Feb 20, 2026

Some researchers see dramatic appetite suppression within hours. Others barely notice a change all week. The difference often comes down to one overlooked variable: when they take their shot.
Timing is not everything. But it is close. The pharmacokinetics of GLP-1 receptor agonists create windows of peak activity, troughs of reduced effect, and transition periods where side effects hit hardest. Understanding these windows, and aligning your injection schedule with your daily routine, can mean the difference between a protocol that feels seamless and one that leaves you nauseated on the couch every Wednesday evening.
Here is the thing most guides will not tell you. There is no single "best" time to take a GLP-1 shot that works for everyone. Clinical trials have not established a definitive optimal hour. The FDA labeling for most GLP-1 receptor agonists simply says "any time of day." But that does not mean timing is irrelevant. One small crossover trial found that morning semaglutide injections before 8am produced roughly 15% lower post-prandial glucose compared to evening doses after 8pm. That margin matters when you are trying to optimize results.
This guide breaks down everything researchers need to know about GLP-1 injection timing. We will cover morning versus evening dosing, the pharmacokinetics behind each medication, which day of the week to choose, how injection site affects absorption speed, and the specific timing protocols for semaglutide, tirzepatide, liraglutide, dulaglutide, and retatrutide. We will also cover the missed dose rules that prevent dangerous doubling, and the common timing mistakes that sabotage otherwise solid protocols. SeekPeptides has compiled the most thorough breakdown available, pulling from clinical data, pharmacokinetic studies, and thousands of real-world researcher experiences.
The consistency principle
Before we get into the specifics, one rule supersedes everything else: consistency beats optimization. Taking your GLP-1 injection at the same time every week (or every day, for daily formulations) matters more than choosing the theoretically perfect hour. Your body adapts to a predictable schedule. Receptors upregulate and downregulate in rhythm with expected drug levels. Side effects become more predictable. And you are far less likely to forget a dose when it is tied to a fixed routine.
That said, if you have not yet established a routine, or if you are struggling with side effects on your current schedule, the information in this guide can help you choose the timing that gives you the best possible experience.
What the clinical data actually says
Most GLP-1 receptor agonist prescribing information does not specify a preferred time of day. The label says "any time of day, with or without meals" for injectable formulations. But "any time" does not mean "all times are equal." It means the manufacturer did not find a statistically significant difference in primary endpoints based on timing in their pivotal trials.
The nuance lies in secondary outcomes and real-world experience. Side effect profiles shift depending on when you inject. Appetite suppression peaks align differently with meal patterns. And the psychological impact of timing, knowing when to expect effects and when they will fade, shapes adherence more than most people realize. Understanding how GLP-1 medications work in practice requires looking beyond the label.
Morning GLP-1 injections: the case for early dosing
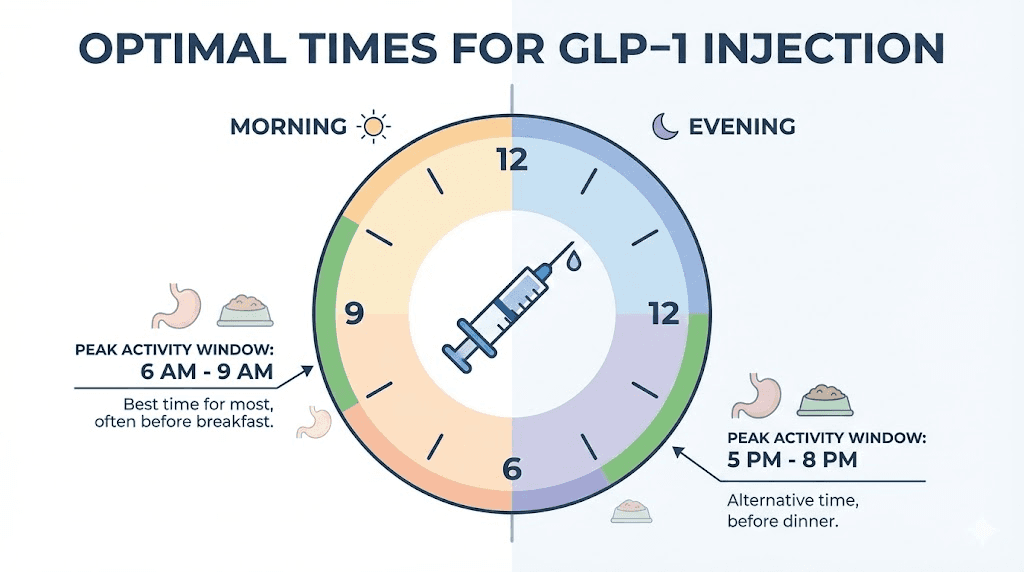
Morning injections have become the most popular choice among GLP-1 users, and for good reason. The logic is straightforward. You inject first thing, appetite suppression builds throughout the day when you need it most, and by the time peak nausea hits a few hours later, you are upright and active rather than trying to sleep through discomfort.
Blood sugar control advantages
One small but noteworthy crossover study compared morning versus evening semaglutide dosing and found approximately 15% lower post-prandial glucose levels with pre-8am administration. The mechanism makes physiological sense. GLP-1 receptor agonists enhance glucose-dependent insulin secretion and suppress glucagon. When these effects align with your first meals of the day, when insulin sensitivity is naturally highest, you get a compounding benefit.
Morning dosing also aligns with the body natural cortisol rhythm. Cortisol peaks in the early morning hours, promoting glucose production. A GLP-1 agonist administered during this window helps counteract the cortisol-driven glucose rise, potentially offering tighter glycemic control through the most metabolically active part of your day.
Appetite suppression alignment
This is where morning injections really shine for weight management. Most people struggle with eating decisions between noon and 8pm. That is when cravings hit hardest, social meals happen, and willpower erodes. A morning injection means appetite suppression kicks in right when you need it.
For weekly formulations like semaglutide and tirzepatide, the peak plasma concentration arrives 1 to 3 days after injection. A Monday morning shot means you are hitting peak suppression by Tuesday or Wednesday, carrying strong effects through the typical workweek when structured eating is easiest. By the weekend, levels are still therapeutic but slightly lower, which some researchers actually prefer since it allows for more flexible social eating.
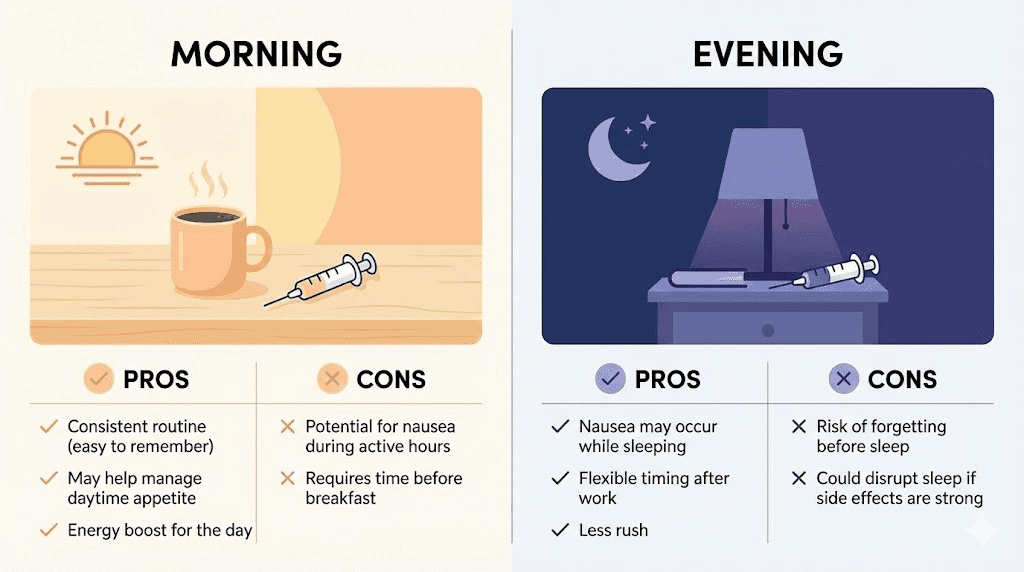
The morning routine advantage
Adherence research consistently shows that medications tied to morning routines have higher compliance rates. You wake up. You inject. It is done for the week. There is no evening decision fatigue, no "I will do it after dinner" that turns into "I forgot." Researchers who track their protocols using tools like the GLP-1 plotter consistently report better adherence with morning scheduling.
Simple. Reliable. Consistent.
Potential morning downsides
Morning injection is not without trade-offs. Nausea from GLP-1 agonists typically peaks 1 to 3 hours after injection. If you inject at 7am, that means potential nausea hitting between 8am and 10am, right when you are commuting, starting work, or sitting in meetings. For some people, this is manageable. For others, especially during dose escalation phases when side effects are strongest, morning nausea can be disruptive.
There is also the food factor. Some researchers report that injecting on a completely empty stomach intensifies initial nausea. A light breakfast 30 to 60 minutes before or after injection can buffer this effect, but that requires planning your morning around the shot rather than the other way around.
Evening GLP-1 injections: the case for nighttime dosing
Evening dosing has a dedicated following, and the reasoning is surprisingly compelling. About 60% of GLP-1 users who experience gastrointestinal side effects report that nighttime injection significantly reduces their perception of nausea, simply because they sleep through the worst of it.
Sleep through the side effects
This is the single strongest argument for evening injection. GI side effects affect 10% to 40% of GLP-1 users, particularly during the first few weeks and during each dose escalation. Nausea, burping, and general stomach discomfort peak within 1 to 3 hours of injection. If you inject at 9pm, you are asleep by the time the worst hits. You wake up feeling fine, or at least much better than you would have felt riding out those hours while conscious.
For researchers dealing with constipation from GLP-1 medications, evening dosing can also be beneficial. The medication works on gastrointestinal motility overnight, and some users find that morning bowel function improves with nighttime administration.
Reduced disruption to daily activities
Consider the practical reality. You have meetings. Calls. A commute. Children to manage. Meals to prepare. An exercise routine. Injecting in the evening, after the day is essentially done, means the medication does its initial work without interfering with any of these activities. The potential for GLP-1 related fatigue also hits while you are already winding down, rather than derailing your productivity.
Next-day appetite control
Evening injection means you wake up with the medication already circulating at meaningful levels. There is no waiting for it to kick in. Breakfast decisions are already influenced by the drug. For researchers who find mornings to be their most vulnerable time for overeating, or who tend to skip breakfast entirely when on GLP-1 therapy, this timing can feel more natural.
The peak concentration from a weekly injection given on, say, Thursday evening would arrive Friday evening through Saturday. Some researchers prefer this alignment because it gives them maximum appetite control heading into the weekend, when social meals and less structured eating become more common.
Potential evening downsides
The biggest risk with evening dosing is forgetting. After a long day, executive function is lower. You are tired. It is easy to fall asleep without remembering your injection. Unlike morning dosing, which gets built into the start-of-day routine, evening dosing competes with relaxation, family time, and simple exhaustion.
There is also a potential sleep disruption angle, though this varies enormously between individuals. Some users report that GLP-1 injections cause mild stomach discomfort that wakes them at 2am or 3am. Others sleep through without issue. If you are prone to sleep disturbances on GLP-1 therapy, evening injection might worsen the problem rather than solve it.
How GLP-1 pharmacokinetics shape your timing decision
Understanding why timing matters requires understanding how these medications move through your body. Every GLP-1 receptor agonist has a distinct pharmacokinetic profile, and these differences fundamentally shape how timing affects your experience.
Semaglutide pharmacokinetics
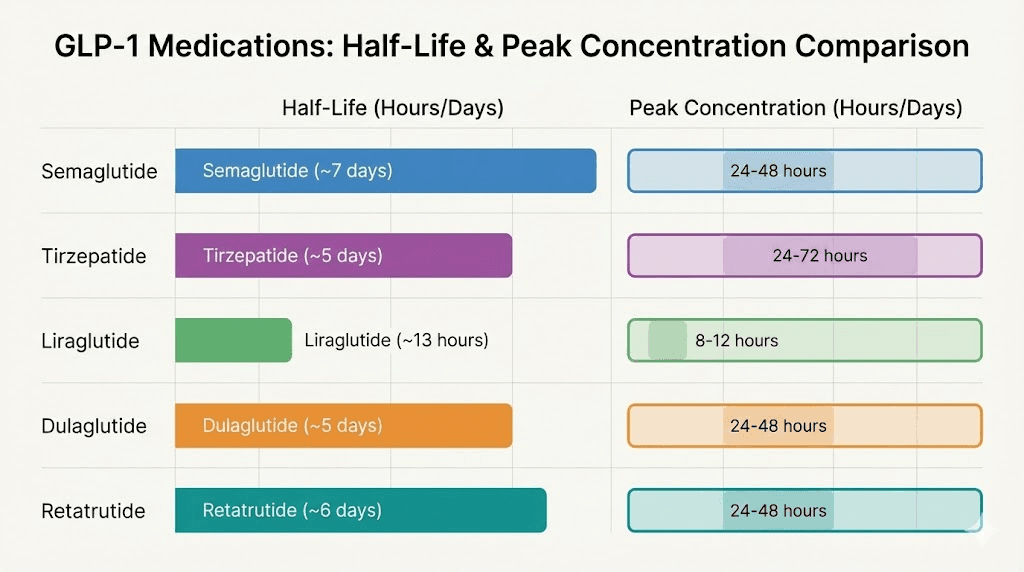
Injectable semaglutide has a half-life of approximately 7 days, or 165 to 184 hours. After subcutaneous injection, it reaches peak plasma concentration (Tmax) in 1 to 3 days. This long half-life is what makes weekly dosing possible. It also means that the exact hour of injection matters less than it would for a short-acting drug.
But "matters less" does not mean "does not matter at all." The initial 24 to 72 hours after injection represent a distinct pharmacokinetic phase where drug levels are rising rapidly. Side effects concentrate in this window. Appetite suppression tends to feel strongest during this ramp-up. And the body response to food, exercise, and stress can shift noticeably. Researchers who track their semaglutide results over time often identify clear patterns in how they feel during this post-injection window versus the latter half of the week.
By day 5, 6, and 7, semaglutide levels are declining but still therapeutic. Some researchers report increased hunger in these final days before their next injection. If this describes you, adjusting your injection day so that this trough period falls on days when your eating environment is most controlled (like structured workdays rather than weekends) can help considerably.
Tirzepatide pharmacokinetics
Tirzepatide has a shorter half-life than semaglutide, approximately 5 days or 120 hours. Peak concentration arrives between 8 and 72 hours post-injection, with most users hitting Tmax around 24 to 48 hours. This means the post-injection side effect window is somewhat compressed compared to semaglutide.
The dual GIP/GLP-1 mechanism of tirzepatide creates a slightly different side effect pattern. Some researchers find the nausea profile somewhat milder but the gastrointestinal effects more persistent. This has timing implications. Because the Tmax window is broader (8 to 72 hours), there is less precision in predicting exactly when peak effects will hit on any given week. Consistency in timing becomes even more important for establishing a predictable pattern you can plan around.
The shorter half-life also means the end-of-week trough is more pronounced with tirzepatide. Researchers using the tirzepatide dosage calculator to dial in their protocols often find that the difference between day 2 effects and day 6 effects is more noticeable than with semaglutide.
How half-life affects time-of-day decisions
Here is the key insight that most timing guides miss. For weekly formulations with multi-day half-lives, the exact hour of injection primarily affects two things: the acute post-injection experience (first 4 to 8 hours) and the day-to-day pattern of your weekly cycle. It does not dramatically change overall drug exposure or total weekly efficacy.
What this means practically is that your choice of morning versus evening should be driven by side effect management and routine compatibility, not by chasing marginally different blood levels. The 15% glucose improvement from morning dosing in that small crossover trial is real but modest. The quality-of-life improvement from sleeping through nausea, if you are someone who experiences significant GI effects, is massive by comparison.
Daily versus weekly formulation timing
The timing calculus changes completely for daily GLP-1 formulations like liraglutide. With a half-life of only 13 hours, liraglutide creates a much more pronounced peak-and-trough pattern within each 24-hour period. The time of day you inject directly affects when you experience maximum appetite suppression and when effects diminish.
For daily formulations, aligning injection time with your most challenging eating period makes intuitive and pharmacokinetic sense. If evenings are when you overeat, an afternoon injection puts peak levels at dinnertime. If mornings are problematic, an early injection provides maximal effect when you need it. We will cover specific medication protocols in detail later in this guide. For general injection guidance, see the linked protocol.
Best day of the week for your GLP-1 shot
For weekly formulations, the day you choose matters almost as much as the time. This is an underappreciated aspect of GLP-1 optimization, and getting it right can significantly improve your experience.
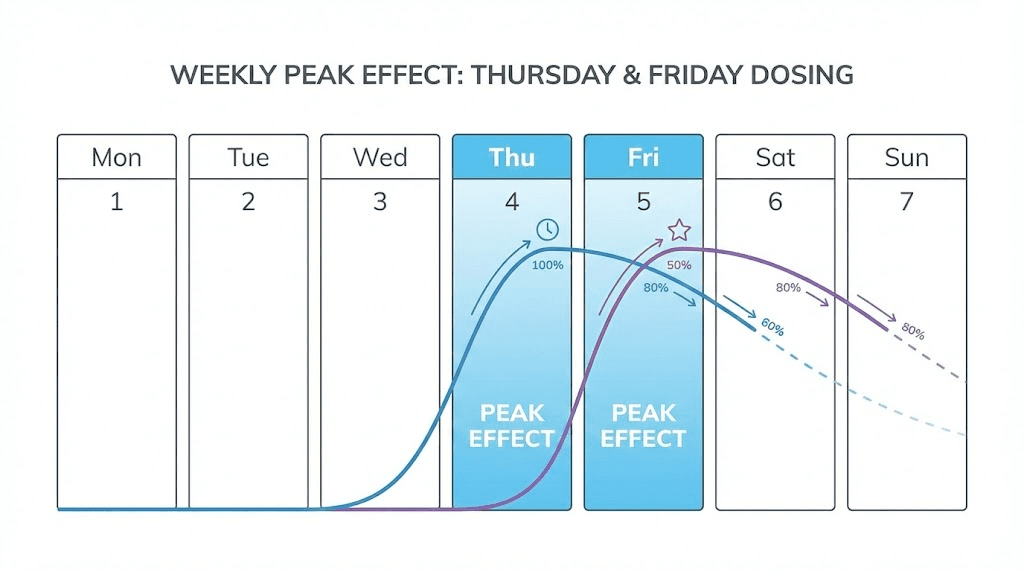
The Thursday/Friday strategy
Many experienced researchers gravitate toward Thursday or Friday injections, and the logic is sound. Here is why.
You inject Thursday evening. Peak effects arrive Friday through Saturday, giving you maximum appetite control heading into the weekend. Weekend meals tend to be less structured, more social, and higher in temptation. Having your strongest suppression aligned with this window provides a natural buffer against the dietary challenges that derail many people.
By Monday and Tuesday, drug levels are still solidly therapeutic but slightly lower. This coincides with the start of the workweek, when routines and structured meals make appetite management easier anyway. The natural trough aligns with the time when environmental factors are already working in your favor.
The side effect angle works too. If your injection causes nausea or fatigue in the first 24 hours, a Thursday evening injection means you ride out the worst on Friday evening and Saturday morning, when you have more flexibility to rest. Compare that to a Monday injection, where the nausea peak hits during Tuesday workday.
Matching your injection day to your lifestyle
The best injection day is the one that creates the least disruption and the most benefit. Consider these factors:
Factor | Best injection day | Why |
|---|---|---|
Weekend overeater | Thursday or Friday | Peak suppression covers Saturday and Sunday |
Heavy side effects | Friday evening | Nausea peaks Saturday, no work disruption |
Weekday lunch struggles | Sunday or Monday | Peak suppression covers Tuesday through Thursday |
Frequent traveler | Fixed day regardless | Consistency beats optimization when schedule shifts |
Active weekends | Monday or Tuesday | Fatigue hits during low-activity weekdays |
Whatever day you choose, the most important thing is keeping it consistent. Semaglutide takes time to build steady-state levels, and changing your injection day frequently undermines this process. Pick a day, commit to it for at least 4 to 6 weeks, and then evaluate whether it is working for your lifestyle.
Can you change your injection day?
Yes, but do it carefully. If you need to shift from, say, Tuesday to Friday, the standard guidance is to ensure at least 48 hours between your old and new injection time. So you would take your Tuesday shot, then wait until Friday (3 days later) for your next one. From there, Friday becomes your new injection day. Never take two doses less than 72 hours apart, regardless of the reason for the shift. If you are considering taking your injection early, make sure to understand the minimum spacing requirements first.
Timing your GLP-1 injection around meals
One of the most common questions researchers ask is whether they should time their injection relative to meals. The answer depends entirely on which formulation you are using.
Injectable GLP-1 agonists and meals
For subcutaneous injectable formulations, including semaglutide, tirzepatide, dulaglutide, and liraglutide, there is no requirement to time your injection around meals. The medication is absorbed through subcutaneous tissue, not the gastrointestinal tract. Food in your stomach does not affect absorption rate or bioavailability of an injected drug.
That said, some researchers find that injecting on a completely empty stomach intensifies the initial nausea. This is not a pharmacokinetic effect but rather a physiological one. GLP-1 agonists slow gastric emptying and reduce appetite. When there is nothing in the stomach to slow down, and GLP-1 signals are telling the brain "you are full," some people experience a wave of nausea that a small amount of food can help buffer.
The practical approach for many successful researchers: eat a light, protein-rich snack about 30 to 60 minutes before injection. Not a full meal. Just enough to have something in the stomach. This can reduce acute nausea without meaningfully affecting the medication pharmacokinetics. For guidance on what to eat, check out our resources on foods to eat while on semaglutide or the tirzepatide food guide.
Oral semaglutide: completely different rules
If you are using oral semaglutide rather than injectable, the timing rules change dramatically. Oral semaglutide must be taken on an empty stomach with no more than 4 ounces (120ml) of plain water. You then need to wait at least 30 minutes before eating, drinking, or taking other oral medications.
This is not a suggestion. It is a requirement. Food reduces the bioavailability of oral semaglutide by up to 40%. Even a small snack can dramatically reduce absorption. The medication uses a special absorption enhancer (SNAC) that only works effectively in a fasting state with minimal water volume.
For oral formulations, morning dosing makes the most practical sense. Take it first thing when you wake up, before coffee, before breakfast, before anything else. Set a timer for 30 minutes, then go about your morning routine. By the time 30 minutes pass, you can eat normally. Sublingual semaglutide follows similar absorption principles, though the delivery mechanism differs.
Meal timing and side effect management
Beyond the injection itself, how you time your meals in the days following injection can significantly affect your side effect experience. Here are the patterns that experienced researchers consistently report:
Smaller, more frequent meals in the 24 to 48 hours after injection help reduce nausea. Eating large, fatty meals during this window is a recipe for misery. The semaglutide diet plan and tirzepatide diet plan both address this in detail. Your stomach is already slowing down. Give it less to process at once.
Hydration matters enormously in the post-injection window. GLP-1 agonists can reduce thirst signals alongside appetite signals. Dehydration worsens nausea. Dehydration worsens constipation. Dehydration worsens fatigue. Set reminders to drink water, especially in the first 48 hours after injection.
Injection site and timing: does location affect absorption?
Where you inject your GLP-1 agonist affects how quickly the drug reaches peak plasma levels, which in turn affects the timing of both therapeutic effects and side effects. This is a detail that most timing guides completely ignore.
Absorption rates by injection site
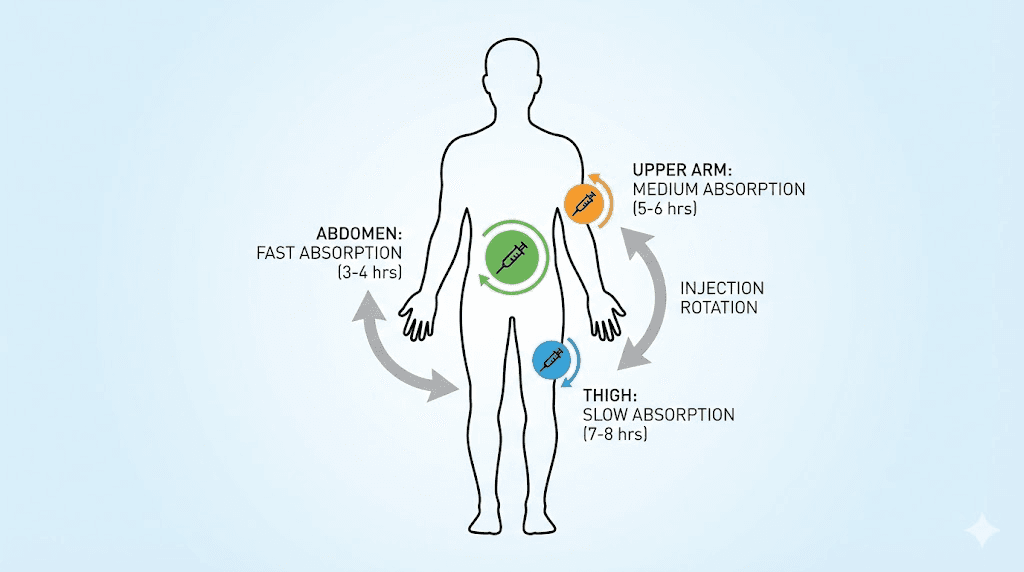
Three primary subcutaneous injection sites are used for GLP-1 agonists, and they do not absorb at the same rate:
Injection site | Absorption speed | Time to peak effect | Best for |
|---|---|---|---|
Abdomen | Fastest | Slightly earlier Tmax | Those wanting quickest onset |
Upper arm | Moderate | Middle range Tmax | Balance of speed and comfort |
Thigh | Slowest | Slightly delayed Tmax | Those wanting gentler onset |
The abdomen has the richest subcutaneous blood supply of the three sites, which is why absorption is fastest there. The thigh has relatively less blood flow to subcutaneous tissue, leading to slower, more gradual absorption. For detailed guidance on technique, review our complete GLP-1 injection site guide.
How injection site interacts with timing
Here is where this gets interesting. If you inject in the abdomen in the morning, you are combining the fastest absorption site with morning alertness. Side effects, if they come, will arrive sooner and potentially feel sharper but resolve faster. The stomach injection technique matters for getting this right.
If you inject in the thigh in the evening, you are combining the slowest absorption site with sleep. The drug enters circulation more gradually, potentially creating a gentler side effect curve that is easier to sleep through. Some researchers deliberately use this combination to minimize the acute post-injection experience.
The difference in absorption speed between sites is relatively modest for long-acting GLP-1 formulations. We are talking about hours, not days. But for researchers who are particularly sensitive to the initial post-injection window, matching site to timing can provide a meaningful quality-of-life improvement.
Rotation and timing consistency
Regardless of which site you prefer, injection site rotation is essential. Using the same spot repeatedly leads to lipohypertrophy, hardened fatty deposits that impair absorption. Lipohypertrophy can change your pharmacokinetic profile unpredictably, making timing optimization pointless because you no longer know how fast the drug is reaching your bloodstream.
Best practice is a 4-week rotation cycle. Inject at least 1 inch (2.5cm) from your last injection spot. Many researchers use a simple system: week 1 left abdomen, week 2 right abdomen, week 3 left thigh, week 4 right thigh. Then repeat. This keeps tissue healthy and absorption predictable.
If you decide to optimize both site and timing, keep the time consistent even as you rotate sites. The slight differences in absorption speed between sites will average out over the rotation cycle, while the consistency of timing maintains your weekly rhythm.
Managing side effects through strategic timing
Side effects are the number one reason people abandon GLP-1 therapy. And timing is one of the most powerful tools you have for managing them. This is not about eliminating side effects entirely, but about structuring your schedule so that when they hit, they interfere with your life as little as possible.
Nausea timing strategies
GLP-1 induced nausea follows a predictable pattern for most users. It peaks 1 to 3 hours after injection, can persist at lower levels for 12 to 24 hours, and typically resolves within 48 hours. During dose escalation phases, nausea may be more intense and last longer. The pattern looks different for each medication, so understanding how semaglutide and tirzepatide side effects compare can help set expectations.
If nausea is your primary concern, the timing strategy is clear. Inject in the evening, ideally 2 to 3 hours before bedtime. This puts the peak nausea window during sleep. You might wake slightly nauseous, but the worst will have passed. By mid-morning, most users feel significantly better.
Alternatively, if your nausea is mild and manageable, morning injection allows you to experience the peak during active hours when physical movement and distraction naturally reduce nausea perception. Lying down tends to make nausea worse. Walking tends to make it better. Some researchers report that injecting before a morning walk or exercise session provides both the distraction and the upright posture that minimize nausea.
Fatigue management
GLP-1 related fatigue affects a significant subset of users, particularly during the first month and during dose escalation. The fatigue typically peaks 4 to 8 hours after injection and can linger for 24 to 48 hours.
For fatigue-prone individuals, evening injection is almost always the better choice. You inject, the fatigue hits while you are sleeping, and you wake up feeling relatively normal. Morning injection, by contrast, can create an afternoon energy crash that disrupts work and productivity. Understanding the relationship between semaglutide and energy levels can help you predict and manage this effect.
Gastrointestinal side effect timing
Beyond nausea, GLP-1 agonists can cause constipation, diarrhea, bloating, and acid reflux. Each has its own timing pattern:
Constipation tends to worsen gradually over the first 48 to 72 hours after injection, then slowly improve as drug levels decrease. For semaglutide-specific strategies, our constipation treatment guide covers evidence-based interventions. The tirzepatide constipation guide addresses the slightly different GI pattern seen with dual-agonist therapy.
Acid reflux and burping typically peak in the first 24 hours and worsen when lying down. If these are your primary side effects, evening injection can actually make things worse because lying down after injection is the worst position for reflux. Morning injection, combined with staying upright, tends to be the better choice. Our guide on semaglutide burping offers additional management strategies.
Diarrhea, when it occurs, tends to hit within the first 24 hours and resolve quickly. If this is a concern, timing your injection for the evening before a day when you have flexible access to a restroom is a sensible precaution. Nobody wants to deal with urgent GI symptoms during a morning commute.
The dose escalation timing adjustment
Here is a timing strategy that not enough guides mention. During dose escalation, when you are moving up to a new, higher dose, temporarily shifting your injection time to the evening (if you normally inject in the morning) can help you tolerate the transition. The first injection at any new dose tends to produce the strongest side effects. Sleeping through that first dose at the new level, then resuming your normal morning schedule the following week, can make escalation significantly more tolerable.
This is especially relevant for tirzepatide dosing, where the escalation steps are larger and side effects at each new dose can be more pronounced. Researchers who use microdosing strategies to bridge between dose levels may not need this adjustment, but for those following standard escalation protocols, it is a valuable tool.
Timing guidelines for specific GLP-1 medications
Each GLP-1 receptor agonist has its own pharmacokinetic personality. The optimal timing strategy varies accordingly. Here is what you need to know for each major medication.
Semaglutide (weekly injectable)
Dosing frequency: Once weekly, same day each week
Half-life: approximately 7 days (165 to 184 hours)
Peak concentration: 1 to 3 days after injection
Recommended timing approach: Most flexible of all GLP-1 formulations due to the long half-life. Morning or evening both work well. Choose based on side effect profile and lifestyle. For a complete breakdown of semaglutide-specific timing, see our dedicated best time to take semaglutide guide.
Key timing considerations:
If nausea is significant, evening injection allows sleeping through peak effects
If blood sugar management is the primary goal, morning injection may offer a slight advantage
Compounded semaglutide follows the same timing principles as brand-name formulations
The 7-day half-life means you have the most forgiving missed-dose window of any weekly GLP-1
Steady state is reached after approximately 4 to 5 weeks of consistent weekly dosing
Dose escalation timing: Standard escalation starts at 0.25mg weekly for 4 weeks, then increases to 0.5mg. Each escalation step can temporarily increase side effects. For the specific unit conversions, our semaglutide units to mg guide provides exact numbers. If you are working with compounded formulations, the 5mg/ml dosage chart clarifies the math.
Tirzepatide (weekly injectable)
Dosing frequency: Once weekly, same day each week
Half-life: approximately 5 days (120 hours)
Peak concentration: 8 to 72 hours after injection
Recommended timing approach: The shorter half-life compared to semaglutide means the end-of-week trough is more noticeable. Strategic day-of-week selection becomes more important. Many tirzepatide users benefit from Thursday or Friday injection to maximize weekend coverage. For complete dosing details, see the tirzepatide dosing guide.
Key timing considerations:
Broader Tmax window (8 to 72 hours) means less precision in predicting peak effects
Dual GIP/GLP-1 mechanism may produce a different side effect timing pattern than pure GLP-1 agonists
Body aches and muscle pain may peak later than GI symptoms, around 24 to 48 hours post-injection
Consider how tirzepatide affects metabolism throughout the weekly cycle
The appetite suppression timeline may differ from semaglutide due to the dual mechanism
Dose escalation timing: Tirzepatide starts at 2.5mg weekly, escalating to 5mg after 4 weeks. For unit conversions, the 2.5mg unit conversion guide has exact figures. The tirzepatide dosing in units guide covers the full escalation protocol.
Liraglutide (daily injectable)
Dosing frequency: Once daily, same time each day
Half-life: approximately 13 hours
Peak concentration: 8 to 12 hours after injection
Recommended timing approach: Because of the short half-life, time of day matters significantly more for liraglutide than for weekly formulations. The medication creates a pronounced peak-and-trough cycle within each 24-hour period.
Key timing considerations:
Morning injection produces peak appetite suppression around mid-afternoon to evening, ideal for those who struggle with afternoon snacking and dinner portions
Evening injection produces peak levels overnight and through the morning, beneficial for those who overeat at breakfast or need better fasting glucose control
The 13-hour half-life means effects noticeably diminish in the latter half of each 24-hour cycle
Consistency is absolutely critical with daily dosing because missed doses create more significant gaps in drug levels
Many liraglutide users tie their injection to a specific daily habit (brushing teeth, morning coffee ritual) to prevent missed doses
Dulaglutide (weekly injectable)
Dosing frequency: Once weekly, same day each week
Half-life: approximately 5 days (120 hours)
Peak concentration: 24 to 72 hours after injection
Recommended timing approach: Similar pharmacokinetic profile to tirzepatide in terms of half-life, though the mechanism is pure GLP-1 agonism. The same day-of-week considerations apply. Dulaglutide is delivered in a pre-filled pen that simplifies the injection process, making timing primarily a lifestyle decision rather than a preparation one.
Key timing considerations:
Side effect profile tends to be somewhat milder than semaglutide, which may reduce the importance of sleep-through timing
Same 48-hour minimum spacing rule applies if changing injection days
Pre-filled pen format means no reconstitution time, making spontaneous timing adjustments easier
Many dulaglutide users report minimal side effects after the first month, at which point timing becomes purely a convenience decision
Retatrutide (weekly injectable, investigational)
Dosing frequency: Once weekly
Half-life: Data from Phase 2 trials suggest approximately 6 days
Peak concentration: Approximately 24 to 72 hours after injection
Recommended timing approach: As a triple agonist (GLP-1/GIP/glucagon), retatrutide may produce a different side effect profile than pure GLP-1 or dual GLP-1/GIP agonists. The glucagon receptor activity adds a thermogenic component that can affect energy levels and body temperature. For dosing specifics, see the retatrutide dosage chart.
Key timing considerations:
The glucagon component may cause increased energy and warmth, which some researchers prefer in the morning rather than before bed
Dose scheduling follows similar principles to other weekly GLP-1 formulations
Injection site rotation follows the same principles outlined in the retatrutide injection guide
Triple agonist mechanism means monitoring for unique side effects that may have their own timing patterns
Being investigational, less real-world timing data exists compared to approved medications
What to do when you miss your injection window
It happens to everyone. Life gets chaotic, routines break, and suddenly you realize you are a day or two past your scheduled injection. Knowing the exact rules for missed doses prevents both dangerous doubling and unnecessary panic.
Semaglutide missed dose rules
If you miss your scheduled semaglutide injection, you have a 5-day (120-hour) grace period. As long as fewer than 5 days have passed since your missed dose, take it as soon as you remember and resume your regular schedule the following week. If more than 5 days have passed, skip the missed dose entirely and take your next regularly scheduled dose on your normal day.
Here is what that looks like practically. You normally inject every Thursday morning. You realize on Saturday afternoon that you forgot. Only 2 days have passed, so you inject Saturday afternoon. Next week, go back to Thursday as usual. But if you do not realize until the following Wednesday (6 days later), you skip the missed dose and just inject Thursday as planned.
Never take two semaglutide doses less than 72 hours apart. This is a hard rule. Doubling up or taking doses too close together does not "make up" for the missed dose. It dramatically increases the risk of severe nausea, vomiting, and other GI side effects without improving efficacy. For more details on how semaglutide works in your body, understanding the pharmacokinetics helps explain why doubling is both unnecessary and risky.
Tirzepatide missed dose rules
Tirzepatide has a shorter grace period: 4 days (96 hours). If fewer than 4 days have passed since your missed dose, take it as soon as possible. If more than 4 days have passed, skip it and resume on your regular schedule.
The shorter window reflects tirzepatide shorter half-life. By day 4 after a missed dose, drug levels have dropped enough that adding a late dose on top of what remains could create unpredictable effects. The same 72-hour minimum spacing between doses applies. For researchers who find themselves frequently missing doses, consider whether your timing strategy needs adjustment. Perhaps switching from morning to evening, or tying the injection to a more reliable routine, would improve adherence. The tirzepatide effectiveness timeline depends heavily on consistent dosing.
Liraglutide missed dose rules
Because liraglutide is a daily injection with a 13-hour half-life, missed dose management is simpler but more urgent. If you miss your daily injection and remember within 12 hours, take it immediately. If more than 12 hours have passed, skip that dose and take your next dose at the regular time the following day.
Never take two liraglutide doses on the same day. The short half-life means drug accumulation from a double dose can cause severe GI side effects.
What about partial doses?
Sometimes an injection goes wrong. The needle slips. Some medication leaks out. You are not sure you got the full dose. In these cases, do not re-inject. You cannot accurately estimate how much entered your body, and a supplemental dose risks giving too much. Accept the partial dose and continue your regular schedule. One slightly reduced dose in a long-term protocol has negligible impact on overall results.
If you are having trouble with injection technique leading to partial doses, review our guides on GLP-1 injection technique and consider whether a peptide injection pen might improve your consistency. Getting the mechanics right matters just as much as getting the timing right.
Building your personal GLP-1 injection schedule
Knowing the theory is one thing. Building a practical schedule that fits your actual life is another. Here is a step-by-step process for designing your optimal injection routine.
Step 1: identify your primary goal
What matters most to you? Rank these in order:
Maximum appetite suppression alignment. You want peak effects to coincide with your hardest eating periods. This drives both your time-of-day and day-of-week decisions.
Minimum side effect disruption. You want to minimize how much nausea, fatigue, and GI effects interfere with your daily life. This typically pushes toward evening dosing.
Optimal blood sugar control. You want the tightest possible glycemic management. Morning dosing may offer a slight edge here.
Maximum adherence. You want whatever schedule you are least likely to forget. This typically means tying the injection to your most consistent daily or weekly routine.
For most researchers focused on weight management, the priority order is: adherence first, side effect management second, appetite alignment third. It does not matter how perfectly timed your shot is if you forget to take it every other week.
Step 2: choose your day of the week (weekly formulations)
Map out your typical week. Which days are most structured? Which days involve the most social eating? When do you have the most flexibility to rest if side effects hit? Use the table from the "best day" section above to match your lifestyle to an injection day.
If you are still unsure, start with Thursday evening. It is the single most popular choice among experienced GLP-1 users for good reason. Peak effects cover the weekend, side effects are manageable over Friday and Saturday, and the end-of-week trough falls on the structured workdays when you need less pharmaceutical help.
Step 3: choose your time of day
For this decision, answer one question honestly: how bad are your side effects?
If your side effects are mild or negligible, inject in the morning. You get the potential glucose benefit, the routine advantage, and daytime appetite suppression alignment.
If your side effects are moderate to severe, inject in the evening. Sleeping through the worst of the nausea and fatigue is worth more than any marginal timing advantage from morning dosing.
If your side effects are unpredictable, start with evening dosing for the first 4 to 6 weeks as you establish your dose. Once you understand your body response pattern, you can experiment with morning if you prefer.
Step 4: build the routine anchor
Your injection needs to be tied to something you already do without thinking. This is called habit stacking, and it is the single most effective adherence strategy.
Examples of effective anchors:
Morning injectors: "After I brush my teeth and before I make coffee" or "Right after my alarm goes off, before I check my phone."
Evening injectors: "Right after I brush my teeth for bed" or "Immediately after I put the kids to sleep."
The key is specificity. "I will inject in the evening" is vague and easy to forget. "I will inject immediately after putting on my pajamas" is specific, tied to an existing behavior, and much harder to skip. Many researchers also set phone alarms as backup, but the habit anchor is the primary system.
Step 5: set up your injection supplies
Timing optimization is meaningless if you spend 15 minutes searching for your supplies every injection day. Create a dedicated injection kit that lives in one place:
Your medication (properly stored, with awareness of semaglutide shelf life or tirzepatide fridge storage times). Alcohol swabs. Syringes or pen needles. A sharps container. Your injection log or tracking app.
Everything in one spot. Ready to go. When your alarm goes off or your routine anchor triggers, you grab the kit and inject. No friction. No delay. No excuses. For storage specifics, our peptide storage guide covers temperature requirements in detail.
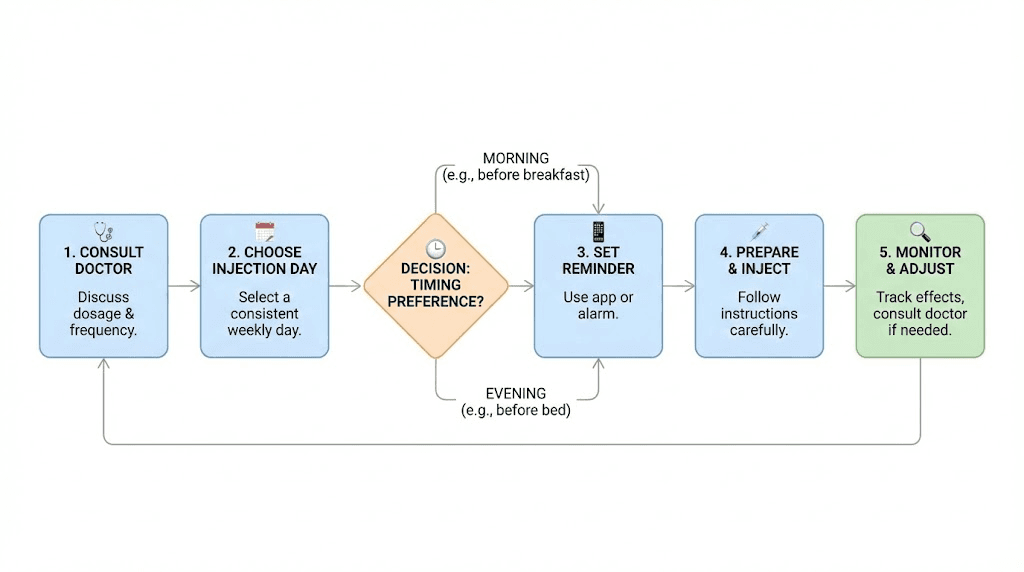
Step 6: track and adjust
Your first timing choice is not your final timing choice. Keep a simple log for the first 4 to 6 weeks tracking:
Injection day and time. Side effects experienced and when they peaked. Appetite suppression pattern throughout the week. Energy levels on injection day versus later in the week. Overall satisfaction with the schedule.
After 4 to 6 weeks, review the data. If your current timing is working well, keep it. If side effects are problematic at specific times, or if your appetite suppression is not aligned with your needs, adjust. Small changes, shifting by a few hours, or moving to a different day, can make a meaningful difference. The GLP-1 plotter tool can help visualize your weekly drug level curves to inform these adjustments.
Common timing mistakes and how to fix them
After analyzing thousands of researcher experiences, certain timing mistakes come up again and again. Recognizing and correcting these can dramatically improve your GLP-1 experience.
Mistake 1: chasing the "perfect" time instead of being consistent
This is the most common and most damaging mistake. A researcher reads that morning might be slightly better for glucose control, so they inject Monday morning. Then they read that evening is better for nausea, so they inject Tuesday evening the following week. Then they try Thursday afternoon. The constant switching prevents the body from establishing a predictable rhythm and makes side effects harder to manage.
The fix: Pick a time. Any reasonable time. Stick with it for at least 4 weeks. Then evaluate. Consistency at a "good enough" time beats constantly chasing the theoretically "perfect" time. Research on how long semaglutide takes to work shows that steady-state levels and consistent results require, above all, consistent dosing.
Mistake 2: injecting at different times each week
Related to mistake 1 but slightly different. Some researchers inject on the same day each week but at wildly different times. Thursday at 7am one week. Thursday at 11pm the next. Thursday at 3pm the week after. While this matters less for weekly formulations than it would for daily ones, it still disrupts the predictability of your side effect and appetite suppression patterns.
The fix: Aim for the same time, within a 2-hour window, each injection day. If your target is Thursday at 8pm, anything between 7pm and 9pm is fine. Do not stress about being exact to the minute, but do keep it in the same general window.
Mistake 3: taking a large meal right after injection
Some researchers inject and then immediately eat a large meal, thinking the food will "buffer" nausea. What actually happens is the GLP-1 agonist starts slowing gastric emptying while a large bolus of food is entering the stomach. The result is often worse nausea, bloating, and discomfort than either the injection alone or the food alone would have caused.
The fix: If you want to eat around injection time, eat a small, light, protein-focused snack 30 to 60 minutes BEFORE injecting. Not after. This gives the food time to begin digestion before the GLP-1-mediated gastric slowing kicks in. The semaglutide food list and tirzepatide foods to avoid provide specific dietary guidance.
Mistake 4: panicking over a late dose and doubling up
You forgot your Thursday injection and remembered Saturday. In a panic, you take Saturday dose and then another one on Thursday, only 5 days later. Or worse, you take a "double dose" on Saturday to compensate. Both of these approaches are dangerous and unnecessary.
The fix: Follow the missed dose rules exactly. For semaglutide, you have a 5-day window. For tirzepatide, 4 days. Take the late dose if within the window and resume your normal schedule the following week. Never take two doses within 72 hours. One missed or late dose has minimal impact on long-term results. A double dose can send you to the emergency room with severe vomiting.
Mistake 5: not adjusting timing during dose escalation
You have been happily injecting at 7am every Thursday for 8 weeks. Then you escalate from 0.5mg to 1mg of semaglutide. The higher dose brings stronger side effects that you were not prepared for at 7am, leading to a miserable workday. Some researchers interpret this as "the medication is not for me" rather than recognizing it as a timing problem specific to escalation.
The fix: When escalating to a new dose, consider temporarily shifting to evening injection for 1 to 2 weeks. Once your body adjusts to the new dose and side effects settle, shift back to your preferred morning time. This one strategy, acknowledged by many experienced researchers and clinicians, prevents a huge amount of unnecessary suffering and premature discontinuation.
Mistake 6: injecting in the same site at the same time
Always injecting in the left side of the abdomen every Thursday morning creates a pattern of tissue damage and inconsistent absorption. Lipohypertrophy develops at the overused site, drug absorption becomes unpredictable, and your carefully optimized timing becomes meaningless because the pharmacokinetics are no longer reliable.
The fix: Rotate injection sites on a fixed schedule while keeping your injection time consistent. Time stays the same. Site rotates. This maintains timing optimization while preserving tissue health and absorption consistency.
Mistake 7: not accounting for travel and time zones
Traveling across time zones throws off injection schedules. A researcher who normally injects at 8am Eastern time flies to the West Coast and injects at 8am Pacific, which is actually 11am Eastern. Three hours is not a big deal for a weekly injection, but for daily liraglutide with its 13-hour half-life, that shift matters. Traveling internationally can create even larger disruptions.
The fix: For weekly injections, stick to your home time zone for injection timing if the travel is short (less than a week). For longer stays, gradually shift your injection time to align with the local schedule. For daily injections, adjust by 1 to 2 hours per day until you match the new time zone. Our travel with semaglutide guide covers these scenarios in detail, including how to keep medication properly stored during transit.
Mistake 8: comparing your timing to others
Online forums are full of people sharing their injection timing with absolute certainty. "Morning is the only way to go." "Evening changed my life." "Friday injection is the best." And they are all correct, for themselves. Their body, their lifestyle, their side effect profile, their eating patterns. None of that necessarily applies to you.
The fix: Use other people experiences as data points, not prescriptions. Your optimal timing is a function of your unique physiology, your daily routine, your side effect sensitivity, and your eating patterns. No forum post can account for all of those variables. Test, track, and find your own rhythm.
Advanced timing optimization
Once you have the basics dialed in, there are additional timing considerations that can further refine your protocol.
Timing GLP-1 injections around exercise
Exercise timing relative to your GLP-1 injection can affect both performance and side effect management. High-intensity exercise within 2 to 4 hours of injection can worsen nausea, as both exercise and the medication reduce blood flow to the GI tract. Many researchers who maintain active exercise routines find that separating their injection from intense workouts by at least 6 to 8 hours provides the best experience.
For weekly formulations, this typically means if you exercise in the morning, inject in the evening, or vice versa. For daily liraglutide, plan your injection for the time of day farthest from your workout window. The relationship between tirzepatide and energy or semaglutide and energy also plays into exercise timing decisions.
Timing around supplements and other medications
Injectable GLP-1 agonists do not have significant drug interactions related to timing because they bypass the gastrointestinal tract. However, GLP-1 agonists slow gastric emptying, which can affect the absorption of oral medications taken around the same time. If you take oral medications that require precise absorption (thyroid medication, certain antibiotics, oral contraceptives), take them at least 1 hour before your GLP-1 injection or consider separating them by several hours.
Supplements are generally less sensitive to timing. B12 supplementation with semaglutide and B12 with tirzepatide are common pairings. Glycine combinations and tirzepatide glycine protocols have their own considerations. For a full list of supplements to consider with tirzepatide, that guide covers timing interactions. The newer tirzepatide glycine B12 compound formulations combine these in a single injection, simplifying the timing question entirely.
Timing for combination protocols
Some researchers use GLP-1 agonists alongside other peptides or medications. If you are combining, say, semaglutide with cagrilintide, the timing of each injection should be coordinated. Most combination protocols recommend same-day injection but at different sites. Cagrilintide dosing follows its own schedule, and understanding cagrilintide side effects helps you plan a timing strategy that accounts for overlapping side effect windows.
The combination of phentermine with semaglutide raises separate timing questions, as phentermine is a stimulant best taken in the morning to avoid insomnia. For a comprehensive comparison of these approaches, see the phentermine vs semaglutide analysis.
Seasonal timing adjustments
Some experienced researchers adjust their timing strategy seasonally. During summer months, when social events, barbecues, and vacations are frequent, they shift their injection day so peak effects cover weekends. During structured winter months, they may prioritize weekday coverage instead. This is an advanced strategy that requires already having a solid baseline protocol established, but it demonstrates the flexibility that understanding pharmacokinetics provides.
Timing considerations when switching medications
If you are switching from semaglutide to tirzepatide or going the other direction, timing the transition correctly matters. The standard approach is to take your last dose of the old medication on its normal schedule and start the new medication on what would have been your next scheduled injection day. This maintains the weekly rhythm while allowing the previous medication to clear. The conversion chart and reverse switching guide provide exact dosing translations.
Long-term timing considerations
As you settle into a GLP-1 protocol over months, your side effect profile typically improves significantly. The nausea that dictated evening dosing during your first month may virtually disappear by month three. At that point, you have the freedom to re-evaluate your timing based on appetite alignment and convenience rather than side effect avoidance. Understanding how long semaglutide treatment typically lasts provides context for this long-term planning. The journey from initial adjustment through potential plateaus to maintenance dosing involves evolving timing needs at each stage.
For researchers who experience their medication becoming less effective over time or wonder why weight loss has stalled on semaglutide, timing is one of many factors worth re-examining. The same applies to those facing weight loss plateaus on tirzepatide or experiencing no results after 4 weeks on semaglutide. While timing alone is unlikely to be the sole cause, it is one piece of the optimization puzzle that is easy to adjust and test.
Emerging GLP-1 delivery methods and timing implications
The GLP-1 landscape is evolving rapidly, with new delivery methods that fundamentally change how we think about timing.
GLP-1 patches
GLP-1 transdermal patches like Onmorlo represent a paradigm shift in timing considerations. Rather than a bolus dose followed by gradual elimination, patches deliver a steady stream of medication over days. The concept of "best time to apply" becomes less about pharmacokinetic optimization and more about practical convenience and skin site rotation. These delivery systems may eventually make many of the timing questions in this guide irrelevant for patch users.
Oral GLP-1 formulations
Oral formulations, including oral tirzepatide and existing oral semaglutide, have strict timing requirements related to food and water intake. The tirzepatide tablets versus injections comparison highlights how fundamentally different the timing strategies are for each route of administration. Tirzepatide drops and other novel delivery methods each carry their own timing rules.
Next-generation molecules
Newer molecules entering the GLP-1 space, including GLP-3 peptides, mazdutide, survodutide, and orforglipron, each have unique pharmacokinetic profiles that will require their own timing optimization strategies. As these become available, the principles in this guide, understanding half-life, aligning peak effects with needs, managing side effect windows, will still apply. Only the specific numbers will change.
Special populations and timing considerations
Certain groups face unique timing challenges that deserve specific attention.
Shift workers
If you work rotating shifts, the concept of "morning" and "evening" injection becomes meaningless. What matters for shift workers is tying injection to a consistent event rather than a time of day. "After my first meal at the start of each shift cycle" or "When I wake up for my longest stretch of shifts" provides the consistency that a clock time cannot when your clock is always changing.
For shift workers on weekly GLP-1 formulations, choose your injection day based on your most consistent day off. Even if your schedule rotates, most shift workers have one day per week that is relatively predictable. That is your injection day.
People with gastroparesis or slow gastric motility
GLP-1 agonists further slow already-compromised gastric emptying. For people with existing gastroparesis, timing the injection so peak effects do not coincide with their largest meal of the day can reduce GI distress. Morning injection before a typically light breakfast, with the understanding that lunch and dinner portions may need to be smaller, often works best for this population.
Researchers also taking insulin
If you use both insulin and a GLP-1 agonist, timing coordination matters. Injecting both at the same time of day is generally fine, but use different injection sites. Never mix insulin and GLP-1 agonists in the same syringe unless specifically using a combination product designed for this purpose. The GLP-1 agonist slowing gastric emptying can affect the glucose peak from meals, which in turn affects insulin timing. Work with your healthcare provider to adjust meal-time insulin doses and timing when starting or adjusting a GLP-1 agonist.
Pregnancy considerations
GLP-1 agonists should be discontinued before pregnancy. The timing question here is about cessation rather than dosing. Semaglutide, with its 7-day half-life, should be stopped at least 2 months before planned conception to ensure complete washout. Tirzepatide, with its 5-day half-life, requires approximately 5 weeks of washout. For detailed guidance, see our resources on GLP-1 use during breastfeeding and pregnancy while on tirzepatide.
Tools for tracking and optimizing your timing
Optimization requires measurement. Here are the approaches that help researchers dial in their timing.
Using the GLP-1 plotter
The GLP-1 plotter visualizes your estimated drug levels throughout the week based on your medication, dose, and injection timing. This makes it easy to see when you are at peak levels, when the trough occurs, and how shifting your injection day or time would change the curve. It is a powerful tool for making informed timing decisions rather than guessing.
Dosage calculators for precise dosing
Accurate dosing is a prerequisite for meaningful timing optimization. If your dose is inconsistent, no amount of timing adjustment will produce consistent results. Use the semaglutide dosage calculator or compounded tirzepatide dosage calculator to ensure every injection delivers the intended amount. For reconstitution math, the peptide reconstitution calculator takes the guesswork out of dilution. The general peptide calculator handles a broader range of calculations for multi-peptide protocols.
For specific conversion questions like how many mg is 40 units of semaglutide, 50 units of semaglutide in mg, 20 units in mg, 100 units in mg, or 10 units in mg, those dedicated guides ensure you are injecting the right amount each time. Tirzepatide users can reference 20 units of tirzepatide in mg and 40 units of tirzepatide in mg for equivalent conversions. And for reconstitution questions like how much bac water to mix with 10mg semaglutide or how to reconstitute 5mg semaglutide, getting the concentration right is essential for accurate dosing at your chosen time.
Simple tracking methods
You do not need complex software. A simple note on your phone works. Record:
Date and time of injection. Injection site used. Side effects experienced (type, severity, timing). Appetite level on a 1 to 10 scale each day. Any notable changes to energy, sleep, or mood.
After 4 to 6 weeks of data, clear patterns emerge. You will see whether mornings or evenings produce fewer side effects for you specifically. You will identify which injection day gives you the best weekly appetite pattern. You will notice how long after injection your side effects peak and resolve. This personalized data is worth more than any generic timing recommendation.
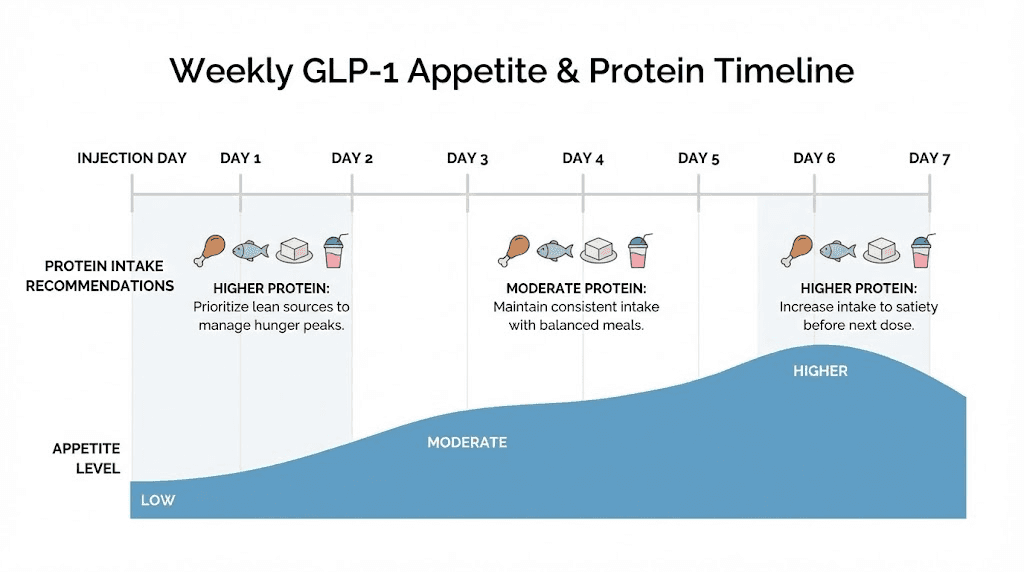
The protein priority and timing synergy
One final timing consideration that ties directly to outcomes: protein intake timing relative to your injection schedule.
GLP-1 agonists reduce appetite and food intake across the board. This means you eat fewer total calories, which is the goal for weight management. But the reduction is often disproportionate, hitting protein intake harder than other macronutrients because protein-rich foods tend to be the most satiating and the hardest to consume when appetite is suppressed.
Low protein intake during GLP-1 therapy leads to excessive muscle loss relative to fat loss. This is one of the most important long-term risks of these medications and is directly addressed by intentional protein timing. Using protein shakes designed for GLP-1 users during the high-suppression days (typically days 1 to 3 after injection) can help maintain adequate protein intake even when eating solid food feels impossible.
The timing connection: understanding when your appetite will be lowest (peak drug levels, days 1 to 3) lets you plan your highest-protein meals for the days when you have relatively more appetite (days 5 to 7). This protein cycling approach, front-loading protein toward the end of your weekly cycle when you can actually eat it, and supplementing with liquid protein during peak suppression, is a strategy that experienced researchers consistently report produces better body composition outcomes.
For more on this topic, explore the semaglutide diet plan, the tirzepatide meal plan, and our broader best peptides for weight loss guide that covers how different compounds interact with nutrition timing.
Frequently asked questions
Does it matter what time of day I take my GLP-1 injection?
For weekly injectable formulations like semaglutide and tirzepatide, the exact hour matters less than consistency. One small study showed morning dosing may offer about 15% better post-prandial glucose control, but the more impactful consideration is whether morning or evening timing better manages your side effects and aligns with your routine. For daily liraglutide, time of day matters more because of the shorter 13-hour half-life. Choose the time that aligns peak appetite suppression with your most challenging eating period.
Should I take my GLP-1 shot in the morning or at night?
Both are valid. Morning works best for researchers with mild side effects who want daytime appetite suppression and a potential glycemic advantage. Evening works best for those with significant nausea or fatigue who prefer to sleep through peak side effects. About 60% of users who experience GI side effects report that evening dosing significantly reduces their perception of discomfort. Start with evening dosing if you are new to GLP-1 therapy, then consider switching to morning once your body adjusts.
Can I change the day of the week I take my GLP-1 shot?
Yes, but maintain at least 48 hours between your old injection time and new injection time. Never take two doses within 72 hours. If switching from Tuesday to Friday, take your Tuesday dose, then wait until Friday (3 days later) for your first dose on the new schedule. Going forward, Friday becomes your new injection day.
What happens if I take my GLP-1 shot a few hours late?
For weekly formulations, a few hours makes virtually no difference. The multi-day half-lives of semaglutide and tirzepatide mean that a 2 to 4 hour shift is pharmacologically negligible. Even a full day late is within the acceptable window. Just take it when you remember and resume your normal schedule the following week.
Do I need to eat before or after my GLP-1 injection?
For injectable formulations, there is no requirement to eat at any specific time relative to injection. However, many researchers find that a small, light snack 30 to 60 minutes before injection reduces acute nausea. For oral semaglutide, you MUST take it on an empty stomach and wait 30 minutes before eating. Food reduces oral semaglutide absorption by up to 40%.
Is it okay to take my semaglutide a day early?
Occasionally taking your injection one day early is generally safe as long as at least 5 days have passed since your previous dose. However, making a habit of early injections is not recommended because it can lead to drug accumulation and increased side effects. If your schedule frequently requires taking it early, consider officially shifting your injection day. For tirzepatide, the same logic applies, but note whether taking tirzepatide early could be causing increased side effects.
What is the best day of the week for a GLP-1 shot?
Thursday or Friday is the most popular choice among experienced users. This timing aligns peak appetite suppression with the weekend, when eating tends to be less structured and more socially influenced. It also means the initial side effect window falls on Friday night and Saturday, minimizing workday disruption. That said, the best day is ultimately the one that fits your lifestyle and allows the most consistent adherence.
How does injection site affect when my GLP-1 kicks in?
Abdominal injections produce the fastest absorption, while thigh injections are the slowest. The difference is hours, not days, so it primarily affects the acute post-injection experience rather than overall weekly efficacy. If you are particularly sensitive to the initial onset effects, choosing a slower absorption site like the thigh can create a gentler ramp-up. Conversely, if you want the quickest onset of appetite suppression, the abdomen is your best choice.
Can I drink alcohol on the same day I take my GLP-1 shot?
It is technically possible but generally not recommended, especially on injection day. GLP-1 agonists slow gastric emptying, which can intensify and prolong the effects of alcohol. The combination also increases the risk of nausea and can further stress the GI tract during the window when side effects are already most likely. If you choose to drink, do so in moderation and preferably 24 or more hours after injection. For specific guidance, see alcohol and semaglutide and alcohol and tirzepatide.
Should I adjust my timing if I experience hair loss on GLP-1 therapy?
Timing adjustments alone will not prevent GLP-1 related hair loss, which is typically caused by rapid weight loss and nutritional deficiencies rather than the timing of the injection itself. However, optimizing your timing to maximize protein and nutrient intake (by aligning higher-appetite days with protein-rich meals) can help mitigate this side effect indirectly. The root cause needs to be addressed through nutrition and supplementation rather than injection scheduling.
What about timing semaglutide with methylcobalamin B12?
Many researchers use semaglutide with methylcobalamin to support energy levels and prevent B12 deficiency. These can be taken at the same time or at different times during the day. The B12 injection uses a different mechanism of absorption and does not interact with GLP-1 pharmacokinetics. If using injectable B12, inject at a different site than your GLP-1 shot.
External resources
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact questions. Whether you are fine-tuning your semaglutide dosage, exploring tirzepatide results, or just getting started with peptides, the resources and community at SeekPeptides are built for exactly this kind of evidence-based optimization.
In case I do not see you, good afternoon, good evening, and good night. May your injection timing stay consistent, your side effects stay manageable, and your results stay on track.