Feb 19, 2026

Of all the gastrointestinal side effects linked to semaglutide, burping has the strongest statistical signal. Not nausea. Not vomiting. Burping. An FDA pharmacovigilance analysis of over 5,400 semaglutide-related GI reports found that eructation carried a reporting odds ratio of 42.03, the highest of any gastrointestinal event in the entire database. That number dwarfs nausea, diarrhea, and constipation. And yet most guides barely mention it.
Here is what that means for you. If you are on semaglutide and burping constantly, you are not imagining things. You are not being dramatic. You are experiencing one of the most statistically overrepresented side effects of this medication. Roughly 7% of people taking Wegovy report excessive burping. At the lower Ozempic doses, the rate drops to about 3-5%. But those numbers undercount the reality, because many people do not report burping as a side effect. They just deal with it.
The burping is not random. It follows a specific mechanism involving delayed gastric emptying, bacterial fermentation, and hydrogen sulfide gas production. Understanding that mechanism is the first step toward managing it. And managing it matters, because uncontrolled burping can make social situations uncomfortable, disrupt sleep, and cause some people to abandon a medication that is otherwise working well for them.
This guide covers every aspect of semaglutide-related burping.
The science behind it. The timeline of when it starts and whether it stops. The specific foods that trigger it. The remedies that actually work. And the warning signs that mean your burping is something more serious than a nuisance. SeekPeptides members frequently ask about managing GI side effects during their peptide protocols, and burping is consistently among the top concerns.
How semaglutide causes burping
Semaglutide is a GLP-1 receptor agonist. It mimics a hormone your body already produces called glucagon-like peptide-1. That hormone does three things simultaneously. It increases insulin secretion when blood sugar rises. It decreases glucagon production, which prevents your liver from dumping stored glucose into your bloodstream. And it slows gastric emptying.
That third function is where burping enters the picture.
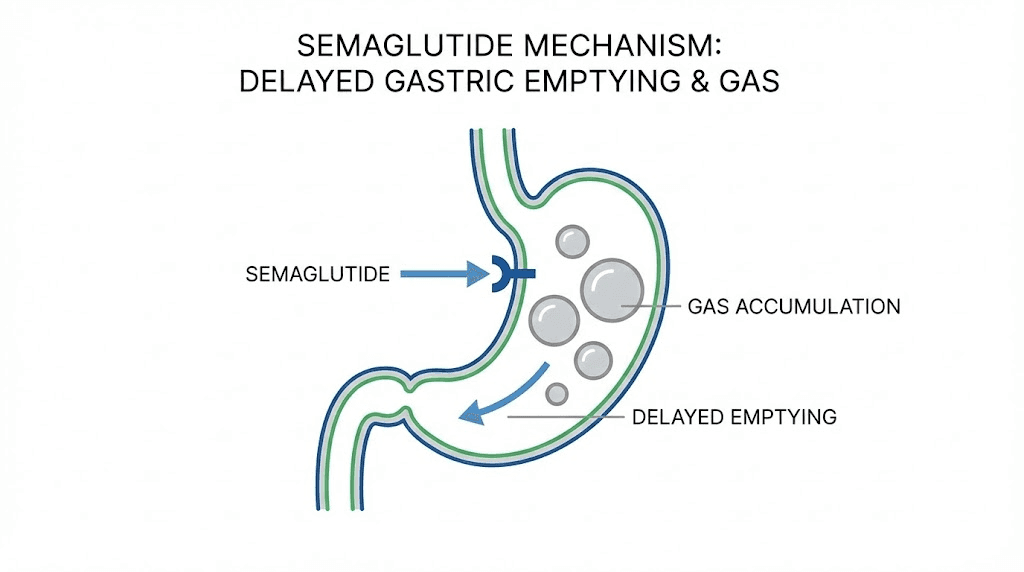
When semaglutide slows your stomach emptying, food sits in your stomach for longer than it normally would. Much longer, in some cases. A meal that would normally move through your stomach in two to three hours might take four to six hours. Maybe longer. The food has not gone bad. It has not spoiled. But it is sitting in a warm, acidic environment with billions of bacteria, and those bacteria are doing what bacteria do. They are fermenting.
Fermentation produces gas. Specifically, it produces hydrogen sulfide, carbon dioxide, and methane. Hydrogen sulfide is the gas responsible for that distinctive rotten-egg smell that many semaglutide users describe. The gas accumulates in your stomach, increases gastric pressure, and your body releases it the only way it can. You burp.
The mechanism is not complicated. But the details matter, because understanding exactly what triggers the gas production helps you prevent it rather than just treating the symptom after it appears. Anyone familiar with how peptides work at the receptor level understands that GLP-1 activation creates systemic metabolic changes, not just appetite suppression.
The delayed gastric emptying cascade
Normal gastric emptying follows a predictable pattern. You eat. Your stomach contracts rhythmically, mixing food with digestive enzymes and acid. The pyloric sphincter opens periodically to release small amounts of partially digested food into your duodenum. The entire process takes roughly two to four hours depending on meal composition.
Semaglutide disrupts this process at multiple points. It reduces the frequency and force of gastric contractions. It increases pyloric sphincter tone, making it harder for food to pass from stomach to small intestine. And it affects the hormonal signaling that coordinates gastric emptying with intestinal readiness. The result is food that sits. And sits. And ferments.
Studies on semaglutide pharmacodynamics show that gastric emptying can be delayed by 20-40% at therapeutic doses. For a meal that normally empties in three hours, that means an extra 36 to 72 minutes of stomach residence time. That is 36 to 72 additional minutes of bacterial fermentation, gas production, and gastric pressure buildup.
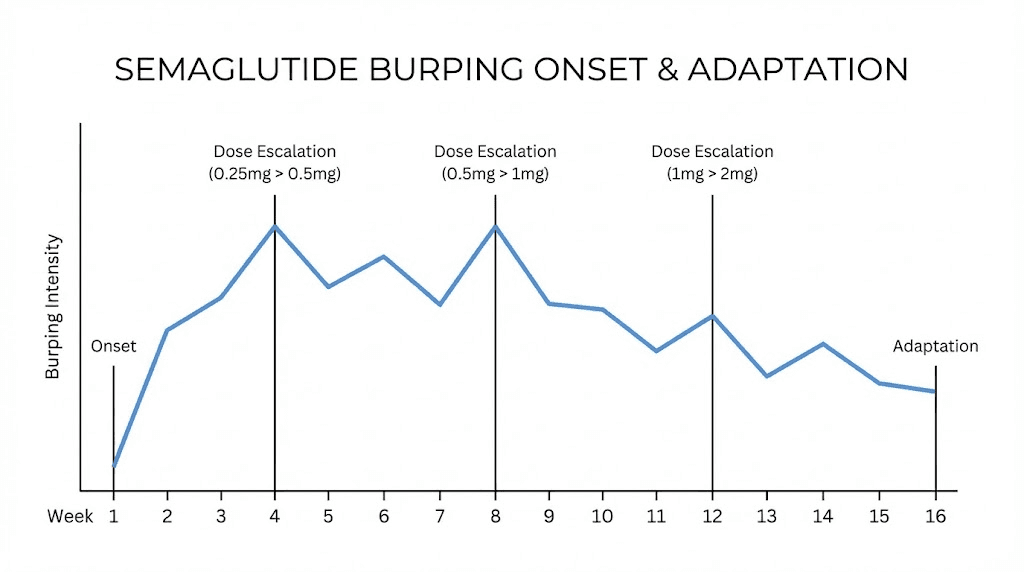
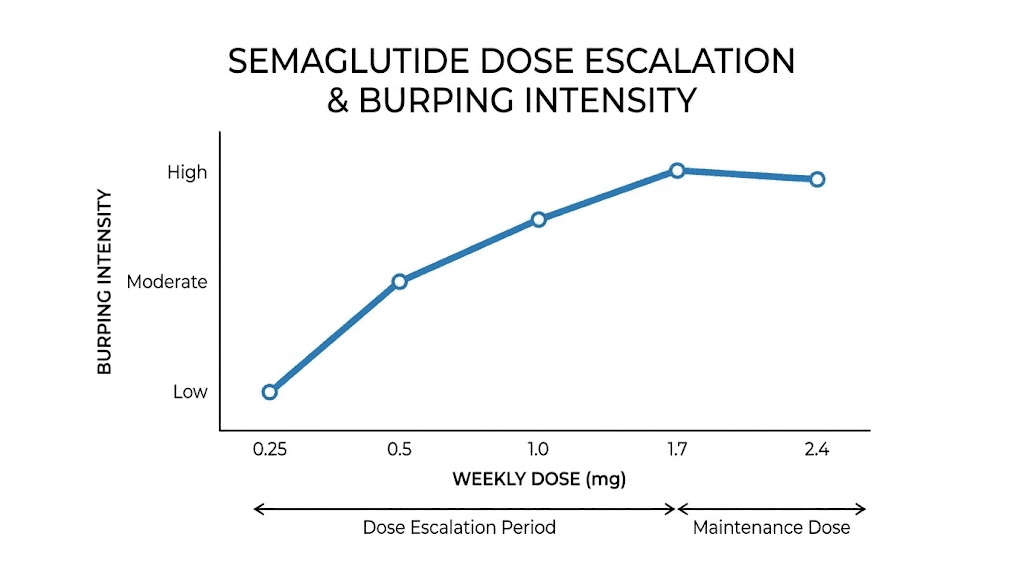
The delay is dose-dependent. Higher doses produce more pronounced emptying delays. This is why many people notice burping worsening after dose escalations. The 0.25mg starting dose causes minimal gastric emptying changes. By the time you reach 1mg or 2.4mg, the effect is substantial.
Hydrogen sulfide and sulfur burps
Not all semaglutide burps smell. But the ones that do carry a distinctive sulfur odor that comes from hydrogen sulfide gas. This gas is produced by sulfate-reducing bacteria in your gut, particularly species like Desulfovibrio and Bilophila. These bacteria thrive on sulfur-containing amino acids found in proteins, cruciferous vegetables, and certain dairy products.
Under normal circumstances, hydrogen sulfide production is balanced by rapid food transit through the digestive tract. Your gut produces small amounts of hydrogen sulfide constantly. You typically do not notice it because the gas is absorbed by intestinal cells, converted to sulfate, and excreted through urine. The system works.
When semaglutide slows gastric emptying, that balance breaks. Sulfur-containing foods linger in the stomach longer. Sulfate-reducing bacteria have more time to convert sulfur compounds into hydrogen sulfide. The gas accumulates faster than your body can absorb and process it. The excess escapes as sulfur burps.
Recent research also shows that semaglutide may directly alter gut microbiome composition. Specifically, it appears to increase populations of Akkermansia muciniphila, a bacterium associated with improved metabolic health but also known to produce hydrogen sulfide as a metabolic byproduct. The medication may simultaneously slow food transit and increase the bacterial population responsible for sulfur gas production. Understanding peptide safety considerations includes recognizing these microbiome effects.
The air swallowing factor
There is another contributor that most guides overlook. Semaglutide-related nausea causes many people to swallow more air than usual. When you feel nauseous, you tend to swallow more frequently, breathe through your mouth more, and eat more slowly with more deliberate swallowing motions. Each swallow sends a small bolus of air into your stomach.
This aerophagia compounds the fermentation-related gas production. You now have both bacterial gas and swallowed air contributing to gastric pressure. The burping becomes more frequent and sometimes more forceful than fermentation alone would produce.
People who experience significant semaglutide fatigue or nausea alongside burping often find that addressing the nausea reduces burping frequency. The two symptoms are linked through this air-swallowing mechanism.
When semaglutide burping starts and how long it lasts
Timing matters. Knowing when to expect burping and how long it typically persists helps you plan your management strategy and set realistic expectations.
Onset timeline
Most people notice burping within the first four to eight weeks of starting semaglutide. The FDA pharmacovigilance data classifies eructation as an "early failure type" event, with a median onset of six days from treatment initiation. That means half of all reported cases began within the first week.
But there is significant individual variation. Some people burp from the very first dose. Others do not notice anything until their first or second dose escalation. The pattern often follows this trajectory:
Week 1-2 (0.25mg dose): Minimal or no burping for most people. The dose is too low to cause significant gastric emptying changes. Mild nausea is more common than burping at this stage.
Week 3-4 (still 0.25mg or transitioning to 0.5mg): Burping begins for early responders. Usually mild and intermittent. Often occurs 30-90 minutes after meals.
Week 5-8 (0.5mg dose): Burping becomes noticeable for many people. Sulfur burps may appear for the first time. The correlation with specific meals becomes apparent.
Week 9-16 (1mg dose and beyond): Peak burping intensity for those who experience it. Dose-dependent gastric emptying delays are most pronounced. This is when people either adapt or seek solutions.
The appetite suppression timeline roughly parallels the burping timeline. Both effects stem from the same GLP-1 receptor activation that slows gastric emptying.
Duration and adaptation
For many people, burping is a temporary side effect that improves as the body adapts to semaglutide. The adaptation timeline varies widely.
Some studies suggest that gastrointestinal side effects improve within four to eight weeks at each dose level. Your body gradually adjusts to the new gastric emptying rate. Stomach contractions begin to partially compensate for the GLP-1-mediated slowing. Gut bacteria populations shift to accommodate the changed transit times.
However, adaptation is not universal. Some people experience persistent burping throughout their entire treatment course. These tend to be individuals with pre-existing gastroparesis, irritable bowel syndrome, or other digestive conditions that amplify the gastric emptying delay. For this group, management strategies become essential rather than optional.
People considering long-term semaglutide use should know that the adaptation process typically completes within three to four months at each stable dose. If burping persists beyond that window, it is unlikely to resolve spontaneously and needs active management.
Foods that trigger semaglutide burping
Diet is the single most controllable factor in semaglutide-related burping. The food you eat determines what your gut bacteria have to work with. Change the substrate and you change the gas output. It really is that direct.
High-sulfur foods to limit
These foods provide the raw material for hydrogen sulfide production. They are not inherently bad foods, and most are nutritionally valuable. But when your gastric emptying is slowed by semaglutide, they spend more time being fermented by sulfate-reducing bacteria.
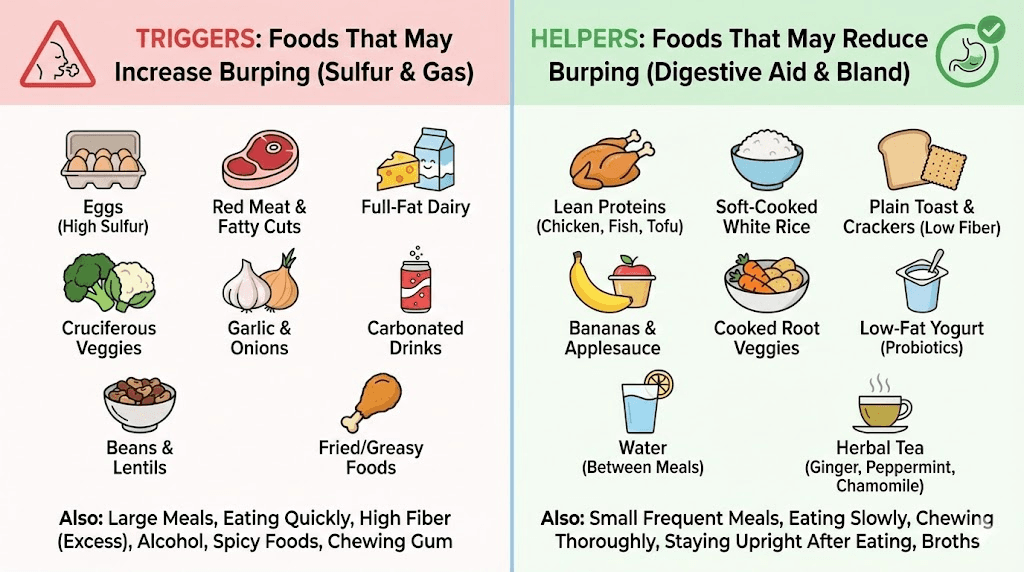
Eggs. Among the highest dietary sources of sulfur-containing amino acids. Egg yolks in particular contain cysteine and methionine in concentrated amounts. Many semaglutide users identify eggs as their number one sulfur burp trigger. You do not need to eliminate eggs entirely, but eating three scrambled eggs for breakfast while on semaglutide is asking for trouble.
Cruciferous vegetables. Broccoli, cauliflower, Brussels sprouts, cabbage, and kale all contain glucosinolates, which are sulfur-containing compounds. These vegetables are among the healthiest foods available, which creates a frustrating dilemma. The solution is portion control and preparation method. Steaming reduces glucosinolate content compared to eating raw. Smaller portions fermented over a shorter period produce less gas.
Alliums. Onions, garlic, leeks, and shallots contain sulfur compounds that contribute to hydrogen sulfide production. Garlic is particularly potent because allicin, its primary bioactive compound, is a sulfur-based molecule. Cooked alliums produce fewer sulfur burps than raw alliums, but the effect is not eliminated entirely.
Red meat. High in sulfur-containing amino acids, particularly methionine and cysteine. Ground beef is frequently identified by semaglutide users as a trigger food. Leaner cuts produce fewer sulfur burps than fattier cuts, because the fat content slows digestion even further on top of the semaglutide effect.
Dairy products. Milk, cheese, and yogurt contain sulfur-containing amino acids. Whey protein is especially concentrated. People who rely on protein shakes to meet their nutritional needs while on semaglutide often discover that whey-based shakes trigger severe sulfur burps. Plant-based protein powders produce significantly less sulfur gas.
Users tracking their semaglutide diet should pay particular attention to sulfur content alongside the standard nutritional considerations. The semaglutide diet plan works best when it accounts for both nutritional adequacy and digestive tolerance.
Gas-producing foods to watch
Beyond sulfur-specific triggers, certain foods produce excess gas through carbohydrate fermentation. These contribute to burping volume even if the burps do not carry sulfur odor.
Beans and legumes. Contain oligosaccharides that humans cannot digest. Gut bacteria ferment these sugars, producing carbon dioxide, hydrogen, and methane. Soaking beans overnight and cooking them thoroughly reduces oligosaccharide content, but does not eliminate it.
Carbonated beverages. This one seems obvious, but many people overlook it. Every sip of soda, sparkling water, or beer delivers carbon dioxide directly into your stomach. When gastric emptying is already delayed, that CO2 has nowhere to go but up. Eliminating carbonated drinks is the single fastest way to reduce burping frequency.
Sugar alcohols. Sorbitol, xylitol, erythritol, and maltitol are poorly absorbed in the small intestine. They reach the colon largely intact and serve as fermentation substrate for gas-producing bacteria. Sugar-free gum, diet candies, and many "keto-friendly" products contain these sweeteners. The combination of semaglutide-delayed transit and sugar alcohol fermentation creates significant gas.
High-fiber foods in excessive amounts. Fiber is essential during semaglutide treatment to maintain digestive regularity. But a sudden large increase in fiber intake overwhelms your gut microbiome capacity. Increase fiber gradually. Five grams per day added over two weeks is much better tolerated than twenty grams added overnight.
Foods that help reduce burping
Just as some foods make burping worse, others actively help reduce it.
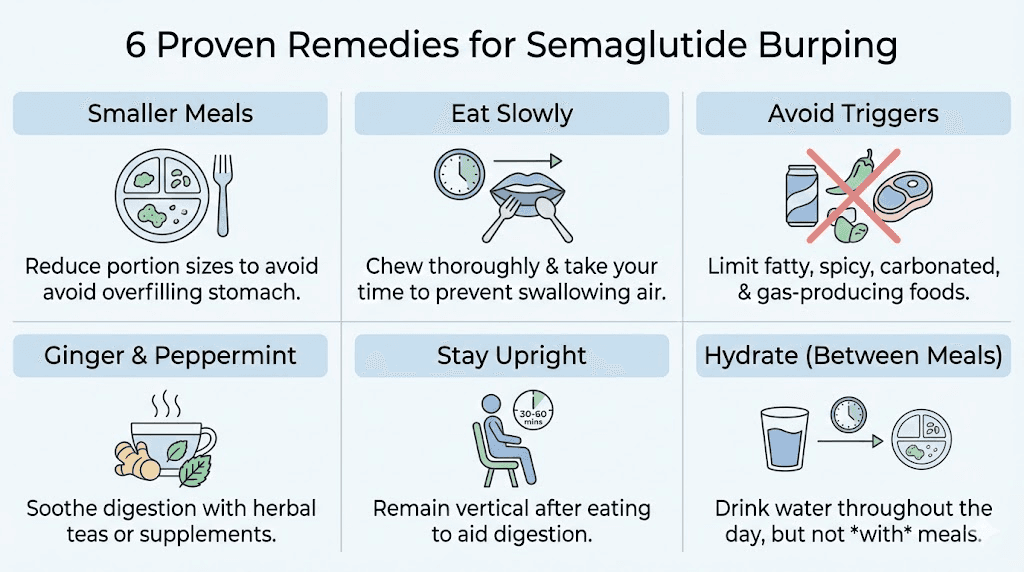
Ginger. A prokinetic food that promotes gastric motility. Ginger tea before or after meals can partially counteract the gastric emptying delay caused by semaglutide. It also has antiemetic properties that reduce the nausea-related air swallowing that contributes to burping. Fresh ginger is more effective than dried or powdered forms.
Pineapple. Contains bromelain, a digestive enzyme that breaks down proteins more efficiently. Multiple semaglutide users report that pineapple chunks or pineapple juice significantly reduce sulfur burps. The mechanism is straightforward. Faster protein digestion means less substrate available for sulfate-reducing bacteria.
Fennel and fennel tea. Has carminative properties that help relax smooth muscle in the digestive tract and facilitate gas expulsion. Fennel tea after meals is a traditional remedy for gas and bloating that works alongside semaglutide management. People following a GLP-1 compatible diet often include fennel as a digestive aid.
Lean proteins. Chicken breast, turkey, and fish contain less sulfur per gram than red meat. They are also digested more quickly, reducing fermentation time. Switching your primary protein source from beef to poultry often produces noticeable improvement in sulfur burp frequency.
Fermented foods. Kimchi, sauerkraut, kefir, and kombucha introduce beneficial bacteria that can help rebalance the gut microbiome. Start with small amounts. Fermented foods can initially increase gas before the beneficial bacterial populations establish themselves. One tablespoon daily is a reasonable starting dose.
Proven remedies for semaglutide burping
Management works. Not every approach works for every person, but the combination of dietary modification, timing adjustments, and targeted interventions resolves or significantly reduces burping for the vast majority of semaglutide users. The strategies below are ordered from simplest and most effective to more targeted interventions.
Meal timing and portion control
This is the highest-impact, lowest-effort change you can make. Eat smaller meals more frequently. Four to six small meals instead of two to three large ones. The logic is simple. Smaller food volumes produce less gas when they ferment. They also clear the stomach faster even with semaglutide-delayed emptying, because there is less total volume to process.
Portion size matters more than most people realize. Before semaglutide, you might eat a full plate and feel fine. On semaglutide, that same plate overwhelms your slowed digestive system. The food has nowhere to go. It sits. It ferments. You burp.
Cut your typical portion in half. If you are still hungry after 20 minutes, eat more. Most people find that the semaglutide appetite suppression kicks in before they finish the half portion. You end up eating less, producing less gas, and feeling more comfortable. People managing their semaglutide schedule should coordinate meal timing with their injection schedule for optimal digestive comfort.
Eating speed matters too. Eating quickly means swallowing more air and delivering larger food boluses to a stomach that cannot process them efficiently. Slow down. Chew each bite 20-30 times. Put your fork down between bites. This simple behavioral change reduces both aerophagia and the volume of food that reaches your stomach per unit time.
Injection timing optimization
When you take your injection relative to meals affects burping severity. Many users report that injecting in the evening or before bed produces fewer daytime GI symptoms compared to morning injections. The logic makes sense. The initial peak of gastric emptying delay occurs during sleep, when you are not eating. By the time you have your first meal, the delay is still present but less intense.
Some people find that eating a light meal before their injection and then fasting for four to six hours afterward reduces burping. This gives the pre-injection food time to clear before the maximum gastric emptying delay kicks in. Others prefer injecting on an empty stomach and waiting two to three hours before eating.
There is no universally optimal timing. Individual variation in semaglutide pharmacokinetics means you need to experiment. Track your burping intensity and timing for two to three weeks while varying your injection timing. The pattern will become clear. Understanding the semaglutide dosing structure helps you plan injection timing that minimizes GI disturbance.
Over-the-counter medications
Simethicone (Gas-X). Works by reducing surface tension of gas bubbles in the stomach, allowing them to coalesce into larger bubbles that are easier to expel. It does not prevent gas formation. It makes the gas that forms easier to release. Simethicone is safe for long-term use and has no significant drug interactions with semaglutide. Take 80-125mg after meals or when burping becomes bothersome.
Bismuth subsalicylate (Pepto-Bismol). Binds hydrogen sulfide in the stomach, reducing sulfur burp odor and intensity. Many semaglutide users call Pepto-Bismol their most effective remedy specifically for sulfur burps. The bismuth compound reacts with hydrogen sulfide to form bismuth sulfide, which is insoluble and passes through the digestive tract without releasing odor. Take one to two tablets when sulfur burps begin. Do not use for more than eight weeks continuously without medical guidance.
Famotidine (Pepcid). Reduces stomach acid production, which can decrease the acidity-driven activation of sulfate-reducing bacteria. Some users report immediate relief from burping after taking famotidine. It also helps with the acid reflux that sometimes accompanies semaglutide burping. Take 10-20mg before meals.
Antacids (Alka-Seltzer, Tums). Neutralize stomach acid and can provide quick relief from burping associated with acid reflux. Alka-Seltzer effervescent tablets also help break up gas bubbles. However, regular antacid use can interfere with nutrient absorption over time. Use as-needed rather than prophylactically.
Digestive enzymes and supplements
Digestive enzyme supplements. Taken before meals, these supplements provide additional protease, lipase, and amylase enzymes that accelerate food breakdown. Faster breakdown means less substrate for bacterial fermentation. Users report that taking a broad-spectrum digestive enzyme 15-20 minutes before meals significantly reduces post-meal burping.
Probiotics. Targeted probiotic strains can help rebalance gut microbiome composition away from sulfate-reducing bacteria toward beneficial species. Look for strains containing Lactobacillus and Bifidobacterium species. These compete with sulfate-reducing bacteria for nutrients and can reduce hydrogen sulfide production over time. Effects take two to four weeks to become noticeable. People exploring semaglutide supplement stacks often include probiotics as a core component.
Peppermint oil capsules. Enteric-coated peppermint oil capsules relax smooth muscle in the digestive tract, which can facilitate gas movement and reduce the pressure that triggers burping. Take one capsule 30-60 minutes before meals. Do not use uncoated peppermint oil capsules, as they dissolve in the stomach and can worsen heartburn.
Activated charcoal. Adsorbs gases in the digestive tract, including hydrogen sulfide. Can provide relief from sulfur burps when taken between meals. However, activated charcoal also adsorbs medications and nutrients, so it must be taken at least two hours away from semaglutide injection and other medications. This timing requirement limits its practical usefulness.
Lifestyle modifications
Stay upright after eating. Gravity helps. When you lie down after a meal, gas that would normally rise to the top of your stomach and be released through a mild burp instead gets trapped. Stay upright for at least 30-60 minutes after eating. A gentle walk after meals further promotes gastric motility and gas expulsion.
Avoid eating close to bedtime. Late-night eating on semaglutide is a recipe for nocturnal burping and morning sulfur burps. Your already-delayed gastric emptying becomes even slower during sleep. Give your stomach at least three to four hours to process food before lying down for the night.
Reduce stress. Stress increases air swallowing and alters gut motility patterns. Both effects worsen semaglutide-related burping. Basic stress management, whether through deep breathing, meditation, or simple relaxation, can measurably reduce burping frequency. This is not pseudoscience. The gut-brain axis is a well-documented physiological system, and stress-related GI symptoms are clinically recognized.
Hydrate adequately. Water helps dilute stomach contents and can facilitate gastric emptying. Sip water throughout the day rather than drinking large volumes at meals, which would further distend an already-slow stomach. Many people on semaglutide underhydrate because their reduced appetite extends to reduced thirst cues. Aim for at least 64 ounces of water daily.
Semaglutide burping versus other GI side effects
Burping does not exist in isolation. It is part of a constellation of gastrointestinal effects that semaglutide produces through the same mechanism. Understanding how these symptoms relate helps you address the root cause rather than chasing individual symptoms.
The GI symptom spectrum
The FDA prescribing information for Wegovy lists the following GI side effect rates at the 2.4mg dose:
Nausea: 44% of patients. The most common GI side effect. Usually peaks in the first four to eight weeks and improves over time. Strongly dose-dependent. People wondering why they are not seeing results early on should know that the GI adaptation period often corresponds with the initial weight loss phase.
Diarrhea: 30% of patients. Can alternate with constipation. Results from altered gut motility patterns as the digestive tract adjusts to changed transit times.
Vomiting: 24% of patients. More common during dose escalation. Usually indicates the stomach is overwhelmed by food volume relative to its emptying capacity.
Constipation: 24% of patients. A paradoxical effect. While semaglutide slows gastric emptying, it can also slow colonic transit in some individuals. Semaglutide constipation requires different management strategies than burping.
Abdominal pain: 20% of patients. Often accompanies gas and bloating. Can indicate gastric distension from accumulated gas and food.
Burping: 7% of patients (reported). Real-world prevalence likely higher due to underreporting.
The pharmacovigilance data tells a more nuanced story. Among the 5,442 GI adverse events reported to the FDA, eructation had a reporting odds ratio of 42.03. That means burping was reported 42 times more frequently relative to semaglutide than to other medications in the database. Compare that to nausea with an ROR of about 4. Burping is not the most common side effect. But it is the most disproportionately associated with semaglutide specifically.
Burping with nausea
When burping and nausea occur together, they create a feedback loop. Nausea causes increased air swallowing. Swallowed air increases gastric distension. Distension triggers more burping. Burping temporarily relieves distension but the nausea persists, restarting the cycle.
Breaking this cycle requires addressing both symptoms simultaneously. Anti-nausea measures like ginger, small meals, and proper hydration reduce the air-swallowing component. Anti-gas measures like simethicone and dietary modification reduce the fermentation component. Together, they interrupt the feedback loop more effectively than targeting either symptom alone.
People experiencing combined nausea and burping should review whether their dosing schedule allows adequate adaptation time between dose increases. Rushing through the titration schedule is the number one cause of severe combined GI symptoms.
Burping with sulfur smell versus odorless burping
The distinction matters for management. Odorless burping is primarily driven by swallowed air and carbon dioxide from general fermentation. Sulfur burps specifically indicate hydrogen sulfide production by sulfate-reducing bacteria.
Odorless burping responds best to behavioral changes. Eat slower. Avoid carbonated drinks. Reduce portion sizes. Stay upright after meals. These modifications reduce air swallowing and general gas production.
Sulfur burps require dietary intervention targeting sulfur-containing foods. Reduce eggs, cruciferous vegetables, alliums, red meat, and dairy. Increase lean proteins, ginger, and pineapple. Consider Pepto-Bismol specifically for sulfur odor reduction. Probiotics help shift bacterial populations away from sulfate-reducing species.
Some people experience both types simultaneously. In that case, combine strategies from both approaches. Start with the behavioral changes (they are easier to implement) and add dietary modifications as needed. Track which specific interventions produce the most improvement for your particular symptom pattern.
Dose-dependent burping patterns
The relationship between semaglutide dose and burping severity follows a predictable pattern. Higher doses produce more pronounced gastric emptying delays, which produce more fermentation, which produces more gas, which produces more burping. Understanding this relationship helps you anticipate and manage symptoms during dose escalation.
Burping at each dose level
0.25mg (initiation dose): Most people experience no burping at this dose. Gastric emptying changes are minimal. If you burp at this dose, you are likely a sensitive responder and should expect more significant symptoms at higher doses. Use this period to establish good dietary habits before symptoms intensify.
0.5mg: Burping begins for some people. Usually mild and intermittent. Typically post-meal and resolves within one to two hours. This is the dose where most people first notice that certain foods seem to cause more gas than before.
1mg: Moderate burping for susceptible individuals. Sulfur burps may appear for the first time. Meal-dependent patterns become clear. This is the dose level where most people who will develop significant burping first notice it as a genuine nuisance rather than a minor curiosity. People tracking their semaglutide dosing should note GI symptoms at each level to identify their personal threshold.
1.7mg: Increased burping frequency and intensity. The transition from 1mg to 1.7mg represents one of the larger proportional dose jumps in the semaglutide titration schedule. Many people who were managing burping adequately at 1mg find that 1.7mg overwhelms their current management strategy.
2.4mg (maintenance dose): Maximum gastric emptying delay. If burping is going to be a persistent issue, it is most apparent at this dose. However, people who have been on semaglutide for several months by the time they reach 2.4mg may have already adapted to the GI effects. The body has had time to adjust.
The semaglutide dosing chart and syringe dosage chart can help you understand exactly where you are in the titration process and anticipate what to expect at the next level.
Managing dose escalation burping
Each dose increase essentially restarts the GI adaptation process. Your body had adjusted to the previous dose and now needs to adjust again. This is normal. It does not mean the medication is wrong for you or that you cannot tolerate higher doses.
Strategies for managing dose-transition burping:
Front-load dietary changes before escalating. If you know a dose increase is coming next week, start reducing sulfur-containing foods and implementing portion control now. Give your digestive system the best possible substrate to work with before adding the additional gastric emptying delay.
Consider extended titration. If burping is severe at a new dose, discuss spending extra time at that level before escalating further. Standard titration calls for four weeks at each dose. Some providers extend to six or eight weeks if GI tolerance is poor. The appetite suppression benefits continue building during this extended period.
Do not skip doses to avoid symptoms. Skipping doses creates inconsistent GLP-1 receptor stimulation, which can actually worsen GI symptoms when you resume. Consistent, on-schedule dosing produces more predictable gastric emptying patterns that your body can adapt to. If you are wondering why you are not losing weight, inconsistent dosing is often the culprit.
When semaglutide burping is a warning sign
Most semaglutide-related burping is benign. Uncomfortable? Yes. Socially inconvenient? Absolutely. Dangerous? Almost never. But there are situations where burping signals something that needs medical attention.
Red flags that require medical evaluation
Severe abdominal pain with burping. Mild discomfort is expected. Sharp, severe, or persistent pain is not. Severe abdominal pain could indicate pancreatitis, a rare but serious side effect of GLP-1 medications. The FDA prescribing information includes pancreatitis as a warning for semaglutide. Pain that radiates to the back, worsens after eating, or is accompanied by fever requires immediate medical evaluation.
Burping with persistent vomiting. Occasional vomiting during dose escalation is common. Persistent vomiting lasting more than 24 hours is not. It can indicate gastroparesis, which is a more severe form of delayed gastric emptying where the stomach essentially stops functioning normally. This requires medication adjustment and possibly additional treatment.
Blood in vomit or stool. Any sign of GI bleeding, whether bright red blood in vomit, dark coffee-ground material in vomit, or black tarry stools, requires immediate medical attention. While semaglutide itself does not typically cause GI bleeding, the combination of increased stomach acid exposure and delayed emptying can exacerbate pre-existing conditions like ulcers or esophagitis.
Inability to keep fluids down. If burping is so severe that it triggers vomiting every time you eat or drink, dehydration becomes a concern. Dehydration on semaglutide is particularly risky because the medication can also affect kidney function. If you cannot maintain adequate hydration for more than 24 hours, contact your healthcare provider.
Progressive worsening over weeks. Burping that gets worse over time rather than staying stable or improving suggests an underlying issue beyond normal semaglutide GI effects. It could indicate a developing infection, gallbladder disease (gallstones are more common during rapid weight loss), or worsening gastroparesis. Anyone monitoring their response to semaglutide should track symptom trends over time.
Yellowing of skin or eyes. Jaundice with burping could indicate gallbladder or liver involvement. Rapid weight loss from semaglutide increases gallstone risk. Gallstones can cause biliary stasis, which produces excessive burping, upper abdominal pain, and jaundice. This needs urgent medical evaluation.
Pre-existing conditions that amplify burping
Certain conditions make semaglutide-related burping significantly worse. If you have any of these, discuss them with your prescriber before starting treatment:
Gastroparesis. If your stomach already empties slowly, adding semaglutide on top creates compounding delays. Food can sit for six to eight hours or more. The fermentation and gas production become extreme. People with diabetic gastroparesis need especially careful titration and monitoring.
GERD (gastroesophageal reflux disease). The combination of increased gastric pressure from gas accumulation and delayed emptying can worsen acid reflux dramatically. Burping in GERD patients often brings stomach acid into the esophagus, causing heartburn and potentially damaging esophageal tissue.
Small intestinal bacterial overgrowth (SIBO). Excess bacteria in the small intestine produce additional gas beyond what normal stomach flora generate. Semaglutide-delayed transit gives these bacteria even more time to ferment food. People with SIBO may experience dramatically worse burping than the general population.
Irritable bowel syndrome (IBS). Visceral hypersensitivity in IBS means that normal amounts of gas feel more painful and uncomfortable. The gas volume that would cause mild burping in a healthy person can cause significant distress in someone with IBS.
Understanding the full picture of peptide safety means accounting for how pre-existing conditions interact with medication effects. Your provider should evaluate your complete medical history before prescribing semaglutide.
Semaglutide burping versus tirzepatide burping
If semaglutide burping is unbearable, you might wonder whether switching to tirzepatide would help. The answer is nuanced.
Tirzepatide also causes burping through the same delayed gastric emptying mechanism. Clinical trial data shows eructation rates of approximately 4% for tirzepatide versus 7% for semaglutide at weight-loss doses. That is a meaningful difference but not a dramatic one. Both medications slow gastric emptying. Both produce fermentation-related gas. Both cause sulfur burps in susceptible individuals.
The overall GI side effect profile differs between the two medications. Comparing semaglutide and tirzepatide side effects reveals that tirzepatide tends to produce slightly less nausea (approximately 27% vs 44% at weight-loss doses) but comparable rates of diarrhea and constipation. The reduced nausea with tirzepatide means less air swallowing, which may partly explain the lower burping rate.
People who switch from semaglutide to tirzepatide sometimes report improvement in burping. Others report no change. And some report that tirzepatide produces different GI symptoms that are equally bothersome. The switching process itself can temporarily worsen GI symptoms as your body adjusts to the new medication pharmacokinetics.
The tirzepatide dosing schedule follows a different titration pattern than semaglutide, which means the timing of GI symptom onset and adaptation will differ even if you experience the same types of symptoms.
Before switching medications specifically because of burping, exhaust the management strategies above. Dietary modification, portion control, simethicone, and Pepto-Bismol resolve burping for the vast majority of semaglutide users without requiring a medication change. The conversion chart between the two medications can help if a switch is ultimately needed.
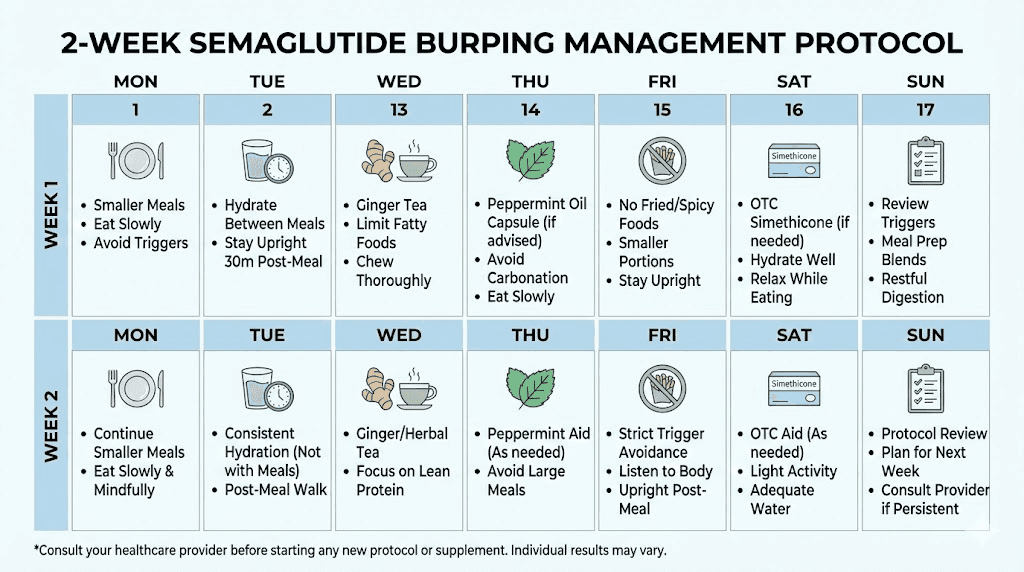
Complete management protocol for semaglutide burping
Rather than trying individual remedies one at a time, here is a structured protocol that addresses all the mechanisms simultaneously. Follow this for two weeks. Most people see significant improvement within that timeframe.
Week one: Foundation changes
Day 1-3: Dietary reset. Eliminate the top sulfur-burp triggers. No eggs, no cruciferous vegetables, no raw onions or garlic, no red meat, no whey protein. Replace with chicken breast, rice, steamed vegetables, and plant-based protein. This is not permanent. It is a diagnostic elimination to see how much of your burping is diet-driven. People developing their semaglutide meal plan can use this elimination period as a starting point.
Day 1-7: Portion control. Cut all meal portions in half immediately. Eat five to six small meals instead of two to three large ones. No meal should exceed the volume of your fist. If you are hungry between meals, that is fine. Eat another small meal. The goal is never filling your stomach more than halfway.
Day 1-7: Eliminate carbonated beverages. All of them. Sparkling water, soda, beer, champagne. Switch to still water, herbal tea, or non-carbonated drinks. This alone reduces burping by 30-50% for many people.
Day 1-7: Start simethicone. Take 80-125mg after each meal. This reduces gas bubble formation and makes any remaining burps less forceful. Available over the counter as Gas-X or store-brand equivalents.
Week two: Refinement
Day 8-10: Reintroduce foods one at a time. Add back one eliminated food category per day. Eggs on day 8. Cruciferous vegetables on day 9. Red meat on day 10. Note which reintroductions cause burping to return. Those are your personal trigger foods. Eliminate them long-term or keep portions very small.
Day 8-14: Add targeted supplements. Start a probiotic containing Lactobacillus and Bifidobacterium strains. Take digestive enzymes 15 minutes before your two largest meals. Add fresh ginger tea after meals if burping persists. These interventions take time to build their effect, so starting in week two allows the foundation changes to show results first.
Day 8-14: Optimize injection timing. If you currently inject in the morning, try switching to evening or bedtime injection. Track burping for the remainder of week two and compare to week one. Some people experience 40-60% reduction in daytime burping just from this timing change.
Ongoing maintenance
After the two-week protocol, you should have a clear picture of what triggers your burping and what manages it. Your ongoing plan will likely include:
A modified diet that limits your personal trigger foods while maintaining nutritional adequacy. Continued portion control with five to six small meals daily. Regular probiotic and digestive enzyme supplementation. As-needed simethicone or Pepto-Bismol for breakthrough symptoms. Optimized injection timing based on your week-two experiment.
Track symptoms monthly. As your body continues to adapt to semaglutide, you may be able to gradually reintroduce trigger foods in small amounts. Many people find that by month four to six, their burping has decreased significantly regardless of dietary changes, because the body has adapted to the altered gastric emptying pattern.
For researchers and members using SeekPeptides resources for protocol optimization, tracking GI side effects alongside treatment outcomes provides valuable data for adjusting both dietary and medication protocols.
The science behind why some people burp more than others
Not everyone on semaglutide burps. Some people experience zero GI symptoms beyond mild appetite reduction. Others are miserable from the first dose. The difference comes down to several biological factors that vary between individuals.
Gut microbiome composition
Your baseline gut microbiome composition determines how much gas your digestive system produces from any given food substrate. People with higher populations of sulfate-reducing bacteria produce more hydrogen sulfide. People with higher populations of methanogenic archaea produce more methane. People with balanced, diverse microbiomes tend to produce less gas overall.
Microbiome composition is influenced by diet, antibiotic history, geography, genetics, and dozens of other factors. Two people eating the same meal on the same semaglutide dose can have dramatically different gas production profiles because their gut bacteria are fundamentally different. This is why blanket dietary advice does not work for everyone. Your gut flora is unique, and your burping triggers will be partially unique as well.
Baseline gastric emptying rate
People with naturally fast gastric emptying have more "buffer" before semaglutide-delayed emptying becomes problematic. If your stomach normally empties in two hours and semaglutide slows it by 30%, your new emptying time is about 2.6 hours. Still within normal range. Minimal fermentation increase. Minimal burping.
But if your baseline emptying time is already slow at four hours and semaglutide adds another 30%, you are now at 5.2 hours. That puts you into territory where fermentation becomes significant. More gas. More burping. More sulfur production.
Baseline gastric emptying varies based on age, diabetes status, thyroid function, and medications. Older adults tend to have slower baseline emptying. People with type 2 diabetes may have subclinical gastroparesis that semaglutide unmasks. Understanding how these factors affect overall semaglutide response requires accounting for individual digestive physiology.
Genetic factors
Certain genetic variants affect GLP-1 receptor sensitivity. People with more sensitive GLP-1 receptors experience stronger gastric emptying delays at lower doses. They may need smaller dose increments and more gradual titration to avoid overwhelming their digestive capacity.
Other genetic variants affect enzyme production in the digestive tract. People with lower natural production of lactase, alpha-galactosidase, or other digestive enzymes are more susceptible to fermentation-related gas because they incompletely digest certain food components. The undigested material becomes bacterial substrate, producing gas.
Dietary baseline
What you ate before starting semaglutide matters. If your pre-semaglutide diet was high in processed foods, sugar, and refined carbohydrates, your gut bacteria are adapted to fermenting those substrates quickly. When semaglutide slows transit and you continue eating the same diet, the bacteria have more time to work on their preferred substrates. Gas production spikes.
Conversely, if your pre-semaglutide diet was already focused on lean proteins, vegetables, and whole grains, your gut bacteria are adapted to a lower-fermentation diet. The addition of semaglutide-delayed emptying produces less dramatic gas increases because there is less fermentable substrate to begin with.
This is why the dietary recommendations for semaglutide emphasize starting dietary changes before or simultaneously with medication initiation. Waiting until burping becomes a problem means you are already behind.
Compounded semaglutide and burping
People using compounded semaglutide sometimes report different burping patterns than those using brand-name Ozempic or Wegovy. There are several potential explanations.
First, compounded semaglutide may have different concentration profiles. If the compounding pharmacy formulation delivers a slightly different pharmacokinetic curve, the gastric emptying pattern will differ. More variable delivery means less predictable GI symptoms.
Second, compounded formulations may include different excipients (inactive ingredients) that affect stomach chemistry. Some excipients are themselves fermentable or can alter stomach pH in ways that influence bacterial gas production.
Third, dosing accuracy varies between compounding pharmacies. If your actual dose is higher than intended due to reconstitution errors, you will experience more pronounced gastric emptying delays and more burping. Use the semaglutide dosage calculator and reconstitution calculator to verify your actual dose.
Proper compounded semaglutide storage also affects the degradation profile. Degraded semaglutide may not produce the same clean GLP-1 receptor activation, potentially causing irregular GI symptoms. Ensure your compounded product is stored at proper temperature and used within the recommended shelf life.
Whether you are using brand-name or compounded semaglutide, the management strategies for burping are identical. The mechanism is the same. The trigger foods are the same. The remedies are the same. The only difference is that compounded formulations introduce an additional variable of manufacturing consistency that brand-name products eliminate.
Semaglutide supplements that help with burping
Beyond the targeted remedies discussed above, certain supplements commonly taken alongside semaglutide can help reduce burping as a secondary benefit.
B12. Semaglutide with B12 is increasingly popular as a combination therapy. While B12 does not directly reduce burping, adequate B12 levels support healthy digestive function and mucosal integrity. B12 deficiency, which semaglutide can worsen through reduced intrinsic factor production, causes digestive dysfunction that can amplify GI symptoms including burping.
Glycine. Semaglutide with glycine is used for mucosal protection and improved GI tolerance. Glycine has been shown to improve gastric motility and protect stomach lining integrity. Some users report reduced burping and bloating when adding glycine supplementation.
Methylcobalamin. Semaglutide with methylcobalamin provides the most bioavailable form of B12 supplementation. Better absorption means more reliable digestive support and less amplification of GI symptoms from nutrient deficiency.
The supplement strategy for GLP-1 medications applies broadly across semaglutide and tirzepatide. Building a targeted supplement protocol that addresses both nutritional needs and GI symptom management produces better outcomes than treating each issue in isolation.
Frequently asked questions
Does semaglutide cause burping?
Yes. Burping occurs in approximately 7% of people taking Wegovy (semaglutide 2.4mg) and 3-5% at lower Ozempic doses. FDA pharmacovigilance data shows burping has the highest reporting odds ratio of any GI side effect at 42.03. The mechanism involves delayed gastric emptying that allows food to ferment and produce gas in the stomach.
Why do my burps smell like rotten eggs on semaglutide?
Sulfur burps occur when sulfate-reducing bacteria in your gut convert sulfur-containing amino acids from food into hydrogen sulfide gas. Semaglutide slows digestion, giving these bacteria more time to produce hydrogen sulfide. Reducing intake of eggs, red meat, cruciferous vegetables, and dairy can significantly reduce sulfur burp frequency. Review our semaglutide diet recommendations for more guidance.
How long does semaglutide burping last?
For most people, burping improves within four to eight weeks at each stable dose as the body adapts. Some people adapt within two weeks. Others experience persistent burping throughout treatment, particularly those with pre-existing digestive conditions. Active management through dietary changes and OTC remedies can reduce symptoms significantly regardless of adaptation timeline.
What is the best medicine for semaglutide burping?
Simethicone (Gas-X) is the most widely recommended first-line treatment for general burping. For sulfur burps specifically, bismuth subsalicylate (Pepto-Bismol) is more effective because it binds hydrogen sulfide. Digestive enzymes taken before meals and probiotics for long-term microbiome support are excellent complementary approaches. Use the peptide dosing guide to ensure your semaglutide dose is not higher than necessary.
Can I take Pepto-Bismol with semaglutide?
Yes. Bismuth subsalicylate does not have clinically significant interactions with semaglutide. However, do not use Pepto-Bismol continuously for more than eight weeks without medical guidance. It contains salicylate, which is chemically related to aspirin. Short-term use for managing sulfur burps is generally considered safe.
Will switching from semaglutide to tirzepatide reduce burping?
Possibly. Clinical trials show tirzepatide has a lower burping rate (approximately 4% vs 7%) compared to semaglutide at weight-loss doses. However, tirzepatide also causes delayed gastric emptying and can produce similar GI symptoms. Review the full side effect comparison before switching, and exhaust management strategies for semaglutide first.
Does semaglutide burping go away after stopping the medication?
Yes. Semaglutide-related burping resolves completely after discontinuation, though it may take one to two weeks for gastric emptying to return to baseline as the medication clears your system. Semaglutide has a half-life of approximately one week, so GI effects diminish gradually rather than stopping immediately. Understanding semaglutide discontinuation effects helps set appropriate expectations.
Should I stop semaglutide because of burping?
Burping alone is not a reason to stop semaglutide. The management strategies outlined in this guide resolve or significantly reduce burping for the vast majority of users. Only stop semaglutide for burping if it is accompanied by severe abdominal pain, persistent vomiting, signs of GI bleeding, or other warning signs described above. Always consult your prescriber before stopping.
External resources
FDA Pharmacovigilance Study on Semaglutide GI Adverse Events (PMC)
National Institute of Diabetes and Digestive and Kidney Diseases: Gas in the Digestive Tract
For researchers committed to optimizing their semaglutide protocols and managing side effects effectively, SeekPeptides offers comprehensive protocol guides, dosing calculators, and a community of experienced members who have navigated these exact challenges.
In case I do not see you, good afternoon, good evening, and good night. May your stomach stay settled, your burps stay silent, and your protocols stay comfortable.