Feb 13, 2026

One glass of wine at dinner. That is all you wanted. But now you are three weeks into your tirzepatide protocol, and something feels different. The wine hits harder. Your stomach protests louder. And that familiar warm buzz arrives faster than it used to, leaving you wondering whether you just made a serious mistake by mixing alcohol with your medication.
You are not imagining it. And you are definitely not alone in asking this question.
Thousands of people starting tirzepatide for weight loss or diabetes management run into this exact dilemma. The prescribing information does not explicitly say "no alcohol." Your doctor might have glossed over it. And the internet gives you everything from "totally fine in moderation" to "absolutely never touch it." The truth, as usual, sits somewhere in the middle, tangled up in pharmacology, individual biology, and a handful of mechanisms that most guides never bother to explain.
This guide covers every angle. The pharmacology behind why alcohol feels different on tirzepatide. The specific risks to your blood sugar, your gut, and your pancreas. What the clinical research actually says about GLP-1 receptor agonists and alcohol cravings. And practical, evidence-based guidelines for making informed decisions about drinking while on this medication. Whether you are on Mounjaro, Zepbound, or a compounded formulation, the science applies equally.
What tirzepatide does inside your body (and why alcohol matters)
Before you can understand the alcohol question, you need to understand what tirzepatide actually does beyond helping you lose weight. This is not just another appetite suppressant. It is a dual incretin receptor agonist that fundamentally changes how your body processes food, regulates blood sugar, and even responds to reward signals in your brain.
Tirzepatide activates two receptor systems simultaneously. The GLP-1 receptor and the GIP receptor. This dual mechanism is what separates it from single-agonist medications like semaglutide. Both receptors play roles in insulin secretion, appetite regulation, and gastric emptying. When you activate both at once, the effects on your digestive system are profound.
Here is the mechanism that matters most for alcohol.
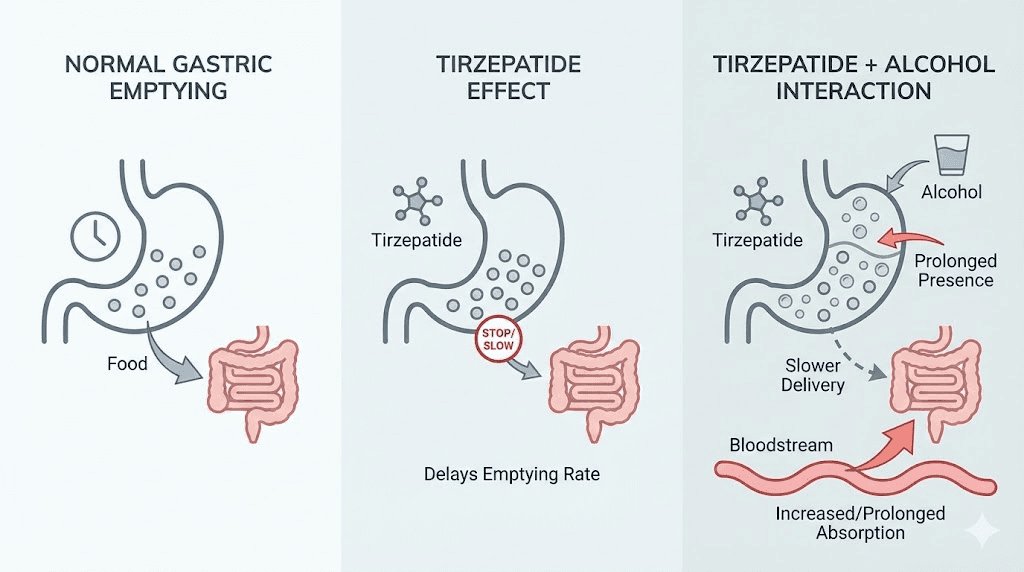
Tirzepatide significantly delays gastric emptying. Your stomach normally processes food and liquids within 2 to 4 hours, pushing contents into the small intestine where most absorption happens. Tirzepatide slows this process down. According to FDA prescribing data, after a first dose of tirzepatide 5 mg, the peak concentration of oral medications was reduced by approximately 50%, and the time to reach peak concentration was delayed by about an hour. This effect is most pronounced after initial doses and diminishes somewhat over time as your body adapts.
Why does this matter for alcohol? Because alcohol absorption depends heavily on gastric emptying speed. When your stomach empties slowly, alcohol sits in the stomach longer before reaching the small intestine. This creates a complicated situation. In some cases, delayed absorption means the alcohol hits you more gradually. In other cases, particularly when you drink on an empty stomach, the alcohol can concentrate in the stomach and then dump into the small intestine all at once, creating an unpredictable spike.
The blood sugar connection
This is where things get genuinely dangerous for some people, and it has nothing to do with how drunk you feel.
Tirzepatide works partly by enhancing insulin secretion when blood sugar rises. Your pancreas releases more insulin in response to food, keeping glucose levels in check. This is excellent for diabetes management and weight loss. But alcohol throws a wrench into this system from a completely different direction.
Ethanol, the active compound in alcoholic drinks, inhibits hepatic gluconeogenesis. That is your liver making new glucose from non-carbohydrate sources, a process that normally keeps your blood sugar stable between meals and overnight. When you drink, your liver prioritizes metabolizing the alcohol over producing glucose. This inhibition can persist for hours after your last drink, well into the next morning.
Now combine these two effects. Tirzepatide enhances insulin action, pulling glucose out of your blood. Alcohol simultaneously prevents your liver from making new glucose to replace what insulin removes. The result can be a significant drop in blood sugar, particularly if you are also taking insulin or sulfonylureas alongside tirzepatide.
According to the Mayo Clinic prescribing information, tirzepatide alone does not typically cause hypoglycemia. But when combined with other glucose-lowering factors, including alcohol, that risk increases substantially. The danger is compounded by the fact that symptoms of hypoglycemia (dizziness, confusion, slurred speech, poor coordination) overlap almost perfectly with symptoms of being drunk. You might think you are just tipsy when your blood sugar is actually crashing.
The GI amplification effect
The most common side effects of tirzepatide are gastrointestinal. Nausea affects roughly 15 to 33% of users depending on the dose, with vomiting, diarrhea, and constipation following close behind. These side effects are most pronounced during the dose escalation phase when your body is still adapting to the medication.
Alcohol is, by itself, a gastrointestinal irritant. It increases stomach acid production, irritates the stomach lining, relaxes the lower esophageal sphincter (promoting acid reflux), and acts as a diuretic that pulls water from your body. Combining these effects with tirzepatide GI side effects creates a compounding problem.
Users consistently report worse nausea, more intense acid reflux, and increased likelihood of vomiting when drinking on tirzepatide compared to their pre-medication experience. This is not a subtle difference. Some describe a single glass of wine triggering hours of nausea that they never would have experienced before starting the medication.
What the research actually says about GLP-1 drugs and alcohol
Here is where the conversation gets fascinating, and where most articles on this topic stop way too short.
There is a growing body of research suggesting that GLP-1 receptor agonists, including tirzepatide, may fundamentally alter how your brain responds to alcohol. Not just the physical absorption and side effects, but the actual reward and craving mechanisms that drive drinking behavior.
The dopamine connection
GLP-1 receptors are not just in your gut and pancreas. They are expressed throughout your brain, particularly in regions tied directly to addiction and reward processing. The ventral tegmental area (VTA), the nucleus accumbens (NAc), and the prefrontal cortex (PFC) all contain GLP-1 receptors. These are the exact brain regions that light up when you drink alcohol, eat something delicious, or experience any pleasurable stimulus.
When tirzepatide activates these receptors, it appears to dampen the dopamine response to rewarding stimuli. A study published in eBioMedicine found that tirzepatide attenuated dopamine reward signaling in the nucleus accumbens and suppressed alcohol drinking and relapse-like behaviors in rodent models. The animals did not just drink less. They showed reduced motivation to seek alcohol even after periods of abstinence.
Another study published in PubMed demonstrated that semaglutide, tirzepatide, and retatrutide all attenuated the interoceptive effects of alcohol in both male and female rats, meaning the animals perceived alcohol differently when GLP-1 receptors were activated. The subjective experience of drinking changed at a neurological level.
Human evidence
The animal data is compelling, but what about humans?
A study published in Scientific Reports (Klausen et al.) examined real-world data and found that both semaglutide and tirzepatide were associated with reduced alcohol consumption in individuals with obesity. Participants reported drinking less, experiencing fewer effects of alcohol intoxication when they did drink, and showed decreased odds of binge drinking.
A study from Virginia Tech researchers found that GLP-1 drugs slowed alcohol absorption, reduced intoxication levels, and cut cravings in a small study of 20 adults. Participants who used GLP-1 receptor agonists showed lower breath alcohol levels compared to controls.
Clinical trials are now underway to formally investigate these effects. ClinicalTrials.gov lists multiple registered studies, including NCT06939088 examining tirzepatide effects on alcohol intake, and NCT06994338 investigating tirzepatide specifically for alcohol use disorder. The scientific community clearly considers this connection significant enough to warrant rigorous clinical investigation.
What this means for you
If you find yourself simply not wanting to drink as much since starting tirzepatide, you are not imagining it. The medication may be directly reducing your brain reward response to alcohol. Many users report that their favorite cocktail just does not taste as appealing, that they lose interest after half a drink, or that the thought of alcohol simply does not cross their mind the way it used to.
This is not a universal experience. Some people report no change in their drinking habits or desires. Individual variation is significant, likely depending on baseline GLP-1 receptor density, drinking patterns, genetic factors, and dose. But the phenomenon is real and increasingly well-documented.
For SeekPeptides members researching peptide protocols, understanding these neurological mechanisms helps contextualize why different people have such dramatically different experiences with alcohol on tirzepatide. It is not just willpower or coincidence. It is pharmacology.
The five real risks of drinking on tirzepatide
Let us move from mechanisms to concrete risks. Not theoretical concerns. Actual, documented dangers that you need to understand before deciding whether and how much to drink while on this medication.
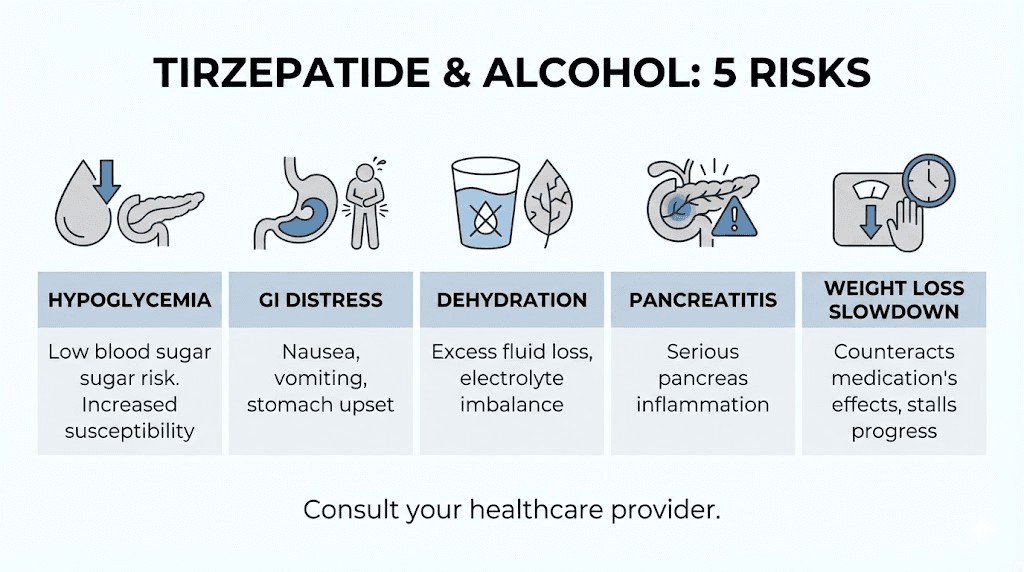
Risk 1: Hypoglycemia (low blood sugar)
This is the most clinically significant risk, and it deserves detailed attention.
As explained above, alcohol blocks your liver from producing glucose while tirzepatide enhances insulin action. The combination can drop your blood sugar into dangerous territory, particularly under these conditions:
You drink without eating adequate food first
You are taking insulin or sulfonylureas alongside tirzepatide
You drink heavily or binge drink
You exercise before or after drinking
You skip meals on the day you drink
Mild hypoglycemia causes shakiness, sweating, irritability, and confusion. Severe hypoglycemia can cause seizures, loss of consciousness, and requires emergency medical intervention. The insidious part is that alcohol masks hypoglycemia symptoms. A blood sugar of 55 mg/dL and three drinks produce nearly identical behavioral signs to an outside observer.
People with type 2 diabetes on combination therapy face the highest risk. But even people using tirzepatide solely for weight loss without diabetes should be aware. The insulin-enhancing effects of tirzepatide do not disappear just because your A1C is normal.
Risk 2: Amplified gastrointestinal distress
Tirzepatide GI side effects and alcohol GI effects are not simply additive. They are synergistic. Your stomach is already operating under altered conditions because of delayed gastric emptying. Adding alcohol, a direct gastric irritant, into this environment creates a perfect storm.
Common experiences reported by users:
Nausea lasting 6 to 12 hours after just 1 to 2 drinks
Severe acid reflux that disrupts sleep
Vomiting triggered by amounts of alcohol that previously caused no problems
Bloating and abdominal discomfort that persists into the following day
Diarrhea or alternating constipation and diarrhea
The foods you eat alongside alcohol matter enormously here. Greasy, heavy foods that further slow gastric emptying will compound the problem. If you choose to drink, eating a moderate, balanced meal first (rather than heavy bar food) can reduce but not eliminate the GI amplification.
Risk 3: Severe dehydration
Tirzepatide changes your relationship with fluids. Many users report reduced thirst signals, possibly related to the appetite-suppressing mechanisms. You may already be drinking less water than you realize. Add nausea (which makes drinking water unappealing) and you have a baseline hydration deficit that many users carry without recognizing it.
Alcohol is a potent diuretic. It suppresses antidiuretic hormone (ADH, also called vasopressin), causing your kidneys to excrete more water than you are taking in. This is why you urinate frequently when drinking and wake up dehydrated the next morning.
Combining tirzepatide dehydration tendencies with alcohol diuretic effects can push you into clinically significant dehydration. Symptoms include severe headache, dizziness, rapid heartbeat, dark urine, dry mouth, and fatigue. In extreme cases, dehydration can contribute to acute kidney injury, which brings us to the next risk.
Risk 4: Pancreatitis
This is rare but serious enough that it demands your attention.
GLP-1 receptor agonists carry a label warning about pancreatitis. Clinical trials showed that tirzepatide had similar pancreatitis rates to placebo overall, but real-world case reports exist. A case report published in the Journal of Clinical Endocrinology and Metabolism documented fatal, fulminant, necrotizing pancreatitis associated with recent tirzepatide initiation. Another case published in PMC documented acute pancreatitis caused by tirzepatide.
Heavy alcohol consumption is independently one of the strongest risk factors for pancreatitis. When you combine a medication that carries some pancreatic risk with a substance that independently damages the pancreas, the math is not in your favor. This is particularly concerning for people who drink heavily, have a history of pancreatitis, or have gallbladder disease.
You do not need to panic about this with moderate, occasional drinking. But binge drinking while on tirzepatide is genuinely reckless from a pancreatic safety standpoint.
Risk 5: Undermining your weight loss results
This risk is not life-threatening, but it might be the one that matters most to your goals.
Alcohol is calorically dense. A standard glass of wine contains 120 to 150 calories. A craft beer runs 200 to 350 calories. A margarita can pack 300 to 500 calories. These are not trivial numbers when you are working with the caloric deficit that tirzepatide creates through appetite suppression.
But the calorie count only tells part of the story. Alcohol disrupts fat metabolism directly. Your liver prioritizes processing ethanol over burning fat, essentially pausing fat oxidation until all the alcohol is metabolized. Depending on how much you drink, this pause can last 12 to 24 hours. If you drink regularly, you are consistently interrupting the metabolic benefits that tirzepatide provides.
Alcohol also degrades sleep quality. Even if you fall asleep easily after drinking, alcohol fragments your sleep architecture, reducing REM sleep and deep sleep. Poor sleep increases cortisol, raises ghrelin (the hunger hormone), and reduces leptin (the satiety hormone). These hormonal shifts can partially counteract tirzepatide appetite suppression the following day, leading to increased hunger, cravings for high-calorie foods, and reduced willpower around dietary choices.
Then there is the decision-making factor. Alcohol impairs judgment. The careful food choices you make while sober, the ones that complement your tirzepatide meal plan, tend to evaporate after a few drinks. Late-night snacking, fast food stops, and "I will get back on track tomorrow" rationalizations are standard alcohol-fueled behaviors that can significantly slow your progress.
How alcohol tolerance changes on tirzepatide
This deserves its own section because the shift catches people completely off guard.
If you used to handle three glasses of wine without issue, do not assume you still can. Many people starting tirzepatide report that their alcohol tolerance drops dramatically. One drink feels like two. Two drinks feel like four. The effects arrive faster, hit harder, and linger longer.
Why tolerance changes
Several mechanisms contribute to this shift.
First, delayed gastric emptying alters absorption kinetics. The timing and intensity of alcohol effects become less predictable. You might feel fine for 30 minutes and then suddenly feel very intoxicated as your stomach releases a bolus of alcohol-containing fluid into your small intestine.
Second, weight loss itself reduces alcohol tolerance. As you lose weight on tirzepatide, your body composition changes. Less body mass means less volume to dilute alcohol, so the same number of drinks produces higher blood alcohol concentrations. If you have lost 15 to 30 pounds since starting the medication, your old drinking habits may produce significantly stronger effects.
Third, the neurological changes discussed earlier may alter your subjective experience of alcohol. If tirzepatide is dampening dopamine reward signals, you might feel the negative effects of alcohol (nausea, fatigue, malaise) more prominently while experiencing less of the pleasurable effects (euphoria, relaxation, social lubrication). This changes the entire risk-reward equation of drinking.
Fourth, many people eat less on tirzepatide due to appetite suppression. Drinking on an emptier stomach accelerates absorption and intensifies effects regardless of medication status.
What users actually report
The range of experiences is wide, but patterns emerge consistently across forums and clinical observations.
Some users report a complete loss of interest in alcohol. The craving simply disappears, as if a switch was flipped. They can sit at a bar with friends and genuinely prefer sparkling water, not because they are forcing themselves, but because alcohol simply does not appeal anymore.
Others notice a dramatic reduction in tolerance without any change in desire. They still want to drink but find that one beer produces effects they used to need three beers to achieve. This group faces the highest risk of accidentally overdrinking because their habits have not caught up with their new physiology.
A smaller group reports minimal changes in either desire or tolerance. Alcohol feels and functions the same as before tirzepatide. This appears more common in people who were light or occasional drinkers before starting the medication.
And an interesting subset reports that certain types of alcohol hit differently. Wine might be intolerable while spirits are fine, or beer causes intense bloating while cocktails are manageable. This likely relates to the carbohydrate content, carbonation, and volume differences between alcohol types interacting with delayed gastric emptying in variable ways.
Safe drinking guidelines while on tirzepatide
The FDA prescribing information for tirzepatide does not include a blanket prohibition on alcohol. There is no formal contraindication. This means that moderate, informed alcohol consumption is not categorically off the table for most people.
But "not contraindicated" is different from "safe and risk-free." Here is a practical framework based on the pharmacology and clinical evidence.
Before you drink: preparation
Eat a substantial, balanced meal at least 30 minutes before your first drink. Not greasy bar food. A meal containing protein, complex carbohydrates, and healthy fats. This slows alcohol absorption further (on top of the already-delayed gastric emptying) and provides glucose reserves that buffer against hypoglycemia.
Hydrate aggressively before you start drinking. Aim for at least 16 to 24 ounces of water before your first alcoholic beverage. Given that tirzepatide already predisposes you to dehydration, starting from a deficit is dangerous.
Check your blood sugar if you are diabetic. Know your baseline number before introducing alcohol into the equation. Have glucose tablets or a fast-acting carbohydrate source accessible.
Know which day you are relative to your last tirzepatide injection. The first 48 to 72 hours after injection, when drug levels are peaking and gastric emptying delay is strongest, carry the highest risk for amplified alcohol effects. If you know you have a social event coming up, some people time their injection to maximize the gap between injection and drinking occasion.
While drinking: guidelines
Start with one drink. Just one. Assess how you feel after 45 to 60 minutes before considering a second. Your old tolerance benchmarks do not apply. Treat yourself as a new drinker discovering your limits for the first time.
The general medical guidance is no more than one drink per day for women and no more than two drinks per day for men. On tirzepatide, many healthcare providers recommend staying at or below these limits.
One standard drink equals 12 ounces of regular beer (5% ABV), 5 ounces of wine (12% ABV), or 1.5 ounces of distilled spirits (40% ABV). Craft beers, generous pours, and cocktails with multiple spirits often contain significantly more alcohol than one standard drink.
Alternate every alcoholic drink with a full glass of water. This sounds like standard advice because it is. It works even better on tirzepatide because you are fighting dehydration from two directions.
Avoid sugary cocktails and mixers. Margaritas, daiquiris, Long Island iced teas, and anything with significant sugar content create blood sugar spikes followed by crashes. The interaction between sugar-driven insulin response and alcohol-driven gluconeogenesis inhibition is particularly risky. Dry wine, spirits with soda water, or light beer are lower-risk choices.
Avoid carbonated alcohol if possible. Beer and sparkling wine can exacerbate the bloating and GI discomfort that tirzepatide already causes. The carbonation creates gas in an already slow-emptying stomach, which is a recipe for misery.
After drinking: recovery
Continue hydrating. Drink at least 16 ounces of water before bed and keep water accessible through the night.
Eat a small snack containing complex carbohydrates before sleep. A piece of toast, some crackers, or a banana can help maintain blood sugar through the night when alcohol gluconeogenesis inhibition is at its strongest.
Monitor for hypoglycemia symptoms through the following morning. Shakiness, excessive sweating, confusion, and irritability upon waking could indicate low blood sugar rather than a standard hangover.
If you are diabetic, check your blood sugar before bed and again upon waking. The risk of delayed hypoglycemia extends well into the following morning, particularly after evening drinking.
Alcohol types ranked by risk on tirzepatide
Not all alcoholic beverages carry equal risk when you are on tirzepatide. The sugar content, carbonation, volume, and ABV all interact with the medication differently.
Lower-risk options
Dry red or white wine (5 oz) contains minimal residual sugar, no carbonation, and a predictable alcohol content. A single glass with dinner is generally the most tolerable option for tirzepatide users. Stick to dry varieties (Cabernet, Pinot Noir, Sauvignon Blanc, Chardonnay) rather than sweet wines (Moscato, Riesling, Port) which add unnecessary sugar.
Spirits with non-sugary mixers are another reasonable choice. Vodka with soda water and lime, gin and tonic (using diet tonic), or whiskey neat or on the rocks deliver alcohol without added sugar or carbonation. The smaller volume compared to beer or wine can be easier on your already-compromised stomach.
Moderate-risk options
Light beer contains less alcohol per serving but involves carbonation and larger fluid volume, both of which can aggravate GI symptoms. If beer is your preference, one light beer is unlikely to cause major problems, but the bloating and discomfort may surprise you compared to pre-tirzepatide experience.
Champagne and sparkling wine combine alcohol with aggressive carbonation. The gas expands in a slow-emptying stomach and can cause significant discomfort, belching, and nausea. Many tirzepatide users report that sparkling wines are by far the least tolerable option.
Higher-risk options
Sugary cocktails are the worst choice on tirzepatide. Margaritas, pina coladas, cosmopolitans, and anything made with simple syrup, fruit juice, or liqueurs deliver massive sugar loads alongside alcohol. This combination creates blood sugar volatility (spike from sugar, crash from alcohol liver inhibition) and adds hundreds of empty calories that directly undermine your weight loss progress.
Binge drinking of any type is categorically high-risk. Three or more drinks in one sitting dramatically increases hypoglycemia risk, pancreatitis risk, severe dehydration, and GI distress. There is no safe way to binge drink on tirzepatide.
Craft beers and high-ABV beverages are deceptive. A single craft IPA at 8 to 10% ABV contains roughly double the alcohol of a standard beer. Many people count it as "one drink" when it is pharmacologically equivalent to nearly two. On tirzepatide, this miscalculation has outsized consequences.
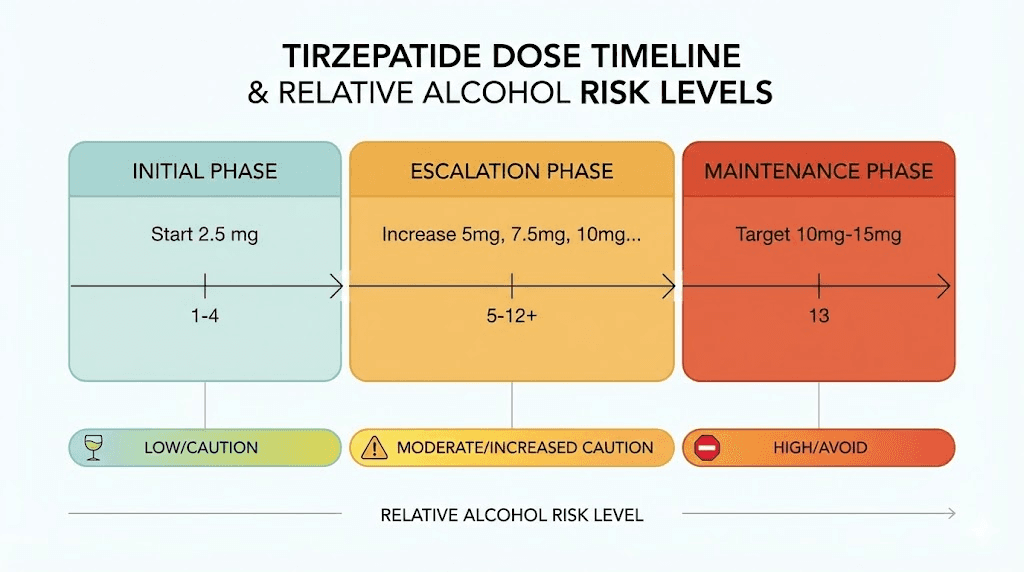
The tirzepatide dosing phase matters
Your risk profile with alcohol changes significantly depending on where you are in your tirzepatide dose escalation.
Initial phase (weeks 1 to 4, starting dose)
During the first month, your body is adjusting to tirzepatide. GI side effects are typically at their peak. Nausea, appetite changes, and digestive unpredictability make this the worst time to introduce alcohol. Many users report that even small amounts of alcohol during the initial phase cause outsized GI distress.
Recommendation: avoid alcohol entirely for the first 2 to 4 weeks if possible. Let your body acclimate to the medication before adding another variable.
Dose escalation phase (months 1 to 4)
Each dose increase temporarily reintroduces GI side effects as your body adjusts to the higher level. The week following each dose increase is essentially a mini version of the initial adjustment period. The standard tirzepatide dosing schedule increases the dose every 4 weeks, so you cycle through adjustment periods repeatedly.
Recommendation: avoid or severely limit alcohol during the first week after each dose increase. By weeks 2 to 4 at each dose level, your GI system has typically adjusted enough to tolerate moderate, careful drinking.
Maintenance phase (stable dose)
Once you reach your maintenance dose and your body has fully adapted (typically after 2 to 4 weeks at a stable dose), the GI side effects generally settle. This is when moderate, informed drinking is most feasible. Your body has established a new baseline, and the gastric emptying delay, while still present, is more predictable.
Recommendation: moderate drinking following the guidelines above is reasonable for most people in the maintenance phase. Still follow all safety precautions, especially around hydration and blood sugar monitoring.
Specific situations and scenarios
Real life is not a clinical trial. Here are practical answers to the scenarios that tirzepatide users actually encounter.
"I have a wedding/party coming up"
Plan your injection timing if possible. Inject 4 to 5 days before the event so drug levels are lower on the day. Eat a full meal before arriving. Set a firm drink limit (two maximum for most people) and tell someone you trust about your limit. Have your car accessible so you can leave when you choose. Alternate every drink with water. Skip the toast champagne if carbonation bothers you and sip your own dry wine instead.
"I want to have a glass of wine with dinner once a week"
This is probably the most manageable scenario. A single glass of dry wine with a full dinner, consumed slowly over the course of the meal, represents minimal risk for most tirzepatide users. Ensure you hydrate before and after. Choose a night when your tirzepatide dose is not freshly administered if possible.
"My friends are pressuring me to drink"
You do not owe anyone an explanation about your medication. "I am not drinking tonight" is a complete sentence. If you want something in your hand, sparkling water with lime looks identical to a vodka soda. Many tirzepatide users report that the medication has given them an unexpected gift in this regard, a genuine, pharmacological disinterest in alcohol that makes saying no effortless rather than difficult.
"I drank too much and feel terrible"
Prioritize hydration immediately. Small, frequent sips of water or an oral rehydration solution (like Pedialyte) are better than gulping large amounts that your slow-emptying stomach may reject. Eat simple, bland carbohydrates (crackers, toast, banana) to support blood sugar. If you are diabetic, check blood sugar every 2 to 3 hours. Contact your healthcare provider if you experience severe abdominal pain (possible pancreatitis warning), persistent vomiting that prevents any fluid intake (dehydration emergency), confusion or loss of consciousness (possible severe hypoglycemia), or blood sugar readings below 54 mg/dL.
"Can I drink the night before my injection?"
Yes, from a pharmacological standpoint, drinking before your injection does not interact with the medication itself. The tirzepatide has not been administered yet, so there is no drug-alcohol interaction occurring. However, if you wake up hungover and dehydrated, administering tirzepatide on top of that is likely to amplify nausea and GI discomfort. Starting your dose adjustment from a dehydrated, nauseated baseline is not ideal.
Better approach: ensure you are well-hydrated and feeling normal before your injection. If you had a heavy night, consider delaying your injection by a day while you recover.
Tirzepatide versus semaglutide: does the alcohol interaction differ?
If you have read about drinking on semaglutide, you might wonder whether tirzepatide is meaningfully different.
The core mechanisms are similar. Both medications delay gastric emptying, enhance insulin action, and activate GLP-1 receptors in the brain reward system. The alcohol risks, hypoglycemia, GI amplification, dehydration, and pancreatitis, apply to both drugs.
However, tirzepatide has unique characteristics that may slightly alter the experience.
Tirzepatide is a dual agonist (GLP-1 plus GIP), while semaglutide is a GLP-1 single agonist. The GIP receptor activation in tirzepatide may contribute additional effects on gastric emptying and reward signaling that semaglutide does not provide. In clinical trials, tirzepatide produced greater weight loss than semaglutide at comparable timepoints, suggesting more potent metabolic effects overall.
The GI side effect profile differs somewhat. Both cause nausea, but the specific patterns, timing, and severity can vary. Some people who struggled with semaglutide GI effects tolerate tirzepatide better, and vice versa. Your alcohol experience may similarly differ between the two medications.
From the alcohol research perspective, the animal studies that examined both drugs found that both reduced alcohol intake and attenuated reward signaling, but tirzepatide dual receptor mechanism may provide a more comprehensive dampening of alcohol reward compared to semaglutide single receptor approach. The dosage relationship between the two medications does not translate directly to alcohol interaction intensity.
The alcohol cravings question: is tirzepatide actually treating addiction?
This is the most provocative question in the current GLP-1 research landscape, and it has direct implications for anyone wondering about drinking on tirzepatide.
Multiple registered clinical trials are now investigating whether tirzepatide and similar drugs could treat alcohol use disorder (AUD). This is not fringe science. These are mainstream clinical trials listed on ClinicalTrials.gov, funded by major institutions, and published in respected journals.
The mechanism is plausible. GLP-1 receptors in the VTA and NAc modulate dopaminergic, glutamatergic, and GABAergic neurotransmission, all three major neurotransmitter systems involved in addiction. By activating these receptors, tirzepatide may be simultaneously reducing the reward you get from alcohol, reducing cravings for alcohol, and reducing the motivation to seek alcohol after periods of abstinence.
Stanford researchers have identified five key things to know about GLP-1 drugs and addiction. First, the preclinical evidence is remarkably consistent across multiple substances (alcohol, nicotine, opioids, cocaine). Second, the effects appear to be centrally mediated rather than just a consequence of feeling sick or full. Third, individual responses vary enormously. Fourth, there may be an optimal dose range for addiction effects that differs from the dose used for weight loss. And fifth, we need large, rigorous human trials before drawing definitive conclusions.
For the everyday tirzepatide user who notices reduced interest in alcohol, this research provides a reassuring scientific framework. You are not being weird. Your brain chemistry is being modulated by the medication in ways that happen to reduce alcohol reward. Whether this is a benefit, a side effect, or a therapeutically useful property depends entirely on your individual relationship with alcohol.
SeekPeptides tracks these emerging research developments closely, providing members with updated summaries as clinical trial results become available. The intersection of peptide therapeutics and addiction neuroscience is one of the most exciting areas of current research.
Special populations and additional considerations
People with type 2 diabetes
If you are using tirzepatide for diabetes (brand name Mounjaro), the alcohol-hypoglycemia risk is your primary concern. This is not theoretical for you. It is a concrete, daily management challenge. Discuss alcohol use openly with your diabetes care team. They can advise on insulin dose adjustments, blood sugar monitoring schedules, and emergency protocols specific to your medication regimen.
The combination of tirzepatide plus insulin plus sulfonylureas plus alcohol creates the highest hypoglycemia risk. If you are on this combination, extreme caution with alcohol is warranted, and many endocrinologists will recommend abstaining entirely.
People with a history of pancreatitis
If you have had pancreatitis before, the threshold for recurrence is lower. Adding alcohol to tirzepatide in this context is medically inadvisable. Even moderate drinking may be enough to trigger a recurrence when combined with GLP-1 receptor agonist effects on the pancreas. Discuss this specifically with your gastroenterologist.
People with liver disease
Tirzepatide is metabolized through proteolytic cleavage rather than hepatic metabolism, which means liver disease does not significantly alter tirzepatide drug levels. However, a compromised liver processes alcohol more slowly and is more vulnerable to alcohol-related damage. The combination of reduced alcohol clearance and tirzepatide GI effects can be particularly problematic.
People taking other medications
Alcohol interacts with hundreds of medications beyond tirzepatide. If you are taking antidepressants, benzodiazepines, sleep medications, pain medications, or blood pressure drugs, the alcohol interaction picture becomes considerably more complex. Discuss your complete medication list with your pharmacist or healthcare provider before drinking on tirzepatide.
People using compounded tirzepatide
If you are using a compounded tirzepatide formulation rather than brand-name Mounjaro or Zepbound, the same alcohol risks apply. The active compound is identical. However, compounded formulations may vary slightly in their reconstitution and concentration, so ensure you know your exact dose and monitor accordingly.
What to do if you want to quit or reduce drinking on tirzepatide
For some people, tirzepatide provides an unexpected catalyst for reducing alcohol consumption. If you are in this group and want to lean into the effect, here are strategies that complement the pharmacological nudge the medication provides.
Replace the ritual, not just the drink
Much of drinking behavior is habitual rather than craving-driven. You drink wine at dinner not because you desperately need wine, but because that is what you do at dinner. Replace the ritual with a non-alcoholic alternative that occupies the same space. Sparkling water with bitters, non-alcoholic craft beverages, herbal tea, or kombucha can fill the glass in your hand without the alcohol in your bloodstream.
Track your consumption honestly
If you are reducing but not eliminating alcohol, track what you actually drink versus what you think you drink. Most people underestimate their consumption by 30 to 50%. A simple note in your phone each time you have a drink provides data you can review with your healthcare provider.
Leverage the reduced cravings
If tirzepatide is reducing your alcohol cravings, this is a window of opportunity. Building alcohol-free habits while the pharmacological support is active makes those habits more likely to stick even if you eventually discontinue the medication. Your brain is essentially getting a neurochemical assist in forming new patterns.
Communicate with your support system
Tell trusted friends, family, or your partner that you are reducing alcohol intake. Social drinking environments are the highest-risk setting for overconsumption. Having allies who understand your goals and can support your decisions makes a meaningful difference.
The bottom line: a decision framework
Can you drink on tirzepatide? Technically, yes. There is no absolute contraindication.
Should you drink on tirzepatide? That depends on a more nuanced assessment.
Consider avoiding alcohol entirely if:
You are in the first 2 to 4 weeks of starting tirzepatide
You just increased your dose within the past week
You have type 2 diabetes on insulin or sulfonylureas
You have a history of pancreatitis
You have liver disease
You tend toward binge drinking
Moderate, careful drinking is likely acceptable if:
You are on a stable maintenance dose
Your GI side effects have settled
You do not have diabetes or other high-risk conditions
You stick to 1 to 2 standard drinks maximum
You eat a full meal beforehand
You hydrate aggressively before, during, and after
The most important principle is this: assume your tolerance has changed. Do not use pre-tirzepatide drinking behavior as your benchmark. Start low, go slow, and pay attention to how your body responds. Your physiology is different now, and your approach to alcohol should reflect that change.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers comprehensive guidance on managing tirzepatide alongside lifestyle factors, including alcohol, nutrition, exercise, and supplementation. Members access detailed protocol management tools and a community of thousands navigating these exact questions.
Frequently asked questions
Does tirzepatide interact directly with alcohol?
There is no direct pharmacological interaction between tirzepatide and alcohol at the molecular level. The FDA prescribing information does not list alcohol as a contraindication. However, the indirect interactions through delayed gastric emptying, enhanced insulin action, and GI side effect amplification create meaningful clinical risks that warrant caution.
How long after taking tirzepatide can I drink?
Tirzepatide is a once-weekly injection with a half-life of approximately 5 days, so the drug is always present in your system between doses. There is no "safe window" where the medication is inactive. However, the gastric emptying delay is most pronounced in the first 24 to 48 hours after injection. Drinking 3 to 5 days after your injection, when drug levels are somewhat lower, may reduce the intensity of GI interactions.
Can tirzepatide cure alcoholism?
No. While preclinical research and early human data suggest that tirzepatide and other GLP-1 receptor agonists may reduce alcohol cravings and consumption, tirzepatide is not approved or indicated for alcohol use disorder. Clinical trials are actively investigating this potential use, but results are pending. If you struggle with alcohol dependence, please seek professional help through established treatment channels.
Will drinking slow my weight loss on tirzepatide?
Yes, almost certainly. Alcohol adds empty calories, pauses fat oxidation, disrupts sleep quality, increases next-day hunger, and impairs dietary decision-making. Regular drinking can significantly reduce the weight loss benefits of tirzepatide. Occasional, moderate drinking has a smaller impact but still contributes to slower progress compared to abstaining. Track your tirzepatide results closely if you choose to include alcohol in your lifestyle.
What should I do if I feel very sick after drinking on tirzepatide?
Stop drinking immediately. Sip water slowly in small amounts. Eat bland carbohydrates if you can keep them down. Monitor for severe symptoms including persistent vomiting, severe abdominal pain (pancreatitis warning), confusion or disorientation (hypoglycemia warning), or inability to keep any fluids down for more than 4 to 6 hours. Contact your healthcare provider or go to urgent care if symptoms are severe or if you suspect hypoglycemia.
Is beer or wine safer on tirzepatide?
Dry wine in a standard 5-ounce pour is generally the best-tolerated alcoholic beverage for tirzepatide users. It avoids the carbonation issues of beer and the sugar content of cocktails. Beer carbonation specifically tends to cause more bloating and GI discomfort when gastric emptying is delayed. Spirits with non-sugary mixers are also reasonable options. Sugary cocktails are the worst choice due to blood sugar volatility.
Can I drink on compounded tirzepatide?
The same guidelines apply to compounded tirzepatide as to brand-name Mounjaro or Zepbound. The active ingredient is identical, so the pharmacological interactions with alcohol are the same. Ensure you know your exact compounded dose and follow the same precautions outlined in this guide.
Does tirzepatide make hangovers worse?
Many users report significantly worse hangovers on tirzepatide, even after drinking less than they used to. The combination of dehydration (from both the medication and alcohol), GI irritation, disrupted sleep, and potential blood sugar instability creates a hangover experience that is disproportionate to the amount consumed. The standard hangover remedies, hydration, electrolytes, rest, bland food, apply but may be less effective than pre-tirzepatide.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your blood sugar stay stable, your hydration stay strong, and your decisions stay informed.