Feb 15, 2026

You did everything right. You followed the titration schedule. You adjusted your meals. You stayed patient through the nausea, the appetite changes, the early weeks of figuring out how your body responds to semaglutide. And then it hit. Not a dramatic side effect. Not something that sent you rushing to urgent care. Something quieter, more persistent, and far more frustrating. Constipation. The kind where days pass without a bowel movement. The kind where you feel bloated, heavy, and uncomfortable no matter what you eat. The kind that makes you wonder whether this medication is actually worth it.
You are not alone. Not even close.
Clinical data from the STEP 1 through STEP 3 trials show that constipation affects up to 24.2% of people taking semaglutide 2.4 mg, compared to just 11.1% on placebo. That means roughly one in four people on a therapeutic weight loss dose will deal with this problem. And while 99.5% of gastrointestinal adverse events in those trials were classified as non-serious, anyone who has gone five days without a bowel movement knows that "non-serious" does not mean "not miserable." The good news is that semaglutide constipation is both well-understood and highly treatable. The mechanisms behind it are clear. The remedies are proven. And with the right approach, most people can manage this side effect without interrupting their treatment. This guide covers every evidence-based strategy available, from simple hydration adjustments to advanced interventions, so you can find what works for your body and get back to feeling like yourself. Resources from SeekPeptides can help you navigate the full landscape of peptide and GLP-1 safety considerations as you work through this process.
Why semaglutide causes constipation
Understanding the mechanism is not just academic. It matters because the treatment you choose should target the specific pathway causing your constipation. Semaglutide is a GLP-1 receptor agonist, and GLP-1 receptors exist throughout the entire digestive tract. When semaglutide binds to those receptors, it triggers a cascade of changes in how your gut moves, absorbs, and processes food.
The primary mechanism is delayed gastric emptying. Semaglutide slows the rate at which food leaves your stomach and enters the small intestine. This is actually one of the reasons the drug works so well for fat loss and blood sugar control. Slower emptying means more gradual glucose absorption, longer satiety signals, and reduced appetite. But that same slowing extends beyond the stomach.
GLP-1 receptors in the colon alter colonic motility directly. When semaglutide activates these receptors, it reduces peristalsis, the coordinated muscular contractions that push waste material through your intestines. Fewer contractions mean slower transit. Slower transit means the colon has more time to absorb water from the stool. More water absorbed means harder, drier stool that is more difficult to pass. This mechanism differs from how other peptides affect the gut, BPC-157 for example works on entirely different pathways involving tissue repair and healing rather than motility suppression.
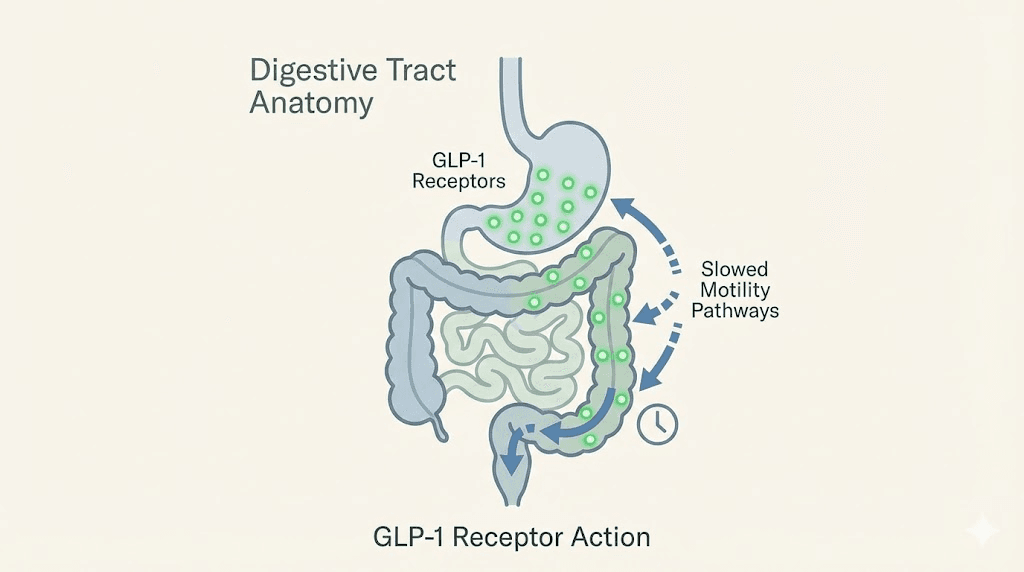
There is another layer to this. Semaglutide inhibits postprandial antral contractions and accelerates pyloric pressure waves. In plain language, the stomach does not churn food as aggressively after meals, and the valve between the stomach and small intestine creates more resistance. Food sits longer. Digestion slows. Everything downstream slows with it.
The reduced intake factor
Here is something most guides miss entirely. Semaglutide dramatically suppresses appetite. When you eat less food, you consume less fiber. Less fiber means less bulk in the stool. Less bulk means weaker peristaltic signals. Your colon essentially receives less "raw material" to work with, and the result is infrequent, difficult bowel movements.
The same goes for fluid intake. Many people on semaglutide simply do not drink enough water because they do not feel thirsty. They are eating smaller meals, often skipping meals entirely, and their overall fluid consumption drops without them realizing it. Dehydration is one of the fastest routes to constipation even without a GLP-1 medication involved. Add semaglutide to the picture and the effect compounds.
Research also suggests that long-term GLP-1 receptor agonist use may elevate GLP-2 release, which affects intestinal growth and absorption patterns. This is a subtler mechanism, but it may contribute to changes in bowel habits over extended treatment periods. Understanding all of these pathways helps explain why a single remedy rarely solves the problem. Effective semaglutide side effect management requires addressing multiple factors simultaneously.
The dose-dependent pattern
Constipation risk rises with dose. The STEP 2 trial demonstrated this clearly. At the 2.4 mg dose, 63.5% of participants reported at least one gastrointestinal adverse event. At 1.0 mg, that number was 57.5%. The relationship is not linear, but it is consistent. Higher doses produce more GLP-1 receptor activation, more motility suppression, and more constipation. This is why the standard semaglutide dosage protocol involves gradual titration. Starting at 0.25 mg and increasing every four weeks gives the gut time to adapt. Rapid dose escalation is one of the most common triggers for severe constipation, and in some cases, it can contribute to gastroparesis risk.
If you are working through your semaglutide dosage chart and notice constipation worsening at a particular dose, that information is valuable. It does not necessarily mean you need to stop. It means you need a more aggressive constipation management strategy at that dose level.
How common is semaglutide constipation
Numbers matter. They tell you whether your experience is normal, whether you should worry, and whether the problem is likely to resolve on its own. If you are trying to understand how semaglutide works on your body, the clinical trial data on constipation is extensive and paints a clear picture.
In the pooled analysis of STEP trials 1 through 3, constipation was reported in 24.2% of participants taking semaglutide 2.4 mg weekly, versus 11.1% in the placebo group. That is a meaningful difference. It tells us that while some baseline constipation exists in any population (hence the 11.1% placebo rate), semaglutide more than doubles the risk.
The median duration of constipation in semaglutide-treated participants was 47 days. In the placebo group, it was 35 days. So not only does semaglutide cause constipation more often, it causes episodes that last longer. Some participants reported constipation persisting for the full 16-week titration period, though it typically improved once the body adjusted to the maintenance dose.
Severity breakdown
Of all gastrointestinal adverse events reported in the STEP trials, 98.1% were classified as mild to moderate. Severe constipation requiring medical intervention was rare. Only 0.5% of GI events were classified as serious. These numbers should provide some reassurance. Semaglutide constipation is common, but it is almost never dangerous, as long as you recognize the warning signs of complications and respond appropriately.
That said, "mild to moderate" covers a wide range. A person who goes from daily bowel movements to every three days may be classified as "mild," but the discomfort, bloating, and disruption to daily life can be significant. The experience often overlaps with other GI symptoms like GLP-1-related fatigue. Clinical classifications and personal experience do not always align.
Comparison across GLP-1 medications
Not all GLP-1 receptor agonists cause constipation at the same rate. This matters if you are considering your options or thinking about switching between medications. Among GLP-1 agonists studied for weight loss, semaglutide has one of the highest constipation rates. The overall incidence of constipation across all GLP-1 receptor agonist studies is approximately 7.9%, meaning semaglutide at 24.2% is roughly three times the class average.
Tirzepatide, the dual GIP/GLP-1 receptor agonist, shows constipation rates of approximately 11% to 20.7% across the SURPASS and SURMOUNT trials, depending on the study phase. Dulaglutide and lixisenatide tend to have lower GI side effect profiles overall. If constipation is a major concern and you are comparing side effect profiles, these differences are worth discussing with your healthcare provider.
Understanding how peptides and GLP-1 medications work at a fundamental level helps you appreciate why these side effect differences exist between compounds.
First-line treatments that work
Before reaching for any supplement or medication, start with the lifestyle foundations. These are not optional extras. They are the base layer of any effective constipation management strategy on semaglutide, just as understanding what peptides are is foundational to any peptide protocol. Most mild to moderate cases respond well to these interventions alone, especially when implemented consistently.
Hydration protocol
Water is the single most important factor. Period.
When semaglutide slows gastric motility, the colon compensates by absorbing more water from the stool. If you are not drinking enough, the stool becomes hard, dry, and difficult to pass. The solution is straightforward, but it requires intention. Most people on semaglutide dramatically underestimate how much water they need because their appetite suppression extends to thirst cues as well.
The target is 73 to 100 ounces of water per day. That translates to roughly 9 to 12 cups. If you are active, live in a warm climate, or exercise regularly, aim for the higher end. If you are following a structured semaglutide diet plan, water intake should be built into that plan as a non-negotiable element.
Practical hydration strategies that work:
Drink 16 ounces of water immediately upon waking, before anything else
Keep a measured water bottle and refill it on a set schedule, not when you feel thirsty
Drink a full glass of water 30 minutes before each meal
Set hourly reminders if you tend to forget
Add electrolytes if you are drinking large volumes, as plain water in excess can dilute sodium levels
Count herbal teas and clear broths toward your daily total
Avoid relying on caffeinated beverages as your primary fluid source. While coffee does have a mild laxative effect in some people, caffeine is also a diuretic. Net hydration from caffeinated drinks is lower than from plain water. If you wonder whether semaglutide gives you energy or drains it, poor hydration is often the real culprit behind fatigue on this medication.
If you are also taking semaglutide with B12, note that adequate hydration supports B12 absorption as well. Two benefits from one habit.
Fiber strategy
Fiber works by adding bulk to the stool and drawing water into the intestinal tract. Both effects promote more regular bowel movements. But fiber on semaglutide requires a strategic approach. Simply "eating more fiber" without a plan can actually make constipation worse if you do not match it with adequate hydration.
The recommended daily fiber intake is 25 to 34 grams per day, depending on age, sex, and activity level. Most Americans get about 15 grams. That gap is significant even without semaglutide in the picture. On semaglutide, when you are eating less food overall, hitting 25 grams of fiber takes deliberate effort.
Two types of fiber matter here. Soluble fiber dissolves in water and forms a gel-like substance. It softens stool and makes it easier to pass. Sources include oats, chia seeds, flaxseeds, psyllium husk, beans, and lentils. Insoluble fiber does not dissolve. It adds bulk and stimulates peristalsis. Sources include whole grains, vegetables, nuts, and wheat bran.
You need both. But if you had to prioritize one, soluble fiber, particularly psyllium husk, is the most effective single intervention for semaglutide-related constipation. It also supports overall gut health by feeding beneficial bacteria in the colon.
Psyllium husk protocol:
Start with 1 teaspoon (about 5 grams) per day mixed in 8 ounces of water
Take it at least 30 minutes before or after your semaglutide injection day meals
After one week, increase to 2 teaspoons per day if tolerated
Maximum effective dose: 3 teaspoons (15 grams) per day, split across meals
Always follow with a full glass of water, psyllium without water can worsen constipation
If you are following a semaglutide-compatible food plan, prioritize high-fiber foods at every meal. This serves double duty: it helps with constipation and supports the nutritional quality of the smaller portions you are eating. Understanding how your semaglutide treatment timeline affects appetite can help you plan fiber intake around the periods when eating is most comfortable.
Exercise approach
Physical activity stimulates peristalsis. This is well-established science. The mechanical action of walking, running, or any rhythmic movement helps push contents through the intestinal tract. For semaglutide users dealing with constipation, regular exercise is a powerful and completely safe intervention.
The target: 20 to 30 minutes of moderate activity most days. Walking is enough. You do not need intense exercise to see benefits. In fact, gentle walking after meals is one of the most effective digestive aids available.
Specific activities that help constipation:
Walking, especially after meals (even 10 to 15 minutes helps)
Yoga, particularly poses that involve twisting and abdominal compression
Light jogging or cycling
Swimming
Abdominal exercises that engage the core musculature
Avoid intense exercise immediately after eating if you are experiencing significant delayed gastric emptying. Light movement is fine. Heavy exercise on a full, slow-emptying stomach can cause nausea and discomfort. Timing matters. If you are exploring peptides for athletic performance alongside your semaglutide treatment, building in digestive-focused movement is especially important.
Bowel habit training
This is the most underutilized strategy on this entire list. And it works.
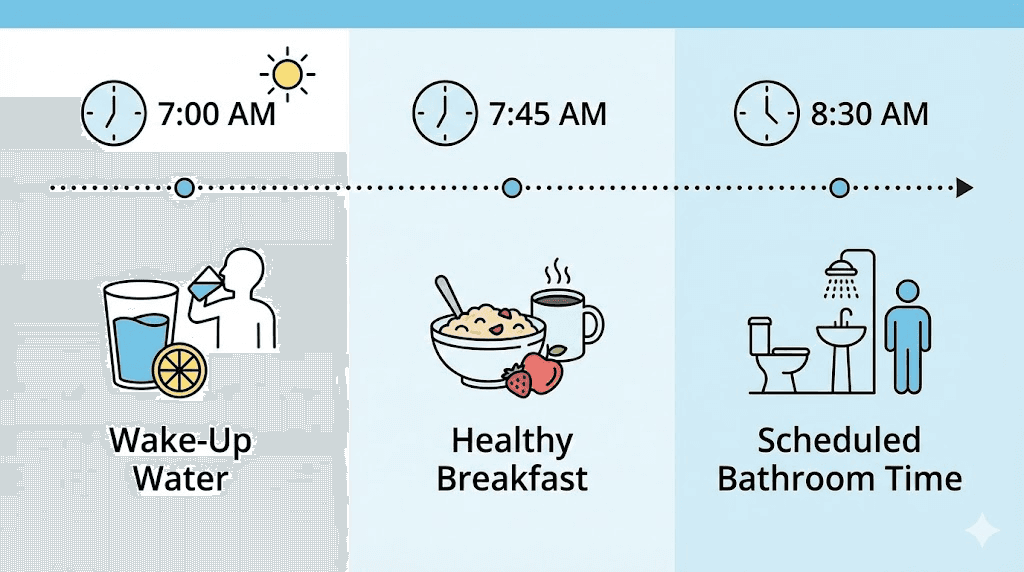
Your colon has a natural rhythm. It is most active in the morning, particularly after the first meal or drink of the day. This is called the gastrocolic reflex. When food enters the stomach, the colon receives a signal to make room by moving existing contents forward. On semaglutide, this reflex is weaker. But it still exists. You can train your body to take advantage of it.
The protocol is simple. Every morning, drink 16 ounces of warm water or warm water with lemon. Eat breakfast, even a small one. Then sit on the toilet for 5 to 10 minutes, whether or not you feel the urge. Do not strain. Just sit. Relax. Give your body the time and the signal.
Use a footstool to elevate your knees above your hips. This straightens the anorectal angle and makes it easier to pass stool without straining. The "Squatty Potty" concept is based on legitimate anatomy. It works.
Consistency matters more than any single session. After two to three weeks of following this routine daily, most people notice a significant improvement in regularity. The body adapts. The reflex strengthens. And the morning routine becomes a reliable part of your day.
Over-the-counter treatments for semaglutide constipation
When lifestyle changes alone are not enough, over-the-counter remedies can fill the gap. The key is choosing the right one for your specific situation, just as you would carefully select the right peptide dosage for any protocol. Not all laxatives are appropriate for semaglutide users, and some can cause more problems than they solve if used incorrectly.
Osmotic laxatives
Polyethylene glycol 3350, sold as MiraLAX, is considered the first-line over-the-counter laxative for semaglutide-related constipation by most gastroenterologists. It works by drawing water into the colon through osmosis, softening the stool and increasing its volume. This triggers gentle peristalsis without the cramping associated with stimulant laxatives.
MiraLAX has minimal systemic absorption, meaning it stays in the gut and does not interact significantly with semaglutide or most other medications. It is well-tolerated for both short-term and longer-term use when needed.
How to use MiraLAX for semaglutide constipation:
Standard dose: 17 grams (one capful) dissolved in 8 ounces of water or clear liquid
Take once daily, preferably in the morning
Effects typically begin within 12 to 72 hours
Can be used daily for up to two weeks without a healthcare provider consultation
For longer use, discuss with your prescriber
Do not combine MiraLAX with stimulant laxatives (like bisacodyl or senna) unless directed by a healthcare provider. Stimulant laxatives force the colon to contract and can cause dependency with regular use. On semaglutide, where the colon is already dealing with reduced motility signals, stimulant laxatives can create a cycle of dependence that is hard to break. The safety profile of any supplement or medication should always be evaluated in the context of your current treatment.
Magnesium supplementation
Magnesium is both a supplement and a constipation treatment. It works through two mechanisms. First, certain forms of magnesium draw water into the intestines through osmosis, similar to MiraLAX. Second, magnesium relaxes the smooth muscle of the intestinal wall, promoting peristalsis. This dual action makes it particularly effective for the type of constipation semaglutide causes.
Not all magnesium is equal for constipation.
Magnesium citrate: The most commonly recommended form for constipation. Well-absorbed, effective, and predictable. Start with 200 mg at bedtime. Increase to 400 mg if needed. Do not exceed 400 mg daily without medical guidance. Magnesium citrate can cause loose stools at higher doses, so finding your threshold is important.
Magnesium oxide: Less well-absorbed systemically, which means more of it reaches the colon where it draws in water. A dose of 400 mg at bedtime is the standard recommendation from gastroenterologists managing GLP-1-related constipation. This form is specifically mentioned in clinical guidance for semaglutide side effect management.
Magnesium glycinate: Better for overall magnesium supplementation and muscle relaxation, but less effective specifically for constipation. If you are taking magnesium primarily for gut motility, citrate or oxide is the better choice.
Magnesium supplementation is generally safe for most adults. However, people with kidney disease should consult their healthcare provider before supplementing, as the kidneys are responsible for clearing excess magnesium. If you are combining semaglutide with other supplements like glycine, coordinate your supplement schedule to avoid taking everything at once.
Stool softeners
Docusate sodium (Colace) is a gentle stool softener that works by allowing water and fats to penetrate the stool, making it softer and easier to pass. It does not stimulate peristalsis. It simply changes stool consistency.
Stool softeners are best used as a preventive measure rather than a treatment for acute constipation. If you know that constipation tends to worsen around certain points in your semaglutide cycle, taking a stool softener proactively can prevent the problem from developing.
Standard dosing: 100 mg once or twice daily with a full glass of water. Effects typically begin within 12 to 72 hours. Stool softeners can be used safely for extended periods, making them a good option for ongoing management during the duration of semaglutide treatment.
Probiotics and prebiotics
The gut microbiome plays a significant role in bowel regularity, and research suggests that GLP-1 medications alter the composition and diversity of gut microbiota. While there are no published clinical trials directly testing probiotics in semaglutide users, the general evidence for probiotics and constipation relief is supportive.
Bifidobacterium lactis is the strain with the strongest evidence for reducing constipation. It has been shown to increase stool frequency and improve stool consistency across multiple randomized controlled trials. Other helpful strains include Lactobacillus rhamnosus and Bifidobacterium longum. Some of these same strains also show promise in reducing gut inflammation, which can compound digestive issues during GLP-1 treatment.
Prebiotics, the non-digestible fibers that feed beneficial gut bacteria, add another layer of support. Sources include inulin, fructooligosaccharides (FOS), and galactooligosaccharides (GOS). These are found naturally in bananas, onions, garlic, asparagus, and chicory root. A prebiotic supplement providing 5 to 10 grams daily can support microbiome health during semaglutide treatment.
The combination of probiotics and prebiotics (often called synbiotics) creates the most supportive environment for gut health. If semaglutide is altering your microbiome while simultaneously slowing transit time, replenishing beneficial bacteria and feeding them properly is a logical intervention.
Complete daily protocol for semaglutide constipation relief
Theory is useful. Protocols are what actually change outcomes. Here is a complete daily schedule combining all of the evidence-based interventions into a single, practical routine. You do not need to implement everything at once. Start with the foundations, assess your response over two weeks, and layer in additional interventions as needed.
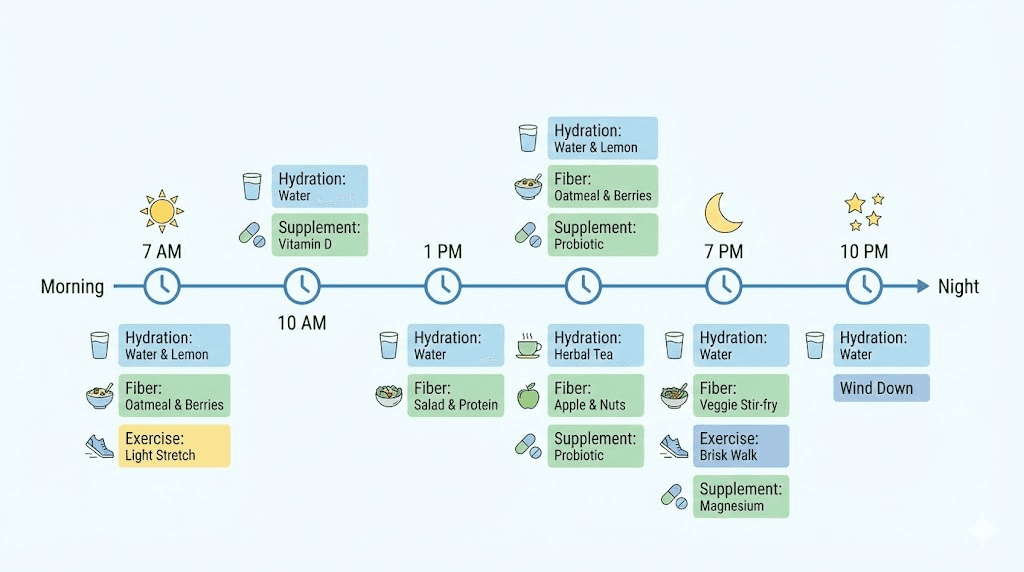
Morning routine (6:00 to 8:00 AM)
Drink 16 ounces of warm water immediately upon waking
Take probiotic supplement on an empty stomach (if using)
Eat breakfast including at least 8 to 10 grams of fiber (oatmeal with chia seeds and berries is an excellent option)
Drink 8 more ounces of water with breakfast
Sit on the toilet for 5 to 10 minutes after breakfast using a footstool
Take a 10 to 15 minute walk after breakfast if possible
Midday routine (11:00 AM to 1:00 PM)
Drink at least 16 ounces of water between breakfast and lunch
Eat lunch with emphasis on vegetables, legumes, and whole grains (target 8 to 10 grams of fiber)
Take psyllium husk supplement with a full glass of water if not getting enough fiber from food (1 to 2 teaspoons)
Walk for 10 minutes after lunch
Afternoon routine (3:00 to 5:00 PM)
Drink another 16 ounces of water
Have a fiber-rich snack if appetite allows (apple with skin, handful of almonds, raw vegetables with hummus)
Get 15 to 20 minutes of moderate exercise (walk, yoga, light activity)
Evening routine (6:00 to 9:00 PM)
Eat dinner with focus on cooked vegetables and lean protein (target 8 to 10 grams of fiber)
Drink 8 ounces of water with dinner
Take 200 to 400 mg of magnesium citrate or magnesium oxide at bedtime
Take stool softener at bedtime if using as a preventive measure
Drink a final 8 ounces of water or herbal tea before bed
This protocol provides approximately 25 to 35 grams of fiber, 80 to 100 ounces of water, 20 to 30 minutes of exercise, and targeted supplementation. For most people experiencing mild to moderate semaglutide constipation, following this consistently for two weeks will produce a noticeable improvement. Think of it like any well-designed cycle plan, consistency over time delivers the results.
If you are also using the semaglutide dosage calculator to track your titration, add a constipation rating to your daily log. Track bowel frequency, consistency, and comfort level. This data helps you identify patterns and adjust your protocol over time. The peptide calculator tools at SeekPeptides can help you stay on top of all your dosing and tracking needs.
Dosage timing and constipation management
When you take your semaglutide injection can influence how constipation affects you throughout the week. While no clinical trial has specifically studied injection timing as a constipation variable, patterns emerge from user experience and pharmacokinetic data that are worth understanding.
Semaglutide reaches peak plasma concentration approximately one to three days after injection. This is when GLP-1 receptor activation is strongest, gastric emptying is most delayed, and constipation risk is highest. By days five through seven, levels are declining before the next dose. If you are learning how to inject GLP-1 medications and choosing where to inject, consider that injection timing and site are both variables worth tracking alongside your bowel habits.
Some strategies related to timing:
Front-load your constipation protocol around injection day. On injection day and the two days following, be especially aggressive with hydration, fiber, and magnesium. This is when motility suppression is strongest, and proactive intervention prevents stool from hardening and accumulating.
Consider injection timing relative to your routine. Many people find that choosing the best injection time can minimize side effect impact. If constipation peaks two days after injection, injecting on a day when you have more control over your routine (weekends, for example) can make management easier.
Track the pattern across your titration. As your dose increases through the standard schedule outlined in any semaglutide dosage chart, constipation may worsen at each new dose level before your body adapts. Keep a simple log. Note your dose, injection day, and bowel movements. After two to three dose cycles, patterns will emerge that allow you to anticipate and prevent problems rather than react to them.
If you are using compounded semaglutide, the same principles apply. The active compound is the same. The pharmacokinetics are the same. Your constipation management protocol should be the same regardless of the formulation source. Whether you are following a 10mg dosage chart or a compounded semaglutide dose chart, the relationship between dose and constipation severity remains consistent.
Dietary strategies that reduce semaglutide constipation
What you eat matters as much as how much you eat. On semaglutide, when appetite is suppressed and portions are smaller, every bite needs to count. A strategic approach to food selection can simultaneously address constipation, meet nutritional needs, and support weight loss goals.
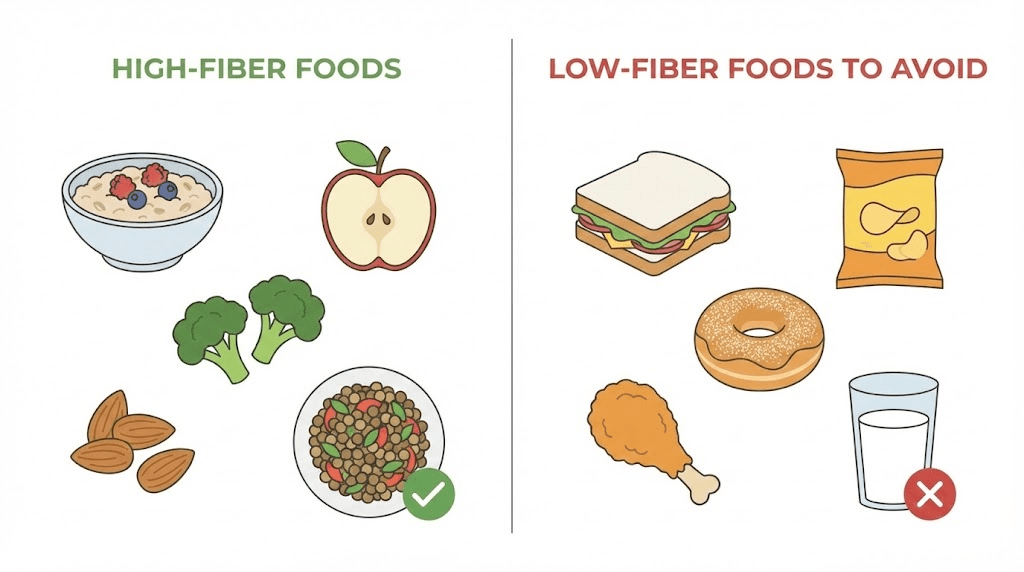
High-fiber foods to prioritize
These foods deliver the most constipation-fighting fiber per serving. Integrate them into your daily semaglutide-compatible meal plan:
Food | Serving size | Fiber (grams) | Type |
|---|---|---|---|
Chia seeds | 2 tablespoons | 10 | Soluble and insoluble |
Black beans | 1/2 cup cooked | 8 | Both |
Lentils | 1/2 cup cooked | 8 | Both |
Psyllium husk | 1 tablespoon | 7 | Soluble |
Avocado | 1/2 medium | 7 | Both |
Oatmeal | 1/2 cup dry | 5 | Soluble |
Raspberries | 1 cup | 8 | Both |
Broccoli | 1 cup cooked | 5 | Insoluble |
Sweet potato | 1 medium with skin | 4 | Both |
Flaxseeds | 2 tablespoons ground | 4 | Both |
A breakfast of oatmeal with chia seeds and raspberries delivers nearly 23 grams of fiber in a single meal. That is close to the entire daily target from one sitting. For semaglutide users with limited appetite, front-loading fiber at breakfast when appetite is often strongest makes strategic sense. Understanding when appetite suppression kicks in helps you plan your highest-fiber meals during the windows when eating is still comfortable.
Foods that can worsen constipation
Just as certain foods help, others make the problem worse. On semaglutide, where gastric emptying is already delayed, high-fat and low-fiber foods sit even longer in the stomach and produce harder, drier stool.
Foods to minimize:
Processed white bread and refined grains
Red meat in large portions (takes longer to digest)
Cheese and full-fat dairy in excess
Fried foods
Highly processed snacks with little fiber content
Bananas (unripe ones are binding; ripe bananas are fine)
This does not mean you need to eliminate these foods entirely. The goal is awareness. If constipation is an active problem, reducing these foods while increasing fiber-rich alternatives creates a more favorable environment for regular bowel movements.
The hydration-fiber connection
This point bears repeating because it is the single most common mistake. Increasing fiber without increasing water makes constipation worse, not better. Fiber absorbs water. If there is not enough water available in the intestinal tract, the fiber itself becomes a dry, bulky mass that is harder to pass than the original problem.
The rule: for every additional 5 grams of fiber you add to your diet, add at least 8 ounces of additional water. If you go from 15 grams to 30 grams of daily fiber, that means an additional 24 ounces of water on top of your baseline intake. If you are managing fluid intake while on semaglutide, make water the priority over all other beverages.
Semaglutide constipation vs tirzepatide constipation
If you are weighing your GLP-1 medication options, or considering a switch, understanding how constipation profiles compare between semaglutide and tirzepatide provides valuable context. Both medications cause constipation. Both work through GLP-1 receptor activation. But the specifics differ.
Factor | Semaglutide (Ozempic/Wegovy) | Tirzepatide (Mounjaro/Zepbound) |
|---|---|---|
Constipation rate | 24.2% (STEP trials) | 11-20.7% (SURPASS/SURMOUNT) |
Median duration | 47 days | Variable (less data available) |
Mechanism | GLP-1 receptor agonism only | Dual GIP/GLP-1 receptor agonism |
Overall GI event rate | 74.2% any GI event | Comparable, varies by dose |
Nausea rate | Higher at equivalent efficacy | 23.5% (comparable to semaglutide) |
Dose dependency | Strong (63.5% at 2.4mg vs 57.5% at 1.0mg) | Present but less pronounced |
The key difference is that tirzepatide also activates GIP receptors, which may modulate some of the pure GLP-1 effects on gut motility. Some researchers theorize that GIP activation partially counterbalances the constipation-promoting effects of GLP-1 activation, though this remains an area of active investigation. Other emerging compounds like retatrutide take this even further with triple receptor activation, and their GI profiles remain under active study.
Both medications benefit from the same constipation management strategies. If you are dealing with tirzepatide side effects, the hydration, fiber, magnesium, and exercise protocols described in this guide apply equally. The tirzepatide diet plan should mirror the fiber-focused approach outlined above. If constipation is your primary concern and you have the option of switching between these medications, discuss the constipation rate differences with your healthcare provider.
For those exploring whether other GLP-1 options might suit them better, understanding the broader peptide landscape for weight loss can help inform the conversation with your prescriber.
When constipation becomes dangerous
Most semaglutide constipation is uncomfortable but not dangerous. Most of it resolves with the interventions described above. But there is a line. And you need to know where it is.
In September of a recent year, the FDA updated the Ozempic label to include a warning about ileus, a condition where the intestines stop contracting entirely, creating a potentially life-threatening blockage. Twenty cases were reported, including two deaths. Ileus is rare. But it is serious enough that every semaglutide user should know the warning signs.
Seek immediate medical attention if you experience
No bowel movement for three or more consecutive days combined with worsening abdominal pain
Severe abdominal pain that is not relieved by gas or a bowel movement
Abdominal distension, where your stomach is visibly swollen and firm to the touch
Vomiting, especially if it is fecal-smelling (a sign of intestinal obstruction)
Complete inability to pass gas, which indicates a potential complete bowel obstruction
Fever with constipation, which may indicate infection or perforation
Blood in the stool or rectal bleeding when straining
Gastroparesis risk factors
Gastroparesis, or stomach paralysis, is another serious complication that has been associated with GLP-1 receptor agonists. It occurs when the stomach loses its ability to empty properly, separate from the intentional slowing effect of the medication. Risk factors that increase gastroparesis likelihood include:
Rapid dose escalation (skipping recommended titration steps)
Pre-existing diabetes with autonomic neuropathy
History of gastric surgery or radiation
Concurrent use of medications that slow motility (certain opioids, anticholinergics)
Pre-existing gastroparesis or severe gastric motility disorders
If you experience persistent nausea, vomiting undigested food hours after eating, severe bloating, or unexplained weight loss (beyond what semaglutide is intended to produce), report these symptoms to your healthcare provider immediately. Understanding the full spectrum of semaglutide-related concerns ensures you know when to act.
The vast majority of semaglutide users will never experience these complications. But awareness is prevention. Know the signs. Trust your body when something feels different from typical constipation discomfort. Reviewing the full peptide and medication safety guide helps you understand the broader context of when side effects cross from manageable to concerning. And do not hesitate to seek medical evaluation if you are concerned.
Advanced strategies when nothing else works
You have tried the water. The fiber. The magnesium. The daily walks. The bowel habit training. And you are still constipated. It happens. Some people are more sensitive to the motility effects of semaglutide than others, and some need more aggressive interventions.
Prescription options
When over-the-counter treatments fall short, several prescription medications can help:
Lubiprostone (Amitiza): A chloride channel activator that increases fluid secretion in the intestines. It directly addresses the excess water absorption that semaglutide promotes. Typical dose is 24 mcg twice daily. It is FDA-approved for chronic idiopathic constipation.
Linaclotide (Linzess): A guanylate cyclase-C agonist that increases intestinal fluid and accelerates transit. It is particularly effective for constipation with abdominal pain. Typical dose is 145 mcg or 290 mcg daily on an empty stomach, at least 30 minutes before the first meal.
Prucalopride (Motegrity): A selective serotonin 5-HT4 receptor agonist that stimulates colonic motility. This is one of the most targeted options for the type of motility reduction semaglutide causes. It works by directly promoting the peristaltic contractions that GLP-1 activation suppresses. Typical dose is 2 mg once daily.
These medications require a prescription and should be discussed with your gastroenterologist or prescribing physician. If your constipation is severe enough to consider prescription intervention, that conversation should also include whether your semaglutide dose needs adjustment. Understanding the relationship between proper dosing and side effect severity is critical for making informed decisions about your treatment plan. Some users also explore complementary approaches like KPV peptide for additional GI support, though this should be discussed with your provider.
Dose modification strategies
Sometimes the answer is not adding more treatments. Sometimes the answer is adjusting the medication itself.
Options your healthcare provider might consider:
Extending the titration period. Instead of increasing every four weeks, hold at the current dose for six to eight weeks until constipation stabilizes. This gives your gut more time to adapt before facing additional motility suppression.
Stepping down temporarily. If constipation becomes severe at a new dose, dropping back to the previous dose for two to four weeks while implementing aggressive constipation management can allow for a more successful upward titration on the second attempt.
Adjusting the target dose. Not everyone needs the maximum 2.4 mg dose for weight loss. Some people achieve excellent results at 1.0 mg or 1.7 mg with significantly less constipation. The right dose balances efficacy with tolerability.
Understanding the full range of semaglutide dosing options gives you the knowledge to have a productive conversation with your healthcare provider about finding the right balance. You might also benefit from reviewing your syringe dosage chart to ensure accurate dosing at whatever level you settle on.
Combination approach for resistant constipation
For the most stubborn cases, a layered approach works best. Rather than trying one thing at a time, implement a combination protocol:
Level 1 (Foundations): Hydration (80-100 oz/day) + fiber (30+ g/day) + daily exercise (30 min) + bowel habit training
Level 2 (Supplementation): Add magnesium citrate (400 mg at bedtime) + psyllium husk (2-3 tsp/day) + probiotic with Bifidobacterium lactis
Level 3 (OTC medications): Add MiraLAX (17 g daily) + stool softener (100 mg twice daily)
Level 4 (Medical intervention): Discuss prescription options + dose modification with healthcare provider
Most people find relief at Level 1 or Level 2. Level 3 handles the majority of remaining cases. Level 4 is reserved for the small percentage who have tried everything and still struggle. The key is systematic escalation rather than random experimentation, the same principle behind any well-structured peptide stacking protocol.
Alternative GLP-1 medications
If constipation remains intolerable despite maximum supportive care and dose optimization, switching to a different GLP-1 medication is a legitimate option. As the comparison data shows, newer compounds like retatrutide and tirzepatide have different side effect profiles. Some people tolerate one GLP-1 agonist much better than another, even though the mechanisms overlap.
The decision to switch should weigh constipation severity against weight loss efficacy, blood sugar control (if applicable), cost considerations, availability, and overall quality of life. It is a nuanced conversation that deserves more than a quick office visit. The peptide cost calculator can help you compare the financial aspects of different treatment options. If your provider dismisses your constipation as "just a side effect," consider seeking a second opinion from a gastroenterologist who specializes in GLP-1-related GI issues. Resources on the best weight loss peptides and optimal weight loss stacks can give you a broader perspective on the options available.
Long-term management and adaptation
One of the most important things to understand about semaglutide constipation is that it often improves over time. The body adapts. GLP-1 receptor sensitivity adjusts. The gut microbiome recalibrates. And the initial severe motility suppression gradually moderates as your system reaches a new equilibrium.
The median duration of constipation in clinical trials was 47 days. That means half of all people who experienced constipation saw it resolve within about seven weeks. Some resolve faster. Some take longer. But the trajectory is generally toward improvement.
During this adaptation period, consistency with your management protocol matters more than intensity. Drinking 100 ounces of water every day for seven weeks will serve you better than drinking 150 ounces for one week and then forgetting about it. The same applies to fiber, exercise, and supplementation. Build habits, not heroic one-time efforts.
If you are in the early weeks of treatment and wondering how long semaglutide takes to work, know that the constipation timeline roughly mirrors the weight loss timeline. Both are most intense during the titration phase and stabilize once you reach maintenance dosing. For a deeper look at the appetite suppression timeline, understanding how these phases overlap with GI side effects can set realistic expectations.
Some people experience constipation only during dose increases, with complete resolution at each stable dose. Others have persistent low-grade constipation that requires ongoing management. Both patterns are normal. Neither indicates a problem with the medication or your response to it. If you are exploring alternative approaches to weight management while dealing with GI side effects, understanding the full range of Ozempic alternatives can help you make informed decisions.
Monitoring your progress
A simple bowel movement journal is one of the most useful tools for long-term management. Track three things daily:
Frequency: How many bowel movements per day?
Consistency: Use the Bristol Stool Scale (Types 3 and 4 are ideal)
Effort: Rate straining on a 1 to 5 scale
Review weekly. Look for trends. Are things improving? Stable? Worsening? This data transforms vague complaints of "I am constipated" into actionable information that you and your healthcare provider can use to adjust your protocol. Many of the same tracking principles apply whether you are monitoring constipation or how long peptides take to work for any purpose. If you are also tracking your weight loss progress to understand why results might plateau, adding constipation data to that tracking gives a more complete picture.
For people tracking their full GLP-1 journey, especially during the early weeks when side effects are most prominent, understanding what to expect in the first month helps contextualize the constipation experience as part of a broader adaptation process.
Special considerations for compounded semaglutide users
A significant number of semaglutide users obtain their medication through compounding pharmacies rather than brand-name Ozempic or Wegovy. If you are using compounded semaglutide, the constipation management approach is identical. The active molecule is the same. The mechanism of action is the same. The side effect profile is the same.
However, compounded semaglutide does introduce some additional considerations worth understanding. Whether you are using injectable or oral semaglutide drops, accuracy in preparation and dosing affects everything downstream, including constipation severity.
Reconstitution accuracy matters. If your compounded semaglutide is supplied as a lyophilized powder requiring reconstitution, dosing accuracy depends entirely on correct mixing ratios. The 10mg mixing guide and the 5mg reconstitution instructions cover the most common vial sizes. The general peptide reconstitution guide explains the principles behind correct dilution. An improperly reconstituted vial could deliver a higher concentration per injection than intended, which would produce more GI side effects, including worse constipation. Use the peptide reconstitution calculator to verify your concentrations.
Storage affects potency. Compounded semaglutide that has not been properly refrigerated or that has been stored beyond its recommended shelf life may have degraded. The general principles in the peptide storage guide apply to semaglutide as well. Degraded peptides can behave unpredictably. If your GI symptoms change suddenly without a dose change, storage issues could be a factor. Learn more about how long peptides last in the fridge and whether peptides expire to protect your investment and your gut.
Unit-to-milligram conversions need precision. If you are using a conversion chart to translate between units and milligrams, double-check your math. Common conversions like 50 units to milligrams, 40 units to milligrams, 20 units to milligrams, or 10 units to milligrams all depend on the concentration of your specific vial. The 100 units conversion is another common reference point. Getting this wrong means getting your dose wrong, which directly affects constipation severity.
Whether you sourced your semaglutide from a major pharmacy or a compounding service like Empower Pharmacy, Direct Meds, or Olympia Pharmacy, the constipation treatment protocol remains the same. The 10mg mixing chart and 5mg mixing chart provide specific guidance regardless of your source. Focus on the fundamentals. The source of your semaglutide does not change how your gut responds to it. Reviewing whether expired semaglutide is safe to use is another important consideration for compounded product users.
The role of complementary supplements
Beyond the core constipation treatments, certain supplements can provide additional support during semaglutide treatment. These are not replacements for the foundational protocol. Think of them as potential additions for people who need extra help. Understanding how to properly mix peptides with bacteriostatic water and handle bacteriostatic water correctly is part of the broader competence that keeps any injectable protocol safe and effective.
B12 supplementation
Vitamin B12 supports nerve function throughout the digestive tract. Some research suggests that GLP-1 medications may reduce B12 absorption over time due to reduced intrinsic factor production and decreased gastric acid secretion. If B12 levels drop, the enteric nervous system, which controls gut motility, may function less efficiently. Supplementing with B12 addresses this potential deficit. Many people combine semaglutide with B12 for this reason. The semaglutide B12 dosage chart provides specific guidance on appropriate supplementation levels.
Glycine
Glycine supplementation alongside semaglutide has gained attention for its potential to support gut lining integrity and reduce inflammation in the digestive tract. While glycine is not a direct constipation treatment, a healthier gut lining may support better motility signaling and more efficient waste transit.
Digestive enzymes
Because semaglutide slows gastric emptying, food sits in the stomach longer. Digestive enzymes taken with meals can help break down food more efficiently even during this extended gastric residence time. This may reduce the bloating and fullness that often accompany semaglutide constipation. Enzymes do not treat constipation directly, but they address the upstream digestive inefficiency that contributes to it. Similar digestive support strategies apply to anyone using tirzepatide or planning meals on tirzepatide, where the same gastric slowing mechanism is at work.
For anyone exploring a broader supplement strategy alongside their GLP-1 medication, the getting started with peptides guide provides a framework for thinking about supplement integration safely and systematically. The common mistakes beginners make guide also highlights pitfalls to avoid when combining multiple supplements with a GLP-1 medication.
Oral semaglutide and constipation differences
If you are using oral semaglutide rather than the injectable form, the constipation risk and management approach is largely the same. The oral formulation (Rybelsus) contains the same semaglutide molecule with an absorption enhancer that allows it to survive the stomach environment and enter the bloodstream through the gastric lining.
Because oral semaglutide is taken daily rather than weekly, the pharmacokinetic profile is slightly different. There is less pronounced peak-and-trough cycling. This may produce more consistent, lower-grade constipation rather than the cyclical pattern some injectable users experience. The management strategies remain identical. Hydration, fiber, exercise, magnesium, and the full protocol outlined in this guide all apply to oral semaglutide users.
One additional consideration for oral semaglutide: the medication must be taken on an empty stomach with no more than 4 ounces of plain water, with no food or other medications for at least 30 minutes afterward. This morning fasting period can interfere with the bowel habit training protocol. If you are using oral semaglutide, adjust your morning routine. Take the medication first. Wait 30 minutes. Then begin your warm water, breakfast, and bathroom routine. The delay does not eliminate the benefit. It just shifts the timing.
For detailed guidance on the differences between injectable and oral formulations, understanding how each route of administration affects your body can help you optimize your overall treatment approach. The broader comparison between research and pharmaceutical peptides also provides context for understanding the quality spectrum available to consumers.
Exercise protocols specifically for constipation relief
The earlier section covered exercise as a foundational strategy. This section goes deeper into specific movements and routines that target digestive motility. These are not general fitness recommendations. These are targeted interventions for a sluggish gut.
Abdominal massage technique
Self-administered abdominal massage following the path of the colon can stimulate peristalsis and help move stool through the system. The technique is simple and can be done at home. Like learning proper injection technique, it is a physical skill that improves with practice.
Lie on your back with knees bent. Using moderate pressure, massage in a clockwise direction, starting at the lower right abdomen (near the appendix area), moving up the right side, across the top of the abdomen, and down the left side. This follows the natural path of the colon: ascending, transverse, and descending. Spend 5 to 10 minutes on this technique, once or twice daily. Many people find it most effective in the morning before getting out of bed or in the evening before sleep.
Yoga poses for constipation
Certain yoga poses create mechanical compression and torsion in the abdominal region that directly stimulates the intestines:
Supine twist (Supta Matsyendrasana): Compresses the colon from both sides alternately
Wind-relieving pose (Pawanmuktasana): Named for its effect on trapped gas and stool
Child pose (Balasana): Gentle abdominal compression
Cat-cow (Marjaryasana-Bitilakasana): Rhythmic alternation stimulates peristalsis
Deep squat (Malasana): Opens the pelvic floor and straightens the anorectal angle
A 15-minute sequence incorporating these poses, performed daily, can significantly improve bowel regularity when combined with the other strategies in this guide. Yoga also activates the parasympathetic nervous system (the "rest and digest" system), which promotes digestive function, a counterbalance to the stress response that can worsen constipation. For those also using peptides for muscle growth or anti-aging, gentle yoga provides recovery benefits that complement those protocols as well.
Walking protocol
Walking is the simplest and most accessible exercise for constipation relief. The rhythmic motion of walking creates gentle mechanical stimulation of the intestines. For maximum digestive benefit:
Walk for 10 to 15 minutes after each meal
Maintain a moderate pace (brisk enough to elevate heart rate slightly)
Total daily walking target: 30 minutes minimum
Morning walks are particularly beneficial as they align with the natural colonic activity peak
If you are managing semaglutide-related fatigue alongside constipation, walking serves double duty. Moderate exercise fights both symptoms simultaneously. The energy boost from walking can offset the lethargy some people experience on semaglutide, while the digestive stimulation addresses the constipation.
Interactions with other medications
Semaglutide constipation can be worsened by other medications you might be taking. Awareness of these interactions allows you to address multiple contributing factors simultaneously.
Common medications that worsen constipation:
Opioid pain medications: These directly suppress intestinal motility through mu-opioid receptors. Combined with semaglutide, the constipation effect is compounded significantly.
Anticholinergic medications: These include certain antihistamines, antidepressants, and bladder medications. They reduce the parasympathetic nervous system signals that promote digestion.
Iron supplements: Iron is notoriously constipating. If you need iron supplementation while on semaglutide, consider iron bisglycinate, which causes less constipation than ferrous sulfate.
Calcium supplements: Particularly calcium carbonate. If constipation is an issue, switch to calcium citrate, which has less constipating effect.
Certain blood pressure medications: Some calcium channel blockers can slow gut motility.
If you are considering combining semaglutide with other medications like phentermine, be aware that the combined effect on your digestive system may differ from either medication alone. The comparison between phentermine and semaglutide is worth reviewing to understand how their side effect profiles interact.
Tell your healthcare provider about every medication and supplement you take. What seems unrelated might be contributing to your constipation. A simple medication adjustment, switching from calcium carbonate to calcium citrate, or from ferrous sulfate to iron bisglycinate, can make a meaningful difference. The same principle of careful combination applies whether you are managing anxiety on GLP-1 medications, addressing headaches from tirzepatide, or dealing with GLP-1 hair loss. Every medication interaction matters.
The psychological impact of chronic constipation
This topic does not get enough attention. Constipation is not just a physical problem. When it becomes chronic, it affects mood, motivation, body image, and even your willingness to continue treatment.
Bloating from constipation can mask weight loss progress on the scale, creating frustration and discouragement. People who are losing fat but retaining stool weight may feel like their semaglutide is not working. If you are experiencing this, the guide on fatigue on GLP-1 medications is worth reading because physical discomfort from constipation and fatigue often compound each other. This frustration can lead to premature discontinuation or inappropriate dose increases, both of which are counterproductive.
The discomfort of chronic constipation also creates stress. Stress activates the sympathetic nervous system, the "fight or flight" response, which further suppresses digestive function. This creates a negative feedback loop: constipation causes stress, stress worsens constipation, worse constipation causes more stress.
Breaking this cycle requires addressing the physical and psychological components simultaneously. The physical interventions are covered throughout this guide. For the psychological component:
Remind yourself that constipation is a temporary phase for most semaglutide users (median 47 days)
Focus on trend data rather than daily scale readings
Measure progress through clothing fit, energy levels, and health markers rather than daily weight
Communicate with your healthcare provider about how constipation is affecting your treatment adherence
If you are feeling discouraged about slow progress, the guide on understanding weight loss plateaus on semaglutide provides perspective on the many factors, constipation included, that can temporarily mask results.
Building a sustainable long-term plan
The goal is not just to treat constipation. The goal is to build a sustainable routine that prevents it from becoming a recurring issue throughout your semaglutide treatment.
Here is the framework for long-term success:
Week 1 to 2: Implement foundations. Increase water to 80+ ounces daily. Add fiber-rich foods to every meal. Begin morning bowel habit training. Walk 20 minutes daily.
Week 2 to 4: Add supplementation if needed. Introduce magnesium (200-400 mg at bedtime). Begin psyllium husk (1-2 teaspoons daily). Start a daily probiotic.
Week 4 to 8: Evaluate and adjust. Review your bowel movement journal. Is frequency improving? Is consistency better? If yes, maintain current protocol. If no, add MiraLAX or stool softener. If still no improvement after two weeks of Level 3 interventions, schedule a conversation with your healthcare provider about prescription options or dose modification.
Week 8 onward: Maintain what works. By this point, most people have found their effective combination. Keep doing it. Do not stop the protocol just because things have improved. Consistency is what keeps the improvement going. The same principle applies to any peptide stack or BPC-157/TB-500 stacking protocol, sustained effort delivers sustained results.
Remember that your needs may change as your semaglutide dose changes. Each dose increase may temporarily worsen constipation, requiring a temporary intensification of your management protocol before things stabilize again. This is normal. Expect it. Prepare for it. And you will navigate it smoothly.
SeekPeptides members access detailed protocols, expert guidance, and community support for managing every aspect of GLP-1 treatment, including side effect management strategies that go beyond what any single article can cover. For those serious about optimizing their semaglutide experience, having a comprehensive resource library and dosing guidance at your fingertips makes the difference between struggling through side effects and managing them confidently.
Frequently asked questions
How long does semaglutide constipation last?
Clinical data from the STEP trials shows a median duration of 47 days for semaglutide-related constipation. Some people experience resolution within two to three weeks, while others deal with it throughout the titration phase (approximately 16 weeks). Most people see significant improvement once they reach a stable maintenance dose. Implementing the hydration, fiber, and exercise strategies in this guide can shorten the duration considerably. The overall semaglutide timeline helps contextualize when side effects typically peak and resolve.
Is MiraLAX safe to take with semaglutide?
Yes. Polyethylene glycol 3350 (MiraLAX) is considered the first-line over-the-counter laxative for semaglutide-related constipation. It has minimal systemic absorption, meaning it stays in the gut and does not interact with semaglutide. The standard dose is 17 grams (one capful) daily dissolved in 8 ounces of liquid. For use beyond two weeks, consult with your healthcare provider. For broader context on safe supplementation, the bioactive peptides for weight loss guide covers safety considerations across multiple compounds.
Can I take magnesium with semaglutide?
Yes. Magnesium citrate or magnesium oxide at 200 to 400 mg taken at bedtime is a safe and effective option for managing semaglutide constipation. Magnesium draws water into the intestines and relaxes intestinal smooth muscle, both of which counter the constipation-promoting effects of semaglutide. People with kidney disease should consult their provider before supplementing with magnesium. The peptide stack calculator can help you coordinate multiple supplements alongside your GLP-1 treatment.
Does constipation mean semaglutide is working?
Not directly. Constipation is a side effect of the same mechanism (slowed gastric motility) that contributes to appetite suppression and weight loss. But constipation itself does not indicate therapeutic effectiveness. Some people lose weight on semaglutide without any constipation. Others experience constipation without significant weight loss. They are correlated but not causally linked. If you are experiencing constipation but not losing weight, both issues can be addressed independently.
Will semaglutide constipation go away on its own?
In many cases, yes. The body adapts to GLP-1 receptor agonism over time, and bowel function often normalizes or significantly improves after the first one to two months. However, "going away on its own" can mean weeks of discomfort. Proactive management with the strategies in this guide accelerates resolution and improves quality of life during the adaptation period. Many users also find the anxiety management strategies helpful during this adjustment phase.
Should I stop semaglutide if constipation is severe?
Do not stop semaglutide without consulting your healthcare provider. Severe constipation should be reported to your prescriber, who may recommend dose adjustment, additional treatments, or a temporary hold on dose escalation. Stopping semaglutide abruptly can lead to withdrawal-like effects including rapid appetite return. If you are weighing whether to continue, the guide on treatment duration considerations provides important context. The goal is to manage the constipation while preserving the therapeutic benefits of the medication.
Does the type of semaglutide matter for constipation?
No. Whether you are using brand-name Ozempic, Wegovy, Rybelsus (oral), or compounded semaglutide, the active molecule is identical. Constipation rates and management strategies are the same across all formulations at equivalent doses. The reconstitution chart and mixing charts can help compounded semaglutide users ensure accurate dosing, which is critical for predictable side effect management.
Can fiber supplements interact with semaglutide absorption?
Fiber supplements should be taken at least one hour before or after semaglutide injection to avoid any theoretical impact on absorption. For oral semaglutide (Rybelsus), take the medication first on an empty stomach as directed, then wait the required 30 minutes before consuming any fiber supplements or food. Psyllium husk and other fiber supplements do not have a known direct interaction with semaglutide, but spacing them appropriately is a reasonable precaution. The fundamentals of peptide injection timing provide useful context for understanding absorption windows.
Is tirzepatide better than semaglutide for constipation?
Clinical data suggests that tirzepatide has a lower constipation rate (11-20.7%) compared to semaglutide (24.2%), though both medications cause constipation as a common side effect. If constipation is your primary concern, this difference may be worth discussing with your provider. The complete side effect comparison between these two medications covers all the GI differences in detail. You may also want to review tirzepatide dosing for weight loss and how fast tirzepatide works to compare the full picture.
External resources
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) - Constipation
Gastrointestinal tolerability of once-weekly semaglutide 2.4 mg (Wharton et al.)
JAMA - Risk of Gastrointestinal Adverse Events Associated With GLP-1 Receptor Agonists
For researchers serious about optimizing their GLP-1 treatment protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Whether you need help with cycle planning, stacking strategies, or safety guidance, the platform provides everything you need in one place.
In case I do not see you, good afternoon, good evening, and good night. May your digestion stay regular, your hydration stay consistent, and your semaglutide journey stay on track.