Feb 8, 2026

Before you dismiss that extra hair in your brush as stress, take a closer look. If you started a GLP-1 medication in the last few months, those loose strands might be telling you something important. Something your prescriber may not have mentioned.
Hair loss during GLP-1 therapy is real. It is measurable. And it is far more common than most people realize.
The FDA Adverse Event Reporting System now shows a reporting odds ratio of 2.46 for alopecia with semaglutide, meaning hair loss reports are nearly two and a half times higher than expected. Clinical trials for tirzepatide found that roughly 5% of participants experienced noticeable hair shedding, compared to less than 1% on placebo. These are not small numbers. They represent thousands of people watching their hair thin while pursuing a healthier weight, caught between the undeniable benefits of weight loss therapy and an unexpected cosmetic consequence that nobody prepared them for. The good news is that GLP-1 related hair loss is almost always temporary, driven by well-understood biological mechanisms, and highly responsive to prevention strategies when you know what to do. This guide covers every dimension of the issue, from the clinical data and biological pathways behind GLP-1 hair shedding to the peptide-based treatments and nutritional protocols that can protect your hair while you continue your weight loss journey. SeekPeptides has compiled the most comprehensive breakdown available, drawing from pharmacovigilance databases, randomized controlled trials, and systematic reviews so you can make informed decisions about your health without sacrificing your hair in the process.
What the research actually says about GLP-1 and hair loss
The conversation around GLP-1 medications and hair loss has shifted dramatically over the past few years. Early clinical trials barely mentioned it. Now, with millions of people taking semaglutide and tirzepatide worldwide, the signal has become impossible to ignore. But what does the data actually show? Not anecdotes. Not forum posts. The hard numbers from controlled studies and pharmacovigilance databases.
FDA adverse event reporting system analysis
The most comprehensive look at GLP-1 hair loss comes from analysis of the FDA Adverse Event Reporting System, known as FAERS. Researchers examined reports submitted between the first quarter of 2022 and the third quarter of 2023, a period when GLP-1 prescriptions surged. The results were striking.
Semaglutide showed a reporting odds ratio (ROR) of 2.46 for alopecia. That means hair loss was reported 2.46 times more frequently than the baseline expectation across all medications in the database. Tirzepatide came in at 1.73, still elevated but noticeably lower than semaglutide. Here is what caught researchers off guard: liraglutide, dulaglutide, and exenatide showed no statistically significant increase in hair loss reports at all. This distinction matters because it suggests that the hair loss phenomenon is not universal across all GLP-1 receptor agonists. Something about the newer, more potent formulations, or perhaps the degree of weight loss they produce, drives the risk higher.
Clinical trial evidence from SURMOUNT-1
The landmark SURMOUNT-1 trial, published by Jastreboff and colleagues, provided some of the cleanest data on tirzepatide and hair loss. This was a randomized, double-blind, placebo-controlled trial. The gold standard. And the numbers were clear.
At the 5 mg dose of tirzepatide, 5.1% of participants (32 cases) experienced hair loss. The 10 mg group saw 5.3% (34 cases). The 15 mg group reported 4.9% (31 cases). Placebo? Just 0.9%, with only 6 cases. The consistency across dose groups is telling. Whether participants took 5 mg or 15 mg, roughly one in twenty experienced noticeable hair shedding. This suggests that the hair loss is not strictly dose-dependent in a linear way but rather connected to the metabolic changes that all therapeutic doses trigger, including significant weight loss with tirzepatide.
Systematic review across five major studies
A systematic review pooling data from 2,905 patients across five studies found that 1.6% of the total GLP-1 patient population of 626,894 experienced some form of hair loss. Only 0.008% reported subsequent hair regrowth during the study periods. The demographics tell an important story too. Women made up between 65.4% and 100% of affected cohorts, depending on the study. The mean age ranged from 44.9 to 57 years. The types of hair loss documented included telogen effluvium (the most common), androgenic alopecia, and alopecia areata. Each of these involves different mechanisms, different prognoses, and different treatment approaches, which is why understanding which type you are dealing with matters enormously for your safety and treatment planning.
One particularly notable case report described a 23-year-old female who developed alopecia areata, an autoimmune form of hair loss, just two months after starting semaglutide. She presented with a well-demarcated round patch of complete scalp hair loss, a pattern distinct from the diffuse thinning seen in telogen effluvium. This case raised questions about whether GLP-1 medications might trigger autoimmune responses in susceptible individuals, adding another layer of complexity to an already nuanced picture.
Understanding why GLP-1 medications cause hair to fall out
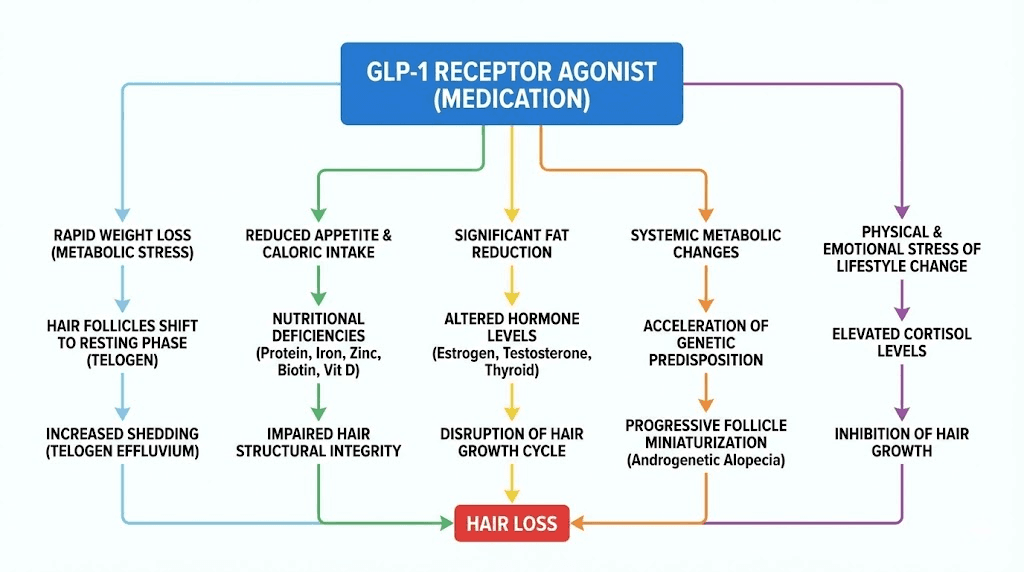
Hair does not just fall out randomly. Every strand follows a precise biological cycle, and anything that disrupts this cycle can push follicles from their growth phase into their resting phase prematurely. GLP-1 medications can trigger this disruption through at least five distinct mechanisms, sometimes acting alone, sometimes in combination. Understanding each one is critical because the right prevention strategy depends entirely on which mechanism is driving your specific hair loss.
Telogen effluvium from rapid metabolic shifts
The most common cause of GLP-1 related hair loss is telogen effluvium, a condition where a large percentage of hair follicles simultaneously shift from the anagen (growth) phase to the telogen (resting) phase. Normally, about 85-90% of your hair is in anagen at any given time, actively growing. Only 10-15% rests in telogen, waiting to shed and make room for new growth.
Rapid weight loss disrupts this balance. When the body senses significant caloric deficit, it reallocates resources away from non-essential functions. Hair growth, metabolically expensive as it is, gets deprioritized. The body essentially decides that maintaining existing hair follicles is less important than preserving organ function and basic metabolic processes. This is a survival mechanism. An ancient one. And your body does not care that you are losing weight intentionally with semaglutide or tirzepatide. It responds the same way it would to famine.
Nutritional deficiency pathways
GLP-1 medications suppress appetite dramatically. That is their primary therapeutic effect for weight management. But reduced food intake means reduced nutrient intake, and several nutrients are absolutely essential for hair follicle cycling. Iron deficiency is perhaps the most significant. Ferritin levels below 30 ng/mL have been consistently associated with increased hair shedding, and many patients on GLP-1 therapy drop below this threshold without realizing it. Zinc plays a critical role in keratin synthesis and cellular division within the hair follicle. Vitamin D receptors are expressed in hair follicles, and deficiency impairs the transition from telogen back to anagen. Biotin supports keratin infrastructure. And protein, the very building block of hair, often falls to inadequate levels when appetite suppression from medications like semaglutide reduces total caloric intake by 30-40%.
Thyroid hormone disruption
Weight loss alters thyroid function. This is well documented. Rapid reduction in body fat affects the conversion of T4 to T3, the active thyroid hormone. T3 directly regulates hair follicle cycling, and even subclinical thyroid dysfunction, levels that fall within the "normal" range but sit at the lower end, can push follicles into premature telogen. Patients on GLP-1 therapy who develop hair loss should always have their thyroid function assessed, including free T3 and free T4, not just TSH alone.
Hormonal changes triggering androgenic patterns
Fat tissue is not inert. It is an endocrine organ. It produces and metabolizes hormones, including estrogen and testosterone. When body fat decreases rapidly, the hormonal environment shifts. For some individuals, particularly women approaching or in perimenopause, this shift can unmask or worsen androgenic alopecia, a pattern of hair thinning driven by dihydrotestosterone (DHT) sensitivity in genetically predisposed follicles. This is different from telogen effluvium. Androgenic alopecia follows a pattern, thinning at the crown and temples in men, diffuse thinning across the top of the scalp in women, and it does not resolve on its own the way telogen effluvium does. Women navigating weight loss during hormonal transitions may benefit from understanding how peptides can support menopause alongside their GLP-1 therapy.
Direct receptor-mediated effects
This is where things get scientifically fascinating. GLP-1 receptors have been identified in murine hair follicles. Their exact function in human hair biology remains under investigation, but the presence of these receptors raises the possibility that GLP-1 medications might directly affect hair follicle cycling, independent of weight loss or nutritional status. Some research suggests that GLP-1 receptor activation in follicular cells may modulate the MAPK/ERK signaling pathway, which, paradoxically, is involved in promoting hair growth in certain contexts.
The direct effect of GLP-1 receptor agonists on human hair follicles remains one of the most intriguing unanswered questions in dermatological pharmacology.
The telogen effluvium connection
Telogen effluvium deserves its own deep dive because it accounts for the vast majority of hair loss seen with GLP-1 medications. Understanding it thoroughly changes everything about how you approach prevention and treatment.
How the hair cycle normally works
Each hair follicle on your scalp operates independently, cycling through three phases. Anagen is the active growth phase, lasting two to seven years. This is when the hair shaft is actively being produced by rapidly dividing cells in the follicle bulb. Catagen is a brief transitional phase of about two weeks, during which the follicle shrinks and detaches from the blood supply. Telogen is the resting phase, lasting about three months, after which the old hair falls out and a new anagen cycle begins.
At any given moment, roughly 85-90% of your approximately 100,000 scalp follicles are in anagen. You shed about 50-100 hairs per day as part of normal cycling. This is invisible because new growth immediately replaces what is lost.
What happens during telogen effluvium
A physiological stressor, and rapid weight loss absolutely qualifies, can cause a large percentage of follicles to simultaneously shift from anagen to telogen. Instead of 10-15% of follicles resting at once, 30% or more might enter telogen simultaneously. The catch is the three-month delay. The triggering event happens first. Then, three months later, all those follicles that prematurely entered telogen begin shedding their hair shafts at the same time.
This is why GLP-1 hair loss typically appears three to six months after starting therapy. Not immediately. People often fail to connect the two events because of this lag. They started tirzepatide six months ago and only now notice increased shedding, so they blame stress, seasonal changes, or aging instead of recognizing the medication-triggered pattern. The withdrawal process from semaglutide can also trigger its own round of telogen effluvium as the body readjusts to eating without pharmaceutical appetite suppression.
How to distinguish telogen effluvium from other types
Telogen effluvium produces diffuse thinning across the entire scalp. Not patches. Not a receding hairline. Just an overall reduction in volume and density. The hair pull test, where a clinician gently pulls on a cluster of about 60 hairs, will yield six or more hairs in active telogen effluvium, compared to one or two normally. The shed hairs will have a small white bulb at the root end, indicating they were in the telogen phase when they released. If you see broken hairs without bulbs, that points to a different problem entirely.
The distinction matters because the treatment approach differs completely. Telogen effluvium is self-limiting. Remove the trigger, and hair regrows. Androgenic alopecia requires ongoing treatment. Alopecia areata involves autoimmune management. Getting the diagnosis right saves you time, money, and unnecessary worry.
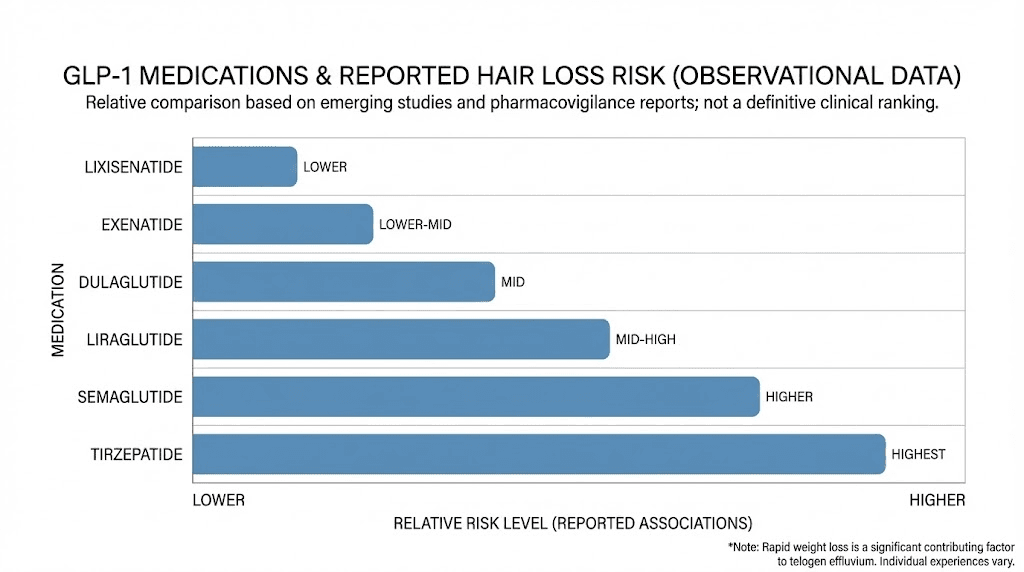
Which GLP-1 medications carry the highest risk
Not all GLP-1 medications are created equal when it comes to hair loss risk. The data reveal meaningful differences between compounds, and understanding these differences can inform conversations with your healthcare provider about medication selection if hair loss is a significant concern for you.
Semaglutide leads the risk profile
With a reporting odds ratio of 2.46 in the FAERS database, semaglutide carries the highest documented risk of alopecia among GLP-1 receptor agonists. This may partly reflect its popularity and widespread use, which increases the total number of adverse event reports. But even accounting for reporting bias, the signal is significant. Semaglutide also tends to produce more rapid and substantial weight loss than older GLP-1 medications, which aligns with the weight-loss-driven telogen effluvium hypothesis. Understanding proper semaglutide dosing in milligrams and starting with appropriate titration may help reduce the speed of weight loss and consequently the hair loss risk.
Tirzepatide occupies the middle ground
Tirzepatide, a dual GIP/GLP-1 receptor agonist, showed a reporting odds ratio of 1.73, elevated but lower than semaglutide. The SURMOUNT-1 trial data showed approximately 5% incidence across all dose levels. The tirzepatide dose chart shows a standard titration from 2.5 mg up to 15 mg, and interestingly, the hair loss rate did not increase meaningfully between the 5 mg and 15 mg groups. For people tracking their tirzepatide dosage in units or following a microdosing tirzepatide protocol, the data suggests that lower doses may not necessarily protect against hair loss if the total weight loss achieved is still substantial.
Older GLP-1 medications show minimal risk
Liraglutide, dulaglutide, and exenatide did not show statistically significant increases in hair loss reports. This is an important finding. These older medications produce less dramatic weight loss compared to semaglutide and tirzepatide, which supports the theory that the rate and magnitude of weight loss, rather than the GLP-1 receptor activation itself, drives most of the hair shedding. If hair preservation is a top priority and the primary goal is moderate weight management rather than substantial loss, these older compounds might warrant discussion with a prescriber.
Emerging compounds and their hair loss profiles
Newer medications in the GLP-1 family and related classes are entering the market. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown even more dramatic weight loss in clinical trials, with some participants losing over 25% of their body weight. Based on the weight-loss correlation data, one would expect hair loss rates to be at least comparable to or potentially higher than those seen with semaglutide and tirzepatide. Anyone researching retatrutide dosing or tracking the availability of retatrutide should factor hair loss risk into their consideration. Similarly, cagrilintide combined with semaglutide (CagriSema) represents another potent combination where the degree of weight loss may heighten hair shedding risk, making proper CagriSema dosing and nutritional support even more important.
How weight loss speed affects hair shedding severity
The single strongest predictor of hair loss during GLP-1 therapy is not which medication you take. It is how fast you lose weight.
The data is clear. Patients who lose more than 20% of their body weight experience alopecia at a rate of 5.3%. Those who lose less than 20% see rates of just 2.5%. That is more than double the risk for aggressive weight loss. This correlation holds across medication types, dosing regimens, and patient demographics. It is the weight loss speed itself that tips hair follicles into premature telogen.
Why rapid loss triggers more shedding
The body does not distinguish between intentional caloric restriction and starvation. When energy intake drops sharply and fat stores deplete rapidly, the hypothalamic-pituitary axis responds by downregulating processes deemed non-essential for survival. Hair production requires significant metabolic resources, including amino acids, minerals, vitamins, and energy. A gradual reduction in body weight allows the body to adapt. Systems adjust incrementally. Nutrient allocation shifts slowly enough that hair follicles can maintain their growth cycle.
Rapid loss overwhelms these adaptive mechanisms. The body enters a kind of metabolic emergency mode. Growth hormone secretion patterns shift. Thyroid output adjusts downward. Insulin and leptin levels drop precipitously, both of which have downstream effects on follicular health. The result is a massive, synchronized wave of follicles transitioning to telogen, producing the dramatic shedding that appears three to six months after the weight loss begins.
The ideal rate of weight loss for hair preservation
Most dermatologists and endocrinologists recommend a weight loss rate of one to two pounds per week, or roughly 0.5-1% of body weight per week, to minimize the risk of telogen effluvium. The problem is that semaglutide and tirzepatide often produce much faster weight loss than this, particularly in the first few months. Many patients lose 5-10 pounds in the first month alone. While this rapid initial loss is partly water weight and glycogen depletion, the metabolic signal to the body is the same.
Working with a healthcare provider to adjust dosing can help moderate the rate of weight loss. Some practitioners advocate for slower titration schedules, keeping patients on lower doses for longer periods before escalating. For those using tirzepatide, understanding the dosing for weight loss in units allows for more granular control. The unit conversions for tirzepatide can be tricky, so using a reliable dosage calculator ensures accuracy. The goal is to find the sweet spot where meaningful weight loss continues, appetite remains well-managed per semaglutide weight loss protocols, but the pace does not trigger a hair follicle crisis.
Caloric floor and protein minimums
Regardless of how aggressively your GLP-1 medication suppresses appetite, you must maintain adequate nutrition. Total caloric intake should not drop below 1,200 calories per day for women or 1,500 calories per day for men for extended periods. These floors exist because below them, essential nutrient intake becomes nearly impossible to maintain even with supplementation. Protein intake deserves special attention. A minimum of 0.8 grams per kilogram of body weight is the baseline recommendation, but many experts in metabolic medicine now recommend 1.0-1.2 grams per kilogram for patients on GLP-1 therapy, specifically to protect against hair loss and muscle wasting.
Nutritional deficiencies that accelerate GLP-1 related hair loss
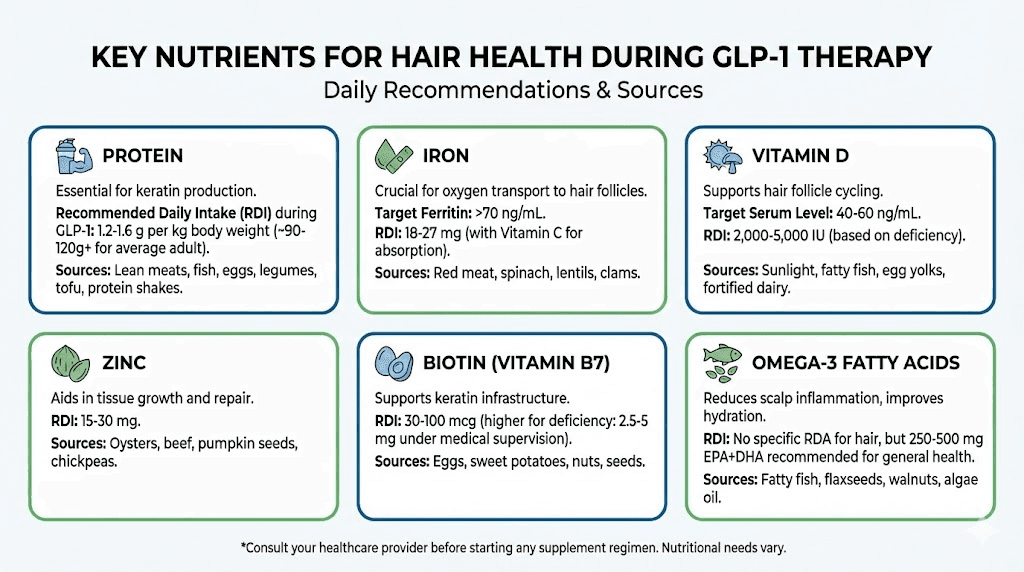
Even if you lose weight at a moderate pace, nutritional deficiencies can independently drive hair shedding. GLP-1 medications reduce appetite so effectively that many patients simply do not eat enough to meet their micronutrient needs. Understanding which nutrients matter most for hair health, and proactively supplementing them, is one of the most effective things you can do to protect your hair during treatment.
Iron and ferritin
Iron deficiency is the most common nutritional cause of hair loss worldwide, and GLP-1 therapy significantly increases the risk of developing it. Reduced food intake means less dietary iron. Gastrointestinal side effects common with these medications, including nausea and reduced gastric acid production, can further impair iron absorption. Ferritin, the storage form of iron, should ideally remain above 40 ng/mL for optimal hair health. Many dermatologists consider levels below 30 ng/mL to be a contributing factor in hair shedding, even when they technically fall within the "normal" laboratory range. If you are experiencing hair loss on a GLP-1 medication, ferritin is the first blood test to request. A simple iron panel with ferritin can reveal a correctable cause that, once addressed, may stop the shedding entirely.
Zinc
Zinc is essential for cellular division in the hair follicle matrix. It also plays a role in the hair follicle regression and recovery cycle, and deficiency has been directly linked to both telogen effluvium and diffuse alopecia. Zinc is found in high concentrations in red meat, shellfish, and legumes. Patients who eat less of these foods due to GLP-1 appetite suppression may fall short. Supplementation of 15-30 mg of elemental zinc daily is commonly recommended during active weight loss, but should be balanced with copper intake (1-2 mg daily) because long-term zinc supplementation can deplete copper stores.
Vitamin D
Vitamin D receptors are present in hair follicles and play a role in anagen initiation. Deficiency, defined as serum 25-hydroxyvitamin D below 30 ng/mL, has been associated with both telogen effluvium and alopecia areata. Many patients on GLP-1 medications are already vitamin D deficient before starting treatment, as obesity itself is associated with lower vitamin D levels due to sequestration in adipose tissue. As fat mass decreases, some stored vitamin D may be released, but this does not guarantee adequacy. Testing and supplementation with 2,000-5,000 IU daily is prudent for anyone experiencing hair concerns during weight loss therapy.
Biotin with an important caveat
Biotin, also known as vitamin B7, supports keratin production and is widely marketed as a hair health supplement. Evidence for its efficacy in people who are not biotin-deficient is limited. However, true biotin deficiency can cause hair loss, and reduced dietary intake during GLP-1 therapy could push levels lower. A daily supplement of 2,500-5,000 mcg of biotin is generally safe, but there is a critical caveat that every patient and prescriber should know about.
Biotin interferes with certain laboratory immunoassays, including thyroid function tests. High biotin levels can cause falsely low TSH readings and falsely elevated free T4, mimicking hyperthyroidism on paper. If you are supplementing biotin and have thyroid labs drawn, you must stop biotin supplementation for at least 48-72 hours before the blood draw. Failure to do so can lead to misdiagnosis, unnecessary medication changes, or missed thyroid dysfunction that may itself be contributing to your hair loss. This interaction is widely documented but frequently overlooked in clinical practice.
Protein
Hair is approximately 95% keratin, a structural protein. Without adequate protein intake, the body simply cannot produce enough keratin to maintain normal hair growth. The recommended minimum during GLP-1 therapy is 0.8-1.2 grams of protein per kilogram of body weight. For a 180-pound (82 kg) person, that means 66-98 grams of protein daily.
Many patients on semaglutide or tirzepatide consume far less than this because their appetite is so suppressed. Protein should be prioritized at every meal. If solid food intake is limited by nausea or early satiety, protein shakes, Greek yogurt, and collagen supplements can help meet minimum requirements without overwhelming a reduced appetite.
Those exploring the combination of semaglutide with B12 are already thinking along the right lines about nutritional support during therapy.
B12 and folate
Vitamin B12 is essential for DNA synthesis in rapidly dividing cells, including those in the hair follicle matrix. Folate works alongside B12 in this process. Reduced dietary intake, combined with potential alterations in gut absorption from GLP-1 gastrointestinal effects, can create deficiencies in both. A B-complex supplement or standalone B12 (methylcobalamin form, 1,000 mcg daily) provides an easy safety net. Folate at 400-800 mcg daily covers the baseline need.
Hormonal changes during GLP-1 therapy and hair follicle impact
Beyond nutrition, the hormonal landscape shifts significantly during GLP-1 mediated weight loss. These hormonal changes can affect hair follicles through pathways entirely separate from nutritional deficiency, which is why some patients experience hair loss despite maintaining excellent nutritional status.
Thyroid axis changes
Rapid weight loss consistently affects the hypothalamic-pituitary-thyroid axis. Total T3 levels often decline during caloric restriction as the body downregulates metabolic rate to conserve energy, a process sometimes called "euthyroid sick syndrome" or "low T3 syndrome." Free T3 may remain in the normal range but trend toward the lower end. Since T3 directly stimulates hair follicle keratinocyte proliferation, even subtle declines can slow hair growth or push follicles into premature catagen and telogen. Monitoring thyroid function every three to six months during active GLP-1 therapy, and specifically requesting free T3 along with TSH and free T4, helps catch these shifts early.
Insulin and IGF-1 signaling
GLP-1 medications improve insulin sensitivity, which is one of their major metabolic benefits. But hair follicles have insulin receptors and respond to insulin-like growth factor 1 (IGF-1). As insulin levels normalize and drop from previously elevated states, IGF-1 levels may also decline. IGF-1 is a growth-promoting signal for hair follicles, and lower levels have been associated with reduced hair growth in some studies. This mechanism may be particularly relevant for patients who had significant insulin resistance before starting GLP-1 therapy. Their follicles were accustomed to a high-insulin, high-IGF-1 environment, and the correction of this environment, while metabolically beneficial, may temporarily disadvantage hair growth.
Estrogen and androgen balance
Adipose tissue contains aromatase, an enzyme that converts androgens to estrogens. As body fat decreases, total aromatase activity decreases, which can shift the androgen-to-estrogen ratio. For women, this shift may unmask genetic susceptibility to androgenic alopecia that was previously masked by higher estrogen levels. For men, the hormonal shift is generally less impactful on hair because male-pattern hair loss is already driven by DHT sensitivity in genetically predisposed follicles regardless of body composition. Women who are experiencing patterned thinning, distinct from diffuse shedding, during GLP-1 therapy should discuss this hormonal mechanism with their dermatologist. It may require different treatment approaches than standard telogen effluvium management, and resources covering peptides for hormone balance and peptide support during perimenopause may provide additional context.
Cortisol and stress hormones
Caloric restriction elevates cortisol. This is a well-established physiological response. Elevated cortisol shifts hair follicles from anagen to catagen, accelerating the progression toward telogen. It also increases inflammation around the follicle, potentially damaging the dermal papilla cells that drive new hair growth. The stress response is compounded when patients are anxious about the hair loss itself, creating a feedback loop where stress about shedding causes more stress hormones, which cause more shedding. Managing stress through sleep optimization, moderate exercise, and mindfulness practices is not just feel-good advice. It is a legitimate hair preservation strategy with physiological mechanisms behind it.
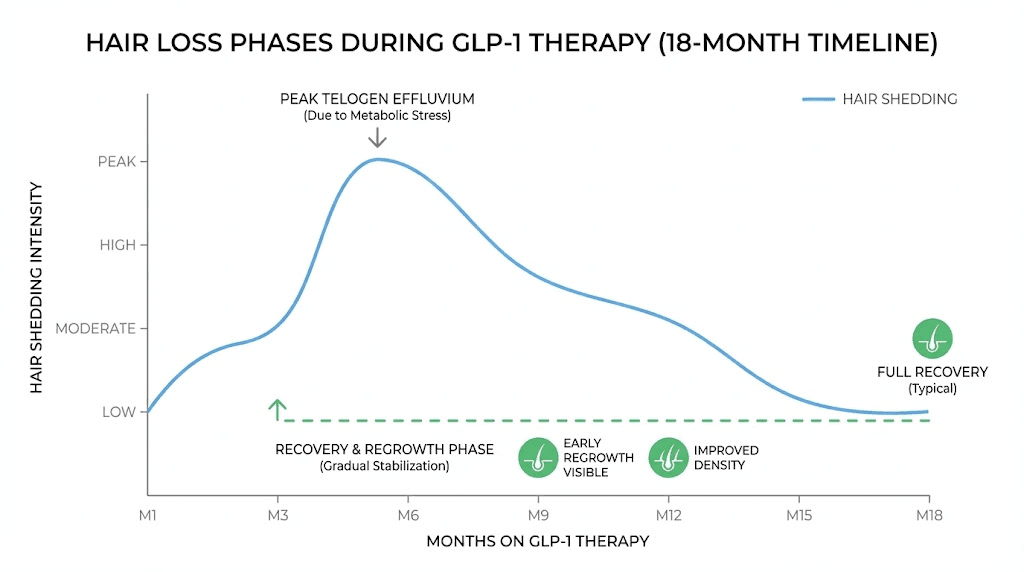
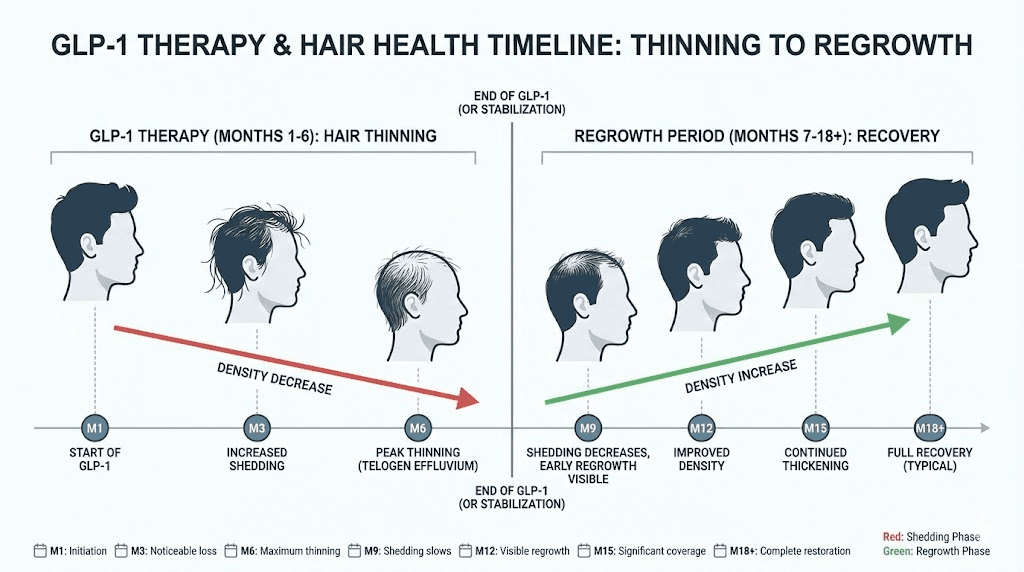
Timeline of GLP-1 hair loss from first dose to recovery
Knowing what to expect and when to expect it can dramatically reduce the anxiety associated with GLP-1 related hair loss. Here is the typical timeline, broken down by phase.
Months one through three: the silent phase
During the first one to three months of GLP-1 therapy, you are unlikely to notice any change in your hair. But changes are happening at the follicular level. As your body enters a caloric deficit and begins losing weight, some follicles are receiving the signal to transition from anagen to catagen and eventually telogen. This process takes time. The hair shaft remains attached during telogen. You will not see shedding yet. This is the critical window for prevention. Implementing nutritional support, adequate protein intake, and optimizing micronutrient status during this phase can reduce the severity of shedding that may come later.
Months three through six: onset of shedding
This is when most patients first notice increased hair fall. More hair in the shower drain. More strands on the pillow. A brush that fills up faster than it used to. The shedding can range from mildly noticeable to alarming, depending on how many follicles were pushed into telogen and how quickly. Women tend to notice this sooner and more acutely than men, partly because women typically start with longer hair that makes shedding more visible, and partly because the female demographic is disproportionately affected. If you are in this phase, the most important thing to understand is that each hair falling out is making room for a new hair. The follicle is not dead. It is resetting.
Months six through nine: peak shedding and early recovery
For most patients, shedding peaks around months four through seven and then gradually diminishes. By months six through nine, many notice that the rate of hair loss has slowed or stopped. Early regrowth may become visible as short, fine hairs appearing along the hairline and part line. These new hairs grow at approximately half an inch per month, so noticeable volume improvement takes additional time.
Months nine through eighteen: regrowth and recovery
Full hair recovery from telogen effluvium typically takes six to twelve months from the point where shedding stops. Since shedding itself may persist for three to six months, the total timeline from first dose to full recovery can span twelve to eighteen months. Some patients recover faster. Some take longer. Individual factors including genetics, nutritional status, hormonal health, and ongoing medication use all influence the timeline. Throughout this process, the hair may go through stages. Regrowth initially appears as fine, sometimes lighter-colored baby hairs. These gradually thicken and darken to match the rest of your hair over subsequent months.
For people who stop their GLP-1 medication, a second round of telogen effluvium can sometimes occur as the body readjusts to increased caloric intake and changing hormonal signals. Understanding what to expect during semaglutide withdrawal helps set realistic expectations and prevent panic about a second shedding episode.
Preventing hair loss while taking semaglutide or tirzepatide
Prevention is always easier than treatment. If you are starting or currently taking a GLP-1 medication and want to minimize hair loss risk, these evidence-based strategies can make a meaningful difference. Not all of them will apply to every person, but implementing even a few can shift the odds significantly in your favor.
Protein prioritization protocol
Make protein the non-negotiable foundation of every meal. Aim for 0.8-1.2 grams per kilogram of body weight daily, with a minimum of 60 grams per day regardless of body weight. Spread protein intake across three to four meals rather than loading it into one sitting, because the body can only utilize about 25-40 grams of protein per meal for muscle and tissue synthesis. When appetite suppression from semaglutide or tirzepatide makes eating difficult, prioritize protein above all other macronutrients. If you can only eat 800 calories in a day, make 350-400 of those calories come from protein sources. Protein shakes, bone broth, Greek yogurt, cottage cheese, and collagen peptides can all contribute to meeting this target without requiring large food volumes.
Micronutrient supplementation from day one
Do not wait for hair loss to start before supplementing. Begin a targeted micronutrient regimen when you start your GLP-1 medication, or ideally even before. A practical daily stack for hair protection includes a high-quality multivitamin as a baseline, plus additional iron (if ferritin is below 50 ng/mL, under medical supervision), zinc at 15-30 mg with 1-2 mg copper, vitamin D3 at 2,000-5,000 IU depending on baseline levels, biotin at 2,500-5,000 mcg (remembering the thyroid lab caveat), and a B-complex covering B12 and folate. This is not overkill. It is insurance against the nutritional gaps that GLP-1 appetite suppression creates, and it supports overall health during a period of significant metabolic change. Anyone following a peptide dosing protocol alongside their GLP-1 medication should ensure supplementation does not interfere with other compounds they may be using.
Gradual dose titration
Work with your prescriber to titrate your GLP-1 medication slowly. Rather than jumping to the maximum dose as quickly as the prescribing guidelines allow, consider staying at each dose level for a longer period. The standard tirzepatide titration moves from 2.5 mg to 5 mg after four weeks, then up from there. Some clinicians extend each step to six or eight weeks, allowing the body more time to adapt. The result is typically slower weight loss but the same total weight loss over a longer period, with potentially less metabolic shock and less hair follicle disruption. For those exploring semaglutide, understanding the unit-to-milligram conversions allows for more precise dose adjustments.
Caloric floor maintenance
Set a hard floor for daily caloric intake and do not go below it, regardless of how little your appetite demands. For women, this floor should be 1,200 calories. For men, 1,500 calories. On days when appetite suppression is severe, use calorie-dense but nutrient-rich foods to meet minimums. A tablespoon of olive oil adds 120 calories. An ounce of nuts adds 160-180. A protein shake with whole milk and peanut butter can contribute 400-500 calories. These additions do not undermine weight loss because even with them, most patients on GLP-1 therapy still maintain a significant caloric deficit. But they do protect against the severe nutritional depletion that drives the worst hair loss outcomes.
Baseline blood work before starting
Before your first dose of any GLP-1 medication, get baseline blood work that includes a complete blood count, comprehensive metabolic panel, ferritin, serum iron, total iron binding capacity, zinc, vitamin D (25-OH), B12, folate, TSH, free T3, free T4, and hemoglobin A1c. This baseline serves two purposes. First, it identifies pre-existing deficiencies that should be corrected before adding the metabolic stress of rapid weight loss. Second, it gives you comparison points for future labs, making it much easier to detect declining levels early and intervene before hair loss occurs.
Treatment options for GLP-1 related hair loss
If prevention was not enough and you are already experiencing noticeable hair shedding, multiple treatment options exist. Some have strong clinical evidence. Others have promising but limited data. The best approach often combines several interventions simultaneously because hair loss is typically multifactorial.
Topical minoxidil
Minoxidil remains the most evidence-based topical treatment for hair loss of almost any etiology. It works by prolonging the anagen phase, increasing follicular blood flow, and stimulating follicular cells to divide. For GLP-1 related telogen effluvium, minoxidil can accelerate the transition back from telogen to anagen, shortening the recovery period. The standard over-the-counter formulation is 5% minoxidil applied to the scalp once or twice daily. Results typically become visible after two to four months of consistent use. One important caveat is that starting minoxidil can itself cause a brief period of increased shedding during the first two to four weeks, as it pushes telogen hairs out to make room for new anagen hairs. This "minoxidil shed" is temporary and actually indicates the medication is working, but it can be psychologically distressing if you are not expecting it.
Low-level laser therapy
Low-level laser therapy (LLLT) uses red light at specific wavelengths (typically 650-670 nm) to stimulate mitochondrial activity in hair follicle cells. Multiple FDA-cleared devices exist, including laser caps, helmets, and combs. Clinical evidence supports modest improvements in hair density and thickness with consistent use, typically three to four sessions per week for 15-25 minutes each. LLLT works best as an adjunct to other treatments rather than a standalone intervention. It is well-tolerated with essentially no side effects, making it an attractive option for patients who prefer non-pharmacological approaches.
Platelet-rich plasma injections
PRP therapy involves drawing a small amount of your blood, concentrating the platelets through centrifugation, and injecting the platelet-rich concentrate directly into the scalp at the level of the hair follicles. Platelets release growth factors, including PDGF, TGF-beta, VEGF, and IGF-1, all of which support follicular health and can stimulate dormant follicles. Studies show that PRP can improve hair density, hair count, and hair thickness in patients with both androgenic alopecia and telogen effluvium. Treatment typically involves three sessions spaced four to six weeks apart, followed by maintenance sessions every six to twelve months. The main drawback is cost, as PRP is not typically covered by insurance and can run several hundred to over a thousand dollars per session.
Correcting identified deficiencies
If blood work reveals specific deficiencies (low ferritin, low vitamin D, low zinc, or low B12), targeted correction may be the single most effective intervention. Oral iron supplementation for low ferritin typically takes three to six months to raise levels adequately. Some patients with very low ferritin benefit from intravenous iron infusions, which can replete stores much more quickly. Vitamin D correction with high-dose supplementation (50,000 IU weekly for eight to twelve weeks, then maintenance dosing) can normalize levels within three months. Zinc and B12 deficiencies respond quickly to oral supplementation. The key insight is that for deficiency-driven hair loss, no amount of minoxidil or laser therapy will work until the underlying deficiency is corrected. Fix the cause first. Then add growth-stimulating treatments if additional support is needed.
Scalp health optimization
Scalp inflammation, seborrheic dermatitis, and folliculitis can all worsen hair loss during GLP-1 therapy. Using a gentle, sulfate-free shampoo and avoiding harsh chemical treatments reduces additional follicular stress. Scalp massage for five minutes daily has been shown in small studies to increase hair thickness, possibly by improving blood flow to the follicles. Avoiding tight hairstyles that put traction on follicles (ponytails, braids, buns) removes another potential contributor to hair loss.
Peptides that support hair growth during weight loss therapy
For those already familiar with the world of peptides and their applications, several peptide compounds show promising effects on hair growth and follicular health. These are not replacements for the foundational strategies discussed above, but they represent an advanced tier of intervention for people who want to be as proactive as possible about hair preservation during GLP-1 therapy. Understanding how peptides work at the cellular level helps explain why they can be particularly effective for hair-related applications.
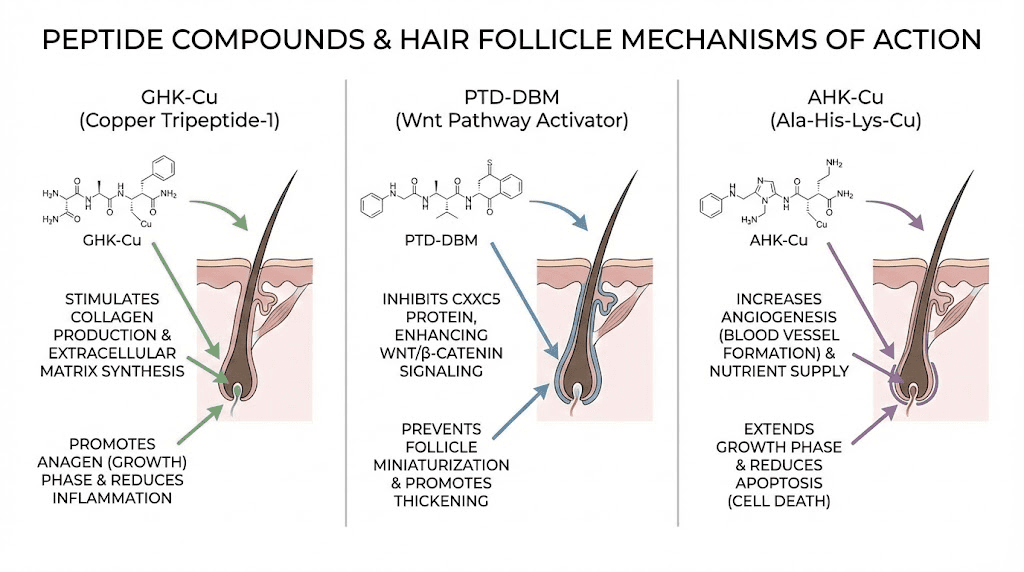
GHK-Cu (copper peptide)
GHK-Cu is a naturally occurring tripeptide that binds copper and plays a central role in tissue remodeling, wound healing, and hair follicle regulation. Research shows that GHK-Cu can enlarge hair follicles, stimulate hair growth, and reduce hair loss when applied topically. It works through multiple mechanisms, increasing blood vessel formation around follicles, reducing inflammation, stimulating collagen synthesis in the dermal papilla, and blocking 5-alpha reductase, the enzyme that converts testosterone to the follicle-damaging DHT. The comprehensive GHK-Cu peptide for hair guide covers application methods and protocols in detail, while the broader copper peptides GHK-Cu guide explains the full range of tissue-repair benefits. For topical application, copper peptides for hair growth are available in serums and can be incorporated into a daily scalp care routine. Those interested in dosing specifics should review the GHK-Cu peptide dosage guide.
PTD-DBM
PTD-DBM is a peptide that has shown remarkable results in hair growth studies, potentially rivaling minoxidil in some preclinical models. It works by activating the Wnt/beta-catenin signaling pathway, which is crucial for hair follicle development and cycling. In mouse studies, PTD-DBM promoted hair regrowth in alopecia models and demonstrated the ability to stimulate new follicle formation, something most treatments cannot do. While human clinical data is still limited, the mechanism is compelling and the preclinical results are among the most impressive seen for any peptide-based hair treatment. The PTD-DBM peptide hair growth guide provides a thorough review of the research and practical considerations for those interested in this compound.
AHK-Cu
AHK-Cu is a newer copper peptide variant that combines the benefits of copper delivery with a specific tripeptide sequence (alanine-histidine-lysine) optimized for follicular uptake. Early research suggests it may be more effective than GHK-Cu for hair-specific applications, though the evidence base is smaller. The AHK-Cu peptide complete guide covers the current state of research and how this peptide differs from its more established cousin.
Peptide shampoos and topical formulations
For those who prefer non-injectable approaches, peptide shampoos containing copper peptides and other hair-supporting peptide sequences offer a low-effort way to deliver these compounds directly to the scalp. While the concentration of active peptides in shampoo formulations is typically lower than in dedicated serums, daily use provides consistent exposure and can complement other interventions. The convenience factor is significant because compliance is the biggest challenge with any hair loss treatment regimen, and using a peptide-containing shampoo requires no additional steps beyond your normal hygiene routine.
Stacking peptides for hair support
Some researchers and practitioners combine multiple hair-supporting peptides for a synergistic effect. A typical stack might include topical GHK-Cu for follicular stimulation and anti-DHT effects, an oral collagen peptide supplement for keratin precursor support, and a peptide stacking approach that considers interactions and timing. Before combining compounds, reviewing the guidelines on how many peptides you can take at once ensures safety. SeekPeptides members access detailed stacking protocols and interaction databases that take the guesswork out of multi-peptide approaches, particularly valuable for people managing the complex intersection of weight loss therapy and hair preservation.
When to see a dermatologist about GLP-1 hair loss
Most GLP-1 related hair loss is telogen effluvium. Most telogen effluvium resolves on its own. But not all hair loss during GLP-1 therapy is benign, and there are specific red flags that warrant professional evaluation sooner rather than later.
Red flags requiring immediate evaluation
See a dermatologist promptly if you notice any of the following. Patchy hair loss with well-defined borders suggests alopecia areata, an autoimmune condition that requires different treatment than telogen effluvium. The case of the 23-year-old woman who developed alopecia areata two months after starting semaglutide demonstrates that GLP-1 medications can potentially trigger autoimmune hair loss in susceptible individuals. Scalp pain, burning, or itching accompanying the hair loss may indicate an inflammatory condition such as scarring alopecia, which can cause permanent follicular damage if not treated promptly. Hair breakage rather than shedding from the root, visible as broken short hairs without the white telogen bulb, suggests a structural hair problem rather than a cycling problem and requires different investigation. Rapid, severe hair loss that exceeds what would be expected for telogen effluvium, losing large clumps rather than diffuse thinning, warrants urgent evaluation.
What to expect at the dermatology visit
A dermatologist evaluating GLP-1 related hair loss will typically perform a thorough scalp examination, often using dermoscopy (a specialized magnifying instrument) to visualize the scalp and hair shafts at high magnification. They may perform a hair pull test, gently pulling on groups of about 60 hairs to quantify active shedding. Blood work will likely include everything mentioned in the baseline panel above, plus potentially ANA and other autoimmune markers if alopecia areata is suspected. In some cases, a scalp biopsy may be recommended to definitively diagnose the type of hair loss and rule out scarring conditions.
Differential diagnosis considerations
Your dermatologist will consider several potential causes beyond GLP-1 related telogen effluvium. Androgenic alopecia, as discussed, can be unmasked or worsened by the hormonal changes of weight loss. Thyroid dysfunction, either overt or subclinical, must be evaluated. Iron deficiency anemia deserves separate consideration even if ferritin is technically "normal." Autoimmune conditions, including alopecia areata and lupus, can present with hair loss. Other medications you may be taking alongside your GLP-1, including metformin, ACE inhibitors, and beta-blockers, can also cause hair loss and should be reviewed. Understanding the full picture of peptide safety and risks applies here as well, especially if you are using any additional compounds alongside your GLP-1 medication.
Long term outlook and hair recovery after GLP-1 treatment
The long-term prognosis for GLP-1 related hair loss is overwhelmingly positive for the majority of patients. Understanding this prognosis in detail can help manage expectations and reduce the anxiety that often accompanies the experience.
Telogen effluvium recovery rates
Telogen effluvium from weight loss, including GLP-1 mediated weight loss, is a self-limiting condition. Once the triggering stressor stabilizes, meaning weight loss slows to a manageable rate and nutritional status improves, follicles begin cycling back from telogen to anagen. Hair regrowth typically begins within three to six months of the shedding phase peaking. Full recovery of previous hair density takes six to twelve months from the onset of regrowth. In total, the cycle from initial shedding to full recovery spans roughly nine to eighteen months.
It is important to set realistic expectations. Recovery is not linear. You may notice periods of accelerated regrowth followed by plateaus. The new hairs that grow in may initially differ in texture or color from your original hair, appearing finer, lighter, or slightly wavier. This is normal and temporary. Over the subsequent months, the new growth will normalize to match the rest of your hair.
Continuing GLP-1 therapy during recovery
You do not necessarily have to stop your GLP-1 medication to recover from hair loss. As long as weight loss has slowed (entering a maintenance phase or losing at a moderate rate), nutritional status is optimized, and no other correctable factors are driving the shedding, hair can recover even while continuing therapy. Many patients reach a weight loss plateau after 12-18 months on GLP-1 therapy, and this stabilization period often corresponds with natural hair recovery as the metabolic stress diminishes. The body adapts to the new normal. Follicles resume their regular cycling. Hair volume gradually returns. Whether you are on a maintenance dose of oral tirzepatide or injectable semaglutide, continuing therapy at a stable dose while supporting hair health through the strategies outlined in this guide is a reasonable approach for most patients.
When hair loss persists beyond expected timelines
If hair shedding continues beyond six to nine months without any improvement, or if regrowth has not begun within twelve months of peak shedding, reevaluation is warranted. Persistent hair loss suggests that something beyond simple telogen effluvium is at play. Chronic telogen effluvium, a condition where shedding persists for more than six months, can occur when the triggering stressor is ongoing, such as continuous aggressive weight loss, unresolved nutritional deficiencies, or untreated thyroid dysfunction. Androgenic alopecia may have been unmasked and will not resolve without targeted treatment. A return to the dermatologist for updated labs, repeat scalp examination, and possibly biopsy is appropriate at this stage.
Protecting your hair if you restart or change GLP-1 medications
Switching from one GLP-1 medication to another, or restarting after a break, carries a theoretical risk of triggering another round of telogen effluvium, particularly if the new medication or restart leads to another phase of rapid weight loss.
Patients who experienced hair loss on semaglutide and switch to tirzepatide, or who explore newer options like retatrutide or cagrilintide, should implement the prevention protocols from day one of the new medication. The risk is likely lower for patients who are already at or near their goal weight and switching for maintenance purposes, but nutritional vigilance remains essential. Tracking everything from your retatrutide dosage calculations to your daily protein intake helps you stay ahead of potential problems. Resources covering the differences between medications, such as the comparison of mazdutide versus tirzepatide, can help inform medication selection decisions where hair loss risk is a consideration.
Supporting your body during the entire weight loss journey
The bigger picture extends beyond hair. GLP-1 mediated weight loss is a significant physiological event that affects virtually every organ system. Hair is the most visible indicator that the body is under metabolic stress, but it is rarely the most medically important one. Muscle preservation, bone density maintenance, cardiovascular adaptation, and metabolic health all require attention during aggressive weight loss. Many of the strategies that protect hair, adequate protein, comprehensive supplementation, moderate pace of loss, and regular monitoring, also protect these other systems. Understanding the best peptide stacks for weight loss and the role of compounds like BPC-157 and TB-500 in tissue repair and recovery can complement your overall health strategy during this period. For those just beginning to explore these compounds, the getting started with peptides guide provides a solid foundation, and the common peptide mistakes beginners make article helps avoid early pitfalls.
Some patients have found benefit in combining their GLP-1 therapy with supportive peptides. The concept of taking peptides alongside Ozempic for healing has gained attention, particularly for individuals managing multiple health goals simultaneously. The inflammation peptides guide covers compounds that may help modulate the inflammatory processes that can contribute to follicular stress during weight loss.
The landscape of GLP-1 therapy continues to evolve rapidly. New delivery methods like GLP-1 patches and new formulations from providers like Evolv GLP-1, Thrive GLP-1, and MMIT GLP-1 programs may eventually offer approaches that minimize metabolic shock and, potentially, hair loss risk. Staying informed through resources like SeekPeptides ensures you have access to the latest evidence as the field evolves.
Building a comprehensive hair protection plan
Pulling everything together, here is how to build a practical, evidence-based hair protection plan that you can implement alongside your GLP-1 therapy. This is not about choosing one strategy over another. The most effective approach layers multiple interventions simultaneously.
Before starting GLP-1 therapy
Get comprehensive baseline blood work including ferritin, vitamin D, zinc, B12, thyroid panel (TSH, free T3, free T4), and a complete blood count. Correct any deficiencies before your first dose. Begin a high-quality multivitamin, vitamin D3 supplementation if levels are below 40 ng/mL, and ensure protein intake is already at 0.8-1.0 grams per kilogram daily. Document your current hair condition with photos, including the hairline, part line, crown, and temples. These baseline photos are invaluable for tracking changes objectively rather than relying on perception, which is heavily influenced by anxiety.
During active weight loss phase
Maintain protein intake at 1.0-1.2 grams per kilogram daily. Do not let total calories drop below your daily floor (1,200 for women, 1,500 for men). Continue all supplements. Recheck blood work at three months and six months. If ferritin, vitamin D, or any other marker has dropped despite supplementation, adjust doses upward. Request slow titration of your GLP-1 medication if possible. Consider adding topical GHK-Cu or a peptide shampoo as a proactive measure. Take monthly hair photos at the same angle and lighting for objective comparison. If you are using a peptide calculator for any supportive compounds, keep precise records of dosing and timing.
If shedding begins
Do not panic. Understand the timeline. If shedding starts at months three to six, it is almost certainly telogen effluvium and it will resolve. Intensify nutritional support. Add topical 5% minoxidil if you are comfortable with it, understanding the initial "minoxidil shed" is temporary. Consider LLLT three to four times per week. Get blood work done immediately to check for correctable deficiencies. If shedding is severe or follows a patchy pattern, see a dermatologist within two weeks. Stress management becomes especially important during this phase, as the anxiety about hair loss can elevate cortisol and worsen the problem. Resources on peptides for anxiety and mood support may be relevant here, and the best peptides for energy can help combat the fatigue that sometimes accompanies both weight loss and the emotional burden of hair shedding.
During recovery phase
Continue all supportive measures until regrowth is well established. Do not stop minoxidil abruptly if you started it, as this can trigger rebound shedding. Gradually reduce frequency over two to three months if you wish to discontinue. Maintain protein and supplement intake. Be patient. Hair grows approximately half an inch per month. If you lost hair at month four and regrowth begins at month eight, you will not see meaningful volume improvement until month twelve or later. Continue monthly photos to document progress objectively.
The connection between weight loss methods and hair outcomes
GLP-1 medications are not the only weight loss approach that can trigger hair shedding. Bariatric surgery, very low calorie diets, and even aggressive exercise regimens can all cause telogen effluvium through the same mechanisms. In fact, hair loss rates after bariatric surgery are often higher than those seen with GLP-1 therapy, with some studies reporting rates of 30-40% in the first year post-surgery. This context is important because it underscores that the hair loss is primarily about the weight loss itself, not the specific medication.
Understanding this broadens the perspective. If you are choosing between weight loss approaches and hair preservation is a high priority, the rate of weight loss matters more than the method. A patient who loses 60 pounds over 18 months on tirzepatide will likely experience less hair impact than one who loses 60 pounds in 6 months through a very low calorie diet, even though neither used surgery. The comparison between semaglutide and tirzepatide becomes relevant here, as the two medications may produce different rates of weight loss in different individuals, and choosing the one that produces a more gradual trajectory could be hair-protective.
For those exploring the full spectrum of weight management options, understanding how different peptides for weight loss in women or fat burning peptides for men affect the body differently can inform a more nuanced approach. Compounds like AOD-9604, 5-amino-1MQ, and tesofensine each work through different metabolic pathways. Some may produce slower, more gradual fat loss that is gentler on hair follicles, while others, like Lipo-C and other lipotropic peptides, support fat metabolism without the dramatic appetite suppression that leads to nutritional depletion. The best fat burning peptide for your situation depends on balancing efficacy with tolerability across all dimensions, including hair preservation.
Those interested in combining approaches can explore the peptides for weight loss and muscle gain guide and the bioactive precision peptides for weight loss article, both of which discuss multi-compound strategies. The peptides for belly fat guide covers targeted approaches that may complement GLP-1 therapy without intensifying the metabolic stress that drives hair loss. Using the peptide calculator for weight loss and the peptide cost calculator can help plan a sustainable, financially viable protocol.
Practical considerations for different demographics
GLP-1 related hair loss does not affect everyone equally. Specific demographic groups face unique considerations that warrant tailored approaches.
Women under 40
Premenopausal women on GLP-1 medications face hair loss primarily from telogen effluvium and nutritional depletion. Their hormonal environment is generally protective against androgenic patterns, so the prognosis is typically excellent with proper nutritional support. Iron status deserves particular attention in menstruating women, as monthly blood loss combined with reduced dietary intake can deplete stores rapidly. The general safe peptides for women guide provides context for women navigating peptide use alongside GLP-1 therapy.
Women over 40 and in perimenopause or menopause
This demographic is at highest risk for GLP-1 related hair loss. The combination of declining estrogen, changing androgen ratios, and the metabolic stress of weight loss creates a perfect storm for follicular disruption. Both telogen effluvium and unmasking of androgenic alopecia are possible. Women in this group should be more aggressive with prevention, consider dermatology evaluation early in the process, and may benefit from exploring peptides for women over 40 and peptides for menopause weight loss that address both the metabolic and hormonal dimensions simultaneously. The menopause peptide guide covers compounds that may support hormonal balance during this transition.
Men
Men are less frequently reported in GLP-1 hair loss studies, but they are not immune. Male-pattern hair loss (androgenic alopecia) is already common and may accelerate during GLP-1 therapy due to shifting androgen metabolism. Men with a family history of baldness should be particularly vigilant. The shorter hairstyles typical of men can make diffuse telogen effluvium less visually obvious, which may explain some of the underreporting. The peptides for men guide covers compounds relevant to male health optimization during weight loss therapy.
Older adults
Adults over 60 on GLP-1 therapy face compounded risk because aging naturally reduces hair density and follicular regenerative capacity. The same degree of telogen effluvium that would be unnoticeable in a 30-year-old can be visually significant in a 65-year-old who already has thinner baseline hair. Additionally, older adults are more likely to have pre-existing nutritional deficiencies, thyroid dysfunction, and polypharmacy that contributes to hair loss. Comprehensive medical evaluation and aggressive nutritional support are particularly important in this age group. The longevity peptides guide covers compounds that support cellular health and tissue regeneration across multiple systems, including the integumentary system.
Understanding the research landscape
The science of GLP-1 medications and hair loss is still evolving. Current understanding is largely based on pharmacovigilance data, clinical trial secondary endpoints, case reports, and small observational studies. No large-scale, randomized controlled trial has been specifically designed to study hair loss as a primary outcome of GLP-1 therapy. This means that while the association is clear and the mechanisms are well-hypothesized, definitive answers about causation, dose-response relationships, and optimal prevention remain areas of active investigation.
Several research questions remain open. Do GLP-1 receptors in human hair follicles play a clinically meaningful role in hair cycling? Does the MAPK/ERK pathway activation by GLP-1 agonists have a net positive or negative effect on follicular health? Are certain genetic profiles more susceptible to GLP-1 related hair loss? Can biomarkers predict which patients will experience significant shedding before it occurs? These questions represent the frontier of knowledge, and the answers, when they come, will refine the prevention and treatment strategies outlined in this guide.
Staying current with peptide research and studies helps you follow the evolving evidence base. The peptide forum guide can connect you with communities discussing real-world experiences with both GLP-1 medications and hair-supporting peptides. Understanding the legal landscape of peptides is also important for anyone considering adding peptide-based hair treatments to their regimen. For a broader view of related compounds, the GLP-3 peptide and amylin receptor agonist guides cover emerging targets in the metabolic peptide space that may eventually offer weight loss with fewer side effects.
For those managing their GLP-1 therapy comprehensively, knowing whether tirzepatide causes fatigue, understanding proper tirzepatide storage in the fridge and refrigeration requirements, and following tirzepatide before and after results from other patients can help set realistic expectations across all dimensions of the treatment experience. The complete peptide list and injectable peptide list serve as comprehensive references for exploring additional supportive compounds.
Whether you are just getting started with peptides or are an experienced researcher looking to optimize your peptide cycle planning, the relationship between weight management and hair health deserves careful attention. Understanding how long peptides take to work and reviewing peptides before and after results provides realistic timelines for the supportive compounds discussed throughout this guide. The practical aspects of peptide use, from reconstitution and bacteriostatic water preparation to mixing protocols, water volume calculations, storage best practices, post-reconstitution storage, and knowing peptide expiration dates, all matter for getting the most out of any hair-supporting peptide protocol. For those using injectable compounds, the peptide injections guide covers technique, while the dosage calculation guide and peptide dosage chart ensure accuracy. Tools like the peptide reconstitution calculator, peptide stack calculator, and peptide calculator make the math straightforward.
The financial aspect of managing hair health during GLP-1 therapy is worth considering as well. Between the medication itself, supplements, potential dermatology visits, PRP treatments, and peptide products, costs can add up. The peptide therapy cost guide and resources on online peptide therapy can help you understand the financial landscape and find cost-effective approaches. For weight loss medication costs specifically, the retatrutide cost guide and retatrutide buying guide cover pricing for this emerging compound. Even public figures like Joe Rogan have discussed peptides and their role in health optimization, bringing mainstream attention to compounds that many in the peptide community have been using for years.
For researchers serious about optimizing both their weight loss journey and their hair health, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, detailed protocols for hair-supporting peptides, and a community of thousands who have navigated these exact challenges. The intersection of GLP-1 therapy, nutritional optimization, and peptide-supported hair health is complex, but with the right information and a systematic approach, you can pursue your weight loss goals without permanently sacrificing your hair.
The data from the peptides for hair growth complete guide reinforces that multiple evidence-based options exist for those who want to be proactive. The skin tightening peptides may also be relevant, since significant weight loss often affects skin elasticity alongside hair health, and some compounds like GHK-Cu benefit both. Similarly, the peptides for wrinkles article discusses copper peptide applications for facial skin that use similar mechanisms to those that support scalp and follicular health. Exploring the broader comparison of peptides versus SARMs helps contextualize where hair-supporting peptides fit within the broader landscape of research compounds. And for those using BPC-157 or TB-500 for recovery alongside their GLP-1 therapy, the BPC-157 and TB-500 stacking guide along with the BPC-157 versus TB-500 comparison provides detailed guidance on combining these compounds safely. The immune system peptides guide rounds out the picture for those looking at comprehensive health support during a period of significant physiological change, since immune function can fluctuate during aggressive weight loss and affect everything from recovery speed to inflammation levels around hair follicles.
The peptide transformation stories shared by community members often touch on the holistic nature of peptide-supported health journeys. Hair, skin, energy, body composition, and recovery are all interconnected. Addressing one in isolation rarely produces the best results. The most successful outcomes come from people who take a systems-level approach, optimizing nutrition, managing their GLP-1 dosing thoughtfully, supporting their body with evidence-based compounds, and giving the process the time it requires.
Frequently asked questions
Does GLP-1 hair loss happen to everyone who takes semaglutide or tirzepatide?
No. Clinical data shows that approximately 5% of tirzepatide users and a slightly higher percentage of semaglutide users experience noticeable hair loss. The majority of patients, roughly 95%, do not experience significant hair shedding. Risk factors include the speed and magnitude of weight loss, pre-existing nutritional deficiencies, age, sex (women are more commonly affected), and individual genetic susceptibility. Maintaining optimal nutrition and moderate weight loss pace significantly reduces your risk.
Will my hair grow back after GLP-1 related hair loss?
In the vast majority of cases, yes. GLP-1 related hair loss is predominantly telogen effluvium, which is a temporary and self-resolving condition. Once the triggering stressor stabilizes, meaning weight loss slows and nutritional status is optimized, hair follicles resume their normal growth cycle. Regrowth typically begins within three to six months after shedding peaks, with full recovery taking six to twelve additional months. The peptides for hair growth guide covers additional strategies to support and accelerate regrowth.
Should I stop taking my GLP-1 medication if I notice hair loss?
This decision should be made with your prescribing healthcare provider and depends on multiple factors, including how much weight you still need to lose, the severity of the hair loss, and whether correctable causes like nutritional deficiencies are contributing. Many patients can successfully manage hair loss while continuing their medication by optimizing nutrition, slowing the rate of weight loss through dose adjustment, and adding hair-supportive treatments. Stopping the medication abruptly can trigger its own set of issues, including potential weight regain and another round of metabolic disruption.
Can I prevent GLP-1 hair loss entirely?
Complete prevention is not guaranteed, but you can significantly reduce your risk and severity. The most effective prevention strategy combines adequate protein intake (1.0-1.2 grams per kilogram daily), comprehensive micronutrient supplementation from day one, gradual dose titration to moderate the rate of weight loss, maintaining a caloric floor, and baseline blood work to identify and correct pre-existing deficiencies. Proactive use of GHK-Cu for hair and other supportive compounds may provide additional protection.
Is GLP-1 hair loss the same as male or female pattern baldness?
Not usually. GLP-1 related hair loss is most commonly telogen effluvium, which causes diffuse thinning across the entire scalp rather than the patterned thinning seen in androgenic alopecia (male or female pattern baldness). However, GLP-1 therapy can unmask or worsen pre-existing androgenic alopecia through hormonal changes associated with fat loss, particularly in women over 40. A dermatologist can distinguish between the two types through examination and, if needed, scalp biopsy. The treatment approach differs significantly between them.
How do I know if my hair loss is from GLP-1 or something else?
The timing is the strongest clue. If hair shedding begins three to six months after starting GLP-1 therapy and is diffuse rather than patchy or patterned, GLP-1 related telogen effluvium is the most likely cause. Blood work should be checked to rule out thyroid dysfunction, iron deficiency, and other medical causes. If shedding occurs in well-defined patches, starts within weeks of starting medication, or is accompanied by scalp symptoms like pain or itching, see a dermatologist promptly, as these patterns suggest other diagnoses. Understanding overall safety and risk factors for any compounds you are taking helps differentiate between potential causes.
Does biotin help with GLP-1 hair loss?
Biotin supplementation may help if you are biotin-deficient, which is more likely during the reduced food intake associated with GLP-1 therapy. However, for people with adequate biotin levels, additional supplementation has limited evidence for improving hair loss. The most important caveat is that biotin can interfere with thyroid blood tests, causing falsely abnormal results. If you supplement biotin, stop it at least 48-72 hours before any thyroid labs to avoid misdiagnosis.
Are there GLP-1 medications that do not cause hair loss?
Older GLP-1 medications including liraglutide, dulaglutide, and exenatide have not shown statistically significant increases in hair loss reports. However, these medications also typically produce less dramatic weight loss, which is likely the key factor. The hair loss appears to be driven more by the magnitude and speed of weight loss than by the specific medication. If hair preservation is a primary concern and moderate weight loss is acceptable, discussing these alternatives with your prescriber is reasonable.
In case I do not see you, good afternoon, good evening, and good night. May your follicles stay active, your nutrients stay abundant, and your recovery stay steady.