Feb 15, 2026

Your appetite vanished. The scale is finally moving. But something feels off. Maybe it is the fatigue that hits by 2pm. Maybe your hair is thinning in the shower drain. Maybe the muscle definition you worked years to build is quietly disappearing under the weight loss everyone keeps congratulating you for.
Here is the problem nobody warns you about when you start tirzepatide. You are eating dramatically less food. Sometimes 40 to 60 percent less than before. And while that calorie deficit drives the weight loss you wanted, it also slashes your intake of essential vitamins, minerals, protein, and micronutrients your body needs to function properly. The medication does not cause nutrient deficiencies directly. But the reduced food intake absolutely can, and often does.
This guide covers every supplement worth considering while on tirzepatide, backed by clinical evidence and practical protocols. Not generic advice. Specific dosages, timing strategies, which forms absorb best, and which supplements to avoid entirely. Whether you are just starting your tirzepatide journey or months into treatment wondering why your energy crashed, this is the reference you will keep coming back to. SeekPeptides built this resource to help researchers and users navigate the nutritional challenges that come with GLP-1 therapy, because the weight loss is only half the equation.
Why tirzepatide users need supplements in the first place
Tirzepatide works through a dual GLP-1 and GIP receptor mechanism that fundamentally changes how your body processes hunger signals. Appetite drops. Food intake plummets. Gastric emptying slows dramatically. All of this is by design. The SURMOUNT-5 trial showed participants lost an average of 20.2 percent of their body weight over 72 weeks, and that kind of transformation requires eating significantly less food for an extended period.
Think about what that means nutritionally.
If you previously ate 2,200 calories per day and now you are eating 1,200 to 1,400, you have cut your nutrient intake by roughly 40 percent. Every vitamin, every mineral, every gram of protein that came from those missing calories is now gone. Your body still needs the same micronutrient levels to maintain bone density, muscle mass, immune function, neurological health, and metabolic processes. It just has far fewer dietary sources to pull from.
The gastrointestinal side effects compound this problem. Nausea affects 17 to 22 percent of tirzepatide users during dose escalation. Vomiting hits 6 to 10 percent. Constipation and diarrhea each affect 13 to 16 percent. Every episode of nausea that makes you skip a meal, every bout of vomiting that eliminates nutrients before absorption, every day of reduced appetite where you barely eat, these all create cumulative nutritional gaps that supplements can help fill.
This is not hypothetical. A narrative review published in the journal Nutrients found that patients on GLP-1 receptor agonists face measurable risks of deficiency in vitamin B12, vitamin D, iron, calcium, magnesium, and several B vitamins. The reduced caloric intake combined with altered gastric motility creates a perfect storm for nutritional insufficiency, particularly in patients who remain on treatment for more than six months.
The difference between tirzepatide and bariatric surgery nutrition
Bariatric surgery patients receive mandatory supplementation protocols because the procedure physically alters nutrient absorption. Tirzepatide does not do this. The medication does not change your absorptive capacity. Your small intestine still works normally. What changes is the quantity and variety of food you consume.
This distinction matters because it means tirzepatide users do not need the aggressive supplementation protocols that gastric bypass patients require. But it also means there are no official FDA-mandated supplementation guidelines for tirzepatide specifically. You and your healthcare provider are largely navigating this on your own, guided by emerging clinical experience rather than established protocols.
The practical approach is targeted supplementation based on individual risk factors and blood work, not blanket megadose protocols. Get your baseline labs done before starting tirzepatide. Recheck every three to six months. Supplement where deficiencies appear or where your reduced dietary intake creates obvious gaps. That is the framework this guide follows.
Protein: the most critical supplement for tirzepatide users
If you only address one nutritional gap while on tirzepatide, make it protein. Nothing else comes close in terms of importance for preserving your health, body composition, and long-term outcomes during rapid weight loss.
Here is why this matters so much. When you lose weight through calorie restriction, roughly 20 to 30 percent of the weight lost comes from lean mass rather than fat. Clinical data from the SURMOUNT trials showed that approximately 25 percent of weight loss with tirzepatide came from lean body mass. That includes muscle tissue, bone density, and organ mass. Adequate protein intake is the single most effective dietary intervention for minimizing that lean mass loss.
How much protein you actually need
The research is clear on this. Tirzepatide users should target 0.7 to 1.0 grams of protein per pound of ideal body weight daily. For someone targeting 160 pounds, that translates to 112 to 160 grams of protein per day. Higher amounts in that range become more important if you are doing resistance training, which you absolutely should be.
The problem is obvious. If you are eating 1,200 to 1,400 calories per day due to appetite suppression, getting 130 grams of protein from whole foods alone is nearly impossible. That would mean roughly 520 calories just from protein, leaving very little room for fats, carbohydrates, fruits, vegetables, and all the other foods you need for micronutrient diversity.
This is where protein supplementation becomes essential, not optional.
Best protein sources for tirzepatide users
Whey protein isolate remains the gold standard for muscle protein synthesis, providing roughly 25 grams of protein per scoop with a complete amino acid profile and rapid absorption. For tirzepatide users specifically, whey isolate works better than whey concentrate because it contains less lactose, which matters when your digestive system is already sensitive from the medication.
Casein protein absorbs more slowly, making it ideal before bed when your body will go 8 or more hours without food. Given that many tirzepatide users already struggle with inadequate caloric intake, a casein shake before sleep provides sustained amino acid delivery overnight without requiring much appetite to consume.
Plant-based options like pea protein and soy protein isolate work well for those who do not tolerate dairy. Pea protein in particular has gained clinical support for muscle preservation comparable to whey in several studies. Blend formulations that combine multiple plant proteins can improve the amino acid profile.
Collagen peptides serve a complementary role but should not replace whey or plant proteins as your primary source. Collagen lacks several essential amino acids for muscle protein synthesis. However, it provides glycine and proline that support joint health, skin elasticity, hair strength, and connective tissue integrity, all areas that can suffer during rapid weight loss. Use collagen as an addition to your protein strategy, not a replacement.
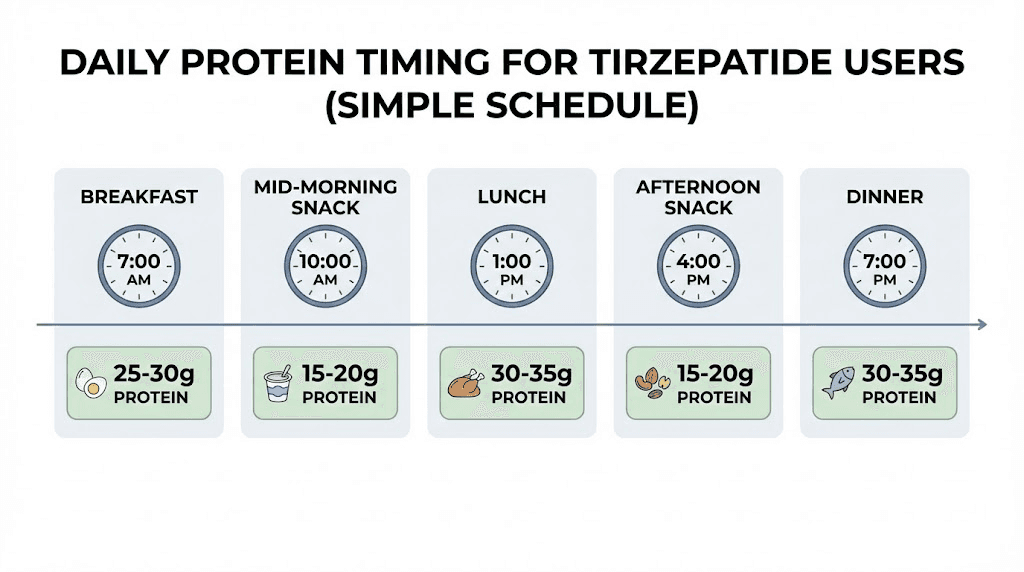
Protein timing protocol
Distribute your protein across the day rather than trying to consume it all at once. Aim for 20 to 30 grams per meal or snack. This maximizes muscle protein synthesis, which has a threshold response. Your body can only use so much protein for muscle building at one time, and the rest gets oxidized for energy.
A practical daily schedule looks like this. Morning shake with 25 to 30 grams whey or plant protein. Lunch with a protein-rich whole food source targeting 25 to 30 grams. Afternoon snack with 15 to 20 grams from a protein bar or shake. Dinner with 25 to 30 grams from whole foods. Optional bedtime casein shake with 25 grams if total intake is still below target. This structure works even on days when appetite is minimal because liquid protein sources require less appetite than solid food.
Vitamin B12: protecting your nervous system
Vitamin B12 deserves its own section because the deficiency risk with GLP-1 medications is well-documented and the consequences are serious. B12 is essential for nerve function, red blood cell formation, DNA synthesis, and energy metabolism. Deficiency causes fatigue, neurological symptoms including numbness and tingling, cognitive impairment, and megaloblastic anemia.
GLP-1 receptor agonists like tirzepatide slow gastric emptying, which may reduce B12 absorption over time. The mechanism involves altered intrinsic factor secretion and changes in gastric acid production, both of which are required for B12 absorption in the small intestine. Studies on metformin, another diabetes medication that affects B12 absorption, show deficiency rates of 5 to 30 percent with long-term use. Early data on GLP-1 medications suggests a similar pattern may emerge.
The compounding factor for tirzepatide users is reduced dietary intake. The primary dietary sources of B12 are animal products, specifically meat, fish, eggs, and dairy. If your overall food intake has dropped significantly, your B12 intake from food has dropped proportionally. Combine reduced dietary intake with potentially impaired absorption, and you have a legitimate deficiency risk that warrants proactive supplementation.
B12 dosage and form
A daily supplement of 500 to 1,000 mcg of methylcobalamin provides adequate coverage for most tirzepatide users. Methylcobalamin is the active, bioavailable form that your body can use immediately without conversion. Cyanocobalamin is cheaper but requires hepatic conversion and may not be optimal for people with MTHFR gene variations.
Sublingual forms dissolve under the tongue and bypass the GI tract entirely, which matters when gastric emptying is slowed. This route provides more reliable absorption than oral tablets that must pass through the same delayed digestive system the medication creates.
If blood work reveals significant B12 deficiency below 300 pg/mL, discuss intramuscular B12 injections with your healthcare provider. Weekly injections of 1,000 mcg can correct deficiency faster than oral supplementation, with monthly maintenance injections thereafter. Many tirzepatide providers now offer compounded formulations that include B12 directly in the injection for this exact reason.
Vitamin D: more than just bone health
Vitamin D deficiency is already epidemic in the general population. Roughly 35 percent of American adults have insufficient levels. For tirzepatide users, the risk increases because vitamin D is a fat-soluble vitamin obtained primarily through fatty fish, fortified dairy, eggs, and sun exposure. When caloric intake drops, dietary vitamin D drops with it.
The connection between vitamin D and weight loss medications runs deeper than simple dietary reduction. Adipose tissue stores vitamin D. As you lose body fat, stored vitamin D is released into the bloodstream, which can initially create a false sense of adequacy on blood tests. Once the stored reserves deplete, levels can drop rapidly. This delayed deficiency pattern means you might test fine at three months but show deficiency at six or nine months.
What vitamin D actually does for tirzepatide users
Beyond bone health, vitamin D plays critical roles in glucose metabolism, immune function, and muscle strength, all areas directly relevant to people on tirzepatide protocols. Research shows that adequate vitamin D status improves insulin sensitivity, which complements the metabolic benefits of tirzepatide. Deficiency has been linked to increased insulin resistance, reduced muscle strength, higher inflammation, impaired immune response, and increased risk of depression.
For people losing significant weight, vitamin D adequacy also supports bone density maintenance. Rapid weight loss increases fracture risk, and vitamin D plus calcium provides the foundational support bones need during this vulnerable period.
Dosage protocol for vitamin D
Most adults benefit from 1,000 to 2,000 IU of vitamin D3 daily as a maintenance dose. This is the form your skin naturally produces from sunlight and converts more efficiently than vitamin D2. Take it with your fattiest meal of the day since it requires dietary fat for absorption.
If blood work shows your 25-hydroxyvitamin D level is below 30 ng/mL, your provider may recommend a loading dose of 5,000 to 10,000 IU daily for 8 to 12 weeks to correct the deficiency, followed by a maintenance dose of 2,000 to 4,000 IU daily. Never megadose vitamin D without blood work confirmation and medical supervision. Vitamin D toxicity is rare but real, and can cause hypercalcemia with kidney damage.
Consider pairing vitamin D3 with vitamin K2 (MK-7 form, 100 to 200 mcg daily). K2 directs calcium into bones where it belongs rather than allowing it to deposit in arteries and soft tissues. This combination provides significantly better bone health outcomes than vitamin D alone.
Calcium: defending your bones during weight loss
Rapid weight loss increases bone turnover and fracture risk. This is well-established in the bariatric surgery literature, and the same principles apply to medication-assisted weight loss. The mechanical loading on bones decreases as body weight drops, and if calcium intake is simultaneously inadequate, bone density can decline faster than it should.
The target is 1,000 to 1,200 mg of calcium daily from all sources combined, including food and supplements. Most adults get 300 to 500 mg from food alone, meaning a supplement providing 500 to 700 mg fills the gap effectively.
Choosing the right calcium form
Calcium citrate absorbs well with or without food and is generally better tolerated than calcium carbonate, which requires stomach acid for absorption and can cause constipation, a side effect you do not need when tirzepatide is already slowing your digestive system. Do not take more than 500 mg of calcium at one time. Split doses improve absorption significantly.
Important interaction: separate calcium supplements from iron supplements and thyroid medications by at least two to four hours. Calcium blocks absorption of both.
Magnesium: the overlooked essential
Magnesium is involved in over 300 enzymatic reactions in the body, including energy production, muscle contraction, nerve signaling, protein synthesis, and blood sugar regulation. Deficiency causes muscle cramps, poor sleep, irritability, constipation, and fatigue, symptoms that overlap with and compound the side effects of tirzepatide itself.
An estimated 50 percent of the US population already consumes inadequate magnesium. When you layer reduced food intake on top of that baseline insufficiency, the gap widens quickly. Tirzepatide users who experience persistent muscle cramps, restless legs, difficulty sleeping, or worsening constipation should evaluate magnesium status as a first step.
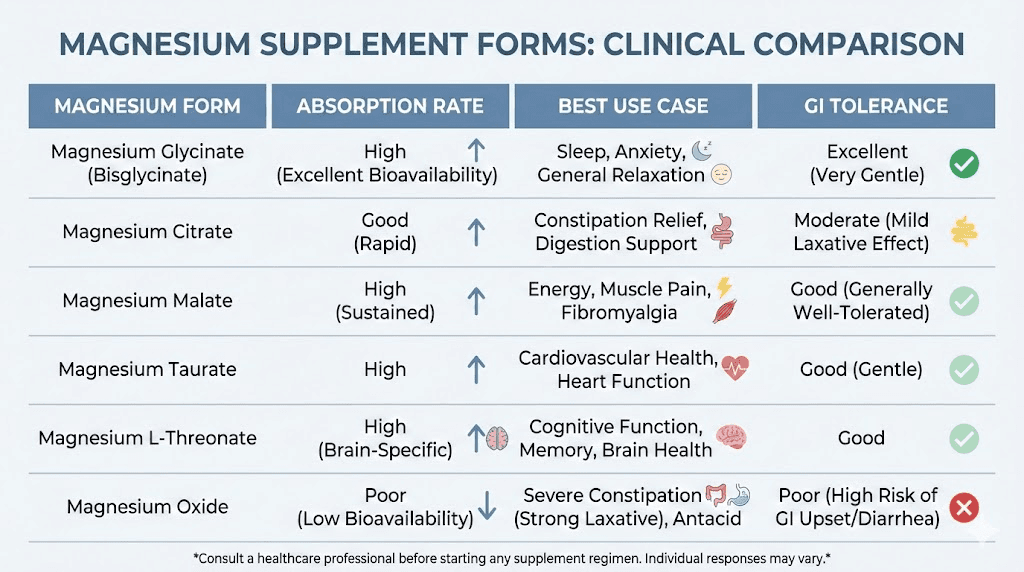
Magnesium forms and dosage
Not all magnesium supplements are equal. The form matters significantly.
Magnesium glycinate (200 to 400 mg daily) is the best choice for most tirzepatide users. It absorbs well, rarely causes GI upset, and the glycine component has calming effects that improve sleep quality. Take it in the evening.
Magnesium citrate (200 to 400 mg daily) absorbs well and has a mild laxative effect. For tirzepatide users dealing with constipation, this dual benefit makes it a strategic choice. However, if you are already experiencing diarrhea as a side effect, avoid this form.
Magnesium oxide is cheap and widely available but absorbs poorly. Only about 4 percent of the magnesium is bioavailable. Skip this form unless cost is the only factor and you are taking it specifically as a laxative.
Magnesium L-threonate crosses the blood-brain barrier and may support cognitive function, but it provides less elemental magnesium per dose and costs significantly more. Consider it if cognitive fog is a prominent symptom.
The upper limit for supplemental magnesium is 350 mg daily from supplements. Higher doses can cause diarrhea and should only be used under medical supervision.
Omega-3 fatty acids: cardiovascular and metabolic support
Tirzepatide already provides cardiovascular benefits through weight loss and improved metabolic markers. Omega-3 supplementation complements these effects through independent anti-inflammatory, triglyceride-lowering, and cardioprotective mechanisms.
The recommended dose is 1,000 to 2,000 mg of combined EPA and DHA daily. EPA (eicosapentaenoic acid) drives the anti-inflammatory and cardiovascular benefits. DHA (docosahexaenoic acid) supports brain health and neurological function. Look for supplements that list specific EPA and DHA amounts rather than just total fish oil, because a 1,000 mg fish oil capsule might only contain 300 mg of combined EPA and DHA.
For tirzepatide users specifically, omega-3s offer three relevant benefits beyond general cardiovascular support. First, they may help maintain insulin sensitivity during weight loss, complementing the metabolic improvements from the medication. Second, the anti-inflammatory effects can reduce systemic inflammation that often accompanies both obesity and rapid weight loss. Third, omega-3s support skin and hair health, which can suffer during significant weight loss due to nutrient redistribution.
Quality and sourcing considerations
Choose omega-3 supplements with third-party purity testing. Fish oil can concentrate heavy metals, PCBs, and other environmental contaminants. Look for USP Verified, NSF Certified, or IFOS (International Fish Oil Standards) certifications. Triglyceride form fish oil absorbs better than ethyl ester form, though both provide clinical benefit.
If you experience fishy burps or GI upset, try enteric-coated capsules, refrigerate the supplement, or take it with your largest meal. Algae-based omega-3 supplements provide a plant-based alternative that avoids the fishy aftertaste entirely while still delivering meaningful EPA and DHA levels.
One important caution: doses above 3,000 mg of combined EPA and DHA daily have been associated with increased atrial fibrillation risk in some studies. Stay within the 1,000 to 2,000 mg range unless your cardiologist specifically recommends higher dosing for severe hypertriglyceridemia.
Iron: supplement only when confirmed deficient
Iron occupies a unique position in the supplement discussion because both deficiency and excess cause problems. Iron deficiency leads to anemia, fatigue, poor exercise tolerance, and impaired cognitive function. Iron overload damages the liver, heart, and pancreas. This is why iron supplementation should never be started without laboratory confirmation of deficiency.
Tirzepatide users face iron deficiency risk through two pathways. Reduced dietary intake means less iron from food sources, particularly if red meat consumption has declined. And the fatigue associated with GLP-1 therapy may mask early symptoms of iron deficiency anemia, delaying diagnosis.
Getting tested and supplementing correctly
Request a complete iron panel including serum iron, ferritin, TIBC (total iron-binding capacity), and transferrin saturation. Ferritin alone can be misleading because it is an acute phase reactant that rises with inflammation regardless of iron status.
If deficiency is confirmed, standard supplementation is 325 mg of ferrous sulfate (65 mg elemental iron) once daily on an empty stomach. Iron absorbs best with vitamin C, so taking it with orange juice or a 250 mg vitamin C tablet enhances uptake. Avoid taking iron with calcium, coffee, tea, or high-fiber foods, all of which significantly reduce absorption.
Iron supplementation commonly causes constipation and stomach upset. For tirzepatide users already managing GI side effects, iron bisglycinate may be better tolerated. It provides comparable iron delivery with substantially less GI irritation. Doses of 25 to 28 mg elemental iron from bisglycinate daily often achieve adequate correction without the digestive burden.
Fiber: managing the constipation equation
Constipation is one of the most common and persistent side effects of tirzepatide treatment. The slowed gastric emptying that reduces appetite also slows colonic motility. When you combine this with dramatically reduced food volume (and therefore reduced dietary fiber), the result is often significant constipation that worsens over time if not addressed.
The daily fiber target is 25 to 30 grams. Most Americans get 15 grams on a full diet. On a calorie-restricted tirzepatide diet, you might be getting 8 to 10 grams. Supplementation bridges this gap.
Best fiber supplements for tirzepatide users
Psyllium husk (Metamucil or generic) is the most versatile option. It forms a gel that softens stool, promotes regular bowel movements, and as a bonus, helps stabilize blood sugar and reduce cholesterol. Start with one teaspoon daily and gradually increase to one tablespoon. Always take with at least 8 ounces of water.
Methylcellulose (Citrucel) is less likely to cause gas and bloating than psyllium, making it better tolerated for tirzepatide users already dealing with GI sensitivity. It dissolves more completely and produces less fermentation in the colon.
Partially hydrolyzed guar gum (Sunfiber) is a well-tolerated prebiotic fiber that normalizes bowel function in both directions, helping with constipation and diarrhea. It dissolves completely in beverages without changing texture and produces minimal gas.
Critical guidance: introduce fiber supplements gradually. Adding 15 grams of fiber overnight to a sensitive GI system will cause bloating, cramping, and gas. Increase by no more than 5 grams every three to five days. And hydrate aggressively. Fiber without adequate water makes constipation worse, not better.
Electrolytes: preventing dehydration and imbalance
Tirzepatide users are at increased risk for electrolyte imbalance through multiple pathways. Reduced food intake means reduced dietary electrolytes. GI side effects including vomiting and diarrhea cause direct electrolyte losses. And the mild diuretic effect that sometimes accompanies significant weight loss further depletes sodium, potassium, and magnesium stores.
Symptoms of electrolyte imbalance include muscle cramps, fatigue, dizziness, headaches, heart palpitations, and brain fog. These symptoms overlap extensively with common tirzepatide side effects, making electrolyte depletion easy to miss and difficult to distinguish from medication-related effects.
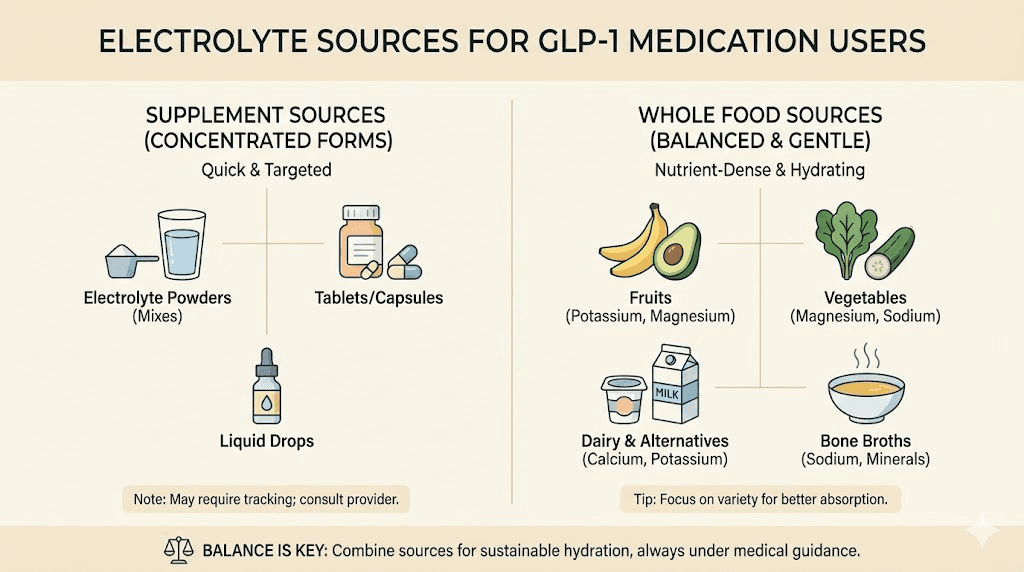
Practical electrolyte strategy
A daily electrolyte supplement or sugar-free electrolyte powder provides sodium, potassium, and magnesium in balanced ratios. Look for products containing at least 500 to 1,000 mg sodium, 200 to 400 mg potassium, and 50 to 100 mg magnesium per serving. Avoid electrolyte products loaded with sugar, artificial sweeteners, or stimulants.
You can also increase electrolyte intake through food choices. Avocados, bananas, spinach, and sweet potatoes provide potassium. Bone broth provides sodium and collagen. Nuts and seeds provide magnesium. But when appetite is suppressed and total food volume is low, a dedicated electrolyte supplement provides reliable coverage that food intake alone may not.
Pay particular attention to hydration if you experience vomiting or diarrhea during dose escalation phases. These episodes can cause rapid electrolyte depletion that exacerbates nausea and creates a cycle of worsening symptoms. Keep electrolyte beverages on hand during titration weeks as a preventive measure.
Ginger root extract: evidence-based nausea management
Nausea is the side effect that drives the most treatment discontinuation with GLP-1 medications. If you cannot tolerate the medication, you cannot benefit from it. Ginger root extract has robust clinical evidence for reducing nausea through multiple mechanisms, including accelerating gastric emptying and modulating serotonin receptors in the gut.
A dose of 500 to 1,000 mg of ginger root extract taken 30 minutes before meals can meaningfully reduce nausea frequency and severity. The evidence base comes primarily from chemotherapy-induced nausea and pregnancy-related morning sickness studies, where ginger consistently outperforms placebo. The mechanism translates directly to GLP-1-related nausea because the underlying pathophysiology involves similar serotonin and vagal nerve pathways.
Standardized ginger extract capsules provide consistent dosing. Fresh ginger tea works but delivers variable amounts of the active gingerol compounds. Ginger chews and candies can help in the moment but typically contain too much sugar and too little ginger to provide reliable therapeutic benefit.
Important note: ginger has mild blood-thinning properties. If you take anticoagulants like warfarin, discuss ginger supplementation with your healthcare provider before starting. For most tirzepatide users, the doses recommended here are safe and well-tolerated.
Probiotics: supporting gut health through transition
Tirzepatide fundamentally alters the gastrointestinal environment. Slowed gastric emptying, changes in bile acid metabolism, shifts in food intake patterns, and potential antibiotic use for side effect management all affect the gut microbiome. Probiotic supplementation can help maintain microbial diversity and resilience during this transition period.
Look for multi-strain formulations containing both Lactobacillus and Bifidobacterium species with at least 10 to 30 billion colony-forming units (CFUs). The diversity of strains matters more than the total CFU count. A product with 15 billion CFUs across 10 strains typically outperforms one with 50 billion CFUs of a single strain.
What the evidence actually shows
Research on probiotics and GLP-1 medications specifically is limited but growing. The theoretical basis is sound. The gut microbiome influences GLP-1 production naturally, and maintaining microbial diversity may support the medication mechanisms. Practically, probiotics help manage the constipation, bloating, and irregular bowel patterns that many tirzepatide users experience.
The most studied strains for GI symptom management include Lactobacillus acidophilus, Lactobacillus rhamnosus GG, Bifidobacterium lactis, and Saccharomyces boulardii. The last one, S. boulardii, is particularly useful during episodes of GI distress because it is a beneficial yeast that survives antibiotic treatment and helps prevent diarrhea.
Take probiotics at least 30 minutes before a meal or at bedtime on an empty stomach for optimal survival through gastric acid. Refrigerated formulations generally maintain higher potency than shelf-stable versions, though modern encapsulation technology has improved shelf-stable survival rates significantly.
Creatine: preserving muscle mass and strength
Creatine monohydrate is the most researched supplement in sports science history, with decades of evidence supporting its safety and efficacy for preserving lean muscle mass. For tirzepatide users, creatine serves a specific and important purpose: helping maintain the muscle tissue that rapid weight loss threatens.
The mechanism is straightforward. Creatine increases phosphocreatine stores in muscle cells, which supports ATP production during resistance exercise. This means better workout performance, faster recovery, and improved muscle protein synthesis response to training. When you are in a caloric deficit on tirzepatide, every advantage for muscle preservation matters.
Dosage and timing
Take 3 to 5 grams of creatine monohydrate daily. No loading phase is necessary. Loading protocols (20 grams daily for a week) saturate stores faster but cause GI bloating that tirzepatide users should avoid. Daily dosing of 3 to 5 grams reaches full saturation within three to four weeks without the GI side effects.
Timing does not matter much. Take it whenever you can consistently remember. With a meal, with your protein shake, or in water on its own. Consistency trumps timing for creatine. The one exception: if you are resistance training (which you should be), taking creatine with your post-workout protein shake combines two muscle-preserving interventions in one convenient window.
Creatine monohydrate is the only form with robust evidence. Creatine HCL, buffered creatine, creatine ethyl ester, and other premium-priced variants have not demonstrated superiority in clinical studies. Save your money and buy micronized creatine monohydrate from a reputable brand with third-party testing.
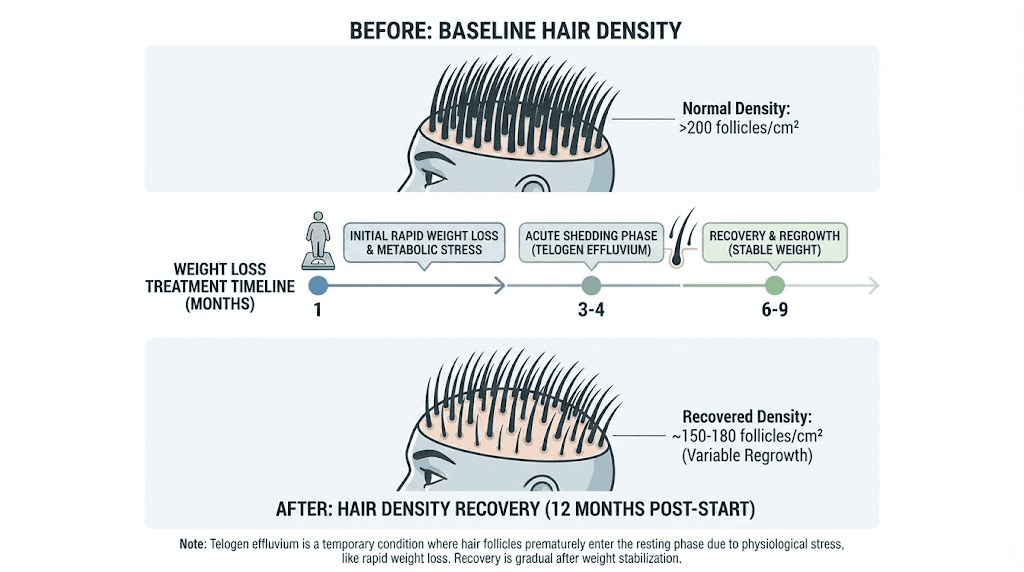
Biotin and zinc: addressing hair thinning
Hair thinning during tirzepatide treatment is one of the most distressing side effects, even though it is not caused by the medication directly. Telogen effluvium, the temporary hair shedding triggered by rapid weight loss, nutritional changes, or physiological stress, affects a meaningful percentage of people on GLP-1 medications. The hair loss typically begins two to four months after significant weight loss starts and can continue for several months.
The good news: it is almost always temporary. Hair regrows within 6 to 12 months after the trigger stabilizes. But nutritional support can minimize the severity and accelerate recovery.
Biotin: helpful but overhyped
Biotin (vitamin B7) is marketed aggressively for hair health. The reality is more nuanced. If you are biotin deficient, supplementation absolutely helps hair quality and growth. But multiple dermatology reviews show no benefit from biotin supplementation in people with normal biotin levels. Since reduced food intake during tirzepatide treatment can reduce biotin intake, a modest supplement of 2,500 to 5,000 mcg daily provides insurance without risk.
One important caveat: biotin in high doses interferes with common laboratory tests, including thyroid panels, troponin (cardiac markers), and hormone levels. Discontinue biotin supplements 48 to 72 hours before any blood work to avoid falsely elevated or depressed results. This is not a theoretical concern. It has caused misdiagnoses and unnecessary procedures.
Zinc for hair and immune support
Zinc plays a direct role in hair follicle health, protein synthesis, and immune function. Deficiency causes hair loss, impaired wound healing, weakened immunity, and altered taste perception. The recommended supplement dose is 15 to 30 mg of zinc daily, taken with food to minimize nausea.
Zinc picolinate and zinc glycinate absorb better than zinc oxide. If you are taking a multivitamin that already contains 15 mg of zinc, you likely do not need additional supplementation unless blood work shows deficiency.
Important: long-term zinc supplementation above 40 mg daily can cause copper deficiency. If you supplement zinc for more than three months, consider adding 1 to 2 mg of copper or choose a supplement that includes both minerals in appropriate ratios.
B-complex vitamins: energy metabolism support
Beyond B12, the entire B-vitamin family supports energy metabolism, neurological function, and cellular processes that become more demanding during rapid weight loss. Thiamine (B1), riboflavin (B2), niacin (B3), pantothenic acid (B5), pyridoxine (B6), and folate (B9) all play interconnected roles in converting the food you eat into cellular energy.
For tirzepatide users eating significantly less food, a comprehensive B-complex supplement provides blanket coverage across all B vitamins. This is one area where a preventive approach makes sense because B vitamin deficiencies develop gradually, cause nonspecific symptoms that mimic tirzepatide side effects, and are easily prevented with inexpensive supplementation.
Thiamine deserves special attention
Thiamine (B1) deficiency risk increases specifically with prolonged vomiting and very low caloric intake, two situations common during tirzepatide titration. Severe thiamine deficiency causes Wernicke encephalopathy, a neurological emergency. While this extreme outcome is rare with GLP-1 medications, subclinical thiamine insufficiency causing fatigue, irritability, and poor concentration is much more common.
A standard B-complex supplement providing 50 to 100 mg of thiamine, along with balanced amounts of other B vitamins, covers this risk. Take it with food to improve absorption and reduce nausea. B vitamins can cause bright yellow urine. This is harmless and simply indicates excess riboflavin (B2) excretion.
A complete multivitamin: the safety net approach
A high-quality daily multivitamin serves as nutritional insurance for tirzepatide users. It does not replace targeted supplementation for specific deficiencies, but it provides baseline coverage across dozens of micronutrients that might otherwise fall through the gaps of a calorie-restricted diet.
Choose a multivitamin designed for your demographic (men vs women, age-appropriate formulations). Look for third-party testing certifications like USP Verified or NSF Certified. Avoid formulations with mega-doses of individual nutrients, excessive iron (unless you are a menstruating woman or confirmed deficient), or proprietary blends with undisclosed amounts.
The multivitamin anchors your supplement strategy. It handles the dozens of trace minerals and vitamins you cannot realistically track individually, things like selenium, chromium, manganese, copper, vitamins A, C, E, and K. Then your targeted supplements (protein, D3, B12, magnesium, omega-3) address the specific high-risk deficiency areas at therapeutic doses that a multivitamin alone cannot provide.
Supplements to avoid while on tirzepatide
Not every supplement is safe or beneficial during tirzepatide treatment. Some can cause dangerous interactions, worsen side effects, or undermine the medication benefits.
Herbal hypoglycemic supplements
Berberine, bitter melon, fenugreek, gymnema sylvestre, and alpha-lipoic acid all have blood sugar lowering effects. When combined with tirzepatide, which already powerfully reduces blood glucose, the additive effect can cause hypoglycemia, dangerously low blood sugar that causes shakiness, confusion, sweating, and in severe cases, loss of consciousness.
If you are taking tirzepatide for type 2 diabetes and also using insulin or sulfonylureas, the hypoglycemia risk from these herbal supplements becomes even more dangerous. Stop all herbal blood sugar supplements before starting tirzepatide and discuss any changes with your prescribing provider.
Stimulant weight loss supplements
Products containing caffeine, synephrine, yohimbine, or other stimulants marketed for weight loss provide no additional benefit when you are already on tirzepatide. The appetite suppression is handled by the medication. These stimulants add cardiovascular risk (elevated heart rate, blood pressure spikes) without meaningful incremental weight loss benefit. The risk-to-reward ratio is terrible.
High-dose single antioxidants
Megadoses of vitamin C (above 2,000 mg daily) or vitamin E (above 400 IU daily) lack evidence for benefit in tirzepatide users and may cause harm. High-dose vitamin E has been associated with increased bleeding risk. High-dose vitamin C causes GI upset and kidney stone risk. Normal dietary amounts and multivitamin levels are fine. Megadosing is not.
Appetite stimulants
This should be obvious, but supplements marketed to increase appetite (certain strains of marijuana-derived compounds, appetite-stimulating herbs) directly counteract the therapeutic mechanism of tirzepatide. If your appetite suppression is so severe that you cannot eat enough to meet basic nutritional needs, discuss dose adjustment with your provider rather than trying to chemically override the medication.
Timing your supplements around tirzepatide injections
Because tirzepatide is injected subcutaneously rather than taken orally, there is no direct absorption interaction between the injection and oral supplements. You do not need to separate your supplements from injection day in the way you would with oral medications. However, there are still strategic timing considerations worth understanding.
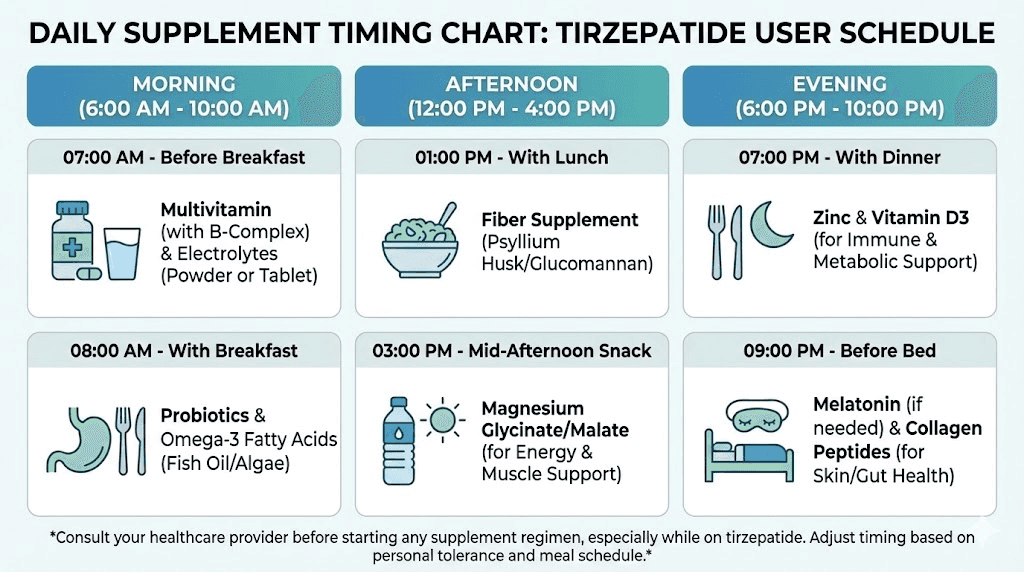
Daily supplement timing framework
Morning with breakfast: Multivitamin, B-complex, vitamin D3 with K2 (with food containing fat), first protein serving, omega-3 (with food)
Between meals: Protein shake as needed, electrolytes
With lunch or dinner: Calcium citrate (first dose), iron (if prescribed, separate from calcium by 2 hours), zinc (with food)
Evening: Magnesium glycinate (30 to 60 minutes before bed), calcium citrate (second dose if splitting), casein protein (optional bedtime shake), probiotics (bedtime on empty stomach)
During dose escalation weeks
The first one to two weeks after each dose increase typically bring the worst GI side effects. During these windows, prioritize the supplements that manage symptoms. Ginger extract 30 minutes before meals. Electrolytes throughout the day. Fiber adjusted carefully. Protein in liquid form since it requires less appetite than solid food.
If nausea makes taking multiple supplements impossible, prioritize in this order: protein (most critical for muscle preservation), electrolytes (prevent dehydration), multivitamin (baseline coverage), and then everything else as tolerated. You can temporarily reduce supplement volume during the worst days and resume full protocols once GI symptoms stabilize, typically within two to three weeks of each dose adjustment.
The complete tirzepatide supplement protocol
Here is everything organized into a practical daily protocol. This represents the evidence-based ideal. Your actual protocol should be customized based on blood work, symptoms, dietary intake, and healthcare provider guidance.
Tier 1: essential for nearly all tirzepatide users
These supplements address the most common and consequential nutritional gaps.
Protein supplement: 25 to 50 grams daily from whey isolate, plant protein, or casein, targeting total intake of 0.7 to 1.0 grams per pound of ideal body weight from all sources
Vitamin D3 with K2: 1,000 to 2,000 IU D3 plus 100 to 200 mcg K2 (MK-7) daily, taken with fat-containing meal
Vitamin B12: 500 to 1,000 mcg methylcobalamin daily, sublingual preferred
Magnesium glycinate or citrate: 200 to 400 mg daily, taken in the evening
Daily multivitamin: High-quality, third-party tested, age and gender appropriate
Fiber supplement: 5 to 15 grams daily, gradually increased, with adequate water
Tier 2: strongly recommended based on individual factors
These supplements provide meaningful benefit for most users but may not be necessary for everyone.
Omega-3 fatty acids: 1,000 to 2,000 mg combined EPA and DHA daily
Calcium citrate: 500 to 700 mg daily in split doses, especially for women and those over 50
Creatine monohydrate: 3 to 5 grams daily, especially for those doing resistance training
Electrolyte supplement: Daily during dose escalation, as needed during maintenance
Probiotics: 10 to 30 billion CFUs multi-strain, especially during first three months
Tier 3: targeted supplementation based on symptoms
Add these only when specific symptoms or blood work indicate a need.
Ginger root extract: 500 to 1,000 mg before meals for nausea management
B-complex: 50 to 100 mg thiamine with balanced B vitamins for energy support
Biotin: 2,500 to 5,000 mcg daily for hair thinning (stop 48 hours before blood work)
Zinc: 15 to 30 mg daily for hair thinning or immune support (add copper if long-term)
Iron: Only with confirmed deficiency, 25 to 65 mg elemental iron with vitamin C
Collagen peptides: 10 to 15 grams daily for skin, hair, joint support
Getting your blood work done: the tests that matter
Supplement protocols without blood work are guessing games. The following tests provide the baseline data you need to supplement intelligently rather than blindly.
Before starting tirzepatide: Complete blood count (CBC), comprehensive metabolic panel (CMP), vitamin D (25-hydroxyvitamin D), vitamin B12, complete iron panel (serum iron, ferritin, TIBC, transferrin saturation), magnesium (RBC magnesium is more accurate than serum magnesium), thyroid panel (TSH, free T3, free T4), lipid panel, HbA1c
At three-month intervals: CBC, CMP, vitamin D, B12, and any previously deficient markers. Add iron panel if fatigue is prominent. Add magnesium if muscle cramps or poor sleep persist.
At six months and annually: Full panel repeat. This is when fat-soluble vitamin stores may begin depleting after initial reserves are used up. Bone density screening (DEXA scan) should be discussed with your provider if you have lost more than 10 percent of body weight.
Bring your supplement list to every blood work review. Your provider needs to know what you are taking to interpret results correctly, especially given the biotin interference issue with laboratory tests mentioned earlier.
How SeekPeptides members optimize their supplement protocols
SeekPeptides provides comprehensive resources for researchers navigating the intersection of peptide therapy and nutritional optimization. Members access detailed supplement protocols tailored to specific GLP-1 medications, including tirzepatide with B12 combinations, glycine formulations, and niacinamide protocols. The platform also offers calculators to help determine precise dosing, including the semaglutide dosage calculator and tirzepatide dosage calculator that thousands of users rely on for accurate protocol planning.
Frequently asked questions
Can I take all my supplements at the same time as tirzepatide?
Yes. Since tirzepatide is injected subcutaneously rather than taken orally, there is no direct absorption interaction with oral supplements. However, spreading your supplements across the day improves individual absorption. Fat-soluble vitamins with meals, magnesium in the evening, and calcium in split doses throughout the day. The injection timing itself does not affect supplement absorption.
Do I need supplements if I eat a healthy diet on tirzepatide?
Even with excellent food choices, the reduced caloric intake on tirzepatide makes it difficult to meet all micronutrient needs through food alone. At 1,200 to 1,400 calories per day, you would need every single calorie to come from nutrient-dense whole foods to approach adequate vitamin and mineral intake. Protein supplementation in particular is almost always necessary because meeting protein targets through food alone at reduced calorie levels is extremely challenging. A well-planned tirzepatide diet helps but rarely eliminates the need for supplementation entirely.
How long should I take supplements while on tirzepatide?
Continue supplementation for the entire duration of tirzepatide treatment and for at least three to six months after discontinuation. The nutritional gaps created by reduced food intake do not resolve immediately when the medication stops. Your body needs time to rebuild stores. Use blood work to determine when individual supplements can be safely reduced or discontinued.
Will supplements reduce tirzepatide effectiveness?
The supplements recommended in this guide do not interfere with tirzepatide efficacy. However, herbal blood sugar supplements like berberine or bitter melon can create dangerous blood sugar drops. Appetite-stimulating supplements counteract the medication mechanism. Stick to the evidence-based supplements listed here and avoid anything marketed to alter blood sugar or appetite independently.
What is the most important supplement if I can only afford one?
Protein. Without question. Preserving lean muscle mass during weight loss determines your metabolic health, physical function, body composition, and long-term maintenance success more than any other single factor. A quality protein powder costs roughly 50 to 80 cents per serving and delivers more measurable benefit per dollar than any other supplement for tirzepatide users. Everything else is secondary to meeting your protein targets.
Should I start all supplements at once when beginning tirzepatide?
No. Start with protein, a multivitamin, and electrolytes from the beginning. Add magnesium and fiber in the first week or two as GI side effects become apparent. Layer in vitamin D, B12, and omega-3 over the first month. Add targeted supplements (zinc, biotin, ginger, probiotics) only as specific needs emerge. This staged approach lets you identify which supplements your body tolerates well and which ones might contribute to GI symptoms during the sensitive early treatment period.
Can I take supplements that my friend recommended who is also on tirzepatide?
What works for one person may not work for another. Individual supplement needs depend on baseline nutritional status, dietary intake, existing health conditions, other medications, genetic variations in nutrient metabolism, and how your body responds to tirzepatide specifically. Use blood work and healthcare provider guidance to customize your protocol. Your friend may need iron supplementation while your iron levels are perfectly fine, or vice versa.
Are there any supplements that help with tirzepatide fatigue?
Fatigue during tirzepatide treatment often stems from multiple factors simultaneously. Low caloric intake, B12 insufficiency, iron deficiency, dehydration, electrolyte imbalance, and poor sleep quality can all contribute. A B-complex vitamin, adequate protein, electrolytes, and magnesium glycinate (for sleep quality) address the most common nutritional causes. If fatigue persists despite supplementation, blood work for thyroid function, iron status, and B12 levels should be prioritized.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your supplements stay effective, your protein stay adequate, and your tirzepatide results stay strong.