Feb 25, 2026

What if the real question is not whether berberine and semaglutide can coexist in your body, but whether combining them actually makes your protocol stronger? Thousands of people take semaglutide for weight loss and blood sugar control. Thousands more take berberine for the same reasons. And a growing number want to use both at the same time, hoping the combination delivers something neither can achieve alone.
The answer is not simple.
Both compounds lower blood sugar. Both affect your gut. Both influence insulin sensitivity through mechanisms that overlap in some places and diverge sharply in others. Get the combination right and you potentially amplify metabolic improvements across multiple pathways simultaneously. Get it wrong and you risk hypoglycemia, debilitating GI side effects, or drug interactions that change how your medications behave in ways you did not expect. The difference between a powerful protocol and a dangerous one often comes down to timing, dosing, and understanding exactly how these two compounds interact at the cellular level.
This guide covers everything researchers need to know about combining berberine with semaglutide. You will learn how each compound works independently, where their mechanisms overlap, what the clinical data actually shows about combining them, specific protocols for safe co-administration, the risks most guides completely ignore, and practical troubleshooting for the problems that come up when people try this combination in the real world. Whether you are already on semaglutide and considering adding berberine, or you are taking berberine and thinking about starting semaglutide, the information here will help you make an informed decision with your healthcare provider. SeekPeptides has compiled the most current research on this topic to give you the evidence-based clarity that surface-level guides simply do not provide.
How semaglutide works in the body
Semaglutide is a GLP-1 receptor agonist. That sounds technical, but the concept is straightforward. Your body naturally produces a hormone called glucagon-like peptide-1 (GLP-1) in response to food. This hormone tells your pancreas to release insulin, slows down stomach emptying, and sends satiety signals to your brain. Semaglutide mimics this hormone, but it lasts much longer than the natural version, which degrades within minutes.
The results speak for themselves. In the STEP clinical trial program, participants taking semaglutide 2.4 mg weekly lost an average of 14.9% to 17.4% of their body weight over 68 weeks. The STEP 1 trial showed 86% of participants lost at least 5% of their baseline weight. The STEP 5 trial demonstrated sustained weight loss of 16.7% at two years. These are not modest numbers. They represent a genuine shift in what pharmaceutical intervention can achieve for weight management.
But weight loss is only part of the story.
Semaglutide reduces HbA1c by approximately 1.1% in people with type 2 diabetes. It lowers fasting blood glucose. It improves cardiovascular risk markers. And it does all of this primarily through one mechanism: activating GLP-1 receptors throughout the body. Understanding this single-pathway approach is critical because it explains exactly why berberine, which works through entirely different pathways, becomes such an interesting complement. For a detailed look at how quickly semaglutide produces results, our timeline guide breaks down what to expect week by week.
How semaglutide controls appetite and blood sugar
Semaglutide works on three fronts simultaneously. First, it stimulates insulin secretion from the pancreas in a glucose-dependent manner. This means it helps your body release insulin when blood sugar is high, but it does not force insulin release when blood sugar is normal. This glucose-dependent action is why semaglutide alone rarely causes dangerous hypoglycemia.
Second, it slows gastric emptying. Food stays in your stomach longer, which means nutrients are absorbed more gradually and blood sugar spikes become smaller and more manageable. This delayed emptying also contributes to the feeling of fullness that makes appetite suppression one of the most noticeable effects for people starting treatment.
Third, and perhaps most importantly for weight loss, semaglutide acts directly on brain regions that control hunger and food reward. It reduces cravings. It decreases food-seeking behavior. It makes smaller portions feel satisfying. Some researchers describe this as a reset of the body hunger thermostat, allowing people to eat less without the constant battle against hunger that derails most traditional diets.
These three mechanisms explain why semaglutide produces such dramatic results. They also explain why the side effects tend to cluster around the digestive system. Nausea, which affects roughly 20% of users in clinical trials, is a direct consequence of slowed gastric emptying. Constipation, diarrhea, and abdominal discomfort follow the same logic. When you fundamentally alter how quickly food moves through the GI tract, digestive complaints are almost inevitable during the adjustment period. Some users also report excessive burping, dizziness, and sleep disruption during the early weeks of treatment. Understanding these baseline side effects is essential before adding any supplement, because you need to know what semaglutide alone does to your body before introducing another variable.
The timeline matters too. Most people begin noticing meaningful changes within the first month of treatment, though the full dose escalation typically takes 16-20 weeks to complete. During that escalation period, side effects shift and evolve as each dose increase triggers a new adjustment phase. Our detailed breakdown of how long GLP-1 medications take to start working covers what to expect at each stage.
How berberine works in the body
Berberine is an alkaloid compound found in several plants, including goldenseal, Oregon grape, and barberry. It has been used in traditional Chinese medicine for centuries, but modern research has identified specific molecular mechanisms that explain its metabolic effects. The primary mechanism involves activation of an enzyme called AMP-activated protein kinase, commonly referred to as AMPK.
AMPK is sometimes called the body metabolic master switch. When activated, it triggers a cascade of metabolic changes: increased glucose uptake by muscle cells, enhanced fat oxidation, reduced glucose production in the liver, and improved insulin sensitivity at the cellular level. Berberine activates AMPK by inhibiting complex I of the mitochondrial respiratory chain, which increases the AMP-to-ATP ratio inside cells. This ratio change is the signal that flips the metabolic switch.
The clinical numbers are meaningful but modest compared to pharmaceutical interventions. A large umbrella meta-analysis found berberine supplementation reduces fasting blood glucose by approximately 0.82 mmol/L (about 15 mg/dL) and HbA1c by roughly 0.63% in people with metabolic disorders. For cholesterol, studies show reductions in LDL of about 25%, triglycerides by 35%, and total cholesterol by 29% in hypercholesterolemic patients taking 500 mg twice daily for three months.
Weight loss from berberine alone is modest, typically 2 to 4 kg (roughly 4.4 to 8.8 pounds) over study periods ranging from 8 to 24 weeks. Compare that to the 15-17% body weight reduction from semaglutide. Berberine is not a replacement for GLP-1 medications. But it may be a valuable addition.
The AMPK pathway and why it matters for semaglutide users
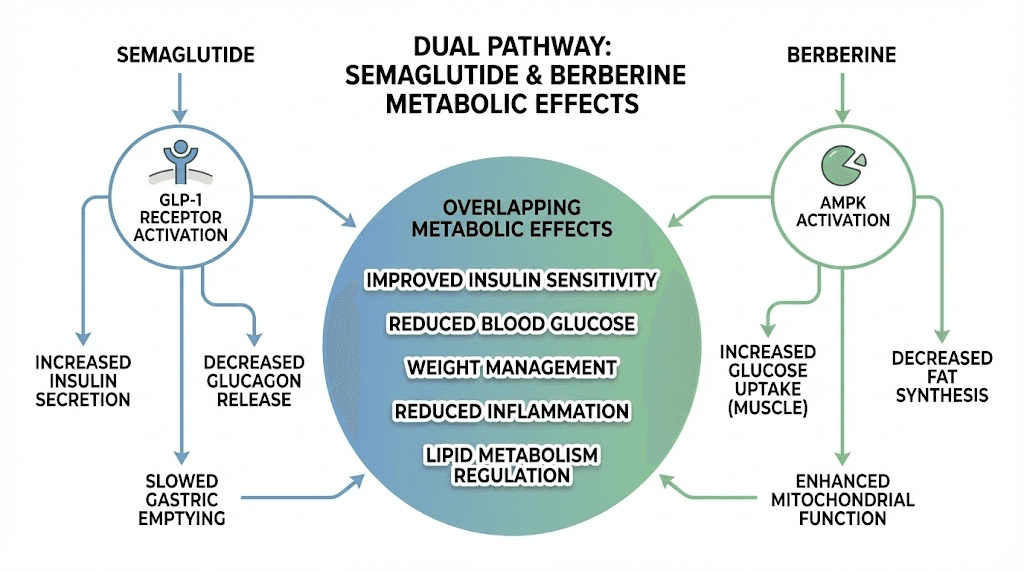
Here is where things get interesting for people already on semaglutide. The AMPK pathway that berberine activates is fundamentally different from the GLP-1 receptor pathway that semaglutide targets. Semaglutide works top-down, mimicking a hormone that tells the body to release insulin and reduce appetite. Berberine works bottom-up, directly changing how individual cells handle glucose and fat at the metabolic level.
In animal studies, berberine reduced body weight and improved glucose tolerance in diabetic mice without altering food intake. That last detail is critical. Semaglutide works largely by reducing how much you eat. Berberine appears to work by changing how your cells process the energy from what you do eat. Different mechanisms. Different targets. Potentially complementary effects.
Research in insulin-resistant rats showed berberine increased insulin sensitivity after five weeks of administration, with fasting insulin and HOMA-IR (a measure of insulin resistance) decreased by 46% and 48% respectively. For people struggling to lose weight on semaglutide alone, the additional insulin-sensitizing effects of berberine could theoretically help break through plateaus by addressing metabolic resistance from a completely different angle. If you have hit a semaglutide plateau after initial success, the AMPK pathway represents a fundamentally different metabolic lever to pull. People exploring visceral fat reduction may find berberine particularly interesting because AMPK activation specifically increases fatty acid oxidation, the process by which stored fat gets broken down and used for energy.
Berberine actually stimulates GLP-1 production
Most people miss this connection entirely. Berberine does not just work through AMPK. It also stimulates your body to produce more of its own GLP-1.
A study published in Biochemical Pharmacology found that berberine activates the bitter taste receptor TAS2R38 in intestinal enteroendocrine cells through the phospholipase C (PLC) signaling pathway, which stimulates GLP-1 secretion. Research in Nature showed that berberine restores GLP-1 secretion in diet-induced obese mice by protecting colon enterocytes from mitochondrial dysfunction. And a study examining berberine metabolites found that berberrubine and palmatine, two compounds your body creates when it processes berberine, significantly increased GLP-1 production and glucose-stimulated secretion in intestinal cells.
Think about what this means for semaglutide users. You are already taking a drug that mimics GLP-1. Berberine may help your body produce more of its own natural GLP-1 on top of that. It is like adding a natural GLP-1 boost alongside the pharmaceutical one. The clinical significance of this combined effect has not been studied directly, but the theoretical framework is compelling.
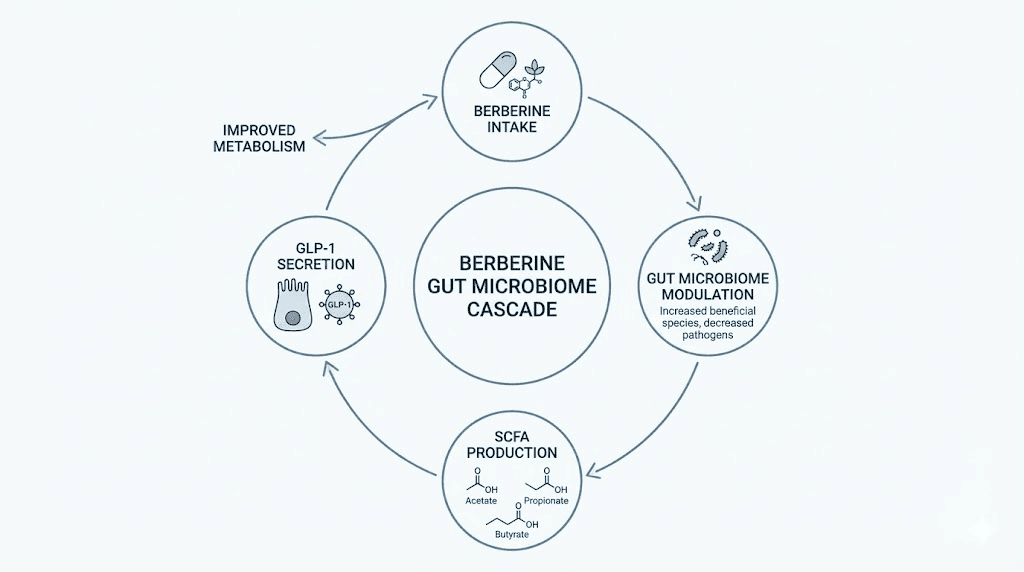
Berberine also influences the gut microbiome in ways that further support GLP-1 production. It promotes the growth of short-chain fatty acid (SCFA) producing bacteria, including Blautia and Allobaculum. These SCFAs, particularly butyrate and acetate, themselves stimulate additional GLP-1 secretion from intestinal L-cells. Research shows berberine increases gene expression of key enzymes in SCFA synthesis pathways by 27% to 86% depending on the specific acid. This creates a cascade: berberine feeds beneficial gut bacteria, those bacteria produce SCFAs, and those SCFAs trigger more GLP-1 release.
Can you actually take berberine and semaglutide together?
Yes. But with important caveats.
There is currently no clinical trial that has specifically studied the combination of berberine and semaglutide in humans. No randomized controlled trial. No large-scale observational study. The evidence for combining them comes from understanding their individual mechanisms, extrapolating from their known pharmacological profiles, and piecing together what we know about their respective safety data. This is an important limitation that honest guides should acknowledge upfront.
What we do know is encouraging. The direct pharmacokinetic interaction between berberine and semaglutide is likely minimal. Semaglutide is a peptide that undergoes proteolytic degradation in the body, meaning it is broken down by enzymes that cut proteins apart. It is not primarily metabolized by the liver CYP450 enzyme system. This matters because berberine is a known inhibitor of several CYP450 enzymes, particularly CYP2D6, CYP2C9, and CYP3A4. If semaglutide relied on these enzymes for metabolism, berberine could dangerously alter its blood levels. But because semaglutide takes a different metabolic route, this particular interaction is unlikely to be clinically significant.
That does not mean the combination is risk-free.
The real risks of combining them
The primary concern is pharmacodynamic, not pharmacokinetic. Both compounds lower blood sugar through different mechanisms. When you stack two glucose-lowering agents, the combined effect can push blood sugar lower than either would alone. For people with diabetes who are also taking metformin, insulin, or sulfonylureas, adding berberine on top of semaglutide creates a multi-layered glucose-lowering effect that significantly increases hypoglycemia risk.
The second major concern is gastrointestinal. Semaglutide causes nausea, vomiting, diarrhea, and constipation in a significant percentage of users, particularly during the dose-escalation phase. Berberine causes its own set of GI side effects: diarrhea, constipation, gas, and stomach cramps. Combining two compounds that both irritate the GI tract is not a recipe for comfort. Some people tolerate the combination well. Others find the digestive side effects intolerable. Understanding semaglutide fatigue patterns can help you distinguish between normal adjustment and problematic reactions.
The third concern involves berberine interaction with P-glycoprotein (P-gp), a transport protein that affects drug absorption and excretion. Berberine inhibits P-gp, which can increase the absorption and decrease the excretion of drugs that are P-gp substrates. While semaglutide itself is not a major P-gp substrate, many other medications that semaglutide users take, such as certain statins, blood pressure medications, and antidepressants, are affected by P-gp inhibition.
Who should avoid this combination entirely
Certain groups should not combine berberine with semaglutide under any circumstances. People with liver disease face increased risk because berberine CYP450 inhibition could affect how their liver processes other medications. Pregnant or breastfeeding women should avoid berberine entirely, as it can cross the placenta and potentially harm the fetus. Anyone with a history of severe hypoglycemia should approach the combination with extreme caution. For those wondering about GLP-1 use during breastfeeding, our dedicated guide covers the current evidence in detail. People who have concerns about how semaglutide affects menstrual cycles should be especially cautious about adding any additional metabolic modifier without medical guidance.
People already taking metformin alongside semaglutide should be particularly careful. A documented interaction shows berberine can increase metformin blood levels when taken approximately two hours before metformin. Triple-stacking semaglutide, metformin, and berberine creates three overlapping glucose-lowering mechanisms with compounding hypoglycemia risk. This is not a theoretical concern. It is a real clinical scenario that requires careful medical supervision.
Potential benefits of combining berberine with semaglutide
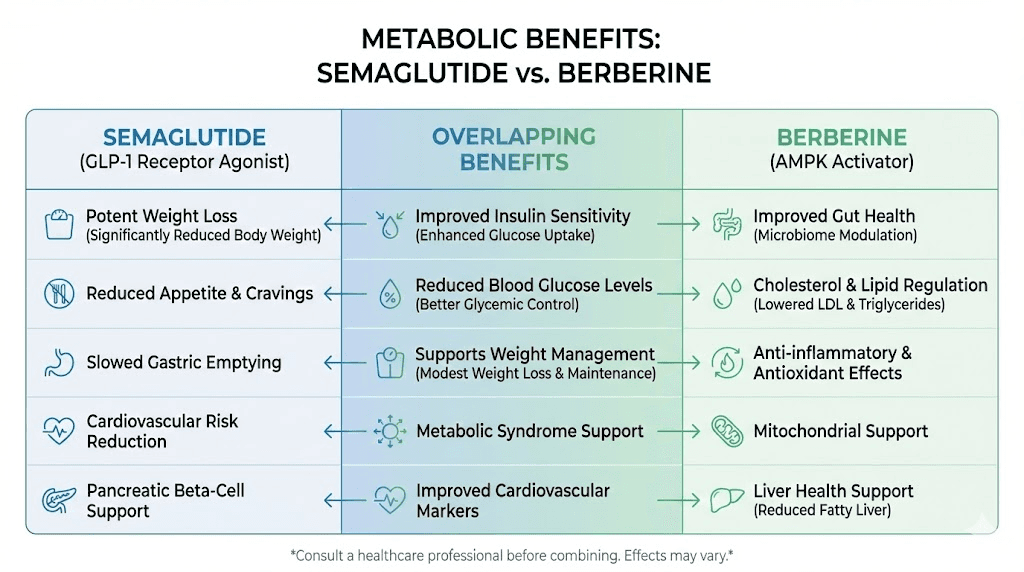
Despite the risks, there are legitimate reasons researchers explore this combination. The potential benefits stem from the fundamentally different mechanisms each compound uses to achieve overlapping metabolic goals.
Enhanced blood sugar control through dual mechanisms
Semaglutide improves blood sugar primarily by enhancing insulin secretion and slowing nutrient absorption. Berberine improves blood sugar by making cells more sensitive to insulin and reducing hepatic glucose output. These are genuinely complementary mechanisms. While semaglutide increases insulin supply, berberine increases insulin demand at the cellular level, making each unit of insulin more effective.
The meta-analysis data suggests meaningful additive potential. Semaglutide alone reduces HbA1c by approximately 1.1%. Berberine alone reduces HbA1c by approximately 0.63%. Whether these effects are simply additive when combined, partially overlapping, or potentially synergistic remains unknown without direct clinical trials. But the theoretical ceiling for combined HbA1c reduction is higher than either agent alone, which matters for people whose blood sugar remains inadequately controlled on semaglutide monotherapy.
For people on semaglutide who find their initial weeks disappointing, berberine addition could theoretically accelerate metabolic improvements. The AMPK activation from berberine begins working within hours of the first dose, while semaglutide typically requires 4-5 weeks of dose escalation to reach therapeutic levels. This difference in onset timing means berberine could potentially fill the metabolic gap during early semaglutide treatment.
Cholesterol and cardiovascular support
Semaglutide primary metabolic benefits center on weight loss and blood sugar. Its effects on cholesterol are largely secondary to weight reduction. Berberine, in contrast, has direct cholesterol-lowering mechanisms through a pathway distinct from statins. Research published in Nature Medicine showed berberine increases LDL receptor expression on liver cells through a post-transcriptional mechanism, enhancing LDL clearance from the bloodstream.
The numbers from clinical studies are significant. Berberine reduced LDL cholesterol by 25%, triglycerides by 35%, and total cholesterol by 29% in hypercholesterolemic patients. A meta-analysis across 14 studies with 1,447 participants found average LDL reductions of 0.46 mmol/L (about 18 mg/dL). For semaglutide users who still have elevated lipid profiles despite weight loss, berberine offers a non-statin option for additional cardiovascular risk reduction.
This is especially relevant because many semaglutide users are managing metabolic syndrome, a cluster of conditions that includes obesity, insulin resistance, elevated blood sugar, high blood pressure, and dyslipidemia. Semaglutide addresses the first three powerfully. Berberine can help with all five, including the lipid abnormalities that semaglutide does not directly target. People who qualify for GLP-1 treatment based on BMI criteria often have multiple metabolic syndrome components, making the multi-targeted approach of combining berberine with semaglutide particularly appealing for comprehensive metabolic improvement.
Gut microbiome and anti-inflammatory effects
Berberine influence on the gut microbiome adds a dimension that semaglutide does not directly provide. Research shows berberine inhibits pathogenic species like Erysipelotrichaceae and Alistipes while increasing beneficial SCFA-producing bacteria including Alloprevotella and Flavonifractor. These microbiome changes are associated with reduced systemic inflammation, improved intestinal barrier function, and enhanced metabolic signaling.
Chronic low-grade inflammation is a driver of insulin resistance and metabolic dysfunction. While semaglutide reduces inflammation indirectly through weight loss, berberine appears to reduce inflammation directly through multiple pathways including NF-kB inhibition, reduced oxidative stress, and microbiome modulation. For researchers exploring peptide approaches to gut health, understanding how berberine affects the gut ecosystem adds valuable context for protocol design. The gut-metabolic connection also explains why dietary choices like foods to avoid on GLP-1 medications matter so much. What you feed your microbiome directly affects how well berberine SCFA-promoting effects play out.
The PREMOTE study, published in Nature Communications, examined berberine effect on gut microbiome composition in people with type 2 diabetes. It found significant shifts in bacterial populations that correlated with improvements in metabolic parameters. These microbiome effects persisted throughout the treatment period, suggesting berberine produces durable changes in gut ecology rather than temporary perturbations.
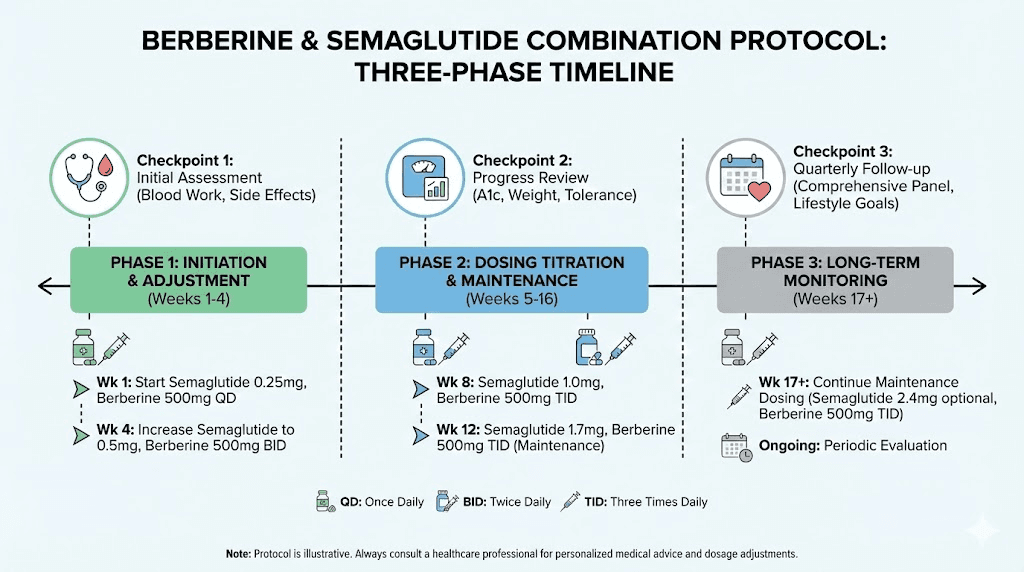
Specific protocols for combining berberine with semaglutide
If you and your healthcare provider decide to try the combination, the approach matters enormously. Random dosing without a structured protocol dramatically increases your risk of side effects while potentially reducing effectiveness.
Protocol 1: conservative start for beginners
This protocol is designed for people who are already stable on semaglutide and want to add berberine cautiously.
Prerequisite: You must be stable on your current semaglutide dose for at least 4-6 weeks with manageable side effects before adding berberine. If you are still experiencing significant nausea, constipation, or other GI issues from semaglutide, do not add berberine yet. Wait until your body has adjusted.
Week 1-2: Begin with 500 mg berberine once daily, taken with your largest meal. This is half the typical starting dose, deliberately conservative to assess tolerance alongside semaglutide. Monitor blood sugar more frequently than usual, at least twice daily if you have a glucose meter.
Week 3-4: If tolerated well, increase to 500 mg berberine twice daily, taken with breakfast and dinner. Continue monitoring blood sugar. Watch for any increase in GI symptoms beyond your semaglutide baseline.
Week 5-8: If still tolerated, you may increase to the standard dose of 500 mg three times daily with meals. This brings you to the 1,500 mg daily dose used in most clinical studies. Many people find that twice daily dosing (1,000 mg total) provides meaningful benefits with fewer GI side effects than the full three-times-daily protocol.
Ongoing monitoring: Track fasting blood glucose, any hypoglycemic episodes (shakiness, dizziness, rapid heartbeat, confusion), and GI symptoms weekly. Report any changes to your healthcare provider promptly.
Protocol 2: berberine-first approach
This protocol is for people currently taking berberine who are about to start semaglutide.
Week 1-4: Continue your current berberine dose. Begin semaglutide at the standard starting dose (0.25 mg weekly for most protocols). The combination of a new medication with an established supplement is generally better tolerated than starting both simultaneously.
Week 5-8: As semaglutide dose escalates (typically to 0.5 mg), reduce berberine to 500 mg twice daily if you were on 1,500 mg. This preemptive reduction accounts for the increased glucose-lowering effect as semaglutide reaches therapeutic levels.
Week 9-12: Reassess. Some people find they need less berberine as semaglutide dose increases. Others maintain the combination well. Blood sugar monitoring guides this decision. If fasting glucose drops below 70 mg/dL at any point, reduce berberine first before adjusting semaglutide.
For detailed information on semaglutide dosing in units, our calculator guides walk through exact conversion and administration steps. The semaglutide dosage calculator can help determine your precise dose requirements based on concentration and target amount. If you are working with compounded semaglutide, our 5mg/mL dosage chart and mixing chart provide the precise measurements needed for accurate dosing. Understanding proper injection technique and optimal injection sites ensures consistent absorption, which becomes more important when you are fine-tuning a multi-compound protocol.
Protocol 3: targeted combination for metabolic syndrome
This advanced protocol is specifically for people managing multiple metabolic syndrome components (elevated blood sugar, high cholesterol, high triglycerides, central obesity) under close medical supervision.
Foundation (Month 1): Establish semaglutide at 0.5 mg weekly. No berberine yet. Focus on tolerating semaglutide, adjusting your diet plan, and establishing baseline metabolic markers (fasting glucose, HbA1c, lipid panel, liver function tests).
Addition (Month 2): Add berberine 500 mg twice daily with meals. Continue semaglutide escalation per your prescriber protocol. Recheck lipid panel at 6 weeks to assess berberine impact on cholesterol and triglycerides.
Optimization (Month 3+): Based on lab results, either increase berberine to 1,500 mg daily (if lipids remain elevated), maintain at 1,000 mg daily (if labs show improvement), or reduce to 500 mg daily (if blood sugar runs low). This individualized approach produces better outcomes than a one-size-fits-all dose.
Target checkpoints:
Fasting glucose: 80-110 mg/dL (ideal range for combination therapy)
HbA1c: Below 6.5% (below 5.7% is normal range)
LDL cholesterol: Below 100 mg/dL (or per cardiologist recommendation)
Triglycerides: Below 150 mg/dL
No hypoglycemic episodes (blood sugar below 70 mg/dL)
Timing your doses for optimal results
Timing matters more than most people realize. Here are the key principles.
Semaglutide timing: Take your weekly injection on the same day each week. The best time of day for semaglutide is whenever you will remember consistently, though many people prefer morning administration to manage any nausea during waking hours.
Berberine timing: Always take berberine with meals. It is better absorbed with food, and taking it on an empty stomach significantly increases the risk of GI side effects. Space doses evenly throughout the day if taking multiple doses.
Injection day consideration: Some people experience more pronounced GI effects on the day of their semaglutide injection. If this applies to you, consider skipping your berberine dose on injection day and resuming the following day. This small adjustment can meaningfully reduce the GI burden during the peak effect window of your semaglutide dose.
The metformin timing rule: If you also take metformin, do not take berberine within two hours before your metformin dose. Research shows berberine taken two hours before metformin can increase metformin blood levels, potentially amplifying side effects. Taking them simultaneously does not appear to cause this interaction, but spacing them by at least two hours in either direction provides an additional safety margin.
Berberine vs semaglutide: head-to-head comparison
Understanding how these two compounds compare directly helps clarify what each brings to the combination and what you can realistically expect from each one alone.
Factor | Berberine | Semaglutide |
|---|---|---|
Type | Natural supplement (alkaloid) | Prescription GLP-1 receptor agonist |
Primary mechanism | AMPK activation | GLP-1 receptor agonism |
Weight loss | 2-4 kg (modest) | 14.9-17.4% body weight (significant) |
HbA1c reduction | ~0.63% | ~1.1% |
Fasting glucose reduction | ~0.82 mmol/L (15 mg/dL) | ~1.2-1.8 mmol/L (22-32 mg/dL) |
LDL reduction | ~25% | Minimal direct effect |
Triglyceride reduction | ~35% | Secondary to weight loss |
Appetite suppression | Minimal | Significant |
GI side effects | Moderate (diarrhea, gas, cramping) | Common (nausea, constipation, diarrhea) |
Administration | Oral, 2-3 times daily | Weekly subcutaneous injection |
Prescription required | No (OTC supplement) | Yes |
Onset of effects | Days to weeks | 4-5 weeks (full dose escalation) |
Cost (monthly) | $15-40 | $300-1,300+ (varies by source) |
Evidence quality | Moderate (many small studies) | High (large RCTs, FDA-approved) |
The comparison makes the complementary nature obvious. Semaglutide dominates in weight loss and appetite control. Berberine offers direct lipid benefits and insulin sensitization that semaglutide does not provide. Neither is a replacement for the other. They address metabolic dysfunction from different angles, which is precisely why the combination interests researchers and clinicians.
For those exploring how semaglutide compares to other GLP-1 medications, our semaglutide vs tirzepatide comparison provides a detailed side-by-side analysis. Understanding how different GLP-1 agonists compare helps contextualize where berberine supplementation might fit into various treatment approaches. Some researchers also look at retatrutide compared to semaglutide as the next-generation options continue to evolve. The landscape of triple agonist comparisons is growing more complex, which makes supplement optimization even more relevant as people try to maximize outcomes from whichever GLP-1 medication they choose. For a broader view of Ozempic alternatives and how they compare on cost, efficacy, and accessibility, our dedicated guide covers the full range of options.
The cost difference also deserves attention. Berberine supplements cost $15-40 per month. Semaglutide, even through compounding pharmacies, runs significantly higher. For people managing tight budgets, berberine addition represents a relatively inexpensive way to potentially enhance metabolic outcomes. Our peptide cost calculator can help you understand the overall financial picture of your protocol.
Why berberine is not "nature ozempic"
Social media has labeled berberine as "nature Ozempic." This comparison is misleading and potentially dangerous. The weight loss difference alone should end the comparison. Berberine produces 2-4 kg of weight loss. Semaglutide produces 15-17% body weight reduction. For a 200-pound person, that is roughly 5-9 pounds from berberine versus 30-34 pounds from semaglutide. These are not comparable results.
The AAFP (American Academy of Family Physicians) has specifically warned that berberine "lacks rigorous evidence" and has "potential harms" when positioned as an alternative to proven GLP-1 medications. The evidence base for berberine, while growing, consists largely of small studies with heterogeneous designs and high risk of bias. The STEP trial program for semaglutide involved thousands of participants in rigorously controlled, multicenter trials.
Where the comparison has some validity is in the overlapping mechanisms. Berberine does stimulate GLP-1 secretion, as discussed earlier. It does improve blood sugar control. It does offer metabolic benefits. But positioning it as an equivalent alternative to a proven pharmaceutical agent does a disservice to people who need the stronger intervention that prescription GLP-1 medications provide. Berberine is a supplement that can complement semaglutide. It is not a substitute for it.
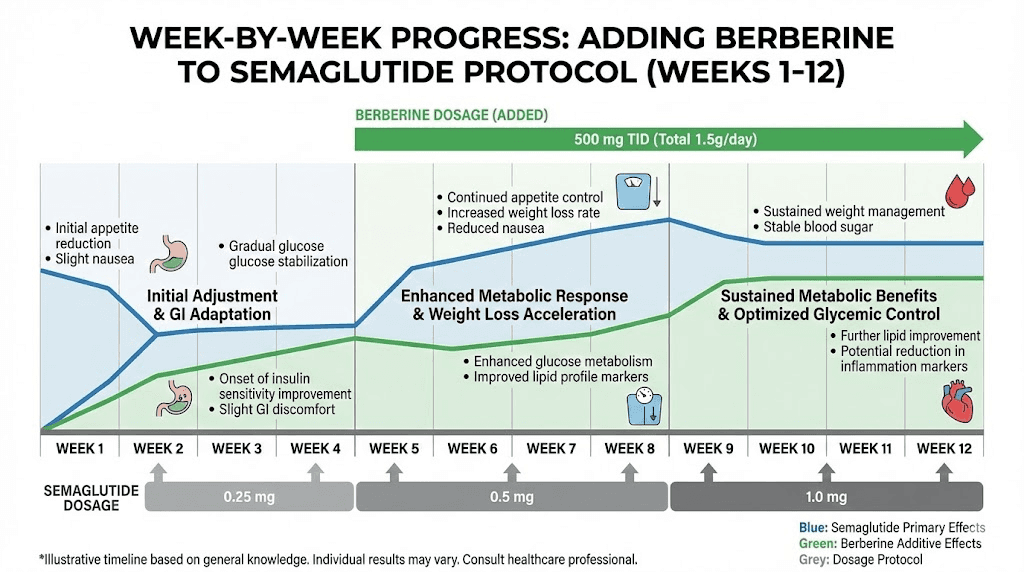
What to expect week by week when adding berberine to semaglutide
Understanding the timeline helps set realistic expectations and reduces anxiety about normal adjustment symptoms. Here is what most people experience when adding berberine to an established semaglutide protocol.
Week 1-2: the adjustment window
The first two weeks are about tolerance, not results. You are introducing a new compound to a GI tract already altered by semaglutide. Expect possible increases in gas, mild bloating, or looser stools. Some people notice no change at all. Others find the first few days uncomfortable before their digestive system adapts. If you followed the conservative protocol and started at 500 mg once daily, these symptoms should be manageable.
Blood sugar may drop slightly, particularly in the 2-4 hours after your berberine dose. This is the AMPK activation working. If you have a glucose monitor, you might see post-meal glucose peaks become slightly lower and shorter. This is a positive sign, not a problem, unless readings drop below 70 mg/dL.
Week 3-4: early metabolic shifts
By week three, GI symptoms typically stabilize. If you increased to 500 mg twice daily at this point, watch for a brief recurrence of digestive adjustment. Most people adapt within 3-5 days of a dose increase.
Fasting blood glucose may begin trending lower. The combined effect of semaglutide GLP-1 activation and berberine AMPK stimulation is now working on two fronts simultaneously. Some people report slightly improved energy levels, which could reflect better glucose utilization at the cellular level. The relationship between semaglutide and energy is complex, and berberine may add a positive dimension by reducing the energy fluctuations associated with insulin resistance.
Week 5-8: measurable changes begin
This is when lab values start to reflect the combination. If you had blood work done before starting berberine, the 6-8 week mark is ideal for follow-up labs. You may see reductions in fasting glucose, improvements in cholesterol ratios (particularly LDL and triglycerides), and potentially lower inflammatory markers like CRP.
Weight loss patterns may or may not change noticeably. Remember, berberine modest weight loss effect (2-4 kg over months) is small compared to semaglutide dramatic results. The before and after results from semaglutide primarily reflect the GLP-1 mechanism, not supplementation. Berberine contribution is more metabolic fine-tuning than scale-moving transformation.
Week 9-12: assessment and optimization
At the 12-week mark, you have enough data to make an informed decision about continuing. Compare your baseline labs to current values. Has fasting glucose improved? Have lipid numbers shifted? Are you tolerating the combination without significant GI distress? If all answers are yes, the combination is working for you. If improvements are minimal and side effects persist, berberine may not be providing sufficient benefit to justify continued use.
This is also when some people discover they can optimize timing and dosing for their specific needs. Maybe twice daily works better than three times daily. Maybe taking berberine with lunch and dinner but not breakfast aligns better with their semaglutide injection schedule. Individual optimization happens through experience, not rigid protocols.
Managing side effects when using both
The most common reason people abandon the berberine-semaglutide combination is side effects. Understanding what to expect and how to manage problems proactively makes the difference between a sustainable protocol and one that lasts two weeks before frustration wins.
Gastrointestinal management strategies
GI side effects are the number one complaint. Both compounds affect the digestive system, and combining them can amplify discomfort beyond what either causes alone. Here are specific strategies that help.
Start low, go slow. This cannot be overstated. Beginning berberine at the full 1,500 mg daily dose while already on semaglutide is asking for trouble. The conservative protocol outlined above (starting at 500 mg once daily) exists for exactly this reason.
Never take berberine on an empty stomach. This single rule prevents most acute GI reactions. Berberine is significantly less irritating when buffered by food. Take it at the beginning of your meal, not after, and not between meals.
Separate your problem windows. If semaglutide causes nausea primarily on days 1-2 after injection, and berberine causes discomfort at certain times, map these windows and avoid overlap. Some people skip berberine for 24-48 hours after their semaglutide injection, then resume at full dose. This intermittent approach sacrifices some berberine consistency but dramatically improves tolerability.
Choosing the right foods while on semaglutide becomes even more important when adding berberine. High-fiber, whole-food meals provide a better buffer for berberine absorption and help manage the slowed gastric emptying from semaglutide. Bland, easy-to-digest foods on high-symptom days reduce the overall GI burden. Our guides on the best foods to eat on semaglutide and foods to avoid on semaglutide provide specific meal frameworks that work well for combination protocols. Getting enough protein is especially important, and protein shakes designed for GLP-1 users can help meet requirements when appetite is suppressed.
Consider berberine form. Standard berberine hydrochloride is the most studied form but also the most likely to cause GI issues. Dihydroberberine, a metabolite form, may offer better absorption with fewer digestive side effects, though the research is more limited. Some people tolerate one form better than the other.
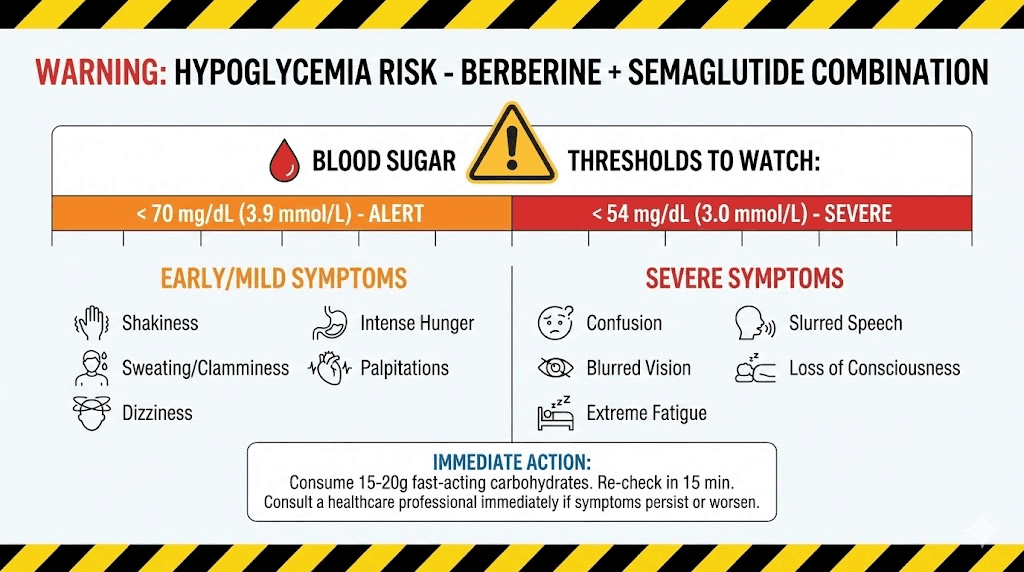
Monitoring for hypoglycemia
Hypoglycemia is the most dangerous potential side effect of the combination. Symptoms include shakiness, dizziness, excessive sweating, rapid heartbeat, confusion, irritability, and blurred vision. If blood sugar drops below 70 mg/dL, it requires immediate treatment with fast-acting glucose.
Practical monitoring guidelines:
Check fasting blood glucose daily for the first two weeks after adding berberine
Check blood sugar before and two hours after meals during the first week
Always carry glucose tablets or a fast-acting sugar source
Set a low glucose alert on your continuous glucose monitor if you have one
Know the signs and do not dismiss early symptoms as "just feeling tired"
People with diabetes on additional glucose-lowering medications face the highest risk. If you are taking metformin, a sulfonylurea, or insulin alongside semaglutide, adding berberine creates three or four overlapping mechanisms all pushing blood sugar down. This requires close medical supervision and possibly dose adjustments to your prescription medications. The risks mirror those discussed in our guide on combining phentermine with semaglutide, where stacking multiple metabolically active agents requires careful coordination.
The energy effects of semaglutide can overlap with or mask hypoglycemic symptoms. If you normally feel energized on semaglutide and suddenly feel fatigued, check your blood sugar immediately rather than assuming it is a normal fluctuation. GLP-1 related fatigue has multiple possible causes, and hypoglycemia from berberine addition should be ruled out first before attributing tiredness to semaglutide itself. Headaches on GLP-1 medications can also signal blood sugar fluctuations that warrant investigation.
What the research says about berberine dosage
Berberine dosing is more nuanced than most supplement guides suggest. The "standard" dose of 500 mg three times daily (1,500 mg total) comes from the clinical trial literature, but this dose was studied in people taking berberine alone, not in combination with GLP-1 agonists. Adjustments are necessary when adding berberine to an existing semaglutide protocol.
Evidence-based dosing ranges
Most clinical studies have used daily doses between 900 mg and 2,000 mg, divided into two to four doses throughout the day. The sweet spot appears to be 1,000-1,500 mg daily for metabolic benefits. Below 900 mg daily, effects are less consistent. Above 2,000 mg daily, side effects increase without proportional benefit gains.
The landmark study by Yin et al. (2008) in Metabolism used 500 mg three times daily in newly diagnosed type 2 diabetic patients and found it reduced HbA1c by 2% and fasting blood glucose by 3.8 mmol/L, comparable to metformin at the same dose schedule. However, these patients were not on any other glucose-lowering medication. The additive effect with semaglutide would be substantially different.
For semaglutide combination use, a more conservative approach is recommended. Starting at 500 mg daily and titrating based on response rather than jumping to the full study dose accounts for the additional glucose-lowering effect already provided by semaglutide. Many people find that 500-1,000 mg daily provides meaningful metabolic support without excessive side effects when combined with a GLP-1 agonist.
Bioavailability and absorption considerations
Berberine has notoriously poor oral bioavailability, typically less than 5%. This means that out of every 500 mg capsule, your body actually absorbs less than 25 mg into systemic circulation. The rest is metabolized in the gut or excreted. Paradoxically, this poor absorption is partly why berberine has such potent effects on the gut microbiome and intestinal GLP-1 production, because most of the compound stays in the GI tract where it interacts directly with gut bacteria and intestinal cells.
Several strategies can improve berberine absorption. Taking it with meals increases absorption. Some formulations include piperine (black pepper extract) to inhibit berberine breakdown, though this also affects other medication metabolism. Dihydroberberine formulations claim 5x better absorption, but this means the effective dose is lower, so you would need to adjust accordingly.
Semaglutide slowed gastric emptying adds another variable. When food stays in the stomach longer, berberine taken with that food also stays in the stomach longer, potentially altering its absorption pattern. No study has specifically examined how GLP-1 agonist-induced delayed gastric emptying affects berberine bioavailability. This is one of many unknowns in the combination approach. For those using injectable versus oral delivery methods for their peptide protocols, the absorption dynamics differ significantly, and berberine GI transit time is affected differently depending on which semaglutide formulation you use.
Other supplements to consider (and avoid) with semaglutide
Berberine is not the only supplement semaglutide users ask about. Understanding the broader supplement landscape helps put the berberine decision in context and highlights which combinations have stronger or weaker evidence.
Supplements with evidence for semaglutide users
Vitamin B12: Semaglutide can reduce B12 absorption over time due to slowed gastric emptying and altered intrinsic factor dynamics. Supplementing B12 with semaglutide is widely recommended, particularly for long-term users. Methylcobalamin is the preferred form, as detailed in our semaglutide methylcobalamin guide.
Glycine: This amino acid supports multiple metabolic pathways and may help with semaglutide-related muscle preservation during weight loss. Our semaglutide with glycine guide covers the rationale and dosing in detail.
Fiber supplements: Given that both semaglutide and berberine can cause constipation, a psyllium husk or similar fiber supplement often helps maintain regularity. Start low (one teaspoon daily) and increase gradually.
Magnesium: Many people with metabolic syndrome are magnesium-deficient. Magnesium glycinate at 200-400 mg daily supports over 300 enzymatic processes including glucose metabolism and can help with the muscle cramps some semaglutide users report.
Probiotics: Given berberine effect on gut microbiome composition, a quality probiotic may help maintain bacterial diversity. Look for formulations containing Lactobacillus and Bifidobacterium strains with at least 10 billion CFU.
Supplements to use with caution alongside semaglutide
Alpha-lipoic acid: Another insulin-sensitizing supplement that could compound hypoglycemia risk. If combining with berberine and semaglutide, monitor blood sugar very closely.
Chromium: Enhances insulin sensitivity. Same hypoglycemia concern as above when stacked with multiple glucose-lowering agents.
Bitter melon extract: Contains compounds with insulin-mimetic properties. Adding this to semaglutide plus berberine creates yet another glucose-lowering mechanism. Not recommended without medical supervision.
The overlap with other GLP-1 supplements applies similarly to supplements recommended for tirzepatide users, since both medications work through GLP-1 receptor activation. Whether you are on semaglutide, oral tirzepatide, or other GLP-1 agonists, the berberine interaction considerations remain largely the same. Some researchers combine their GLP-1 protocol with peptides specifically chosen to complement Ozempic, and understanding how each addition affects the overall metabolic picture prevents accidental overcorrection.
The supplement landscape for GLP-1 users extends well beyond berberine. GLP-1 specific probiotics have emerged as another popular addition, targeting the gut microbiome from a different angle than berberine. While berberine promotes SCFA-producing bacteria through antimicrobial selectivity (killing bad bacteria while sparing good ones), probiotics directly introduce beneficial bacterial strains. The two approaches are theoretically complementary, though again, no clinical trial has studied the triple combination of semaglutide, berberine, and probiotics.
What to avoid entirely
High-dose niacin (vitamin B3): Can worsen blood sugar control, counteracting both semaglutide and berberine effects.
Goldenseal supplements: Goldenseal contains berberine. Taking goldenseal in addition to a berberine supplement means you are unknowingly doubling your berberine dose, which increases side effects and hypoglycemia risk.
St. John Wort: A potent CYP enzyme inducer that could alter berberine metabolism unpredictably. Also interacts with many prescription medications.
Alcohol also deserves mention. The question of drinking while on semaglutide is common, and adding berberine does not simplify the picture. Alcohol can independently lower blood sugar, and combining it with two glucose-lowering compounds increases hypoglycemia risk further. Moderate consumption with food is generally the safest approach, but individual tolerance varies widely. If you also take tirzepatide, the alcohol guidance for tirzepatide follows similar principles.
For people exploring phentermine vs semaglutide or considering whether phentermine qualifies as a GLP-1, the supplement interaction profile changes significantly. Phentermine is a stimulant with different cardiovascular and metabolic effects than semaglutide, and adding berberine to phentermine carries distinct risks that should not be conflated with the semaglutide combination discussed here.
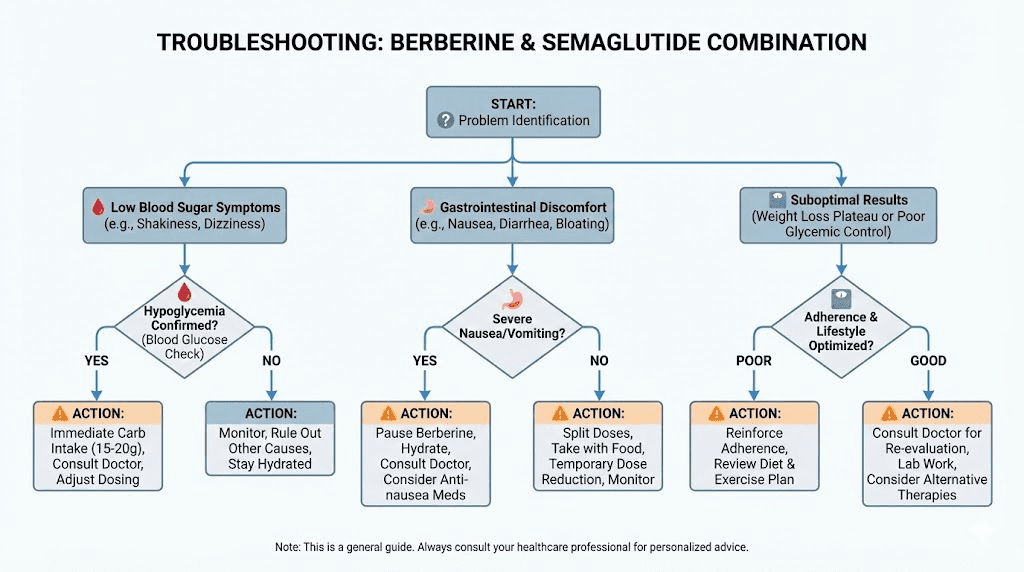
Real-world troubleshooting
Theory and practice often diverge. Here are the most common problems people encounter when combining berberine with semaglutide, along with specific solutions.
Problem: GI side effects became intolerable after adding berberine
Solution: Cut berberine dose in half immediately. If you were at 1,500 mg daily, drop to 500 mg once daily with your largest meal. Hold at this dose for two full weeks. If symptoms resolve, try increasing to 500 mg twice daily after the two-week stabilization period. If symptoms do not resolve at 500 mg daily, berberine may not be compatible with your GI tolerance on semaglutide. Not everyone can tolerate the combination, and that is a valid outcome, not a failure.
Problem: blood sugar dropping too low
Solution: Reduce berberine first, not semaglutide. Berberine is the addition to your protocol, and it is easier to adjust. Drop to the lowest effective dose (500 mg daily) and monitor for one week. If hypoglycemia continues, discontinue berberine and discuss with your provider whether your semaglutide dose needs adjustment. For guidance on semaglutide dose adjustments, our dosing chart covers the standard escalation and de-escalation protocols.
Problem: not seeing additional benefits from berberine
Solution: Give it time. Berberine effects on blood sugar and cholesterol typically require 8-12 weeks of consistent use to become measurable on lab work. If you have been taking berberine for less than 8 weeks, you may not have given it enough time. If 12 weeks pass without measurable improvement in any metabolic parameter, berberine may not provide meaningful additional benefit for your specific situation. Some people respond more strongly to berberine than others, and non-response is common.
Problem: weight loss stalled despite the combination
Weight loss plateaus on semaglutide are common and typically unrelated to berberine. Our comprehensive guide on why you are not losing weight on semaglutide covers the most common causes: dose too low, dietary choices undermining the caloric deficit, insufficient physical activity, metabolic adaptation, or medication interactions. Berberine adds modest metabolic support but cannot overcome fundamental caloric surplus or dose inadequacy. People who experience the four-week no-results frustration sometimes turn to supplements prematurely when the real issue is insufficient dose escalation or unrealistic timelines.
If you are experiencing a plateau, focus on the basics first. Are you eating enough protein? Are you moving your body regularly? Has your semaglutide dose been escalated appropriately? Is stress or sleep affecting your metabolism? Some people find success with a structured semaglutide diet plan that specifically accounts for reduced appetite. Others explore whether weight loss without exercise on semaglutide is realistic for their situation. Address these factors before assuming berberine supplementation should be solving the problem. The best stack of peptides and supplements for weight loss is the one that addresses your specific metabolic bottleneck, not a generic combination.
Problem: medication interactions with other prescriptions
Solution: This is where berberine CYP450 inhibition becomes clinically relevant. If you take statins (especially simvastatin or atorvastatin), certain antidepressants (SSRIs metabolized by CYP2D6), blood thinners (warfarin), or immunosuppressants (cyclosporine), berberine can increase their blood levels by slowing their metabolism. The combination of semaglutide and berberine itself may be safe, but berberine interaction with your other medications could create problems semaglutide never would alone.
Always provide your healthcare provider with a complete list of every medication and supplement you take. The interaction potential is not with semaglutide directly but with the broader medication profile that many semaglutide users have. Our guide on peptide safety and risk assessment covers the general principles of evaluating compound interactions.
Long-term considerations
The question of duration matters. How long should you take berberine alongside semaglutide? Is this a short-term metabolic boost or a long-term addition?
The honest answer is that nobody knows. Long-term studies on berberine supplementation beyond 24 weeks are scarce. Long-term studies on the berberine-semaglutide combination do not exist. What we can say is that berberine effects on blood sugar and cholesterol appear to persist as long as supplementation continues and reverse when it stops, similar to most metabolic interventions.
Some researchers take a cyclical approach: 12 weeks on berberine, 4 weeks off, then reassess whether to resume. This cycling strategy theoretically prevents tolerance development and gives the liver periodic breaks from CYP450 inhibition. Whether cycling is actually necessary or beneficial is unknown. It is a precautionary approach rather than an evidence-based one.
SeekPeptides members access detailed protocol databases, including combination supplement strategies for GLP-1 users, that are regularly updated as new research emerges. For researchers serious about optimizing their semaglutide protocols with evidence-based supplementation, having access to curated, current information is invaluable.
The duration of semaglutide treatment itself is an important consideration. Most people use semaglutide for months to years. The STEP 5 trial showed continued weight loss at two years. If you plan long-term semaglutide use, the decision about berberine supplementation becomes a long-term one as well, which makes safety monitoring and periodic lab work even more important. The concern about semaglutide withdrawal symptoms and weight regain also affects berberine strategy. If you eventually discontinue semaglutide, maintaining berberine supplementation could provide some continued metabolic support during the transition, though the magnitude of that support would be far smaller than what semaglutide provided.
Long-term users should also consider whether GLP-1 related hair loss, which some people experience during rapid weight loss, warrants additional nutritional attention. Berberine does not directly address this concern, but ensuring adequate protein, biotin, and iron intake becomes more important when multiple compounds are influencing metabolic rate and nutrient absorption.
Special populations and considerations
PCOS and insulin resistance
Polycystic ovary syndrome involves significant insulin resistance, and both berberine and semaglutide have been studied independently for PCOS management. Berberine has shown particular promise in PCOS research, with studies demonstrating improved ovulation rates, reduced androgen levels, and better insulin sensitivity markers. For women with PCOS who are on semaglutide, berberine addition could theoretically address the hormonal dysregulation that semaglutide does not directly target.
However, PCOS involves complex hormonal interactions. Any supplementation changes should be discussed with an endocrinologist or reproductive endocrinologist who understands the full clinical picture. Women exploring peptide-based weight loss approaches and those dealing with menopause-related weight gain face unique hormonal variables that affect how both semaglutide and berberine perform. The broader relationship between peptides and hormone balance adds additional layers of complexity for women managing reproductive health alongside metabolic optimization. Understanding these interconnections helps avoid the common mistake of optimizing one system while inadvertently disrupting another.
Type 2 diabetes on multiple medications
People with type 2 diabetes often take multiple medications: metformin, semaglutide, possibly a sulfonylurea or SGLT2 inhibitor, statins, and blood pressure medications. Adding berberine to this medication stack introduces interactions at multiple levels. The glucose-lowering effect stacks with metformin and semaglutide. The CYP450 inhibition affects statin metabolism. The P-glycoprotein inhibition could alter several drug levels simultaneously.
For this population, berberine should only be added under close medical supervision with regular lab monitoring. The potential benefits are real, but so are the interaction risks when the medication list grows beyond two or three agents.
People using compounded semaglutide
Many people access semaglutide through compounding pharmacies rather than brand-name products. Our compounded semaglutide guide covers the differences in detail. When using compounded semaglutide, the same berberine interaction principles apply, but there may be additional variables related to compounded formulation purity, concentration accuracy, and storage requirements. Understanding how to reconstitute semaglutide properly and storage requirements becomes even more important when you are managing multiple compounds in your protocol.
The pharmacy sourcing landscape for semaglutide continues to evolve, and quality varies significantly between providers. Other popular compounding sources include Olympia Pharmacy and Direct Meds. Ensuring you are getting properly compounded semaglutide is a prerequisite before optimizing your protocol with supplementation. If your semaglutide quality is inconsistent, adding berberine will not fix the underlying problem.
For those new to compounded semaglutide, understanding the preparation process is essential. Our guides on reconstituting semaglutide, mixing 5mg vials, and mixing 10mg vials cover the technical details. Proper storage in the refrigerator ensures potency throughout your vial life. The peptide reconstitution calculator removes guesswork from the preparation process.
The bottom line on berberine and semaglutide together
Combining berberine with semaglutide is plausible, potentially beneficial, and not without risk. The evidence for the combination is theoretical rather than proven by direct clinical trials. The mechanisms are complementary: semaglutide drives weight loss and appetite reduction through GLP-1 receptor activation while berberine enhances insulin sensitivity, lowers cholesterol, modulates the gut microbiome, and even stimulates additional GLP-1 production through different pathways.
The key principles for anyone considering this combination are straightforward. First, stabilize on semaglutide before adding berberine. Second, start berberine at a low dose and increase gradually. Third, monitor blood sugar frequently, especially in the first few weeks. Fourth, never combine them without informing your healthcare provider. Fifth, be prepared to reduce or discontinue berberine if side effects or interactions become problematic. And sixth, set realistic expectations. Berberine is a supplement with modest but real metabolic effects. It is not going to transform your semaglutide results overnight.
For researchers who want to explore this combination intelligently, SeekPeptides provides comprehensive protocol guides, dosing calculators, and a community of experienced researchers who have navigated these exact decisions. The semaglutide dosage calculator helps ensure your base medication dosing is dialed in before adding supplementation, and our peptide calculator covers broader protocol planning needs.
Making informed decisions about supplement-medication combinations requires good data, careful monitoring, and honest assessment of both benefits and risks. The worst approach is guessing. The best approach is systematic, measured, and supervised by someone who understands the full picture of your health. If you are just getting started with peptides and GLP-1 research, building a solid foundation of knowledge before adding supplements like berberine will serve you far better than diving into complex stacking protocols prematurely. For those further along in their journey, our peptide stacking guide covers the principles that apply to any multi-compound protocol, whether pharmaceutical or supplemental.
For researchers serious about optimizing their metabolic protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
Can I take berberine and semaglutide at the same time of day?
Yes, but spacing them may reduce GI side effects. Take semaglutide as prescribed (weekly injection at any time). Take berberine with meals. If you inject semaglutide in the morning, you can take your first berberine dose with lunch or dinner to reduce overlap of GI effects. There is no strict pharmacological reason to separate them by hours, since semaglutide is injected and berberine is oral, they enter the body through different routes entirely.
Will berberine make my semaglutide work better for weight loss?
Berberine is unlikely to dramatically improve semaglutide weight loss results. The appetite suppression from semaglutide is far more powerful than anything berberine provides. Where berberine may help is with metabolic parameters like insulin sensitivity, cholesterol, and blood sugar control that contribute to overall metabolic health beyond the number on the scale. Think of berberine as metabolic fine-tuning, not a weight loss amplifier.
How long should I wait after starting semaglutide before adding berberine?
Most experts recommend waiting at least 4-6 weeks after reaching a stable semaglutide dose. This means completing the initial dose-escalation period and allowing your body to adjust to semaglutide side effects before introducing another compound that affects the GI tract and blood sugar. If you are still experiencing significant nausea or digestive issues from semaglutide at the 6-week mark, wait longer until those symptoms stabilize.
Is berberine safe to take with compounded semaglutide?
The same principles apply whether you use brand-name or compounded semaglutide. The active ingredient is the same semaglutide peptide. The interaction profile with berberine does not change based on the source. However, ensure your compounded semaglutide is from a reputable pharmacy and properly stored, as our guide on compounded semaglutide storage explains.
Can I take berberine with tirzepatide instead of semaglutide?
The same general principles apply to tirzepatide (Mounjaro/Zepbound), which also activates GLP-1 receptors along with GIP receptors. The blood sugar lowering and GI side effect concerns are similar. Our semaglutide vs tirzepatide side effects comparison covers how these medications differ, and our tirzepatide supplement guide addresses supplementation in that specific context.
What blood tests should I get before combining berberine with semaglutide?
Baseline labs should include fasting glucose, HbA1c, comprehensive metabolic panel (includes liver and kidney function), and a full lipid panel (total cholesterol, LDL, HDL, triglycerides). Repeat these at 8-12 weeks after adding berberine to assess response. Liver function tests are particularly important because berberine inhibits CYP450 enzymes and could theoretically affect liver enzyme levels, especially in people with pre-existing liver conditions.
Does berberine interfere with semaglutide absorption?
No. Semaglutide is administered by subcutaneous injection, which means it enters the bloodstream through tissue under the skin, bypassing the GI tract entirely. Berberine is taken orally and acts primarily in the gut. They do not compete for absorption. Even for oral semaglutide formulations, the absorption mechanism is specifically engineered to work in the stomach environment and is unlikely to be significantly affected by berberine taken at a different time.
Should I stop berberine if I get a stomach virus while on semaglutide?
Yes. Any acute illness that causes vomiting or diarrhea increases dehydration and hypoglycemia risk. Temporarily discontinue berberine during acute GI illness. Maintain semaglutide unless your healthcare provider advises otherwise, as stopping and restarting can cause its own side effect issues. Resume berberine at a reduced dose once symptoms resolve and you are eating normally again.
Can I take berberine if I am switching from semaglutide to tirzepatide?
Yes, but time the transition carefully. The switching process between GLP-1 medications involves dose adjustments and a new side effect adaptation period. Consider pausing berberine during the switch and reintroducing it once you are stable on the new medication, typically 4-6 weeks after reaching your target tirzepatide dose. The side effect profiles differ between semaglutide and tirzepatide, so your berberine tolerance may change as well.
Is berberine better than metformin for semaglutide users?
These are fundamentally different categories. Metformin is a prescription medication with decades of clinical evidence and FDA approval. Berberine is a supplement with growing but more limited evidence. For people with diabetes, metformin remains the standard of care and should not be replaced with berberine without medical guidance. For people without diabetes who want additional metabolic support beyond semaglutide, berberine may be an option worth discussing with their provider since it does not require a prescription.
Does berberine help with the nausea from semaglutide?
No. Berberine does not have anti-nausea properties and may actually worsen nausea by adding GI irritation. If semaglutide nausea is a significant problem, address it directly through dose timing, dietary adjustments, and if necessary, anti-nausea medications. Do not add berberine hoping it will improve digestive symptoms. Understanding the optimal timing for semaglutide and choosing the best time for your GLP-1 injection often makes more difference for nausea management than any supplement.
Can I use berberine with oral semaglutide instead of injectable?
The same principles apply to oral semaglutide formulations and sublingual semaglutide. However, oral semaglutide has specific absorption requirements (empty stomach, limited water, 30-minute fasting window) that should not be disrupted by berberine. Take berberine with a later meal, never during the oral semaglutide absorption window.
What if I want to use berberine with a next-generation GLP-1 like retatrutide?
Retatrutide is a triple agonist (GLP-1/GIP/glucagon) that produces even greater weight loss than semaglutide or tirzepatide in clinical trials. The retatrutide vs semaglutide comparison shows key differences in mechanism and potency. Because retatrutide has stronger metabolic effects, the margin for adding berberine safely may be narrower. The hypoglycemia risk could be higher, and the GI side effects more pronounced. Wait for more clinical data before combining berberine with triple agonists. The cagrilintide-semaglutide combination (CagriSema) is another emerging approach that may change the supplementation calculus as more data becomes available.
External resources
Berberine-induced GLP-1 and type 2 diabetes mechanisms - PubMed review
Semaglutide for overweight and obesity treatment - PMC comprehensive review
PREMOTE study: Berberine, gut microbiome, and type 2 diabetes - Nature Communications
In case I do not see you, good afternoon, good evening, and good night. May your blood sugar stay stable, your protocols stay evidence-based, and your metabolic health stay on an upward trajectory.