Feb 12, 2026
The confusion keeps spreading. Phentermine. GLP-1. Two terms that show up in the same conversations, the same search results, the same weight loss forums. And somewhere along the way, people started assuming they were the same thing.
They are not. Not even close.
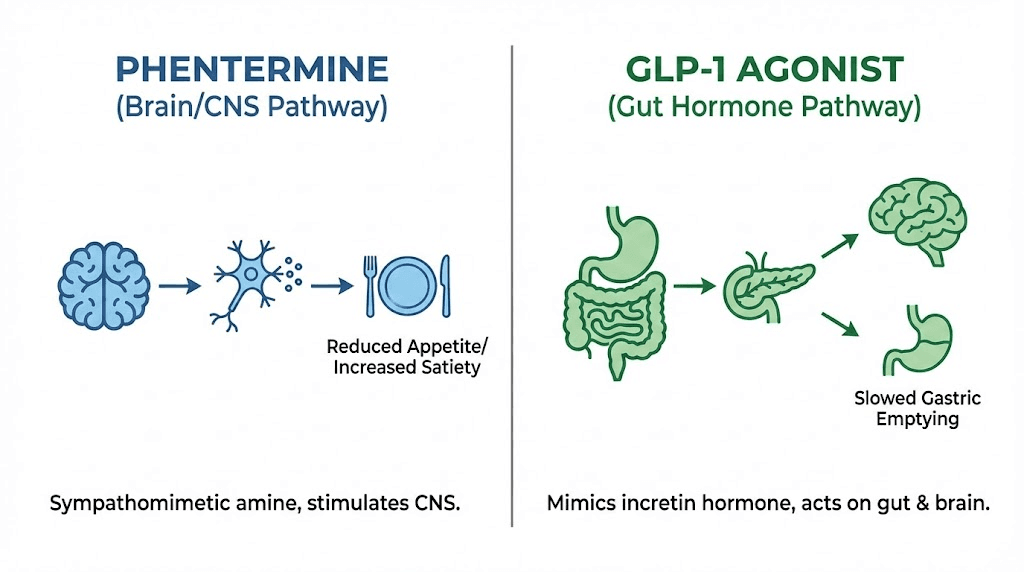
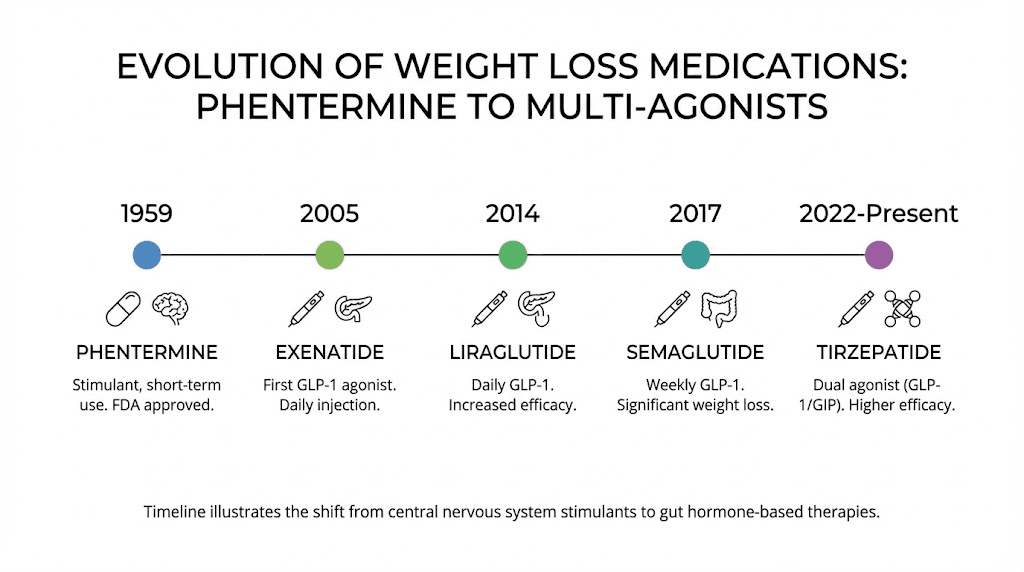
Phentermine is a central nervous system stimulant that has been around since 1959. It works in your brain. GLP-1 receptor agonists like semaglutide and tirzepatide are peptide-based medications that mimic a hormone your gut already produces. One revs up your nervous system to blunt hunger. The other works with your body's own signaling pathways to regulate appetite, digestion, and blood sugar from the ground up. The mechanisms are completely different, the side effects are different, the duration of treatment is different, and the long-term outcomes are different. Lumping them together because they both help people lose weight is like saying a bicycle and a jet engine are the same thing because they both move you forward.
This guide breaks down every meaningful distinction between phentermine and GLP-1 medications. You will understand exactly how each one works at the molecular level, what kind of weight loss to realistically expect, which side effects to watch for, how long you can safely use each option, and whether combining them is even worth considering. SeekPeptides has spent extensive time analyzing the clinical data behind both drug classes, and the differences matter more than most people realize.
If you have been wondering whether phentermine belongs in the GLP-1 category, or whether one might work better for your situation, everything you need is right here.
The short answer: phentermine is not a GLP-1
No. Phentermine is not a GLP-1 receptor agonist, and it does not belong to the GLP-1 drug class in any way. This is not a gray area or a matter of classification debate. These medications are as different as ibuprofen and insulin.
Phentermine is a sympathomimetic amine. That means it mimics the effects of your sympathetic nervous system, the fight-or-flight response that increases heart rate, raises alertness, and suppresses appetite. The FDA first approved it in 1959, making it one of the oldest weight loss medications still prescribed today. It is classified as a Schedule IV controlled substance because of its chemical similarity to amphetamines and its potential for dependence.
GLP-1 receptor agonists are an entirely separate class. GLP-1 stands for glucagon-like peptide-1, a hormone your intestines naturally release after you eat. This hormone tells your brain you are full, slows down how fast food leaves your stomach, and helps regulate insulin and blood sugar levels. Medications like semaglutide and tirzepatide are synthetic versions of this hormone, designed to activate the same receptors at higher and more sustained levels than your body produces on its own.
The distinction matters because it affects everything downstream. How the drug enters your system. What it does once it gets there. How long the effects last. What happens when you stop taking it. And most importantly, what kind of results you can realistically expect.
How phentermine actually works
Understanding phentermine requires looking at what happens in your brain when you take it. This is a top-down medication. It starts in the central nervous system and works outward.
The neurotransmitter cascade
When you swallow a phentermine tablet, the drug crosses the blood-brain barrier within about 30 minutes. Once inside your brain, it triggers the release of three key neurotransmitters: norepinephrine, dopamine, and to a much lesser extent, serotonin. Norepinephrine is the primary player here. It is the same chemical your body floods your system with during a stressful situation, and it directly suppresses your appetite by acting on the hypothalamus, the brain region responsible for hunger and satiety signals.
The dopamine release is secondary but still important. It creates a mild sense of alertness and well-being that many users describe as feeling more focused and energetic. This is why phentermine is classified alongside other sympathomimetic amines. It literally mimics the effects of sympathetic nervous system activation.
Think of it this way. Your body has a natural appetite suppression system that kicks in during high-stress situations. You have probably experienced this yourself. A stressful deadline, a scary situation, an intense workout. Your hunger vanishes. Phentermine artificially activates this same pathway, keeping your appetite suppressed throughout the day without the actual stress.
What phentermine does not do
Here is where the critical distinction begins. Phentermine does not affect your gut hormones. It does not slow gastric emptying. It does not improve insulin sensitivity. It does not regulate blood sugar. It does not interact with GLP-1 receptors, GIP receptors, or any of the incretin pathways that GLP-1 medications target. It is purely a brain-based appetite suppressant that works through stimulant mechanisms.
This means phentermine does not address any of the metabolic factors that drive weight gain beyond simple calorie intake. If your weight challenges involve insulin resistance, hormonal imbalances, or disrupted satiety signaling from the gut, phentermine only addresses one piece of a much larger puzzle.
The timeline of phentermine effects
Phentermine works fast. Most people notice reduced appetite within the first 24 to 48 hours. The peak effects typically hit within the first one to two weeks. Weight loss during this period can be rapid, often three to five pounds in the first week, though much of this is water weight.
By week four to six, however, many people notice the appetite-suppressing effects beginning to fade. This is called tachyphylaxis, and it is one of the biggest limitations of phentermine therapy. Your brain adapts to the elevated norepinephrine levels and starts compensating, requiring either higher doses (which increases side effect risk) or cycling off the medication entirely.
The typical phentermine prescription lasts 12 weeks at most. Some physicians extend this to six months, but beyond that, the risk-to-benefit ratio becomes unfavorable for most patients. The FDA approval specifically states short-term use only.
How GLP-1 receptor agonists actually work
GLP-1 medications take the opposite approach. Instead of forcing appetite suppression through stimulant pathways, they work with your body's natural hunger regulation system. The difference is not subtle.
The incretin effect
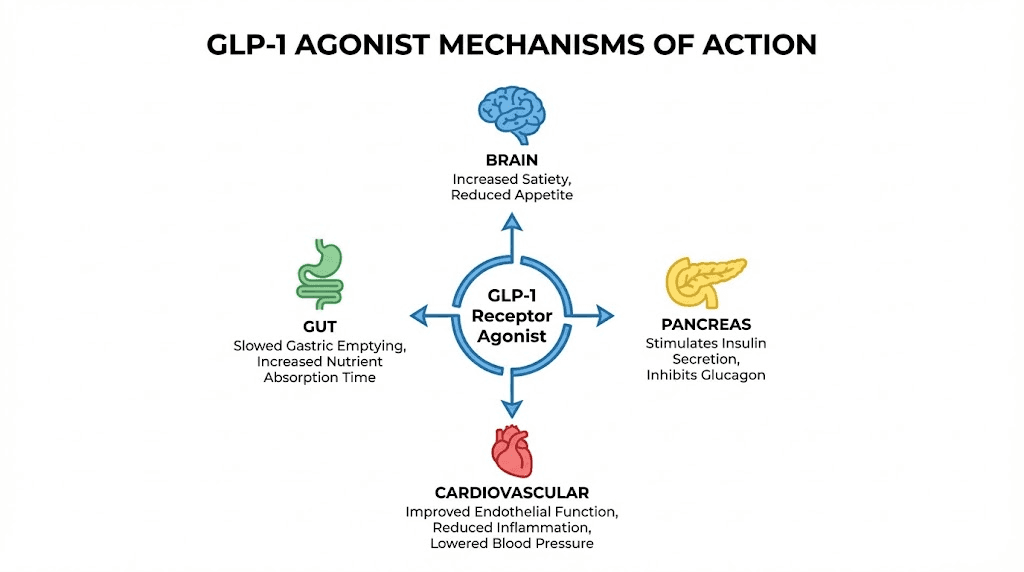
After you eat a meal, your intestinal L-cells release a hormone called GLP-1. This hormone does several things simultaneously. It signals your pancreas to release insulin in a glucose-dependent manner, meaning it only increases insulin when blood sugar is actually elevated. It suppresses glucagon, a hormone that raises blood sugar. It slows gastric emptying, keeping food in your stomach longer so you feel full for extended periods. And it acts directly on appetite centers in the brain, creating a genuine sensation of satiety rather than artificially blocking hunger signals.
The problem with natural GLP-1 is that it degrades rapidly. Your body breaks it down within two to three minutes through an enzyme called DPP-4. You produce it, it does its job briefly, and then it vanishes.
Medications like semaglutide and tirzepatide solve this problem by modifying the GLP-1 molecule to resist DPP-4 degradation. Semaglutide has a half-life of approximately 168 hours, which is roughly one week. This means a single weekly injection maintains therapeutic GLP-1 receptor activation around the clock, something your body could never achieve on its own.
Multiple mechanisms working together
What makes GLP-1 medications fundamentally different from phentermine is the breadth of their effects. They do not just suppress appetite through one pathway. They address weight management from multiple angles simultaneously.
Appetite regulation happens both centrally (in the brain) and peripherally (in the gut). Semaglutide suppresses appetite through direct action on brain regions that control food reward and hunger, while also slowing digestion so food sits in your stomach longer. Users often describe this as simply not thinking about food anymore, rather than fighting through hunger the way phentermine users do.
Blood sugar regulation adds another layer. Improved insulin sensitivity means your body processes carbohydrates more efficiently, reducing the blood sugar spikes and crashes that drive cravings and overeating. This is why GLP-1 medications were originally developed for type 2 diabetes, and the weight loss benefits were initially considered a welcome side effect.
Cardiovascular protection is the third layer. Semaglutide (as Wegovy) received FDA approval for reducing cardiovascular risk in overweight and obese adults, making it the first weight loss medication to also demonstrate heart protection. Phentermine, being a stimulant, actually increases cardiovascular strain in some patients.
Tirzepatide: the dual-agonist advantage
If semaglutide represents the next generation beyond phentermine, tirzepatide represents the generation after that. While semaglutide activates only GLP-1 receptors, tirzepatide activates both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. This dual mechanism produced the most impressive weight loss results ever seen in clinical trials for any medication.
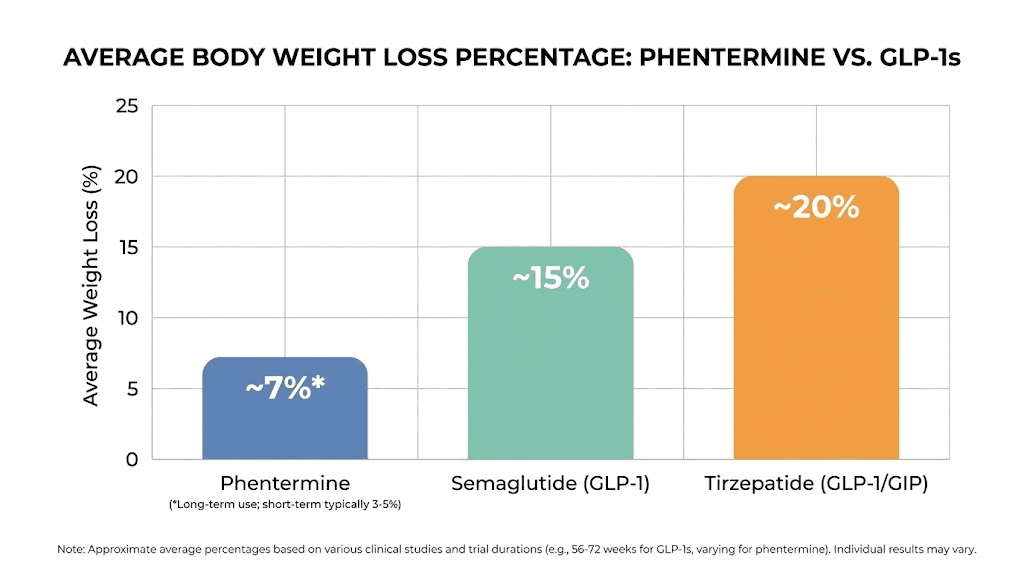
In the SURMOUNT-1 trial, participants taking the highest dose of tirzepatide (15mg weekly) lost an average of 22.5% of their body weight over 72 weeks. That translates to roughly 52 pounds for someone starting at 230 pounds. Compare that to phentermine's typical 5-10% body weight loss over 12 weeks, and the magnitude of the difference becomes clear.
Tirzepatide is not technically classified as a pure GLP-1 receptor agonist because of its dual action, but it belongs firmly in the incretin-based medication family. It has nothing in common with phentermine's stimulant mechanism. Other dual and triple agonists are currently in development, pushing the incretin approach even further.
Weight loss results: a head-to-head comparison
Numbers tell the real story. When you compare the weight loss outcomes of phentermine versus GLP-1 medications across clinical trials and real-world data, the gap is substantial.
Phentermine weight loss data
Phentermine typically produces 5-10% total body weight loss over 12 to 24 weeks of use. For a 200-pound person, that means losing 10 to 20 pounds. Most of this weight loss occurs in the first four to eight weeks, with diminishing returns as tolerance develops.
A meta-analysis of phentermine studies found that the average weight loss attributable to the drug (beyond placebo) was approximately 3.6 kg (about 8 pounds) over the study periods. When combined with topiramate in the formulation Qsymia, results improve to 7-11% body weight loss over one year, but this requires the addition of a second medication with its own side effect profile.
The bigger concern is what happens after stopping. Approximately 40% of people who discontinue phentermine regain the weight they lost. Weight regain typically begins around eight weeks after stopping and continues for about 20 weeks before plateauing.
Semaglutide weight loss data
Semaglutide (Wegovy) at the 2.4mg weekly dose produces an average of 14.9% total body weight loss over 68 weeks, according to the landmark STEP 1 trial. For a 200-pound person, that is roughly 30 pounds. And unlike phentermine, the weight loss trajectory continues improving throughout the treatment period rather than plateauing after a few weeks.
The STEP 5 trial, which extended follow-up to two years, showed that participants maintained an average weight loss of 15.2%. This long-term sustained loss is something phentermine simply cannot achieve because of its short-term use limitation and tolerance development. If you have been wondering how long to stay on semaglutide, the evidence supports ongoing use for as long as clinically appropriate.
Tirzepatide weight loss data
Tirzepatide raises the bar even higher. The SURMOUNT-1 trial demonstrated:
5mg dose: 15% body weight loss at 72 weeks
10mg dose: 19.5% body weight loss at 72 weeks
15mg dose: 22.5% body weight loss at 72 weeks
For a 230-pound person on the highest dose, that is losing approximately 52 pounds. Over a third of participants on the 15mg dose lost more than 25% of their body weight. These are results that no tirzepatide dosing protocol with phentermine could come close to matching.
The comparison table
Factor | Phentermine | Semaglutide (Wegovy) | Tirzepatide (Zepbound) |
|---|---|---|---|
Average weight loss | 5-10% body weight | 15% body weight | 15-22.5% body weight |
Treatment duration | 12 weeks (max 6 months) | Long-term/ongoing | Long-term/ongoing |
Time to peak results | 4-8 weeks | 40-68 weeks | 40-72 weeks |
Administration | Daily oral tablet | Weekly injection | Weekly injection |
Drug class | Sympathomimetic amine | GLP-1 receptor agonist | Dual GLP-1/GIP agonist |
Controlled substance | Yes (Schedule IV) | No | No |
Cardiovascular benefit | No (may increase risk) | Yes (FDA approved) | Under study |
Weight regain after stopping | ~40% regain all weight | Significant regain if stopped | Significant regain if stopped |
Side effects: stimulant versus peptide
The side effect profiles of these two drug classes reflect their fundamentally different mechanisms. Phentermine side effects come from stimulant activity. GLP-1 side effects come from hormonal and digestive changes. Understanding which set of side effects you are more likely to tolerate can help inform your decision.
Phentermine side effects
Because phentermine activates your sympathetic nervous system, its side effects read like a list of fight-or-flight symptoms:
Increased heart rate and blood pressure affect many users and can be dangerous for those with pre-existing cardiovascular conditions
Insomnia is one of the most commonly reported issues, since the stimulant effect does not stop when you want to sleep
Dry mouth occurs frequently due to reduced salivary gland activity
Restlessness and anxiety come from the same norepinephrine surge that suppresses appetite
Headaches are common in the first one to two weeks as your body adjusts
Constipation or diarrhea can occur as secondary effects
More serious but less common risks include pulmonary hypertension, valvular heart disease, and psychosis. The dependency risk is real. Phentermine is chemically related to amphetamine, and withdrawal symptoms can include depression, fatigue, disturbed sleep, and rebound appetite increases when you stop taking it.
GLP-1 medication side effects
GLP-1 side effects are primarily gastrointestinal, which makes sense given that these drugs work through gut hormone pathways:
Nausea is the most common side effect, affecting 40-50% of users at some point. It is usually worst during the first four to eight weeks and improves as your body adjusts. The slow dose titration schedule exists specifically to minimize this
Vomiting and diarrhea can accompany the nausea period but typically resolve
Constipation affects some users due to slowed gastric motility
Fatigue can occur, especially in the early weeks. Semaglutide fatigue is well-documented and usually temporary
Injection site reactions are mild and uncommon with proper injection technique
GLP-1 medications are not stimulants. They do not cause insomnia, jitteriness, increased heart rate, or the anxious energy that phentermine produces. In fact, semaglutide has demonstrated cardiovascular protective effects, the exact opposite of phentermine's cardiovascular strain.
However, GLP-1 medications carry their own serious (though rare) risks. Pancreatitis has been reported in clinical trials, though the absolute risk is low. Thyroid C-cell tumors were observed in rodent studies (not confirmed in humans), which is why these medications carry a boxed warning about medullary thyroid carcinoma. GLP-1 related hair loss has also been reported by some users, though this is more likely related to rapid weight loss than to the medication itself.
Tolerability comparison
Here is the practical difference. Most people who start phentermine tolerate it well initially but find side effects increasingly problematic over time as the stimulant effects accumulate. Most people who start GLP-1 medications experience their worst side effects in the first month and then find them steadily improving. The trajectories move in opposite directions.
If you are someone who is sensitive to stimulants, gets anxious easily, has trouble sleeping, or has any cardiovascular concerns, phentermine's side effect profile is the one to worry about. If you are someone with a sensitive stomach, a history of nausea with medications, or gastrointestinal conditions, GLP-1 side effects may be more challenging for you. But the GLP-1 side effects generally improve with time, while phentermine's do not.
Duration of use: weeks versus years
This is one of the most important practical differences between phentermine and GLP-1 medications, and it directly impacts long-term outcomes.
Phentermine: a 12-week window
The FDA approved phentermine specifically for short-term use. Most prescriptions last 12 weeks. Some physicians extend this to 24 weeks or even longer in certain cases, but the original approval and most clinical guidelines recommend against prolonged use.
Why the limitation? Three reasons.
First, tolerance. As mentioned earlier, your brain adapts to the elevated norepinephrine levels, and the appetite-suppressing effect diminishes. By week eight to twelve, many users report that the medication feels noticeably weaker.
Second, dependency risk. Because phentermine is structurally related to amphetamine and is classified as a Schedule IV controlled substance, longer use increases the potential for psychological and physical dependence. Withdrawal symptoms upon cessation are well-documented.
Third, cardiovascular strain. Sustained sympathetic nervous system activation puts additional stress on the heart and blood vessels. Short-term exposure is manageable for most healthy individuals, but cumulative effects over months or years could increase cardiovascular risk.
GLP-1 medications: designed for the long haul
GLP-1 receptor agonists were designed from the ground up for long-term use. Semaglutide and tirzepatide have been studied in trials lasting one to two years, with ongoing extension studies tracking outcomes even further. There is no tolerance development in the way phentermine experiences it, no dependency risk, and no classification as a controlled substance.
This long-term design matters because obesity is increasingly understood as a chronic condition. Just as you would not take blood pressure medication for 12 weeks and then stop, the rationale behind GLP-1 medications is that sustained treatment produces sustained results. The STEP 4 trial demonstrated this directly: when semaglutide was withdrawn after 20 weeks, participants regained approximately two-thirds of their lost weight over the following 48 weeks.
The message is clear. For lasting weight management, the medication needs to stay in the picture. And only GLP-1 medications are designed to allow that safely.
The complete list of GLP-1 medications available
Since phentermine is not a GLP-1, it helps to know exactly what is in the GLP-1 class. The category has expanded significantly, and new options continue to emerge.
Pure GLP-1 receptor agonists
These medications activate only the GLP-1 receptor:
Semaglutide (Ozempic/Wegovy/Rybelsus) is the most well-known. Ozempic is the diabetes formulation, Rybelsus is the oral version, and Wegovy is the weight management formulation at a higher dose. All contain the same active ingredient
Liraglutide (Victoza/Saxenda) was the first GLP-1 approved specifically for weight loss (as Saxenda). It requires daily injections rather than weekly, which makes it less convenient than semaglutide
Dulaglutide (Trulicity) is approved for diabetes but shows weight loss benefits. It is given weekly
Exenatide (Byetta/Bydureon) was the first GLP-1 receptor agonist approved by the FDA in 2005. The original formulation required twice-daily injections, though an extended-release version is available
Lixisenatide (Adlyxin) is a daily GLP-1 agonist primarily used for diabetes management
Dual and multi-agonists
These medications build on the GLP-1 framework by adding additional receptor targets:
Tirzepatide (Mounjaro/Zepbound) activates both GLP-1 and GIP receptors. Mounjaro is the diabetes brand, Zepbound is the weight management brand. It currently produces the most weight loss of any approved medication
Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. Still in clinical trials, it has shown even greater weight loss than tirzepatide in early data
Mazdutide is another dual GLP-1/glucagon agonist in development, primarily being studied in Asian populations
Cagrilintide is an amylin analog being studied in combination with semaglutide (CagriSema) that may produce weight loss exceeding tirzepatide
None of these medications share any mechanism with phentermine. Every single one works through gut hormone signaling pathways. SeekPeptides tracks the development of these medications closely, and the pipeline continues to expand with new dual and triple agonists entering clinical trials regularly.
Can you take phentermine and GLP-1 medications together?
This is one of the most commonly asked questions, and the answer is more nuanced than a simple yes or no.
What the data says
There is no direct pharmacological interaction between phentermine and GLP-1 receptor agonists. They work through completely different mechanisms and do not compete for the same receptors or metabolic pathways. From a pure drug-interaction standpoint, combining them is technically possible.
Some physicians do prescribe both medications simultaneously, particularly in cases where a patient has significant weight to lose and GLP-1 medications alone have not produced sufficient results. The theoretical rationale is that attacking appetite through two distinct pathways, stimulant-based and hormonal, might produce additive weight loss.
The important caveats
However, this combination has not been studied in randomized controlled trials. No major study has evaluated the safety and efficacy of taking phentermine and semaglutide or tirzepatide together. Everything we know comes from physician experience and small observational datasets.
The phentermine drug label actually recommends against combining it with other weight loss medications. While this warning was written before GLP-1 medications existed in their current form, it reflects a general caution about polypharmacy in weight management.
Potential risks of combination therapy include amplified gastrointestinal side effects (since both drugs can cause nausea and digestive changes), increased cardiovascular strain from phentermine combined with the fluid shifts that GLP-1 medications can cause, and the challenge of sorting out which medication is causing any side effects that develop.
An interesting research finding
One notable finding from recent observational data suggests that phentermine may actually be useful after discontinuing GLP-1 medications. Patients who had modest responses to GLP-1 therapy (losing less than 20 pounds) showed additional weight loss when switched to phentermine. This suggests the two drug classes might work better in sequence rather than simultaneously for some patients.
If you are considering combining these medications, this is absolutely a conversation to have with a physician who understands both drug classes. The potential benefits need to be weighed against the unknowns, and monitoring becomes essential.
Cost comparison: what you will actually pay
The financial difference between phentermine and GLP-1 medications is enormous, and for many people, this is the deciding factor.
Phentermine costs
Phentermine is generic and has been for decades. Without insurance, a month's supply typically costs $15 to $75 at most pharmacies. With insurance or discount programs, it can be as low as $4 to $10 per month. It is one of the cheapest prescription medications available for any condition.
Even Qsymia (the phentermine/topiramate combination) is relatively affordable compared to GLP-1 options, typically running $100 to $200 per month without insurance.
GLP-1 medication costs
Brand-name GLP-1 medications are expensive. Wegovy and Zepbound carry list prices exceeding $1,000 per month without insurance. Even with insurance, copays can range from $25 to $500+ depending on your plan and coverage tier.
Compounded semaglutide offers a more affordable alternative. Compounding pharmacies can produce semaglutide at significantly lower costs, though the regulatory landscape for compounded GLP-1 medications continues to evolve. Affordable tirzepatide options also exist through compounding, though again with caveats about regulation and quality control.
For researchers who want to understand exact dosing regardless of the cost pathway, tools like the semaglutide dosage calculator help ensure accurate administration whatever the source.
The cost-per-result calculation
Here is where the comparison gets interesting. Phentermine costs less per month but produces less weight loss over a shorter period. GLP-1 medications cost more per month but produce significantly more weight loss sustained over a longer period.
If you factor in cost per pound lost and cost per month of sustained weight maintenance, the gap narrows considerably. A 12-week course of phentermine at $50/month ($150 total) that produces 15 pounds of loss, 40% of which comes back, gives you a net sustained loss of about 9 pounds for $150. That is roughly $17 per pound of sustained weight loss.
A year of semaglutide at even $300/month (compounded pricing) that produces 30 pounds of sustained loss costs $3,600 total, or about $120 per pound of sustained weight loss. More expensive in absolute terms, but the amount of weight lost and the duration of maintenance are dramatically different.
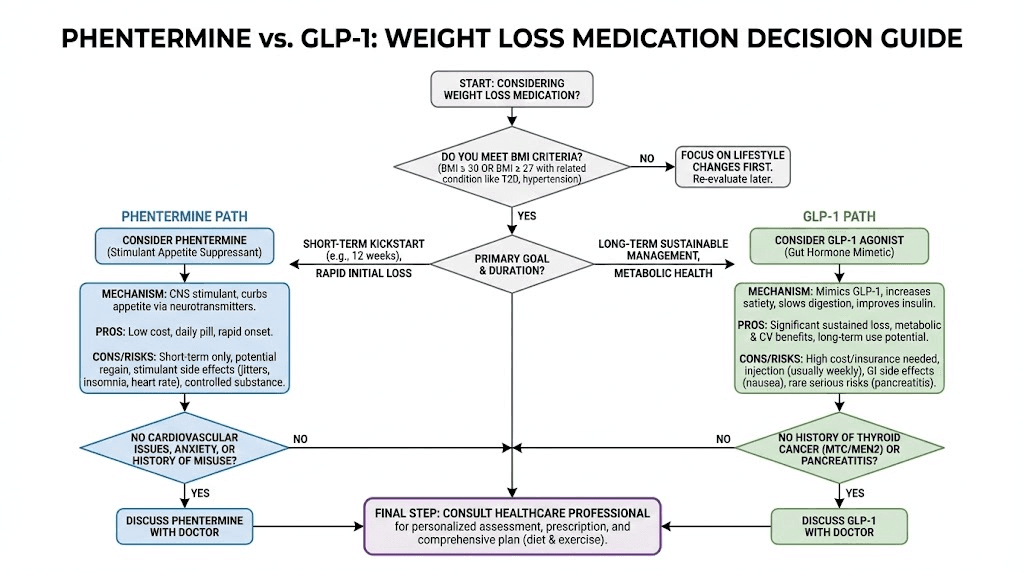
Who should consider phentermine instead of GLP-1 medications
Despite the weight loss advantage of GLP-1 medications, phentermine still has legitimate uses. It is not the right choice for everyone, but neither is it obsolete.
Phentermine may be appropriate when:
You need a short-term jumpstart. If you have 10-20 pounds to lose and need rapid appetite suppression to establish new eating habits, a 12-week course of phentermine combined with diet changes and exercise can be effective
Cost is the primary barrier. If GLP-1 medications are financially out of reach and insurance does not cover them, phentermine at $15-50/month provides a real, evidence-based option
You cannot tolerate GLP-1 side effects. Some people experience severe, persistent nausea or gastrointestinal symptoms on GLP-1 medications that do not resolve with time or dose adjustments
You need immediate results. Phentermine starts working within 24-48 hours, while GLP-1 medications take weeks to months to reach full therapeutic effect. If motivation from early results is important for adherence, the rapid onset matters
You are already close to your goal weight. The moderate weight loss phentermine produces may be sufficient for someone who needs to lose a smaller amount rather than undergo the commitment of long-term GLP-1 therapy
Phentermine is not appropriate when:
You have cardiovascular disease, uncontrolled hypertension, or a history of heart problems
You have a history of substance abuse or addiction
You are looking for long-term weight management (beyond 3-6 months)
You have type 2 diabetes (GLP-1 medications provide metabolic benefits phentermine cannot)
You have significant weight to lose (50+ pounds) where sustained therapy is essential
Who should consider GLP-1 medications instead of phentermine
For the majority of people with significant weight to lose, GLP-1 medications represent the more effective and more sustainable option. The clinical evidence is overwhelming.
GLP-1 medications are better suited when:
You have substantial weight to lose. If your target is 30, 50, or 100+ pounds, the magnitude of weight loss GLP-1 medications can produce is simply not achievable with phentermine
You need long-term management. Obesity is a chronic condition for many people. A medication you can safely take for years is fundamentally different from one limited to 12 weeks
You have type 2 diabetes or prediabetes. GLP-1 medications were literally designed for this population. They provide blood sugar control alongside weight loss
Cardiovascular health matters. If you have elevated cardiovascular risk, semaglutide's proven heart-protective effects give it an advantage that phentermine's stimulant properties cannot match
You want to address root metabolic issues. GLP-1 medications improve insulin sensitivity, regulate gut hormones, and may even reduce systemic inflammation. They address the metabolic drivers of weight gain, not just the symptom of hunger
Previous attempts with stimulant-based approaches have failed. If you have tried phentermine or similar medications and experienced tolerance, rebound weight gain, or dependency concerns, GLP-1 medications offer a completely different approach
Understanding your specific dosing requirements and whether oral formulations or injections work better for your lifestyle helps narrow the options within the GLP-1 class itself.
The pharmacological classification breakdown
For those who want the technical details, here is exactly where each medication sits in the pharmacological classification system. This makes it crystal clear that phentermine and GLP-1 medications are entirely separate entities.
Phentermine classification
Drug class: Sympathomimetic amine / anorectic agent
Mechanism: Releases norepinephrine and dopamine centrally
DEA Schedule: Schedule IV controlled substance
Chemical relation: Structural analog of amphetamine (alpha-methylphenethylamine)
FDA approval: 1959 (one of the oldest approved weight loss drugs)
Brand names: Adipex-P, Lomaira
Combination product: Qsymia (phentermine + topiramate)
Route: Oral (tablet or capsule)
Duration: Short-term use only (12 weeks recommended, 24 weeks maximum for most patients)
GLP-1 receptor agonist classification
Drug class: Incretin mimetics / GLP-1 receptor agonists
Mechanism: Activates GLP-1 receptors peripherally and centrally
DEA Schedule: Not a controlled substance
Chemical relation: Modified peptide hormone sequences (no relation to amphetamines)
FDA approval: Exenatide in 2005 (first in class), semaglutide for weight loss in 2021
Brand names: Ozempic, Wegovy, Rybelsus, Mounjaro, Zepbound, Saxenda, Trulicity, and others
Route: Injection (subcutaneous, weekly for most) or oral formulations
Duration: Designed for long-term use (ongoing as clinically appropriate)
The two classes do not share a single pharmacological feature. Different chemical structure. Different mechanism. Different receptor targets. Different regulatory classification. Different treatment duration. The only thing they share is the endpoint of reduced appetite and weight loss, achieved through completely unrelated pathways.
Why the confusion exists in the first place
Understanding why people confuse phentermine with GLP-1 medications helps explain the broader landscape of weight loss pharmacology and where misconceptions come from.
The weight loss medication explosion
Before semaglutide became a household name, the weight loss medication landscape was dominated by a handful of drugs: phentermine, orlistat (Alli/Xenical), and a few others. Phentermine was the most prescribed weight loss medication in the United States for decades. When GLP-1 medications suddenly dominated headlines and conversations, many people assumed they were related to or replacements for phentermine.
The media did not help. News articles frequently compare phentermine and GLP-1 medications without clearly explaining that they are fundamentally different drug classes. Headlines like "Ozempic vs. Phentermine" create the impression that these are competing versions of the same thing rather than completely different approaches to the same problem.
The physician factor
Adding to the confusion, many physicians prescribe both phentermine and GLP-1 medications for weight loss. Patients sometimes transition from one to the other, or even take both simultaneously. When the same doctor prescribes both drugs for the same condition, it is natural to assume they are similar.
Weight loss clinics frequently offer both options, presenting them as alternatives on a menu. This side-by-side presentation reinforces the misconception that they belong to the same category, when in reality they are as different as antibiotics and pain relievers, two completely separate tools that happen to be used in overlapping situations.
The brand name labyrinth
The proliferation of brand names does not help either. Semaglutide alone has three brand names (Ozempic, Wegovy, Rybelsus). Tirzepatide has two (Mounjaro, Zepbound). When people are trying to keep track of which medication does what, adding phentermine (Adipex, Lomaira) and Qsymia into the mix creates a confusing landscape where category boundaries blur.
SeekPeptides exists in part to clear up exactly this kind of confusion. Understanding what each medication actually is, how it works, and where it fits in the treatment landscape is essential for making informed decisions about your health.
Phentermine and GLP-1 together: the emerging combination approach
While phentermine is not a GLP-1, the two are increasingly being discussed in combination contexts. This section covers what we know and what we do not.
The theoretical rationale
Combining phentermine (which suppresses appetite through CNS stimulation) with a GLP-1 medication (which suppresses appetite through gut hormone signaling) could theoretically produce additive weight loss. You are attacking the same problem from two completely different angles. Each mechanism covers gaps the other misses.
Phentermine's immediate appetite suppression could help bridge the gap during the weeks when GLP-1 medications are still being titrated to therapeutic doses. Semaglutide takes time to suppress appetite fully, and the slow titration schedule means patients may not feel the full effect for 16 to 20 weeks. Phentermine could provide appetite control during this ramp-up period.
What observational data shows
Small observational studies and clinical experience reports suggest that the combination can be effective for patients who respond partially to either medication alone. Some weight loss clinics report that patients on combination therapy lose more weight than on either medication individually.
One notable finding from Epic Research showed that patients who lost less than 20 pounds on GLP-1 therapy went on to lose additional weight when switched to phentermine. This suggests that the two approaches may work better in sequence for non-responders rather than simultaneously.
The risks and unknowns
The honest answer is that we do not know enough. No randomized controlled trial has evaluated this specific combination. The potential concerns include:
Additive cardiovascular effects (phentermine's stimulant properties combined with GLP-1's effects on heart rate)
Compounded gastrointestinal side effects
The challenge of managing two separate dose titrations simultaneously
Unknown long-term safety of the combination
If you are exploring combination approaches, this is strictly territory for physician supervision. Do not combine these medications without medical guidance.
Common misconceptions about both drug classes
Beyond the basic confusion about whether phentermine is a GLP-1, several other misconceptions circulate that are worth addressing directly.
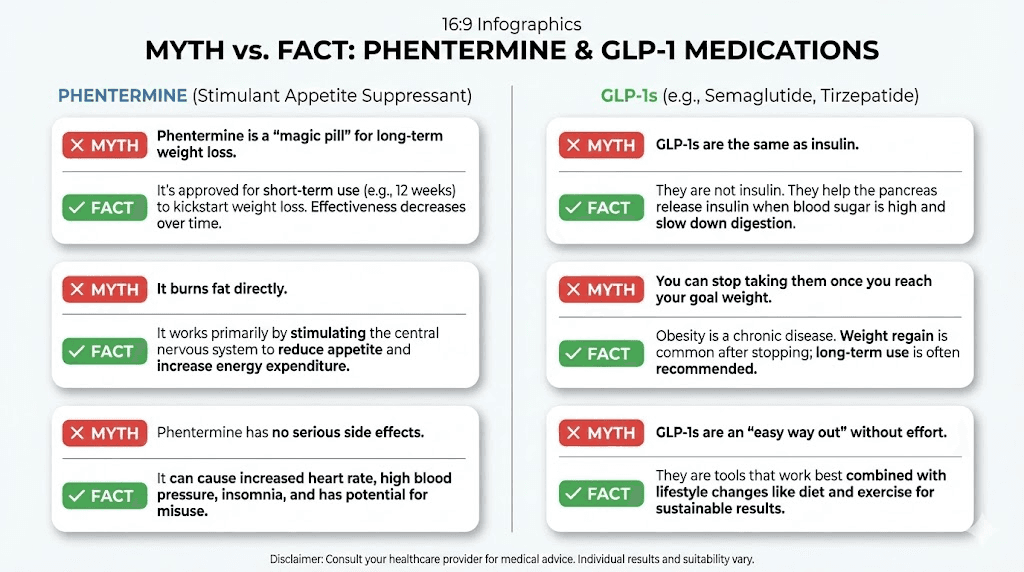
Misconception 1: phentermine is dangerous because it is related to amphetamine
While phentermine is structurally similar to amphetamine, it is significantly less potent and has a much lower abuse potential. This is why it is classified as Schedule IV (lower risk) rather than Schedule II (where amphetamines sit). Tens of millions of prescriptions have been written since 1959. At appropriate doses for appropriate durations, phentermine has a well-established safety profile. The risks are real but manageable with proper medical supervision.
Misconception 2: GLP-1 medications are just for diabetes
GLP-1 receptor agonists were originally developed for type 2 diabetes, and that is still a primary indication. But the weight loss benefits are not a side effect that was discovered accidentally and repurposed. Semaglutide (as Wegovy) and tirzepatide (as Zepbound) have dedicated FDA approvals specifically for chronic weight management in adults, independent of diabetes status. The cardiovascular protection approval further expands the medical use case beyond both diabetes and weight loss.
Misconception 3: you will regain all weight when you stop either medication
Weight regain after stopping is a concern for both drug classes, but the picture is more nuanced than the doom-and-gloom headlines suggest. With phentermine, approximately 40% of users regain all lost weight, but 42% maintain all the weight they lost, and 25% maintain at least 10% body weight loss. The key factors are lifestyle changes made during treatment.
With GLP-1 medications, the STEP 4 trial showed significant regain after stopping semaglutide, but patients who maintained dietary changes and exercise habits fared better than those who did not. The medication creates a window of opportunity for building sustainable habits, not a permanent crutch. Though for many people, ongoing treatment remains the most effective approach.
Misconception 4: the more expensive medication is always better
Not necessarily. If you need to lose 15 pounds and can commit to 12 weeks of strict dietary adherence with the help of appetite suppression, phentermine at $30/month may accomplish your goal perfectly well. Spending $300+/month on a GLP-1 medication for a modest weight loss target may not represent the best value for your situation.
The reverse is also true. Choosing phentermine because it is cheaper when you need to lose 80 pounds and manage type 2 diabetes is a false economy. The right medication depends on your specific clinical situation, not the price tag alone.
Misconception 5: natural alternatives are equivalent to either drug class
No supplement, herb, tea, or "natural GLP-1 booster" produces effects comparable to prescription phentermine or prescription GLP-1 receptor agonists. The magnitude of appetite suppression and metabolic change these medications produce is pharmacological, meaning it requires therapeutic drug concentrations that food-based compounds simply cannot achieve.
There are natural ways to modestly increase GLP-1 production, including high-protein meals, fiber intake, and certain fermented foods. But these produce GLP-1 levels measured in the low picomolar range, while medications like semaglutide create sustained nanomolar-range receptor activation. The difference is roughly 1,000-fold.
Understanding what matters for your decision
The question "is phentermine a GLP-1?" usually reflects a deeper question: which medication is right for me? Answering that requires honest assessment of several factors.
Your weight loss goals
Be specific. "I want to lose weight" is not specific enough. How much weight? What is your timeline? Is this about health metrics (blood sugar, blood pressure, cardiovascular risk) or primarily aesthetic? The answers shape which medication class makes sense.
For modest goals (10-20 pounds) with a short timeline, phentermine remains a viable option. For substantial goals (30+ pounds) with long-term maintenance in mind, GLP-1 medications are the evidence-based choice. For goals that involve metabolic health improvement alongside weight loss, GLP-1 medications provide benefits phentermine fundamentally cannot.
Your medical history
Cardiovascular conditions, diabetes, anxiety disorders, sleep problems, substance use history, gastrointestinal conditions, thyroid disease, all of these factor into which medication class is safer and more appropriate for you.
Phentermine is contraindicated in patients with cardiovascular disease, hyperthyroidism, glaucoma, history of drug abuse, or concurrent use of MAO inhibitors. GLP-1 medications carry warnings about medullary thyroid carcinoma, pancreatitis history, and severe gastrointestinal disease.
Your tolerance for side effects
Stimulant side effects (insomnia, jitteriness, elevated heart rate) versus gastrointestinal side effects (nausea, digestive changes). Most people tolerate one category better than the other. Your personal history with medications can help predict which side effect profile you are more likely to manage successfully.
Your financial situation
This is a practical reality. Affordable GLP-1 options exist through compounding pharmacies and patient assistance programs, but they still cost significantly more than generic phentermine. If budget is a serious constraint, phentermine may be the only pharmacological option available, and some weight loss is better than no weight loss.
Your timeline and commitment
Phentermine requires a short-term commitment (12 weeks) but demands that you build sustainable habits during that window because the medication support ends. GLP-1 medications allow for a longer-term commitment with ongoing support but require sustained treatment for sustained results.
Neither approach works without effort. Both medications are tools that create favorable conditions for weight loss. The actual weight loss still requires dietary changes, activity changes, and behavioral adjustments. The medication just makes those changes dramatically easier to implement and maintain.
How reconstitution and administration differ
For researchers and individuals who work with compounded formulations, understanding the practical differences in administration between these drug classes is important.
Phentermine administration
Phentermine is simple. It comes as an oral tablet or capsule. You take it once daily, typically in the morning before breakfast or one to two hours after breakfast. Some formulations (like Lomaira) are taken three times daily before meals. There is no mixing, no reconstitution, no injection required.
The daily oral administration is both an advantage (convenience, no injection anxiety) and a disadvantage (daily adherence required, easy to miss doses, once-daily dosing means drug levels fluctuate throughout the day).
GLP-1 medication administration
Most GLP-1 medications require subcutaneous injection, typically once weekly. For branded products like Wegovy and Zepbound, this involves a pre-filled autoinjector pen that requires minimal technique. Choose an injection site, press the pen against your skin, click a button, and wait for the injection to complete.
For compounded GLP-1 formulations, the process involves more steps. You may need to reconstitute semaglutide or reconstitute tirzepatide from lyophilized powder, which requires bacteriostatic water in specific amounts, proper sterile technique, and accurate dose calculations. Tools like the peptide reconstitution calculator make the math straightforward, but the process requires attention to detail.
Understanding proper storage is also critical for compounded formulations. Semaglutide storage requirements and tirzepatide refrigeration guidelines differ from phentermine (which simply sits in your medicine cabinet at room temperature).
Oral GLP-1 options are expanding. Oral semaglutide drops and tirzepatide sublingual drops offer non-injection routes, though absorption and bioavailability differ from injectable forms. The oral versus injection comparison for tirzepatide is worth examining if injection anxiety is a barrier.
The role of diet and lifestyle with each medication
Both phentermine and GLP-1 medications work best when combined with dietary and lifestyle changes. But the specific nutritional considerations differ between the two drug classes.
Eating on phentermine
Because phentermine's primary effect is appetite suppression through stimulant mechanisms, the main dietary advice is straightforward: use the reduced appetite to establish a caloric deficit and build healthier eating patterns that can persist after the medication ends. The challenge is that phentermine does not change what foods appeal to you, it just makes you less interested in eating overall. Without deliberate nutritional planning, people on phentermine may eat less but not necessarily eat better.
The stimulant effect also tends to suppress thirst along with hunger, making dehydration a real concern. Adequate water intake becomes especially important.
Eating on GLP-1 medications
GLP-1 medications change the eating experience more fundamentally. Slowed gastric emptying means food sits in your stomach longer, which has practical implications. Large meals become uncomfortable. High-fat meals become especially problematic because fat takes the longest to digest, and adding a GLP-1's gastric slowing on top of that can cause significant discomfort.
This is why specific dietary adjustments for tirzepatide and semaglutide meal planning exist as dedicated topics. The medication actually changes your relationship with food at a physiological level, not just the amount you want to eat but how your body processes what you do eat.
Protein intake becomes especially important on GLP-1 medications because the significant caloric reduction can lead to muscle loss alongside fat loss. Researchers working with tirzepatide diet protocols typically prioritize protein at 1.0 to 1.2 grams per kilogram of body weight daily to preserve lean mass.
Users also need to monitor their intake of specific nutrients. B12 supplementation with semaglutide and B12 with tirzepatide has become standard practice because reduced food intake can lead to micronutrient deficiencies over time. Glycine supplementation and tirzepatide with glycine formulations address related nutritional concerns in compounded preparations.
Looking at the future of both drug classes
The trajectories of phentermine and GLP-1 medications point in very different directions. Understanding where each is headed helps frame your decision with a longer-term perspective.
Phentermine's future
Phentermine is unlikely to see significant innovation. It is a 60+ year old generic medication with a well-understood mechanism and established limitations. Research continues on combination products (like Qsymia), and phentermine may find a secondary role as a bridge medication during GLP-1 titration or as an alternative for GLP-1 non-responders. But it is not going to become more effective, safer for long-term use, or fundamentally different from what it is today.
GLP-1 and beyond
The GLP-1 space is exploding with innovation. Retatrutide (the triple agonist) showed 24.2% body weight loss in Phase 2 trials, potentially exceeding tirzepatide. Oral formulations of both semaglutide and tirzepatide are advancing, with high-dose oral semaglutide (Rybelsus successor) showing weight loss comparable to injectable formulations. GLP-1 patches are in development that could eliminate injections entirely.
CagriSema (cagrilintide + semaglutide) combines an amylin analog with a GLP-1 agonist for yet another dual-mechanism approach. Early data suggests it may produce weight loss exceeding tirzepatide.
The pipeline is deep and the direction is clear: incretin-based therapies are where weight loss pharmacology is headed. Phentermine is not part of this future. It remains a useful legacy tool for specific situations, but the innovation is happening entirely in the GLP-1 and multi-agonist space.
For researchers serious about understanding and optimizing these newer approaches, SeekPeptides provides comprehensive protocol guides, dosing calculators, and evidence-based resources that evolve as quickly as the science does.
Frequently asked questions
Is phentermine the same thing as a GLP-1?
No. Phentermine is a sympathomimetic amine (stimulant-based appetite suppressant) that works by releasing norepinephrine in the brain. GLP-1 receptor agonists are peptide-based medications that mimic the gut hormone GLP-1 to regulate appetite, digestion, and blood sugar. They share no mechanism, no chemical structure, and no pharmacological classification.
Which one produces more weight loss?
GLP-1 medications produce significantly more weight loss on average. Semaglutide produces approximately 15% body weight loss over 68 weeks, while tirzepatide produces up to 22.5% at the highest dose over 72 weeks. Phentermine typically produces 5-10% body weight loss over 12-24 weeks.
Can I switch from phentermine to a GLP-1?
Yes, many patients transition from phentermine to GLP-1 medications. There is no pharmacological contraindication to switching. Your physician will typically discontinue phentermine before starting the GLP-1 titration schedule, though some may overlap the two during the transition period. The switching process varies depending on the specific medications involved.
Why is phentermine a controlled substance but GLP-1 medications are not?
Phentermine is classified as Schedule IV because of its structural similarity to amphetamine and its potential for physical and psychological dependence. GLP-1 medications have no stimulant properties, no abuse potential, and no relation to amphetamines. They carry no controlled substance classification.
Do both medications cause weight regain when stopped?
Both can lead to weight regain after discontinuation, but for different reasons. Phentermine rebound is driven by the return of pre-treatment appetite levels once the stimulant effect ends. GLP-1 rebound occurs because the hormonal appetite regulation returns to baseline. In both cases, lifestyle changes made during treatment help mitigate weight regain. The key difference is that GLP-1 medications are designed for long-term use, making continued treatment a viable option for maintaining results.
Is phentermine safer than GLP-1 medications?
Neither is categorically safer. Phentermine carries cardiovascular risks (increased heart rate, blood pressure, potential cardiac effects) and dependency potential. GLP-1 medications carry gastrointestinal risks and rare but serious concerns about pancreatitis and thyroid effects. The relative safety depends entirely on your individual health profile. A person with heart disease would find GLP-1 medications safer. A person with a history of pancreatitis might find phentermine safer.
Can I take phentermine and semaglutide together?
Technically possible, and some physicians do prescribe them together, but this combination has not been studied in clinical trials. The phentermine label recommends against combining with other weight loss medications. If your physician recommends this combination, it should be with careful monitoring and clear justification.
Does insurance cover both equally?
No. Phentermine is a generic medication and is almost universally covered by insurance at very low copays ($4-15/month). GLP-1 medications for weight loss have variable coverage, and many insurance plans exclude them or place them on high-cost specialty tiers. Affordable alternatives through compounding pharmacies and manufacturer programs exist but require more effort to access.
External resources
For researchers committed to understanding the full landscape of weight management peptides and medications, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, community support, and tools that evolve as rapidly as the science itself.
In case I do not see you, good afternoon, good evening, and good night. May your medications stay effective, your choices stay informed, and your progress stay consistent.