Feb 24, 2026

Tired of reading about tirzepatide formulations that promise comfort but deliver confusion? You are not alone. The combination of tirzepatide with vitamin B6 has become one of the most talked about compound formulations in the GLP-1 space, and for good reason. Nausea derails more tirzepatide weight loss journeys than almost any other factor. It forces dose reductions. It causes missed injections. It makes people quit entirely, sometimes just weeks before the results would have started showing.
Vitamin B6, also known as pyridoxine, has been used for decades to combat nausea in settings ranging from pregnancy to chemotherapy. When compounding pharmacies began adding it directly to compounded tirzepatide formulations, the idea was simple: deliver the anti-nausea support at the exact same time as the peptide that causes it. No separate supplements to remember. No timing guesswork. Just one injection that handles both the weight loss mechanism and the gastrointestinal fallout.
This guide covers everything about the tirzepatide with B6 combination, from the science behind pyridoxine and nausea relief to practical dosing considerations, how it compares to tirzepatide with B12 and tirzepatide with glycine, storage protocols, side effect management, and the regulatory landscape that shapes availability. Whether you are researching this compound for the first time or comparing additive options before starting a protocol, you will find specific answers here, not vague summaries.
What is tirzepatide with B6?
Tirzepatide with B6 is a compounded injectable formulation that combines two active ingredients into a single subcutaneous injection. The first is tirzepatide, a dual GIP/GLP-1 receptor agonist that targets both glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1 pathways simultaneously. The second is pyridoxine hydrochloride, the pharmaceutical form of vitamin B6.
This is not a brand-name product. It is a custom preparation made by licensed compounding pharmacies that combine these two ingredients based on a prescriber order. The FDA-approved versions of tirzepatide, sold under the brand names Mounjaro for type 2 diabetes and Zepbound for weight management, contain tirzepatide alone without any vitamin additives.
Compounding pharmacies create these combination formulations for a specific reason. By including pyridoxine directly in the injection, the anti-nausea agent arrives in the body at exactly the same time as the peptide. This proactive approach differs from taking a separate B6 supplement orally, which requires digestion, absorption through the gut, and conversion before it can exert its effects. The injectable route bypasses all of that.
The typical compounded formulation uses pyridoxine at a concentration of 50 mg/mL. Even at the smallest injection volumes, this delivers approximately 5 mg of vitamin B6, which is well above the recommended daily allowance of 1.3 to 2.0 mg for adults. At larger injection volumes corresponding to higher tirzepatide doses in units, patients may receive 20 to 30 mg of pyridoxine per injection, which remains well below the tolerable upper intake level of 100 mg per day.
How tirzepatide works and why nausea happens
Understanding the B6 addition requires understanding why tirzepatide causes gastrointestinal problems in the first place. Tirzepatide is not a simple appetite suppressant. It operates through two distinct receptor pathways that affect digestion, blood sugar regulation, and satiety signaling in ways that are fundamentally different from older weight loss medications.
The dual-agonist mechanism
Tirzepatide activates GLP-1 receptors and GIP receptors simultaneously. The GLP-1 activation slows gastric emptying, which means food stays in the stomach longer. This creates a powerful feeling of fullness that reduces caloric intake. It also stimulates insulin secretion when blood sugar rises and suppresses glucagon release, both of which help regulate glucose levels. The GIP activation adds metabolic benefits that pure GLP-1 agonists like semaglutide do not provide, including enhanced fat oxidation and improved lipid metabolism.
This dual mechanism is what makes tirzepatide more effective than single-agonist medications. In the SURMOUNT-1 clinical trial, participants on the highest dose of tirzepatide lost an average of 22.5% of their body weight over 72 weeks. That level of weight reduction was unprecedented for a pharmaceutical intervention. But the same mechanisms that drive this dramatic weight loss also create the side effects that make early treatment so challenging.
Why nausea is the most common side effect
Nausea occurs because tirzepatide dramatically slows how quickly food moves from the stomach into the small intestine. When gastric emptying drops by 20% to 40%, the stomach holds food longer than the brain expects. This mismatch between what the digestive system is doing and what the nervous system anticipates triggers nausea signals through the vagus nerve and brainstem emetic centers.
The numbers from clinical trials tell the story clearly. Across the SURPASS trials for type 2 diabetes, nausea affected 12% to 24% of participants depending on the dose. In the SURMOUNT trials for obesity, gastrointestinal adverse events increased with dose: 39% at 5 mg, 46% at 10 mg, and 49% at the 15 mg dose. Nausea specifically was reported in up to 32% of participants. Vomiting affected up to 12%, and diarrhea hit up to 23%.
These are not small numbers.
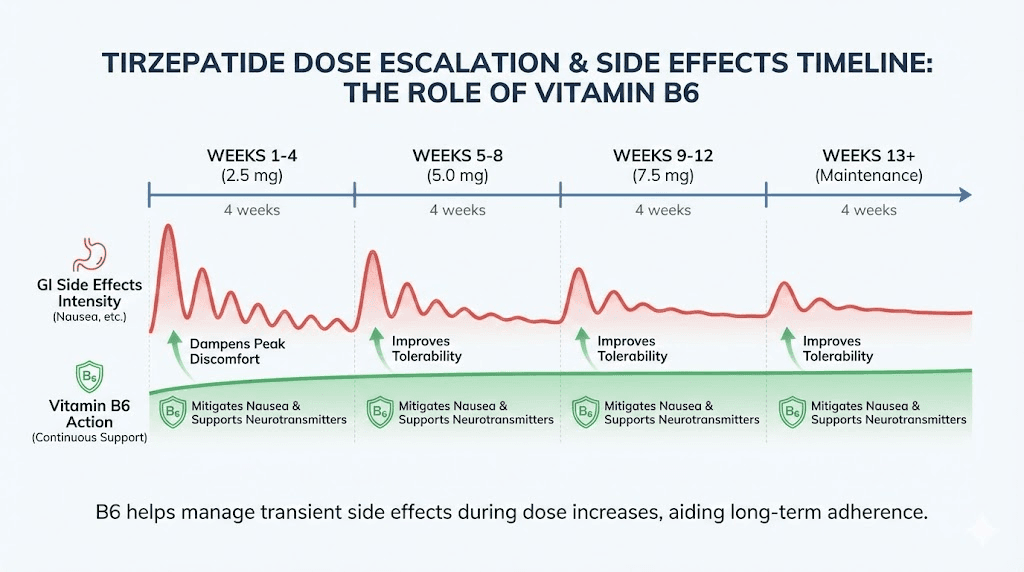
Most gastrointestinal side effects are classified as mild to moderate in severity and tend to occur primarily during dose escalation periods. This means the first four to eight weeks of treatment, and then again each time the dose increases, are the windows where nausea is most likely to disrupt a protocol. For many people, the body adjusts over time. But for some, the nausea is severe enough to force microdosing approaches or even complete discontinuation.
This is exactly where vitamin B6 enters the picture.
How vitamin B6 reduces nausea
Pyridoxine does not simply mask nausea symptoms. It works at the neurochemical level, modulating the same neurotransmitter systems that generate nausea signals in the first place. Understanding this mechanism explains why B6 has been used in clinical settings for nausea management long before anyone thought to combine it with GLP-1 medications.
The neurotransmitter connection
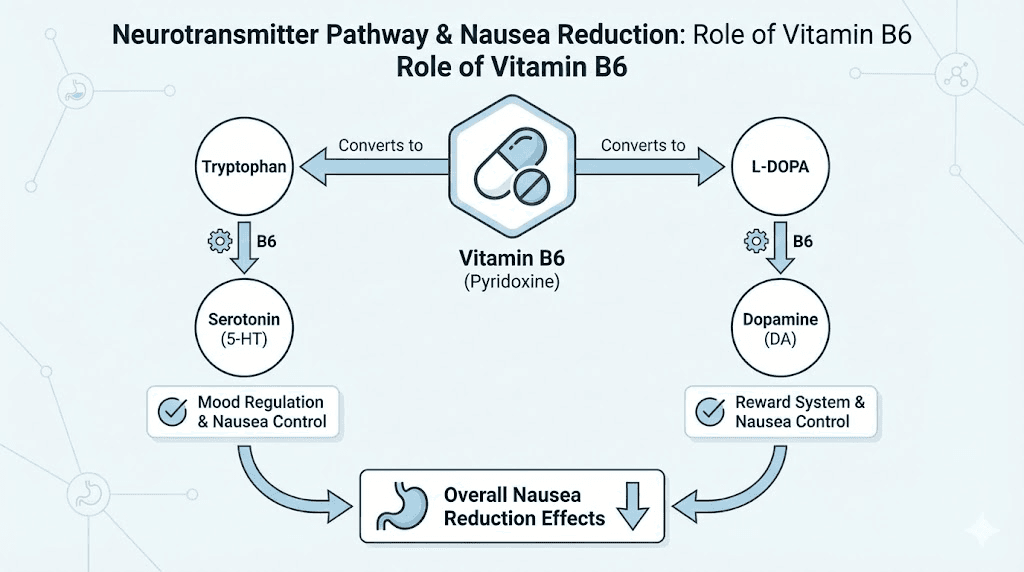
Vitamin B6 is a cofactor for more than 100 enzymatic reactions in the human body. Among the most important for nausea relief are the reactions that produce serotonin, dopamine, and gamma-aminobutyric acid (GABA). The active form of B6, pyridoxal 5-phosphate (PLP), is required by the enzyme aromatic L-amino acid decarboxylase (AADC), which catalyzes the final step in producing both serotonin from tryptophan and dopamine from L-DOPA.
Why does this matter for nausea?
Serotonin plays a central role in the emetic response. About 90% of the body serotonin is found in the gastrointestinal tract, where it regulates gut motility and communicates with the brainstem through the vagus nerve. When tirzepatide slows gastric emptying, serotonin signaling in the gut becomes disrupted. Pyridoxine helps stabilize this signaling by ensuring adequate serotonin synthesis and metabolism, preventing the wild fluctuations that trigger nausea.
GABA provides an additional layer of protection. As the primary inhibitory neurotransmitter in the brain, GABA calms overactive nerve signals, including the ones that drive the nausea response. By supporting GABA synthesis, vitamin B6 effectively turns down the volume on nausea signaling pathways. The result is not that nausea disappears entirely. Rather, its intensity and duration decrease enough for most people to continue their tirzepatide dosing protocol without interruption.
Clinical evidence for B6 and nausea
The evidence base for pyridoxine as an anti-nausea agent comes primarily from obstetric medicine. A landmark randomized, double-blind, placebo-controlled trial published in Obstetrics and Gynecology found that vitamin B6 at 25 mg every eight hours significantly reduced nausea severity compared to placebo. A systematic review and meta-analysis published in the Journal of Clinical Medicine confirmed that pyridoxine supplementation, both alone and in combination with other agents, significantly improved nausea symptoms as measured by standardized scoring tools.
The FDA has recognized this evidence. The combination of doxylamine and pyridoxine is an FDA-approved treatment for nausea and vomiting during pregnancy, marketed under brand names like Diclegis and Bonjesta. This is not a supplement claim or alternative medicine theory. Pyridoxine anti-nausea efficacy has regulatory validation.
No randomized controlled trials have specifically studied the tirzepatide-plus-B6 compound formulation. The rationale for the combination is based on extrapolation from the established anti-nausea evidence, the known neurotransmitter mechanisms, and anecdotal reports from clinicians and patients who use the compounded formulation. This is an important distinction. The evidence is plausible and supported by mechanism, but it has not been directly tested in the specific context of GLP-1 induced nausea through a rigorous clinical trial.
Benefits of B6 beyond nausea relief
While nausea reduction is the primary reason compounding pharmacies add pyridoxine to tirzepatide, vitamin B6 provides several additional benefits that are particularly relevant for people on GLP-1 therapy. These secondary benefits are not dramatic on their own, but they address common challenges that arise during weight loss treatment.
Energy production and fatigue management
Fatigue is a frequent complaint during tirzepatide therapy. Some of this tiredness comes from caloric restriction, as tirzepatide naturally reduces food intake by 20% to 30% in many users. Some comes from metabolic adjustments as the body shifts energy sources. And some relates to micronutrient depletion that occurs when food intake drops significantly.
Vitamin B6 plays a direct role in energy metabolism. It helps the body extract ATP from stored glycogen, convert amino acids into glucose through gluconeogenesis, and metabolize fatty acids for energy production. People on GLP-1 medications who experience fatigue may benefit from the additional pyridoxine, particularly if their reduced food intake has lowered their B6 levels below optimal.
The energy benefit is modest. Do not expect a stimulant effect or anything resembling caffeine. What B6 provides is metabolic support that helps prevent the kind of sluggishness and brain fog that sometimes accompany significant caloric deficits.
Protein metabolism during weight loss
Muscle preservation is one of the biggest concerns during rapid weight loss. When people lose 15% to 20% of their body weight on tirzepatide, not all of that loss comes from fat. Without adequate protein intake and proper metabolic support, a significant portion can come from lean muscle mass.
Vitamin B6 is essential for protein metabolism. It helps break down amino acids, facilitates their transport and utilization, and supports the transamination reactions that allow the body to use dietary protein efficiently. For people following high-protein tirzepatide meal plans designed to protect muscle mass, adequate B6 status ensures that the protein they eat actually gets used for muscle maintenance rather than being inefficiently metabolized.
This is also why protein shakes for GLP-1 users have become so popular. The combination of high protein intake with adequate B6 creates the best conditions for preserving lean tissue during aggressive weight loss.
Mood stabilization and emotional eating
Weight loss journeys are emotional. The relationship between food, mood, and behavior patterns runs deep, and disrupting it through pharmaceutical intervention can create psychological challenges that pure calorie counting never produces.
Pyridoxine supports the synthesis of dopamine and serotonin, both of which regulate mood, motivation, and reward processing. Adequate levels of these neurotransmitters help maintain emotional stability during the significant dietary and behavioral changes that tirzepatide therapy requires. When B6 levels drop too low, symptoms can include irritability, anxiety, difficulty concentrating, and depressive mood, all of which increase the risk of emotional eating and protocol abandonment.
Tirzepatide and anxiety is a topic that comes up frequently in patient communities. While the compound B6 formulation is not a treatment for anxiety disorders, the neurotransmitter support it provides may help buffer against the mood fluctuations that sometimes accompany GLP-1 therapy.
Immune function support
Vitamin B6 supports immune function by promoting the production of white blood cells and antibodies. During periods of caloric restriction and rapid weight loss, the immune system can become compromised. The additional pyridoxine in the compound formulation provides a small but potentially meaningful layer of immune support during what is already a metabolically stressful period for the body.
How tirzepatide with B6 compares to other compound additives
Vitamin B6 is just one of several additives that compounding pharmacies include in tirzepatide formulations. Understanding the differences helps you evaluate which formulation, if any, aligns with your specific needs and concerns. Each additive brings different properties to the table, and none of them fundamentally change how tirzepatide itself works.
Tirzepatide with B6 vs tirzepatide with B12
Compounded tirzepatide with B12 is probably the most common combination on the market. Methylcobalamin or cyanocobalamin, the two forms of vitamin B12, are added primarily for energy support and to prevent the B12 deficiency that can develop during prolonged caloric restriction. B12 is critical for red blood cell formation, neurological function, and DNA synthesis.
The key difference between B6 and B12 as additives comes down to their primary benefit. B6 targets nausea through neurotransmitter modulation. B12 targets energy and prevents deficiency. If nausea is your primary concern during tirzepatide dose escalation, B6 is the more directly relevant additive. If fatigue and low energy are your bigger challenges, B12 may be more helpful.
Many compounders now offer triple combinations including tirzepatide, glycine, and B12, or even formulations with both B6 and B12. These multi-additive compounds try to address multiple side effects simultaneously. The tirzepatide methylcobalamin combination specifically uses the more bioavailable form of B12 for maximum absorption.
Tirzepatide with B6 vs tirzepatide with glycine
Glycine in tirzepatide formulations serves a dual purpose. As an amino acid, glycine supports digestion, promotes collagen production, aids sleep quality, and helps stabilize blood sugar. It also acts as a chemical stabilizer for the tirzepatide molecule itself, potentially improving the shelf life and consistency of the compounded product.
For nausea specifically, glycine has mild calming effects on the digestive system, but it does not match the established evidence base that pyridoxine has for nausea reduction. Glycine excels more in the areas of gut comfort, bloating reduction, and formulation stability. If gastrointestinal distress beyond just nausea is your concern, glycine may actually be the better choice. If pure nausea reduction is the priority, B6 has stronger supporting evidence.
Tirzepatide with B6 vs tirzepatide with niacinamide
Niacinamide (vitamin B3) in tirzepatide compounds serves yet another purpose. Niacinamide supports cellular energy production through NAD+ pathways, reduces inflammation, and supports skin barrier function. The skin benefit is notable because rapid weight loss can affect skin elasticity and health, making niacinamide a forward-thinking addition for people concerned about loose skin.
However, niacinamide does not directly address nausea. It also carries a risk of flushing in sensitive individuals at higher doses. For nausea management specifically, B6 remains the superior choice.
Additive | Primary benefit | Nausea relief | Energy support | Evidence strength | Best for |
|---|---|---|---|---|---|
Vitamin B6 | Anti-nausea | Strong | Moderate | Established (pregnancy studies) | People with significant nausea |
Vitamin B12 | Energy, nerve health | Minimal | Strong | Well-established for deficiency | People with fatigue or B12 deficiency |
Glycine | Gut comfort, stability | Mild | Minimal | Limited for nausea specifically | People with bloating and GI discomfort |
Niacinamide | Cellular energy, skin | None | Moderate | Established for NAD+ support | People concerned about skin health |

Dosing and administration of tirzepatide with B6
The tirzepatide component of the compound follows the same dose escalation protocol as standard tirzepatide. The B6 component scales automatically based on injection volume, since the pyridoxine is dissolved at a fixed concentration in the same solution.
Standard tirzepatide dose escalation
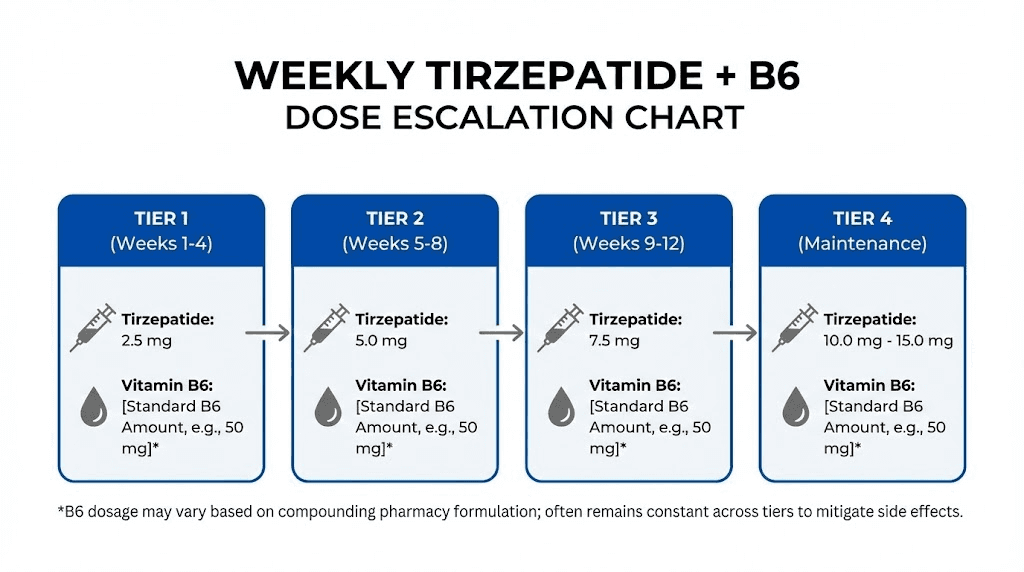
The established starting dose for compounded tirzepatide is 2.5 mg once weekly for the first four weeks. This allows the body to adjust to the GLP-1 and GIP receptor activation before increasing the dose. After four weeks at 2.5 mg, the dose typically increases to 5 mg weekly. From there, dose escalation continues in 2.5 mg increments every four weeks based on tolerability and response, up to a maximum of 15 mg weekly.
The complete escalation schedule looks like this:
Weeks 1 to 4: 2.5 mg once weekly
Weeks 5 to 8: 5 mg once weekly
Weeks 9 to 12: 7.5 mg once weekly
Weeks 13 to 16: 10 mg once weekly
Weeks 17 and beyond: 12.5 mg or 15 mg once weekly (if needed)
For people using microdose tirzepatide schedules, the escalation is even more gradual. Microdosing protocols may start at 1 mg or less and increase in smaller increments, which already helps reduce nausea but may benefit even more from the B6 addition.
How the B6 component scales with dose
With pyridoxine fixed at 50 mg/mL in the compounded solution, the amount of B6 delivered per injection depends on the total injection volume. This creates a natural scaling effect where higher tirzepatide doses, which tend to cause more nausea, also deliver more anti-nausea pyridoxine.
At a 2.5 mg starting dose, the injection volume is typically small, delivering approximately 5 to 10 mg of pyridoxine. At the 10 mg maintenance dose, the larger injection volume delivers 20 to 30 mg of pyridoxine. Even at the maximum tirzepatide dose, the pyridoxine delivery stays well below 50 mg, far under the 100 mg daily tolerable upper limit established by the National Institutes of Health.
This self-scaling design is one of the elegant aspects of the compound formulation. You do not need to calculate or adjust your B6 intake separately. The formulation handles it automatically. Use our peptide calculator to understand injection volumes at different concentrations, and the peptide reconstitution calculator if you are working with lyophilized formulations.
Injection technique and site selection
The compound is administered as a subcutaneous injection, just like standard tirzepatide. The three recommended injection sites are the abdomen (at least two inches from the navel), the front of the thighs, and the back of the upper arms. Injecting tirzepatide in the stomach area tends to be the most popular site due to ease of access and consistent absorption.
Rotate injection sites with each dose. Do not inject in the same spot consecutively. Injection site reactions including redness, swelling, or itching can occur and are more common when the same area is used repeatedly. The pyridoxine in the compound formulation does not typically increase injection site discomfort, though some users report a mild warming sensation at the injection site that resolves within minutes.
Choosing the right syringe matters too. Refer to our tirzepatide syringe dosage guide to match your syringe type with your prescribed volume. Using a syringe that is too large makes it difficult to draw small volumes accurately. Using one that is too small may require multiple draws.
Timing and consistency
Inject on the same day each week. The specific day does not matter as much as consistency. If you are wondering about the best time to take a GLP-1 shot, most practitioners recommend morning or early afternoon administration. Some users find that injecting in the evening increases overnight nausea, which disrupts sleep. Others report no difference regardless of timing.
If you need to shift your injection day, you can adjust by a day or two. Taking tirzepatide a day early is generally acceptable as long as you maintain roughly seven-day intervals going forward. What you want to avoid is stacking doses too close together or going too long between injections, as both scenarios can worsen side effects.
Managing side effects on tirzepatide with B6
Even with the B6 addition, tirzepatide can still cause side effects. Pyridoxine reduces nausea severity and frequency for many users, but it does not eliminate all gastrointestinal symptoms or prevent every possible adverse reaction. A complete management strategy addresses multiple symptoms simultaneously.
Nausea management beyond B6
If the B6 in your compound is not fully controlling nausea, additional strategies can help. Dietary modifications are first line. Eating smaller, more frequent meals reduces the volume of food sitting in a stomach that is emptying more slowly. Avoiding high-fat and greasy foods is critical, as these take the longest to digest and exacerbate the delayed gastric emptying effect.
Foods to avoid on tirzepatide include fried items, heavy cream-based dishes, excessive red meat portions, and spicy foods during the dose escalation phase. Conversely, foods that work well with tirzepatide tend to be lean proteins, cooked vegetables, and easily digestible carbohydrates like rice and toast.
Ginger is a natural anti-emetic that complements B6 well. The combination of pyridoxine and ginger has been studied in obstetric settings and shows additive benefits. Peppermint tea can also soothe an upset stomach. Some practitioners prescribe ondansetron (Zofran) for severe nausea that does not respond to dietary changes and the B6 in the compound.
Constipation and digestive discomfort
Constipation on tirzepatide is the second most common gastrointestinal complaint after nausea. The slowed gastric motility that reduces appetite also slows transit time through the entire digestive tract, leading to harder stools and less frequent bowel movements. Vitamin B6 does not directly address constipation, so this symptom requires separate management.
Adequate water intake is essential. Many tirzepatide users underestimate how much fluid they need, especially when eating less food (which normally provides a significant portion of daily water intake). Fiber supplementation, magnesium citrate, and regular physical activity all support healthy bowel function during GLP-1 therapy.
Diarrhea on tirzepatide affects a smaller but still significant number of users, particularly during dose escalation. While it seems contradictory that the same medication can cause both constipation and diarrhea, these occur in different individuals and sometimes at different points in the same person treatment timeline.
Headaches and body aches
Headaches during tirzepatide therapy often relate to dehydration, blood sugar fluctuations, or caloric restriction rather than the medication itself. The B6 in the compound may help slightly by supporting neurotransmitter balance, but hydration and adequate nutrition are the primary solutions.
Body aches on tirzepatide and muscle pain can occur during rapid weight loss as the body adapts to metabolic changes. These symptoms are generally transient and respond well to adequate protein intake, gentle exercise, and proper supplementation.
Sleep disruption
Insomnia on tirzepatide is an underreported side effect that some users experience, particularly when nausea or gastrointestinal discomfort disrupts nighttime rest. The B6 in the compound may offer a small benefit here through its role in melatonin synthesis. Pyridoxine is a cofactor in the conversion of tryptophan to serotonin, which is then converted to melatonin, the sleep hormone. Adequate B6 levels support this conversion pathway.
That said, the B6 delivered through the weekly injection is not equivalent to a daily sleep supplement. If sleep disruption is a persistent issue, explore timing adjustments, evening eating habits, and sleep hygiene practices as primary interventions.
Fatigue and energy levels
Energy levels on tirzepatide follow a predictable pattern for most users. The first few weeks often bring noticeable fatigue as the body adjusts to reduced caloric intake. By weeks four to six, most people report stabilized or even improved energy as the metabolic benefits of weight loss begin to manifest. The B6 in the compound supports this transition by maintaining the enzymatic pathways involved in energy extraction from macronutrients.
Tirzepatide and metabolism is a complex topic. The medication does not increase basal metabolic rate in the traditional sense, but it does improve metabolic efficiency, insulin sensitivity, and fat oxidation, all of which contribute to better energy utilization over time.
Storage, stability, and handling
Compounded tirzepatide with B6 requires proper storage to maintain potency and safety. Because this is a compounded product, storage requirements may differ slightly from brand-name tirzepatide, and the addition of pyridoxine introduces its own stability considerations.
Refrigeration requirements
Tirzepatide requires refrigeration. Store the compounded vial at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Properly refrigerated compounded tirzepatide typically maintains potency for 28 to 90 days depending on the compounding pharmacy formulation and beyond-use dating assigned.
The pyridoxine component is relatively stable and does not impose additional storage challenges beyond what tirzepatide already requires. Vitamin B6 is stable in aqueous solutions at the pH ranges typically used in compounded injectables, and it does not degrade faster than tirzepatide itself under proper refrigeration.
Temperature excursions
If your tirzepatide with B6 is left out of the fridge, the standard guidance is that brief room temperature exposure (under 86 degrees Fahrenheit) for up to 24 hours is generally acceptable. Extended exposure to heat degrades the tirzepatide peptide chain faster than it affects the pyridoxine, so the tirzepatide stability is the limiting factor.
For travel, use an insulated cooler bag with ice packs. Our guide to traveling with GLP-1 medications covers TSA rules, temperature maintenance during flights, and international travel considerations. The same principles apply to compounded tirzepatide with B6.
Expiration and potency
Compounded tirzepatide does expire. Unlike brand-name medications with extensive stability testing, compounded formulations have shorter beyond-use dates, typically 30 to 90 days. The compounding pharmacy will assign a specific expiration date based on their stability testing data. Do not use the product past this date, regardless of how it looks or smells.
Pyridoxine is sensitive to light exposure. While the tirzepatide component is also light-sensitive, the B6 can degrade when exposed to prolonged UV or bright light. Keep the vial in its original packaging or wrapped in foil if the packaging is translucent. Store in the back of the refrigerator where light exposure is minimal.
The regulatory landscape
Understanding the regulatory context around compounded tirzepatide with B6 is important for making informed decisions. This is not a straightforward topic, and the rules have shifted significantly in recent years.
FDA approval status
Tirzepatide with B6 is not an FDA-approved combination product. The FDA has approved tirzepatide alone under two brand names: Mounjaro for type 2 diabetes management and Zepbound for chronic weight management. These brand-name products do not contain vitamin B6 or any other additives.
Compounding pharmacies are able to create custom formulations like tirzepatide with B6 under specific regulatory frameworks. Section 503A of the Federal Food, Drug, and Cosmetic Act allows licensed compounding pharmacies to prepare customized medications when a prescriber writes a patient-specific prescription. Section 503B covers outsourcing facilities that can compound without individual prescriptions but must follow additional manufacturing standards.
The shortage question
Compounding of tirzepatide has been legally available primarily during periods when the brand-name product was listed on the FDA drug shortage list. When tirzepatide was removed from the shortage list in late 2024, the legal basis for compounding became more restricted. The addition of B6, B12, glycine, or niacinamide creates a different formulation that some compounders have argued allows continued preparation under different regulatory provisions.
This legal landscape is actively evolving. Court challenges, FDA enforcement actions, and state pharmacy board decisions continue to shape what compounding pharmacies can and cannot do with tirzepatide formulations. Always verify that your compounding pharmacy is properly licensed and operating within current regulatory guidelines.
Safety considerations with compounded formulations
Compounded medications do not undergo the same rigorous testing for safety, efficacy, and quality that FDA-approved products require. This does not mean they are inherently unsafe, but it does mean that quality varies between compounding pharmacies. Some pharmacies have excellent quality control, independent third-party testing, and strict manufacturing protocols. Others operate with less oversight.
When evaluating a compounding pharmacy for tirzepatide with B6, look for PCAB (Pharmacy Compounding Accreditation Board) accreditation, third-party potency and sterility testing, proper state licensing, and a track record free of FDA warning letters or recalls. Our guides on specific compounding pharmacies like Empower tirzepatide, BPI Labs tirzepatide, and Southend pharmacy tirzepatide provide detailed quality analyses.
Avoid grey market tirzepatide sources entirely. The risk of contamination, incorrect potency, or counterfeit products is not worth any cost savings. Your health is not the place to cut corners.
Who should consider tirzepatide with B6
Not everyone needs the B6 formulation. For some people, standard tirzepatide is perfectly tolerable, and the added cost of a compounded formulation with pyridoxine offers no meaningful benefit. For others, the B6 addition can be the difference between completing a full dose escalation and abandoning treatment.
Ideal candidates
The tirzepatide with B6 compound makes the most sense for people who have experienced significant nausea on GLP-1 medications in the past, whether from tirzepatide itself or from semaglutide. If you have tried standard tirzepatide and could not tolerate the nausea during dose escalation, the B6 formulation offers a built-in countermeasure.
It also makes sense for people who are particularly sensitive to gastrointestinal disruption. Those with a history of motion sickness, severe morning sickness during pregnancy, or easily triggered nausea from other medications tend to have more pronounced GLP-1 related nausea. The pyridoxine addition provides targeted neurochemical support for exactly these individuals.
People concerned about maintaining energy levels and mood stability during aggressive caloric restriction also benefit from the compound. The metabolic and neurotransmitter support that B6 provides, while not dramatic, creates a slightly smoother experience during what is already a challenging physiological transition.
Who may not need it
If you have used tirzepatide or semaglutide before without significant nausea, the B6 addition is unlikely to provide noticeable benefits. The same applies if you already supplement with a high-quality B-complex vitamin that includes adequate pyridoxine. Doubling up on B6 from both the compound and oral supplements is unnecessary and, at very high levels over extended periods, can actually cause peripheral neuropathy, the very symptom that B6 deficiency also causes.
For people primarily concerned about hair loss during GLP-1 therapy or skin quality issues, the B6 formulation is not specifically targeted at those concerns. Niacinamide formulations may be more relevant for skin, and nutritional interventions including biotin and zinc address hair loss more directly.
Vitamin B6 deficiency and GLP-1 therapy
The relationship between GLP-1 medications and micronutrient status deserves attention. When tirzepatide reduces food intake by 20% to 30%, it also reduces the intake of vitamins and minerals that come from food. Vitamin B6 is a water-soluble vitamin that the body does not store in large amounts, making consistent intake important.
Signs of B6 deficiency
Deficiency in vitamin B6 can manifest gradually, and many of its symptoms overlap with common tirzepatide side effects, which makes identification tricky. Key signs include:
Peripheral neuropathy: tingling or numbness in the hands and feet
Mood changes: irritability, anxiety, depressive symptoms
Fatigue and weakness: beyond what caloric restriction alone explains
Skin rashes: seborrheic dermatitis, particularly on the face and scalp
Cracked lips and mouth corners: a condition called cheilosis
Impaired immune function: more frequent infections than usual
Confusion or difficulty concentrating: related to impaired neurotransmitter synthesis
If you are on tirzepatide and experiencing persistent tiredness, anxiety, or body aches that do not resolve with standard management strategies, it may be worth having your B6 levels tested. A simple blood test for pyridoxal 5-phosphate (PLP), the active form of B6, can determine whether deficiency is contributing to your symptoms.
Why GLP-1 users are at higher risk
Several factors increase the risk of B6 depletion during GLP-1 therapy. Reduced food intake is the most obvious. But beyond that, the metabolic changes induced by significant weight loss increase the body demand for B6. Protein metabolism, which requires adequate B6, intensifies when the body is breaking down both dietary protein and its own tissues during weight loss. The body needs more B6 at exactly the time when dietary intake of B6 is dropping.
Additionally, certain common medications interact with B6 status. Proton pump inhibitors, which some tirzepatide users take for reflux, can impair B6 absorption. Oral contraceptives also deplete B6 levels. People taking these medications alongside tirzepatide face a compounded risk of deficiency.
The compound formulation with B6 addresses this proactively. Rather than waiting for deficiency symptoms to appear and then supplementing reactively, the pyridoxine built into each injection provides ongoing replenishment. This preventive approach aligns with how supplement recommendations for tirzepatide users increasingly emphasize proactive rather than reactive micronutrient support.
Practical considerations for getting started
If you have decided that tirzepatide with B6 is worth exploring, several practical steps will help you navigate the process smoothly.
Getting a prescription
Tirzepatide with B6 requires a prescription from a licensed healthcare provider. This is not a supplement or over-the-counter product. Your prescriber needs to specify tirzepatide with pyridoxine on the prescription, along with the concentration, volume, and dispensing instructions specific to the compounding pharmacy being used.
Many telehealth providers and weight loss clinics now offer tirzepatide prescriptions and can direct the prescription to a compounding pharmacy of your choice. When speaking with your provider, ask specifically about the B6 compound formulation if nausea management is a priority for you. Some providers default to B12 formulations simply because those are more commonly stocked, but B6 formulations are available from most major compounding pharmacies.
Questions to ask your compounding pharmacy
Before filling a prescription for compounded tirzepatide with B6, ask these specific questions:
What is the pyridoxine concentration per mL?
What form of pyridoxine is used (hydrochloride is standard)?
What is the beyond-use date assigned to this formulation?
Does the pharmacy conduct third-party potency testing?
Does the pharmacy conduct sterility testing on each batch?
Is the pharmacy PCAB accredited or state licensed for sterile compounding?
What is the recommended storage protocol?
These questions are not excessive. They represent the minimum due diligence for any compounded injectable medication.
Cost considerations
Compounded tirzepatide with B6 typically costs less than brand-name Mounjaro or Zepbound, which can run over $1,000 per month without insurance. Affordable tirzepatide options through compounding pharmacies have been one of the driving forces behind the popularity of compound formulations.
The addition of B6 may add a small amount to the compounding cost compared to a plain tirzepatide compound, but the difference is typically minimal. Some pharmacies include the B6 at no additional charge as part of their standard tirzepatide formulation. Others offer it as an optional add-on. Peptide cost calculators can help you compare pricing across different sources and formulations.
Insurance does not typically cover compounded medications. Plan to pay out of pocket. Some pharmacies offer payment plans like Afterpay or monthly subscription pricing that makes the cost more manageable.
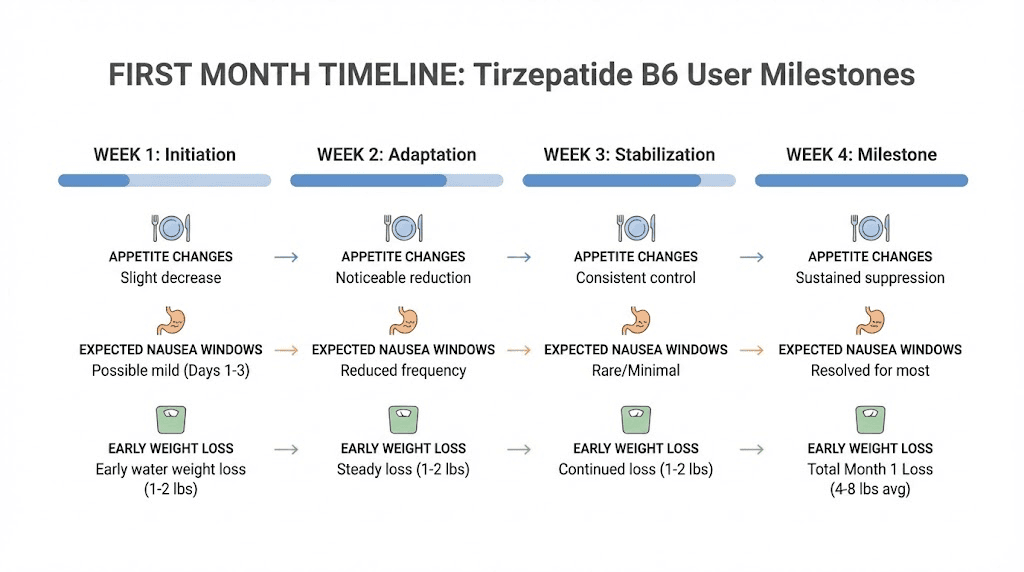
What to expect in the first month
The first four weeks on tirzepatide with B6 at the 2.5 mg starting dose set the foundation for the entire protocol. Most people experience some appetite suppression within the first week, though full appetite suppression may take two to three weeks to fully develop.
Nausea, if it occurs, typically peaks 24 to 72 hours after each injection. With the B6 compound, many users report that nausea is milder and shorter in duration compared to their experience with standard tirzepatide. This is not guaranteed, as individual responses vary, but it is the most commonly reported benefit.
Weight loss during the first month is often modest at the 2.5 mg dose, typically 2 to 5 pounds. The real weight loss acceleration begins at the 5 mg dose and above. How fast tirzepatide works depends on multiple factors including starting weight, diet adherence, activity level, and individual metabolic response. Looking at tirzepatide before and after results shows the wide range of outcomes possible.
Combining tirzepatide B6 with diet and lifestyle strategies
The compound formulation works best when paired with intentional dietary and lifestyle modifications. Tirzepatide, regardless of additives, is a tool that amplifies the effects of good habits. Without those habits, results plateau faster and side effects linger longer.
Nutritional priorities
A structured diet plan for tirzepatide users should prioritize protein above all other macronutrients. Aim for 0.7 to 1.0 grams of protein per pound of target body weight. This protects muscle mass during rapid weight loss and supports the protein metabolism pathways that vitamin B6 facilitates.
Hydration is second in importance. The reduced food intake means less water from food sources, while the altered digestion patterns increase the need for adequate fluid. Target a minimum of 64 ounces of water daily, and increase that amount if you exercise or live in a warm climate.
A comprehensive list of foods that work well during GLP-1 therapy includes lean poultry, fish, eggs, Greek yogurt, cottage cheese, tofu, legumes, cooked vegetables, whole grains, and fruits. These foods are nutrient-dense, relatively easy to digest, and provide the vitamins and minerals that reduced eating may otherwise deplete.
Alcohol and tirzepatide is another important consideration. Alcohol adds empty calories, can worsen nausea, and interferes with the metabolic processes that B6 supports. Reducing or eliminating alcohol during active weight loss maximizes both the effectiveness of the medication and the benefits of the pyridoxine additive.
Exercise considerations
Resistance training is the single most important exercise modality during GLP-1 mediated weight loss. It sends the signal that muscle tissue is needed and should not be sacrificed for energy. Two to three resistance training sessions per week, focusing on compound movements like squats, deadlifts, rows, and presses, provides the stimulus needed to preserve lean mass.
Cardiovascular exercise supports overall health and can increase the caloric deficit, but it should not come at the expense of resistance training. Walking 30 to 60 minutes most days is sufficient for cardiovascular health without adding excessive stress to a body that is already adapting to reduced caloric intake and pharmaceutical intervention.
Supplementation beyond B6
While the compound formulation provides B6, other nutritional gaps may need attention. A comprehensive supplement strategy for tirzepatide users typically includes:
Vitamin D: often low in overweight individuals and further depleted by caloric restriction
Magnesium: supports muscle function, sleep quality, and bowel regularity
Omega-3 fatty acids: anti-inflammatory support during metabolic transition
Probiotics: gut health support as digestive patterns change
Electrolytes: sodium, potassium, and magnesium balance during increased water intake
The GLP-1 companion guide provides a more comprehensive breakdown of nutritional support during weight loss medication therapy.
Switching to or from tirzepatide with B6
If you are currently on a different tirzepatide formulation or a different GLP-1 medication entirely, switching to the B6 compound involves specific considerations.
Switching from standard tirzepatide to the B6 compound
This is the simplest transition. You continue at your current dose and simply switch to a vial that includes pyridoxine. No dose adjustment is needed. The tirzepatide component is identical, and the B6 addition does not interact with tirzepatide efficacy or pharmacokinetics.
The best time to make this switch is at the beginning of a new vial, so you do not waste medication from a partially used vial of the non-B6 formulation.
Switching from semaglutide to tirzepatide with B6
Switching between GLP-1 medications requires medical guidance. Tirzepatide and semaglutide have different receptor profiles, potencies, and dose ranges. The tirzepatide vs semaglutide dosage chart shows approximate equivalent doses, but there is no perfect one-to-one conversion.
Generally, the transition involves completing your current semaglutide cycle, allowing one week for washout, and then starting tirzepatide at the 2.5 mg starting dose regardless of your previous semaglutide dose. Some practitioners use a more aggressive crossover for patients who were on higher semaglutide doses, but the conservative approach minimizes the risk of severe side effects during the transition.
The B6 compound formulation is particularly appealing for people switching from semaglutide who experienced significant nausea. If nausea was the reason for the switch, the built-in pyridoxine provides a layer of protection that plain tirzepatide does not.
Considering other delivery methods
Tirzepatide is also available in non-injectable formats. Oral tirzepatide versus injection is a comparison many people explore, especially those who dislike needles. Tirzepatide drops, tirzepatide tablets, and orally disintegrating tablets each have their own absorption profiles and bioavailability characteristics.
The B6 compound formulation is currently available only as an injectable. Oral tirzepatide formulations may include different additives or none at all. If the anti-nausea benefit of B6 is important to you and you prefer non-injectable delivery, you would need to supplement with oral pyridoxine separately.
What happens if tirzepatide with B6 is not working
Not everyone responds ideally to any medication, and tirzepatide with B6 is no exception. If you are not seeing the results you expected or the B6 does not seem to be controlling your nausea, several strategies can help.
Persistent nausea despite B6
If nausea remains problematic even with the pyridoxine compound, consider whether the underlying cause is truly GLP-1 related or something else. Dietary triggers are the most common overlooked factor. Many people underestimate how much their eating habits need to change on tirzepatide. Large meals, high-fat foods, eating too quickly, and drinking large volumes of liquid with meals can all worsen nausea regardless of B6 supplementation.
Dose escalation speed is another factor. If you are increasing your dose every four weeks as per the standard schedule and experiencing severe nausea each time, ask your prescriber about extending the time at each dose to six or eight weeks. Slower escalation gives the body more time to adapt, and the B6 has more opportunity to provide its protective effect at each tier.
Insufficient weight loss
Not losing weight on tirzepatide is a frustration that affects a meaningful number of users. The B6 additive does not directly influence weight loss, so if the medication itself is not producing results, the pyridoxine will not change that outcome. Weight loss failure on tirzepatide usually traces back to insufficient dose (need to escalate further), caloric intake still exceeding expenditure despite reduced appetite, metabolic adaptation, or underlying medical conditions like hypothyroidism or PCOS that require separate treatment.
If your tirzepatide stops working after an initial period of success, this may represent a plateau rather than medication failure. Plateaus are normal in weight loss and typically require adjustments to diet, exercise, or dose rather than abandoning the medication entirely. The plateau management strategies that apply to semaglutide are equally relevant for tirzepatide.
Exploring combination approaches
Some practitioners combine tirzepatide with other agents for enhanced results. Phentermine and tirzepatide together is one combination that has been explored for plateau-breaking. AOD-9604 with tirzepatide targets additional fat loss pathways. These combinations require medical supervision and are not universally recommended, but they represent options for people who have plateaued on tirzepatide alone.
SeekPeptides members access detailed protocol guidance for combining agents safely, including drug interaction databases, dosing schedules, and community experiences from thousands of researchers who have navigated similar challenges.
Comparing tirzepatide B6 to other GLP-1 options
Tirzepatide is not the only GLP-1 medication available, and the B6 compound is not the only way to manage nausea. Understanding how this formulation fits into the broader landscape helps you make an informed choice.
Tirzepatide vs semaglutide
The semaglutide vs tirzepatide comparison is the most common matchup people evaluate. Tirzepatide dual GIP/GLP-1 mechanism produces greater average weight loss (22.5% vs 15% to 17% for semaglutide in comparable trials) but also tends to cause more gastrointestinal side effects, particularly at higher doses. The B6 compound formulation is one strategy for getting the superior weight loss of tirzepatide while managing its higher nausea risk.
Semaglutide is also available as a compounded formulation with various additives including B12, glycine, and methylcobalamin. If you are considering whether to start with semaglutide or tirzepatide, the side effect comparison is worth reviewing carefully.
Tirzepatide vs retatrutide
The next generation of weight loss peptides includes triple agonists like retatrutide, which activates GLP-1, GIP, and glucagon receptors simultaneously. The three-way comparison of semaglutide, tirzepatide, and retatrutide shows that retatrutide may produce even greater weight loss than tirzepatide, but it is not yet FDA-approved and is only available through research sources.
For those interested in retatrutide, our guides on retatrutide dosing, availability, and how it compares to Ozempic provide comprehensive analysis.
Other GLP-1 alternatives
The GLP-1 field is expanding rapidly. Survodutide, CagriSema, orforglipron, and mazdutide are all in various stages of development or approval. Each has its own side effect profile and may or may not benefit from B6 addition. As these medications become available, the compound formulation landscape will continue to evolve.
For researchers evaluating the full landscape of weight loss peptides, SeekPeptides provides continuously updated comparison guides, clinical trial summaries, and community experiences that help navigate this rapidly changing field.
Reconstitution and preparation
If you receive tirzepatide with B6 as a lyophilized (freeze-dried) powder rather than a pre-mixed solution, you will need to reconstitute it before use. This process is straightforward but requires attention to sterile technique and proper dilution.
Reconstitution basics
Reconstituting tirzepatide follows the same general process regardless of whether the formulation includes B6. The key steps are:
Gather supplies: bacteriostatic water, alcohol swabs, appropriate syringes
Swab the vial tops with alcohol and allow to dry
Draw the prescribed amount of bacteriostatic water
Inject the water slowly into the peptide vial, aiming at the glass wall rather than directly onto the powder
Swirl gently, do not shake, until fully dissolved
Allow the solution to clear completely before drawing your first dose
For specific volume calculations, how much bacteriostatic water to mix with 10mg tirzepatide covers the math in detail. Our reconstitution calculator automates the calculation for any vial size and desired concentration.
When the formulation includes B6, the pyridoxine is typically already incorporated into the lyophilized powder or provided as a pre-mixed solution. Check with your compounding pharmacy for specific preparation instructions, as the presence of B6 may slightly alter the appearance of the reconstituted solution. A faint yellow tint is normal and comes from the pyridoxine, it does not indicate degradation.
Long-term considerations
Tirzepatide therapy is not a short-term intervention for most users. Weight management may require ongoing treatment for months or years, and understanding the long-term implications of the B6 compound formulation matters for sustained success.
B6 accumulation and upper limits
While vitamin B6 is water-soluble and excess amounts are excreted through urine, chronic high-dose supplementation can cause problems. The tolerable upper intake level for adults is 100 mg per day. At the doses delivered through the compound formulation (5 to 30 mg per week), accumulation to toxic levels is extremely unlikely. The weekly dosing schedule, combined with the body rapid clearance of water-soluble vitamins, provides a substantial safety margin.
However, if you are also taking oral B6 supplements, a B-complex vitamin, and eating B6-rich foods like poultry, fish, potatoes, and bananas, your total weekly intake could be higher than you realize. Ask your healthcare provider about monitoring if you are combining multiple B6 sources long-term.
Maintenance dosing and long-term plans
Once you reach your goal weight, the question becomes whether to continue tirzepatide and at what dose. Most practitioners recommend continuing at a lower maintenance dose to prevent weight regain. The nausea issue typically resolves by this point, as the body has fully adapted to the medication. The B6 component becomes less critical for nausea management but continues to provide metabolic and neurotransmitter support.
Some people transition from the B6 compound to standard tirzepatide for maintenance, reasoning that the anti-nausea benefit is no longer needed once they are on a stable dose. Others continue with the compound formulation for the ongoing nutritional support. Either approach is reasonable and should be guided by your individual experience and practitioner recommendations.
For researchers serious about optimizing their protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, detailed comparison tools, and a community of thousands who have navigated these exact decisions.
Frequently asked questions
Does the B6 in compounded tirzepatide actually reduce nausea?
Vitamin B6 (pyridoxine) has established clinical evidence for reducing nausea in pregnancy and motion sickness settings. While no randomized controlled trial has specifically studied the tirzepatide-plus-B6 combination, the neurochemical mechanism, specifically the modulation of serotonin and GABA in the brainstem emetic centers, provides a plausible basis for benefit. Many users and clinicians report reduced nausea severity with the B6 formulation, though individual responses vary. Read more about getting started with compounded tirzepatide.
Can I take separate B6 supplements instead of the compound?
Yes, oral pyridoxine supplements are available over the counter. However, the compound formulation delivers B6 directly into subcutaneous tissue, bypassing the digestive system. This is relevant because tirzepatide itself slows gastric emptying, which can impair the absorption of oral supplements. The injectable route ensures consistent B6 delivery regardless of how your gut is functioning on any given day.
Is tirzepatide with B6 more expensive than plain tirzepatide?
The addition of pyridoxine typically adds a minimal amount to the compounding cost, often less than $10 to $20 per month difference. Some pharmacies include B6 at no extra charge. Compare pricing using our peptide cost calculator and check guides on specific pharmacies for current pricing information.
Can I switch from tirzepatide with B12 to tirzepatide with B6?
Yes. The switch is straightforward since only the vitamin additive changes. Continue at your current tirzepatide dose and simply use the B6 formulation for your next vial. No washout period or dose adjustment is needed. Some people choose to switch specifically because B6 targets nausea more directly than the B12 formulation.
How long does the nausea reduction from B6 last after each injection?
The pyridoxine from each injection is metabolized over several days. Most users report that the anti-nausea benefit is most noticeable in the first 48 to 72 hours after injection, which conveniently aligns with the window when tirzepatide nausea is typically most intense. By mid-week, both the nausea trigger and the B6 protection diminish together.
Is there anyone who should avoid the B6 compound?
People taking levodopa (for Parkinson disease) should use caution, as high-dose pyridoxine can reduce levodopa effectiveness. People with a history of B6-related peripheral neuropathy should avoid additional supplementation. Anyone with kidney disease should consult their prescriber, as impaired renal function can alter B6 metabolism. For most other people, the B6 compound is well-tolerated.
Does tirzepatide with B6 work for type 2 diabetes management?
Tirzepatide is FDA-approved for type 2 diabetes under the brand name Mounjaro. The compounded formulation with B6 contains the same active peptide and would be expected to provide the same glucose-lowering effects. The B6 additive does not interfere with tirzepatide mechanism for blood sugar control. However, compounded formulations are not FDA-approved products, and your endocrinologist should be involved in any decision to use compounded tirzepatide for diabetes management.
What color should tirzepatide with B6 look like?
A clear to slightly yellow solution is normal. The yellow tint comes from the pyridoxine. If the solution is cloudy, contains visible particles, or has changed color to brown or amber, do not use it and contact your pharmacy. Proper storage and refrigeration prevents most degradation issues.
External resources
PMC: Tirzepatide-induced gastrointestinal manifestations systematic review
PubMed: Pyridoxine for nausea and vomiting randomized controlled trial
In case I do not see you, good afternoon, good evening, and good night. May your nausea stay mild, your protocols stay consistent, and your results stay worth the effort.