Feb 19, 2026

Some people lose 30 pounds in three months on semaglutide. Others lose 30 pounds in three months, then nothing for the next eight weeks. Same medication. Same dose. Completely different trajectories.
The difference is not willpower. It is not genetics. And it is certainly not the medication "stopping working," despite what every forum post seems to suggest.
A semaglutide plateau is one of the most predictable, most misunderstood, and most solvable problems in GLP-1 therapy. Nearly every person who takes semaglutide long enough will hit one. The weight loss that felt effortless suddenly grinds to a halt. The scale refuses to move. Frustration builds. And the temptation to quit, to assume the medication has failed, becomes overwhelming.
But here is what experienced researchers and clinicians know that most people do not: a plateau is not a failure. It is a signal. Your body is telling you something specific, and once you understand the message, breaking through becomes a matter of strategy, not luck. The mechanisms behind semaglutide plateaus are well documented. The solutions are concrete. And the people who push past them consistently share a handful of approaches that separate temporary stalls from permanent progress.
This guide covers everything. The science behind why plateaus happen. The exact timeline most people experience them. The seven most common causes. And a complete, step-by-step protocol for restarting weight loss when progress stalls. Whether you have been on semaglutide for three months or twelve, whether you are on 0.25 mg or the maximum 2.4 mg dose, and whether this is your first plateau or your third, the path forward starts here.
What a semaglutide plateau actually is
A semaglutide plateau is a period of four or more weeks where body weight remains essentially unchanged despite continued medication use and consistent effort. It is not a bad week. It is not normal fluctuation. It is a sustained stall that persists long enough to indicate something fundamental has shifted in how the body responds to therapy.
Understanding this distinction matters.
Weight naturally fluctuates by 2 to 5 pounds day to day based on water retention, sodium intake, hormonal cycles, and bowel regularity. A true plateau sits underneath all of that noise. The trend line goes flat. Someone checking their semaglutide one month results might see the scale bounce between 195 and 198 for weeks. That is fluctuation, not a plateau. But when the weekly average stays at 196 for a full month, that is a stall worth addressing.
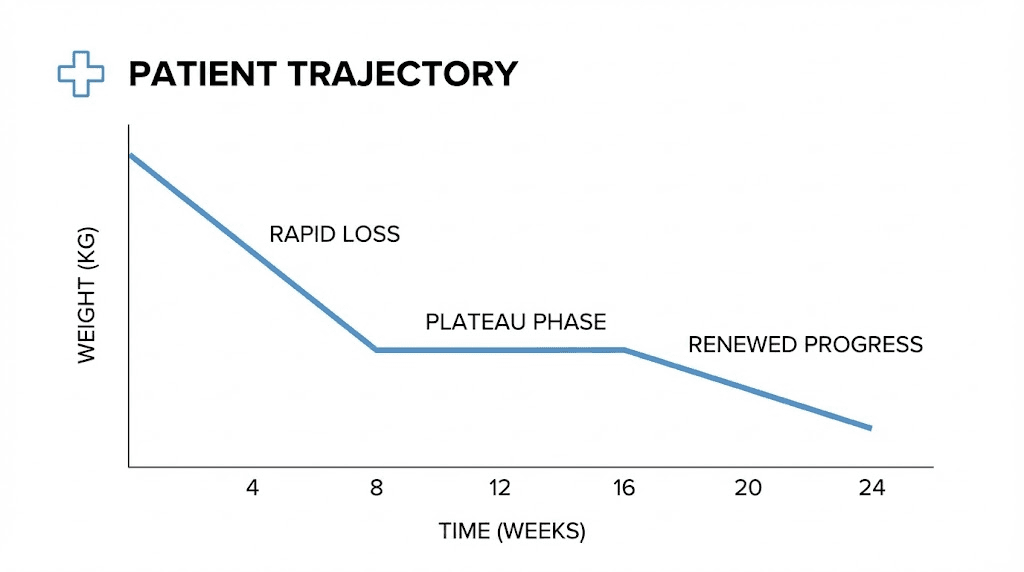
Research from the STEP trials, which evaluated how fast semaglutide works across thousands of participants, shows that weight loss follows a predictable curve. Rapid initial loss gives way to slower progress, which eventually levels off around months 12 to 15 for most users at the 2.4 mg dose. But many people experience interim plateaus much earlier, sometimes as soon as four weeks into treatment, particularly during dose escalation phases.
The critical insight is this: a plateau does not mean semaglutide has stopped working. The medication continues to activate GLP-1 receptors, suppress glucagon, slow gastric emptying, and signal satiety to the brain. What has changed is the balance between what the drug does and what the body does in response. That response, metabolic adaptation, is the real story behind every plateau. Understanding whether GLP-1 and Ozempic are the same thing helps clarify that the medication class itself produces this predictable pattern regardless of brand name.
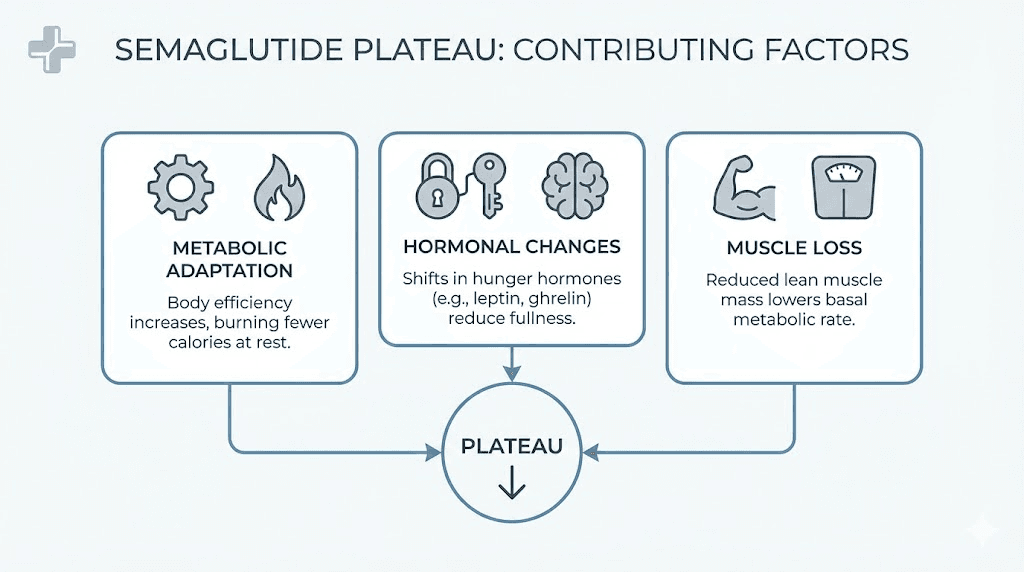
The science of metabolic adaptation on GLP-1 therapy
Your body does not want to lose weight. That statement sounds dramatic, but it is the foundation of every plateau you will ever experience. From an evolutionary perspective, the human body treats sustained weight loss as a threat. It responds with a coordinated defense that involves hormones, metabolism, appetite regulation, and energy expenditure. Understanding this defense system is the first step toward defeating it.
Resting metabolic rate decline
As you lose weight, your body requires fewer calories to maintain basic functions. This is simple physics. A 220-pound person burns more calories at rest than a 190-pound person, even if their body composition is identical. But the decline in metabolic rate during weight loss goes beyond what the numbers predict.
Research shows that the body reduces its resting metabolic rate by approximately 15 to 20 calories per pound of weight lost. Lose 30 pounds, and your daily calorie needs drop by 450 to 600 calories. That deficit that produced weight loss at the start of treatment may now be a maintenance level. The semaglutide diet plan that worked perfectly three months ago needs recalibrating.
This is called adaptive thermogenesis. It is the body deliberately slowing its engine beyond what weight loss alone would predict. Studies demonstrate that metabolic rate can decrease by an additional 5 to 15 percent on top of the expected reduction, creating a gap between predicted and actual calorie burn that makes continued weight loss progressively harder.
Hormonal recalibration
Weight loss triggers a cascade of hormonal changes designed to restore the body to its previous weight. Leptin, the hormone that signals satiety, decreases as fat stores shrink. Ghrelin, the hunger hormone, increases. Thyroid hormone output may decline slightly, further reducing metabolic rate. And insulin sensitivity improves, which is beneficial for health but means the body becomes more efficient at storing energy from the food you eat.
Semaglutide partially counteracts these changes. It suppresses appetite through central nervous system pathways, which is why appetite suppression on semaglutide remains effective even during a plateau. But the drug cannot fully override every compensatory mechanism the body deploys. When the hormonal shift becomes strong enough, weight loss stalls.
Muscle mass loss and its metabolic consequences
This is the factor most people underestimate. Clinical trial data from the STEP program shows that approximately 26 to 40 percent of weight lost on GLP-1 therapy comes from lean mass rather than fat. Lean tissue, primarily muscle, is metabolically active. It burns calories at rest. Every pound of muscle you lose reduces your resting metabolic rate by roughly 6 to 10 calories per day.
Lose 10 pounds of muscle over six months of semaglutide therapy, and your daily calorie burn drops by an additional 60 to 100 calories, on top of the reduction from fat loss. This compounds the metabolic slowdown and accelerates the timeline to a plateau.
The relationship between semaglutide and fatigue often traces back to this muscle loss. Less muscle means less strength, less energy, and a body that tires more easily, which in turn reduces daily activity and further widens the gap between calories consumed and calories burned. This is also why GLP-1 fatigue tends to worsen over time rather than improve, creating a vicious cycle where fatigue reduces activity and reduced activity accelerates metabolic decline.
The role of GLP-1 receptor desensitization
There is an additional mechanism worth understanding. Over time, the GLP-1 receptors in the brain and gut can become partially desensitized to continuous stimulation. This does not mean the medication stops working entirely. But it does mean the same dose produces a slightly weaker signal than it did during the first few weeks of treatment.
This receptor adaptation explains why appetite suppression on semaglutide often feels most powerful during the initial months and then gradually moderates. The medication is still working. The receptors are simply responding with less intensity. Some researchers believe this adaptation is partially reversible with periodic dose adjustments or medication holidays, though the evidence for these approaches remains limited.
When semaglutide plateaus typically happen
Plateaus do not strike randomly. They follow a pattern that, once you understand it, becomes almost predictable. Knowing when to expect a stall helps you prepare for it rather than panic when it arrives.
The dose escalation plateau (weeks 4 to 12)
Semaglutide dosing follows a stepwise titration. You start at 0.25 mg weekly, increase to 0.5 mg after four weeks, then 1.0 mg, then 1.7 mg, and finally 2.4 mg. Each dose increase is separated by at least four weeks. During this escalation, weight loss can be uneven. Some people lose aggressively at lower doses and then stall when moving to the next tier. Others see minimal results until reaching higher doses.
This early plateau is usually the easiest to break. It resolves on its own as the dose increases and the medication reaches therapeutic levels. If you are currently in the dose escalation phase and concerned about a stall, check your semaglutide dosage in units to confirm you are on track with the titration schedule. The semaglutide dosage calculator can help verify your current dose is correct for your progression.
The three-month plateau (weeks 12 to 16)
This is the most common plateau. By month three, the initial rapid weight loss phase has ended. The body has begun adapting. Appetite suppression, while still present, may feel less dramatic than it did during the first few weeks. And the calorie deficit that drove early weight loss has narrowed as the body adjusts to a lower weight.
Many people hit this plateau while still on a sub-maximal dose. The solution often involves a combination of dose optimization, dietary adjustment, and the introduction or modification of exercise, strategies covered in detail below.
The set point plateau (months 6 to 12)
Set point theory, while not fully proven in controlled human research, describes a phenomenon that virtually every long-term GLP-1 user recognizes. After significant weight loss, the body appears to "defend" a particular weight range. Progress slows dramatically. The scale refuses to budge. And no amount of short-term dietary restriction seems to make a difference.
This plateau is the hardest to break because it represents the body operating exactly as designed. Every compensatory mechanism, reduced metabolic rate, increased hunger hormones, improved calorie efficiency, is firing simultaneously. Breaking through requires a comprehensive, multi-pronged approach that addresses all of these factors at once.
The maximum dose plateau (months 9 to 15)
For people who have reached the 2.4 mg maximum dose of semaglutide, this plateau represents the medication doing everything it can. There is no higher dose to escalate to. The weight loss curve has flattened, and any further progress must come from optimizing everything around the medication. This is where understanding how long to stay on semaglutide becomes particularly relevant, because the answer depends heavily on whether you can successfully navigate this phase. Many people at this stage explore adding compounded formulations with added nutrients to support metabolism, or consider whether switching between GLP-1 medications might restart progress.
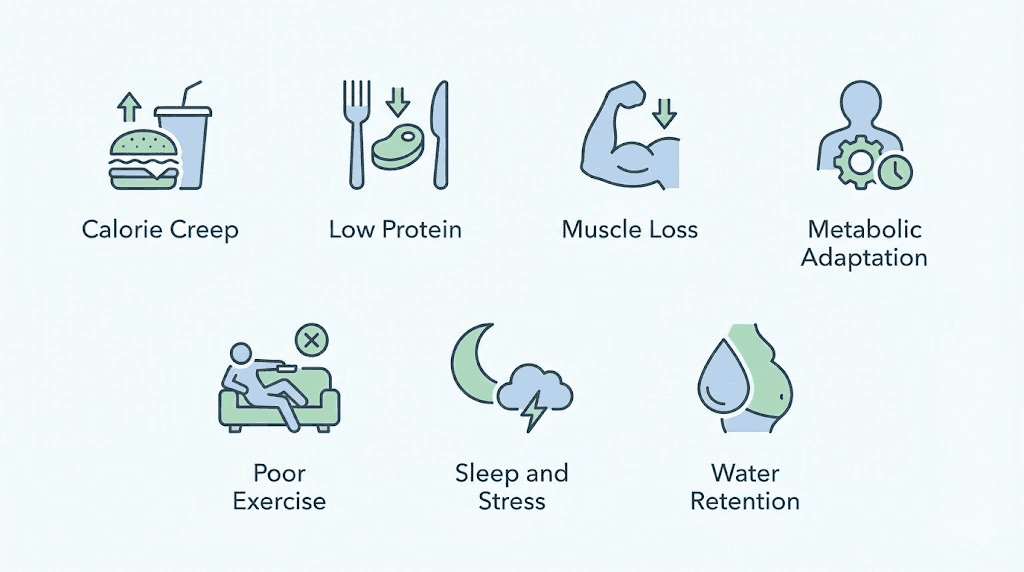
The seven most common causes of a semaglutide plateau
Research identifies seven distinct factors that drive semaglutide plateaus. Most people experience a combination of three or four simultaneously. Identifying which factors apply to your situation is essential for choosing the right corrective strategy.
1. Calorie creep
This is the most common and most underestimated cause. During the first weeks of semaglutide therapy, appetite suppression is dramatic. Many people eat 40 to 60 percent less without conscious effort. Food simply does not interest them. But over time, the body adjusts. Appetite gradually returns, not fully, but enough that portion sizes start creeping upward.
A person who was eating 1,200 calories per day during month one may be eating 1,600 to 1,800 calories by month four without realizing it. That 400 to 600 calorie increase, combined with a lower metabolic rate, erases the deficit entirely. Understanding the best foods to eat while on semaglutide helps combat this problem by emphasizing high-satiety, nutrient-dense options that keep calorie density low while maintaining nutritional adequacy.
The fix is straightforward but requires honesty: track food intake for one week. Not forever. Just long enough to see where the calories are hiding.
2. Insufficient protein intake
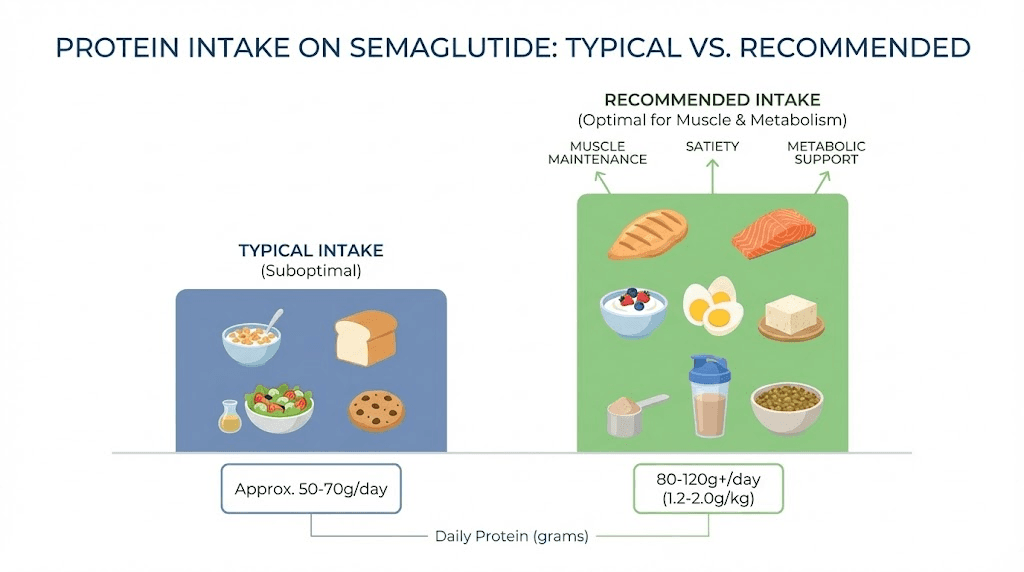
This deserves its own section later in this guide because it is that important. For now, understand that most people on semaglutide consume far too little protein. Reduced appetite leads to smaller meals, and smaller meals tend to be carbohydrate-heavy because carbs are easy to eat in small quantities. Protein requires more volume and more chewing, so it gets skipped.
The result is accelerated muscle loss, which drives metabolic slowdown, which causes the plateau. Research suggests GLP-1 users need 1.2 to 1.6 grams of protein per kilogram of body weight daily to preserve lean mass. Most are getting half that amount. If you are also exploring peptides for muscle growth to complement your GLP-1 therapy, adequate protein intake becomes even more critical because these peptides work synergistically with dietary protein to support lean tissue.
3. Loss of lean muscle mass
Connected to insufficient protein but distinct in its causes. Muscle loss during semaglutide therapy happens for three reasons: reduced calorie intake without adequate protein, reduced physical activity due to fatigue or decreased motivation, and the direct metabolic effects of rapid weight loss.
Every pound of muscle lost reduces daily calorie burn. Over months, this compounds into a significant metabolic handicap. The relationship between semaglutide and energy levels often reflects this muscle loss, as less muscle mass means less physical capacity and more perceived fatigue.
4. Metabolic adaptation beyond prediction
As discussed in the science section above, the body reduces its metabolic rate beyond what weight loss alone would predict. This adaptive thermogenesis creates a hidden calorie surplus. You think you are eating at a deficit based on your calculations, but your body is burning fewer calories than any calculator predicts.
Clinical studies show that adaptive thermogenesis can account for 100 to 300 extra calories per day of reduced expenditure. That is enough to completely stall weight loss even on a well-planned protocol.
5. Inadequate or inappropriate exercise
Many semaglutide users either exercise too little or exercise in ways that do not support continued weight loss. Steady-state cardio, walking on a treadmill for 30 minutes at the same speed every day, produces diminishing returns over time. The body adapts to repetitive exercise just as it adapts to calorie restriction.
The solution involves progressive resistance training and varied cardiovascular intensity. But there is a nuance here: overtraining can also cause plateaus by increasing cortisol and driving water retention. The balance matters, and finding it requires a structured approach.
6. Sleep deprivation and chronic stress
Poor sleep elevates ghrelin (the hunger hormone) and reduces leptin (the satiety hormone). It also impairs glucose metabolism, increases insulin resistance, and promotes fat storage, particularly visceral fat around the midsection. Studies show that sleeping less than six hours per night can reduce fat loss by up to 55 percent even when calorie intake remains constant.
Chronic stress compounds this through cortisol elevation. Sustained high cortisol promotes abdominal fat storage, increases appetite for high-calorie foods, and impairs the body ability to mobilize fat stores for energy. Together, poor sleep and chronic stress can completely neutralize the metabolic benefits of semaglutide.
7. Water retention masking fat loss
This is the stealth plateau. You are actually losing fat, but the scale does not reflect it because your body is retaining water. This happens commonly during periods of high sodium intake, hormonal fluctuations (particularly in women during menstrual cycles), after intense exercise (muscle repair requires water), and during periods of high stress (cortisol promotes water retention).
The telltale sign of a water retention plateau: your clothes fit better, your measurements are decreasing, but the scale stays flat. This is technically not a true plateau, but it feels like one and causes the same frustration.
How to break through a semaglutide plateau
Breaking a plateau requires addressing multiple factors simultaneously. Adjusting one variable rarely works because plateaus are almost always caused by a combination of mechanisms working together. The following protocol addresses each major driver systematically.
Step 1: Verify your dose is optimized
Before changing anything else, confirm that your medication dose is appropriate. If you are still in the titration phase, the plateau may resolve with the next dose increase. If you are at a sub-maximal dose and tolerating the medication well, discuss a dose increase with your prescriber.
The standard semaglutide titration for weight loss follows this schedule:
Weeks 1 to 4: 0.25 mg weekly
Weeks 5 to 8: 0.5 mg weekly
Weeks 9 to 12: 1.0 mg weekly
Weeks 13 to 16: 1.7 mg weekly
Week 17 onward: 2.4 mg weekly (maintenance dose)
Use a semaglutide dosage calculator to verify your current dose is accurate. If you are using compounded semaglutide, understanding your semaglutide dosage chart is especially important because compounded formulations require precise measurement. The conversion between units and milligrams must be exact to ensure you are receiving the intended dose. Many users find that checking their semaglutide dosage in units against the semaglutide dosage chart in units reveals dosing errors they never suspected. Even small inaccuracies compound over weeks. If your vial concentration is 5 mg/mL, the 5mg vial dosage chart can help verify exact draw volumes. For 10 mg vials, use the 10mg dosage chart instead.
Evidence suggests that staying on the maximum tolerated dose for 16 to 20 weeks, even during a plateau, can sometimes yield renewed weight loss without any other changes. The body needs time to adjust to the new metabolic environment created by full-dose therapy. Patience is not glamorous advice, but it is evidence-based. For those using compounded formulations, the compounded dosage calculator can verify accuracy across different concentration vials, and understanding unit-to-milligram conversions eliminates one common source of dosing uncertainty. Always cross-reference with the 20-unit conversion guide or the 10-unit conversion guide when adjusting your protocol.
Step 2: Audit your calorie intake
For one week, track everything you eat and drink. Everything. The coffee creamer. The handful of almonds. The cooking oil. The condiments. Research consistently shows that people underestimate calorie intake by 30 to 50 percent, and this underestimation increases over time as dietary habits become routine.
You are not tracking to obsess over numbers. You are tracking to identify the gap between perception and reality. Common sources of hidden calories during semaglutide therapy include:
Liquid calories: Juices, smoothies, sweetened coffee drinks, alcohol
Cooking fats: Oil, butter, and sauces added during preparation
Snacking: Small bites that feel insignificant but add up
Weekend overcompensation: Strict weekdays followed by relaxed weekends
If you discover that calorie intake has crept up, the semaglutide diet plan guide provides a structured framework for resetting your nutrition. Focus on meals that combine high protein, moderate healthy fats, and fiber-rich carbohydrates to maximize satiety per calorie. The foods that work well with GLP-1 therapy apply broadly regardless of which specific medication you use, because the appetite and digestion changes are similar across the class.
Step 3: Fix your protein intake immediately
This is the single highest-impact change most plateau-stalled users can make. Protein does three things that directly counter the mechanisms behind a plateau:
First, it preserves muscle mass. Adequate protein intake, combined with resistance training, dramatically reduces the proportion of weight lost from lean tissue. Second, it has the highest thermic effect of any macronutrient. Your body burns 20 to 30 percent of protein calories just digesting and processing them, compared to 5 to 10 percent for carbohydrates and 0 to 3 percent for fats. Third, protein is the most satiating macronutrient, keeping you fuller longer and reducing the likelihood of calorie creep.
Target 1.2 to 1.6 grams of protein per kilogram of body weight daily. For a 180-pound (82 kg) person, that translates to 98 to 131 grams of protein per day. Distribute this evenly across three to four meals, aiming for 25 to 35 grams per meal.
Practical protein sources that work well with semaglutide-reduced appetite (high protein density, low volume):
Greek yogurt: 15 to 20 grams per cup
Eggs: 6 grams each
Chicken breast: 31 grams per 4 ounces
Cottage cheese: 14 grams per half cup
Whey protein shake: 25 to 30 grams per scoop
Tuna: 25 grams per can
Edamame: 17 grams per cup
If you struggle to hit protein targets due to reduced appetite, protein shakes and semaglutide with B12 supplementation can help bridge the gap. B12 supports energy production and metabolism, which becomes especially important when calorie intake is restricted. Some compounded formulations include methylcobalamin (active B12) specifically to address this concern. SeekPeptides members get access to detailed macronutrient calculators that adjust protein targets based on body weight, activity level, and GLP-1 therapy phase, taking the guesswork out of plateau-phase nutrition.
One often-overlooked protein strategy: front-loading protein at breakfast. Many semaglutide users skip breakfast entirely because they wake up without hunger. But consuming 30 to 40 grams of protein within an hour of waking kickstarts muscle protein synthesis for the day. Even a simple protein shake accomplishes this. Combined with supplements that support GLP-1 therapy, this single habit change can meaningfully affect lean mass preservation over weeks and months.
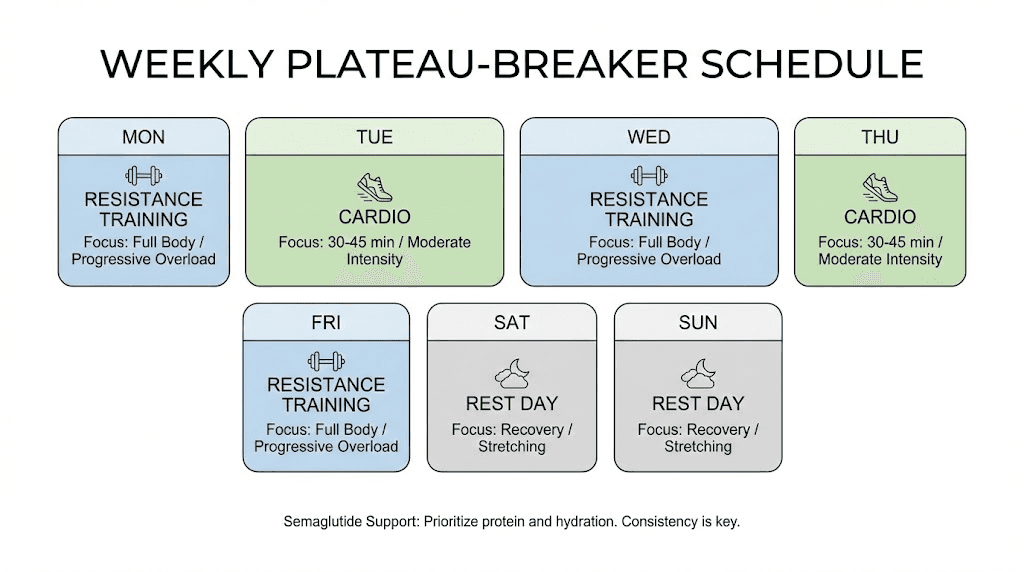
Step 4: Implement progressive resistance training
This is non-negotiable for breaking a plateau. Cardiovascular exercise alone will not solve the problem because it does not address the muscle loss that drives metabolic slowdown. Resistance training sends a signal to the body that muscle tissue is essential and should be preserved, even during calorie restriction.
A minimum effective protocol for semaglutide users hitting a plateau:
Frequency: 3 sessions per week, minimum. 4 is better.
Focus: Compound movements that engage multiple muscle groups simultaneously. Squats, deadlifts, rows, presses, and lunges. These exercises produce the greatest metabolic stimulus per minute of training.
Progression: Increase weight, reps, or sets each week. Progressive overload is what drives muscle preservation and growth. Doing the same workout with the same weights for months produces the same diminishing returns as walking at the same speed on the treadmill.
Sample weekly schedule:
Monday: Lower body (squats, lunges, leg press, Romanian deadlifts)
Wednesday: Upper body push (bench press, overhead press, dips, tricep work)
Friday: Upper body pull and posterior chain (rows, pulldowns, deadlifts, bicep work)
Optional Saturday: Full body circuit or active recovery
If you are new to resistance training, start with body weight exercises and progress to weights over 4 to 6 weeks. The goal is not to become a powerlifter. It is to provide sufficient mechanical stimulus to preserve the muscle tissue you have while the medication works on fat stores.
Combine this with moderate cardiovascular exercise, 150 minutes per week of moderate intensity or 75 minutes of vigorous intensity, and you create a metabolic environment that resists adaptation. Walking remains one of the most underrated tools here. Adding 2,000 to 4,000 extra steps per day can increase daily calorie expenditure by 100 to 200 calories without triggering the cortisol response associated with intense training.
Proper injection site selection can also affect your training. Injecting in the abdomen before an intense core workout may cause discomfort. Similarly, injecting into the thigh before a heavy leg day creates unnecessary friction. Plan your injection site around your training schedule to avoid any interference.
For those considering additional peptide support for recovery and muscle preservation during a plateau, understanding how various peptides complement GLP-1 therapy can be valuable. The relationship between peptides and fat loss extends well beyond GLP-1 agonists alone. Growth hormone peptides and healing peptides can support body composition goals through mechanisms that GLP-1 therapy does not address directly. The peptide calculator helps with accurate dosing across protocols, and the reconstitution calculator ensures proper preparation regardless of which peptides are in your stack.
Step 5: Optimize sleep and manage stress
Sleep is not optional. It is a metabolic intervention. Research from the University of Chicago found that reducing sleep from 8.5 to 5.5 hours per night decreased fat loss by 55 percent during a calorie-controlled diet. The participants eating the same calories and doing the same exercise lost dramatically less fat simply because they slept less.
Target 7 to 9 hours of quality sleep per night. Quality matters as much as quantity:
Consistent schedule: Same bedtime and wake time, including weekends
Cool environment: 65 to 68 degrees Fahrenheit is optimal for sleep quality
Dark room: Blackout curtains or a sleep mask
No screens 60 minutes before bed: Blue light suppresses melatonin production
No caffeine after 2 PM: Caffeine has a half-life of 5 to 6 hours
Stress management is equally critical. Chronic stress elevates cortisol, which directly promotes fat storage in the abdominal area and increases appetite for calorie-dense foods. Effective stress reduction strategies include:
10 minutes of daily meditation or deep breathing
Regular physical activity (which also addresses the exercise component)
Social connection and support
Setting boundaries around work and obligations
Professional support when needed
The connection between semaglutide fatigue and sleep quality is bidirectional. Poor sleep worsens fatigue, and semaglutide-related fatigue can impair sleep quality. Breaking this cycle requires intentional sleep hygiene practices, not just hoping it resolves on its own. If fatigue has become a significant issue during your plateau, the GLP-1 and energy guide covers strategies for improving energy levels that complement the sleep optimization described here.
Step 6: Consider strategic supplementation
Certain supplements can support plateau-breaking when combined with the lifestyle changes above. None of them work in isolation, but they can provide meaningful support to an otherwise solid protocol.
B12 (methylcobalamin): Reduced calorie intake often leads to micronutrient deficiencies, and B12 is among the most common. B12 supports energy metabolism, red blood cell production, and neurological function. Compounded semaglutide formulations that include B12 address this directly. If your formulation does not include it, a standalone supplement of 1,000 to 2,500 mcg daily (sublingual methylcobalamin) is a reasonable addition.
Glycine: Research on semaglutide with glycine shows potential benefits for sleep quality, collagen synthesis, and metabolic health. Glycine may also support GLP-1 receptor signaling. Typical supplemental doses range from 3 to 5 grams before bed.
Magnesium: Involved in over 300 enzymatic reactions including energy metabolism, muscle function, and sleep regulation. Magnesium glycinate (200 to 400 mg before bed) supports both sleep quality and muscle recovery.
Omega-3 fatty acids: EPA and DHA support insulin sensitivity, reduce inflammation, and may help preserve lean mass during calorie restriction. Aim for 2 to 3 grams of combined EPA/DHA daily from fish oil or algal oil.
Creatine monohydrate: The most well-researched supplement for muscle preservation and performance. 3 to 5 grams daily supports muscle function, strength, and may help counteract the lean mass loss associated with GLP-1 therapy. Particularly valuable for people engaged in resistance training. For a complete supplementation framework during GLP-1 therapy, the supplement guide for GLP-1 users covers additional options beyond those listed here.
Vitamin D: Often overlooked but critical. Vitamin D deficiency is common in overweight and obese individuals because fat tissue sequesters this vitamin. As you lose weight, stored vitamin D is released, but levels may still be inadequate. Vitamin D supports muscle function, immune health, and mood, all of which affect plateau recovery. Test your levels and supplement accordingly, typically 2,000 to 5,000 IU daily.
Step 7: Be patient with the timeline
This might be the hardest step. After weeks of watching the scale climb down, staring at the same number for a month feels like torture. But plateaus have a natural lifespan.
Most semaglutide plateaus last 4 to 8 weeks when no corrective action is taken. With the strategies above, many people see renewed progress within 2 to 4 weeks. The key is making changes simultaneously rather than sequentially. Adjusting diet one week, then exercise the next, then sleep the week after, rarely works because each change is too small to overcome the combined compensatory mechanisms driving the stall.
Instead, implement all changes at once. Fix protein, start resistance training, optimize sleep, and audit calories in the same week. The compounding effect of multiple interventions is greater than the sum of their individual parts.
The protein problem on GLP-1 therapy
Protein deserves its own deep dive because it is the single most impactful nutritional factor for plateau resolution, and the one most semaglutide users get wrong.
Why GLP-1 users undereat protein
Semaglutide reduces appetite powerfully. When you are not hungry, you eat whatever requires the least effort. Crackers. A piece of toast. Half a banana. A few bites of leftovers. These foods are almost entirely carbohydrates and fats. Protein requires more effort to prepare, more effort to chew, and more volume to achieve adequate intake.
The result is a daily pattern that looks like this for many semaglutide users:
Breakfast: Coffee (0g protein) or a small yogurt (8g protein)
Lunch: Half a sandwich or some soup (10 to 15g protein)
Dinner: A few bites of whatever is served (15 to 20g protein)
Total: 33 to 43 grams of protein
For a 170-pound person, the minimum target is approximately 93 grams daily. This person is getting less than half of what they need. Over weeks and months, the muscle loss compounds, metabolic rate declines, and a plateau becomes inevitable.
How to hit protein targets with reduced appetite
The strategies that work best are those that increase protein density, delivering more protein per bite:
Protein-first eating: At every meal, eat the protein source first, before anything else. When appetite is limited, this ensures protein gets prioritized over less critical macronutrients.
Protein shakes as meal supplements: A high-quality whey or plant-based protein shake mixed with water delivers 25 to 30 grams of protein in a form that goes down easily even when solid food feels unappealing. This is not replacing meals. It is supplementing them.
High-protein snack swaps: Replace carbohydrate-heavy snacks with protein-rich alternatives. Jerky instead of crackers. Greek yogurt instead of regular yogurt. String cheese instead of chips. Cottage cheese instead of a granola bar.
Timing around medication: Finding the best time of day to take semaglutide can help align your appetite windows with protein-rich meals. Some people find that taking semaglutide in the evening allows for better appetite during daytime meals when protein intake is more manageable.
For detailed meal planning, the complete food list for semaglutide users provides specific food choices optimized for GLP-1 therapy, with emphasis on protein-dense options that support plateau recovery.
Resistance training protocols for GLP-1 users
Exercise during GLP-1 therapy serves a different purpose than exercise without medication. The primary goal shifts from calorie burning to muscle preservation and metabolic rate protection. This distinction changes everything about how training should be structured.
Why cardio alone fails during a plateau
Cardiovascular exercise burns calories during the activity, but it does little to preserve muscle mass or elevate resting metabolic rate. In fact, excessive cardio during calorie restriction can accelerate muscle loss by adding to the overall energy deficit without providing the mechanical stimulus muscles need to justify their metabolic cost.
Running on a treadmill for 45 minutes might burn 400 calories, but if 50 of those calories come from muscle protein breakdown (which happens during sustained cardio in a calorie deficit), you are paying a metabolic tax that compounds over time. This is not an argument against cardio. It is an argument for prioritizing resistance training and treating cardio as a supplement, not the foundation.
The minimum effective dose for muscle preservation
Research on preserving lean mass during weight loss with GLP-1 therapy suggests the following minimum thresholds:
Frequency: 2 to 3 resistance training sessions per week (3 to 4 is optimal)
Volume: 2 to 3 sets per exercise, 8 to 12 repetitions per set
Exercises: 4 to 6 compound movements per session
Progressive overload: Increase weight by 2.5 to 5 percent when you can complete all prescribed sets and reps
Rest periods: 90 seconds to 3 minutes between sets for strength-focused work
Beginner-friendly protocol for semaglutide users
If you have never resistance trained before, do not let that become an excuse. Start with bodyweight movements and progress from there.
Phase 1 (weeks 1 to 4): Bodyweight foundations
Bodyweight squats: 3 sets of 12
Wall push-ups or knee push-ups: 3 sets of 10
Assisted lunges (holding a chair): 3 sets of 10 each leg
Seated rows with resistance band: 3 sets of 12
Glute bridges: 3 sets of 15
Phase 2 (weeks 5 to 8): Light weights
Goblet squats with dumbbell: 3 sets of 10
Dumbbell bench press: 3 sets of 10
Dumbbell rows: 3 sets of 10 each arm
Romanian deadlifts with dumbbells: 3 sets of 10
Overhead press with dumbbells: 3 sets of 10
Phase 3 (weeks 9 onward): Progressive loading
Barbell or heavy dumbbell squats: 3 sets of 8 to 10
Bench press: 3 sets of 8 to 10
Barbell rows: 3 sets of 8 to 10
Deadlifts: 3 sets of 6 to 8
Overhead press: 3 sets of 8 to 10
Accessory work: 2 sets of 12 to 15 for lagging areas
The key is consistency and progression, not intensity for its own sake. Three focused sessions per week, progressively adding weight, will produce more metabolic benefit than six unfocused sessions with random exercises and no plan.
When to consider switching medications
Sometimes the best strategy for a persistent semaglutide plateau is not to fight harder with the same medication but to consider alternatives. This decision should always involve a healthcare provider, but understanding the options helps you have an informed conversation.
Tirzepatide as an alternative
Tirzepatide, a dual GIP/GLP-1 receptor agonist, has demonstrated superior weight loss to semaglutide in head-to-head trials. The SURMOUNT-5 study showed tirzepatide produced 20.2 percent weight loss at 72 weeks compared to 13.7 percent for semaglutide. For detailed comparison data, the semaglutide vs tirzepatide comparison page breaks down the differences comprehensively. The dosage comparison chart shows how the two medications compare across dose ranges.
If you are plateauing on maximum-dose semaglutide, switching to tirzepatide addresses the plateau through a fundamentally different mechanism. The addition of GIP receptor agonism provides metabolic benefits that GLP-1 agonism alone cannot deliver. The side effect comparison between the two medications can help you weigh the tradeoffs, and the switching guide covers the practical logistics of transitioning between medications.
For those considering this switch, the semaglutide to tirzepatide conversion chart provides dosing equivalencies to ensure a smooth transition without losing momentum.
Combination approaches
Some healthcare providers address semaglutide plateaus by adding complementary medications rather than switching entirely. Common combinations include:
Semaglutide plus phentermine: Phentermine adds sympathomimetic appetite suppression and a slight metabolic boost. The combination of phentermine and semaglutide together has shown promise in breaking plateaus, though it requires careful medical supervision. For a head-to-head comparison of the two medications individually, see the phentermine vs semaglutide analysis.
Compounded formulations with added nutrients: Compounded semaglutide formulations often include additional ingredients like B12, glycine, or other nutrients that may support metabolic function during therapy. These enhanced formulations are available from compounding pharmacies like Empower Pharmacy and Olympia Pharmacy. Others explore options through vendors like Direct Meds for compounded formulations that include additional metabolic support ingredients.
Emerging options
The GLP-1 landscape is evolving rapidly. Newer medications in clinical trials show even greater weight loss potential. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown weight loss of up to 24 percent in early trials. For those interested in the latest developments, the retatrutide vs semaglutide comparison provides current research data.
Oral formulations are also entering the market. Oral semaglutide drops and oral GLP-1 pills like orforglipron may offer alternative delivery methods that some people find more convenient or better tolerated. The orforglipron vs tirzepatide comparison covers this emerging option in detail. Some users also explore tirzepatide drops as a sublingual alternative to injections, and the oral vs injection comparison for tirzepatide weighs the benefits and limitations of each delivery method.
Additionally, innovative delivery systems like GLP-1 patches represent another emerging option for people who dislike both injections and oral medications. These transdermal approaches are still early in development but could eventually provide another avenue for GLP-1 therapy with different absorption profiles.
Lifestyle factors that sabotage plateau recovery
Even with perfect medication management and solid training, certain lifestyle patterns can prevent plateau resolution. These are the factors most guides skip because they are uncomfortable to discuss.
Alcohol consumption
Alcohol affects semaglutide plateau recovery through multiple pathways. It provides empty calories (7 calories per gram, nearly as calorie-dense as fat). It impairs fat oxidation for up to 24 hours after consumption. It disrupts sleep architecture. It reduces protein synthesis. And it lowers inhibitions around food choices, leading to calorie-dense eating decisions that would not happen while sober.
Understanding alcohol and semaglutide interactions is essential during a plateau. The short version: if you are trying to break a plateau, eliminating alcohol for 4 to 8 weeks is one of the most impactful single changes you can make. One drink per week has minimal impact. Three or more drinks per week can measurably slow fat loss. The same principle applies to those using tirzepatide, as the alcohol and tirzepatide guide covers similar territory for the dual agonist.
Inconsistent injection timing and technique
Semaglutide is injected subcutaneously once weekly. Consistency in timing, while not critical to the millisecond, does matter for maintaining steady blood levels. Large variations in injection timing (giving the injection on Monday one week and Thursday the next) can create fluctuations in drug levels that affect appetite suppression consistency.
Injection technique also matters. Proper GLP-1 injection technique ensures the full dose is delivered subcutaneously. Injecting too shallow (intradermally) or too deep (intramuscularly) can affect absorption rates and drug efficacy. Rotating injection sites between the abdomen, thigh, and upper arm helps prevent lipodystrophy, localized fat tissue changes that can impair absorption over time.
If you are using compounded semaglutide, proper reconstitution technique is equally important. Incorrect reconstitution can result in inconsistent dosing, which manifests as unpredictable appetite suppression and uneven weight loss, both of which can mimic a plateau. The 5mg semaglutide reconstitution guide walks through the process step by step, and using the correct amount of bacteriostatic water for 10mg vials or 5mg vials ensures consistent concentration throughout the vial life.
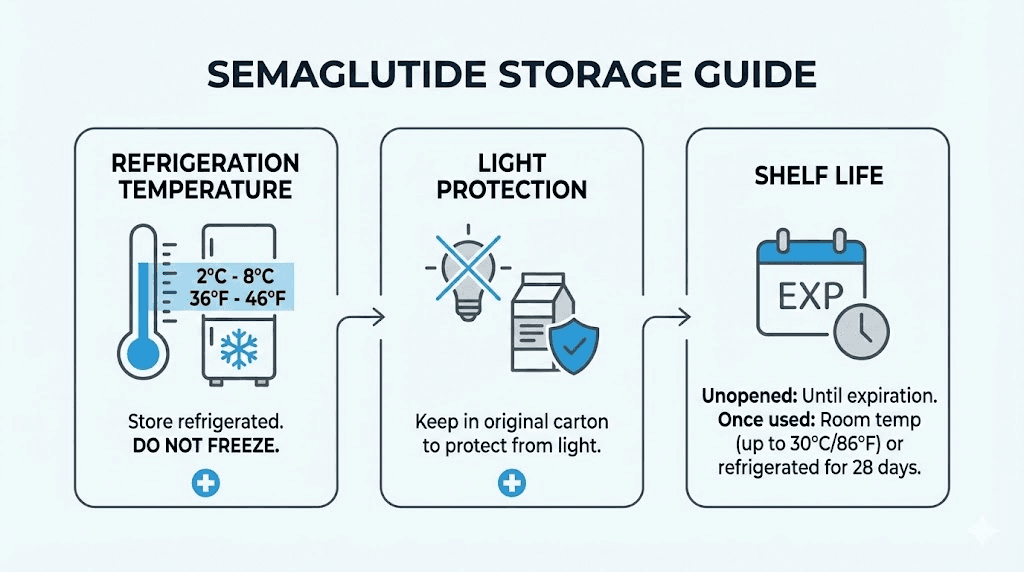
Medication storage errors
Improperly stored semaglutide loses potency. If your medication has been exposed to heat, direct sunlight, or freezing temperatures, you may be receiving a sub-therapeutic dose without knowing it. This is one of the most overlooked causes of an apparent plateau.
Compounded semaglutide has specific storage requirements. Understanding whether compounded semaglutide needs refrigeration and how long it lasts in the fridge ensures you are always using potent medication. Similarly, checking whether expired semaglutide is still effective can rule out degraded medication as a plateau cause.
The plateau mindset: psychology of stalled progress
A plateau is not just a physical event. It is a psychological one. And the mental response to a plateau often determines whether someone breaks through or gives up entirely.
The frustration spiral
It starts with the scale. Flat. Again. For the third week in a row. Frustration builds. You start questioning the medication. Maybe it has stopped working. Maybe your body is different. Maybe this was never going to work long-term.
This frustration leads to behavioral changes that make the plateau worse. Comfort eating increases. Exercise motivation drops. Sleep suffers because stress is elevated. The plateau feeds itself through the psychological response it creates.
Recognizing this spiral is the first step to breaking it. A plateau is not evidence of failure. It is evidence that your body is functioning exactly as evolution designed it to function. The medication has not stopped working. The battlefield has shifted. Many experienced GLP-1 users describe similar frustrations in the SeekPeptides community, where shared experiences normalize the plateau phase and reduce the isolation that makes it harder to push through.
Non-scale victories matter more than you think
During a plateau, the scale becomes an unreliable indicator of progress. But other metrics often continue improving:
Waist circumference: May continue decreasing even when weight stalls
Body composition: Fat loss may continue while muscle gain offsets it on the scale
Blood markers: A1C, fasting glucose, triglycerides, blood pressure often continue improving
Energy levels: Many people report improved energy during plateaus, especially if they have addressed energy levels on semaglutide through proper supplementation
Clothing fit: Sizes may continue dropping even when weight does not
Physical performance: Strength, endurance, and cardiovascular fitness continue improving with consistent training
Taking body measurements weekly (waist, hips, chest, thighs, arms) provides a more complete picture of progress than the scale alone. Many people discover they are losing fat and gaining muscle simultaneously, a phenomenon called body recomposition that shows no change on the scale but dramatic changes in the mirror.
Setting realistic expectations
The STEP trials showed that average weight loss with semaglutide 2.4 mg was approximately 14.9 percent of body weight at 68 weeks. But "average" is misleading. Some participants lost 25 percent or more. Others lost less than 5 percent. The distribution is wide, and comparing yourself to outlier results shared on social media is a recipe for disappointment.
A more useful framework: a sustained loss of 10 percent or more of body weight produces significant health benefits, including reduced cardiovascular risk, improved insulin sensitivity, better blood pressure, reduced joint stress, and improved sleep apnea. If you have lost 10 percent and plateaued, you have already achieved a medically meaningful outcome. The question is not whether the medication worked. It did. The question is whether additional loss is achievable with the strategies outlined above.
Advanced plateau-breaking strategies
For people who have implemented the basics, optimized protein, started resistance training, fixed sleep, and still find themselves stuck, these advanced approaches can provide the edge needed to restart progress.
Calorie cycling
Instead of eating the same calorie target every day, alternate between higher and lower calorie days. This can help prevent the metabolic adaptation that occurs with sustained calorie restriction. A common approach:
Training days (3 to 4 per week): Eat at maintenance calories with high protein
Rest days (3 to 4 per week): Eat 300 to 500 calories below maintenance
The higher-calorie days help maintain metabolic rate and support recovery from training, while the lower-calorie days create the deficit needed for fat loss. The average weekly deficit is similar to a straight calorie restriction approach, but the metabolic signaling is different because the body never fully adapts to a single intake level.
Strategic refeed days
One day per week or every two weeks, intentionally increase calorie intake to maintenance or slightly above, with the extra calories coming primarily from carbohydrates. This temporarily boosts leptin levels, increases thyroid hormone output, and provides a psychological break from restriction.
A refeed is not a "cheat day." It is a controlled, strategic increase in carbohydrate intake designed to send specific hormonal signals. The difference matters. A cheat day often involves 3,000 to 5,000 uncontrolled calories of whatever sounds good. A refeed involves an additional 300 to 500 calories above maintenance, primarily from complex carbohydrates, consumed alongside adequate protein.
NEAT optimization
Non-exercise activity thermogenesis (NEAT) accounts for a surprisingly large portion of daily calorie expenditure. It includes fidgeting, walking, standing, household chores, and all movement that is not formal exercise. Research shows that NEAT can vary by up to 2,000 calories per day between individuals and decreases significantly during weight loss.
Practical NEAT-boosting strategies:
Take phone calls while walking
Stand at a desk for portions of the workday
Park farther from destinations
Take stairs instead of elevators
Do household chores actively
Set a timer to stand and move for 5 minutes every hour
Increasing daily step count from 5,000 to 10,000 steps can boost daily calorie expenditure by 200 to 400 calories, enough to restart fat loss during a plateau without additional formal exercise. Tools like the GLP-1 plotter can help visualize your weight trajectory over time and distinguish between true plateaus and normal fluctuation patterns, making it easier to decide when NEAT optimization alone is sufficient versus when more aggressive interventions are needed.
Timed eating windows
Time-restricted eating (eating within a defined window of 8 to 10 hours daily) can complement semaglutide therapy during a plateau. This approach works not through magical metabolic effects but through practical calorie reduction: fewer hours to eat generally means less food consumed.
A common pattern for semaglutide users: first meal at noon, last meal by 8 PM. This 8-hour window naturally eliminates late-night snacking, one of the most common sources of excess calories during a plateau. Pair this with protein-first eating, and the combination creates a practical framework for controlling intake without obsessive calorie counting.
Body composition focus over scale weight
This mindset shift can transform how you experience a plateau. Stop chasing a number on the scale. Start tracking body composition instead.
When you add resistance training while taking semaglutide, something remarkable can happen. You lose fat. You gain muscle. The scale barely moves. But your waist shrinks. Your clothes fit better. You look different. You feel stronger.
This is body recomposition, and it is arguably a better outcome than pure weight loss because it preserves metabolic rate, improves functional capacity, and creates a more sustainable long-term result. Someone who weighs 175 pounds with 25 percent body fat is in a dramatically different metabolic situation than someone who weighs 175 pounds with 35 percent body fat, even though the scale shows the same number.
Track your progress with measurements, progress photos, and how clothing fits. These metrics tell the real story during a plateau. Many people who feel "stuck" are actually making excellent progress that the scale simply cannot capture.
Hydration as a plateau variable
Dehydration is surprisingly common during GLP-1 therapy. Reduced food intake means reduced water intake from food (which normally provides 20 to 30 percent of daily hydration). Gastrointestinal side effects like semaglutide constipation and semaglutide burping can further discourage fluid consumption. And many semaglutide users drink less simply because they are eating less and do not feel as thirsty.
Dehydration slows fat metabolism, reduces exercise performance, impairs recovery, and causes water retention (paradoxically, drinking less water makes the body hold more). Target a minimum of half your body weight in ounces of water daily. A 180-pound person should aim for 90 ounces, approximately 11 cups. During exercise, add another 16 to 24 ounces per hour of activity.
What the research actually says about long-term semaglutide outcomes
Understanding the long-term trajectory helps put plateaus in perspective. The SELECT trial, which followed semaglutide users for up to four years, provides the best available data on what happens beyond the initial weight loss phase.
The weight loss curve
Weight loss with semaglutide follows a predictable pattern across large populations:
Months 1 to 3: Rapid weight loss, often 4 to 8 percent of body weight
Months 3 to 6: Continued but slowing weight loss, reaching 8 to 12 percent
Months 6 to 12: Further slowing, reaching 12 to 15 percent
Months 12 to 18: Plateau phase for most users, weight stabilizes
Beyond 18 months: Weight maintenance with continued medication use
This curve is not a failure. It is the expected outcome. Semaglutide was never designed to produce indefinite weight loss. It was designed to produce significant weight loss followed by sustained maintenance at a lower body weight. The plateau is actually the medication succeeding at its primary long-term goal: preventing weight regain.
What happens when you stop
Understanding semaglutide withdrawal is relevant during a plateau because many people consider stopping when progress stalls. The data is sobering: participants who stopped semaglutide in clinical trials regained approximately two-thirds of their lost weight within one year.
This does not mean you must stay on semaglutide forever. But it does mean that stopping during a plateau, hoping to "reset" and restart later, is generally not an effective strategy. The plateau is a phase to work through, not a signal to stop. For those who do need to discontinue, understanding the full picture of what happens when you stop semaglutide helps set realistic expectations for weight management after medication.
Tracking your plateau recovery
Once you implement the strategies above, systematic tracking helps you identify what is working and what needs adjustment.
What to track
Weekly weigh-in: Same day, same time, same conditions (morning, after bathroom, before eating). Record weekly averages rather than daily weights to smooth out fluctuations.
Weekly measurements: Waist, hips, chest, and thigh circumference. Use a flexible tape measure in the same position each time.
Daily protein intake: Track for at least the first 4 weeks until high-protein eating becomes automatic.
Training log: Record exercises, sets, reps, and weights. Progressive overload only happens when you track it.
Sleep quality: Hours slept and subjective quality rating (1 to 10).
Energy levels: Subjective daily rating helps identify patterns.
When to expect results
With a comprehensive approach addressing all major factors:
Week 1 to 2: Water weight changes from dietary adjustments (scale may drop or increase based on sodium and carb changes)
Week 2 to 4: First signs of renewed fat loss, often visible in measurements before the scale
Week 4 to 8: Consistent downward trend reestablished for most people
Week 8 to 12: New baseline rate of loss established, typically slower than initial rate but sustained
If you do not see any progress after 8 weeks of full implementation, consult your healthcare provider. There may be underlying medical factors (thyroid dysfunction, medication interactions, hormonal imbalances) that require specific testing and treatment. Understanding whether your GLP-1 medication affects metabolism directly can help frame these conversations with your provider.
SeekPeptides members access detailed tracking templates, progress calculators, and protocol adjustment guides designed specifically for GLP-1 therapy. The platform provides the tools needed to systematically identify and address plateau causes, with support from a community of researchers who have navigated these same challenges. The peptide cost calculator can also help evaluate whether switching formulations or adding complementary protocols makes financial sense alongside clinical sense.
Common mistakes that prolong a semaglutide plateau
Knowing what NOT to do is as important as knowing what to do. These are the most common errors that keep people stuck in plateaus far longer than necessary.
Mistake 1: Cutting calories too aggressively
The instinct when weight loss stalls is to eat even less. This backfires spectacularly. Extreme calorie restriction accelerates muscle loss, further reduces metabolic rate, increases cortisol, impairs thyroid function, and triggers the body most aggressive compensatory mechanisms. The result: more metabolic adaptation, not less.
A moderate deficit of 300 to 500 calories below maintenance is sufficient. Anything beyond that during a plateau is counterproductive.
Mistake 2: Doing more cardio instead of resistance training
When progress stalls, many people double their cardio. More treadmill. More elliptical. More running. This approach burns calories during the activity but does nothing to address the underlying cause of the plateau, which is metabolic rate decline driven by muscle loss. Adding resistance training is far more effective than adding cardio volume.
Mistake 3: Ignoring the medication itself
Checking that your semaglutide is properly stored, not expired, correctly reconstituted (if compounded), and properly injected seems basic, but these factors cause more "mystery plateaus" than most people realize. The shelf life of semaglutide is finite, and degraded medication will not produce the same effects as fresh product. If you are traveling with your medication, understanding how to travel with semaglutide ensures potency is maintained through temperature changes and transit conditions.
Mistake 4: Comparing to others
Social media is full of dramatic transformation stories. Someone lost 50 pounds in four months. Someone else lost 80 pounds in a year. These stories, while inspiring, represent the far end of the bell curve. Comparing your plateau to someone else highlight reel creates unrealistic expectations and unnecessary frustration.
Your results depend on your starting weight, your body composition, your genetics, your medication response, your adherence, your exercise history, your stress levels, your sleep quality, your age, your hormonal profile, and dozens of other factors that are unique to you. The only useful comparison is to your own previous results and to realistic clinical trial averages. Looking at real GLP-1 before and after results from actual users can help calibrate expectations, but remember that the people sharing results online tend to be outliers in either direction.
Mistake 5: Stopping the medication during a plateau
As discussed above, stopping semaglutide during a plateau typically leads to rapid weight regain. The medication is still providing value even when the scale is not moving. It is preventing regain. It is maintaining appetite suppression. It is supporting the metabolic improvements achieved during the weight loss phase. Stopping removes all of these benefits simultaneously.
Frequently asked questions
How long does a semaglutide plateau usually last?
Most semaglutide plateaus last 4 to 8 weeks without intervention. With the comprehensive strategies outlined in this guide, addressing protein, exercise, sleep, and calorie management simultaneously, many people see renewed progress within 2 to 4 weeks. Plateaus lasting longer than 12 weeks despite full implementation of these strategies warrant a conversation with your healthcare provider about potential underlying factors.
Is it normal to plateau on semaglutide after 3 months?
Yes, extremely normal. The three-month mark is the most common time for the first significant plateau. Initial rapid weight loss has ended, the body has begun adapting to the new calorie intake and medication effects, and the calorie deficit has narrowed. This is not a sign that the medication has failed. It is a predictable phase that nearly every user experiences. Review your semaglutide progress timeline to see how your results compare to typical expectations.
Should I increase my semaglutide dose to break a plateau?
If you are not yet at the maximum dose (2.4 mg weekly for weight loss), a dose increase may help and should be discussed with your prescriber. However, dose increases alone rarely break plateaus caused by metabolic adaptation. Use the semaglutide dosage calculator to verify your current dose and consult your provider about whether escalation is appropriate. Evidence suggests combining a dose increase with lifestyle modifications produces better results than either approach alone.
Can I switch from semaglutide to tirzepatide to overcome a plateau?
Switching to tirzepatide is a viable option for persistent semaglutide plateaus. Tirzepatide dual mechanism (GLP-1 plus GIP) produced 20.2 percent weight loss versus 13.7 percent for semaglutide in head-to-head trials. The conversion chart helps guide the transition, and the comprehensive comparison covers all relevant differences. This decision should always involve your healthcare provider.
Does semaglutide stop working over time?
Semaglutide does not stop working. The medication continues to activate GLP-1 receptors, suppress appetite, and slow gastric emptying regardless of how long you take it. What changes is the body compensatory response. Metabolic adaptation, hormonal recalibration, and muscle loss create conditions where the same dose produces different outcomes. The medication is doing its job. The body is doing its job too, and those two jobs eventually reach equilibrium, which is what a plateau represents.
How much weight should I expect to lose after breaking a plateau?
After breaking a plateau, weight loss typically resumes at a slower rate than the initial phase. Expect 0.5 to 1.5 pounds per week rather than the 2 to 4 pounds per week common in early treatment. This slower rate is sustainable and more likely to be maintained long-term. Total additional weight loss after a plateau varies widely but typically ranges from 5 to 15 additional pounds before the next equilibrium point.
Will exercise alone break a semaglutide plateau?
Exercise alone is unlikely to break a plateau if nutrition and sleep are not also optimized. However, adding resistance training is the single most impactful exercise change you can make. It preserves and builds muscle, which directly counters the metabolic slowdown driving the plateau. Combine resistance training with adequate protein (1.2 to 1.6 g/kg/day) for maximum impact.
What foods should I avoid during a semaglutide plateau?
Focus less on foods to avoid and more on foods to prioritize. High-protein, moderate-fat, fiber-rich foods should form the foundation of every meal. That said, common plateau-prolonging foods include liquid calories (juice, sweetened coffee, alcohol), ultra-processed snacks, and refined carbohydrates that provide calories without satiation. The foods to avoid guide applies broadly to GLP-1 therapy and provides specific recommendations. For a more positive approach, the complete food list for semaglutide focuses on what to eat rather than what to skip, with emphasis on foods that support plateau recovery.
Can taking semaglutide a day early or late affect my plateau?
Small timing variations of 1 to 2 days are unlikely to cause a plateau on their own. However, consistently inconsistent timing can create fluctuations in blood drug levels that affect appetite suppression. The guidance on injection timing flexibility applies similarly to semaglutide. Pick a consistent day and approximate time each week and stick with it as closely as practical.
Does semaglutide cause hair loss during a plateau?
Hair loss with GLP-1 therapy is related to rapid weight loss and nutritional deficiency, not to the medication directly or to a plateau phase. In fact, plateaus often coincide with reduced hair shedding because the rapid weight loss that triggers telogen effluvium has slowed. If you experienced GLP-1 related hair loss during active weight loss, it typically resolves within 3 to 6 months after weight stabilizes.
Should I take supplements during a semaglutide plateau?
Targeted supplementation can support plateau recovery when combined with dietary and exercise changes. Key supplements include B12 (especially if using non-compounded formulations), protein powder, magnesium, omega-3 fatty acids, and creatine. The glycine supplementation guide for semaglutide covers an often-overlooked amino acid that supports sleep quality and metabolic health, both of which directly affect plateau duration.
External resources
STEP 1 Trial: Semaglutide for Weight Loss (New England Journal of Medicine)
SELECT Trial: Long-term Semaglutide Weight Loss Effects (Nature Medicine)
Once-Weekly Semaglutide for Weight Management: Clinical Review (PMC)
GLP-1 Agonists and Exercise (Frontiers in Clinical Diabetes)
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact plateau challenges.
In case I do not see you, good afternoon, good evening, and good night. May your plateaus stay temporary, your protein stay high, and your progress stay consistent.