Feb 13, 2026

Your first injection is done. The semaglutide is in your system. And now you are staring at the fridge, waiting for something to change. Waiting for the hunger to vanish. Waiting for the food noise to go quiet. Waiting for that switch everyone talks about online, the one that supposedly flips the moment the medication enters your bloodstream.
It does not work like that.
Not exactly, anyway. The relationship between semaglutide and appetite suppression is more nuanced than the internet would have you believe, more layered than a simple yes-or-no answer can capture. Some people notice subtle changes within 24 to 48 hours of their first injection. Others wait weeks before feeling anything different at all. And the reasons for this variation reveal something important about how semaglutide actually works inside your body, something that goes far beyond a single molecule binding to a single receptor.
This guide breaks down the complete appetite suppression timeline from your first injection through maintenance dosing. You will learn what the clinical trials actually show, what the brain science explains about why timing varies so dramatically between individuals, and what you can do if semaglutide is not suppressing your appetite as quickly as you expected. Because understanding the real mechanism behind semaglutide appetite suppression is the difference between working with the medication and fighting against your own expectations.
SeekPeptides has compiled the most comprehensive breakdown available, pulling from clinical data, pharmacological research, and thousands of real-world user experiences to give you the answer that actually matches reality.
The short answer: no, but it is complicated
Semaglutide does not suppress appetite immediately in the way most people imagine. There is no sudden loss of hunger. No moment where food becomes repulsive. No on-off switch.
But here is what makes the answer complicated. The medication begins working in your body almost immediately after injection. Semaglutide starts binding to GLP-1 receptors within hours. It begins slowing gastric emptying. It starts sending signals to your brain. The machinery is turning before you finish dinner that night.
The problem is perception versus pharmacology. Your body needs time to respond to those signals in a way you can actually feel. And the starting dose of 0.25 mg is intentionally low, designed to let your digestive system adapt before the real appetite suppression kicks in at higher doses.
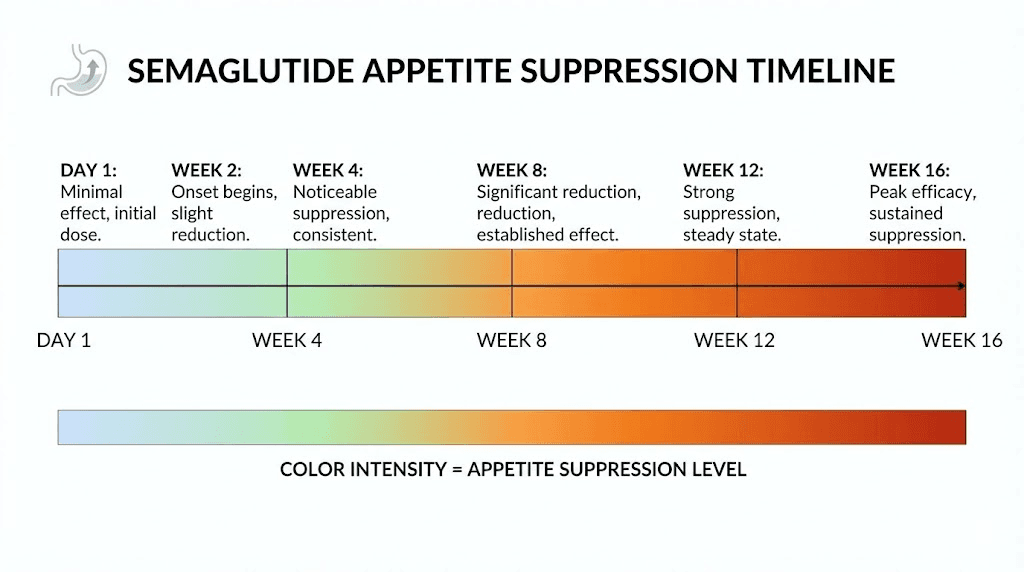
Think of it this way. The medication is whispering to your appetite from day one. By week four, it is speaking clearly. By the time you reach maintenance doses, it is making itself impossible to ignore. The volume increases gradually, not all at once.
How semaglutide actually suppresses appetite
Understanding why semaglutide does not work instantly requires understanding what it does inside your body. The mechanism is not simple. It involves your gut, your brain, your blood sugar, and your entire relationship with food. Multiple systems are being activated simultaneously, and each one operates on a slightly different timeline.
The GLP-1 receptor system
Semaglutide is a GLP-1 receptor agonist. That means it mimics a hormone your body already produces called glucagon-like peptide-1. Your gut releases natural GLP-1 after you eat, and it plays a role in regulating hunger and satiety. The problem is natural GLP-1 breaks down in minutes. Semaglutide has been engineered to last for days.
This extended duration is why you inject it once weekly rather than multiple times daily. The molecular modifications that keep semaglutide active in your bloodstream are also why it takes time to build up to effective concentrations. Your body processes the medication slowly and steadily, reaching peak blood levels approximately 24 to 72 hours after each injection before gradually declining until the next dose.
The brain pathways
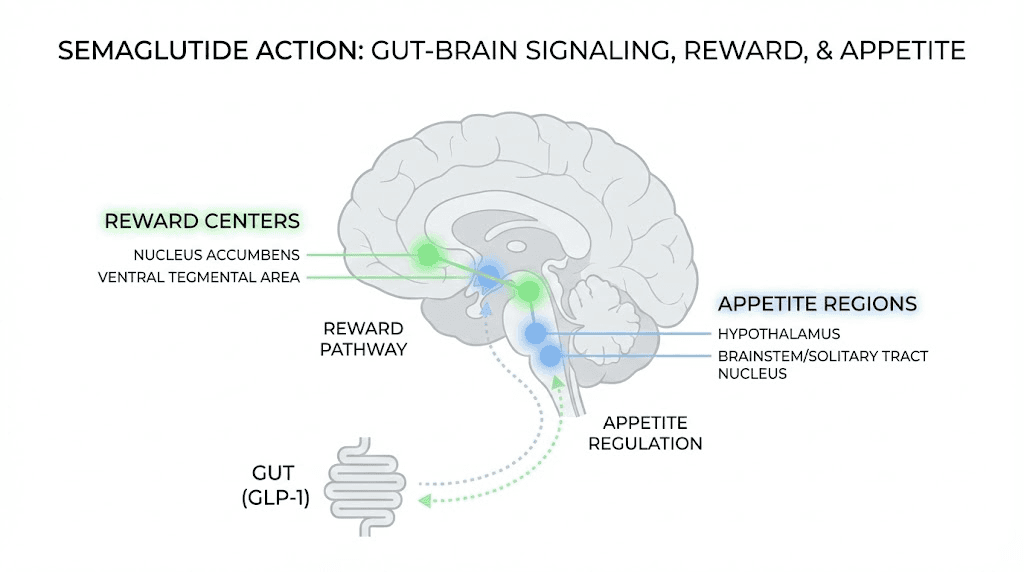
The most important appetite-related effects happen in your brain. Semaglutide crosses into the central nervous system and activates GLP-1 receptors in several critical regions. The hypothalamus, which controls hunger and satiety signals. The nucleus tractus solitarius in the brainstem, which processes gut signals. And the reward centers that drive food cravings and what researchers call "food noise."
In the hypothalamus, semaglutide activates neurons that suppress appetite (called POMC/CART neurons) while simultaneously inhibiting neurons that drive hunger (called NPY/AgRP neurons). This dual action, pushing down hunger while pulling up fullness, is what creates that profound shift in eating behavior that users describe.
But these neural pathways need sustained stimulation to produce noticeable effects. One dose starts the process. Consistent weekly dosing builds the signal strength over time. This is pharmacology, not magic. The brain needs repeated exposure at increasing concentrations to fully modulate appetite circuits.
Gastric emptying
Semaglutide also slows how quickly food moves from your stomach to your small intestine. This is called delayed gastric emptying, and it creates a physical sensation of fullness that lasts longer after each meal. Food sits in your stomach for extended periods, sending sustained stretch signals that tell your brain you have had enough.
This mechanism does begin working relatively quickly after each injection. Some people notice they feel fuller faster within the first few days. But the degree of gastric slowing intensifies as blood concentrations rise with each subsequent dose, and the most pronounced effects occur at the higher maintenance doses of semaglutide.
Blood sugar stabilization
Semaglutide was originally developed for type 2 diabetes, and its blood sugar effects contribute to appetite regulation. By improving insulin sensitivity and reducing blood sugar spikes after meals, semaglutide eliminates many of the glucose-driven hunger signals that cause cravings between meals. Stable blood sugar means fewer urgent feelings of needing to eat. This effect begins within the first week but becomes more consistent as the medication builds in your system over subsequent weeks of dosing.
The real timeline: what to expect at each stage
Clinical research and thousands of user reports paint a consistent picture of how appetite suppression develops over time. This is not an overnight transformation. It is a gradual shift that most people only recognize in hindsight, looking back at how their relationship with food changed week by week.
Days 1 to 3: the quiet start
Most people feel nothing dramatic. Some feel nothing at all. Your first injection of 0.25 mg is a fraction of the therapeutic dose, intentionally kept low to help your body adjust. Semaglutide reaches peak blood concentration within one to three days, but at this low dose, the effects are subtle at best.
What some people notice: slightly less interest in snacking. Meals feel a tiny bit more satisfying. The urge to eat after dinner is a little quieter. These changes are so small that many people dismiss them entirely.
What most people notice: nothing obvious. Perhaps some mild nausea. Maybe slight fatigue. The digestive system is adjusting, and the brain is just beginning to receive the first faint signals from the medication.
Here is the important thing. Just because you cannot feel it working does not mean it is not working. The medication is already binding to receptors, already influencing gastric emptying, already beginning the slow process of modulating your appetite circuits. You simply have not crossed the threshold of conscious awareness yet.
Week 1: subtle shifts
By the end of the first week, approximately 30 to 40 percent of users report some noticeable change in appetite. The most common descriptions involve reduced "food noise," that constant background chatter about what to eat next, when to eat, whether there is something good in the pantry. For many people, this is the first sign that semaglutide is doing something.
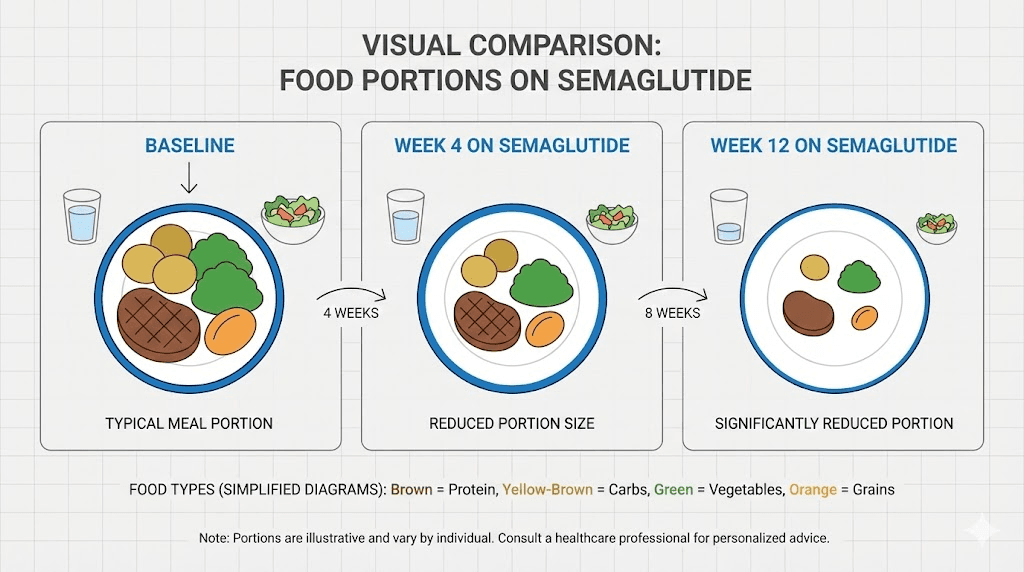
Portion sizes may naturally decrease by 10 to 15 percent without conscious effort. You might leave food on your plate for the first time in memory. You might realize at 2pm that you forgot about your usual snack without even thinking about it.
The nausea that some people experience during week one can itself reduce appetite, but this is a side effect, not the therapeutic mechanism. True appetite suppression feels different from nausea-driven food avoidance. The medication is designed to reduce desire for food, not make food repulsive. If you are experiencing significant fatigue or constant nausea, talk to your healthcare provider about managing these side effects while the medication builds in your system.
Weeks 2 to 4: building momentum
This is where things get interesting for most people. As semaglutide concentrations stabilize and you begin dose titration to 0.5 mg at week four, appetite suppression becomes more consistent and more noticeable. The research shows that steady-state blood levels take approximately four to five weeks of consistent dosing to achieve. Each weekly injection adds to the cumulative concentration in your bloodstream.
During this period, most users report feeling fuller faster at meals, reduced cravings especially for high-calorie foods, decreased portion sizes of 20 to 30 percent compared to baseline, less frequent thoughts about food between meals, and an easier time saying no to foods they would normally find irresistible.
The clinical data supports this timeline. A study published in Diabetes, Obesity and Metabolism found that semaglutide reduced ad libitum energy intake by approximately 24 percent compared to placebo, with effects becoming measurable within the first four weeks. By week 12, the reduction in energy intake reached approximately 35 percent.
If you are on compounded semaglutide, the timeline may differ slightly depending on the specific formulation and concentration, but the general pattern of gradual onset holds true across all forms of the medication.
Weeks 4 to 8: the inflection point
Most users identify this period as when appetite suppression becomes unmistakable. You are now on 0.5 mg or transitioning to 1.0 mg, and the medication has had time to fully integrate with your neural appetite circuits. The effects are no longer subtle.
Food noise goes from quieter to genuinely silent for many people. Meals become a conscious decision rather than an impulse. Some users describe forgetting to eat entirely, something they never imagined possible before starting the medication. The change in relationship with food feels fundamental rather than surface-level.
This is also the period where measurable weight loss begins accelerating. When appetite suppression becomes reliable, the calorie deficit it creates becomes consistent, and consistent deficits produce visible results. Most people lose 2 to 4 percent of body weight in the first eight weeks.
Weeks 8 to 16: full therapeutic effect
By this point, you are approaching or have reached the maintenance dose of 1.7 mg or 2.4 mg. Appetite suppression is at or near its peak. The STEP 1 clinical trial demonstrated that participants on semaglutide 2.4 mg experienced a 35 percent reduction in energy intake compared to placebo, with these effects stabilizing around week 12 to 16 of treatment.
At full therapeutic doses, semaglutide users consistently report eating 500 to 1,000 fewer calories per day compared to their pre-medication baseline. That reduction is not driven by willpower or restriction. It is driven by genuinely reduced hunger and increased satiety after smaller meals.
For context on dosing calculations during this phase, the semaglutide dosage calculator can help you understand the relationship between your dose in milligrams and units on your syringe, especially if you are using semaglutide measured in units rather than milligrams.
Month 4 and beyond: sustained suppression
Long-term data from the STEP 5 trial, which followed participants for 104 weeks, confirms that appetite suppression remains stable on maintenance dosing. The medication does not lose effectiveness over time for most users. At the two-year mark, 77.1 percent of semaglutide users had lost at least 5 percent of baseline body weight, compared to 34.4 percent of those on placebo.
The sustained nature of semaglutide appetite suppression distinguishes it from many previous weight loss medications where tolerance developed quickly. The GLP-1 receptor signaling pathway appears to maintain its effectiveness with continued stimulation, provided the dose remains consistent.
The dose titration factor: why starting low matters
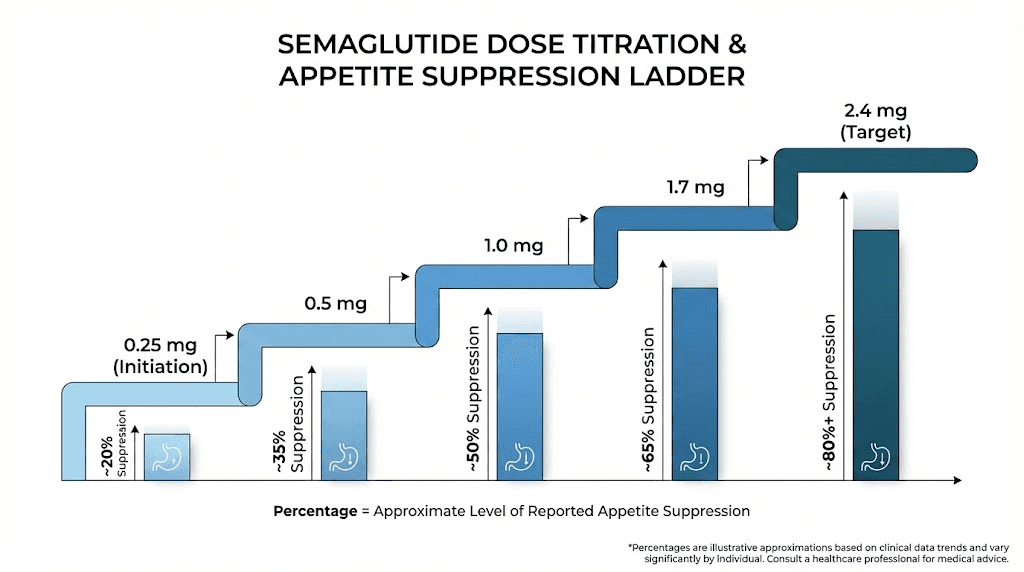
One of the biggest misconceptions about semaglutide and appetite is that the starting dose should produce the full effect. It should not. The 0.25 mg starting dose is approximately 10 percent of the maximum therapeutic dose of 2.4 mg. Expecting full appetite suppression at 0.25 mg is like expecting a whisper to fill a stadium.
The standard titration schedule
The prescribed dose escalation follows a specific pattern designed to balance effectiveness against side effects. Understanding where you are in this schedule helps explain why your appetite suppression may feel incomplete.
Weeks 1 to 4: 0.25 mg weekly. This is the adaptation phase. Minimal appetite suppression for most people. Your body is learning to process the medication without overwhelming your digestive system. The primary goal here is tolerability, not results.
Weeks 5 to 8: 0.5 mg weekly. Doubling the dose produces the first noticeable effects for most users. This is when many people first experience reliable appetite reduction. Your semaglutide dose in units has increased enough to cross the threshold of perceptible change.
Weeks 9 to 12: 1.0 mg weekly. Another doubling. Appetite suppression becomes consistent and measurable for the majority of users. Calorie intake reductions of 20 to 30 percent are typical at this dose level. Weight loss begins accelerating noticeably.
Weeks 13 to 16: 1.7 mg weekly. Getting close to maximum therapeutic dose. Appetite suppression is strong and reliable. Most users report significant changes in eating patterns, food preferences, and hunger levels by this point.
Week 17 onward: 2.4 mg weekly (maintenance). Full therapeutic dose. Maximum appetite suppression achieved. The STEP trials documented the most robust effects at this dose level. This is where the 35 percent reduction in energy intake and the silencing of food noise reach their peak.
Every step in this schedule matters. Jumping to higher doses too quickly increases nausea, vomiting, and other GI side effects without meaningfully improving appetite suppression speed. The gradual approach actually gets you to effective suppression faster by keeping you on the medication rather than stopping due to intolerable side effects.
Why some people feel it faster than others
Not everyone follows the textbook timeline. Some people report dramatic appetite changes within days. Others wait months. The variation is real, documented in clinical trials, and has specific biological explanations.
Metabolic rate and body composition
Your baseline metabolism affects how quickly semaglutide reaches effective concentrations. People with higher lean muscle mass relative to body fat tend to metabolize medications differently than those with higher body fat percentages. Semaglutide distributes into tissues based on blood flow and receptor density, which varies between individuals.
Body weight itself matters too. A 0.25 mg dose in someone weighing 150 pounds represents a different concentration per kilogram than the same dose in someone weighing 300 pounds. While the titration schedule is the same for everyone, the effective concentration reaching your brain receptors may be proportionally lower in larger individuals during early dosing.
GLP-1 receptor sensitivity
Just as pain receptors vary in sensitivity between people, GLP-1 receptors show natural variation. Some individuals have receptors that respond strongly to even small amounts of semaglutide, producing noticeable appetite changes at the 0.25 mg starting dose. Others have receptors that require higher concentrations before producing perceptible effects.
This is not a defect. It is normal biological variation. Someone who does not feel appetite suppression at 0.25 mg is not broken or a non-responder. They may simply need higher doses to activate their specific receptor configuration, which is exactly what the titration schedule provides.
Prior dieting history
Your history with calorie restriction, yo-yo dieting, and weight cycling can affect how quickly you perceive appetite changes. People who have been chronically restricting calories often have upregulated hunger hormones, particularly ghrelin. Their bodies have been fighting against reduced food intake for years. Semaglutide needs to overcome this hormonal resistance before appetite suppression becomes obvious.
Conversely, people who have been eating intuitively without chronic dieting sometimes notice appetite changes more quickly because their hunger signaling is already calibrated normally. The medication does not have to fight against years of compensatory hormonal adaptation.
Gut microbiome composition
Emerging research suggests that the composition of your gut bacteria influences how you respond to GLP-1 medications. Certain bacterial populations affect local GLP-1 production and sensitivity, which in turn influences how your body responds to synthetic GLP-1 analogs like semaglutide. While this research is still early, it may explain some of the individual variation in response timing.
Psychological factors
Expectation shapes perception. People who expect immediate dramatic results may not notice subtle early changes because they are looking for a sledgehammer when the medication delivers a gentle nudge. People with moderate expectations are more likely to notice and appreciate the gradual shift in appetite that begins early in treatment.
Stress and sleep quality also play enormous roles. High cortisol levels from chronic stress actively oppose appetite suppression by driving hunger signals that can overpower the medication effects. Poor sleep disrupts hunger hormones like leptin and ghrelin, making it harder for semaglutide to establish appetite control. If you are not seeing results on semaglutide, these lifestyle factors deserve examination before assuming the medication is not working.
The science of food noise and how semaglutide quiets it
One of the most profound effects users describe is not simply reduced hunger. It is the quieting of food noise. That constant mental chatter about food. What is for lunch? Is there chocolate in the house? When can I eat again? What sounds good right now? This relentless internal food dialogue affects millions of people, and its reduction is often the first sign that semaglutide is working.
What food noise actually is
Food noise is not hunger. It is obsessive preoccupation with eating that persists regardless of whether you are physically hungry. Neuroscientists describe it as hyperactivation of reward circuits related to food, particularly in the ventral tegmental area (VTA) and nucleus accumbens, brain regions that process pleasure and motivation.
For some people, food noise is quiet and manageable. For others, it dominates their waking hours, making it nearly impossible to focus on work, relationships, or anything beyond the next meal. Research published in Nature suggests that obesity is associated with altered dopamine signaling in these reward circuits, creating a self-reinforcing cycle of food preoccupation.
How semaglutide addresses food noise
Semaglutide reduces food noise through its effects on brain reward pathways. Specifically, it modulates dopamine signaling in the VTA and reduces the anticipatory reward associated with food. You still enjoy eating. Food still tastes good. But the desperate urgency, the inability to think about anything else, the compulsive planning of meals, these fade.
A study from the Pennington Biomedical Research Center found that semaglutide reduced reward-related brain activity in response to food images by approximately 30 percent. This neurological change is what users describe as "the noise going quiet" or "the switch flipping."
Critically, this food noise reduction often begins before obvious appetite suppression. Some people report quieter food thoughts within the first week, even at the starting dose, before they notice any change in actual hunger or portion sizes. The brain reward modulation appears to be more sensitive to low-dose semaglutide than the hypothalamic appetite circuits, creating a staged effect where mental preoccupation decreases first and physical hunger reduction follows.
What the clinical research actually shows
The STEP clinical trial program provides the most robust data available on semaglutide appetite suppression. These were large, randomized, placebo-controlled trials involving thousands of participants, and their findings consistently demonstrate the timeline we have been discussing.
STEP 1 trial findings
The landmark STEP 1 trial enrolled 1,961 adults with obesity or overweight plus at least one weight-related comorbidity. Participants received either semaglutide 2.4 mg or placebo for 68 weeks. The semaglutide group experienced mean weight loss of 14.9 percent compared to 2.4 percent for placebo, with 86 percent of the semaglutide group losing at least 5 percent of body weight.
More relevant to the appetite question, the study measured changes in eating behavior using validated questionnaires. Participants on semaglutide reported significantly improved control of eating, reduced food cravings, and decreased preference for high-fat foods. These changes emerged gradually over the first 12 to 16 weeks before stabilizing.
The appetite substudy data
A dedicated substudy examining semaglutide effects on appetite, energy intake, and food preference in subjects with obesity found that semaglutide reduced ad libitum energy intake by approximately 24 percent at week 12 compared to placebo. The reduction was driven by decreased fat and carbohydrate intake, while protein intake remained relatively preserved.
Participants also reported reduced hunger ratings of approximately 20 percent, increased fullness ratings of approximately 25 percent, and reduced desire to eat by approximately 20 percent. All measures showed progressive improvement from weeks 4 through 12, confirming the gradual onset pattern.
The gastric emptying study
A separate study by Friedrichsen and colleagues specifically measured semaglutide effects on gastric emptying and appetite in adults with obesity. They found that semaglutide 2.4 mg delayed gastric emptying by approximately 38 minutes compared to baseline, with effects present at the first measurement point and increasing over subsequent weeks.
This gastric delay contributed to a 35 percent reduction in energy intake during a standardized meal test, with participants reporting feeling full significantly faster and maintaining fullness for longer periods after eating. The combination of delayed gastric emptying and central appetite suppression created a synergistic effect greater than either mechanism alone.
Long-term STEP 5 data
The two-year STEP 5 trial demonstrated that appetite suppression remains stable over extended treatment. Participants maintained their reduced caloric intake and weight loss for the full 104 weeks without developing tolerance. At week 104, 61.8 percent of semaglutide users had lost 10 percent or more of baseline weight, and 36.1 percent had lost 20 percent or more.
This sustained efficacy over two years addresses one of the biggest concerns about long-term semaglutide use for appetite management. The medication does not appear to lose its appetite-suppressing effects with continued use, provided dosing remains consistent.
Comparing semaglutide appetite suppression with other GLP-1 medications
Semaglutide is not the only GLP-1 medication available, and understanding how its appetite effects compare with alternatives helps set appropriate expectations.
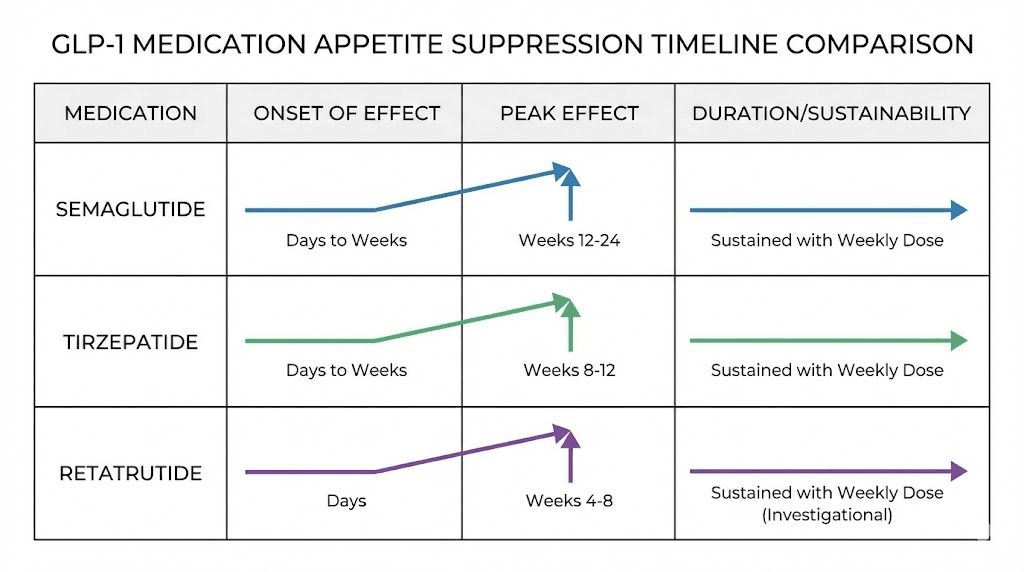
Semaglutide vs tirzepatide
Tirzepatide is a dual GIP/GLP-1 receptor agonist that targets an additional pathway beyond what semaglutide reaches. In head-to-head comparisons, tirzepatide has demonstrated greater weight loss, with the SURMOUNT-1 trial showing mean weight loss of 22.5 percent at the highest dose compared to semaglutide typical results of 14.9 percent.
Regarding appetite suppression speed, some users report faster onset with tirzepatide appetite suppression compared to semaglutide, potentially due to the additional GIP receptor activation. However, both medications follow the same general pattern of gradual onset with dose titration. If you are considering switching between the two, understanding the transition process is important for maintaining appetite control during the switch.
The dosage comparison between semaglutide and tirzepatide is not straightforward because they work through different receptor profiles. What matters for appetite suppression is reaching an effective concentration for your individual biology, which requires patience regardless of which medication you choose.
Semaglutide vs retatrutide
Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors. Early trial data suggests even greater appetite suppression and weight loss potential, with participants losing up to 24 percent of body weight in clinical trials. The glucagon receptor activation may accelerate the onset of appetite effects, though the medication is not yet widely available. If you are interested in this newer compound, understanding retatrutide dosing protocols can help you discuss options with your healthcare provider.
Oral semaglutide vs injectable
Semaglutide is available in both injectable and oral formulations. The oral form (brand name Rybelsus) reaches effective blood levels through a different absorption pathway, which can affect the timeline for appetite suppression. Oral semaglutide typically requires higher milligram doses to achieve similar blood concentrations as injectable forms, and the appetite effects may take slightly longer to become noticeable due to variable absorption.
What to do if semaglutide is not suppressing your appetite
You have been on semaglutide for a few weeks. Maybe a few months. And you are still hungry. Still thinking about food constantly. Still eating portions that feel unchanged. This is frustrating, but it is also more common than you might think, and it almost always has a solvable cause.
You have not given it enough time
This is the most common explanation, and it is the hardest to accept. If you are still in the first four weeks on the starting dose, you are not yet at a pharmacologically effective concentration for appetite suppression. Full steady-state levels take four to five weeks of consistent dosing to achieve, and meaningful appetite suppression typically requires higher doses than the 0.25 mg starting point.
Patience is not just a virtue here. It is a pharmacological necessity. The medication physically cannot produce its full effect until it has time to accumulate in your tissues and establish sustained receptor activation. If you have been on the medication for less than eight weeks and are still titrating up, the most likely answer is that you have not yet reached your effective dose.
Your dose needs adjustment
Not everyone responds at the same dose. Some people experience strong appetite suppression at 1.0 mg. Others need the full 2.4 mg to feel meaningful effects. If you have been at a particular dose for more than four weeks without noticeable appetite changes, discuss dose escalation with your prescriber.
This is especially relevant for people on compounded semaglutide, where concentration accuracy can vary between compounding pharmacies. If you suspect your compounded product is not delivering the expected dose, switching to a different pharmacy or formulation may help. Understanding the specific conversion between milligrams and units for your particular vial concentration ensures you are taking the correct dose.
Lifestyle factors are overriding the medication
Semaglutide is powerful, but it cannot overcome everything. Chronic sleep deprivation, high stress levels, and certain dietary patterns can actively oppose its appetite-suppressing effects.
Sleep deprivation increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone), creating a hormonal environment that fights against semaglutide signaling. Even one night of poor sleep can increase hunger by 20 to 30 percent the following day. Chronic poor sleep compounds this effect dramatically.
High stress elevates cortisol, which drives appetite through an entirely different pathway than the one semaglutide targets. Cortisol-driven hunger is particularly resistant to GLP-1-based suppression because it operates through stress-eating circuits rather than metabolic hunger circuits.
High-glycemic diets create blood sugar spikes and crashes that generate urgent hunger signals independent of the GLP-1 system. If you are eating refined carbohydrates and sugars at every meal, the glucose rollercoaster can partially override semaglutide appetite control. Following a semaglutide-compatible diet plan that emphasizes protein, fiber, and healthy fats can significantly enhance the medication appetite-suppressing effects.
Medical factors affecting response
Certain medical conditions can reduce semaglutide effectiveness for appetite suppression. Insulin resistance, thyroid disorders, PCOS, and certain medications (particularly antipsychotics, some antidepressants, and corticosteroids) can all counteract semaglutide appetite effects to varying degrees.
If you have been on an appropriate dose for an adequate duration, addressed sleep and stress, optimized your diet, and still experience minimal appetite suppression, discuss with your healthcare provider whether underlying medical conditions might be reducing your response. Blood work to check thyroid function, insulin levels, and cortisol can identify treatable factors.
You may need a different medication
Approximately 10 to 15 percent of semaglutide users are classified as low responders, experiencing significantly less appetite suppression and weight loss than the average participant in clinical trials. For these individuals, switching to a dual-agonist like tirzepatide or adding complementary approaches may produce better results.
Some healthcare providers also combine semaglutide with phentermine or other appetite-modulating medications for patients who respond partially. These combinations target different appetite pathways simultaneously, potentially overcoming resistance that a single medication cannot address alone.
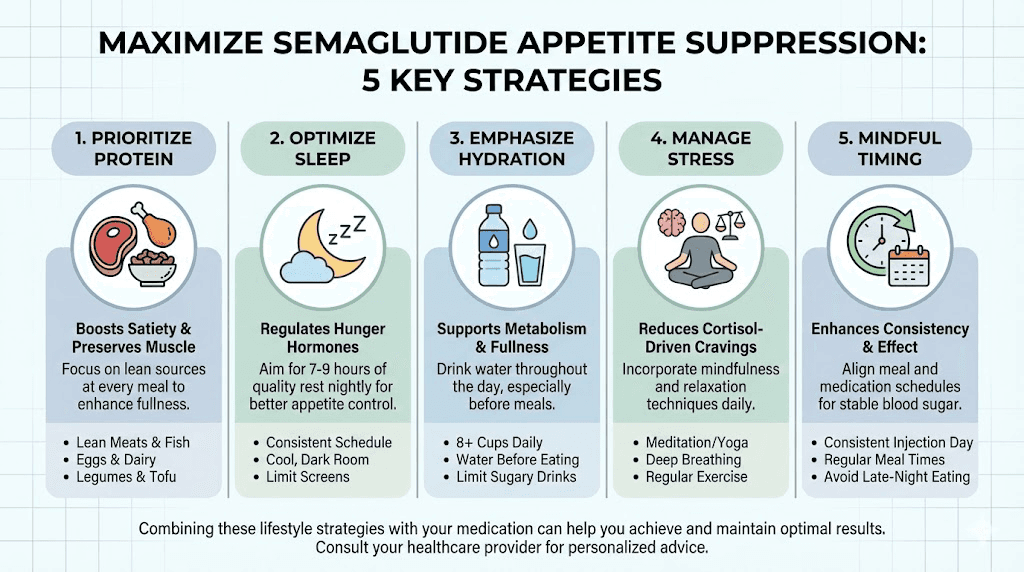
Maximizing semaglutide appetite suppression
While you cannot force semaglutide to work faster than pharmacology allows, you can create conditions that support and amplify its appetite effects. These strategies do not replace the medication. They work alongside it to enhance and accelerate results.
Protein-first eating
Protein is the most satiating macronutrient. When combined with semaglutide gastric emptying effects, high-protein meals produce remarkable levels of sustained fullness. Aim for 25 to 30 grams of protein at each meal. Start every meal with your protein source before moving to vegetables and then carbohydrates.
Research consistently shows that protein intake above 1.2 grams per kilogram of body weight preserves lean muscle mass during weight loss while enhancing satiety. This is especially important on semaglutide because the medication reduces overall calorie intake, and without adequate protein, some of that weight loss comes from muscle rather than fat.
Hydration strategy
Dehydration mimics hunger signals. Many people mistake thirst for appetite, eating when they actually need water. Aim for a minimum of 64 ounces of water daily, more if you are physically active. Drinking a full glass of water 20 to 30 minutes before meals enhances the fullness signal that semaglutide creates.
Some semaglutide users find that nausea and reduced appetite make it harder to drink adequate water. If this is the case, small frequent sips throughout the day work better than trying to drink large volumes at once. Electrolyte supplementation may also be necessary, especially during the first few weeks when GI side effects are most common.
Sleep optimization
Getting seven to nine hours of quality sleep per night is one of the most powerful appetite-regulating interventions available. Sleep deprivation does not just make you tired. It fundamentally disrupts the hormonal balance that semaglutide relies on to suppress appetite. Prioritize sleep as aggressively as you prioritize your injection schedule.
Stress management
Chronic stress actively opposes semaglutide appetite effects through cortisol-mediated pathways. Regular stress management practices, whether meditation, exercise, therapy, or simply reducing commitments, can measurably improve how effectively semaglutide suppresses your appetite.
Consistent injection timing
Taking semaglutide on the same day each week at approximately the same time maintains the most stable blood levels. Erratic dosing creates peaks and valleys in drug concentration, which can make appetite suppression feel inconsistent. The best time to take semaglutide is whatever time you will take it consistently, week after week.
Proper reconstitution and storage
If you are using compounded semaglutide that requires reconstitution, proper preparation is critical for effectiveness. Incorrectly mixed semaglutide may not deliver the expected dose, leading to reduced appetite suppression. Following precise reconstitution protocols and proper storage conditions ensures you are getting the full therapeutic benefit from each injection.
The role of semaglutide formulation in appetite suppression speed
Not all semaglutide is created equal when it comes to how quickly appetite effects appear. The specific formulation you are using, whether brand-name injectable, compounded injectable, or oral, can influence the timeline.
Brand-name injectable (Wegovy/Ozempic)
The pre-filled pens from Novo Nordisk deliver consistent, precise doses with optimal pharmacokinetics. The absorption profile from subcutaneous injection is well-characterized and predictable. When clinical trial timelines are discussed, they refer to these formulations. Appetite suppression timelines from clinical studies apply most directly to users of brand-name injectable semaglutide.
Compounded injectable semaglutide
Compounded semaglutide from compounding pharmacies uses the same active molecule but may differ in formulation characteristics that affect absorption. Some compounding pharmacies add ingredients like B12 or cyanocobalamin that do not affect semaglutide absorption but may provide additional benefits. Others use different concentrations that require careful reconstitution with bacteriostatic water.
The appetite suppression timeline for compounded semaglutide should be similar to brand-name versions, but inconsistencies in compounding quality can create variation. If your compounded semaglutide seems less effective than expected, the formulation itself may warrant investigation. Checking the concentration accuracy using the semaglutide mixing chart for your specific vial size can help verify that your doses are correct.
Oral semaglutide
Oral semaglutide (Rybelsus) has fundamentally different pharmacokinetics than injectable forms. Only about 1 percent of the oral dose is absorbed, which is why oral doses are measured in milligrams (3, 7, or 14 mg) compared to the microgram-equivalent injectable doses. The absorption is also affected by food, stomach acid, and timing relative to meals.
Appetite suppression from oral semaglutide may develop on a slightly different timeline than injectable, with some users reporting slower onset due to the variable absorption. However, the eventual appetite effects at therapeutic doses are comparable between oral and injectable formulations.
Sublingual semaglutide
Some providers offer sublingual (under the tongue) formulations of semaglutide, similar to sublingual peptide delivery systems. These bypass the digestive system for more predictable absorption than oral capsules but may not achieve the same blood levels as direct subcutaneous injection. The appetite suppression timeline for sublingual formulations is less well-studied in clinical trials.
Week-by-week appetite journal: what to track
Tracking your appetite changes objectively helps you recognize progress that might otherwise go unnoticed. Subjective feelings of hunger are hard to measure, but specific behaviors are not. Here is what to monitor each week.
Hunger intensity before meals
Rate your hunger on a 1 to 10 scale before each meal. A score of 1 means no hunger at all, 10 means ravenous. Over the first 8 to 12 weeks, you should see a gradual decrease in pre-meal hunger scores. This happens so slowly that you will not notice it without tracking. Looking back at four weeks of data reveals patterns your daily experience obscures.
Portion sizes
Photograph your plate before eating for the first few weeks, then again every month. Visual comparison over time is one of the most powerful ways to see appetite suppression in action. Most people are surprised by how much their portions have decreased when they compare month one to month three.
Snacking frequency
Count how many times per day you eat outside of planned meals. Snacking frequency typically decreases before meal portion sizes do, making it an early indicator of appetite suppression. If you notice yourself skipping your usual 3pm snack without thinking about it, the medication is working even if you are not yet eating less at dinner.
Food noise levels
Rate your food preoccupation daily on a 1 to 10 scale. How much time did you spend thinking about food outside of mealtimes? This metric often shows improvement before any other measure, sometimes within the first week. The quieting of food noise is one of the earliest and most reliable signs that semaglutide is beginning to modulate your appetite circuits.
Cravings
Note specific cravings and their intensity. Semaglutide tends to reduce cravings for high-fat and high-calorie foods preferentially over other food categories. If you notice that your usual craving for ice cream at 9pm has faded from a 9 out of 10 to a 4 out of 10, that is meaningful progress even if your overall hunger feels unchanged.
Semaglutide appetite suppression and exercise
Physical activity interacts with semaglutide appetite effects in complex and sometimes counterintuitive ways. Understanding this interaction helps you optimize both your exercise routine and your medication results.
Acute exercise effects
Moderate-intensity exercise temporarily suppresses appetite through a mechanism separate from semaglutide. The combination of exercise-induced appetite suppression and semaglutide-induced appetite suppression can create periods of very low hunger, particularly in the hours following a workout. Some users report finding it difficult to eat enough after exercising on semaglutide.
This is a double-edged sword. While reduced appetite supports weight loss, excessively low calorie intake impairs muscle preservation and recovery. If you are exercising regularly on semaglutide, consciously prioritizing post-workout nutrition, even when you are not hungry, helps maintain muscle mass and exercise performance.
Resistance training considerations
Resistance training is particularly important for semaglutide users because it signals your body to preserve lean muscle during weight loss. Without strength training, approximately 25 to 40 percent of weight lost on semaglutide comes from lean mass rather than fat. With regular resistance training, this can be reduced to 10 to 20 percent.
The appetite effects of semaglutide can make it challenging to consume enough protein and calories to support muscle growth. Some users benefit from peptides that support muscle preservation alongside their semaglutide protocol, though this should be discussed with a healthcare provider.
Endurance exercise
Long-duration cardio increases calorie expenditure and can amplify semaglutide weight loss effects. However, extended exercise sessions also trigger hunger hormone responses that may temporarily override semaglutide appetite suppression. Finding the balance between exercise volume and appetite management is individual and may require experimentation.
Common myths about semaglutide and immediate appetite suppression
Misinformation about semaglutide spreads quickly online. Separating fact from fiction helps you maintain realistic expectations and avoid premature discouragement.
Myth: the first injection kills your appetite completely
Reality: The starting dose is one-tenth of the therapeutic dose. Complete appetite elimination at 0.25 mg would actually be a concerning sign of excessive sensitivity, not a positive outcome. Gradual onset is by design.
Myth: if you do not feel it in week one, it will not work for you
Reality: Clinical trials show that non-responders cannot be identified during the first four weeks of treatment. Many eventual strong responders notice nothing during the initial titration period. Judging medication effectiveness before reaching at least 1.0 mg and maintaining it for four weeks is premature.
Myth: appetite suppression should be constant and complete
Reality: Even at therapeutic doses, semaglutide reduces appetite. It does not eliminate it. You will still experience hunger, especially before meals. The difference is that hunger feels manageable, meals satisfy more quickly, and the obsessive preoccupation with food diminishes. If someone tells you they never feel hungry on semaglutide, they are likely confusing nausea with appetite suppression or exaggerating their experience.
Myth: you should feel nauseous for the medication to be working
Reality: Nausea is a side effect, not an indicator of efficacy. Many people achieve excellent appetite suppression with minimal or no nausea. Others experience significant nausea without proportionate appetite reduction. The two effects are related but not equivalent. Nausea-driven food avoidance is not the same as therapeutic appetite suppression.
Myth: compounded semaglutide works differently than brand-name
Reality: The active molecule is the same. While compounded formulations may vary in quality between pharmacies, properly compounded semaglutide produces the same pharmacological effects as brand-name versions. The timeline for appetite suppression should be equivalent when the medication is correctly prepared and dosed.
Myth: you can speed up appetite suppression by taking higher doses faster
Reality: Accelerating the titration schedule increases side effects without meaningfully speeding up the establishment of appetite suppression. The gradual approach allows your GLP-1 receptors and digestive system to adapt, actually producing more stable and sustainable appetite control than rapid dose escalation.
Semaglutide appetite suppression and specific populations
Different populations may experience appetite suppression on different timelines or with different characteristics. Understanding these variations prevents unnecessary concern if your experience differs from the average.
People with type 2 diabetes
Semaglutide was first approved for diabetes management, and people with type 2 diabetes may experience appetite effects differently due to their underlying metabolic condition. Insulin resistance can affect GLP-1 receptor sensitivity, potentially slowing the onset of appetite suppression. However, the blood sugar stabilization effects of semaglutide often reduce glucose-driven hunger relatively quickly, even before full appetite suppression develops.
Women vs men
Hormonal differences between women and men can influence semaglutide appetite effects. Women often experience cyclical variation in appetite related to menstrual cycles, which can make semaglutide effects harder to detect consistently. Some women over 40 report that hormonal changes during perimenopause affect their response to GLP-1 medications, though clinical trial data shows comparable overall weight loss between sexes.
People on multiple medications
Drug interactions can affect semaglutide appetite effects. Medications that increase appetite (certain antidepressants, antipsychotics, corticosteroids) can partially counteract semaglutide appetite suppression. If you are taking medications known to increase appetite, discuss with your prescriber whether adjustments might be appropriate.
Additionally, the delayed gastric emptying caused by semaglutide can affect the absorption of other oral medications. This is primarily a timing consideration rather than an appetite issue, but it is worth discussing with your healthcare provider to ensure all your medications are working optimally.
People with a history of eating disorders
Semaglutide appetite suppression in individuals with binge eating disorder or other eating disorders requires careful medical supervision. The medication can be beneficial by reducing binge urges and food preoccupation, but the powerful appetite effects may also interact unpredictably with disordered eating patterns. This is a population where medical monitoring is especially important.
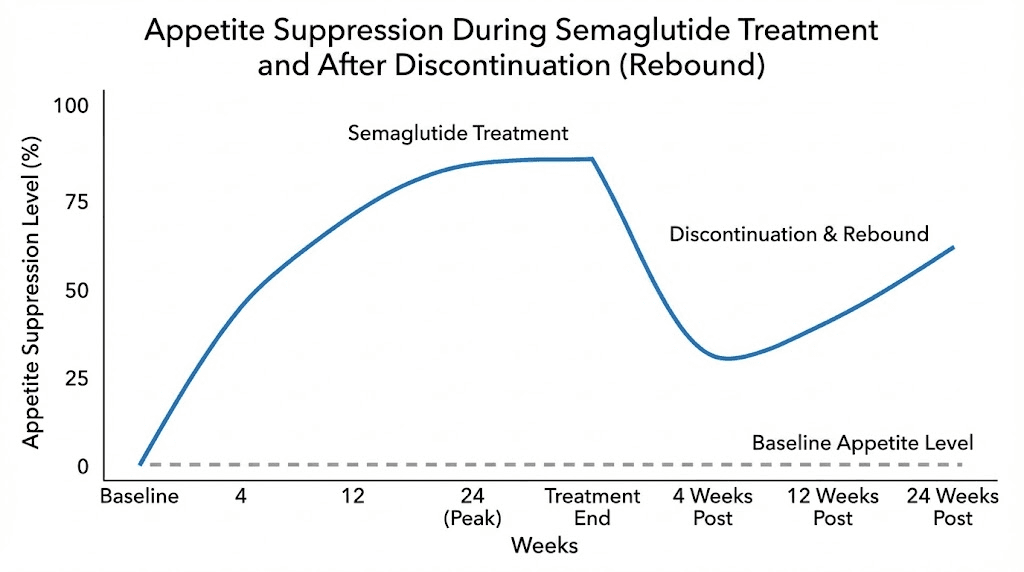
What happens to appetite if you stop semaglutide
Understanding the durability of appetite effects after discontinuation is important for long-term planning. The research here is clear and sobering.
The return of appetite
When semaglutide is discontinued, appetite returns to near-baseline levels within two to four weeks. The medication does not permanently rewire your appetite circuits. It suppresses them for as long as it is present in your system. Once blood concentrations decline below effective levels, hunger signals rebound.
The STEP 4 trial specifically examined this question. Participants who switched from semaglutide to placebo after 20 weeks regained approximately two-thirds of their lost weight over the following 48 weeks, driven largely by the return of pre-treatment appetite levels.
This is why understanding what happens when you stop semaglutide is critical for making informed decisions about treatment duration. The appetite suppression is real and powerful, but it is medication-dependent.
Strategies for managing appetite after discontinuation
For people who eventually stop semaglutide, behavioral and dietary habits established during treatment can partially buffer the return of appetite. Protein-prioritized eating, regular meal timing, sleep optimization, and stress management all contribute to appetite regulation independent of medication. Building these habits while semaglutide makes appetite management easier creates a foundation that persists after discontinuation.
Some healthcare providers recommend gradual dose reduction rather than abrupt discontinuation, allowing the body to adjust to decreasing levels of GLP-1 stimulation. This approach may ease the transition and reduce the shock of appetite rebound, though it is not yet supported by formal clinical trial data.
Combining semaglutide with other appetite-supporting approaches
Semaglutide works best as part of a comprehensive approach rather than as a standalone solution. Several evidence-based strategies complement its appetite effects.
Dietary fiber
Soluble fiber creates a gel-like substance in your stomach that slows digestion, amplifying semaglutide gastric emptying effects. Aim for 25 to 35 grams of fiber daily from whole food sources. Vegetables, legumes, oats, and berries are excellent sources that pair well with the protein-first eating strategy.
Mindful eating practices
Semaglutide reduces hunger, but it does not automatically change eating habits. Mindful eating practices, including eating slowly, chewing thoroughly, and paying attention to fullness signals, help you recognize and respond to the satiety signals that semaglutide amplifies. Many users find that combining semaglutide with mindful eating produces greater appetite control than either approach alone.
Behavioral therapy
Cognitive behavioral therapy focused on eating behaviors can address psychological drivers of overeating that semaglutide does not directly target. Emotional eating, stress eating, and habitual eating patterns have psychological components that benefit from therapeutic intervention alongside pharmacological appetite suppression.
Supplements and additional peptides
Some users explore complementary approaches alongside semaglutide. Adding glycine to semaglutide has gained attention for its potential to support metabolic health. The combination of semaglutide with vitamin B12 is commonly offered by compounding pharmacies to address potential nutrient deficiencies during reduced caloric intake.
For those exploring the broader peptide landscape, understanding what peptides are and how they work provides context for these complementary approaches. The peptide calculator and other tools at SeekPeptides can help with dosing calculations for various protocols.
Frequently asked questions
Does semaglutide suppress appetite on the first day?
Semaglutide begins working in your body within hours of the first injection, but most people do not notice obvious appetite suppression on day one. The starting dose of 0.25 mg is intentionally low, and while the medication starts binding to GLP-1 receptors immediately, perceptible appetite reduction typically takes one to four weeks to develop. Some people report subtle changes like reduced food noise within the first few days, but these are mild and easy to miss.
How long does it take for semaglutide to fully suppress appetite?
Full appetite suppression develops over 8 to 16 weeks as you titrate through increasing doses. The medication reaches steady-state blood levels after about four to five weeks at each dose, and most people experience peak appetite suppression at the maintenance dose of 1.7 to 2.4 mg. Clinical trials show that energy intake reductions stabilize around week 12 to 16 at approximately 35 percent below baseline.
Will I feel hungry at all on semaglutide?
Yes. Semaglutide reduces appetite significantly but does not eliminate hunger entirely. You will still experience normal hunger before meals, which is healthy and expected. What changes is the intensity, the duration, and the urgency of hunger. Meals satisfy you more quickly, fullness lasts longer, and the obsessive thoughts about food between meals diminish substantially. If you are not seeing changes after four weeks, discuss dose adjustment with your provider.
Can I speed up semaglutide appetite suppression?
You cannot safely accelerate the dose titration beyond the prescribed schedule. However, you can optimize the conditions for appetite suppression by prioritizing sleep (7 to 9 hours), managing stress, eating protein-rich meals (25 to 30 grams per meal), staying well hydrated, and exercising regularly. These lifestyle factors amplify semaglutide effects and may help you notice appetite changes earlier in treatment.
Why does semaglutide suppress some people appetite faster than others?
Individual variation in response timing depends on metabolism, body composition, GLP-1 receptor sensitivity, prior dieting history, stress levels, sleep quality, and concurrent medications. People with faster metabolisms and lower body fat percentages tend to reach effective blood concentrations sooner. Those with chronic stress, poor sleep, or appetite-increasing medications may experience delayed onset.
Is nausea a sign that semaglutide is suppressing my appetite?
Nausea and appetite suppression are related but separate effects. Nausea comes from the GI effects of semaglutide (primarily delayed gastric emptying), while true appetite suppression involves central brain signaling. You can have appetite suppression without nausea and nausea without appetite suppression. Many people who achieve excellent long-term appetite control experience minimal nausea beyond the first few weeks of treatment.
What if semaglutide stops suppressing my appetite over time?
Long-term clinical trial data (STEP 5, 104 weeks) shows that semaglutide maintains its appetite-suppressing effects over at least two years of continuous use. If you feel the appetite effects diminishing, common causes include metabolic adaptation, increased stress, worsening sleep, or changes in diet quality. True pharmacological tolerance to semaglutide appetite effects has not been demonstrated in clinical research.
Does the form of semaglutide (injectable vs oral) affect how fast appetite suppression starts?
Injectable semaglutide (Wegovy, Ozempic, compounded) generally provides more predictable and potentially faster appetite effects than oral semaglutide (Rybelsus). This is because injectable forms achieve more consistent blood levels due to complete absorption from the injection site, while oral forms have approximately 1 percent bioavailability with variable absorption affected by food, stomach acid, and timing.
External resources
For researchers serious about understanding and optimizing their weight management protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized protocol tools, and a community of thousands who have navigated these exact questions about semaglutide appetite suppression and beyond.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay manageable, your doses stay consistent, and your patience stay rewarded.