting into the semaglutide vial.
Comparing 5mg vials to 10mg vials
Many researchers switch between vial sizes as they titrate through the standard semaglutide protocol. Understanding how reconstitution math changes between the two prevents costly confusion.
The math side by side
Factor | 5mg Vial + 2mL BAC Water | 10mg Vial + 2mL BAC Water |
|---|---|---|
Concentration | 2.5mg/mL | 5mg/mL |
0.25mg dose | 10 units | 5 units |
0.5mg dose | 20 units | 10 units |
1.0mg dose | 40 units | 20 units |
2.4mg dose | 96 units | 48 units |
Total doses at 0.25mg | 20 | 40 |
Vial duration at 1mg/week | 5 weeks | 10 weeks |
The 10mg vial with 2mL of water produces the same concentration that a 5mg vial with 1mL produces: 5mg/mL. If you are comfortable with higher concentrations and have steady hands with a syringe, the 10mg vial offers better value per milligram. If you prefer more forgiving measurements, the 5mg vial with 2mL gives you a lower concentration with larger, easier-to-read unit markings on your syringe.
For a detailed breakdown of reconstitution math with larger vials, see the complete guide on mixing bacteriostatic water with 10mg semaglutide. The principles are identical. Only the numbers change.
When to use 5mg vials versus 10mg vials
Choose the 5mg vial when you are in the early titration phases (0.25-0.5mg weekly). The vial lasts long enough at these low doses that stability is never a concern within the 28-day window. A single 5mg vial covers 10-20 weeks of your starting phase.
Switch to 10mg vials when you reach the higher maintenance doses (1.7-2.4mg weekly). At these doses, you burn through a 5mg vial in about two weeks. A 10mg vial gives you roughly a month at the same dose, which aligns better with the 28-day stability window after reconstitution. This matching of vial size to dose requirements minimizes waste and ensures you are always working with fresh solution.
Storage rules after reconstitution
Your reconstituted semaglutide solution is a dissolved protein in water. Like all proteins in solution, it degrades over time through multiple mechanisms. Proper storage slows these processes and maintains potency throughout the usable life of the vial.
Temperature requirements
Refrigerate immediately after reconstitution. The target range is 2-8 degrees Celsius (36-46 degrees Fahrenheit). Standard refrigerator temperature, not the door shelf where temperatures fluctuate, but the main compartment where the temperature stays consistent. The back of the middle shelf typically offers the most stable temperature in most household refrigerators.
Never freeze reconstituted semaglutide. Freezing creates ice crystals that physically damage peptide structures. The lyophilized powder form can tolerate freezing because the water has already been removed. Once reconstituted, the solution must stay liquid. A frozen vial of reconstituted semaglutide should be discarded. The damage is irreversible.
Light protection
Semaglutide degrades when exposed to UV light. The peptide bonds absorb UV energy and can break. Store your vial in the original packaging or wrap it in aluminum foil if the packaging has been discarded. Do not leave reconstituted vials on a countertop near a window or under bright lights for extended periods. Even brief UV exposure during dose drawing is fine. It is prolonged, cumulative exposure that causes measurable degradation.
The 28-day rule
Discard any remaining solution 28 days after reconstitution, regardless of how much is left. This applies even if the solution still looks clear and the vial has been stored perfectly. After 28 days, the bacteriostatic preservative begins losing effectiveness. Simultaneously, even well-stored peptides undergo gradual hydrolysis, a chemical reaction with water that cleaves peptide bonds and creates inactive fragments.
If you find yourself consistently discarding leftover solution, re-evaluate your reconstitution ratio or vial size. Wasting peptide is wasting money. Align your vial size with your dose so that you use the full vial within the 28-day window. For longer-term semaglutide storage considerations, the 28-day post-reconstitution rule is non-negotiable.
Room temperature exposure limits
Brief periods at room temperature during dose drawing are perfectly fine. The concern is cumulative time outside refrigeration. Most guidelines suggest reconstituted semaglutide can tolerate up to 48 hours at room temperature (below 30 degrees Celsius) without significant degradation. Beyond 48 hours, potency loss becomes measurable.
A practical rule: remove the vial from the refrigerator, draw your dose, and return it within 10 minutes. Do not leave it sitting on the bathroom counter overnight. Do not carry it in your pocket for hours. The less cumulative room temperature exposure, the better the potency over the life of the vial.
Using a semaglutide reconstitution calculator
If the math in this guide feels overwhelming, you are not alone. Most researchers do not want to do unit conversions in their head every week. That is exactly why the SeekPeptides reconstitution calculator exists.
How it works
Enter three values: your vial size in milligrams (5mg), the volume of bacteriostatic water you added (in milliliters), and your desired dose in milligrams. The calculator returns your exact concentration and the number of units to draw on a U-100 insulin syringe. No formulas. No rounding errors. Just the number you need.
The semaglutide-specific dosage calculator goes a step further. It includes the standard titration schedule, shows you how many doses remain in your vial at each titration step, and calculates when you will need to reconstitute your next vial. For researchers managing a multi-month protocol, this planning functionality prevents supply gaps.
When manual calculation still matters
Calculators are tools, not replacements for understanding. If you cannot verify the calculator output with basic math, you cannot catch errors. Always spot-check by running the simple formula: dose in mg divided by concentration in mg/mL equals volume in mL. Multiply by 100 for units on a U-100 syringe. If the calculator and your math agree, you are good. If they do not, recheck both before drawing your dose.
Understanding the underlying peptide dosage calculation principles means you can adapt to any vial size, any water volume, and any dose without being dependent on a specific tool. The calculator saves time. The knowledge saves errors.
Special considerations for compounded semaglutide
Not all 5mg semaglutide vials are identical. Compounded semaglutide may come in different salt forms, with different excipients, and in different physical states. These differences can affect reconstitution.
Lyophilized versus liquid compounded formulations
Some compounded semaglutide arrives already in liquid form. These pre-reconstituted vials do not require you to add bacteriostatic water. They come at a stated concentration, ready to draw and inject. The information in this guide applies specifically to lyophilized (freeze-dried powder) vials that require reconstitution.
If your compounded semaglutide arrives as a liquid at a specific concentration (for example, 2.5mg/mL in a 2mL vial), skip the reconstitution step entirely and proceed directly to dose calculation based on the labeled concentration. Always verify with the compounding pharmacy documentation that accompanies the product.
Semaglutide sodium versus semaglutide base
This distinction matters for precise dosing. Semaglutide sodium is the salt form, which has a slightly higher molecular weight than semaglutide base. A vial labeled as 5mg of semaglutide sodium contains slightly less active semaglutide by weight than a vial labeled as 5mg semaglutide base.
In practical terms, the difference is small enough that standard dosing protocols do not adjust for it. But if you are comparing products from different sources and one labels as sodium while the other labels as base, understand that they are not quite identical milligram-for-milligram. Most compounded semaglutide in the United States uses the sodium salt form.
Additional excipients
Some compounded formulations include additional ingredients like vitamin B12, glycine, or other compounds. These additions do not change the reconstitution process for lyophilized vials. You still add the same amount of bacteriostatic water based on the semaglutide content. However, the additional ingredients may affect the appearance of the reconstituted solution (B12 adds a pink tint, for example) and may have their own stability profiles.
Always follow the specific reconstitution instructions provided by the compounder when available. If no instructions are provided, the standard ratios in this guide apply to any 5mg semaglutide lyophilized vial regardless of additional excipients.
Troubleshooting reconstitution problems
Even experienced researchers occasionally encounter issues during reconstitution. Here is what to do when things do not go as planned.
The powder will not dissolve
If gentle swirling for 10 minutes does not produce a clear solution, try these steps in order. First, check whether the bacteriostatic water was at room temperature. Cold water dramatically slows dissolution. Let the vial sit at room temperature for 15 minutes, then try gentle swirling again.
Second, verify the powder was still intact before reconstitution. If the vial was exposed to moisture before you opened it, the powder may have partially degraded. A properly stored lyophilized semaglutide vial contains a single white-to-off-white cake or powder at the bottom. If it looks discolored, stuck to the sides, or has an unusual appearance, the vial may have been compromised during shipping or storage.
Third, if the solution has visible particles or remains cloudy after 15 minutes of gentle mixing at room temperature, do not use it. The risk of injecting denatured peptide or contaminants is not worth the cost savings of trying to salvage a compromised vial.
You accidentally added too much water
This happens. You aimed for 2mL and accidentally added 2.5mL. The solution is not ruined. Your semaglutide is perfectly fine. The only thing that changed is the concentration.
Recalculate: 5mg divided by 2.5mL equals 2mg/mL instead of the planned 2.5mg/mL. Adjust your unit calculations accordingly. Using the peptide calculator, enter the actual water volume you added, and it gives you the corrected dose in units. A minor inconvenience, not a catastrophe.
You accidentally added too little water
Same principle in reverse. If you added 1.5mL instead of 2mL, your concentration is 5mg divided by 1.5mL equals 3.33mg/mL. Recalculate your doses at this concentration. You can also add the remaining 0.5mL to bring the total to 2mL. Just make sure to swab the stopper again before the second puncture and use proper sterile technique throughout.
Air bubbles in the reconstituted vial
A few small air bubbles in the vial after reconstitution are normal and harmless. They will not affect potency or dosing accuracy as long as you draw your dose carefully. Hold the vial upright when drawing so the needle tip is submerged below any surface bubbles. If a bubble enters your syringe, hold the syringe needle-up, tap the barrel to move the bubble to the top, and gently push it out before injecting.
The vial rubber stopper is damaged
Repeated punctures through the same spot can core the rubber stopper, creating small rubber particles that fall into the solution. Prevent this by inserting the needle at a slight angle and rotating puncture sites around the stopper surface with each use. If you see visible rubber fragments in the solution, draw through a filter needle or discard the vial. Injecting rubber particles is never acceptable.
How long a 5mg vial lasts at each dose
Planning your peptide supply requires knowing exactly how many weeks a single vial covers at each dose in the titration protocol. This table assumes the 2mL reconstitution ratio (2.5mg/mL) with weekly injections.
Weekly Dose | mg Used per Week | Weeks per 5mg Vial | Doses per Vial |
|---|---|---|---|
0.25mg | 0.25 | 20 weeks | 20 |
0.5mg | 0.5 | 10 weeks | 10 |
1.0mg | 1.0 | 5 weeks | 5 |
1.7mg | 1.7 | ~2.9 weeks | ~2.9 |
2.4mg | 2.4 | ~2.1 weeks | ~2.1 |
Here is the important catch. The 28-day stability window limits how long you can actually use a reconstituted vial, regardless of how much peptide remains. At the 0.25mg starting dose, a 5mg vial theoretically lasts 20 weeks. But once reconstituted, you should discard any remaining solution after 28 days.
This means at 0.25mg weekly, you will use only 1mg of the 5mg in the vial before the 28-day window closes. That is 4mg wasted. The solution? Add less bacteriostatic water to increase concentration and reduce waste. Or better yet, consider the reconstitution math before purchasing. At very low doses, smaller vials (if available) or pre-mixed formulations may be more cost-effective. Understanding semaglutide timelines helps you plan vial purchases around your expected dose increases.
Minimizing waste during early titration
The most cost-effective approach during early titration is to reconstitute with less water. If you use 1mL instead of 2mL, your concentration is 5mg/mL. At 0.25mg weekly, you draw 5 units per dose and use 1mg over four weeks, with 4mg remaining. You can continue using the same vial through your dose increases, discarding only when the 28-day mark hits or when you have used the full 5mg.
Better still, if you know you will be on 0.25mg for four weeks and then 0.5mg for the next four weeks, you can plan your reconstitution date so that the 28-day window covers both titration steps. Four weeks at 0.25mg uses 1mg. Four weeks at 0.5mg uses 2mg. Total: 3mg used within 28 days, with 2mg remaining. Not perfect, but far less waste than 4mg unused.
Injection technique after reconstitution
Proper reconstitution sets you up for accurate dosing. But the injection itself has its own technique requirements that affect both comfort and absorption.
Choosing injection sites
Semaglutide is administered subcutaneously, meaning just under the skin into the fat layer. The three recommended injection sites are the abdomen (at least 2 inches from the navel), the front of the thigh, and the back of the upper arm. Rotation between these sites reduces the risk of lipodystrophy, a condition where repeated injections in the same spot cause fat tissue to harden or waste away.
Each site absorbs semaglutide at slightly different rates due to varying blood flow and fat thickness. The abdomen typically offers the fastest absorption, followed by the thigh, then the arm. Most protocols recommend picking one general area for consistency, then rotating specific spots within that area. For detailed injection site guidance applicable to all GLP-1 peptides, rotation patterns matter more than most people realize.
Drawing the dose from your reconstituted vial
Before each draw, swab the vial stopper with a fresh alcohol pad. Wait for it to dry. Draw air into your syringe equal to the dose volume, insert the needle into the vial, push the air in, then invert the vial and draw your dose. This positive pressure technique makes drawing easier and more accurate.
Check for air bubbles after drawing. Any bubble displaces liquid volume, meaning you have drawn less semaglutide than your target. Tap them out, push the excess air back into the vial, and verify your volume before removing the needle. This small ritual takes 15 seconds and ensures every dose is accurate. For a broader overview of peptide injection techniques, the fundamentals apply across all subcutaneous peptides.
Injection timing and frequency
Semaglutide is a once-weekly injection. Pick a consistent day each week and stick with it. The specific day does not matter, but the consistency does. Semaglutide has a half-life of approximately 168 hours (one week), so weekly dosing maintains steady blood levels. Shifting your injection day by a day or two occasionally is fine. Shifting by four or five days disrupts the steady state and may increase breakthrough symptoms between doses.
There is no strong evidence favoring morning versus evening injections. Some researchers prefer morning to avoid potential nausea interfering with sleep. Others prefer evening so any initial side effects occur during rest. Choose based on personal tolerance and stick with your schedule.
What happens when you get the water volume wrong
Mistakes happen. Understanding the consequences helps you decide whether to continue with a miscalculated vial or start fresh.
Too much water: doses are weaker than intended
If you added 3mL instead of 2mL, your concentration dropped from 2.5mg/mL to 1.67mg/mL. Every dose you draw at the 2.5mg/mL unit calculations is actually delivering about 67% of the intended dose. You will not feel the full effects, weight loss may slow, and appetite suppression may be insufficient.
The fix is simple. Recalculate your doses based on the actual concentration. At 1.67mg/mL, a 0.25mg dose requires 15 units instead of 10. A 0.5mg dose requires 30 units instead of 20. Adjust and continue. The peptide itself is unaffected. Only the concentration changed.
Too little water: doses are stronger than intended
This is the more concerning scenario. If you added 1mL instead of 2mL, your concentration is 5mg/mL, double what you calculated for. Drawing 10 units at this concentration delivers 0.5mg instead of the intended 0.25mg. That is double your starting dose, which may trigger significant gastrointestinal side effects including nausea, vomiting, and diarrhea.
If you suspect you have been overdosing due to a reconstitution error, recalculate immediately. The fix is the same: adjust your unit draw based on the actual concentration. You can also add additional bacteriostatic water to bring the volume (and therefore the concentration) back to your intended ratio. But keep total volume reasonable for the vial size.
When to discard and start over
Discard the vial if you are uncertain how much water was added. Guessing at concentration is unacceptable when dosing a pharmacologically active compound. The cost of one wasted vial is trivial compared to the consequences of consistent over or under-dosing across weeks of your protocol.
Also discard if the solution appears cloudy, contains particles, has been left at room temperature for more than 48 hours, or is past the 28-day mark. When in doubt, throw it out. This is not the place to cut corners.
Comparing reconstitution approaches across GLP-1 peptides
Semaglutide is not the only GLP-1 receptor agonist that researchers work with. Understanding how reconstitution differs across the category helps researchers who use multiple peptides maintain separate, accurate protocols.
Semaglutide versus tirzepatide reconstitution
Tirzepatide reconstitution follows the same basic principles but with different typical vial sizes and concentrations. Tirzepatide commonly comes in 10mg, 15mg, and 30mg vials. The reconstitution math is identical: total mg divided by mL of water added equals concentration. But tirzepatide doses tend to be higher (up to 15mg weekly), requiring different water volumes to keep injection volumes manageable.
Researchers working with both peptides should maintain separate labeled vials and separate syringes. Mixing up vials when both are clear, colorless solutions in similar glass containers is an easy and dangerous mistake. For a direct comparison of these two peptides beyond reconstitution, see the complete semaglutide versus tirzepatide analysis.
Reconstitution standards across peptide types
The fundamental reconstitution technique applies universally: aim water at the vial wall, never shake, use bacteriostatic water for multi-dose vials, and refrigerate immediately. What changes between peptides is the typical vial size, common reconstitution volumes, and resulting concentrations.
BPC-157 typically comes in 5mg vials and is reconstituted with 1-2mL of BAC water. General peptide reconstitution follows the same formula regardless of the specific peptide. The key is always matching your water volume to your dosing needs, using the reconstitution calculator to verify your math before drawing any dose.
Advanced tips for experienced researchers
Once you have mastered basic reconstitution, these refinements optimize accuracy and minimize waste.
Dead volume compensation
Every syringe has dead volume, the small amount of liquid that remains in the needle hub and syringe tip after you push the plunger fully. On a standard insulin syringe, this is approximately 0.007-0.012mL (roughly 1 unit). Over multiple draws from a single vial, dead volume losses accumulate.
For a vial with 20 draws, you lose approximately 0.14-0.24mL to dead volume. At 2.5mg/mL concentration, that is 0.35-0.6mg of semaglutide you paid for but never received. Some researchers compensate by adding an extra 0.1-0.2mL of bacteriostatic water during reconstitution, accepting a slightly lower concentration in exchange for more usable doses. Others use low dead-volume syringes designed to minimize this waste.
Temperature acclimation before drawing doses
Cold solution drawn directly from the refrigerator is more viscous than room-temperature solution. This means the plunger requires slightly more force, which can make precise dose drawing harder. Let the vial warm slightly (5 minutes at room temperature) before drawing your dose. This improves flow without meaningfully impacting stability since the exposure time is minimal.
Documentation and tracking
Keep a simple log for each vial: reconstitution date, water volume added, concentration, and a running tally of doses drawn with dates. This serves two purposes. First, it ensures you never lose track of the 28-day window. Second, it creates a record that helps troubleshoot if your results change unexpectedly mid-vial. If you notice reduced appetite suppression starting at dose 8 of 10, your log tells you exactly when the vial was reconstituted and how many times the stopper has been punctured. SeekPeptides members track their protocols through comprehensive logging systems designed for exactly this kind of multi-week monitoring.
Frequently asked questions
Can I use 3mL of bacteriostatic water with a 5mg semaglutide vial?
Yes. Adding 3mL produces a concentration of 1.67mg/mL. This is a perfectly valid ratio that works well for lower doses. At 0.25mg weekly, you would draw 15 units. The advantage is that measurement precision is very forgiving at this concentration. The disadvantage is that higher doses require large injection volumes. At 2.4mg, you would need 144 units, exceeding a standard 100-unit syringe. This ratio works best during early titration phases at lower doses.
How do I know if my semaglutide went bad after reconstitution?
Properly reconstituted semaglutide is clear and colorless. If the solution turns cloudy, develops visible particles, changes color, or develops an unusual odor, it has degraded and should be discarded. Reduced effectiveness despite consistent dosing can also indicate degradation, though this is harder to confirm objectively. Stick to the 28-day storage limit to minimize this risk.
Is it safe to reuse syringes for drawing doses?
No. Syringes and needles are single-use devices. Reusing them introduces contamination risk into both the vial and the injection. Used needles also dull rapidly. A dulled needle causes more tissue damage, more pain, and creates a larger opening in the rubber stopper that accelerates coring. Fresh syringe, fresh needle, every single draw. This is fundamental peptide safety practice.
What if I left my reconstituted vial out overnight?
A single overnight at room temperature (below 30 degrees Celsius) is within the acceptable tolerance for reconstituted semaglutide. Most stability data supports up to 48 hours at room temperature without significant degradation. Return the vial to the refrigerator as soon as you realize the mistake and continue using it. Do not extend the 28-day window to compensate, and do not leave it out again. Repeated room temperature excursions have cumulative effects on peptide stability.
Can I mix semaglutide with tirzepatide in the same syringe?
Do not combine different peptides in the same syringe or the same vial. Each peptide has specific stability requirements, and combining them can cause aggregation, degradation, or altered pharmacokinetics. Keep each peptide in its own vial, draw with its own syringe, and inject at separate sites. If you are researching both peptides, maintain completely separate reconstitution and dosing protocols. For guidance on transitioning between these peptides, sequential use is the standard approach.
Does the brand of bacteriostatic water matter?
The brand matters less than the specification. Any bacteriostatic water that contains 0.9% benzyl alcohol in USP-grade sterile water meets the requirement. Avoid bacteriostatic water from unverified sources. Check for proper packaging, lot numbers, and expiration dates. Opened bacteriostatic water vials should themselves be discarded after 28 days. For more on choosing the right water for peptide mixing, the specification matters more than the label.
How many total doses will I get from one 5mg vial?
Total doses depend on your weekly dose. At 0.25mg: 20 doses. At 0.5mg: 10 doses. At 1mg: 5 doses. At 1.7mg: approximately 3 doses. At 2.4mg: approximately 2 doses. Remember that the 28-day stability limit may prevent you from using all available doses at lower dose levels. Plan your reconstitution timing to align with your current dose requirements.
What is the best reconstitution ratio for beginners?
The 2mL ratio (producing 2.5mg/mL) is the best choice for most researchers starting out. It balances measurement precision with practical injection volumes across the full titration range. The unit calculations produce clean, round numbers at the most common doses. More experienced researchers may prefer higher concentrations for smaller injection volumes, but beginners benefit from the forgiving measurement margins of the 2mL ratio. Use the semaglutide dosage calculator to double-check your math regardless of experience level.
External resources
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based reconstitution guides, free calculators, proven dosing protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your reconstitutions stay sterile, your concentrations stay accurate, and your results stay consistent.