Feb 26, 2026

Experienced researchers have noticed something about the latest wave of compounded semaglutide formulations. The vials no longer contain just semaglutide. Compounding pharmacies have started adding ingredients, and one addition keeps showing up over and over again. L-carnitine. It is in the marketing materials. It is in the product names. It is the reason some clinics charge a premium for their proprietary weight loss blends. But does adding L-carnitine to semaglutide actually do anything meaningful, or is this just another upsell dressed in scientific language?
That question matters more than most people realize. Because semaglutide fatigue, muscle loss, and metabolic slowdown are real concerns for anyone on a GLP-1 protocol. And L-carnitine, at least on paper, targets every single one of those problems. It shuttles fatty acids into mitochondria for energy production. It may help preserve lean tissue during caloric restriction. It could address the energy crashes that send people searching for answers at week three of their protocol.
This guide breaks down everything you need to know about the semaglutide and L-carnitine combination. What the research actually shows. What remains theoretical. How compounding pharmacies formulate these blends. What dosing protocols look like in practice. And whether this combination makes sense for your specific situation. SeekPeptides has analyzed the available evidence, the compounding formulations, and the real-world reports to give you the most complete picture available anywhere.
No hype. No overselling. Just the data, the mechanisms, and the practical details you need to make an informed decision.
What semaglutide with L-carnitine actually is
Semaglutide with L-carnitine is a compounded formulation that combines two substances into a single injectable solution. The semaglutide component is a GLP-1 receptor agonist that reduces appetite, slows gastric emptying, and improves blood sugar regulation. The L-carnitine component is a naturally occurring amino acid derivative that plays a critical role in fatty acid metabolism. When compounding pharmacies put them together, the goal is straightforward. Use semaglutide to create the caloric deficit and appetite suppression. Use L-carnitine to make sure the body burns fat efficiently during that deficit.
This is not an FDA-approved combination.
That point deserves emphasis because it changes the entire risk-benefit calculation. The FDA has approved semaglutide on its own for weight management under brand names like Wegovy and Ozempic. The FDA has recognized L-carnitine (specifically levocarnitine) as a dietary supplement with established safety data. But no drug product containing both substances together has received FDA approval. Every semaglutide-plus-L-carnitine formulation on the market comes from a compounding pharmacy, not a pharmaceutical manufacturer.
Compounding pharmacies create these formulations under different brand names. CarniSema is one of the more recognized names, combining semaglutide with L-carnitine in a single vial. Some pharmacies also produce CarniTide, which pairs L-carnitine with tirzepatide instead. Others simply label their products as semaglutide/levocarnitine compounds without branded names.
The formulations vary. Typical concentrations include semaglutide at 1 mg/mL or 2 mg/mL combined with L-carnitine at 100 mg/mL. Some pharmacies adjust these ratios based on prescriber preference. The semaglutide dosage follows the same escalation pattern as standalone semaglutide. The L-carnitine comes along for the ride at whatever concentration the pharmacy chose for that vial.
How L-carnitine works in the body
Understanding why anyone would add L-carnitine to semaglutide requires understanding what L-carnitine does on its own. And what it does is remarkably specific.
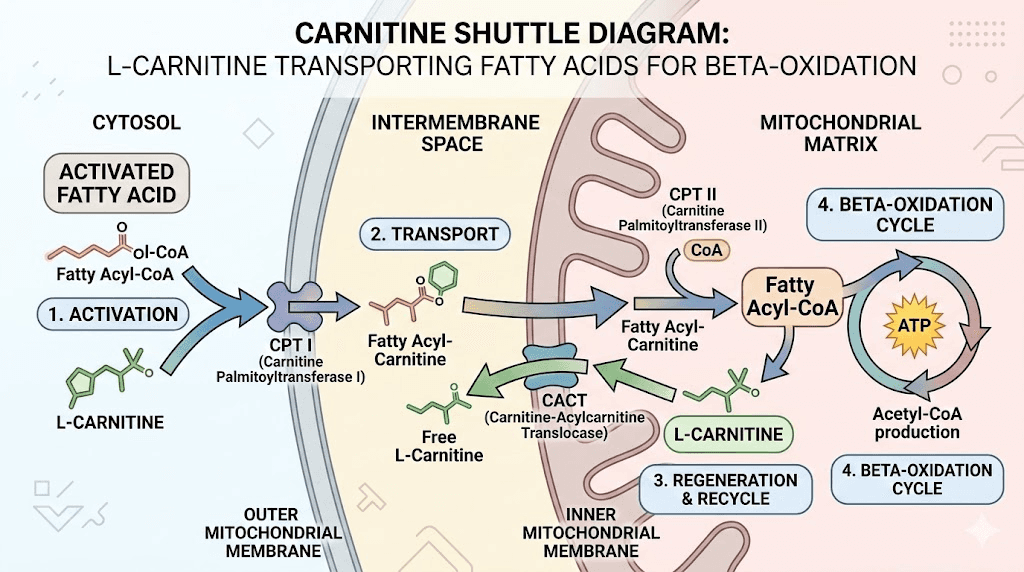
L-carnitine is an amino acid derivative synthesized primarily in the liver and kidneys from the amino acids lysine and methionine. Its primary biological function involves transporting long-chain fatty acids across the inner mitochondrial membrane. Without adequate carnitine, fatty acids cannot enter the mitochondria for beta-oxidation, which is the process that converts stored fat into usable energy.
Think of it as a shuttle system.
Fat molecules are too large to pass through the mitochondrial membrane on their own. They need a carrier. L-carnitine is that carrier. It binds to long-chain fatty acids, forms a compound called acylcarnitine, and transports the fatty acid through the membrane into the mitochondrial matrix where beta-oxidation can occur. Once inside, the fatty acid gets broken down into acetyl-CoA units that enter the citric acid cycle to produce ATP, the energy currency your cells run on.
The body produces about 20 mg of L-carnitine per day from endogenous synthesis. The rest comes from diet, primarily red meat and dairy products. Total body stores range from 20 to 25 grams in a healthy adult, with approximately 95% stored in skeletal and cardiac muscle tissue. Blood plasma levels typically range from 40 to 60 micromoles per liter.
Several forms of carnitine exist, and the distinctions matter for understanding supplement formulations:
L-carnitine (levocarnitine) is the biologically active form and the one used in most compounded semaglutide formulations
Acetyl-L-carnitine (ALCAR) is an acetylated form that crosses the blood-brain barrier more readily and is more commonly studied for cognitive applications
L-carnitine L-tartrate is a form often used in sports supplements due to faster absorption rates
Propionyl-L-carnitine shows particular benefit for circulation and is studied in peripheral vascular disease
When compounding pharmacies add L-carnitine to semaglutide, they use levocarnitine, the standard bioactive form. This is the same form that has the strongest evidence base for fat metabolism support and the longest safety track record in clinical use.
What happens when L-carnitine levels drop
During significant caloric restriction, which is exactly what happens on semaglutide, the body demands more from its fat oxidation pathways. More fat needs to be mobilized and burned for energy because food intake has decreased substantially. This increased demand can, theoretically, create a greater need for the carnitine shuttle system.
Some researchers have noted that obese individuals may have relatively lower carnitine levels compared to lean individuals, though the evidence on this point is mixed. A systematic review published in the Journal of the International Society of Sports Nutrition examined both the benefits and concerns of L-carnitine supplementation, noting that while supplementation can increase carnitine availability, the clinical significance varies widely depending on the individual and the context.
Carnitine deficiency is rare in healthy adults eating a varied diet. But subclinical insufficiency, where levels are technically adequate but not optimal for high metabolic demand, is harder to rule out. This is where the theoretical case for adding L-carnitine to a weight loss protocol begins to take shape.
Why clinics combine L-carnitine with semaglutide
The rationale for combining these two substances comes down to addressing specific limitations of GLP-1 therapy. Semaglutide is remarkably effective at producing weight loss. The STEP clinical trials demonstrated 14.9% average body weight reduction at 2.4 mg weekly over 68 weeks. But that weight loss is not entirely fat.
Here is the problem that drives the entire compounding trend.
Approximately 25 to 40% of the weight lost on GLP-1 medications comes from lean body mass, including muscle. This means that for every 10 pounds someone loses on semaglutide, roughly 3 to 4 pounds of that may be muscle tissue rather than fat. The American Diabetes Association has highlighted this as a significant concern, noting that preserving lean mass during GLP-1-induced weight loss remains a clinical challenge.
Muscle loss matters for several important reasons. Skeletal muscle is metabolically active tissue that burns calories at rest. Losing muscle reduces basal metabolic rate, which makes weight maintenance harder once the medication stops. Muscle loss also affects physical function, bone density support, insulin sensitivity, and long-term health outcomes, particularly in older adults and women who may already have lower baseline muscle mass.
L-carnitine enters the picture as a potential solution. The theory goes like this. If L-carnitine enhances fat oxidation by shuttling more fatty acids into mitochondria, the body may preferentially burn fat for energy rather than breaking down muscle protein. By improving the efficiency of fat metabolism, L-carnitine could shift the ratio of fat-to-lean-mass loss in a more favorable direction.
The energy deficit problem
Fatigue on semaglutide is one of the most commonly reported side effects. Many users experience significant energy drops, particularly during the first several weeks of treatment and during dose escalation phases. The causes are multifactorial, involving reduced caloric intake, changes in blood sugar regulation, and shifts in metabolic substrate utilization.
L-carnitine supplementation addresses this from a specific angle. If fatty acid transport into mitochondria is the rate-limiting step in fat oxidation during caloric restriction, then increasing carnitine availability could help the body access stored fat for energy more efficiently. More efficient fat burning means more available ATP. More ATP means more energy.
This is not just theoretical hand-waving. Users of combined semaglutide-L-carnitine formulations consistently report feeling more sustained energy during calorie restriction, improved stamina during physical activity, and enhanced overall metabolic support. Whether these reports reflect genuine pharmacological synergy or placebo effect remains an open question, but the pattern of anecdotal reports is consistent enough to warrant serious consideration.
The metabolic flexibility argument
Metabolic flexibility refers to the body's ability to switch between burning carbohydrates and burning fat depending on what fuel is available. People with good metabolic flexibility transition smoothly between fuel sources. People with poor metabolic flexibility, which includes many individuals carrying excess weight, struggle to efficiently oxidize fat even when glucose availability drops.
Semaglutide creates conditions where fat oxidation should increase. Caloric intake drops. Insulin levels improve. Stored fat should become the primary fuel source. But if the metabolic machinery for fat oxidation is suboptimal, which it often is in the population most likely to use semaglutide, then the theoretical benefit of enhanced carnitine availability becomes more compelling.
L-carnitine does not fix poor metabolic flexibility on its own. But it removes one potential bottleneck in the fat oxidation pathway. Combined with the appetite suppression and metabolic improvements from semaglutide, the combination could produce outcomes that neither substance achieves alone.
SeekPeptides members access detailed compound analysis guides that break down the evidence behind every popular semaglutide additive, including protocols and dosing information based on the latest research.
What the research actually shows
Separating marketing claims from evidence requires looking at what studies exist for each component individually and for the combination together. The research picture is informative but incomplete.
L-carnitine for weight loss: the meta-analysis data
A systematic review and meta-analysis published in Clinical Nutrition ESPEN analyzed 37 randomized controlled trials involving 2,292 participants. The findings showed that L-carnitine supplementation significantly decreased body weight with a weighted mean difference of negative 1.21 kg, reduced BMI by negative 0.24 kg per square meter, and decreased fat mass by negative 2.08 kg compared to placebo groups. The optimal dose identified was 2,000 mg per day for maximum weight reduction effect.
An earlier meta-analysis from Obesity Reviews, examining 9 studies with 911 participants, found that subjects receiving carnitine lost significantly more weight than control groups, with a mean difference of negative 1.33 kg. The weight loss was statistically significant but modest in absolute terms.
These numbers deserve context. A 1 to 2 kg additional weight loss over study periods ranging from 4 to 52 weeks is meaningful but not transformative on its own. L-carnitine is not a powerful weight loss agent in isolation. Its value in the context of semaglutide therapy lies not in dramatic additional weight loss, but in potentially improving the quality and composition of that weight loss.
L-carnitine for body composition
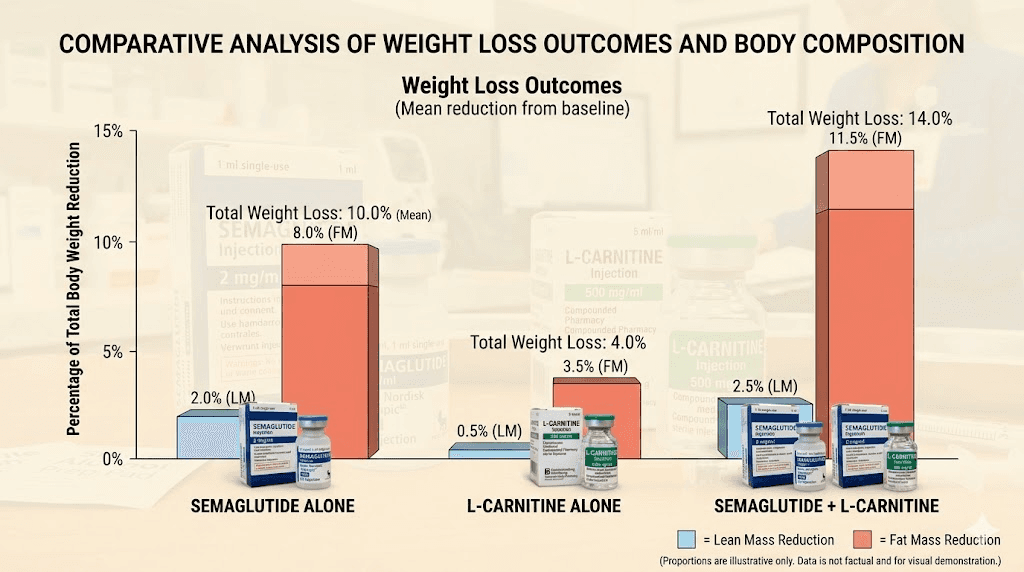
The more interesting finding from the meta-analysis data is the fat mass reduction of 2.08 kg compared to placebo. When total weight loss is modest (1.21 kg) but fat mass loss is larger (2.08 kg), the math suggests that L-carnitine supplementation may actually support lean mass preservation while preferentially reducing fat stores. This is exactly the outcome that clinicians hope to achieve by combining it with semaglutide weight loss protocols.
A 2024 case series published in the Journal of Clinical Endocrinology reported that patients receiving combination therapy of semaglutide with L-carnitine showed 18% greater fat mass reduction compared to GLP-1 monotherapy, with improved energy scores on validated fatigue assessments. While case series carry less evidentiary weight than randomized controlled trials, this preliminary data aligns with the mechanistic rationale for the combination.
Semaglutide and lean mass: the baseline problem
Understanding the magnitude of the lean mass problem helps contextualize why additives like L-carnitine attract interest. Research from Mass General published data showing that approximately 40% of weight lost from semaglutide comes from lean mass. The STEP trials confirmed this pattern. Regeneron Pharmaceuticals has invested in developing bimagrumab specifically to address this issue, with interim results from the COURAGE trial showing that combining bimagrumab with semaglutide improved the quality of weight loss by preserving lean mass.
The Endocrine Society presented data at ENDO 2025 demonstrating that consuming more protein may protect patients taking anti-obesity drugs from muscle loss. Combined with exercise, high-protein diets showed the greatest benefit for lean mass preservation. This research creates a broader context in which L-carnitine supplementation represents just one piece of a comprehensive approach to maintaining muscle during semaglutide-induced weight loss.
What we do not know
No large-scale, randomized, double-blind, placebo-controlled trial has directly compared semaglutide alone versus semaglutide plus L-carnitine. The 2024 case series is promising but small. The meta-analyses on L-carnitine were conducted in general weight loss populations, not specifically in GLP-1 users. The mechanistic rationale is sound, but the clinical evidence for the specific combination remains preliminary.
This is an important distinction that every researcher should understand. The evidence supports using L-carnitine for modest weight loss and fat mass reduction. The evidence supports semaglutide for substantial weight loss. The theory behind combining them is scientifically reasonable. But the evidence for the combination itself is still building.
Dosing protocols for semaglutide with L-carnitine
Dosing for the combined formulation follows established patterns for each individual component. The semaglutide component uses the standard escalation schedule that applies to all semaglutide dosing protocols. The L-carnitine component is added at a fixed concentration within the vial.
Standard semaglutide escalation in compounded formulations
The semaglutide component follows the familiar titration pattern:
Weeks 1 through 4: 0.25 mg subcutaneously once weekly
Weeks 5 through 8: 0.5 mg subcutaneously once weekly
Weeks 9 through 12: 1.0 mg subcutaneously once weekly
Weeks 13 through 16: 1.7 mg subcutaneously once weekly (if tolerated)
Week 17 and beyond: 2.4 mg subcutaneously once weekly (maximum maintenance dose)
This escalation schedule exists for good reason. Semaglutide causes gastrointestinal side effects, primarily nausea and bloating, that improve as the body adapts to each dose level. Rushing the titration causes unnecessary discomfort and higher dropout rates. The same principle applies when L-carnitine is present in the formulation.
When using compounded vials with concentrations of 1 mg/mL semaglutide combined with 100 mg/mL levocarnitine, the injection volume determines both doses simultaneously. At the starting dose of 0.25 mL (delivering 0.25 mg semaglutide), the patient also receives 25 mg of L-carnitine. At the maximum dose of 2.4 mL (delivering 2.4 mg semaglutide), the patient receives 240 mg of L-carnitine per injection.
The L-carnitine dosing question
Here is where the formulation math gets interesting. The meta-analysis data identified 2,000 mg per day as the optimal L-carnitine dose for weight management. But most compounded semaglutide/L-carnitine formulations deliver only 25 to 240 mg per weekly injection, depending on the semaglutide dose being administered. That is substantially below the evidence-based optimal dose.
Some clinics address this gap by recommending additional oral L-carnitine supplementation alongside the compounded injection. The oral route can deliver the 2,000 mg daily dose that the research supports for maximum fat oxidation benefit. The injectable L-carnitine in the compounded vial then serves as a supplementary dose with potentially better bioavailability due to bypassing first-pass metabolism.
Others use higher concentration formulations. Some compounding pharmacies offer semaglutide/L-carnitine vials with 200 mg/mL or even 500 mg/mL L-carnitine concentrations. These deliver more meaningful L-carnitine doses per injection but may require larger injection volumes.
Practical dosing protocol
Based on the available evidence, a reasonable protocol for combining semaglutide with L-carnitine looks like this:
The injection component:
Use the compounded semaglutide/L-carnitine formulation according to the standard semaglutide titration schedule
Inject subcutaneously once weekly at the standard injection sites (abdomen, thigh, or upper arm)
Follow the same injection technique as standalone semaglutide
The oral supplement component (optional but recommended for full dosing):
500 to 2,000 mg L-carnitine or acetyl-L-carnitine daily
Taken with meals for better absorption
Start at 500 mg daily and increase as tolerated
Morning dosing is preferred as L-carnitine may cause restlessness if taken late in the day
Monitoring schedule:
Weight and body composition assessment every 4 to 6 weeks
Lipid panel and HbA1c every 3 months
Liver function tests at baseline and 6 months
Energy and fatigue assessment at each check-in
Use the semaglutide dosage calculator to determine your exact semaglutide dose, then discuss L-carnitine addition with your prescribing provider. The peptide reconstitution calculator can help if you are working with lyophilized formulations that require mixing.
How to store semaglutide with L-carnitine
Storage requirements for the combined formulation are essentially the same as standalone semaglutide storage. The semaglutide component is the stability-limiting factor in the formulation. L-carnitine is quite stable and does not impose additional storage constraints.
Refrigerate between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). Keep the vial in its original box to protect from light. Do not freeze. Once reconstituted or opened, most compounding pharmacies assign a beyond-use date of 28 to 90 days, depending on the specific formulation and the pharmacy standards.
If your vial gets left out of the refrigerator, the same rules apply as with standard compounded semaglutide. Brief excursions at room temperature (up to 86 degrees Fahrenheit or 30 degrees Celsius) for less than 14 days are generally tolerable. Extended exposure to heat degrades the semaglutide component. The L-carnitine component is more heat stable, so the semaglutide dictates the storage protocol. See our guide on what to do if semaglutide is left out overnight for more details on handling temperature excursions.
For travel situations, the same cold chain principles apply. Keep the vial in an insulated cooling case with ice packs. Do not expose to direct sunlight or extreme temperatures. Our semaglutide travel guide covers everything you need to know about maintaining proper storage during trips.
Side effects and safety considerations
The side effect profile of the combined formulation includes everything associated with semaglutide on its own, plus a few considerations specific to L-carnitine supplementation.
Semaglutide side effects (the dominant factor)
The gastrointestinal side effects of semaglutide remain the primary concern in the combination. These include nausea (which affects roughly 40 to 50% of users during titration), constipation, dizziness, bloating, and occasional sleep disturbance. These typically improve with time as the body adjusts to each dose level.
The first week on semaglutide is often the hardest. Most side effects peak during dose escalation periods and fade over the following two to three weeks. The same pattern applies when using the L-carnitine combination. Adding L-carnitine does not appear to worsen semaglutide side effects based on available reports, and some users report that the L-carnitine component actually helps with GLP-1-related fatigue.
L-carnitine-specific considerations
L-carnitine supplementation at doses up to 2,000 mg per day has an established safety profile with several decades of clinical use. Common side effects are mild and include occasional nausea or stomach discomfort, a fishy body odor at higher doses (caused by trimethylamine production), diarrhea at very high doses, and increased appetite in some individuals.
The more significant safety consideration involves TMAO (trimethylamine N-oxide). When gut bacteria metabolize unabsorbed L-carnitine, they produce trimethylamine, which the liver then converts to TMAO. Elevated TMAO levels have been associated with increased cardiovascular disease risk in some observational studies. However, a systematic review published in the Journal of the International Society of Sports Nutrition noted that while L-carnitine supplementation did increase fasting plasma TMAO levels, higher TMAO was not associated with inflammatory or oxidative stress markers in supplementation studies.
This TMAO concern is worth understanding but should not be overstated. The association between TMAO and cardiovascular risk comes primarily from observational studies in people eating high amounts of red meat. Whether supplemental L-carnitine produces the same risk profile is unclear. People who eat plant-based diets and then supplement with L-carnitine may actually produce less TMAO because their gut microbiome has fewer TMAO-producing bacteria.
Drug interactions
L-carnitine has relatively few drug interactions. It may enhance the effects of blood-thinning medications like warfarin. It may interact with thyroid medications in some individuals. And it can theoretically interact with certain antibiotics that affect carnitine transport.
Semaglutide has its own interaction profile, primarily through delayed gastric emptying which can affect the absorption of other oral medications. If you are taking other medications alongside semaglutide, discuss the L-carnitine addition with your prescriber. The combination of semaglutide, L-carnitine, and other substances like berberine requires careful medical oversight.
Who should avoid this combination
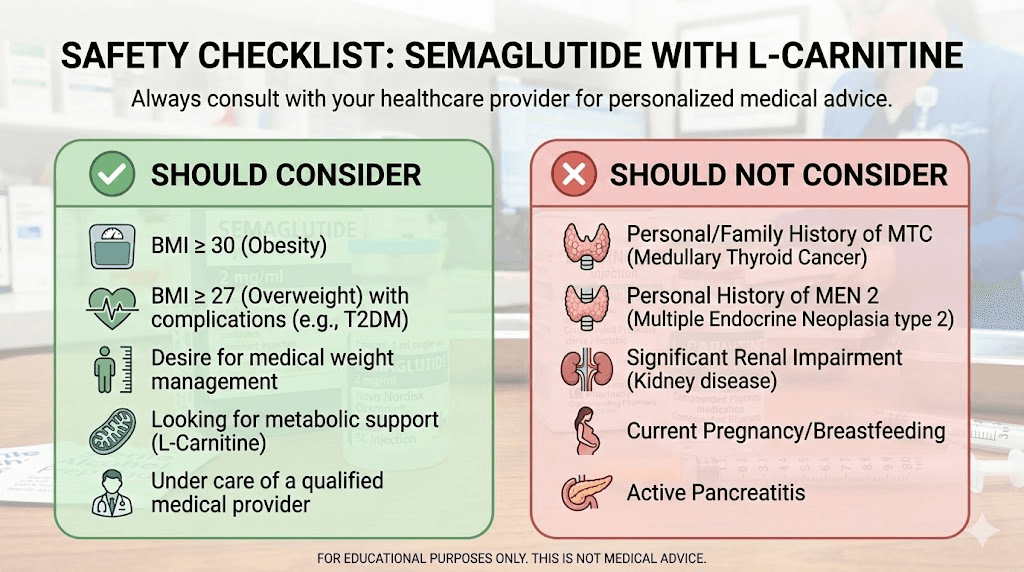
Certain populations should exercise extra caution or avoid the semaglutide/L-carnitine combination entirely:
Individuals with a history of seizure disorders (high-dose L-carnitine may lower seizure threshold in susceptible individuals)
People with hypothyroidism on thyroid replacement therapy (L-carnitine may affect thyroid hormone levels)
Individuals with kidney disease (impaired carnitine clearance may lead to accumulation)
Pregnant or breastfeeding individuals (semaglutide is contraindicated)
Anyone with a known allergy to either component
L-carnitine compared to other semaglutide additives
L-carnitine is not the only substance that compounding pharmacies add to semaglutide. Understanding how it compares to other common additives helps you evaluate whether L-carnitine is the right choice for your protocol, or whether a different additive better matches your needs.
Semaglutide with B12 (cyanocobalamin or methylcobalamin)
Semaglutide with B12 is the most common compounded formulation. Vitamin B12 supports energy metabolism, red blood cell production, and neurological function. The rationale for adding B12 is that reduced food intake on semaglutide can lead to lower B12 intake, particularly in people who already have marginal B12 status. Methylcobalamin, the active form of B12, is preferred by many compounding pharmacies over cyanocobalamin.
The evidence for B12 supplementation during GLP-1 therapy is reasonable. B12 deficiency can cause fatigue, numbness, and cognitive issues, all of which overlap with semaglutide side effects. But B12 does not address fat oxidation or lean mass preservation the way L-carnitine does. The two additives serve different purposes.
Semaglutide with glycine
Semaglutide with glycine is another popular combination. Glycine is an amino acid with anti-inflammatory properties, roles in collagen synthesis, and potential benefits for sleep quality. Some triple-compound formulations include semaglutide, glycine, and B12 together.
Glycine does not directly address fat oxidation or lean mass preservation in the way L-carnitine does. Its benefits are more general, supporting overall metabolic health, antioxidant production (through glutathione synthesis), and potentially reducing inflammation during weight loss. For someone whose primary concern is energy and fat metabolism, L-carnitine is the more targeted choice. For someone dealing with inflammation, joint discomfort, or sleep issues on semaglutide, glycine may be more relevant.
Semaglutide with NAD+
NAD+ (nicotinamide adenine dinucleotide) is gaining attention as a semaglutide additive. NAD+ is a coenzyme involved in cellular energy production, DNA repair, and metabolic regulation. It supports mitochondrial function from a different angle than L-carnitine. While L-carnitine delivers the fuel (fatty acids) to mitochondria, NAD+ helps the mitochondria actually process that fuel efficiently.
The combination of both L-carnitine and NAD+ with semaglutide represents a comprehensive approach to mitochondrial support during weight loss, though no clinical trials have evaluated this triple combination.
Comparison summary
Additive | Primary benefit | Fat metabolism | Muscle preservation | Energy support | Evidence strength |
|---|---|---|---|---|---|
L-carnitine | Fat oxidation, lean mass | Strong | Moderate | Moderate | Meta-analyses exist |
B12 | Energy, nerve function | Minimal | Minimal | Strong (if deficient) | Well-established |
Glycine | Anti-inflammatory, sleep | Minimal | Minimal | Indirect | Emerging |
NAD+ | Mitochondrial function | Moderate | Possible | Strong | Preliminary |
Niacinamide | Skin, metabolism | Minimal | Minimal | Indirect | Limited for weight loss |
For detailed guides on each additive, explore our resources on tirzepatide with glycine, tirzepatide with niacinamide, tirzepatide with B6, and tirzepatide with B12, which cover the same additives in the context of tirzepatide therapy.
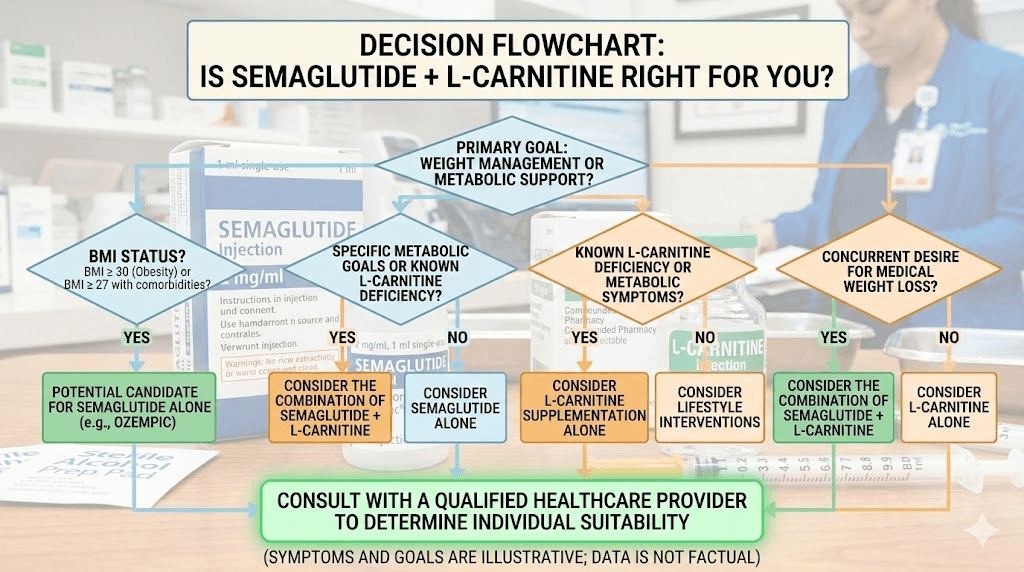
Who benefits most from semaglutide with L-carnitine
Not everyone on semaglutide needs L-carnitine. The combination makes the most sense for specific populations with specific concerns.
People experiencing significant fatigue
If semaglutide is draining your energy despite proper hydration, adequate protein intake, and appropriate dose titration, L-carnitine may help. By supporting more efficient fat oxidation, L-carnitine provides an alternative energy pathway that can partially compensate for reduced caloric intake. This is particularly relevant for people who were previously sedentary and have poor baseline metabolic flexibility.
People concerned about muscle loss
Anyone prioritizing body composition over scale weight should consider the L-carnitine addition. If your goal is to lose fat while preserving as much muscle as possible, L-carnitine in combination with high-protein nutrition and resistance training represents a comprehensive approach. The meta-analysis data showing greater fat mass reduction relative to total weight loss supports this application.
People with poor baseline fat metabolism
Some individuals simply do not oxidize fat efficiently. Markers of poor fat metabolism include heavy reliance on carbohydrates for energy, difficulty fasting for even short periods, energy crashes between meals, and a history of failed diets despite significant caloric restriction. For these individuals, L-carnitine removes a potential bottleneck in the fat-burning pathway.
People on extended protocols
The longer someone uses semaglutide, the more cumulative lean mass loss becomes. For people on extended semaglutide protocols lasting six months or longer, the body composition impact adds up. L-carnitine supplementation throughout the protocol duration may help limit this cumulative effect.
Active individuals and athletes
People who exercise regularly while on semaglutide have higher metabolic demands and greater potential to benefit from enhanced fat oxidation. L-carnitine supplementation has been studied extensively in the athletic performance context, with some studies showing improved fat oxidation during exercise and modest improvements in recovery. For someone combining semaglutide with a serious exercise program, L-carnitine fits naturally into the protocol.
Who does NOT need L-carnitine with semaglutide
People who eat red meat regularly (the richest dietary source of L-carnitine) may already have adequate carnitine levels and derive minimal additional benefit from supplementation. People who respond well to semaglutide alone with good energy levels and satisfactory body composition changes do not need to add complexity to their protocol. And people primarily seeking appetite suppression without specific concerns about body composition or energy may find that standard semaglutide appetite suppression is sufficient on its own.
Practical considerations for getting started
If you have decided that semaglutide with L-carnitine is worth trying, several practical details deserve attention before you begin.
Finding a compounding pharmacy
Not all compounding pharmacies are equal. Look for pharmacies that hold PCAB (Pharmacy Compounding Accreditation Board) accreditation, provide certificates of analysis for their products, use USP-grade ingredients, and have established track records with GLP-1 formulations. Many of the pharmacies reviewed in our vendor guides, including Empower Pharmacy, Olympia Pharmacy, and Elevate Health, offer semaglutide formulations with various additives.
Understanding what you are paying for
Compounded semaglutide/L-carnitine typically costs more than compounded semaglutide alone. The price premium ranges from modest (10 to 20% more) to significant (50% or more) depending on the pharmacy and the specific formulation. Consider whether you could achieve similar results by purchasing standard compounded semaglutide and taking oral L-carnitine supplements separately. The cost savings of the DIY approach can be substantial, though you sacrifice the convenience of a single injection.
Getting the prescription
Semaglutide requires a prescription regardless of the formulation. The L-carnitine component can be obtained over the counter as a supplement, but the combined injectable formulation requires a prescriber order to a compounding pharmacy. Many telehealth platforms now offer compounded semaglutide with L-carnitine as an option. When speaking with your provider, ask specifically about the L-carnitine concentration in the formulation and whether they recommend additional oral supplementation.
Setting realistic expectations
Adding L-carnitine to semaglutide will not double your weight loss. It will not eliminate all side effects. It will not turn a mediocre protocol into an exceptional one. What it may do is improve the quality of your weight loss by shifting more of it toward fat, provide modest energy support during caloric restriction, and support better body composition outcomes when combined with exercise and appropriate nutrition.
The people who benefit most are those who layer L-carnitine on top of an already solid foundation. That foundation includes proper semaglutide titration, adequate protein intake (aim for 1.0 to 1.2 grams per pound of lean body mass), regular resistance training at least 2 to 3 times per week, proper hydration, and consistent injection timing.
The compounding pharmacy landscape
The availability of semaglutide/L-carnitine formulations has expanded rapidly as compounding pharmacies compete for market share in the GLP-1 space. Understanding the current landscape helps you navigate your options.
Branded formulations
Several compounding pharmacies have created branded names for their L-carnitine GLP-1 combinations. CarniSema combines semaglutide with L-carnitine. CarniTide combines tirzepatide with L-carnitine. These branded names are pharmacy-created marketing terms, not standardized pharmaceutical products. The actual formulations can vary between pharmacies using the same brand name.
Quality considerations
When evaluating compounding pharmacies for L-carnitine formulations, focus on several quality markers. The pharmacy should use pharmaceutical-grade levocarnitine, not dietary supplement-grade material. The semaglutide should come from verified sources that meet USP standards. The final formulation should undergo sterility testing and potency verification. And the pharmacy should provide clear beyond-use dating based on stability data, not guesswork.
The FDA has issued warnings about compounded semaglutide products in general, noting dosing errors and quality concerns. These warnings apply to all compounded semaglutide products, not specifically to L-carnitine combinations, but they underscore the importance of choosing a reputable pharmacy. The same vigilance you would apply when buying grey market peptides should be applied to compounded pharmaceutical formulations.
The alternative approach: separate dosing
Some researchers and clinicians prefer keeping the components separate rather than relying on compounded combinations. This approach offers several advantages:
Dose control: You can adjust L-carnitine dosing independently of semaglutide dosing
Cost flexibility: Oral L-carnitine supplements are inexpensive, often costing less than $20 per month at 2,000 mg daily
Evidence-based dosing: You can take the 2,000 mg daily dose supported by meta-analysis data, rather than the lower dose dictated by the compounded vial concentration
Fewer supply chain risks: If the compounding pharmacy runs out of the combination, you are not left without either component
The disadvantage of separate dosing is lower compliance. One injection is easier to remember than one injection plus daily oral supplements. And injectable L-carnitine may have better bioavailability than oral forms, particularly in individuals with gut absorption issues (which can be affected by semaglutide-induced changes to gastric emptying).
Combining L-carnitine with exercise on semaglutide
The synergy between L-carnitine and exercise during semaglutide therapy deserves specific attention because this is where the combination may produce its most meaningful benefits.
Why exercise matters more than the supplement
Let us be direct about this. No supplement, including L-carnitine, replaces exercise for lean mass preservation during GLP-1-induced weight loss. The data is clear. Patients who engage in regular resistance exercise while on semaglutide or tirzepatide preserve significantly more muscle mass than those who remain sedentary. L-carnitine is an add-on to this foundation, not a substitute for it.
How L-carnitine enhances exercise outcomes
During aerobic exercise, L-carnitine supplementation may increase the proportion of energy derived from fat oxidation versus glycogen. This means more fat burned per exercise session, glycogen sparing for sustained performance, potentially faster recovery between sessions, and less post-exercise fatigue.
During resistance training, L-carnitine has been studied for its effects on recovery and muscle damage markers. Some studies show reduced muscle damage indicators (creatine kinase, lactate dehydrogenase) following intense exercise in supplemented individuals. This could translate to better training consistency and volume over time, which is the primary driver of muscle preservation.
A practical exercise protocol
For someone on semaglutide with L-carnitine supplementation, a balanced exercise approach includes:
Resistance training (3 times per week): Focus on compound movements (squats, deadlifts, presses, rows) that work large muscle groups. These movements provide the strongest stimulus for muscle preservation during caloric deficit. Aim for 3 to 4 sets of 6 to 12 repetitions per exercise.
Moderate cardio (2 to 3 times per week): Walking, cycling, or swimming at an intensity where you can maintain conversation. This supports fat oxidation and cardiovascular health without excessive energy expenditure that could further compromise lean mass.
Recovery: Adequate sleep (7 to 9 hours), proper hydration, and strategic protein timing (20 to 30 grams within 2 hours of resistance training).
Taking 1,000 to 2,000 mg of oral L-carnitine approximately 60 to 90 minutes before exercise is a common protocol based on the pharmacokinetics of oral carnitine absorption. The injectable L-carnitine from the weekly semaglutide shot contributes to overall carnitine stores but does not replace pre-exercise timing for acute exercise benefits.
For more on optimizing nutrition during GLP-1 therapy, our guides on foods to eat on semaglutide and semaglutide diet plans provide comprehensive nutritional frameworks.
Common mistakes when using semaglutide with L-carnitine
Knowing what not to do saves as much trouble as knowing what to do. These are the most frequent mistakes people make with this combination.
Relying on L-carnitine instead of fixing the fundamentals
If your protein intake is below 0.7 grams per pound of body weight, no amount of L-carnitine will prevent muscle loss. If you are completely sedentary, L-carnitine will not preserve lean mass. If your semaglutide dose is wrong or your titration is too aggressive, L-carnitine will not fix the side effects. Get the basics right first. Then consider L-carnitine as an optimization layer.
Expecting dramatic results from the injected dose alone
As discussed above, the L-carnitine dose in most compounded semaglutide vials is well below the 2,000 mg daily dose supported by research. People who think the injection provides adequate L-carnitine dosing may be getting an expensive placebo effect. If you are serious about L-carnitine benefits, supplement orally to reach evidence-based doses.
Ignoring the TMAO concern in high-risk populations
For most healthy adults, TMAO production from L-carnitine supplementation is not a significant risk. But for individuals with existing cardiovascular disease, elevated cholesterol, or multiple cardiac risk factors, the TMAO question deserves discussion with a cardiologist. This is not a reason to avoid L-carnitine universally, but it is a reason for certain populations to approach supplementation with more caution.
Choosing a pharmacy based on price alone
The cheapest compounded semaglutide/L-carnitine is not necessarily the best value. Quality testing, sterility assurance, and accurate potency matter enormously with injectable products. An underdosed or contaminated product is worse than no product at all. Spend the time to research pharmacy credentials rather than defaulting to the lowest price point. Our vendor guides for Direct Meds, BPI Labs, and other providers offer quality comparison information.
Titrating too quickly
Some people assume that because L-carnitine supports energy, they can tolerate faster semaglutide dose escalation. This is incorrect. The gastrointestinal side effects of semaglutide are driven by the GLP-1 receptor activation, not by energy availability. Rushing through dose escalation leads to more nausea, vomiting, and potential dropout regardless of L-carnitine status.
Semaglutide with L-carnitine versus tirzepatide with L-carnitine
Since both semaglutide and tirzepatide are available in compounded formulations with L-carnitine, you may wonder which base GLP-1 to choose.
Tirzepatide is a dual GIP/GLP-1 receptor agonist that has shown greater weight loss in head-to-head comparisons with semaglutide. The SURMOUNT-1 trial demonstrated up to 22.5% total body weight reduction at the 15 mg dose. Some preliminary data suggests that tirzepatide may produce a more favorable body composition profile than semaglutide, with relatively more fat loss and less lean mass loss, though this has not been definitively established.
If tirzepatide already preserves lean mass somewhat better than semaglutide, the marginal benefit of adding L-carnitine may be smaller with tirzepatide than with semaglutide. Conversely, semaglutide users may have more to gain from L-carnitine supplementation precisely because the lean mass loss concern is relatively greater.
Both combinations are available from compounding pharmacies. Tirzepatide compound formulations come in a wider variety of additive combinations. The choice between semaglutide and tirzepatide should be based on your individual response, side effect profile, and prescriber recommendation, not primarily on which base GLP-1 pairs better with L-carnitine.
For a detailed comparison of side effect profiles, see our guide on semaglutide vs tirzepatide side effects. And for those considering switching between the two, our conversion chart provides equivalent dosing guidance.
What to track when using this combination
Measuring the right things determines whether L-carnitine is actually adding value to your protocol or just adding cost.
Body composition, not just weight
A bathroom scale tells you nothing about whether L-carnitine is working. You need body composition data. DEXA scans provide the gold standard for measuring fat mass versus lean mass. BIA (bioelectrical impedance analysis) scales offer a less accurate but more accessible alternative for tracking trends over time. Measure body composition every 4 to 6 weeks and track the ratio of fat loss to lean loss. If L-carnitine is working, you should see a higher proportion of fat loss relative to total weight loss compared to what published data shows for semaglutide alone.
Energy levels
Track your subjective energy on a consistent scale. Rate your energy level on a 1 to 10 scale at the same time each day, ideally in the afternoon when semaglutide-related fatigue tends to be most prominent. After 4 to 6 weeks on the combination, compare your average energy scores to your baseline before adding L-carnitine. If energy has not improved, the L-carnitine component may not be providing meaningful benefit for you specifically.
Exercise performance
If you exercise regularly, track your training metrics. Can you maintain the same weights and repetitions as before starting semaglutide? Are you recovering well between sessions? Can you sustain longer duration cardio without excessive fatigue? These are practical indicators of whether L-carnitine is supporting your physical performance during caloric restriction.
Blood markers
Lipid panels every 3 months can reveal whether fat metabolism is shifting. Improvements in triglyceride levels may indicate enhanced fatty acid oxidation. HbA1c provides insight into glucose regulation. Complete metabolic panels can detect any liver or kidney function changes. If TMAO is a concern for your risk profile, some labs now offer TMAO testing as well.
The bottom line on semaglutide with L-carnitine
Semaglutide with L-carnitine is a scientifically reasonable combination with preliminary supporting evidence but without definitive clinical proof of superiority over semaglutide alone. The mechanistic rationale is strong. L-carnitine enhances fat transport into mitochondria. Semaglutide creates the caloric deficit that demands increased fat oxidation. Together, they should theoretically produce better body composition outcomes than semaglutide alone.
The meta-analysis data supports L-carnitine for modest additional fat loss and possibly better lean mass preservation. The case series data on the specific combination shows promising early results. But we are still waiting for the kind of large-scale randomized trials that would make this recommendation ironclad.
For most people on semaglutide, the priority list should look like this. First, optimize protein intake. Second, implement resistance training. Third, ensure proper semaglutide titration and adherence. Fourth, consider L-carnitine supplementation, either through a compounded formulation or as a separate oral supplement at 2,000 mg daily. This ordering reflects the strength of evidence for each intervention.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based compound guides, detailed protocol builders, and a community of thousands who have navigated these exact questions about GLP-1 medications and their formulation options.
Frequently asked questions
Can I add L-carnitine to my existing semaglutide prescription?
If you are already using compounded semaglutide, ask your prescriber to switch your formulation to one that includes L-carnitine. Alternatively, you can take oral L-carnitine supplements (500 to 2,000 mg daily) alongside your current semaglutide injection. The peptide calculator can help determine your current semaglutide dose. You do not need a new prescription for oral L-carnitine supplements, as they are available over the counter.
Does semaglutide with L-carnitine cause more nausea?
Based on available reports and clinical observations, adding L-carnitine does not increase nausea compared to semaglutide alone. The gastrointestinal side effects of the combination are driven primarily by the semaglutide component. Some users actually report slightly less nausea, possibly because improved energy metabolism reduces the malaise associated with caloric restriction, though this is anecdotal.
How long does it take for L-carnitine to work with semaglutide?
L-carnitine supplementation takes approximately 2 to 4 weeks to significantly increase tissue carnitine stores. Energy improvements may be noticed within the first 1 to 2 weeks. Body composition differences typically become measurable after 4 to 8 weeks of consistent supplementation at adequate doses. This timeline aligns roughly with the semaglutide response timeline, making it difficult to attribute specific improvements to the L-carnitine component versus the natural adaptation to semaglutide.
Is injectable L-carnitine better than oral?
Injectable L-carnitine bypasses first-pass metabolism in the gut and liver, resulting in higher bioavailability. Oral L-carnitine has approximately 14 to 18% bioavailability, meaning only a fraction of the ingested dose reaches systemic circulation. However, oral L-carnitine at adequate doses (2,000 mg daily) still achieves meaningful increases in tissue carnitine levels. The injectable form in compounded semaglutide provides a supplemental dose with better absorption, but the total dose per injection is typically too low to serve as the sole source of supplemental L-carnitine.
Can I take acetyl-L-carnitine instead of L-carnitine with semaglutide?
Acetyl-L-carnitine (ALCAR) is converted to L-carnitine in the body and supports the same fatty acid transport function. ALCAR has the additional benefit of crossing the blood-brain barrier, which may provide cognitive and mood support. For someone experiencing semaglutide brain fog alongside physical fatigue, ALCAR may be a preferred oral supplement. The dosing is similar, with 1,000 to 2,000 mg daily being the commonly studied range.
Does L-carnitine help with the semaglutide plateau?
Weight loss plateaus on semaglutide, which we cover in detail in our semaglutide plateau guide, occur for complex metabolic reasons. L-carnitine may provide modest help by supporting continued fat oxidation during adaptive thermogenesis, but it is not a reliable solution for breaking through plateaus. Dose adjustment, dietary changes, and exercise modifications are more effective plateau-breaking strategies.
Should I stop L-carnitine when I stop semaglutide?
There is no medical requirement to stop L-carnitine when discontinuing semaglutide. Many people continue L-carnitine supplementation during the weight maintenance phase to support ongoing fat metabolism and energy production. L-carnitine does not cause dependence or withdrawal effects. If you are tapering off semaglutide, our guide on semaglutide withdrawal covers what to expect.
Is semaglutide with L-carnitine safe for people with diabetes?
Semaglutide is FDA-approved for type 2 diabetes management (as Ozempic). L-carnitine supplementation has been studied in diabetic populations, with a meta-analysis of randomized controlled trials showing improvements in glycemic control, body weight, and cardiovascular risk factors. The combination may be particularly relevant for people with diabetes who want to optimize both weight loss and metabolic health. However, blood sugar monitoring should be more frequent when starting the combination, and medication adjustments (particularly for insulin or sulfonylureas) may be necessary. Always work with an endocrinologist or diabetes specialist.
External resources
L-carnitine supplementation meta-analysis: 37 randomized controlled trials (PubMed)
Systematic review: benefits and concerns of L-carnitine supplementation (PMC)
American Diabetes Association: GLP-1 therapies and muscle preservation
In case I do not see you, good afternoon, good evening, and good night. May your fat oxidation stay efficient, your lean mass stay preserved, and your protocols stay evidence-based.