Feb 17, 2026

Before you increase your next dose, read this. Constipation on tirzepatide is not something you push through. It is not a minor inconvenience that resolves on its own. For some users, it becomes the single biggest barrier to continuing treatment, turning what should be a transformative weight loss journey into a daily struggle with bloating, discomfort, and frustration that makes every meal feel like a gamble.
Here is the reality. Clinical trials show that constipation affects anywhere from 6% to 17% of people using tirzepatide, depending on the dose and the condition being treated. That might sound manageable on paper. But when you are the one who has not had a normal bowel movement in five days, those percentages mean nothing. What matters is finding relief that actually works.
The good news is that tirzepatide constipation is both predictable and treatable. The mechanism behind it is well understood, the solutions are backed by evidence, and most people find significant improvement once they implement the right combination of strategies. This guide covers every proven treatment, from simple hydration adjustments and fiber protocols to magnesium supplementation, natural laxative foods, probiotics, exercise techniques, and over-the-counter options that gastroenterologists actually recommend. You will also learn the warning signs that require immediate medical attention, because while constipation is common, certain complications are genuinely dangerous.
Whether you are just starting tirzepatide and want to prevent constipation before it begins, or you are already dealing with it and need solutions that work today, this is the most comprehensive resource available. SeekPeptides created this guide because digestive side effects are the number one reason people consider stopping GLP-1 medications, and that decision should never happen because someone did not know how to manage a treatable problem.
Why tirzepatide causes constipation
Understanding why tirzepatide causes constipation is the first step toward treating it effectively. This is not random. The mechanism is specific, predictable, and directly tied to how the medication works.
Tirzepatide is a dual-acting peptide. It activates both the GLP-1 receptor and the GIP receptor, which is what makes it so effective for weight loss and blood sugar control. But one of those receptors, specifically GLP-1, has a powerful effect on the gastrointestinal tract that most people do not anticipate until they experience it firsthand.
The GLP-1 component and gastric emptying
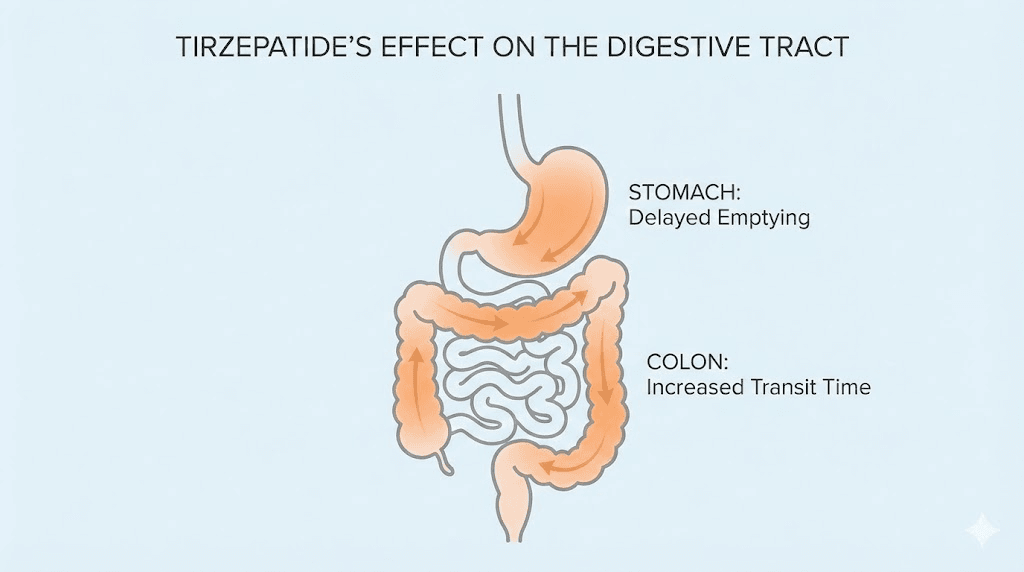
GLP-1 receptor activation slows gastric emptying. That is actually the point. When food stays in your stomach longer, you feel fuller for longer, you eat less, and you lose weight. The appetite suppression that makes tirzepatide so effective is directly connected to this delayed stomach emptying.
But the slowdown does not stop at the stomach.
When gastric emptying slows, the entire digestive transit time increases. Food moves through the small intestine more slowly. It reaches the colon later than normal. And here is where constipation begins. The colon has one primary job when it comes to stool formation: absorbing water. The longer stool sits in the colon, the more water the colon absorbs. More water absorbed means harder, drier stool. Harder stool means more difficult bowel movements. This cascade, from slower gastric emptying to increased colonic water absorption to harder stool, is the fundamental mechanism behind tirzepatide side effects like constipation.
The effect is dose-dependent. At lower doses like 2.5 mg, the GLP-1 activation is moderate. At higher doses like 10 mg or 15 mg, the receptor activation is stronger, gastric emptying slows more dramatically, and constipation becomes more likely. This is why the standard tirzepatide dosing guide recommends gradual titration, starting low and increasing slowly over months.
The GIP component: a smaller role
What about GIP? Tirzepatide is often described as a "twincretin" because it activates both GLP-1 and GIP receptors. But when it comes to gastrointestinal side effects, GIP plays a relatively minor role compared to GLP-1. The GIP receptor is primarily involved in insulin secretion and fat metabolism, not gut motility. So while tirzepatide is unique in its dual action, the constipation problem is driven almost entirely by the GLP-1 side of the equation.
This is useful to know because it means the same constipation management strategies that work for pure GLP-1 agonists like semaglutide also work for tirzepatide. If you have read about managing side effects from semaglutide versus tirzepatide, you will find significant overlap in the digestive management approach.
Additional contributing factors
The GLP-1 mechanism is the primary cause, but several secondary factors make tirzepatide constipation worse:
Reduced food intake. When you eat significantly less, there is simply less bulk moving through the digestive system. Less bulk means less stimulation of the intestinal muscles that push stool forward. Many tirzepatide users find their appetite drops dramatically, especially in the first few weeks. Understanding what to eat on tirzepatide becomes essential not just for nutrition but for maintaining regular bowel function.
Dehydration. Reduced food intake often means reduced fluid intake as well, since a significant portion of daily hydration comes from food. If you are eating half as much and not compensating with extra water, your body has less fluid available. The colon responds by absorbing even more water from stool, making the constipation worse.
Dietary changes. People on tirzepatide naturally gravitate toward certain foods and away from others. Many find that high-fiber foods feel too heavy or uncomfortable to eat in large quantities. Following a proper tirzepatide diet plan can help counteract this tendency, but many users default to low-fiber foods that are easier on a sensitive stomach, which only compounds the constipation problem.
Reduced physical activity. Some tirzepatide users, particularly in the early weeks, experience fatigue that reduces their activity level. Less movement means less natural stimulation of the intestinal muscles. The GLP-1 fatigue that some people experience can create a vicious cycle where tiredness leads to inactivity, which leads to worse constipation, which leads to more discomfort and less motivation to move.
How common is tirzepatide constipation
Numbers matter here. Understanding the actual prevalence helps you calibrate your expectations and recognize that what you are experiencing is normal, not a sign that something is seriously wrong.
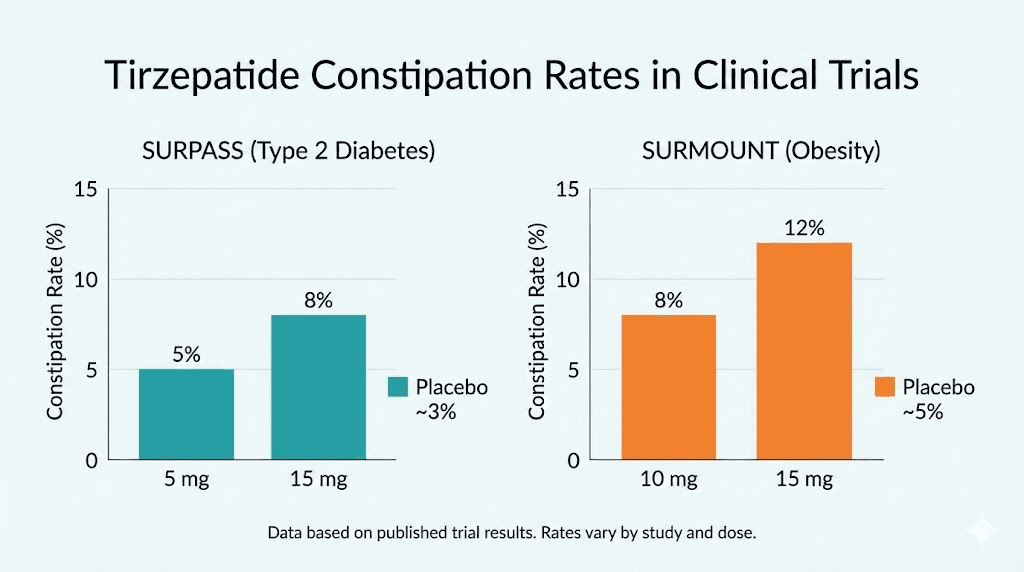
The data comes from two major clinical trial programs. The SURPASS trials studied tirzepatide for type 2 diabetes. The SURMOUNT trials studied it for weight loss in people without diabetes. The constipation rates were different between these two programs, and the difference is telling.
SURPASS trials (type 2 diabetes)
In the SURPASS trials, constipation affected approximately 6% to 7% of tirzepatide users, compared to about 1% on placebo. That is a meaningful difference, roughly six to seven times the background rate, but the absolute numbers were relatively low. Most diabetes patients using tirzepatide did not experience significant constipation at the doses used in these trials.
SURMOUNT trials (weight loss)
The SURMOUNT trials told a different story. Constipation rates jumped to 11% to 17% of participants, compared to about 5% on placebo. The higher rates in weight loss trials likely reflect several factors: higher doses used for weight management, greater caloric restriction, more dramatic changes in eating patterns, and the simple fact that weight loss patients often undergo more significant dietary shifts.
These numbers mean that roughly one in six to one in ten people using tirzepatide for weight loss will experience constipation significant enough to report in a clinical trial setting. The actual number in real-world practice may be higher, since clinical trials have strict protocols and regular medical oversight that real-world users often lack.
Meta-analysis data
A meta-analysis examining tirzepatide gastrointestinal effects across multiple trials found an overall constipation incidence of 2.54% for tirzepatide versus 0.85% for comparators. That number is lower than the individual trial figures because it includes all doses and all indications weighted together. The important takeaway is that tirzepatide consistently causes more constipation than placebo or active comparators, across every study, at every dose.
The dose-response relationship
Higher doses mean more constipation. This pattern is consistent across all trial data. If you are following a tirzepatide dose chart and planning to titrate up, understanding this relationship helps you prepare. At 2.5 mg, constipation is relatively uncommon. At 5 mg, it increases modestly. At 10 mg and 15 mg, rates climb further. This is why microdosing approaches and slow titration schedules have become popular, they give the body more time to adapt to each dose level before increasing.
Timeline: when does it start and when does it improve
Most gastrointestinal side effects from tirzepatide improve over the first few months of treatment. The body adapts. The gut adjusts to the new transit speed. For many users, constipation is worst during the first four to eight weeks at a new dose level and then gradually improves. This is encouraging, but those first few weeks can be miserable if you are not prepared.
Understanding how fast tirzepatide works for weight loss compared to how quickly side effects develop is important for setting expectations. Weight loss builds gradually over weeks and months. Side effects like constipation often appear within the first week at a new dose. This mismatch, experiencing the downsides before seeing the full benefits, is why so many people need a solid constipation management plan from day one.
Hydration strategies that actually work
Water is the foundation. No other constipation treatment will work optimally if you are dehydrated. This sounds basic, but on tirzepatide, maintaining adequate hydration requires deliberate effort because the medication fundamentally changes how much you eat and, consequently, how much fluid you take in through food.
How much water you actually need
The standard recommendation is 64 ounces per day, which is about eight cups. For tirzepatide users, that should be considered the absolute minimum, not the target. Most gastroenterologists recommend 80 ounces or more for people experiencing medication-related constipation. Some research suggests that people on GLP-1 medications may benefit from up to 100 ounces daily, particularly during the first months of treatment when side effects are most pronounced.
But raw volume is not the whole story.
Timing matters. Drinking 40 ounces first thing in the morning and then very little for the rest of the day is less effective than distributing intake evenly. Aim for consistent intake throughout the day, with slightly more in the morning when the gastrocolic reflex is strongest. A practical approach is to drink 16 ounces upon waking, then 8 to 10 ounces every hour or two throughout the day.
Electrolyte considerations
Plain water is good. Water with electrolytes is often better. When you increase water intake significantly, you can dilute electrolyte concentrations in the blood, which can cause its own set of problems including fatigue and muscle cramps. Adding a pinch of salt to your water, using an electrolyte supplement, or incorporating mineral-rich beverages can help maintain balance.
This is especially relevant for tirzepatide users who are eating less. Reduced food intake means reduced electrolyte intake from food sources. The combination of eating less and drinking more plain water can create an electrolyte imbalance that actually worsens tirzepatide fatigue and digestive sluggishness. Knowing which supplements to take with tirzepatide can help address both the constipation and the electrolyte considerations simultaneously.
Beverages that help versus beverages that hurt
Helpful: Warm water (especially in the morning, stimulates peristalsis), herbal teas like peppermint or ginger, warm lemon water, broth-based soups, and coconut water for natural electrolytes.
Neutral: Regular water, sparkling water (may cause bloating in some people but does not worsen constipation), and diluted fruit juices.
Potentially problematic: Excessive coffee (more than 2 to 3 cups daily can be dehydrating despite its mild laxative effect), alcohol (dehydrating and slows gut motility), and sugary drinks (can worsen digestive symptoms). Understanding the relationship between drinking on tirzepatide and digestive health is important, because alcohol compounds the dehydration problem significantly.
The warm water protocol
One evidence-based approach deserves special mention. Warm water, consumed first thing in the morning on an empty stomach, has been shown to stimulate gastric motility and trigger the gastrocolic reflex more effectively than cold or room-temperature water. The protocol is simple: drink 16 ounces of warm (not hot) water within five minutes of waking, before coffee, before food, before anything else. Then wait 20 to 30 minutes before eating breakfast. Many tirzepatide users report that this single habit makes a noticeable difference in their morning bowel regularity.
The fiber protocol for tirzepatide users
Fiber is complicated on tirzepatide. Too little makes constipation worse. Too much, too fast, makes bloating unbearable. The key is the right type of fiber, at the right dose, introduced at the right pace.
Understanding fiber types
Not all fiber is created equal. There are two main categories, and they do fundamentally different things in the gut.
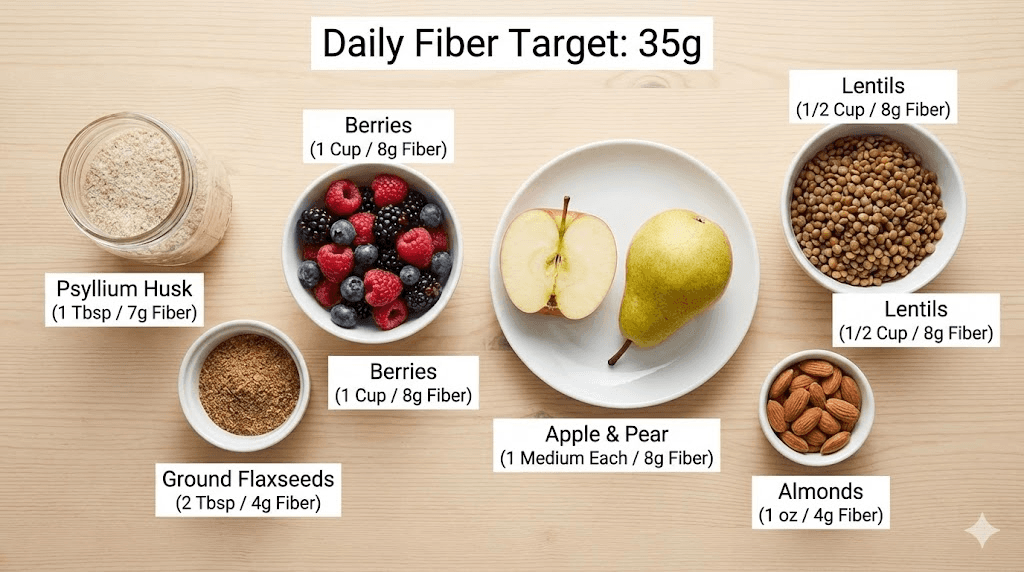
Soluble fiber dissolves in water and forms a gel-like substance. It softens stool and makes it easier to pass. Sources include psyllium husk, oat bran, chia seeds, ground flaxseeds, and fruits like apples and pears. For tirzepatide constipation, soluble fiber is generally the most helpful and the best tolerated.
Insoluble fiber does not dissolve in water. It adds bulk to stool and helps it move through the intestines faster. Sources include wheat bran, whole grains, vegetables, and fruit skins. Insoluble fiber is valuable, but it can worsen bloating and discomfort in tirzepatide users if introduced too aggressively, because the already-slow transit means that bulky stool sits in the colon even longer.
The ideal approach for tirzepatide users emphasizes soluble fiber first, with insoluble fiber added gradually as tolerated.
Daily fiber targets
General dietary guidelines recommend 25 grams daily for women and 34 grams daily for men. Most Americans get about 15 grams. On tirzepatide, when food intake drops, fiber intake often drops even further, sometimes to single digits. The goal is to reach those recommended levels gradually.
A safe titration schedule looks like this:
Week 1: Add 5 grams of soluble fiber daily (one tablespoon of psyllium husk mixed in a full glass of water).
Week 2: Increase to 10 grams daily (psyllium plus ground flaxseed or chia seeds added to meals).
Week 3: Increase to 15 grams daily, incorporating food sources like oatmeal, beans (in small portions), and fruit.
Week 4 and beyond: Gradually work toward the full 25 to 34 gram target, adjusting based on how your body responds.
The critical rule: every gram of fiber needs extra water. If you increase fiber without increasing water intake, you will make the constipation worse, not better. For every 5 grams of added fiber, aim for an additional 8 ounces of water.
Best fiber supplements for tirzepatide users
Psyllium husk is the gold standard. It is a soluble fiber that absorbs water and forms a soft, gel-like stool. Start with one teaspoon (about 3 grams of fiber) mixed in 8 to 12 ounces of water, taken once daily. Increase to twice daily after a week if tolerated. Psyllium has the strongest evidence base for treating medication-related constipation.
Acacia fiber is a gentler alternative for people who find psyllium causes too much bloating. It ferments more slowly in the gut, producing less gas. Start with one teaspoon daily and increase gradually.
Partially hydrolyzed guar gum (PHGG) is another well-tolerated option that dissolves completely in water and does not change the texture or taste of beverages. It is particularly good for people who dislike the thick texture of psyllium.
Understanding the full picture of foods to avoid on tirzepatide alongside the foods that help constipation creates a comprehensive dietary approach that addresses multiple side effects simultaneously.
Natural laxative foods that help
Before reaching for supplements or medications, several whole foods have clinically demonstrated laxative effects that work particularly well for tirzepatide-related constipation. These are not folk remedies. They are backed by randomized controlled trials.
Kiwifruit: the research standout
Kiwifruit has emerged as one of the most effective natural treatments for constipation, supported by multiple clinical trials. The mechanism is multifaceted. Kiwi contains actinidin, a proteolytic enzyme that enhances upper gastrointestinal motility. It also has a high water-holding capacity that keeps stool soft, plus it contains both soluble and insoluble fiber in an easily digestible form.
The protocol is simple. Eat one to two green kiwifruits daily. Studies show significant improvements in bowel frequency, stool consistency, and ease of defecation within two to four weeks. Many tirzepatide users report noticeable improvement within the first week. The fruit is low in calories, well tolerated even when appetite is suppressed, and tastes good, which matters when eating feels like a chore.
Prunes and prune juice
Prunes contain sorbitol, a natural sugar alcohol with osmotic laxative properties. Sorbitol draws water into the colon, softening stool and stimulating bowel movements. Prunes also contain significant fiber and phenolic compounds that stimulate intestinal contractions.
Start with three to four prunes daily or 4 ounces of prune juice in the morning. Some people find prune juice more effective than whole prunes because the liquid form delivers sorbitol more rapidly to the colon. If you tolerate the initial dose well, you can increase to six to eight prunes or 8 ounces of juice daily.
Ground flaxseeds
One to two tablespoons of ground flaxseeds daily provide both soluble and insoluble fiber, plus omega-3 fatty acids that have mild anti-inflammatory effects on the gut lining. Ground flaxseeds must be consumed in the ground form, as whole seeds pass through the digestive system without being broken down.
Mix ground flaxseeds into yogurt, oatmeal, smoothies, or water. They have a mild, nutty flavor that blends easily with most foods. Always follow with a full glass of water. Flaxseeds are particularly useful for tirzepatide users because they are calorie-dense in small amounts, helping maintain nutritional intake when appetite is low.
Chia seeds
Chia seeds absorb up to 12 times their weight in water, forming a gel that softens stool and adds gentle bulk. Two tablespoons provide about 10 grams of fiber, making them one of the most fiber-dense foods available. Soak them in water or liquid for at least 15 minutes before consuming to maximize their water-holding capacity.
A simple chia pudding made the night before, two tablespoons of chia seeds in a cup of liquid with a splash of vanilla, makes an easy breakfast option that delivers significant constipation relief. Combined with the dietary modifications outlined in our guide to eating on tirzepatide, these natural options create a food-first approach to digestive management.
Other helpful foods
Several other foods deserve mention. Pears and apples contain sorbitol and pectin, both of which have mild laxative effects. Leafy greens provide magnesium and fiber. Sweet potatoes offer soluble fiber and are generally well tolerated. Warm broth soups add hydration and gentle nutrition. Fermented foods like sauerkraut and kimchi provide probiotics that support overall gut health.
When building meals around these foods, the tirzepatide diet plan framework helps ensure you are getting adequate nutrition alongside constipation management, especially since reduced appetite can make meal planning challenging.
Magnesium for tirzepatide constipation
Magnesium is one of the most effective supplements for tirzepatide constipation. It works through a different mechanism than fiber, which means combining the two often produces better results than either one alone. But not all forms of magnesium work the same way, and choosing the wrong type can mean the difference between relief and disappointment.
How magnesium relieves constipation
Certain forms of magnesium are osmotic laxatives. They draw water into the intestinal lumen through osmosis, increasing the fluid content of stool and stimulating peristalsis, the wave-like contractions that move stool through the colon. This directly counteracts the primary mechanism of tirzepatide constipation, which is excess water absorption by the colon.
There is also a secondary benefit. Magnesium relaxes smooth muscle tissue, including the muscles of the intestinal wall. This relaxation can ease cramping and make bowel movements less painful when stool has become hard and difficult to pass.
Magnesium citrate: the acute relief option
Magnesium citrate is the most potent form for constipation relief. It has strong osmotic properties and typically produces a bowel movement within 30 minutes to 6 hours. Doses of 200 to 400 mg of elemental magnesium as citrate are commonly used for acute constipation.
This form works fast. Too fast, sometimes. Starting with a lower dose (200 mg) and adjusting upward is wise. Magnesium citrate is best used as an occasional rescue remedy rather than a daily maintenance supplement, because regular use at high doses can cause dependency and electrolyte imbalances.
Magnesium glycinate: the daily maintenance option
For ongoing constipation management, magnesium glycinate is the preferred choice. It provides a gentler laxative effect while also supporting sleep quality and muscle relaxation. The glycine component has calming properties, which makes this form ideal for evening dosing.
The typical daily dose is 300 to 400 mg of elemental magnesium as glycinate, taken with dinner or before bed. Effects are gentler than citrate but more consistent over time. Most tirzepatide users find that daily magnesium glycinate, combined with adequate fiber and hydration, provides reliable bowel regularity within one to two weeks.
This is one of the key supplements recommended for tirzepatide users, addressing constipation while also helping with the muscle cramps and sleep disruption that some people experience.
Magnesium oxide: the budget option
Magnesium oxide is the least bioavailable form, meaning less is absorbed into the bloodstream. For constipation purposes, this is actually an advantage, because more magnesium stays in the intestines where it can draw water into the stool. It is also the cheapest option.
Doses of 400 to 800 mg of magnesium oxide daily can effectively relieve constipation. The downside is that it can cause more cramping and urgency than glycinate, and it does not provide the same systemic benefits for sleep and muscle relaxation.
Magnesium protocol for tirzepatide users
For prevention (starting from day one of tirzepatide): 300 mg magnesium glycinate daily, taken in the evening.
For mild constipation: 400 mg magnesium glycinate daily, plus dietary fiber protocol.
For moderate constipation: 400 mg magnesium glycinate daily plus 200 mg magnesium citrate as needed (up to twice per week).
For acute relief: 400 mg magnesium citrate as a one-time dose, followed by increased water intake. If no bowel movement within 6 hours, consult your healthcare provider before repeating.
People with kidney disease should consult their doctor before supplementing with magnesium, as impaired kidney function can affect magnesium clearance. This is one of the many nuances covered in our peptide safety guide that applies broadly to supplement use alongside peptide-based medications.
Probiotics and gut health support
The gut microbiome plays a significant role in bowel regularity. Tirzepatide changes the gut environment in multiple ways: altered transit time, different dietary patterns, and shifts in the composition of what reaches the colon for bacterial fermentation. Probiotics can help restore balance and support regular bowel movements, but the strain specifics matter enormously.
Strains with evidence for constipation
Bifidobacterium lactis has the strongest evidence for constipation relief. Multiple randomized controlled trials show that this strain increases bowel movement frequency and improves stool consistency. Look for supplements providing at least 1 billion CFU of B. lactis daily. Some studies used up to 17 billion CFU with good results and minimal side effects.
Multi-strain Lactobacillus and Bifidobacterium blends have also shown benefit. Combinations that include L. acidophilus, L. rhamnosus, B. longum, and B. lactis appear to work synergistically. These multi-strain products are widely available and generally well tolerated.
Bifidobacterium longum BB536 is another well-studied strain that improves bowel frequency in constipated individuals. It also has evidence for reducing bloating, which is a common companion symptom to constipation on tirzepatide.
Prebiotic fiber: feeding the good bacteria
Probiotics are the bacteria. Prebiotics are what feed them. Certain types of fiber serve as fuel for beneficial gut bacteria, promoting their growth and activity. Inulin, fructooligosaccharides (FOS), and galactooligosaccharides (GOS) are the most studied prebiotics for constipation.
Start slowly. Very slowly. Prebiotics can cause significant gas and bloating when introduced too quickly, and tirzepatide users with already-slow digestion are especially sensitive. Begin with 2 to 3 grams daily and increase by 1 to 2 grams per week as tolerated. Food sources like onions, garlic, bananas, and asparagus provide natural prebiotics in moderate amounts.
Fermented foods as a complement
Yogurt, kefir, sauerkraut, kimchi, and kombucha provide live bacteria alongside nutrients. These are not replacements for targeted probiotic supplements, but they support a diverse microbiome that functions better overall. Small servings of fermented foods can be easier to tolerate than large supplement doses for people whose appetite and stomach capacity are limited by tirzepatide.
For a deeper exploration of how peptides interact with digestive health, our guide on peptides for gut health covers the broader landscape of compounds that support gastrointestinal function, including options like BPC-157 that researchers study specifically for gut healing and KPV peptide which has been investigated for its role in gut inflammation.

Exercise and movement for digestive relief
Movement stimulates the gut. This is not theoretical. Physical activity directly increases intestinal motility through mechanical stimulation, increased blood flow to the digestive organs, and activation of the parasympathetic nervous system that governs digestive function.
Why exercise matters more on tirzepatide
When tirzepatide slows your gastric emptying and colonic transit, your intestines need external stimulation to compensate. Exercise provides that stimulation. Studies show that moderate physical activity can reduce colonic transit time by up to 30%, which directly counteracts the slowdown caused by GLP-1 receptor activation.
The effect is both acute and chronic. A single bout of exercise can trigger a bowel movement within hours. Regular exercise over weeks and months improves baseline gut motility, making constipation less likely to develop in the first place. This dual benefit makes exercise one of the most powerful and underutilized tools for tirzepatide constipation management.
The ideal exercise protocol
Frequency: Most days of the week. Aim for at least five days out of seven.
Duration: 30 minutes of moderate activity per session. You do not need to do an hour. Thirty minutes is the threshold at which most studies show significant improvements in bowel function.
Intensity: Moderate. Brisk walking, cycling, swimming, or light jogging. High-intensity exercise can actually temporarily worsen digestive symptoms by diverting blood away from the gut to the working muscles. Moderate intensity keeps blood flowing to the digestive organs while still providing mechanical stimulation.
Timing: Morning exercise, particularly after warm water and before or shortly after breakfast, is ideal. This timing leverages the natural gastrocolic reflex that is strongest in the morning. Many people find that a 20 to 30 minute walk after breakfast consistently triggers a bowel movement within the following hour.
Specific movements that help
Walking is the simplest and most effective exercise for constipation. The upright posture, the rhythmic leg movement, and the gentle bouncing of the abdominal organs all contribute to intestinal stimulation. If you can do nothing else, walk.
Yoga poses that involve twisting, like seated spinal twists and supine twists, apply gentle pressure to the abdominal organs and can help move trapped gas and stool. Forward folds compress the abdomen and stimulate peristalsis. Even five to ten minutes of yoga-based abdominal movement can provide relief.
Core exercises like gentle crunches, bicycle legs, and pelvic tilts strengthen the abdominal muscles that assist with defecation. Strong abdominal muscles generate better intra-abdominal pressure, which makes bowel movements easier and more complete.
If tiredness from tirzepatide makes intense exercise difficult, even gentle movement helps. A slow 15-minute walk is infinitely better than sitting all day. The threshold for benefit is surprisingly low, and consistency matters more than intensity.
Bathroom habits and positioning techniques
This section might seem basic. It is not. Proper timing and positioning can make the difference between a productive bowel movement and a frustrating, incomplete one, especially when stool is harder than normal due to tirzepatide.
The gastrocolic reflex: timing is everything
The gastrocolic reflex is a physiological response where eating triggers increased motility in the colon. In simple terms, when food enters your stomach, your colon gets a signal to make room by moving things along. This reflex is strongest in the morning and after the largest meal of the day.
For tirzepatide users, leveraging this reflex is essential. The protocol is straightforward: eat a meal (even a small one), then wait 15 to 30 minutes, then sit on the toilet for 5 to 10 minutes regardless of whether you feel an urge. Do this consistently, at the same time each day. Over days and weeks, your body learns to associate this time and position with defecation, and the reflex strengthens.
Do not rush it. Do not strain. If nothing happens after 10 minutes, get up and try again after the next meal. Straining can cause hemorrhoids and anal fissures, which create additional problems on top of constipation.
The squatting position
Modern toilets are not designed for human anatomy. Sitting at a 90-degree angle puts the puborectalis muscle in a position that partially blocks the rectal canal. This muscle is designed to maintain continence when you are upright, but it can make defecation more difficult when you are simply sitting.
The solution is to elevate your feet using a footstool, commonly known as a Squatty Potty or similar product, placed in front of the toilet. Raising your knees above your hips creates a position closer to a natural squat, which straightens the anorectal angle and allows stool to pass more easily. Studies show that this position reduces straining time by an average of 50% and improves the sensation of complete evacuation.
For tirzepatide users dealing with hard, dry stool, this positioning adjustment is particularly valuable. It reduces the force needed to pass stool, which decreases the risk of complications from straining.
The breathing technique
Bearing down with held breath, the instinctive approach to straining, is counterproductive. It increases pressure on hemorrhoids and can cause blood pressure spikes. Instead, use diaphragmatic breathing during bowel movements.
Inhale deeply, allowing your belly to expand. As you exhale slowly through slightly parted lips, gently brace your abdominal muscles as if you were blowing up a balloon. This technique generates intra-abdominal pressure more evenly and effectively than straining, with less risk of complications. Repeat for several breath cycles, relaxing between efforts.
Over-the-counter treatments that work
When lifestyle modifications alone are not enough, over-the-counter treatments offer additional relief. These options are safe for most adults when used as directed, but understanding which type to use and when matters.
Stool softeners: docusate sodium
Docusate sodium (Colace) is a surfactant that allows water and fat to penetrate stool, making it softer and easier to pass. It is the gentlest OTC option and the least likely to cause cramping or urgency. For tirzepatide users, it is often the best first-line OTC treatment because it directly addresses the primary problem, hard, dry stool from excess water absorption in the colon.
Dosing: 100 mg once or twice daily. Effects typically begin within 12 to 72 hours. Docusate works best as a preventive measure taken daily rather than an acute treatment when constipation is already severe.
Limitations: It is not a strong laxative. If stool is severely impacted, docusate alone may not be sufficient. It works best in combination with hydration, fiber, and magnesium.
Osmotic laxatives: polyethylene glycol (MiraLAX)
Polyethylene glycol 3350, commonly sold as MiraLAX, is an osmotic laxative that draws water into the colon. It is odorless, tasteless, and dissolves completely in any beverage. PEG 3350 has extensive safety data supporting daily use for up to six months, and it is one of the most commonly recommended OTC treatments for chronic constipation by gastroenterologists.
Dosing: 17 grams (one capful) dissolved in 8 ounces of liquid, taken once daily. Effects typically begin within 1 to 3 days. Some people need to adjust the dose up or down, using half a capful for milder constipation or up to two capfuls for more severe cases, under medical guidance.
Advantages: It does not cause cramping in most people. It does not create dependency with proper use. It is effective regardless of dietary changes, making it particularly useful during periods when appetite is severely suppressed and dietary interventions are limited.
Considerations: Some people experience bloating when first starting MiraLAX. Starting with half a dose for the first few days can minimize this. Always take it with adequate fluid.
Stimulant laxatives: use sparingly
Stimulant laxatives like bisacodyl (Dulcolax) and sennosides (Senokot) work by directly stimulating the nerves in the colon wall, causing contractions that push stool forward. They are effective but should not be used as a first-line daily treatment. Regular use of stimulant laxatives can lead to dependency, where the colon becomes less responsive to normal stimuli and requires the laxative to function.
When to use: As an occasional rescue treatment when you have not had a bowel movement in four or more days despite other measures. Not as a daily maintenance strategy.
Dosing: Follow package directions. Take in the evening for a morning bowel movement. Do not exceed recommended doses.
Combination approach for tirzepatide users
The most effective OTC strategy usually combines products rather than relying on a single one. A common gastroenterologist-recommended approach for tirzepatide users:
Daily maintenance: Docusate sodium 100 mg twice daily plus MiraLAX 17 grams once daily.
Additional support: Psyllium fiber supplement and magnesium glycinate 300 to 400 mg daily.
Rescue only: Bisacodyl or sennosides if no bowel movement for 4 or more days despite the above regimen.
This layered approach addresses multiple mechanisms simultaneously, softening stool, drawing water into the colon, adding bulk, and providing mineral support, which is why it works better than any single treatment alone. If you are also managing other tirzepatide side effects like headaches or anxiety, coordinating all your management strategies with your healthcare provider ensures nothing conflicts.
When diet and supplements are not enough
Sometimes, despite doing everything right, lifestyle measures are simply not sufficient. This is not a failure. Some people have more pronounced GLP-1 sensitivity, pre-existing slow transit, or other factors that make their constipation more resistant to first-line treatments. When that happens, prescription options exist.
When to talk to your doctor
Consider seeking medical advice for constipation management if:
You have been implementing hydration, fiber, magnesium, and OTC treatments consistently for two or more weeks without meaningful improvement. You are having fewer than three bowel movements per week despite treatment. The constipation is significantly affecting your quality of life, causing severe bloating, pain, or nausea. You are considering stopping tirzepatide because of the constipation, which means the side effect is outweighing the benefit.
Your prescribing doctor needs to know about persistent constipation. It affects treatment decisions, including whether to adjust your tirzepatide dosage and how to modify your treatment plan going forward.
Prescription options your doctor may consider
Lubiprostone (Amitiza) is a prescription medication that increases fluid secretion in the small intestine, helping stool move more easily through the colon. It is specifically approved for chronic idiopathic constipation and can be effective for medication-related constipation.
Linaclotide (Linzess) works by increasing fluid secretion in the intestines and accelerating colonic transit. It also reduces visceral pain, which can be helpful for tirzepatide users experiencing abdominal discomfort alongside constipation.
Prucalopride (Motegrity) is a selective serotonin type 4 receptor agonist that stimulates colonic motility. Unlike stimulant laxatives, it does not cause dependency with long-term use. It is specifically designed for chronic constipation that has not responded to conventional treatments.
These prescription options are generally safe to use alongside tirzepatide, but the decision should always be made in consultation with a healthcare provider who understands both medications.
A note on bowel obstruction
Rare case reports have documented bowel obstruction in patients using GLP-1 receptor agonists, including tirzepatide. This is an extremely uncommon but serious complication. The risk is highest in patients with pre-existing gastroparesis, a history of bowel surgery, or severe chronic constipation. This is why treating constipation proactively, rather than ignoring it, is so important. Preventing severe constipation is far safer than dealing with its extreme complications.
Dose adjustment strategies
If constipation is severe and resistant to treatment, adjusting how you take tirzepatide may be more effective than adding more constipation remedies.
Slower titration
The standard tirzepatide titration schedule increases the dose every four weeks. Some people benefit from spending more time at each dose level, six to eight weeks instead of four, before moving up. This gives the gut more time to adapt to the GLP-1 effects at each dose, reducing the severity of constipation when the next increase occurs.
Reviewing the tirzepatide dose chart with your prescriber and discussing a modified titration schedule is a reasonable step if constipation is significantly impacting your quality of life. Many clinicians are open to slower titration when side effects are bothersome, especially since the weight loss benefits are cumulative regardless of titration speed.
Staying at a lower dose
Not everyone needs to reach the maximum dose. If you are losing weight effectively at 5 mg but constipation becomes unmanageable at 7.5 mg, staying at 5 mg is a legitimate clinical decision. The goal is sustainable treatment, not the highest possible dose. Understanding the differences between various compound dosage levels helps you have an informed conversation with your provider about where the right balance is for your body.
Microdosing approaches
Some tirzepatide users, particularly those using compounded versions, experiment with microdosing protocols that use smaller, more frequent doses rather than one larger weekly dose. The theory is that smaller doses produce a more gradual GLP-1 activation with less dramatic effects on gut motility. While this approach lacks formal clinical trial data, anecdotal reports from the community suggest it can reduce gastrointestinal side effects for some individuals.
Any dose modification should be discussed with your healthcare provider. Understanding the exact unit conversions, such as how many units make up 2.5 mg or how many units equal 5 mg, is essential for accurate dosing. Our compounded tirzepatide dosage calculator can help with precise unit calculations when working with compounded formulations at various concentrations like 10 mg/ml, 20 mg/ml, or 30 mg/ml formulations.
Comparing tirzepatide to alternatives
For some people, switching to a different GLP-1 medication with a different side effect profile may be worth discussing. The comparison between semaglutide and tirzepatide shows overlapping but not identical side effect patterns. Some people tolerate one better than the other. Our semaglutide versus tirzepatide comparison tool helps users understand the differences, including the dosage equivalencies between the two medications.
Newer dual and triple agonists like mazdutide and retatrutide are also entering the landscape. While their constipation profiles are still being studied, having awareness of emerging options means you can discuss them with your prescriber if tirzepatide constipation remains unmanageable.
Building a complete daily constipation prevention plan
Individual treatments help. But the most effective approach combines multiple strategies into a cohesive daily routine. Here is a comprehensive prevention plan designed specifically for tirzepatide users, incorporating everything covered above.
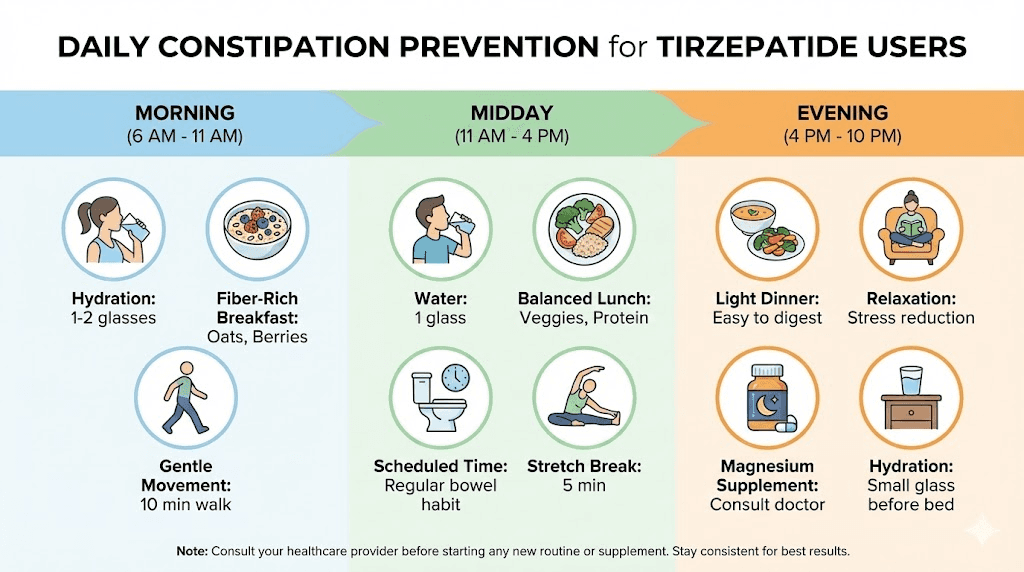
Morning routine (within the first hour of waking)
Drink 16 ounces of warm water immediately upon waking. Wait five minutes. Take one tablespoon of psyllium husk mixed in 10 ounces of water. Follow with your morning supplements: magnesium glycinate 300 to 400 mg (if not taken the night before) and a probiotic containing Bifidobacterium lactis. Eat breakfast within 30 to 60 minutes of waking, even if it is small. Include a fiber source: oatmeal with ground flaxseeds, or yogurt with chia seeds, or simply two green kiwifruits.
Within 15 to 30 minutes after eating, sit on the toilet with a footstool elevating your feet. Spend 5 to 10 minutes using the diaphragmatic breathing technique. Do not force anything.
Then move. A 20 to 30 minute walk, a gentle yoga session, or any moderate physical activity.
Midday habits
Continue drinking water consistently, aiming for 8 to 10 ounces every hour. If you eat lunch, include fiber-rich foods: vegetables, legumes, fruit, or whole grains. Have three to four prunes or 4 ounces of prune juice as a snack. Take docusate sodium 100 mg if it is part of your regimen.
Evening routine
Eat dinner with fiber-rich components. Take your evening supplements: docusate sodium 100 mg (second dose if applicable) and magnesium glycinate 300 to 400 mg if you take it at night. MiraLAX 17 grams dissolved in a beverage if it is part of your regimen (many people prefer taking it in the evening).
Continue hydration but taper off 1 to 2 hours before bed to avoid disrupting sleep with bathroom trips.
Weekly review
Track your bowel movements. Frequency, consistency, ease, and any symptoms. This data helps you identify what is working and what is not, and gives your healthcare provider objective information when you discuss your treatment plan. If you are consistently having three or more comfortable bowel movements per week, your plan is working. If not, adjust.
This prevention plan integrates with the broader health considerations of being on tirzepatide, from managing muscle-related side effects to ensuring proper nutrition with B12 supplementation and other adjuncts like niacinamide or glycine that some users find beneficial for overall well-being during treatment.
Warning signs that need immediate medical attention
Constipation on tirzepatide is common and usually manageable. But certain symptoms indicate something more serious that requires prompt medical evaluation. Do not ignore these warning signs.
Go to the emergency room or call 911 if you experience
Inability to pass stool or gas. If you cannot pass stool and also cannot pass gas, this may indicate a bowel obstruction. Complete obstruction is a medical emergency that requires immediate evaluation and potentially surgical intervention.
Severe, persistent abdominal pain. Mild cramping with constipation is normal. Severe, constant pain that does not come and go, or that worsens progressively, is not. This could indicate obstruction, perforation, or another surgical emergency.
Persistent vomiting combined with constipation. When constipation is accompanied by repeated vomiting, especially if the vomit has a fecal odor, this suggests a significant obstruction that requires emergency care.
Abdominal distension that is visibly increasing. A bloated, visibly distended abdomen that is tender to the touch and getting progressively worse needs evaluation. This can indicate obstruction, ileus, or other serious conditions.
Fever combined with abdominal symptoms. Constipation alone does not cause fever. If you have constipation plus fever, something else is happening, potentially an infection, inflammation, or perforation that requires immediate diagnosis.
See your doctor within 24 to 48 hours if you experience
Constipation lasting more than one week despite treatment. If you have been implementing hydration, fiber, magnesium, and OTC laxatives for a full week with no bowel movement, medical evaluation is needed.
Blood in stool. While this can be from hemorrhoids (common with straining), any blood in the stool warrants evaluation to rule out other causes.
Significant abdominal pain that interferes with daily activities. Pain that prevents you from working, sleeping, or functioning normally needs assessment.
New or worsening nausea that accompanies constipation. Nausea on tirzepatide is common, but if it is getting worse alongside worsening constipation, the combination may indicate a more serious motility problem.
A note on gastroparesis
People with established gastroparesis, a condition where the stomach empties abnormally slowly, should use tirzepatide with extra caution. The GLP-1 component further slows an already-slow stomach, which can lead to severe constipation, nausea, and potentially dangerous complications. If you have a history of gastroparesis, your doctor should be aware before starting tirzepatide, and your constipation management plan needs to be more aggressive from the start.
This is one reason why understanding the full range of side effect differences between GLP-1 medications is so important. Individual factors like gastroparesis history, baseline gut motility, and medication sensitivity all influence which treatment is safest.
Frequently asked questions
How long does tirzepatide constipation last?
For most users, constipation is worst during the first four to eight weeks at each new dose level and then gradually improves as the body adapts. Many people find that by the third or fourth month of stable dosing, their bowel function returns to near-normal with only minimal ongoing management. However, some users experience persistent constipation that requires continued treatment throughout their time on tirzepatide. Proactive management using the strategies in this guide, from targeted supplements to proper hydration, can significantly shorten the duration of significant symptoms.
Can I take MiraLAX every day while on tirzepatide?
Yes. Polyethylene glycol 3350 (MiraLAX) has safety data supporting daily use for up to six months. Many gastroenterologists recommend it as part of a daily regimen for people on GLP-1 medications who experience chronic constipation. The standard dose is 17 grams (one capful) daily, dissolved in any beverage. Discuss long-term use with your healthcare provider, and combine it with hydration and fiber for optimal results.
Does tirzepatide constipation get worse at higher doses?
Clinical trial data consistently shows a dose-response relationship between tirzepatide and constipation. Higher doses produce stronger GLP-1 receptor activation, greater slowing of gastric emptying, and more pronounced effects on colonic water absorption. If you are planning to increase your dose according to a tirzepatide dosing schedule, prepare your constipation management plan before each increase, not after symptoms appear.
Is tirzepatide constipation different from semaglutide constipation?
The mechanism is essentially the same because both medications activate GLP-1 receptors. Tirzepatide also activates GIP receptors, but GIP has minimal impact on gut motility compared to GLP-1. The semaglutide constipation treatment strategies are nearly identical to tirzepatide strategies. Some users who switch between the two medications report different levels of constipation severity, which likely reflects individual variation in receptor sensitivity rather than fundamental differences in mechanism.
Will fiber supplements make bloating worse on tirzepatide?
They can, if introduced too quickly. The key is gradual introduction. Start with one teaspoon of psyllium husk or acacia fiber daily and increase by one teaspoon per week. Always take fiber with a full glass of water. If bloating occurs, reduce the dose and increase more slowly. Soluble fiber supplements like psyllium and acacia tend to cause less bloating than insoluble fiber or high-dose prebiotics. The foods to avoid guide can help you identify which fiber sources are best tolerated alongside tirzepatide.
Can exercise really help with tirzepatide constipation?
Absolutely. Studies show that moderate physical activity reduces colonic transit time by up to 30%. For tirzepatide users, a 30-minute walk most days of the week is one of the most effective interventions available. The effect is both immediate, a single walk can trigger a bowel movement, and cumulative, regular exercise improves baseline gut motility over weeks and months. Even if GLP-1 related fatigue makes vigorous exercise difficult, gentle walking is sufficient to make a meaningful difference.
Should I stop tirzepatide because of constipation?
Constipation alone is rarely a reason to stop tirzepatide, because effective treatments exist. Most people can manage the symptom successfully with the combination of hydration, fiber, magnesium, and OTC treatments described in this guide. However, if constipation is severe, resistant to all treatments, and significantly impacting your quality of life, discuss this with your prescriber. Options include slower titration, staying at a lower dose, or potentially switching to an alternative medication. The decision to stop should be made collaboratively with your healthcare provider, not out of frustration with a treatable side effect.
What if I have not had a bowel movement in over a week?
One week without a bowel movement despite active treatment warrants a call to your healthcare provider. While not always an emergency, prolonged absence of bowel movements increases the risk of fecal impaction and other complications. Your doctor may recommend a prescription intervention, an enema, or an in-office evaluation depending on your symptoms. Do not wait for the situation to become an emergency. A week is the reasonable threshold for seeking professional guidance.
For ongoing questions about managing tirzepatide treatment holistically, SeekPeptides provides comprehensive resources covering everything from reconstitution protocols to proper storage and refrigeration requirements.
Additional considerations for specific populations
Women on tirzepatide
Women experience constipation at higher rates than men in general, and tirzepatide can amplify this baseline difference. Hormonal fluctuations throughout the menstrual cycle also influence gut motility, with progesterone (dominant in the luteal phase) slowing colonic transit. Women using tirzepatide may notice that constipation worsens during the second half of their cycle. Planning for increased magnesium and fiber during those weeks can help smooth out the fluctuation.
Women exploring peptides for weight loss should be aware of these gender-specific considerations when evaluating their options and building management plans. Similarly, women navigating menopause-related weight loss with tirzepatide may face compounded constipation challenges as declining estrogen further affects gut motility.
Men on tirzepatide
Men typically need higher fiber intake (34 grams versus 25 grams for women) and often have larger body sizes that require proportionally more hydration. Men using tirzepatide for weight loss should aim for the upper end of water intake recommendations, 80 to 100 ounces daily, and may need slightly higher magnesium doses (400 mg glycinate) due to larger body mass.
People using compounded tirzepatide
If you are using compounded tirzepatide rather than brand-name Zepbound or Mounjaro, the constipation management approach is identical. The active compound is the same regardless of source. However, compounded versions may come in different concentrations, requiring careful attention to compound dosage charts to ensure accurate dosing. Inaccurate dosing, whether too high or too low, can affect both efficacy and side effects including constipation.
Understanding the differences between sources, from Empower pharmacy to Lavender Sky to Peptide Sciences and other providers of compounded tirzepatide, can help you make informed decisions about your treatment source.
People using tirzepatide with companion supplements
Many tirzepatide users take additional supplements to support their treatment. B12 supplementation is common because GLP-1 medications can affect B12 absorption over time. Glycine and niacinamide are also used by some for various supporting purposes. None of these should interfere with constipation management, but awareness of your full supplement stack helps your healthcare provider give comprehensive advice.
Some users also explore tirzepatide drops or oral versus injection formats, though the constipation mechanism remains the same regardless of administration route since the GLP-1 receptor activation is systemic.
Understanding the bigger picture: gut health on GLP-1 medications
Constipation is the most common gastrointestinal side effect of tirzepatide, but it exists within a broader context of gut health changes that happen when you start a GLP-1 medication. Understanding this bigger picture helps you manage not just constipation but your overall digestive well-being.
The gut-brain connection
GLP-1 receptors exist in both the gut and the brain. Tirzepatide activates both sets of receptors, which is part of how it suppresses appetite and promotes satiety. But this dual activation also means that the medication can affect mood, energy, and anxiety levels alongside digestive function. Stress and anxiety, in turn, can worsen constipation by activating the sympathetic nervous system, which inhibits digestive function. Managing mental health alongside physical symptoms creates a more comprehensive treatment approach.
The relationship between peptides and mental health is an active area of research, and understanding how GLP-1 medications interact with both gut and brain function provides a more complete picture of what you are experiencing.
Long-term gut adaptation
The gut is remarkably adaptable. Over months of tirzepatide treatment, the enteric nervous system, the network of neurons that controls gut function independently of the brain, adjusts to the new baseline of GLP-1 activation. Transit times stabilize. Water absorption patterns normalize somewhat. The microbiome shifts to accommodate new dietary patterns.
This adaptation is why many users find that constipation improves significantly after the first three to six months, even without changing their management approach. The early months are the hardest. Persevering through them with active management sets the foundation for long-term success.
The role of inflammation in gut motility
Chronic low-grade inflammation can impair gut motility independently of medication effects. For people with pre-existing inflammatory conditions, tirzepatide constipation may be more severe. Supporting gut health with anti-inflammatory strategies, including anti-inflammatory peptides like KPV that researchers investigate for gut applications, and inflammation-targeting compounds may provide additional benefit for this subset of users.
The peptides for gut health resource page at SeekPeptides provides a comprehensive overview of compounds being studied for various aspects of gastrointestinal function, from mucosal healing to motility support to inflammatory modulation.
What to expect month by month
Knowing what to expect at each stage of tirzepatide treatment helps you plan your constipation management and set realistic expectations.
Month 1: the adjustment period
Constipation typically appears within the first one to two weeks. It may be mild at the starting dose of 2.5 mg, or it may be more significant if your gut is particularly sensitive to GLP-1 activation. This is when you should implement your full prevention plan: hydration, fiber, magnesium, and movement. Do not wait for constipation to become severe before acting. Prevention is dramatically easier than treatment.
During this first month, you are also adjusting to reduced appetite and new eating patterns. Pay close attention to what you eat and ensure that reduced quantity does not mean reduced fiber and fluid quality. Many new tirzepatide users benefit from understanding the timeline for tirzepatide effects so they can align their expectations for both weight loss and side effect management.
Months 2 to 3: titration and adaptation
If you are following the standard titration schedule, you will increase to 5 mg at month two and potentially to 7.5 mg at month three. Each dose increase can temporarily worsen constipation. Have your rescue strategies ready: extra magnesium citrate on hand, MiraLAX if needed, and awareness of the warning signs that require medical attention.
The good news is that most users notice their baseline constipation improving during this period, even as dose increases create temporary setbacks. The gut is adapting. Weight loss is typically becoming visible by now, which helps motivation. Tracking before and after progress can reinforce the value of persevering through side effects. Results like those seen in weight loss result compilations remind users that the temporary discomfort serves a meaningful purpose.
Months 4 to 6: stabilization
For the majority of users, constipation management becomes routine and less burdensome during this period. You have identified which strategies work best for your body. Your gut has adapted to the medication. Your dietary patterns are established. Many people can reduce their OTC laxative use during this phase, maintaining only basic prevention with fiber, hydration, and magnesium.
Some users plateau in their weight loss during this period and wonder why they are not losing weight on tirzepatide. Constipation itself can affect the scale, since retained stool adds physical weight. Ensuring regular bowel movements helps provide more accurate weight measurements and avoids the discouragement of a stalling scale.
Beyond 6 months: maintenance
Long-term tirzepatide users generally find that constipation management becomes second nature. The strategies that work are well established. The body has fully adapted. Some people can reduce or discontinue certain interventions while maintaining regularity. Others need ongoing support, and that is completely normal. The goal is not to eliminate all management, but to find a sustainable routine that keeps you regular without being a burden.
If you are also monitoring other aspects of your treatment, like whether tirzepatide is properly stored (understanding temperature stability and expiration considerations), maintaining treatment efficacy supports consistent side effect management as well. A medication that has degraded due to improper storage may produce inconsistent GLP-1 activation, which can make side effects more unpredictable.
Connecting constipation management to your broader treatment goals
Constipation is not an isolated problem. It connects to everything else about your tirzepatide experience, from weight loss effectiveness to nutritional status to mental health to treatment adherence.
Severe constipation reduces food intake further (you feel too full and bloated to eat), which can lead to nutritional deficiencies. It causes discomfort that reduces physical activity, which worsens both constipation and weight loss outcomes. It creates frustration and discouragement that makes people consider stopping treatment. And it affects the accuracy of weight measurements, creating a misleading picture of progress.
Managing constipation effectively is therefore not just about comfort. It is about optimizing your entire treatment experience. Every strategy in this guide, from morning warm water to evening magnesium to daily walks, contributes to an environment where tirzepatide can do its job effectively while you maintain your quality of life.
SeekPeptides exists to provide exactly this kind of comprehensive, interconnected guidance. Whether you are exploring peptides for weight loss broadly, comparing the best weight loss peptides, investigating stacking strategies, or managing the day-to-day realities of treatment, having reliable, evidence-based information makes the difference between a treatment that transforms your health and one that gets abandoned too soon.
Understanding the full landscape of tools available to you, from peptide calculators to semaglutide dosage calculators to reconstitution calculators and cost calculators, empowers you to manage your treatment confidently. Resources on how peptides work, what peptides are, dosage charts, and injection guides provide the foundational knowledge that makes everything else, including side effect management, more intuitive.
For those just beginning their journey, our getting started guide covers the basics, while awareness of common beginner mistakes helps you avoid the pitfalls that derail many newcomers. Proper storage practices and thoughtful cycle planning round out a treatment approach that is as comprehensive as it is practical.
Additional relevant considerations include understanding unit-to-milligram conversions at various levels, whether you are working with 40 units or 50 units, and knowing the specifics of 7.5 mg dosing. These details matter for accurate treatment, which directly impacts the consistency and severity of side effects like constipation.
For users considering combination approaches, understanding whether phentermine can be combined with GLP-1 medications and how phentermine compares to GLP-1 agonists helps inform treatment decisions. Similarly, some users look into broader comparisons like phentermine versus semaglutide when evaluating their options.
The relationship between GLP-1 medications and other side effects also provides useful context. Understanding semaglutide fatigue patterns and whether semaglutide affects energy levels helps users anticipate how these medications influence daily function, including the motivation to exercise, which directly impacts constipation management. Knowing the best time of day to take GLP-1 medications and following a proper GLP-1 diet plan or food guide for GLP-1 users contributes to a holistic approach.
Whether you are also exploring peptides for targeted fat loss, looking at belly-specific approaches, researching peptide options for men, or investigating bioactive precision approaches, having your constipation managed frees you to focus on the bigger picture of your health transformation.
Other resources that round out your knowledge include understanding hair-related considerations with GLP-1 medications, learning proper injection sites and injection technique, knowing whether GLP-1 is the same as brand-name medications, understanding considerations for breastfeeding mothers, and staying aware of innovations like GLP-1 patches that may change how these medications are delivered in the future.
Even comparisons beyond tirzepatide, such as semaglutide combined with glycine, semaglutide with B12, compounded semaglutide options, semaglutide timeline expectations, alcohol interactions with semaglutide, semaglutide withdrawal patterns, semaglutide weight loss plateaus, and early-stage semaglutide results, help provide context for understanding how different GLP-1 medications compare in practice.
For those interested in understanding autoimmune considerations alongside GLP-1 treatment, our guide on peptides for autoimmune diseases explores this intersection in detail. And the peptide stack calculator can help users planning multi-compound approaches ensure compatibility and proper scheduling.
For researchers serious about optimizing their treatment outcomes, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions successfully.
External resources
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) - Constipation
PubMed - Search for tirzepatide gastrointestinal effects meta-analyses
In case I do not see you, good afternoon, good evening, and good night. May your digestion stay comfortable, your bowels stay regular, and your treatment stay on track.