Feb 12, 2026

You expected nausea. Maybe some stomach issues. Everyone warned you about those. But nobody mentioned the bone-deep exhaustion that hit around day four, the kind that makes your couch feel like a gravity well and your alarm clock feel like an enemy combatant. You are not imagining it. You are not lazy. And you are definitely not the only one dragging through your afternoons wondering if something is seriously wrong.
Semaglutide fatigue is real. Clinical trials confirm it affects roughly 6 to 11 percent of users, making it one of the most common side effects that nobody seems to talk about until it lands on them. The tiredness can range from mild sluggishness to full-blown exhaustion that derails workouts, kills productivity, and makes you question whether this medication is worth it at all.
Here is the good news. It is almost always temporary. And it is almost always fixable. The researchers, clinicians, and experienced users who have navigated this side effect have mapped out exactly why it happens, when it peaks, and what you can do about it starting today. This guide covers every mechanism behind semaglutide-related fatigue, a detailed week-by-week timeline so you know what to expect, and a complete toolkit of evidence-based strategies that actually restore your energy. Whether you are on semaglutide for weight management or exploring GLP-1 options, understanding fatigue puts you back in control of your protocol and your day.
What semaglutide fatigue actually feels like
Not all fatigue is created equal. Some people describe semaglutide-related tiredness as a mild heaviness in their limbs. Others compare it to the exhaustion that follows a bad flu, where every task requires conscious effort and rest never quite recharges you. The distinction matters because understanding your specific type of fatigue helps identify which mechanism is driving it and, more importantly, which solution will actually work.
There are three main patterns.
The first is acute onset fatigue. This type hits within the first 24 to 72 hours after your injection and typically correlates with your body processing the medication. It tends to peak on days two and three, then gradually lifts before your next dose. If this sounds familiar, the mechanism is usually hormonal adjustment as your GLP-1 receptors respond to the new signaling patterns.
The second pattern is cumulative fatigue. This builds slowly over weeks rather than appearing in sharp post-injection waves. You might not notice it immediately. But by week three or four, you realize that your baseline energy has quietly dropped. You are sleeping the same hours but waking up less rested. Your workouts feel harder. Your mental sharpness has dimmed. This pattern almost always traces back to inadequate caloric intake, nutrient gaps, or both.
The third is persistent fatigue. This variant does not improve with time, dose adjustments, or lifestyle changes. It deserves medical attention because it may indicate an underlying issue that semaglutide is unmasking rather than causing, such as vitamin B12 deficiency, thyroid dysfunction, or iron depletion.
Recognizing which pattern matches your experience is the first step toward fixing it. Most people fall into the first or second category, and the solutions for those are straightforward.
The seven mechanisms behind semaglutide fatigue
Fatigue on semaglutide does not have a single cause. It has several, and they often stack on top of each other. Understanding all seven mechanisms gives you the ability to troubleshoot systematically rather than guessing.
1. Calorie deficit shock
This is the most common driver. Semaglutide reduces appetite so effectively that many users cut their caloric intake by 30 percent or more without even trying. That is the whole point of the medication. But when you drop from 2,500 calories to 1,500 overnight, your body interprets the shift as a potential threat. It responds by conserving energy, downregulating metabolic processes, and making you feel tired to reduce activity.
Think of it this way. Your body has been running on a particular fuel budget for years. Semaglutide effectively slashes that budget in half within days. The fatigue is your body saying it needs time to recalibrate, to switch from expecting a surplus to efficiently operating on less. This recalibration typically takes two to four weeks, assuming you are still eating enough to support basic functions.
The fix is not to eat more just for the sake of eating more. The fix is to eat strategically, prioritizing nutrient-dense foods that deliver maximum energy per bite. More on that in the solutions section.
2. Blood sugar regulation shifts
Semaglutide changes the way your body handles glucose. It enhances insulin secretion when blood sugar is elevated and suppresses glucagon release, which together create a smoother, more stable blood sugar curve. That sounds like a benefit, and it is. But there is a catch.
If your body has spent years riding the blood sugar roller coaster, with sharp spikes after meals followed by crashes that sent you reaching for snacks, then a stable, lower blood sugar level can actually feel like hypoglycemia even when your numbers are perfectly normal. This phenomenon, called relative hypoglycemia, triggers fatigue, brain fog, and irritability as your nervous system adjusts to the new normal.
The adjustment period for blood sugar regulation typically runs four to eight weeks. During this window, your brain gradually recalibrates its glucose sensors and learns that the new, lower baseline is not dangerous.
3. Gastrointestinal side effects and dehydration
Nausea, vomiting, diarrhea, and reduced food intake all contribute to dehydration. And dehydration is one of the fastest paths to fatigue. Even mild dehydration, a loss of just 1 to 2 percent of body water, has been shown to reduce cognitive function, increase perceived effort during physical activity, and trigger feelings of tiredness.
The problem compounds itself. When you feel nauseous, you drink less. When you have diarrhea, you lose fluids and electrolytes faster. When you vomit, you lose both water and the minerals your muscles and nerves need to function properly. The result is a fatigue that feels physical, because it is. Your cells are literally struggling to maintain normal operations without adequate hydration.
Electrolyte losses matter as much as water losses here. Sodium, potassium, and magnesium all play critical roles in energy production at the cellular level. Losing them through GI side effects without replacing them creates a fatigue that no amount of sleep will fix.
4. Muscle mass loss and sarcopenia risk
Research presented at ENDO 2025 found that approximately 40 percent of the weight lost on semaglutide comes from lean mass, including muscle. A 24-month retrospective cohort study published in PMC confirmed that semaglutide use is associated with muscle loss and functional decline, particularly in older adults and at higher doses.
Muscle is metabolically active tissue. It burns calories at rest, supports posture and movement, and serves as a reservoir for amino acids that your body uses during stress. When you lose muscle, your basal metabolic rate drops, your capacity for physical activity decreases, and your subjective energy levels plummet. The fatigue from muscle loss is different from calorie-deficit fatigue. It feels like weakness rather than sleepiness, an inability to do things that used to feel easy.
Women and older adults face the highest risk. The ENDO 2025 data showed that being older, female, or eating less protein was linked to greater muscle loss. Critically, losing more muscle was also linked to less improvement in blood sugar control, creating a vicious cycle where the fatigue-causing muscle loss also undermines one of the medication's primary benefits.
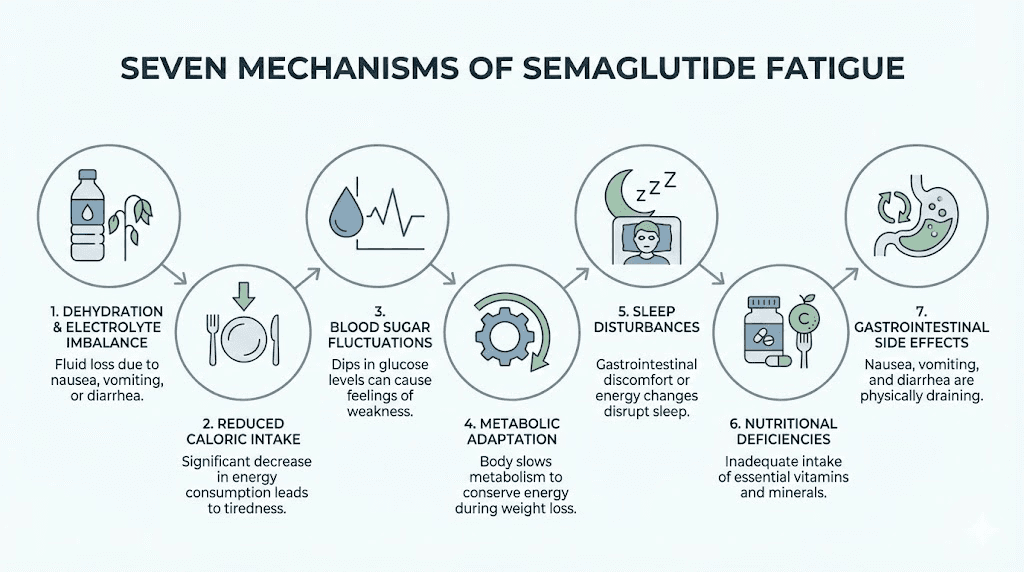
5. Nutrient depletion
When you eat less, you absorb fewer vitamins and minerals. But semaglutide adds another layer to this problem. By slowing gastric emptying and altering gut motility, it can change how efficiently your body extracts nutrients from the food you do eat.
Three nutrients deserve special attention.
Vitamin B12. Studies show that long-term semaglutide use can lower B12 levels by altering absorption in the stomach and intestines. B12 deficiency causes fatigue, weakness, cognitive fog, and neurological symptoms. If you are taking semaglutide with B12 supplementation, you may already be ahead of this problem. If not, it is worth testing.
Iron. A pilot study analyzing semaglutide's influence on intestinal iron absorption found that the increase in iron levels after oral iron absorption testing was notably diminished following semaglutide introduction. Reduced iron absorption can lead to iron deficiency anemia, one of the most common medical causes of fatigue worldwide.
Zinc. Research found that weight reduction by semaglutide was accompanied by significant decreases in serum zinc levels. Zinc is essential for immune function, wound healing, and energy metabolism. Depletion contributes to fatigue, impaired taste (which further reduces food intake), and weakened immunity.
6. Central nervous system effects
GLP-1 receptors are not limited to your gut and pancreas. They are expressed throughout the brain, including regions that regulate mood, motivation, and energy. Research published in the Journal of Neuropsychiatry and Clinical Neurosciences shows that GLP-1 modulates the release of serotonin, dopamine, gamma-aminobutyric acid, and glutamate.
These neurotransmitters do not just affect your mood. They directly influence your perceived energy levels, your motivation to move, and your capacity to focus. When semaglutide activates GLP-1 receptors in the ventral tegmental area and nucleus accumbens, it modulates the reward pathways that previously drove food-seeking behavior. The reduction in food-related dopamine signaling can manifest as a general decrease in motivation and energy that feels like fatigue even when your body is physically rested.
This mechanism is less well-studied than the metabolic causes, but it may explain why some users experience fatigue that does not respond to nutritional interventions alone.
7. Thyroid function changes
A case report published in the European Journal of Medical and Health Sciences documented semaglutide-induced subclinical hypothyroidism in a patient receiving both levothyroxine and semaglutide. The patient presented with increasing fatigue, weakness, and shortness of breath.
While this is not common, semaglutide can influence thyroid function in subtle ways. Research from Pharmacy Times showed that patients on semaglutide who lost over 5 pounds saw the greatest reduction in TSH levels (-0.55 mU/L). For most people, this shift is clinically insignificant. But for those with borderline thyroid function, pre-existing hypothyroidism, or who are on thyroid medication, the change can tip them into symptomatic territory where fatigue becomes persistent.
If your fatigue does not improve after eight weeks and you have any history of thyroid issues, a simple TSH and free T4 blood test can rule this out or confirm it.
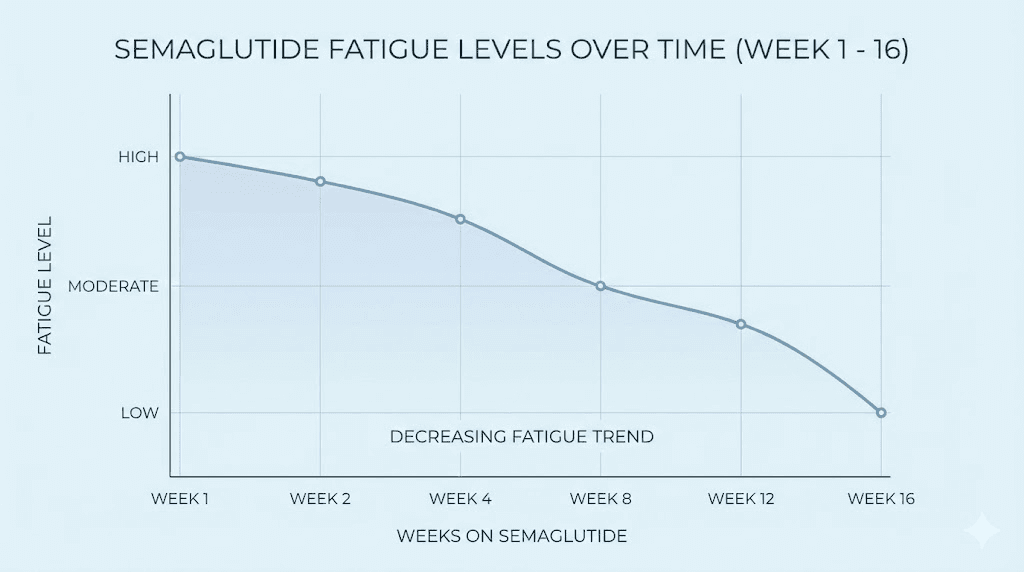
Week-by-week fatigue timeline
Knowing what to expect removes the anxiety of wondering whether something is wrong. Here is what the research and clinical experience show about semaglutide fatigue at each stage of treatment.
Weeks 1 to 2: the adjustment phase
This is typically the hardest stretch. Your body is encountering GLP-1 receptor activation at levels it has never experienced before. The starting dose is intentionally low (0.25 mg for most protocols), but even this amount triggers significant changes in appetite signaling, gastric emptying speed, and insulin dynamics.
Fatigue during this phase usually correlates with GI side effects. If you are nauseous, eating less, and slightly dehydrated, tiredness is the inevitable result. Most users rate their fatigue at 5 to 7 out of 10 during this window. The fatigue tends to be worst in the 24 to 48 hours after injection, then partially lifts before the next dose.
What helps most during weeks one and two: aggressive hydration, electrolyte supplementation, eating small frequent meals even when appetite is suppressed, and giving yourself permission to rest without guilt.
Weeks 3 to 4: the turning point
Most users begin to notice improvement here. GI side effects typically lessen as the body adapts to the medication. Appetite suppression remains strong, but the nausea that prevented eating usually fades. With better food intake and fewer GI losses, hydration and nutrient status improve.
However, this is also when dose escalation often begins. Moving from 0.25 mg to 0.5 mg can temporarily reignite fatigue symptoms as the body adjusts to the higher dose. If this happens, recognize it as the same adjustment process you already survived, not a new problem.
Fatigue at this stage typically drops to 3 to 5 out of 10. The post-injection tiredness pattern may persist but becomes less severe and shorter in duration.
Weeks 5 to 8: stabilization
By week five, most users report that fatigue has become manageable or has resolved entirely. The body has adapted to semaglutide's effects on appetite, digestion, and blood sugar. Energy levels may not match pre-medication baseline yet, especially if significant weight loss has occurred, but the debilitating exhaustion of the early weeks is typically gone.
The exception is users who have not addressed the underlying drivers. If you are still under-eating protein, skipping electrolytes, and ignoring hydration, fatigue persists regardless of how long you have been on the medication. The timeline only applies when you are actively managing the controllable factors.
Weeks 9 to 16: the energy return
Something interesting happens in this phase. As weight loss accumulates, many users report that their energy levels actually exceed pre-medication baseline. Carrying less weight means less strain on joints, cardiovascular system, and respiratory function. Sleep quality often improves as sleep apnea lessens and hormonal profiles shift. The metabolic benefits of reduced visceral fat translate into more stable energy throughout the day.
Long-term data supports this. The STEP 1 trial published in the New England Journal of Medicine found that after 68 weeks of semaglutide treatment, patients reported significantly better physical functioning and energy levels compared to baseline.
The complete fatigue fix protocol
This is the actionable section. Every strategy here is backed by clinical evidence or consistent user experience. Apply them systematically rather than cherry-picking, because semaglutide fatigue usually has multiple causes operating simultaneously.
Protein prioritization
This is the single most impactful change you can make. Research from ENDO 2025 directly links higher protein intake to reduced muscle loss on semaglutide. The recommended target is 1.2 to 1.6 grams of protein per kilogram of body weight per day. For a 180-pound person, that translates to roughly 98 to 131 grams of protein daily.
When appetite is suppressed, meeting this target requires strategic eating. Protein should be the first thing on your plate at every meal. If you can only eat a small amount, make it protein. If you are using semaglutide for fat loss, protecting muscle mass is not optional. It is essential for maintaining metabolic rate, functional capacity, and long-term energy.
Practical protein targets by meal:
Breakfast: 25 to 35 grams (eggs, Greek yogurt, protein shake)
Lunch: 30 to 40 grams (chicken breast, fish, lean beef)
Dinner: 30 to 40 grams (salmon, turkey, tofu for plant-based)
Snack: 15 to 20 grams (cottage cheese, protein bar, edamame)
If nausea makes solid food difficult, liquid protein sources like whey protein mixed with water or bone broth can provide adequate amino acids without triggering GI distress. The goal is not perfect meals. The goal is hitting your protein number by any means necessary.
Hydration protocol
Aim for 64 to 80 ounces of fluid daily as a baseline. If you are experiencing GI side effects, increase to 90 to 100 ounces. But do not just drink plain water. You need electrolytes.
A practical hydration schedule:
Morning: 16 ounces of water with electrolyte powder immediately upon waking
Mid-morning: 16 ounces of water or herbal tea
Afternoon: 16 ounces of water with electrolyte powder
Evening: 16 ounces of water or broth
Extra: 8 to 16 ounces for every episode of vomiting or diarrhea
Key electrolytes to track: sodium (2,000 to 3,000 mg daily), potassium (2,500 to 3,500 mg daily from food and supplements), and magnesium (300 to 400 mg daily). Magnesium glycinate is the preferred form because it is well-absorbed and less likely to cause additional GI issues.
Strategic meal timing
When your appetite is crushed, the temptation is to skip meals entirely and eat one large meal when hunger finally appears. This approach guarantees fatigue. It creates blood sugar valleys that deepen tiredness, prevents consistent nutrient delivery, and makes it nearly impossible to hit adequate protein targets.
Instead, eat four to five smaller meals spaced three to four hours apart. Each meal should be 300 to 500 calories and contain at least 25 grams of protein. This pattern:
Maintains steady blood sugar levels
Prevents the energy crashes that come from long fasting periods
Makes it easier to consume adequate total nutrition despite reduced appetite
Reduces nausea compared to larger, less frequent meals
Even if you are not hungry, set timers and eat by the clock during the first four to eight weeks. Your appetite signals are temporarily disrupted. Trusting them completely will lead to under-eating, which leads to fatigue, which makes everything harder.
Micronutrient supplementation
Based on the nutrient depletion research, a targeted supplementation protocol can prevent or reverse fatigue caused by deficiencies. This is not about taking every vitamin on the shelf. It is about addressing the specific nutrients that semaglutide is known to deplete or impair absorption of.
Essential supplements while on semaglutide:
Vitamin B12: 1,000 to 2,000 mcg sublingual methylcobalamin daily. Sublingual delivery bypasses the GI tract, which matters because semaglutide may impair B12 absorption through the stomach.
Iron: If blood work shows low ferritin or low iron, supplement with 18 to 65 mg of elemental iron with vitamin C to enhance absorption. Take iron at least two hours away from semaglutide injection.
Zinc: 15 to 30 mg daily with food.
Magnesium glycinate: 300 to 400 mg daily, preferably before bed (also supports sleep quality).
Vitamin D3: 2,000 to 4,000 IU daily with a fat-containing meal.
Omega-3 fatty acids: 1,000 to 2,000 mg EPA/DHA daily for anti-inflammatory support.
Get blood work done before starting semaglutide if possible, and recheck at 8 and 16 weeks. This gives you objective data rather than guesswork. The most important markers to test: complete blood count, iron panel with ferritin, B12, folate, vitamin D, magnesium, zinc, and thyroid function (TSH and free T4).
Exercise modification
Exercise during semaglutide-induced fatigue requires a mindset shift. The goal is not to maintain your pre-medication intensity. The goal is to preserve muscle mass and support metabolic health while respecting your body's current energy capacity.
During weeks one to four, reduce exercise volume by 30 to 50 percent. Keep intensity moderate. Prioritize resistance training over cardio because preserving muscle is more important than burning additional calories while your body adapts. Walking is the perfect low-impact activity during this phase. It burns calories without depleting glycogen stores, supports circulation, and actually boosts energy rather than draining it.
After week four, gradually increase volume based on how you feel. The key metric is recovery. If you need more than 48 hours to feel recovered from a workout, you are doing too much. Scale back and reassess.
A modified exercise schedule for the adjustment period:
Monday/Thursday: Full-body resistance training (compound movements, 3 sets of 8-12 reps)
Tuesday/Friday/Saturday: 20 to 30 minute walk
Wednesday/Sunday: Rest or gentle stretching
This schedule preserves muscle stimulus while keeping total energy expenditure manageable. As fatigue resolves, add volume and intensity incrementally. Do not return to your previous routine overnight.
Sleep optimization
Sleep is when your body repairs, restores, and recalibrates. On semaglutide, the importance of quality sleep multiplies because your body is already managing significant metabolic changes. Poor sleep on top of medication adaptation creates a fatigue feedback loop that becomes difficult to escape.
Practical sleep strategies:
Consistency: Same bedtime and wake time every day, including weekends.
Temperature: Keep your bedroom at 65 to 68 degrees Fahrenheit. Weight loss can change your thermoregulation, so you may need to adjust.
Light exposure: 10 to 15 minutes of morning sunlight to set circadian rhythm. Minimize blue light exposure 60 to 90 minutes before bed.
Magnesium: 300 mg magnesium glycinate 30 to 60 minutes before bed supports both sleep quality and the mineral replenishment that semaglutide users need.
Caffeine cutoff: No caffeine after 12 PM. This matters more when your system is already stressed by medication adaptation.
Injection timing adjustment
If your fatigue follows a clear post-injection pattern, where it peaks 24 to 48 hours after your weekly dose, timing your injection strategically can minimize the impact on your most important days.
Many users find that injecting on Thursday or Friday evening allows the worst fatigue to coincide with the weekend when rest is more accessible. Others prefer Sunday evening so the fatigue hits during Monday and Tuesday, leaving the rest of the week relatively unaffected. There is no universally correct answer. The right timing depends on your schedule, your social obligations, and which days you can afford to operate at reduced capacity.
Experiment with injection timing during the first month. Once you identify your personal fatigue pattern, lock in the timing that creates the least disruption.
When semaglutide fatigue is not normal
Most semaglutide fatigue resolves within four to eight weeks. If yours does not, something else may be going on. Here are the red flags that warrant medical evaluation rather than continued self-management.
Persistent fatigue beyond 8 weeks with no improvement despite adequate nutrition, hydration, and sleep. This suggests an underlying condition that semaglutide may be exposing.
Fatigue accompanied by hair loss. This combination points to nutrient deficiency, thyroid dysfunction, or excessive caloric restriction. All three need medical workup.
Extreme weakness or muscle wasting. If you notice rapid loss of strength, difficulty climbing stairs, or trouble carrying groceries, screen for sarcopenia. A DEXA scan can quantify lean mass changes.
Cognitive symptoms beyond brain fog. Severe confusion, memory problems, or numbness/tingling in extremities can indicate B12 deficiency or neurological effects that require immediate attention.
Dizziness or fainting. This may indicate hypotension from dehydration or, less commonly, dosage-related issues affecting blood pressure or blood sugar.
The safety-first principle applies here. When in doubt, get blood work done. A basic metabolic panel, CBC, thyroid panel, B12, iron studies, and vitamin D level will identify or rule out nearly every medical cause of persistent fatigue. The cost of testing is minimal compared to the cost of ignoring a treatable condition.
Semaglutide fatigue versus tirzepatide fatigue
If you are considering switching from semaglutide to tirzepatide or vice versa, understanding the fatigue differences between these two GLP-1 medications helps set expectations.
Tirzepatide fatigue has been reported at similar rates to semaglutide fatigue. However, because tirzepatide acts on both GLP-1 and GIP receptors (dual agonism), the fatigue profile can differ in subtle ways. Some users report that tirzepatide fatigue is more closely tied to GI side effects, while semaglutide fatigue has a broader range of causes including the central nervous system effects described earlier.
Factor | Semaglutide | Tirzepatide |
|---|---|---|
Fatigue prevalence | 6 to 11% | 5 to 10% |
Primary mechanism | GLP-1 receptor activation | Dual GLP-1/GIP activation |
Peak fatigue timing | Weeks 1 to 4 | Weeks 1 to 4 |
Resolution timeline | 4 to 8 weeks | 4 to 8 weeks |
CNS effects | More studied | Less studied |
Muscle loss risk | Higher (40% lean mass) | Lower (more fat-selective) |
If fatigue is your primary concern and you have not yet started treatment, the data slightly favors tirzepatide for preserving lean mass, which may translate to less fatigue from muscle loss. But the difference is modest, and individual responses vary significantly. Both medications produce fatigue that is typically temporary and manageable with the strategies outlined above.
The role of dosing in fatigue management
Dose escalation is one of the most predictable triggers for semaglutide fatigue. Every time you increase your dose, you may experience a mini-version of the initial adjustment phase. Understanding this pattern prevents unnecessary concern and helps you plan accordingly.
Standard semaglutide dose escalation
The typical semaglutide dosing schedule for weight management follows this progression:
Weeks 1 to 4: 0.25 mg weekly
Weeks 5 to 8: 0.5 mg weekly
Weeks 9 to 12: 1.0 mg weekly
Weeks 13 to 16: 1.7 mg weekly
Week 17 onward: 2.4 mg weekly (maintenance dose)
Each step up can temporarily increase fatigue for 5 to 14 days. The higher the jump, the more noticeable the effect. Users who escalate slowly, spending extra time at each dose if side effects are significant, tend to experience less overall fatigue than those who follow the fastest possible escalation schedule.
Microdosing and slower titration
Some clinicians advocate for slower titration in patients who are sensitive to side effects. Instead of jumping from 0.25 mg to 0.5 mg at week five, they may have patients try 0.375 mg for two weeks as an intermediate step. This approach trades speed of weight loss for tolerability, and for fatigue-prone individuals, it can make a significant difference.
If you are using compounded semaglutide, you have more flexibility with dosing increments. Standard pharmaceutical Ozempic comes in fixed-dose pens that limit your options, but compounded formulations allow precise dose adjustments. Using the semaglutide dosage calculator can help you determine the right amount to draw from your vial at any given step.
When to pause dose escalation
If fatigue at your current dose has not resolved after three to four weeks, do not escalate to the next dose. Adding more semaglutide on top of unresolved fatigue compounds the problem. Stay at your current dose until fatigue improves to a manageable level (3 out of 10 or less), then proceed with escalation.
Communicate with your prescriber about this approach. Most clinicians support extending the timeline at any given dose if the patient is experiencing significant side effects. The long-term nature of semaglutide treatment means there is no rush to reach the maximum dose.
Nutrition strategies that specifically combat fatigue
General advice to eat healthy is useless when you are fatigued and have no appetite. You need specific, practical strategies that account for the unique challenges of eating on semaglutide.
The anti-fatigue meal framework
Every meal should include three components:
Protein anchor: 25 to 35 grams of lean protein as the foundation
Complex carbohydrate: Whole grains, sweet potatoes, or legumes for sustained energy
Healthy fat: Avocado, olive oil, nuts, or fatty fish for satiety and nutrient absorption
This combination prevents blood sugar spikes and crashes, delivers steady energy, and maximizes nutrient density per calorie consumed. When appetite is minimal, every calorie needs to work hard.
The nausea-friendly food list
When GI side effects make eating difficult, these foods are generally well-tolerated while still providing meaningful nutrition:
Bone broth: Hydrating, protein-rich (6 to 10 grams per cup), easy on the stomach, contains collagen and minerals
Greek yogurt: 15 to 20 grams of protein per serving, cool temperature soothes nausea
Scrambled eggs: Soft texture, high-quality protein, quick to prepare
Crackers with nut butter: Bland enough to tolerate, provides protein and healthy fats
Smoothies: Blend protein powder, banana, spinach, and nut milk. Cold temperature helps with nausea. Liquid format bypasses some gastric emptying issues.
Rice and chicken: Simple, bland, well-tolerated, provides both protein and carbohydrates
Avoid fatty, greasy, or heavily spiced foods during the first four weeks. These trigger the GI side effects that drive dehydration and worsen fatigue. You can reintroduce them gradually as your tolerance improves.
Meal prep for low-energy days
The irony of semaglutide fatigue is that you need to eat well to combat it, but the fatigue itself makes cooking feel impossible. The solution is batch preparation on your higher-energy days.
Spend 60 to 90 minutes on the weekend preparing:
Grilled chicken breast (5 to 6 portions)
Hard-boiled eggs (12)
Rice or quinoa (large batch)
Pre-cut vegetables for quick stir-fry
Pre-portioned snack bags with nuts and dried fruit
With these prepared, assembling a balanced meal takes under five minutes even on your worst fatigue days. The difference between having prep-ready food and having an empty fridge on a fatigued day is often the difference between adequate nutrition and skipping meals entirely.
Semaglutide fatigue and mental health
Fatigue and mood are deeply intertwined. Persistent tiredness can trigger or worsen anxiety and depression, which in turn deepen fatigue through disrupted sleep, reduced motivation, and altered neurotransmitter function. On semaglutide, this relationship deserves careful attention.
GLP-1 receptors in the brain interact with reward and mood pathways. While most research focuses on semaglutide's potential benefits for mental health (reduced inflammation, improved metabolic health), some users report mood changes during the adjustment period that contribute to an overall sense of exhaustion.
If you notice that your fatigue is accompanied by persistent sadness, loss of interest in activities you previously enjoyed, or significant anxiety that was not present before starting semaglutide, discuss this with your healthcare provider. These symptoms may respond to medication adjustment, counseling, or targeted interventions that address both the metabolic and psychological dimensions of fatigue.
Social support matters here too. Joining a community of people navigating the same experience can reduce the isolation that fatigue creates. Knowing that others have gone through the same exhaustion and emerged on the other side provides both practical tips and emotional reassurance. SeekPeptides members often share their experiences navigating side effects, including fatigue management strategies that worked for their specific situations.
Special populations and fatigue considerations
Not everyone experiences semaglutide fatigue the same way. Certain groups face higher risks and may need modified approaches.
Older adults (over 60)
The 24-month retrospective cohort study on semaglutide and sarcopenia specifically highlighted older adults as a vulnerable population. Age-related muscle loss is already a concern, and semaglutide-induced lean mass reduction compounds it. For older adults, the protein target should be at the higher end of the range (1.4 to 1.6 g/kg/day), and resistance training is not optional, it is essential.
Additionally, older adults are more likely to have pre-existing conditions that contribute to fatigue, including thyroid dysfunction, B12 deficiency, and chronic diseases. Comprehensive blood work before starting semaglutide is especially important for this group.
Women
The ENDO 2025 data specifically identified women as being at higher risk for muscle loss on semaglutide. Hormonal factors, including menopause and menstrual cycle variations, can interact with semaglutide's effects to amplify fatigue at certain times of the month.
Women in perimenopause or menopause should be particularly vigilant about fatigue that does not resolve, as it may indicate a hormonal imbalance that requires separate treatment. Iron deficiency is also more common in premenopausal women due to menstrual losses, and semaglutide's effect on iron absorption makes this risk even more significant.
People with existing thyroid conditions
If you have hypothyroidism and are taking levothyroxine, semaglutide can alter thyroid hormone levels in ways that affect fatigue. Monitor your TSH and free T4 levels more frequently during the first six months of semaglutide use. Your levothyroxine dose may need adjustment as your body weight changes.
People with diabetes
For those using semaglutide for type 2 diabetes management, fatigue may be related to blood sugar changes rather than the mechanisms described above. The interplay between semaglutide, insulin, and other diabetes medications creates a more complex picture where hypoglycemia becomes a real possibility, not just a relative sensation. Blood glucose monitoring is essential for this group to distinguish between semaglutide adaptation fatigue and actual low blood sugar events.
Supplements and compounds that pair with semaglutide for energy
Beyond basic micronutrient supplementation, several compounds have specific evidence for supporting energy levels during GLP-1 therapy.
Creatine monohydrate (3 to 5 grams daily). Creatine supports ATP production in both muscle and brain tissue. For semaglutide users losing lean mass, creatine provides dual benefits: it helps maintain muscle mass and supports cognitive energy. It is one of the most well-researched performance supplements available with an excellent safety profile.
Coenzyme Q10 (100 to 200 mg daily). CoQ10 plays a direct role in mitochondrial energy production. Users on calorie-restricted diets often have reduced CoQ10 levels, which can contribute to fatigue. Supplementation supports cellular energy without affecting semaglutide's mechanisms.
Adaptogenic herbs. Ashwagandha (300 to 600 mg daily) and rhodiola rosea (200 to 400 mg daily) have clinical evidence for reducing perceived fatigue and supporting stress resilience. They work through cortisol modulation and may help offset the energy demands of metabolic adaptation.
B-complex vitamins. While B12 deserves individual supplementation, a comprehensive B-complex provides the full range of B vitamins that support energy metabolism. B1 (thiamine), B2 (riboflavin), B3 (niacin), B5 (pantothenic acid), and B6 (pyridoxine) all play roles in converting food into cellular energy.
Avoid high-dose caffeine as a fatigue solution. While moderate caffeine (200 to 300 mg daily) is fine, relying on caffeine to mask fatigue creates a dependency cycle and can worsen dehydration. It also does not address any of the underlying causes. Use it as a bridge, not a solution.
Tracking your fatigue: the data-driven approach
What gets measured gets managed. Tracking your fatigue patterns helps you identify triggers, measure improvement, and communicate effectively with your healthcare provider.
A simple daily tracking system:
Fatigue score: Rate energy level 1 to 10 at three times daily (morning, afternoon, evening)
Food log: Track total protein intake (grams) and approximate total calories
Hydration: Track total fluid intake (ounces)
Sleep: Hours slept and subjective sleep quality (1 to 10)
Injection day: Note which day you injected and correlate with fatigue scores
Exercise: Type, duration, and intensity
After two to three weeks of tracking, patterns emerge. You might discover that your fatigue is worst on injection days two and three, that skipping breakfast triggers afternoon crashes, or that your energy improves dramatically on days when you hit your protein target. These patterns transform vague frustration into specific, actionable intelligence.
Many SeekPeptides members use tracking tools to monitor their protocols and identify exactly which adjustments made the biggest difference in their energy levels. Having data rather than feelings to guide your decisions leads to faster resolution of fatigue.
What the research says about long-term energy on semaglutide
The long-term picture for energy on semaglutide is genuinely encouraging. While early fatigue is real and sometimes significant, the trajectory for most users points upward.
The STEP 1 trial (New England Journal of Medicine) demonstrated that at 68 weeks, patients on semaglutide 2.4 mg reported improved physical functioning compared to placebo. The STEP 5 trial, extending to 104 weeks, showed sustained improvements in quality of life measures that include energy and vitality.
The mechanism behind long-term energy improvement is straightforward. As excess weight decreases, the body operates more efficiently. Joint pain lessens. Cardiovascular capacity improves. Sleep apnea resolves. Inflammation drops. Hormonal profiles normalize. Insulin sensitivity increases. All of these changes contribute to higher sustained energy levels.
For most users, the math works out clearly: four to eight weeks of adaptation fatigue followed by months or years of improved energy. The temporary cost is real, but the long-term return is substantial.
This does not mean you should simply endure fatigue passively. Actively managing it with the strategies above makes the adjustment period shorter and less severe. But knowing that the trajectory is positive can help you push through the hardest days with confidence that improvement is coming.
Creating your personal anti-fatigue action plan
Rather than trying to implement every strategy simultaneously, build your action plan in phases that match the fatigue timeline.
Phase 1: Before starting semaglutide (week 0)
Get baseline blood work (CBC, iron panel, B12, vitamin D, thyroid, metabolic panel)
Stock kitchen with protein-rich, nausea-friendly foods
Buy electrolyte powder and key supplements
Begin tracking baseline energy, sleep, and nutrition
Set up meal prep routine
Use the semaglutide dosage calculator to understand your starting protocol
Phase 2: First injection through week 4
Prioritize hydration (64 to 80+ ounces daily with electrolytes)
Eat protein first at every meal (target: 1.2 to 1.6 g/kg/day)
Eat by the clock, four to five small meals, even without appetite
Reduce exercise volume by 30 to 50 percent
Track fatigue daily to identify patterns
Take B12, magnesium, and zinc supplements
Sleep 7 to 9 hours nightly, non-negotiable
Phase 3: Weeks 5 through 8 (stabilization)
Maintain all Phase 2 strategies
Gradually increase exercise volume if fatigue improving
Recheck blood work at week 8
Evaluate whether dose escalation is appropriate based on fatigue score
Reintroduce more diverse foods as GI tolerance improves
Phase 4: Week 9 onward (optimization)
Energy should be returning to baseline or improving
Shift focus from fatigue management to performance optimization
Increase exercise intensity progressively
Continue monitoring protein intake and supplementation
If fatigue persists, investigate underlying causes with healthcare provider
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed semaglutide dosing guides, stacking protocols, and expert support for managing side effects like fatigue.
Frequently asked questions
Does semaglutide fatigue go away?
Yes. For the vast majority of users, semaglutide fatigue resolves within four to eight weeks of starting treatment. The most intense fatigue occurs during the first two weeks and gradually improves as your body adapts to the medication. Long-term studies show that after 68 weeks, patients report better energy levels than their pre-treatment baseline.
Why does semaglutide make me so tired?
Semaglutide causes fatigue through multiple mechanisms: reduced caloric intake creating an energy deficit, blood sugar regulation changes, dehydration from GI side effects, muscle mass loss, nutrient depletion (especially B12, iron, and zinc), central nervous system effects on neurotransmitter signaling, and potential thyroid function changes. Most users experience fatigue from two or three of these mechanisms simultaneously.
Can I take caffeine while on semaglutide?
Moderate caffeine intake (200 to 300 mg daily, roughly two to three cups of coffee) is generally safe with semaglutide. However, caffeine can worsen dehydration and GI side effects, so balance it with extra water intake. Avoid using caffeine as your primary fatigue management strategy, as it masks symptoms without addressing causes.
Should I stop semaglutide if I am too tired?
Do not stop semaglutide without consulting your prescriber. Fatigue alone is rarely a reason to discontinue treatment. Instead, try the management strategies in this guide, including protein optimization, hydration, supplementation, and exercise modification. If fatigue persists beyond eight weeks despite these interventions, discuss dose adjustment or further evaluation with your healthcare provider.
Does the semaglutide dose affect fatigue severity?
Yes. Higher doses are associated with more fatigue, and each dose escalation can temporarily reintroduce fatigue symptoms. The 0.25 mg starting dose typically produces less fatigue than the 2.4 mg maintenance dose. Slower titration with more time at each dose level generally reduces fatigue severity.
Is semaglutide fatigue different from ozempic fatigue?
No. Ozempic is simply a brand name for semaglutide. The fatigue profile is identical because the active ingredient is the same. The difference between Ozempic and other semaglutide products like Wegovy is the approved indication and dosing range, not the fatigue characteristics.
Can semaglutide fatigue cause weight loss to stall?
Indirectly, yes. Severe fatigue reduces physical activity, which lowers total daily energy expenditure. It can also lead to poor food choices (reaching for quick energy from simple carbs) and disrupt sleep, which affects metabolic hormones like leptin and ghrelin. If you notice your weight loss has stalled, addressing fatigue may help restart progress.
What blood tests should I get if semaglutide fatigue does not improve?
Request a comprehensive panel including: complete blood count (CBC), iron panel with ferritin, vitamin B12, folate, vitamin D, magnesium, zinc, thyroid function (TSH and free T4), fasting glucose, and HbA1c. These tests cover the most common medical causes of persistent fatigue during semaglutide treatment.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your energy stay steady, your protein stay high, and your fatigue stay temporary.