Feb 23, 2026

Experienced researchers know something about retatrutide that most beginners overlook entirely. The starting dose is not just a formality. It is not simply the lowest number on a chart you rush through to reach the "real" dose. The starting dose of retatrutide is where your entire protocol succeeds or fails, and getting it wrong creates problems that follow you for months.
Here is the reality. Retatrutide is the first triple-receptor agonist ever developed, activating GLP-1, GIP, and glucagon receptors simultaneously. That triple mechanism makes it the most powerful weight loss peptide in clinical development, with phase 2 trial participants losing up to 24.2% of their body weight at the highest dose. But that same triple mechanism means the body needs time to adjust. Skip the adjustment period, and you are looking at nausea, vomiting, and GI distress that can derail your protocol before it even begins.
This guide covers everything about the retatrutide starting dose. You will find the exact doses used in clinical trials, the titration schedules that produced the best results with the fewest side effects, week-by-week expectations for your first month, and specific strategies for managing the transition period. Whether you are coming from semaglutide or tirzepatide or starting fresh with a GLP-1 agonist for the first time, the information here will help you begin safely and effectively.
The difference between a smooth start and a miserable one often comes down to details that most dosing charts never explain.
What is retatrutide and why does the starting dose matter
Retatrutide (LY3437943) is a 39-amino-acid peptide developed by Eli Lilly that functions as a triple hormone receptor agonist. Unlike semaglutide, which targets only the GLP-1 receptor, or tirzepatide, which targets GLP-1 and GIP receptors, retatrutide activates all three metabolic receptors at once. GLP-1. GIP. And glucagon.
Each receptor does something different.
The GLP-1 receptor activation slows gastric emptying, enhances insulin secretion in response to glucose, and promotes satiety. This is the mechanism most people recognize from medications like Ozempic and Wegovy. The GIP receptor activation facilitates glucose-dependent insulin release and plays a critical role in lipid metabolism, helping reduce fat deposition and improve overall energy balance. Then there is the glucagon receptor, which is unique to retatrutide among the current generation of weight loss peptides. Glucagon receptor activation promotes thermogenesis, increases energy expenditure, and mobilizes fat stores from the liver. This third receptor is what gives retatrutide its edge in weight loss outcomes, driving results that exceed what dual agonists can achieve alone.
But three receptors activating simultaneously means three times the adjustment your body needs to make.
The starting dose exists specifically to give your gastrointestinal system, your metabolic signaling pathways, and your appetite regulation centers time to calibrate. Rush this process, and the body responds with nausea, vomiting, diarrhea, and sometimes all three at once. The phase 2 clinical trial data showed that participants who began at higher starting doses experienced nearly double the rate of GI side effects compared to those who titrated gradually from lower amounts.
That is not a minor difference. That is the difference between staying on protocol and quitting in week two.
The recommended starting dose of retatrutide
The short answer is simple. Most protocols begin at 0.5 mg to 2 mg administered subcutaneously once per week. The longer answer depends on which clinical trial data you reference, your prior experience with GLP-1 agonists, and your individual tolerance profile.
Clinical trial starting doses
The landmark phase 2 trial published in the New England Journal of Medicine randomized 338 participants across multiple dose groups. The study design tells us exactly what the researchers considered safe and effective starting points.
Participants assigned to the 1 mg maintenance group started at 1 mg and stayed there. Simple. But participants assigned to higher maintenance doses of 4 mg, 8 mg, or 12 mg were started at either 2 mg or 4 mg, then escalated every four weeks. The trial specifically compared outcomes between groups that started at 2 mg versus those that started at 4 mg to understand how the starting dose affected tolerability.
The results were clear. Starting at 2 mg produced significantly fewer GI side effects than starting at 4 mg. Both groups eventually reached the same maintenance doses, but the path to get there was dramatically different in terms of comfort and adherence. Participants who began at 2 mg reported milder nausea, less vomiting, and fewer instances of diarrhea during the escalation phase. This finding shaped every subsequent retatrutide dosing schedule recommendation.
More recent protocols and community research have pushed starting doses even lower, with many beginning at 0.5 mg per week. This ultra-conservative approach gives the body even more time to adapt, which is particularly valuable for people who have never used a GLP-1 agonist before. The fundamental guide to peptides provides useful background for those entirely new to the space.
The standard 0.5 mg starting protocol
A 0.5 mg weekly starting dose has become increasingly popular outside of formal clinical trials. The logic is straightforward. If 2 mg produced fewer side effects than 4 mg, then 0.5 mg should produce even fewer side effects than 2 mg. And the anecdotal evidence supports this reasoning.
At 0.5 mg per week, most people report minimal to no GI symptoms. Appetite suppression is mild but noticeable. Energy levels remain stable. The body begins adjusting to triple receptor activation without the shock of a full therapeutic dose. This approach works especially well for people who are sensitive to medications in general, those who have experienced significant nausea on semaglutide or tirzepatide, or anyone who prioritizes comfort during the initial adaptation period.
The trade-off is pace. Starting at 0.5 mg means it takes longer to reach therapeutic doses where significant weight loss occurs. But the argument is that a slower start with better adherence ultimately produces better outcomes than a faster start that triggers side effects severe enough to cause missed doses or protocol abandonment.
Alternative 1 mg and 2 mg starting points
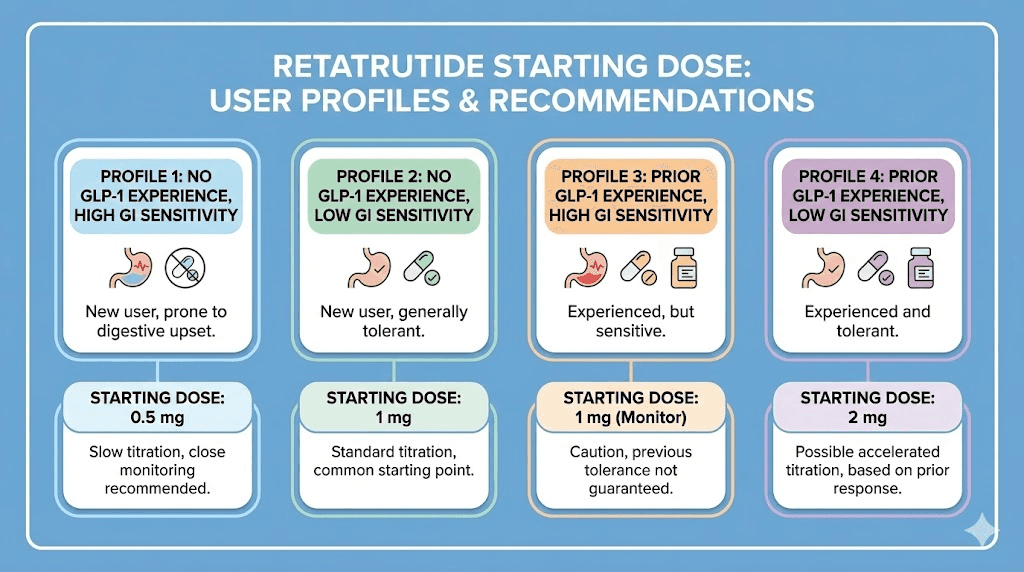
For people with prior GLP-1 agonist experience, starting at 1 mg or 2 mg is reasonable and well-supported by clinical data. If you have already spent months on semaglutide or tirzepatide, your body has already adapted to GLP-1 receptor activation and potentially GIP receptor activation as well. The only truly new element with retatrutide is the glucagon receptor component.
This prior adaptation means you can tolerate a higher starting dose without the full spectrum of GI side effects that a GLP-1 naive person would experience. The 2 mg starting point from the phase 2 trial was specifically designed for this scenario, since the trial participants included people with varying levels of prior medication exposure.
A practical framework looks like this. Never used a GLP-1 agonist before? Start at 0.5 mg and review the getting started with peptides guide for fundamentals. Coming from low-dose semaglutide or tirzepatide? Start at 1 mg. Coming from moderate to high-dose compounded semaglutide or tirzepatide? Start at 2 mg. Coming from high-dose tirzepatide specifically? You may tolerate 2 mg comfortably since your body already handles dual receptor activation.
Regardless of starting point, the principle remains the same. Give the body time to adjust before pushing higher.
Why starting low prevents problems
The urge to skip ahead is understandable. You have read about 24% body weight reduction. You want results. The starting dose feels like wasted time. But the clinical evidence is overwhelming. Starting low is not conservative. It is strategic.
GI side effects and dose relationship
Gastrointestinal symptoms are the most common adverse events reported with retatrutide, and they follow a clear dose-dependent pattern. In the phase 2 trial, nausea was reported by 16.2% of participants in the lowest dose groups but climbed to over 45% in higher dose groups without proper titration. Vomiting showed a similar pattern. Diarrhea was reported across all dose groups but was significantly more frequent and more severe at higher doses.
The mechanism behind this is straightforward. GLP-1 receptor activation slows gastric emptying. When you suddenly activate GLP-1 receptors at a high level, the stomach slows dramatically. Food sits longer than the body expects. The result is nausea, bloating, and sometimes vomiting. Add GIP and glucagon receptor activation on top of that, and you have three separate pathways all affecting digestion simultaneously.
Starting low allows each receptor system to calibrate gradually. The stomach adjusts to slower emptying. The intestines adapt to changed motility patterns. The liver calibrates to glucagon-driven metabolic changes. This adaptation does not happen overnight. It takes weeks, which is exactly why the clinical protocols build in four-week intervals between dose increases. Understanding how peptides interact with the body at the receptor level makes this process less frustrating and more logical.
The phase 2 trial evidence
The New England Journal of Medicine study provides the most rigorous data available on retatrutide starting doses. Here is what the numbers actually show.
Participants randomized to the 4 mg dose with a 2 mg starting dose had significantly fewer GI adverse events than those started directly at 4 mg. The same pattern held for the 8 mg groups. Those started at 2 mg and escalated to 8 mg tolerated the journey better than those started at 4 mg and escalated to 8 mg. The GI symptom rates nearly doubled when participants skipped the lower starting dose.
At 48 weeks, the weight loss results were striking across all dose groups. The 1 mg group lost 8.7% of body weight. The 4 mg group lost 17.1%. The 8 mg group lost 22.8%. And the 12 mg group, which started at 2 mg and titrated up every four weeks, lost 24.2% of body weight. Compare that to 2.1% in the placebo group. The retatrutide versus semaglutide comparison becomes even more dramatic when you consider these results came from a 48-week trial, not the 68-week trials used for semaglutide data. Even the mazdutide comparison and survodutide data show that retatrutide occupies a class of its own in weight loss efficacy.
But here is the critical detail. The participants who achieved those impressive results did so because they stayed on protocol. And they stayed on protocol because the gradual starting dose made the journey tolerable. The best weight loss medication in the world does nothing if side effects cause you to quit.
How the body adapts to triple receptor activation
Understanding what happens biologically during those first weeks at the starting dose helps explain why patience matters.
During week one at a low starting dose, GLP-1 receptors begin responding to the new agonist. Gastric emptying slows slightly. Appetite may decrease modestly. Insulin signaling begins to shift. Most people notice subtle changes but nothing dramatic.
By weeks two and three, GIP receptor effects become more pronounced. Lipid metabolism begins shifting. Fat storage patterns start changing. The body enters a new metabolic state where energy balance is being recalibrated. Some people notice energy fluctuations during this period as the body adjusts to using different fuel sources more efficiently.
The glucagon receptor effects layer in over weeks three and four. Hepatic glucose output adjusts. Thermogenesis increases slightly. Fat mobilization from visceral stores accelerates. This is the receptor that makes retatrutide unique, and it is also the one that requires the most adaptation time. The timeline for retatrutide to kick in reflects this layered activation process.
By week four, all three receptor systems are working together. The body has established a new baseline. Increasing the dose from this adapted state is far more comfortable than hitting the body with full triple activation on day one.
Complete starting dose titration schedule
Titration means gradually increasing the dose over time. Every effective retatrutide protocol includes a titration schedule, and the starting dose is simply the first step on that ladder. The question is how fast you climb.
Conservative titration protocol
This approach prioritizes comfort and minimal side effects above all else. It takes longer to reach therapeutic doses but produces the smoothest experience.
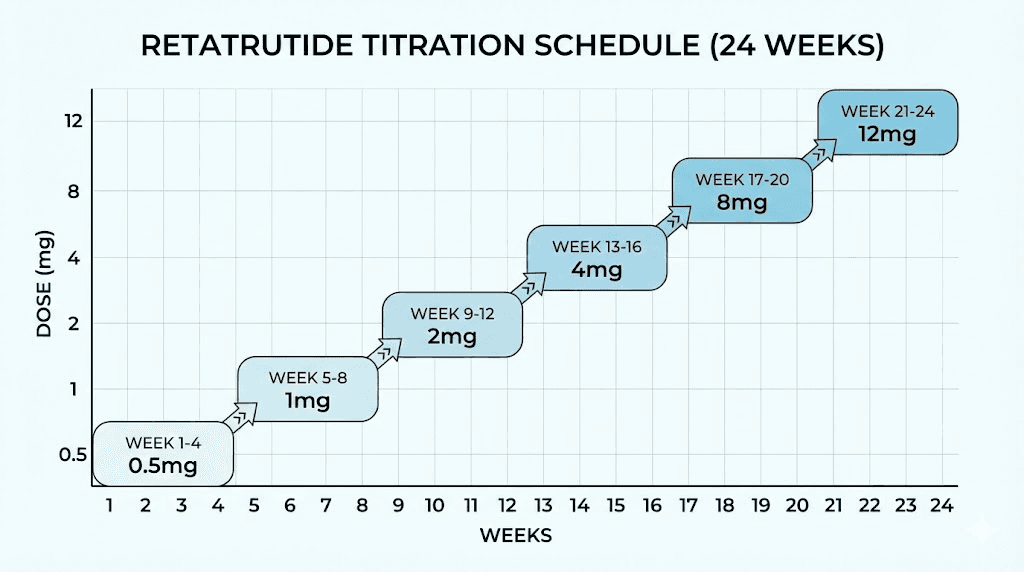
Weeks 1 through 4: 0.5 mg once weekly
Weeks 5 through 8: 1 mg once weekly
Weeks 9 through 12: 2 mg once weekly
Weeks 13 through 16: 4 mg once weekly
Weeks 17 through 20: 6 mg once weekly
Weeks 21 through 24: 8 mg once weekly
Weeks 25 and beyond: 10 to 12 mg once weekly (if needed and tolerated)
This protocol reaches the 8 mg therapeutic range in approximately 20 weeks. That feels slow. But the drop-out rate on conservative titration schedules is dramatically lower than on aggressive ones. You can use the retatrutide dosage calculator to plan your specific schedule based on your vial concentration and desired weekly dose.
Standard titration protocol
This is closest to what the phase 2 clinical trial used. It balances pace with tolerability.
Weeks 1 through 4: 2 mg once weekly
Weeks 5 through 8: 4 mg once weekly
Weeks 9 through 12: 8 mg once weekly
Weeks 13 and beyond: 8 to 12 mg once weekly (based on response and tolerance)
This protocol reaches the therapeutic range in approximately 8 weeks. Most clinical outcomes were measured on this type of schedule. If you have prior experience with tirzepatide dosing or semaglutide and tolerated those well, this standard approach is reasonable. The full dose chart breaks this down into more detail.
Aggressive titration protocol (not recommended)
Some people attempt to reach high doses quickly by starting at 4 mg or skipping dose levels entirely. The data does not support this approach. In the phase 2 trial, participants started at 4 mg without escalation experienced significantly more adverse events than those who began at 2 mg. The time saved by skipping starting dose levels is typically lost to days spent managing severe nausea, missed doses from feeling too sick to inject, and sometimes complete protocol abandonment.
There is no clinical scenario where starting at 4 mg or higher is recommended for someone new to retatrutide. Even if you have extensive experience with other peptides for fat loss or the best weight loss peptides on the market, the glucagon receptor component is entirely new to your system and requires adaptation time. The peptide safety principles that apply to all research peptides are especially relevant when working with a first-in-class triple agonist.
What to expect during your first four weeks
Knowing what is normal during the initial weeks prevents unnecessary worry and helps you distinguish between expected adaptation effects and genuine warning signs that require attention.
Week 1 at the starting dose
The first injection often produces the most anxiety and the least actual effect. At 0.5 to 2 mg, the dose is low enough that many people report feeling almost nothing for the first few days. This is normal and does not mean the peptide is not working.
Common week one experiences include mild appetite reduction that comes and goes, slight changes in how food tastes or appeals, occasional mild nausea, particularly after larger meals, and a subtle sense of fullness that arrives earlier during meals than usual. Some people feel nothing at all during week one. That is also completely normal.
The amount of retatrutide you should take during this first week should remain at your chosen starting dose regardless of whether you feel effects. The body is calibrating. Receptor sensitivity is adjusting. The absence of dramatic effects does not indicate a need for a higher dose.
Retatrutide has a half-life of approximately six days. This means the peptide concentration builds steadily with each weekly injection. By the end of week one, you have not yet reached steady-state levels. True effects become more apparent once steady state is achieved, typically after three to four weekly injections at the same dose. This gradual onset is similar to the timeline for other GLP-1 agonists to start working, though the triple receptor activation adds additional complexity to the process.
Weeks 2 through 4 adaptation period
This is where the adaptation happens. Each weekly injection adds to the circulating retatrutide level, and by week two or three, most people notice more consistent appetite suppression. Meals become smaller naturally. Cravings for high-calorie foods may diminish. Some people report that their relationship with food begins shifting, where eating becomes more about fuel and less about emotional satisfaction.
GI effects, if they appear, typically show up during this period. Mild nausea after eating is the most common complaint. It tends to occur after meals that are too large or too fatty, because the slowed gastric emptying cannot handle the same volume it processed before. Adjusting meal size and composition resolves this for most people. The foods to avoid on GLP-1 agonists apply equally to retatrutide.
Energy levels may fluctuate. Some people feel slightly fatigued as the body adjusts to new metabolic signaling. Others report stable or even increased energy as the glucagon receptor activation boosts thermogenesis. The GLP-1 fatigue phenomenon is well documented and typically resolves within two to four weeks. If fatigue persists, it may indicate a need to increase protein intake or adjust meal timing.
Weight changes during the first month at a starting dose are variable. Some people lose 2 to 4 pounds from reduced appetite alone. Others see minimal scale movement but notice changes in bloating, water retention, or how their clothes fit. Do not use the first month to judge whether retatrutide works. The weight loss timeline patterns observed with tirzepatide apply in principle to retatrutide as well, with significant results coming at higher therapeutic doses after proper titration. The before and after results people share online typically reflect months of use at therapeutic doses, not the starting dose period.
Signs that the starting dose is working
Because the starting dose is intentionally low, the signs of it working are subtle. Look for reduced interest in snacking between meals, feeling satisfied with smaller portions, less mental preoccupation with food, earlier satiety signals during meals, and reduced cravings for sugary or highly processed foods.
You may also notice improved blood sugar stability if you monitor glucose levels. The GLP-1 and GIP receptor activation at even low doses can smooth out postprandial glucose spikes. Some people report better sleep quality, though this is less consistently documented. If you are coming from another medication and wondering about the transition, the semaglutide withdrawal symptom guide and switching medication guide address what happens when transitioning between different GLP-1 agonists.
The key point is that the starting dose is doing its job even when the effects feel minor. It is priming your receptor systems, establishing tolerance, and laying the foundation for higher doses to work effectively without overwhelming your body. Understanding the typical timeline for peptides to work helps calibrate expectations across all peptide protocols, not just retatrutide.
Managing side effects at the starting dose
Even at the lowest starting doses, some people experience side effects. Knowing how to manage them makes the difference between a temporary inconvenience and a protocol-ending problem.
Nausea and appetite changes
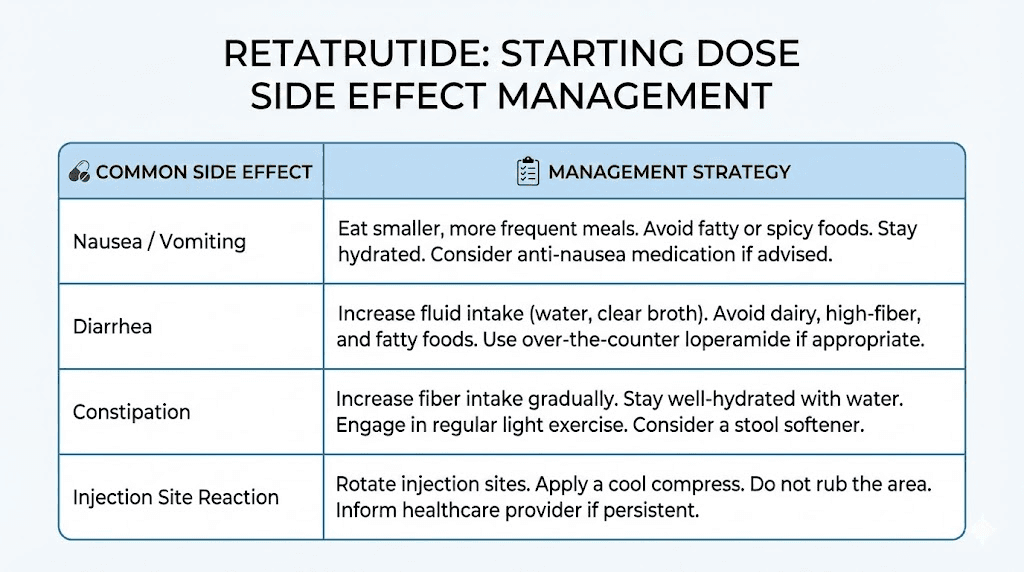
Nausea is the single most reported side effect across all GLP-1 agonist peptides, and retatrutide is no exception. At the starting dose, nausea is typically mild and often connected to specific triggers rather than being constant. The most common triggers are eating too much at one sitting, eating high-fat or greasy foods, eating too quickly, and lying down shortly after a meal.
Management strategies that work include eating five to six smaller meals throughout the day instead of three large ones, choosing lean proteins, vegetables, and complex carbohydrates over fatty or fried options, eating slowly and stopping at the first sign of fullness, staying upright for at least 30 minutes after eating, and sipping ginger tea or peppermint tea if nausea occurs. The recommended foods for GLP-1 users provide an excellent framework for meal planning during the starting dose period and beyond.
If nausea is persistent and does not respond to dietary adjustments, it may indicate that even the starting dose is too high for your current tolerance. Reducing from 1 mg to 0.5 mg, or from 2 mg to 1 mg, is a perfectly valid approach. There is no failure in adjusting. There is only failure in pushing through severe symptoms until you quit entirely. The burping and nausea patterns common with GLP-1 agonists often respond well to dose reduction and slower titration.
Digestive adjustments
Beyond nausea, the starting dose can cause constipation, diarrhea, or alternating between the two. Slowed gastric emptying changes the transit time through the entire digestive tract, and different people respond differently to that change.
Constipation is common because slower transit means more water absorption from the stool. Staying well hydrated, consuming adequate fiber, and maintaining physical activity all help. The constipation management strategies used for semaglutide apply directly to retatrutide as well.
Diarrhea occurs less frequently at starting doses but can happen, particularly in people sensitive to GI changes. If diarrhea occurs, ensure adequate hydration and electrolyte replacement. Oral rehydration solutions can help maintain balance during episodes. The issue typically resolves within one to two weeks as the body adapts.
Bloating and increased gas are also reported during the first few weeks. These symptoms relate to changes in gut motility and bacterial fermentation patterns. Reducing carbonated beverages, avoiding foods known to produce gas, and taking short walks after meals can all help. For persistent digestive issues, the GI timeline guides provide realistic expectations for how long these adjustments typically take. The peptides and gut health relationship is complex, and some people find that adding supportive gut health peptides alongside retatrutide eases the transition.
Fatigue and energy changes
Some people feel tired during the first week or two on retatrutide. This is partly metabolic, as the body adjusts to new hormonal signaling, and partly caloric, as reduced food intake means less available energy. The relationship between GLP-1 agonists and energy is complex.
Ensuring adequate protein intake is critical. Most experts recommend 0.7 to 1.0 grams of protein per pound of body weight when using GLP-1 agonists to prevent muscle loss and maintain energy. Protein shakes designed for GLP-1 users can help meet these targets when appetite is suppressed.
Fatigue that persists beyond three to four weeks at the starting dose warrants investigation. It could indicate inadequate caloric intake, nutritional deficiencies, dehydration, or rarely, an underlying condition unmasked by the metabolic changes. Track your daily caloric and protein intake during the starting dose period to identify gaps early. The semaglutide fatigue guide covers troubleshooting approaches that apply to all GLP-1 class peptides including retatrutide. Understanding whether fatigue is a direct peptide effect or a caloric deficit symptom changes the management approach entirely.
Injection site management
Retatrutide is administered subcutaneously, typically in the abdomen, thigh, or upper arm. At the starting dose, injection volume is small, which minimizes injection site reactions. However, some people develop mild redness, itching, or a small bump at the injection site.
Rotating injection sites is essential. Use a different location each week, maintaining at least one inch of separation between injection spots. The abdomen generally provides the most comfortable injection experience because of the subcutaneous fat layer available. Our guide on where to inject retatrutide covers optimal sites and rotation patterns in detail.
Allow the solution to reach room temperature before injecting. Cold injections sting more and can cause more localized irritation. Fifteen to twenty minutes out of the refrigerator is sufficient. Do not microwave or heat the vial. Do not use a syringe or needle more than once. The peptide injection guide covers proper injection technique step by step.
Retatrutide starting dose compared to semaglutide and tirzepatide
If you have used semaglutide or tirzepatide, understanding how their starting doses compare to retatrutide helps set expectations and informs your approach.
Semaglutide typically starts at 0.25 mg per week for the first four weeks, then increases to 0.5 mg. This is a GLP-1-only starting dose, meaning one receptor system activates. The transition is relatively gentle because only gastric emptying and appetite regulation are changing. Most people tolerate the semaglutide starting dose with minimal issues. The semaglutide appetite suppression timeline typically shows effects within the first one to two weeks. You can review the semaglutide dosage chart for the complete titration schedule and compare it to retatrutide progression.
Tirzepatide starts at 2.5 mg per week for four weeks before increasing to 5 mg. As a dual GLP-1/GIP agonist, two receptor systems activate simultaneously. The starting dose is deliberately conservative to allow for this dual adaptation. Side effects at the tirzepatide starting dose are generally manageable but more noticeable than semaglutide because of the additional GIP receptor activation. The compounded tirzepatide starting dose guide provides additional context for research peptide users.
Retatrutide adds the glucagon receptor on top of GLP-1 and GIP. Three systems adjusting simultaneously requires more adaptation time. This is why conservative starting doses of 0.5 to 2 mg are recommended, compared to the relatively higher starting point of 2.5 mg for tirzepatide. The absolute milligram numbers are less important than the receptor load each dose represents.
Here is a comparison of the starting approaches.
Peptide | Starting dose | Receptors activated | Weeks at starting dose | Max studied dose | Max weight loss |
|---|---|---|---|---|---|
Semaglutide | 0.25 mg | GLP-1 only | 4 weeks | 2.4 mg (7.2 mg in STEP-UP) | ~17-20% |
Tirzepatide | 2.5 mg | GLP-1 + GIP | 4 weeks | 15 mg | ~22% |
Retatrutide | 0.5-2 mg | GLP-1 + GIP + Glucagon | 4 weeks | 12 mg | ~24-28% |
The table tells an important story. Each generation of weight loss peptide activates more receptors, starts at a dose calibrated for that receptor load, and achieves greater weight loss at the therapeutic range. But each also requires more careful starting dose management. More power means more responsibility during the onboarding phase.
If you are switching from semaglutide to retatrutide, the full comparison between the two peptides helps you understand what changes to expect. If you are coming from tirzepatide, our guide on retatrutide dosing after tirzepatide addresses the specific considerations for that transition.
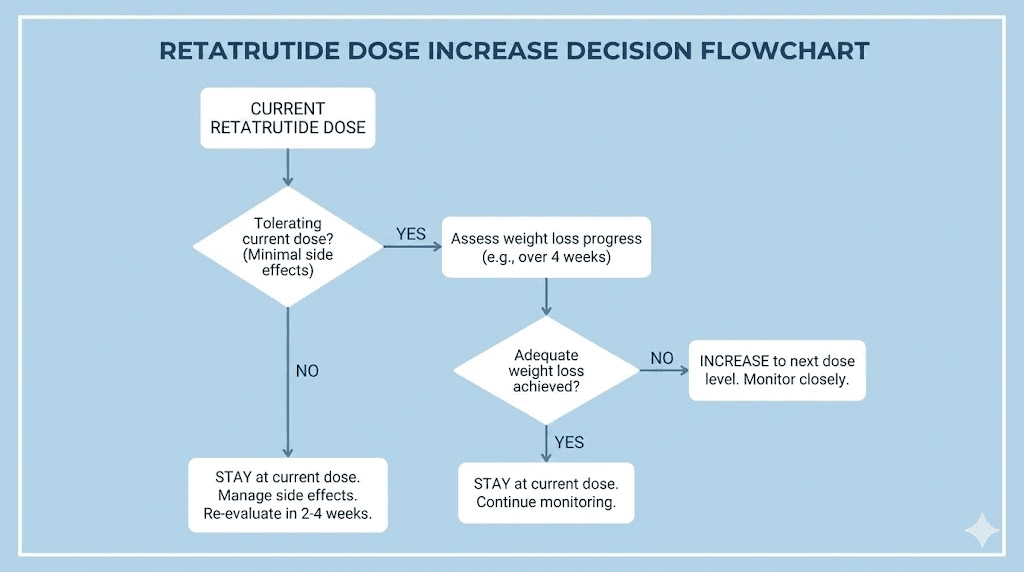
When to increase from the starting dose
The starting dose is temporary. It is the foundation, not the destination. But knowing when to step up requires paying attention to specific signals from your body.
Signs that you are ready to increase
After four weeks at your starting dose, evaluate these indicators. You have tolerated the current dose with minimal or no GI side effects for at least two consecutive weeks. Your appetite suppression has stabilized and you are no longer seeing progressive changes at the current level. Weight loss has slowed or plateaued at the current dose. You feel physically and mentally ready for the next step.
All four indicators should be present before increasing. Missing even one suggests waiting another one to two weeks. The guide to determining your retatrutide dose provides additional decision frameworks for dose adjustments throughout your entire protocol.
When to stay at the starting dose longer
There are valid reasons to remain at the starting dose beyond the standard four weeks.
If you are still experiencing nausea, bloating, or digestive issues at week four, do not increase. Your body is telling you it needs more time. Increasing the dose while side effects are active will amplify those effects, not resolve them. Stay at the current dose until GI symptoms have resolved for at least two full weeks.
If you are losing weight consistently at the starting dose, there is no urgent reason to increase. Some people with high baseline body weight or metabolic sensitivity see meaningful results even at low doses. Riding a low effective dose as long as it works preserves room for future increases when you need them.
If you are managing other health conditions or medications, a slower titration gives you and your healthcare provider more time to monitor interactions and adjust other treatments as needed. The starting dose period is an excellent time to establish baseline measurements for blood glucose, liver function, and lipid panels. Some people use the starting dose period to also address related concerns like GLP-1 related hair loss prevention by optimizing nutrition and supplementation before higher doses begin.
How much to increase by
Standard increases follow the dose doubling pattern used in clinical trials. From 0.5 mg, increase to 1 mg. From 1 mg, increase to 2 mg. From 2 mg, increase to 4 mg. From 4 mg, increase to 6 or 8 mg. From 8 mg, increase to 10 or 12 mg.
Each increase should be followed by another four-week stabilization period before the next adjustment. The retatrutide peptide dosage chart maps out these progression steps, and the dosage calculator helps you determine exact injection volumes for each dose level based on your vial concentration.
Some people find that half-step increases work better for their tolerance. Instead of jumping from 2 mg to 4 mg, they go from 2 mg to 3 mg for two weeks, then to 4 mg. This micro-titration approach is not reflected in clinical trial protocols but has gained popularity among research peptide users who have the flexibility to adjust their doses more precisely.
Injection timing and the starting dose
When you inject matters almost as much as how much you inject, especially during the starting dose period when your body is still calibrating to triple receptor activation.
Most people inject retatrutide once per week on the same day. Consistency is critical. The six-day half-life means drug levels rise and fall on a predictable cycle. Injecting at the same time each week keeps those levels as stable as possible, which reduces the likelihood of breakthrough side effects from concentration peaks and valleys.
Morning versus evening injection is a matter of personal preference. Some researchers prefer morning injections because appetite suppression kicks in during the day when eating decisions are made. Others prefer evening injections so that any initial nausea passes during sleep. During the starting dose period specifically, evening injection has a practical advantage. If the body reacts to the new peptide with nausea or fatigue, sleeping through the initial response means less disruption to daily activities.
The best injection timing research for GLP-1 agonists generally applies to retatrutide as well. There is no pharmacological difference in absorption based on time of day. Choose the time that works best for your schedule and stick with it.
For injection technique specifically, subcutaneous injection into the abdomen, thigh, or upper arm is standard. The GLP-1 injection technique guide covers the step-by-step process including proper angle, pinch technique, and post-injection care. Using a peptide injection pen can simplify the process for those who find syringe handling difficult.
Nutrition strategy during the starting dose
What you eat during the starting dose period shapes your entire retatrutide experience. The right nutritional approach can virtually eliminate GI side effects while supporting body composition improvements even at low doses.
Protein first. Every meal should lead with protein. Aim for 25 to 40 grams per meal, targeting 0.7 to 1.0 grams per pound of goal body weight daily. This is non-negotiable. Weight loss peptides work best when muscle is preserved, and adequate protein is the primary defense against muscle catabolism during caloric reduction. Protein shakes formulated for GLP-1 users make hitting these targets realistic when appetite is suppressed.
Hydration is everything. Dehydration amplifies every GI side effect. Nausea worsens. Constipation becomes more likely. Fatigue increases. Drink at least 64 ounces of water daily, more if you exercise. Adding electrolytes, especially sodium, potassium, and magnesium, prevents the electrolyte imbalances that sometimes accompany reduced food intake. Supplement protocols for GLP-1 users include specific electrolyte recommendations.
Meal structure matters. Five to six smaller meals spread throughout the day work significantly better than three large meals during the starting dose period. Slowed gastric emptying means the stomach processes food more slowly. Overfilling the stomach triggers nausea. Small, frequent meals keep the stomach from overloading while maintaining adequate caloric and nutritional intake.
The GLP-1 agonist diet plan and foods to avoid list provide detailed meal frameworks that transfer directly to retatrutide use. Foods that commonly trigger nausea include greasy or fried items, very sweet foods, large portions of red meat, carbonated beverages, and anything eaten too quickly.
Exercise at the starting dose
Physical activity during the starting dose period requires thoughtful adjustment. The body is adapting to significant metabolic changes, and exercise adds another variable to manage.
Light to moderate exercise is generally safe and beneficial from day one. Walking, gentle cycling, yoga, and light resistance training support metabolic function without overtaxing a body in transition. The peptides and athletic performance relationship is well documented, and maintaining activity during the starting period supports better outcomes long term.
High-intensity exercise should be approached with caution during the first two to four weeks. Reduced caloric intake combined with new metabolic signaling can affect energy availability, recovery capacity, and blood sugar stability during intense workouts. Monitor how you feel carefully. If lightheadedness, excessive fatigue, or nausea occurs during exercise, reduce intensity and ensure adequate pre-workout nutrition.
Muscle preservation strategies become relevant even at the starting dose. Resistance training two to three times per week, combined with adequate protein intake, sends muscle-building signals that counteract the catabolic effects of caloric restriction. This is not about building new muscle during the starting phase. It is about preserving what you have while the body shifts to burning fat for fuel.
SeekPeptides members access detailed exercise protocols designed specifically for people using GLP-1 agonists, including workout templates calibrated for each phase of the titration process from starting dose through maintenance.
Common starting dose mistakes
Years of community experience with GLP-1 agonists have revealed patterns of mistakes that repeat across different peptides. Retatrutide is no exception. Avoiding these errors can save you weeks of discomfort and frustration.
Mistake 1: Starting too high because of prior GLP-1 experience. Having tolerated 15 mg of tirzepatide does not mean you can start retatrutide at 4 mg. The glucagon receptor component is entirely new to your system. Even experienced GLP-1 users need to start retatrutide at 1 to 2 mg maximum and titrate from there.
Mistake 2: Increasing the dose because the starting dose is not working. The starting dose is not supposed to produce dramatic weight loss. It is an adaptation period. Judging the starting dose by the scale after one or two weeks leads to premature dose increases and unnecessary side effects. Give the full four weeks before evaluating effectiveness.
Mistake 3: Ignoring mild side effects and increasing anyway. Mild nausea at 1 mg becomes moderate nausea at 2 mg and potentially severe nausea at 4 mg. Side effects generally scale with dose increases. If you are already experiencing symptoms at the starting dose, increasing will make them worse. Wait for complete resolution before moving up.
Mistake 4: Not adjusting diet during the starting dose period. Eating the same volume and types of food you ate before starting retatrutide is a recipe for nausea. The diet plan principles for GLP-1 agonists should be implemented from day one, not after problems arise. Smaller meals, lean proteins, adequate hydration, and reduced fat intake make the starting dose period significantly more comfortable.
Mistake 5: Comparing timelines with other people. Individual responses to the starting dose vary enormously. Some people feel strong effects at 0.5 mg. Others feel almost nothing at 2 mg. Genetic variation in receptor density, body composition, metabolic rate, and prior medication history all influence the starting dose experience. Your protocol is yours. Comparing it to someone else is misleading and often leads to inappropriate dose adjustments.
Mistake 6: Inconsistent injection timing. Retatrutide has a half-life of approximately six days. Injecting at the same time each week maintains stable blood levels and smooth receptor activation. Varying your injection day by two or three days creates peaks and valleys in drug concentration that can trigger intermittent side effects and reduce effectiveness during the starting phase. Our best time to inject GLP-1 guide discusses timing strategies in depth.
Mistake 7: Not tracking anything during the starting period. The starting dose period is your baseline. Weight, measurements, appetite levels, side effects, energy, sleep quality, and food intake should all be tracked from day one. This data becomes invaluable when making dose adjustment decisions later. Without it, you are guessing. And guessing with a triple-receptor agonist is a poor strategy. Tools like the GLP-1 plotter can help visualize your progress from the very first week.
Mistake 8: Using the wrong syringe or measuring incorrectly. At starting doses of 0.5 to 2 mg, the injection volumes are small. Using a 3 mL syringe instead of an insulin syringe makes precise measurement nearly impossible. A 1 mL insulin syringe with 100-unit markings provides the precision needed for accurate starting doses. The peptide dosage calculation guide walks through the math of converting milligrams to units based on your vial concentration.
Mistake 9: Not having a plan beyond the starting dose. Starting retatrutide without a full titration plan leads to arbitrary dose changes and inconsistent results. Before your first injection, map out your complete schedule from starting dose through target maintenance dose. The full dosage chart and dosage calculator make this planning straightforward.
Reconstitution and preparation for your starting dose
Before you can inject your first starting dose, you need to properly prepare the peptide. Retatrutide typically comes as a lyophilized (freeze-dried) powder that must be reconstituted with bacteriostatic water before use.
The reconstitution process is straightforward but requires attention to detail. Draw the appropriate amount of bacteriostatic water into a sterile syringe. Insert the needle into the retatrutide vial and angle it so the tip touches the glass wall. Inject the water slowly, letting it run down the side of the vial rather than blasting it directly onto the powder cake. This gentle approach preserves peptide integrity.
Never shake the vial. Gently swirl it in a circular motion to help the powder dissolve. The solution should become clear with no visible particles within one to five minutes. If cloudiness persists after five minutes of gentle swirling, wait and try again. Do not use the solution if particles remain visible.
The amount of bacteriostatic water you add determines the concentration of your solution, which in turn determines how many units you draw for each dose. Our guide for mixing 10 mg retatrutide vials provides exact water amounts and corresponding unit measurements for each starting dose level. The retatrutide reconstitution chart covers additional vial sizes and concentrations.
For general reconstitution principles that apply across all peptides, the complete peptide reconstitution guide walks through the process in detail, and the peptide reconstitution calculator handles the math automatically.
Once reconstituted, store the vial in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Do not freeze reconstituted retatrutide. Freezing damages the peptide structure and reduces potency. Most conservative guidelines recommend using reconstituted retatrutide within 28 days, though some sources cite stability up to 60 days under proper refrigeration. The peptide storage guide covers best practices for maintaining potency throughout the use period.
When drawing your starting dose, use an insulin syringe for precision. The small volumes involved at starting doses (often 5 to 10 units depending on concentration) require the accuracy that insulin syringes provide. Draw slowly, tap out air bubbles, and confirm the exact number of units before injecting. Every unit matters at the starting dose because even small measurement errors represent a larger percentage of the total dose when the dose itself is small.
Starting dose considerations for specific populations
Not everyone approaches the starting dose from the same position. Specific situations call for modified approaches.
People new to GLP-1 agonists
If retatrutide is your first exposure to any GLP-1 receptor agonist, start at the lowest practical dose. A 0.5 mg weekly starting dose gives your body the gentlest possible introduction to receptor activation. You are not just adapting to GLP-1 signaling but to GIP and glucagon signaling simultaneously, with no prior adaptation to any of the three.
Expect the first two weeks to be an observation period. You may feel subtle effects or nothing at all. Both are normal. By weeks three and four, most GLP-1 naive users begin noticing appetite changes. This is the timeline to watch. If four weeks pass with zero perceptible effect, consider a small increase to 1 mg rather than jumping to 2 mg.
Our getting started with peptides guide provides broader context for first-time peptide users, covering everything from sourcing to injection technique to setting realistic expectations.
People switching from other GLP-1 agonists
Switching from semaglutide or tirzepatide to retatrutide is increasingly common as people seek greater weight loss results. The approach depends on what you are switching from and at what dose.
From semaglutide at any dose, your GLP-1 receptors are pre-adapted. Starting retatrutide at 1 to 2 mg is reasonable. From tirzepatide, both your GLP-1 and GIP receptors are adapted, so 2 mg is a comfortable starting point for most people. The timing of the switch matters too. If you stop tirzepatide and wait two weeks (roughly four half-lives) before starting retatrutide, the previous medication will have largely cleared, and you are starting closer to baseline.
Some people prefer an overlap approach, where they start retatrutide at a low dose while tapering off their previous medication. This requires careful management and is beyond the scope of standard starting dose guidance. The retatrutide onset timeline after tirzepatide provides specific guidance for this transition.
People with higher body weight
Body weight influences drug distribution and can affect the perceived strength of a starting dose. A person weighing 300 pounds experiences a 1 mg dose differently than a person weighing 180 pounds, simply because the same amount of drug distributes across more tissue.
However, the clinical trial data does not support weight-based starting dose adjustments for retatrutide. The phase 2 trial used the same starting doses across all participants regardless of body weight, and the GI side effect profile was similar across weight categories. The starting dose is about receptor adaptation, not about achieving a specific blood concentration per kilogram of body weight.
That said, people with higher body weight may notice less appetite suppression at the starting dose, which is expected. The therapeutic effect scales with dose, and higher body weight generally requires higher maintenance doses. The starting dose still serves its adaptation purpose regardless of body weight. Use the peptide calculator to plan your full dose progression.
People with GI sensitivity
If you have a history of GI issues, whether from previous GLP-1 agonist use, conditions like IBS or GERD, or general digestive sensitivity, starting at the absolute lowest dose is critical. Begin at 0.5 mg and plan for extended stays at each dose level. Instead of four weeks between increases, consider six to eight weeks.
Pre-emptive dietary changes help enormously. Shift to smaller, more frequent meals before your first injection. Reduce fatty and fried food intake. Increase water consumption. These changes create a baseline of reduced GI stress that makes the addition of retatrutide more tolerable.
Some people with known GI sensitivity also benefit from starting their first injection in the evening. This allows any initial nausea to occur during sleep rather than during active hours. Others prefer morning injections so they can manage any symptoms while awake and responsive. There is no clinically proven best time. The best time to take a GLP-1 shot depends on individual preference and lifestyle, and the same applies to retatrutide.
The science behind starting low and titrating slow
Understanding the pharmacological rationale for gradual dosing helps build patience during what can feel like an unnecessarily slow process.
Retatrutide is a 39-amino-acid peptide coupled to a fatty diacid moiety. This acylation is what gives it its extended half-life of approximately six days, allowing for once-weekly dosing. But this also means the drug accumulates in the body over multiple doses before reaching steady state.
Steady state, the point where drug levels plateau because the amount entering the body equals the amount being cleared, takes approximately four to five half-lives to achieve. For retatrutide, that is 24 to 30 days at a given dose. This is precisely why four-week intervals between dose increases make pharmacological sense. It takes roughly four weeks for each new dose level to fully manifest its effects.
During those four weeks, receptor desensitization and adaptation occur. GLP-1 receptors that initially respond strongly to the agonist gradually calibrate their sensitivity. The result is that GI effects that were prominent in week one diminish by week four, even though drug levels are actually higher by week four than week one. The receptors have adapted to the new baseline.
This adaptation is specific to each receptor type. GLP-1 adaptation happens relatively quickly, usually within two to three weeks. GIP receptor adaptation follows a similar timeline. Glucagon receptor adaptation may take slightly longer because fewer tissues in the body have adapted to exogenous glucagon agonism previously.
When you increase the dose, you are essentially resetting the adaptation clock.
The higher drug level stimulates receptors above their adapted baseline, causing a temporary return of effects like nausea. But because the receptors have already partially adapted, the effects are milder than they would have been if you had started at the higher dose from the beginning.
This is the entire logic of titration distilled into one sentence: each dose level builds tolerance that makes the next level more tolerable.
The guide to how peptides work covers these receptor dynamics in broader context, explaining how the body interacts with exogenous peptides across different therapeutic applications. For understanding the specific triple mechanism of retatrutide, the complete retatrutide dose guide provides additional pharmacological detail. The concept of peptide dosing principles applies across all injectable peptides, and understanding them helps you appreciate why the starting dose approach exists in the first place.
Tracking progress from the starting dose
What you track during the starting dose period forms the foundation for every dose adjustment decision you will make for the duration of your protocol.
Weight: Weigh yourself daily at the same time (ideally morning, after using the bathroom, before eating). Daily weight fluctuates by 1 to 3 pounds from water, sodium, and digestive contents. Track the weekly average, not individual daily readings. A trending weekly average is the most reliable indicator of actual fat loss. The one-month results patterns seen with semaglutide provide a useful comparison for what to expect with retatrutide, though the triple mechanism typically accelerates results once therapeutic doses are reached.
Measurements: Take waist, hip, chest, and limb circumference measurements every two weeks. Body composition can shift without dramatic scale changes, especially during the starting dose period when water retention patterns are adjusting.
Appetite: Rate your hunger and satiety on a 1 to 10 scale before and after meals. This subjective tracking reveals patterns that pure numbers miss. Many people notice appetite suppression strengthening gradually over weeks, confirming that the starting dose is engaging receptors even when the scale is not moving dramatically.
Side effects: Log any GI symptoms, injection site reactions, energy changes, mood shifts, or sleep alterations. Include severity (mild, moderate, severe), duration, and any triggers you can identify. This log becomes critical when deciding whether to increase, maintain, or decrease your dose.
Food intake: Track total calories and protein grams daily. Reduced appetite at the starting dose means you may be eating significantly less without realizing it. Falling below 1200 calories or dropping protein below 0.6 grams per pound of body weight can trigger muscle loss, fatigue, and metabolic slowdown. Awareness prevents these issues.
The GLP-1 plotter is a useful tracking tool for visualizing your dose progression and weight trend over time. Combining that with the peptide cost calculator helps you plan the financial aspects of your protocol alongside the dosing aspects.
Starting dose and long-term protocol planning
The starting dose is the first chapter, not the whole story. Planning your full protocol from the beginning helps you maintain perspective during the slow early weeks.
A typical retatrutide protocol runs 24 to 48 weeks, with some people continuing indefinitely. The starting dose period occupies the first 4 to 8 weeks. The titration phase takes another 8 to 16 weeks. And the maintenance phase, where you settle at your optimal dose, covers the remaining weeks.
Knowing this timeline helps contextualize the starting dose. If your total protocol is 48 weeks, the four weeks you spend at the starting dose represent less than 10% of the total journey. It is a small investment in adaptation that pays dividends in comfort, adherence, and ultimately results throughout the remaining 90% of the protocol.
The full retatrutide dose schedule maps out the entire trajectory from starting dose through maintenance. Understanding the complete path helps manage expectations during the early phase when weight loss is minimal and the focus is entirely on adaptation. If you are wondering whether retatrutide is available for your protocol, the retatrutide availability guide covers current access options, and the online sourcing guide addresses procurement logistics.
Cost planning should also start at the beginning. The starting dose uses the least product per week, making it the most affordable phase of the protocol. As doses increase, weekly consumption rises proportionally. The retatrutide cost guide helps you budget for the entire protocol based on your planned dose progression. Understanding the overall cost of peptide protocols prevents financial surprises that could force premature protocol termination. Some researchers source through bulk retatrutide options to reduce per-milligram costs over longer protocols.
For researchers serious about optimizing their peptide protocols, SeekPeptides provides the most comprehensive resource available. Members access detailed dosing protocols, evidence-based guides, and a community of experienced researchers who have navigated these exact questions about starting doses, titration schedules, and long-term protocol management.
Starting dose for different retatrutide vial sizes
Retatrutide research peptides come in several common vial sizes. Your vial size determines how you calculate your starting dose in terms of injection volume.
5 mg vial: If you reconstitute 5 mg with 2 mL (200 units) of bacteriostatic water, each unit on an insulin syringe contains 0.025 mg. A 0.5 mg starting dose would be 20 units. A 1 mg starting dose would be 40 units. A 2 mg starting dose would be 80 units. This size is economical for the starting dose period since lower doses mean the vial lasts longer.
10 mg vial: Reconstituting 10 mg with 2 mL (200 units) gives 0.05 mg per unit. A 0.5 mg starting dose would be 10 units. A 1 mg dose would be 20 units. A 2 mg dose would be 40 units. This is the most common vial size and works well across all dose levels. The 20 mg vial dosing guide covers the larger vial calculations for those planning longer protocols.
Precision matters most at the starting dose because the absolute volumes are small. Drawing 10 units versus 12 units is a 20% dose difference, which is significant when you are trying to maintain a precise starting dose. Use high-quality insulin syringes with clear markings and take your time when drawing each dose. The guide to mixing peptides with bacteriostatic water covers the complete preparation process from start to finish, and the water volume guide explains how different water amounts change your concentration and unit calculations.
The peptide reconstitution calculator handles all these calculations instantly. Enter your vial size, water volume, and desired dose, and it returns the exact number of units to draw. This eliminates math errors that are especially consequential at the starting dose level.
Frequently asked questions
What is the lowest effective starting dose of retatrutide?
The lowest commonly used starting dose is 0.5 mg administered once weekly. While clinical trials began at 1 to 2 mg, community protocols often start lower to minimize side effects. Even at 0.5 mg, receptor activation begins and the body starts adapting to triple agonism. The complete retatrutide dose guide covers dosing from the lowest starting point through the highest therapeutic levels.
How long should I stay at the starting dose before increasing?
A minimum of four weeks is recommended at any dose level before increasing. This allows the body to reach steady state and adapt to the current level of receptor activation. If you are still experiencing side effects at week four, extend the starting dose period by two to four additional weeks until symptoms resolve. The dose schedule outlines the standard four-week intervals used in clinical trials.
Can I start retatrutide at a higher dose if I previously used tirzepatide?
Prior tirzepatide experience means your GLP-1 and GIP receptors are already adapted. Starting at 2 mg is reasonable for most people coming from moderate to high-dose tirzepatide. However, the glucagon receptor component is new regardless of your tirzepatide history, so starting above 2 mg is not recommended. The post-tirzepatide retatrutide dosing guide addresses this transition specifically.
What should I eat during the starting dose period?
Focus on smaller, more frequent meals with lean proteins, complex carbohydrates, and vegetables. Avoid large portions, high-fat foods, fried foods, and highly processed items. Stay hydrated with at least 64 ounces of water daily. The recommended food list for GLP-1 agonist users provides a comprehensive framework that applies directly to retatrutide.
Is nausea at the starting dose a sign the dose is too high?
Mild nausea that occurs occasionally, particularly after meals, is a normal adaptation response and does not necessarily indicate the dose is too high. However, persistent nausea throughout the day, nausea that interferes with eating or daily activities, or nausea accompanied by frequent vomiting suggests the dose exceeds your current tolerance. Reducing by half and staying at the lower level for four weeks before retrying is a safe approach.
How do I calculate my starting dose from a reconstituted vial?
Divide the total peptide in the vial by the total units of water added, then multiply by your desired dose. For example, a 10 mg vial reconstituted with 200 units of water gives 0.05 mg per unit. For a 1 mg starting dose, draw 20 units. The reconstitution chart and calculator make this process simple.
Should I take supplements during the starting dose period?
Adequate protein intake is the top priority, as GLP-1 agonists can reduce total food consumption. A quality multivitamin, vitamin B12, and an electrolyte supplement help prevent deficiencies during reduced caloric intake. Supplement recommendations for GLP-1 users apply equally to retatrutide, since the appetite suppression mechanisms are similar across the class.
Can the starting dose cause hair loss?
Hair loss is not typical at starting doses. When it occurs with GLP-1 agonists, it is usually related to rapid weight loss and caloric restriction at higher therapeutic doses, not to the peptide itself. The starting dose period, with its minimal weight loss, carries very low risk. Our guide on retatrutide and hair loss covers this topic in detail, including prevention strategies.
What happens if I miss a starting dose injection?
If you miss a weekly injection, take it as soon as you remember within three to four days of the planned date, then return to your regular schedule. If more than four days have passed, skip the missed dose and take the next one on schedule. Do not double up. Retatrutide has a six-day half-life, which means partial therapeutic levels persist even when a dose is missed, but consistency is important for steady adaptation during the starting period.
What is the difference between retatrutide and Ozempic starting doses?
Ozempic (semaglutide) and retatrutide use completely different starting dose strategies because of their different mechanisms. Ozempic starts at 0.25 mg weekly with only GLP-1 receptor activation. Retatrutide starts at 0.5 to 2 mg weekly with triple receptor activation. The milligram numbers are not directly comparable because each peptide has different potency per milligram at its target receptors. What matters is the approach: both start low and titrate up over months.
Can I split my starting dose into two injections per week?
Splitting the weekly dose into two smaller injections is sometimes done to reduce peak drug concentration and minimize GI side effects. For example, instead of 2 mg once weekly, you would inject 1 mg twice weekly. This approach is not validated in clinical trials but has theoretical merit for people with high GI sensitivity. The trade-off is the inconvenience of more frequent injections and potentially faster use of supplies. The microdosing GLP-1 guide discusses this concept in broader context.
Where can I source retatrutide for research?
Retatrutide is currently available through research peptide suppliers while clinical trials continue. The retatrutide buying guide covers sourcing considerations, quality verification, and what to look for in a supplier. You can also check our reviews of specific vendors like Peptide Sciences and Paradigm Peptides for retatrutide specifically.
How does the retatrutide starting dose affect blood sugar?
Even at the starting dose, GLP-1 and GIP receptor activation improves glucose-dependent insulin secretion. This means postprandial (after-meal) blood sugar spikes may decrease within the first week. People without diabetes typically notice smoother energy levels after meals. People with type 2 diabetes should monitor blood glucose closely during the starting period, as the addition of retatrutide may require adjustments to existing diabetes medications to prevent hypoglycemia.
Is there a retatrutide starting dose for people with type 2 diabetes?
The phase 2 trial for type 2 diabetes used similar starting doses to the obesity trial, with gradual titration. Weight loss results were slightly lower in the diabetes population (16.9% at the highest dose versus 24.2% in the obesity trial), but glycemic improvements were substantial. Blood sugar management at the starting dose is generally favorable, but coordination with a healthcare provider who manages diabetes medications is important to prevent hypoglycemic events as retatrutide begins improving insulin sensitivity.
External resources
ClinicalTrials.gov - Retatrutide Phase 2 Study (NCT04881760)
ClinicalTrials.gov - Retatrutide Phase 3 Study (NCT06859268)
For researchers committed to getting the most from their retatrutide protocols, SeekPeptides offers comprehensive protocol guidance, dosing calculators, and a community of thousands who have navigated these exact starting dose decisions.
In case I do not see you, good afternoon, good evening, and good night. May your starting dose stay smooth, your titration stay steady, and your results stay lasting.