Feb 27, 2026

Tired of stepping on the scale and seeing the number go up, not down, while injecting tirzepatide every week? You are not imagining things. You are not failing. And you are certainly not alone.
Thousands of people report gaining weight on tirzepatide after weeks or months of steady loss. Some gain back a few pounds. Others watch the scale climb past their starting weight. The confusion is real. The frustration is worse. You are doing everything you were told to do, and the medication that was supposed to solve the problem seems to be making it worse.
Here is the thing nobody talks about. Tirzepatide is the most effective weight loss peptide available, with clinical trials showing average reductions of 15 to 22 percent of body weight over 72 weeks. But that is an average. Averages hide enormous variation. Some people lose 30 percent. Others plateau early. A small but significant number actually gain weight while taking it. And the reasons stretch far beyond willpower or calorie counting.
This guide breaks down every documented cause of weight gain on tirzepatide, from fluid shifts and metabolic adaptation to medications working against you and medical conditions hiding underneath. More importantly, it gives you a concrete plan to identify your specific cause and fix it. No vague advice. No generic suggestions. Specific protocols backed by research and real-world experience from the SeekPeptides community.
How tirzepatide causes weight loss in the first place
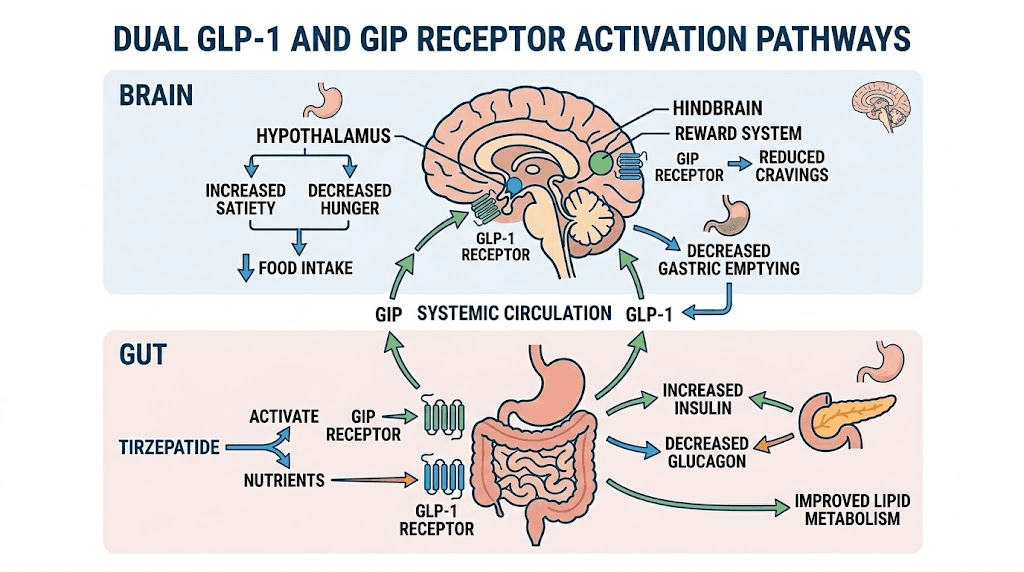
Before you can understand why weight gain happens, you need to understand the mechanism that produces weight loss. Tirzepatide is a dual GLP-1 and GIP receptor agonist. That means it activates two separate hormonal pathways simultaneously, something no other weight loss medication does.
The GLP-1 pathway slows gastric emptying. Food sits in your stomach longer. You feel full faster. You stay full longer. Your brain receives satiety signals it was not receiving before. The GIP pathway amplifies these effects and adds its own contribution to appetite suppression through central nervous system activity.
Together, these two pathways produce several measurable effects. Appetite decreases dramatically. Most people report eating 30 to 40 percent fewer calories without trying. Metabolic rate changes. Food preferences shift toward lighter, less calorie-dense options. And insulin sensitivity improves, which changes how your body stores and uses fat.
The SURMOUNT-1 trial demonstrated that participants taking the highest dose of tirzepatide lost an average of 21.3 percent of their body weight over 72 weeks. Of that weight loss, approximately 75 percent came from fat mass and 25 percent from lean mass. That ratio matters. Keep it in mind. It will come up again when we discuss muscle loss and metabolic slowdown.
When this system works correctly, weight comes off steadily. Not linearly, never linearly, but the overall trend moves down. When weight starts moving up instead, something is interfering with one or more of these pathways. Finding that interference is the key to fixing the problem.
Medical reasons you might be gaining weight on tirzepatide
Not all weight gain is about what you eat or how much you move. Some of it is purely physiological, and some of it involves other medications or medical conditions actively working against tirzepatide. Let us start with the causes that have nothing to do with your behavior.
Water retention and fluid shifts
This is the most common reason for sudden weight gain on tirzepatide, and the most misunderstood. Your body weight fluctuates by 2 to 6 pounds daily based on hydration, sodium intake, glycogen storage, and hormonal cycles. That is a normal range. It does not reflect fat gain.
When you start tirzepatide, your body rapidly improves glucose control. Better glucose control changes how your kidneys handle sodium and water. During the first 2 to 8 weeks, this adjustment alone can add 2 to 6 pounds of water weight, even while fat is actively being lost. Your measurements might shrink while the scale goes up.
Constipation compounds this problem. Tirzepatide constipation affects roughly 15 to 20 percent of users, particularly during dose increases. Backed-up stool adds physical weight. It also slows digestion further, increasing water retention throughout the digestive tract. Managing constipation is not just a comfort issue. It directly affects scale readings.
Menstrual cycles create additional fluid fluctuations. Women may see the scale jump 3 to 7 pounds around their period due to estrogen-driven water retention. When weight loss on tirzepatide is happening at a rate of 1 to 2 pounds per week, a single menstrual cycle can wipe out an entire month of progress on the scale. The fat loss is still happening. You just cannot see it.
Metabolic adaptation slowing your progress
Your body does not want to lose weight. That sounds dramatic, but it is biologically accurate. Every pound you lose triggers a cascade of metabolic adjustments designed to bring you back to your previous weight. This process is called adaptive thermogenesis, and it is one of the biggest obstacles to sustained weight loss on any medication.
Here is what happens. As you lose weight, your basal metabolic rate drops. A smaller body burns fewer calories at rest. That is simple physics. But the drop goes beyond what physics predicts. Your body actually becomes more efficient, burning 10 to 15 percent fewer calories than expected for your new weight. Hormones shift. Ghrelin, the hunger hormone, increases. Leptin, the satiety hormone, decreases. Your thyroid function may subtly downregulate.
A fascinating study published in Cell Metabolism found that tirzepatide did not significantly impact metabolic adaptation in humans, but it did increase fat oxidation. This means the medication helps you burn more fat specifically, even as your overall metabolic rate declines. However, if your calorie intake stays the same while your metabolic rate drops, weight loss stalls. Eat even slightly more, and weight gain begins.
Most people hit this wall between weeks 24 and 36. The SURMOUNT clinical trials confirmed this timeline. Weight loss typically plateaus after 6 to 9 months, regardless of dose. This is not the medication failing. This is biology doing exactly what it evolved to do.
Lean muscle loss lowering your metabolic rate
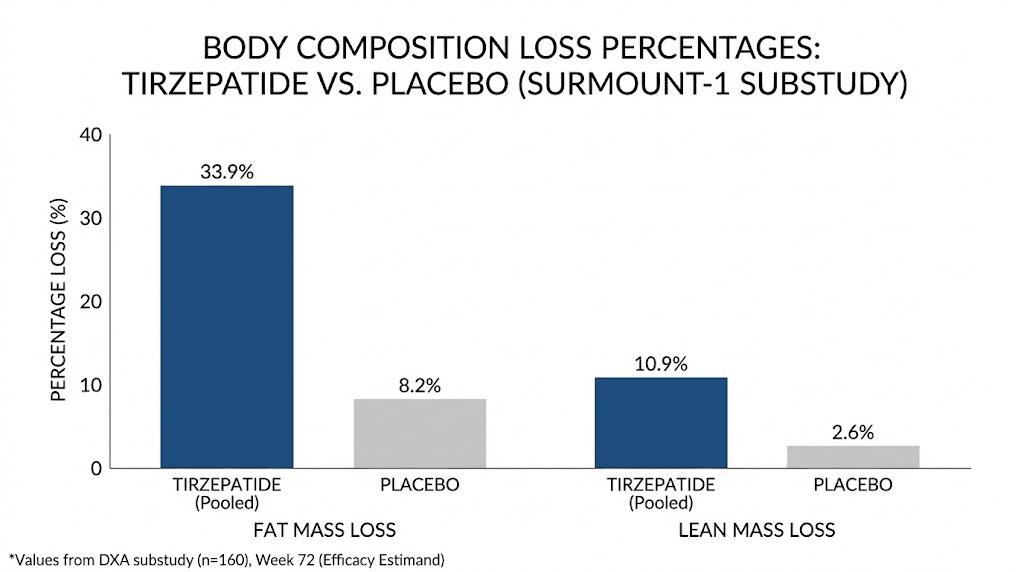
This one is critical. Data from the SURMOUNT-1 trial showed that approximately 25 percent of weight lost on tirzepatide comes from lean mass, not fat. Lean mass includes muscle. Muscle burns calories at rest. Lose enough muscle, and your metabolism drops significantly beyond what would happen from fat loss alone.
Here are the numbers. The change in body weight, fat mass, and lean mass from baseline to week 72 was 21.3 percent, 33.9 percent, and 10.9 percent respectively with tirzepatide. That 10.9 percent lean mass reduction represents a meaningful metabolic disadvantage. Each pound of muscle burns approximately 6 to 7 calories per day at rest. Lose 10 pounds of muscle, and your daily calorie burn drops by 60 to 70 calories. Over months, that adds up to real weight regain.
The fix is straightforward. Resistance training and adequate protein intake protect lean mass during weight loss. Without them, you are essentially lowering your metabolic ceiling with every pound lost, making future weight gain progressively easier.
Tolerance to gastrointestinal side effects
This is the sneaky one. Early in treatment, tirzepatide side effects like nausea, reduced appetite, and food aversions drive dramatic calorie reduction. Many people report eating 800 to 1200 calories daily during the first few months because they simply cannot eat more. The weight falls off quickly.
Then the side effects fade. Your body adapts. The nausea subsides. Appetite slowly returns. You do not notice at first because the return is gradual. A few extra bites here. A snack you would not have wanted last month. An extra serving that suddenly seems reasonable. Before you realize what is happening, your calorie intake has climbed from 1000 to 1800 calories daily.
Meanwhile, your metabolism has dropped from the weight loss. You are now eating more while burning less. The math starts working against you. This pattern is so common that researchers have given it a name: the GI tolerance paradox. The very side effects that drove your initial weight loss disappear, removing one of the key mechanisms that kept calories low.
Subtherapeutic dosing
Tirzepatide follows a titration schedule for a reason. You start at 2.5 mg and gradually increase to 5 mg, then 7.5 mg, 10 mg, 12.5 mg, or 15 mg. Each increase brings stronger appetite suppression and metabolic effects.
Some people stay at lower doses too long. Maybe the side effects scared them. Maybe their provider was cautious. Maybe they could not afford the higher dose. Whatever the reason, remaining at 2.5 or 5 mg when your body has adapted to that dose means the medication is no longer providing sufficient appetite suppression. The threshold at which tirzepatide meaningfully reduces food intake rises as your body acclimates.
Check your dosage in units against the recommended titration schedule. If you have been at the same dose for more than 8 weeks without progress, a dose increase may be exactly what you need. Consult your provider about moving to the next step in the dosage chart.
Medications that promote weight gain
This is one of the most overlooked causes. Certain medications actively promote weight gain through mechanisms that can partially or fully counteract tirzepatide. If you are taking any of the following, they may be sabotaging your results.
Antipsychotics are the biggest offenders. Olanzapine, quetiapine, and risperidone cause weight gain of 10 to 30 pounds in many users through mechanisms involving histamine, serotonin, and dopamine receptor blockade. These drugs increase appetite, reduce physical activity, and alter fat storage patterns. Research published in the American Journal of Psychiatry documented that GLP-1 receptor agonist weight loss was significantly attenuated in patients concurrently using certain psychiatric medications.
Antidepressants vary widely. Mirtazapine, paroxetine, and amitriptyline are notorious for weight gain. Mirtazapine alone can cause 5 to 12 percent body weight increase through appetite stimulation and reduced energy expenditure. Other antidepressants like bupropion tend to be weight-neutral or even promote slight weight loss. The specific medication matters enormously.
Corticosteroids like prednisone increase appetite, promote fluid retention, alter fat distribution, and reduce insulin sensitivity. Even short courses can add several pounds. Chronic steroid use creates a metabolic environment that fights weight loss at every level.
Insulin and sulfonylureas promote weight gain as part of their mechanism of action. Sulfonylureas cause an average gain of 4 to 5 pounds by stimulating insulin release. Insulin itself promotes fat storage. If you are taking tirzepatide for type 2 diabetes alongside these medications, the weight gain effects can partially offset tirzepatide benefits.
Anticonvulsants including gabapentin and pregabalin cause weight gain in 10 to 25 percent of users. Gabapentin in particular increases appetite and reduces physical activity through sedation. Beta-blockers slow metabolism by 5 to 10 percent in some individuals, though the effect varies by specific medication. Lithium and valproate both promote significant weight gain through multiple pathways.
The critical question is not whether to stop these medications. Never stop prescribed medication without medical guidance. The question is whether alternatives exist that are weight-neutral. Many psychiatric and neurological medications have alternatives that achieve the same therapeutic effect without the metabolic burden. Talk to your prescribing physician about this specific concern.
Underlying medical conditions
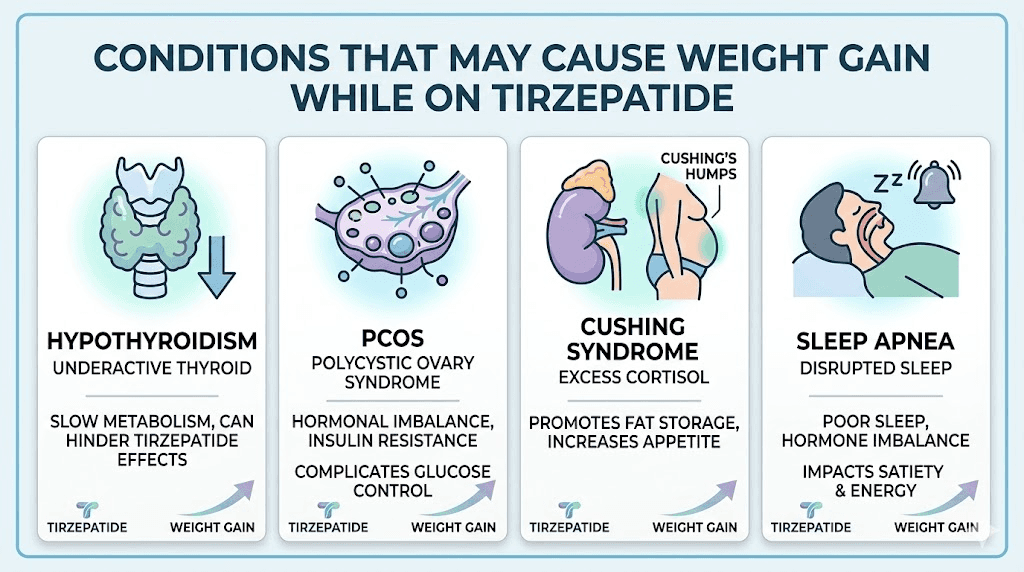
Several medical conditions can cause weight gain that overpowers tirzepatide effects. The most common is hypothyroidism. An underactive thyroid reduces metabolic rate by 10 to 30 percent, depending on severity. Subclinical hypothyroidism, where TSH is elevated but T4 remains normal, is easy to miss on standard blood panels and can silently undermine weight loss efforts.
Cushing syndrome, whether from excess cortisol production or chronic steroid use, causes characteristic central weight gain. The distribution pattern is distinctive: fat accumulates around the midsection, face, and upper back while limbs may remain relatively thin. If your weight gain follows this pattern, cortisol testing should be a priority.
Polycystic ovary syndrome (PCOS) affects up to 10 percent of women and creates insulin resistance that directly opposes tirzepatide mechanisms. PCOS weight gain tends to be resistant to standard interventions. Women with PCOS may need higher tirzepatide doses and additional interventions like metformin to see results comparable to the general population.
Less common but worth investigating: sleep apnea disrupts hormonal regulation of appetite and metabolism. Insulin resistance beyond what tirzepatide can overcome. Hormonal imbalances including perimenopausal changes that shift fat distribution and storage patterns.
Menstrual cycle and hormonal fluctuations
Tirzepatide and menstrual changes deserve their own section because the impact is so significant and so commonly confused with actual weight gain.
Tirzepatide does not directly target reproductive hormones. It does not alter estrogen or progesterone. But rapid weight loss changes your hormonal landscape indirectly. Body fat produces estrogen. Lose fat quickly, and estrogen levels shift. This can temporarily change cycle timing, flow intensity, and the severity of premenstrual symptoms, including water retention.
Women on tirzepatide commonly report weight fluctuations of 3 to 7 pounds around their menstrual cycle. That is larger than typical fluctuations because tirzepatide-driven metabolic changes amplify the hormonal effects on fluid balance. Some months the weight drops right back after menstruation. Other months it lingers for an extra week. The unpredictability adds psychological stress on top of the physical frustration.
Most menstrual-related changes stabilize within 3 to 6 months as your body adapts to both the medication and your new weight. If they persist beyond that window, or if cycle changes are dramatic, consult your healthcare provider to rule out other causes.
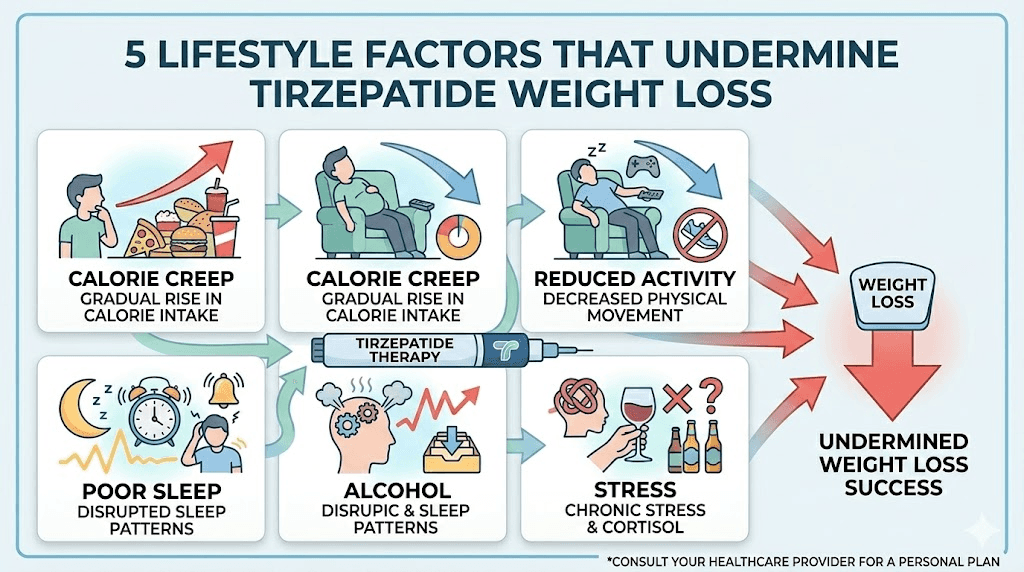
Lifestyle factors that undermine tirzepatide results
Medical causes are only part of the picture. Lifestyle factors play an equal or greater role in determining whether tirzepatide produces sustained weight loss or frustrating plateau and regain. These are the factors you can control, which makes them both the most actionable and the most uncomfortable to confront.
Calorie creep and the false security of appetite suppression
Tirzepatide reduces appetite. It does not eliminate it. And appetite suppression is not constant. It fluctuates throughout the day, throughout the week, and throughout your treatment. The danger lies in the gap between perceived appetite and actual calorie consumption.
During peak appetite suppression, you eat less without thinking about it. Meals are smaller. Snacking disappears. You might skip a meal entirely because you genuinely forgot. This feels effortless. It also sets a dangerous expectation that weight loss should always feel effortless.
Then calorie creep begins. It is subtle. A handful of nuts after dinner (170 calories). A larger portion of rice because you are a little hungrier today (100 extra calories). A sweetened coffee instead of black (150 calories). An extra tablespoon of olive oil while cooking (120 calories). Individually, none of these changes register. Collectively, they can add 300 to 500 calories daily. Over a week, that is 2100 to 3500 extra calories, enough to fully offset the calorie deficit tirzepatide created.
The fix is not calorie counting forever. It is periodic awareness. Track everything you eat for 3 to 5 days every month. Compare it to what you were eating during your weight loss phase. The gap is usually obvious and fixable once you see it. Use our peptide calculator alongside a food tracking app to maintain alignment between your protocol and your nutrition.
Reduced physical activity and NEAT decline
NEAT stands for Non-Exercise Activity Thermogenesis. It includes everything you do physically that is not structured exercise: walking, fidgeting, standing, cleaning, climbing stairs, carrying groceries. NEAT accounts for 15 to 30 percent of total daily calorie expenditure in most people. That is more than most exercise sessions.
When you lose weight, NEAT drops. You move less without realizing it. Steps per day decline. You sit more. You fidget less. Your body is conserving energy as part of the adaptive thermogenesis response discussed earlier. Research shows that NEAT can decrease by 200 to 500 calories daily after significant weight loss.
Tirzepatide fatigue makes this worse. Some users report reduced energy, particularly during dose increases or during the first few months of treatment. GLP-1 fatigue is a recognized side effect that can significantly reduce both structured exercise and daily movement. The caloric impact of moving less, combined with the metabolic slowdown from weight loss, creates a double deficit that easily produces weight gain.
Aim for 7000 to 10000 steps daily regardless of how you feel. Use a fitness tracker or phone pedometer. The data does not lie, even when your perception tells you that you are moving enough. Small increases in daily walking can offset NEAT declines and break plateaus that no amount of dieting will fix.
Poor sleep disrupting hormonal regulation
Sleep deprivation is a weight gain accelerator. Period. Sleeping less than 6 hours per night increases ghrelin (hunger hormone) by 15 to 28 percent and decreases leptin (satiety hormone) by a similar margin. The result is stronger hunger signals that can overpower tirzepatide appetite suppression.
It gets worse. Poor sleep increases cortisol, which promotes fat storage in the abdominal area specifically. It reduces insulin sensitivity, partially negating one of tirzepatide major benefits. And it impairs decision-making, making you more likely to reach for calorie-dense comfort foods when tired.
Tirzepatide insomnia is reported by a subset of users, creating a particularly frustrating cycle: the medication that should help you lose weight disrupts the sleep you need to lose weight. If this applies to you, addressing sleep quality becomes just as important as any dietary or exercise intervention.
Prioritize 7 to 9 hours of sleep. Keep a consistent sleep schedule. Avoid screens 60 minutes before bed. Keep your bedroom cool (65 to 68 degrees Fahrenheit). Consider magnesium glycinate supplementation, which has evidence for both sleep improvement and metabolic support.
Chronic stress and cortisol elevation
Cortisol is the stress hormone that directly promotes weight gain, particularly around the midsection. Chronic stress, whether from work, relationships, financial pressure, or the frustration of weight gain itself, keeps cortisol elevated throughout the day.
Elevated cortisol does three things that fight tirzepatide. First, it increases appetite, specifically for high-calorie, high-carbohydrate foods. Second, it promotes fat storage in visceral adipose tissue, the dangerous deep belly fat that surrounds organs. Third, it reduces the effectiveness of insulin, undermining one of tirzepatide key metabolic benefits.
The irony is brutal. Stressing about weight gain on tirzepatide can literally cause more weight gain. The cortisol response from anxiety about the scale creates a feedback loop that makes the problem worse. Breaking this cycle requires conscious intervention: meditation, deep breathing, walking in nature, reduced caffeine, and sometimes professional support through therapy or counseling.
Alcohol consumption
Drinking on tirzepatide creates problems beyond the obvious calorie addition. Alcohol contains 7 calories per gram, nearly as calorie-dense as fat. A single glass of wine adds 120 to 150 calories. A cocktail can add 200 to 400 calories. Two drinks per evening, four nights a week, adds 1600 to 3200 calories weekly.
But the caloric content is only part of the problem. Alcohol impairs fat oxidation for 12 to 24 hours after consumption. Your body prioritizes metabolizing alcohol over burning fat, meaning every drink creates a window where fat loss essentially stops. Alcohol also reduces inhibition around food choices, increases late-night eating, disrupts sleep quality, and promotes inflammation that can cause water retention.
You do not have to eliminate alcohol entirely. But if you are gaining weight on tirzepatide and drinking regularly, alcohol reduction is one of the highest-impact changes you can make. Try eliminating it completely for 30 days and monitor what happens to the scale. The results often speak for themselves.
When weight gain is actually a good sign
Not all weight gain is bad. This section might seem counterintuitive in a guide about why you are gaining weight on tirzepatide, but it is important to understand that the scale is a crude tool. It cannot distinguish between fat, muscle, water, or food weight.
Body recomposition
If you started resistance training alongside tirzepatide, something remarkable can happen. You lose fat while gaining muscle simultaneously. The scale might stay flat or even climb slightly, while your body visibly transforms. Clothes fit differently. Your waist shrinks. Your arms and legs look more defined.
This is body recomposition, and it is the ideal outcome. Muscle is denser than fat. A pound of muscle occupies less space than a pound of fat but weighs the same. Gaining 3 pounds of muscle while losing 3 pounds of fat shows zero change on the scale despite dramatic improvement in body composition.
How do you know if recomposition is happening? Measure beyond the scale. Track waist circumference weekly. Take progress photos monthly. Use body fat calipers or a DEXA scan if available. If your measurements are improving while the scale is static or slightly up, celebrate. You are achieving the best possible outcome.
Fluid normalization after early dehydration
Early tirzepatide treatment often causes mild dehydration through reduced food intake, nausea-related fluid loss, and changes in kidney function. The rapid initial weight loss many people experience includes a significant water component. When your body eventually rehydrates and stabilizes, some of that water weight returns.
This is healthy and expected. Dehydration is not sustainable and not desirable. The fluid normalization might add 2 to 4 pounds that represent your body returning to appropriate hydration levels. This is not the medication failing. This is your body healing.
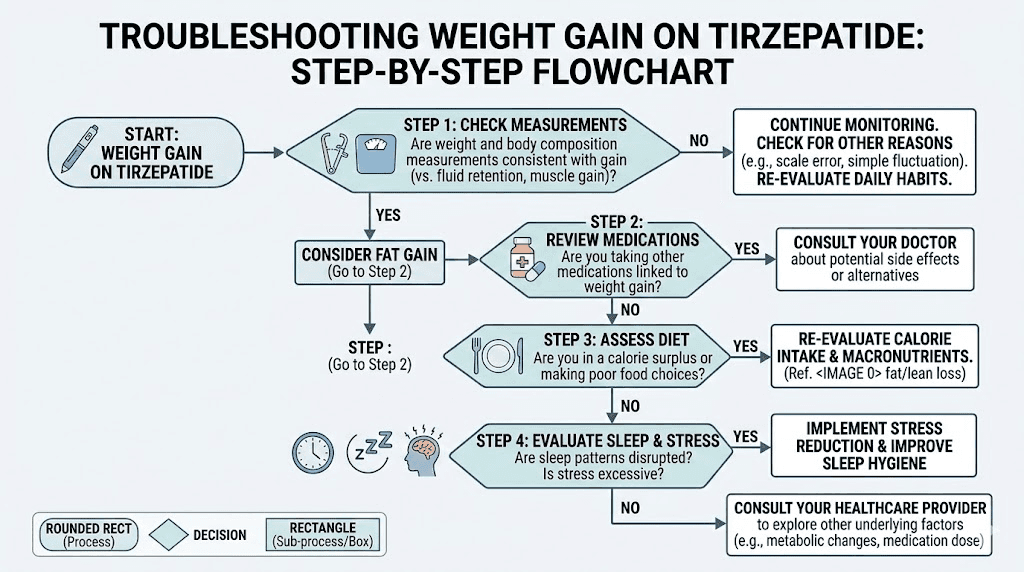
How to troubleshoot and fix weight gain on tirzepatide
Enough about causes. Let us talk solutions. This section provides a systematic protocol for identifying why you are gaining weight and implementing targeted fixes. Follow this sequence. Do not skip steps.
Track more than just scale weight
Stop using the scale as your only metric. Start tracking these measurements weekly, always at the same time of day under the same conditions.
Waist circumference is the single most useful non-scale measurement. Measure at your navel while standing relaxed. A decreasing waist circumference while the scale goes up almost certainly means body recomposition, not fat gain.
Hip circumference provides context for waist measurements. The waist-to-hip ratio is a better predictor of health outcomes than BMI or body weight alone.
Progress photos capture visual changes the scale misses. Take front, side, and back photos in consistent lighting and clothing every two weeks. The difference between week 1 and week 12 is often dramatic, even when the scale has barely moved.
Clothing fit is an underrated metric. If your clothes are getting looser while the scale climbs, trust the clothes. They do not lie.
Energy and mood also matter. Weight gain from muscle and improved nutrition often comes with better energy, better sleep, and improved mood. Weight gain from metabolic dysfunction or medication interactions often comes with fatigue, brain fog, and worsening mood. The pattern tells the story.
Optimize protein intake
Protein is the single most important macronutrient for weight loss on tirzepatide. It preserves lean muscle mass, which maintains your metabolic rate. It has the highest thermic effect of any macronutrient, meaning your body burns 20 to 30 percent of protein calories just digesting and processing them. And it promotes satiety, extending the appetite suppression effects of tirzepatide.
Aim for 1.2 to 1.6 grams of protein per kilogram of body weight daily. For a 180-pound person, that is approximately 100 to 130 grams daily. Distribute it across meals, targeting 25 to 40 grams per meal. Protein shakes formulated for GLP-1 users can help reach these targets when solid food volume is limited by tirzepatide appetite suppression.
This is where most people fall short. Reduced appetite on tirzepatide naturally reduces protein intake along with everything else. But while cutting total calories is the goal, cutting protein specifically undermines the entire process. Make protein the priority at every meal, even if it means eating less of everything else.
Add resistance training
Resistance training is not optional for anyone losing weight on tirzepatide. It is essential. Without it, you are accelerating muscle loss, lowering your metabolic rate, and setting yourself up for weight regain.
You do not need to become a bodybuilder. You need a basic, consistent program that challenges your major muscle groups 2 to 3 times per week. Compound movements are most efficient: squats, deadlifts, bench press, rows, and overhead presses. If you are new to resistance training, start with machines or bodyweight exercises. Hire a trainer for your first month if possible.
The research is unequivocal. People who combine GLP-1 agonists with resistance training lose more fat, retain more muscle, and maintain weight loss longer than those who rely on medication alone. A recent systematic review found that structured exercise during weight loss peptide treatment reduced lean mass loss by 30 to 50 percent compared to sedentary controls.
Review your medication list
Print out a complete list of every medication, supplement, and over-the-counter product you take. Bring it to your healthcare provider and specifically ask: "Which of these can cause weight gain, and are there weight-neutral alternatives?"
The medications most likely to interfere were listed earlier: antipsychotics, certain antidepressants, corticosteroids, insulin, sulfonylureas, gabapentin, pregabalin, beta-blockers, lithium, and valproate. But the list extends beyond these. Some allergy medications, sleep aids, and even certain supplements can affect weight.
Never stop medications without medical guidance. But advocating for weight-neutral alternatives when they exist is appropriate and important. Your psychiatrist, for example, may be able to switch you from paroxetine (weight-promoting) to sertraline (weight-neutral) with the same therapeutic benefit.
Consider dose adjustment
If you have been at the same tirzepatide dose for more than 8 weeks and your weight loss has stalled or reversed, a dose increase may help. The standard titration schedule calls for increases every 4 weeks until you reach the dose that produces adequate results.
Some people find that splitting their dose helps maintain more consistent appetite suppression throughout the week. Splitting tirzepatide dose twice a week is something some providers recommend, particularly at higher doses where GI side effects are problematic. Smaller, more frequent doses can maintain steadier blood levels and more consistent appetite control.
Others explore microdosing tirzepatide as a maintenance strategy after reaching their target weight. The right dose for weight loss may differ from the right dose for weight maintenance. Work with your provider to find the optimal approach for your stage of treatment.
Sleep and stress protocols
If sleep or stress is contributing to your weight gain, these protocols can help.
Sleep protocol: Set a consistent bedtime and wake time, including weekends. Eliminate caffeine after noon. Keep your bedroom at 65 to 68 degrees. Use blackout curtains or a sleep mask. Consider magnesium glycinate (200 to 400 mg before bed). If tirzepatide-related insomnia persists, discuss timing your injection in the morning rather than evening.
Stress protocol: Implement one daily stress-reduction practice. Start with 10 minutes of guided meditation using a free app like Insight Timer. Add a daily 20-minute walk outdoors, preferably in nature. Limit news consumption to once daily. Consider reducing caffeine if you consume more than 200 mg daily. Journal for 5 minutes before bed to clear racing thoughts.
These are not luxury additions. For people whose weight gain is stress or sleep-driven, these protocols are as important as any medication adjustment or dietary change.
Breaking a tirzepatide weight loss plateau
A plateau is not the same as weight gain, but it often precedes it. Understanding how to break through a plateau can prevent the frustration that leads to abandoning good habits and sliding into regain.
Understanding the metabolic set point
Your body has a weight range it defends aggressively. This concept, called the set point or settling point, explains why weight loss eventually stalls even on effective medications. Your body perceives the calorie deficit as a threat and activates multiple defense mechanisms simultaneously: increased hunger, decreased metabolism, reduced energy, improved calorie absorption efficiency.
Tirzepatide is powerful enough to override some of these mechanisms. But it cannot override all of them indefinitely. The plateau represents the point where tirzepatide appetite suppression and your body defensive mechanisms reach equilibrium. Neither side is winning.
The good news from clinical trials: most people who maintain tirzepatide treatment continue losing weight, albeit more slowly, even after hitting a plateau. The SURMOUNT-4 trial showed that people who continued tirzepatide after their initial plateau lost an additional 5.5 percent of body weight, while those switched to placebo regained 14 percent. The medication is still working. The visible results just slow down.
Calorie cycling strategies
Eating the same calorie amount every day can perpetuate metabolic adaptation. Your body becomes efficient at operating on that exact intake. Calorie cycling, alternating between higher and lower calorie days, can disrupt this pattern.
A practical approach: eat your normal reduced calories 5 days per week. On 2 non-consecutive days, increase calories by 20 to 30 percent, primarily from protein and complex carbohydrates. This sends your metabolism a signal that food scarcity is not permanent, partially resetting some adaptive thermogenesis effects.
Do not confuse this with binge days or cheat days. The increase should be modest, controlled, and focused on nutrient-dense foods. Think extra servings of lean protein, sweet potatoes, and fruits, not pizza and ice cream. The goal is metabolic signaling, not psychological relief.
Exercise timing and type
If you have been doing the same exercise routine for months, your body has adapted to it. Just as metabolic adaptation reduces the calorie cost of daily living, exercise adaptation reduces the calorie cost of your workouts. You burn fewer calories doing the same exercises at the same intensity as when you started.
Change something. If you have been walking, add intervals. If you have been doing moderate-intensity cardio, try high-intensity interval training. If you have been doing machines, switch to free weights. If you have been doing the same weight for weeks, increase it. Novel stimulus is what breaks plateaus.
Timing matters too. Some evidence suggests that exercising in a fasted state promotes greater fat oxidation. Others show that post-meal walking improves glucose disposal and insulin sensitivity. Experiment with different timing to find what produces the best results for your body. There is no single correct answer, only the answer that works for you.
When to contact your healthcare provider
Not all weight gain on tirzepatide is benign. Some patterns require medical evaluation because they may indicate serious underlying conditions or medication complications.
Red flag symptoms
Contact your healthcare provider urgently if you experience any of the following alongside weight gain.
Rapid gain of more than 2 to 3 pounds in a single day or more than 5 pounds in a week. This pace suggests fluid retention from cardiac, renal, or hepatic causes, not fat accumulation. It requires prompt medical assessment.
Swelling in legs, ankles, or feet (peripheral edema) combined with weight gain can indicate heart failure, kidney dysfunction, or venous insufficiency. Do not attribute this to normal weight fluctuation.
Breathing difficulty, especially when lying flat or during mild exertion, combined with weight gain is a potential sign of fluid accumulation around the lungs (pleural effusion) or worsening heart function.
Severe abdominal pain with weight gain, particularly in the upper right quadrant, can indicate gallbladder disease. GLP-1 and GIP agonists increase gallbladder disease risk due to reduced gallbladder motility during rapid weight loss.
New symptoms suggestive of thyroid dysfunction: extreme fatigue, cold intolerance, constipation, dry skin, hair thinning, and brain fog. These warrant thyroid function testing including TSH, free T4, and free T3.
Medical workup checklist
If you are gaining weight on tirzepatide without an obvious lifestyle explanation, request the following tests from your healthcare provider.
Thyroid panel: TSH, free T4, free T3, and thyroid antibodies. Subclinical hypothyroidism is easily missed and easily treated.
Fasting insulin and glucose: Assess insulin resistance severity. If insulin resistance is extreme, tirzepatide alone may be insufficient.
Cortisol: Either a morning serum cortisol or a 24-hour urinary free cortisol. Rules out Cushing syndrome and chronic cortisol elevation.
Complete metabolic panel: Checks kidney function, liver function, and electrolyte balance. Identifies organ dysfunction that can cause fluid retention.
Hemoglobin A1C: Tracks long-term blood sugar control. Unexpectedly high A1C despite tirzepatide suggests either non-adherence or a condition requiring additional intervention.
Sex hormones: For women, test estrogen, progesterone, testosterone, and DHEA-S to evaluate PCOS and perimenopausal changes. For men, test total and free testosterone, as low testosterone promotes fat gain and muscle loss.
The long-term perspective on tirzepatide and weight
Weight management with tirzepatide is a long-term proposition. The research is clear on this point. Stopping tirzepatide leads to weight regain in most people. A post-hoc analysis of the SURMOUNT-4 trial found that only 28 percent of participants maintained 90 percent or more of their weight loss after discontinuation, while 72 percent regained more than 10 percent of the weight they had lost.
Even more concerning, when weight is regained after stopping GLP-1 medications, it tends to come back as fat rather than muscle. This creates a worse body composition than before treatment. More fat, less muscle, lower metabolic rate, and greater difficulty losing weight in the future. This phenomenon makes a strong case for maintaining treatment long-term rather than using tirzepatide as a short-term fix.
However, long-term use does not mean the same dose forever. Many providers are exploring maintenance dosing strategies. Weaning off tirzepatide gradually while building sustainable habits is one approach. Maintaining weight loss after tirzepatide requires deliberate strategy: high protein intake, consistent resistance training, regular physical activity, and ongoing monitoring of weight and body composition.
For researchers serious about optimizing their peptide protocols, SeekPeptides provides comprehensive evidence-based guides, protocol databases, and a community of thousands who have navigated these exact challenges. Members access detailed tirzepatide dosing protocols, diet plans optimized for GLP-1 users, and troubleshooting resources that go far beyond what a single article can cover.
Compounding factors and combination strategies
Sometimes the answer is not just one thing. Weight gain on tirzepatide often results from multiple factors compounding simultaneously. Mild metabolic adaptation plus moderate muscle loss plus a subtle increase in calorie intake plus slightly worse sleep can combine to produce significant weight gain, even though no single factor alone would cause it.
This is why the systematic approach matters. Address one factor and you might see modest improvement. Address three or four simultaneously and the results multiply. The most successful tirzepatide transformations come from people who optimize everything: dosing, nutrition, exercise, sleep, stress, and medication interactions.
Some people explore additional compounds alongside tirzepatide to address specific issues. Tirzepatide with glycine and B12 is a popular combination that addresses potential nutrient deficiencies from reduced food intake. Supplements to take with tirzepatide can support areas where the medication creates secondary deficiencies, including B vitamins, magnesium, and electrolytes.
Tirzepatide with niacinamide has gained attention for potential metabolic benefits beyond weight loss. B12 supplementation is particularly important because reduced food intake naturally reduces B12 consumption, and B12 deficiency causes fatigue that further reduces physical activity.
Combining phentermine with tirzepatide is something some providers consider for patients who have plateaued, though this combination requires careful medical supervision. AOD-9604 with tirzepatide is another combination explored in research contexts for enhanced fat-targeted weight loss.
Understanding your tirzepatide dosing
Dosing errors or suboptimal protocols contribute to weight gain more often than people realize. Let us review the key dosing considerations.
If you are using compounded tirzepatide, accurate reconstitution is critical. Errors in the mixing process can result in either too much or too little active compound per injection. Too little and you lose appetite suppression. Too much and side effects become unbearable, leading to inconsistent dosing.
Use the compounded tirzepatide dosage calculator to verify your math. Cross-reference with the reconstitution chart to confirm your bacteriostatic water volume. Check your syringe dosage against the conversion chart. Small errors in any of these steps can significantly alter your actual dose.
Injection technique also matters. Subcutaneous injection means the needle enters the fatty tissue just below the skin. Injecting too deep (into muscle) or too shallow (into the dermis) changes absorption kinetics. Stomach injection, thigh injection, and upper arm are all acceptable sites, but absorption rates vary slightly between locations. Rotating injection sites prevents lipodystrophy and maintains consistent absorption.
Storage affects potency. Refrigerated tirzepatide maintains full potency for its shelf life. Tirzepatide left at room temperature degrades over time. If your vial has been exposed to heat, direct sunlight, or prolonged room temperature storage, the compound may be less potent than expected, resulting in reduced effectiveness. Warmth exposure and expiration are common causes of reduced efficacy that many people overlook. Compounded tirzepatide expiration dates tend to be shorter than brand-name formulations, so check your vial carefully.
Comparing tirzepatide to alternatives for resistant weight gain
If you have addressed all the factors above and are still gaining weight on tirzepatide, it may be worth understanding how it compares to alternatives. Not because you should switch without medical guidance, but because informed conversations with your provider lead to better outcomes.
Semaglutide versus tirzepatide is the most common comparison. Tirzepatide generally produces greater weight loss due to its dual mechanism, but some people respond better to semaglutide for reasons not fully understood. Individual pharmacogenomics, meaning how your genes affect medication metabolism, plays a significant role. The dosage comparison chart shows equivalent doses and expected responses for both compounds.
Switching from tirzepatide to semaglutide or vice versa is a legitimate strategy when one medication produces inadequate results. The conversion chart helps providers transition patients between the two. Some people who plateau on tirzepatide find renewed progress after switching to semaglutide, possibly due to differences in receptor activation patterns.
Retatrutide is a newer triple agonist (GLP-1, GIP, and glucagon receptor) that shows even greater weight loss in clinical trials. Retatrutide versus tirzepatide comparisons suggest retatrutide may produce superior results in some populations, though it is not yet widely available. For those interested, switching from tirzepatide to retatrutide is an emerging topic in the weight loss peptide space.
Other peptides for weight loss exist beyond the GLP-1 class. Fat-burning peptides like AOD-9604, MOTS-c, and tesofensine work through entirely different mechanisms and may be useful additions or alternatives for specific situations. Explore the full peptide stack for weight loss options to understand the complete landscape.
Diet optimization while on tirzepatide
What you eat matters as much as how much you eat. Tirzepatide reduces total calorie intake, but it does not optimize food quality. The wrong foods at the right calorie level can still promote weight gain through inflammation, insulin spikes, and nutrient deficiencies that impair metabolism.
Foods to prioritize on tirzepatide include lean proteins (chicken, fish, turkey, tofu, eggs), non-starchy vegetables, healthy fats (avocado, olive oil, nuts in measured portions), and complex carbohydrates (sweet potatoes, quinoa, brown rice). The tirzepatide diet plan emphasizes protein-first eating: begin every meal with protein, then add vegetables, then fat, then carbohydrates. This sequence optimizes satiety and minimizes insulin spikes.
Foods to avoid on tirzepatide include ultra-processed foods, liquid calories (juices, sodas, sweetened coffee), fried foods, and high-sugar snacks. These foods bypass many of the appetite-suppressing mechanisms tirzepatide activates. Liquid calories in particular are problematic because they pass through the stomach quickly, minimizing the gastric emptying delay that tirzepatide relies on for satiety.
The tirzepatide meal plan provides structured guidance for daily eating. Some people find that planning meals in advance eliminates the decision fatigue that leads to poor choices when appetite returns unpredictably.
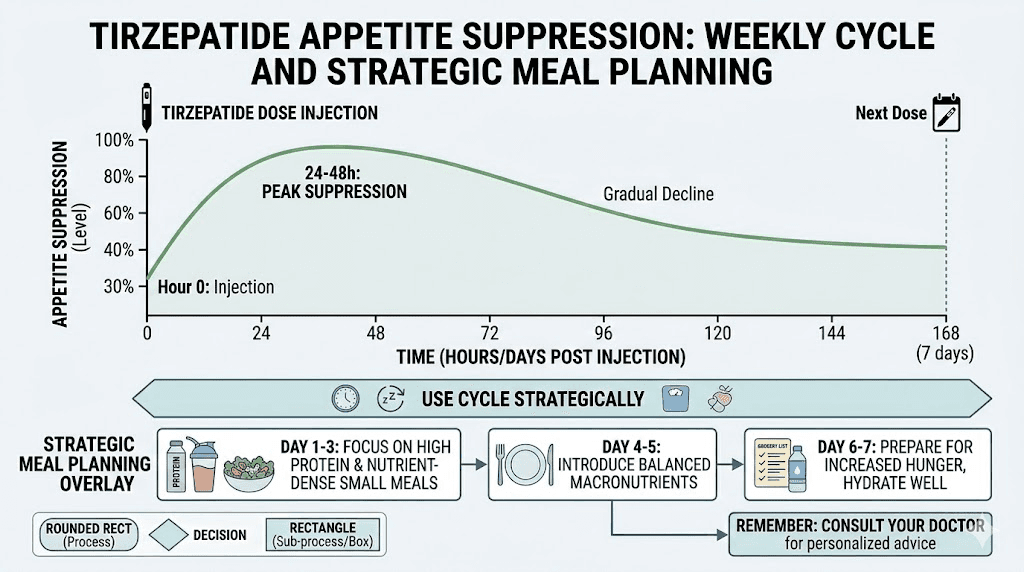
Injection timing and administration
When you inject tirzepatide can affect appetite suppression patterns throughout the week. Most people inject once weekly, but the appetite-suppressing effect is not constant over those seven days. It typically peaks 24 to 48 hours after injection and gradually decreases through the end of the week.
If your weight gain coincides with overeating during the last 2 to 3 days before your next injection, the timing is the clue. Some strategies that help include timing your injection to precede your socially challenging days (inject Wednesday if weekends are your struggle), planning lighter meals specifically for days 5 through 7, and discussing split dosing with your provider to maintain more consistent levels.
Taking tirzepatide a day early is generally acceptable and can be useful for schedule management, but consistency matters more than perfection. A stable weekly routine outperforms an irregular schedule, even if the irregular schedule theoretically optimizes timing.
Injection site reactions can affect absorption and consequently effectiveness. If you experience persistent redness, itching, or lumps at your injection sites, these could indicate poor absorption. Proper injection site rotation and technique can resolve most of these issues.
Psychological factors and the weight loss mindset
The psychological dimension of weight gain on tirzepatide deserves honest discussion. Weight gain after investing financially, emotionally, and physically in a medication protocol triggers a specific kind of distress that can spiral into behaviors that make the problem worse.
The most common psychological trap is all-or-nothing thinking. "The medication is not working, so why bother eating well?" This leads to abandoning dietary discipline entirely, which accelerates weight gain. One bad week becomes a bad month. A small regain becomes a large one. The medication was still helping, just not as visibly, and removing the behavioral scaffolding around it eliminates the remaining benefit.
Another trap is scale obsession. Weighing daily, or multiple times daily, and reacting emotionally to every fluctuation creates a stress response that, as discussed, promotes cortisol-driven weight gain. Weekly weigh-ins under consistent conditions provide meaningful data. Daily readings provide mostly noise.
Tirzepatide-related anxiety is a real phenomenon, and weight gain exacerbates it. If you find yourself in a cycle of anxiety about your weight, poor sleep from the anxiety, cortisol elevation from the poor sleep, and weight gain from the cortisol, seek professional support. This is not weakness. This is neurochemistry, and it responds to intervention.
What the research says about long-term outcomes
The weight management field has learned hard lessons over decades. Every medication that produces weight loss also faces the challenge of weight regain. Tirzepatide is the most effective tool currently available, but it exists within the same biological reality as everything that came before.
The SURMOUNT-4 trial provides the clearest long-term data. After 36 weeks of tirzepatide-driven weight loss, participants were randomized to continue tirzepatide or switch to placebo. Those who continued lost an additional 5.5 percent of body weight. Those who stopped regained 14 percent. More troubling, the regained weight was disproportionately fat rather than lean mass. The body composition after regain was worse than before treatment began.
A separate analysis found that within 5 to 8 months of stopping tirzepatide, 72 percent of participants had regained more than 10 percent of their total body weight loss. Only 28 percent maintained 90 percent or more of their results. These numbers underscore that tirzepatide is not a short-term solution. It is, for most people, a long-term or permanent intervention.
For people experiencing weight gain while still on tirzepatide, these numbers actually provide reassurance. The medication is still preventing the full regain that would occur without it. Your current weight, even if higher than your lowest on treatment, is almost certainly lower than it would be without the medication. The goal shifts from maximizing loss to optimizing maintenance while addressing the specific factors causing the upward trend.
SeekPeptides members gain access to comprehensive long-term management strategies, including maintenance protocols, community support from others navigating the same challenges, and evidence-based guidance that evolves as new research emerges.
Specific protocols for different weight gain patterns
Not all weight gain looks the same. Here are targeted protocols for the most common patterns.
Pattern 1: sudden gain of 3 to 7 pounds over 1 to 2 days
Most likely cause: Water retention. Could be from sodium intake, menstrual cycle, constipation, or new medication.
Protocol: Do not panic. Do not reduce calories further. Drink 80 to 100 ounces of water daily for 3 to 5 days. Reduce sodium to under 2000 mg daily. If constipated, add magnesium citrate (400 mg) and increase fiber intake. Weigh again in one week. If the gain persists, check for new medications or medical causes.
Pattern 2: gradual gain of 1 to 2 pounds per week over 4 or more weeks
Most likely cause: Calorie creep plus metabolic adaptation. GI tolerance has improved and appetite has returned without caloric awareness.
Protocol: Track all food intake for 7 consecutive days. Calculate average daily calories. Compare to your maintenance calories (use the peptide calculator plus a TDEE calculator). Increase protein to 1.4 g per kg body weight. Add or intensify resistance training. Discuss dose adjustment with your provider.
Pattern 3: weight loss stopped and slowly reversing despite good habits
Most likely cause: Metabolic adaptation at current dose. Possible underlying medical condition.
Protocol: Request comprehensive blood work (thyroid panel, fasting insulin, cortisol, sex hormones, metabolic panel). Review all medications for weight-promoting effects. Consider calorie cycling. If on lower tirzepatide dose, discuss titration upward. Ensure adequate sleep and stress management. Give interventions 4 to 6 weeks before reassessing.
Pattern 4: significant regain after stopping or reducing tirzepatide
Most likely cause: Loss of appetite suppression combined with metabolic adaptation and depleted lean mass.
Protocol: Restart or increase tirzepatide dose with provider guidance. Prioritize resistance training to rebuild lean mass. Increase protein to maximum recommended levels (1.6 g per kg). Address any behavioral patterns (stress eating, poor sleep, alcohol) that intensified after medication changes. Consider the restarting protocol approach, which applies similar principles when resuming GLP-1 therapy.
Frequently asked questions
Is it normal to gain weight on tirzepatide?
Weight fluctuations of 2 to 5 pounds are normal throughout treatment. True sustained weight gain affecting more than 5 percent of body weight over 2 to 3 months is less common but documented. It usually has identifiable causes including medication tolerance, concurrent medications promoting weight gain, medical conditions, or lifestyle factors. The systematic troubleshooting approach in this guide will help you identify your specific cause.
How long does tirzepatide take to start working for weight loss?
Most people notice appetite reduction within the first week. Measurable weight loss typically begins within 2 to 4 weeks. However, initial results vary significantly based on starting dose, individual metabolism, and baseline weight. Some people lose 5 to 10 pounds in the first month. Others see minimal scale movement for 6 to 8 weeks before weight loss accelerates.
Can tirzepatide cause weight gain in the first few weeks?
Yes, temporarily. Early treatment can cause water retention as your body adjusts to improved glucose control. This typically adds 2 to 6 pounds of water weight in weeks 2 through 8 and resolves on its own. Simultaneous fat loss may be occurring, but water weight masks it on the scale. Track waist measurements to see the full picture.
Should I stop tirzepatide if I am gaining weight?
No. Stopping tirzepatide almost always leads to greater weight regain than continuing it. Data from the SURMOUNT-4 trial shows 14 percent weight regain after discontinuation. Instead, work with your provider to identify the cause of weight gain and adjust your protocol accordingly. Weaning off tirzepatide should only be done under medical supervision and with a clear maintenance strategy.
Does exercise help with weight gain on tirzepatide?
Absolutely. Exercise addresses multiple causes of weight gain simultaneously. Resistance training preserves muscle mass and metabolic rate. Cardiovascular exercise improves insulin sensitivity and burns calories. General physical activity counters NEAT decline. Exercise also improves sleep quality, reduces stress, and enhances mood, all of which indirectly support weight loss.
How much protein do I need while on tirzepatide?
Aim for 1.2 to 1.6 grams per kilogram of body weight daily, distributed across meals. For a 180-pound (82 kg) person, that is roughly 100 to 130 grams per day. Prioritize complete protein sources: eggs, poultry, fish, lean meat, dairy, and protein shakes when whole food volume is difficult due to appetite suppression.
Can I switch to semaglutide if tirzepatide is causing weight gain?
Switching is an option worth discussing with your provider. Some people respond better to semaglutide and vice versa. Use the switching dosage chart for proper dose equivalence during the transition. However, address all other potential causes before switching, as the same factors that cause weight gain on tirzepatide may also affect semaglutide results.
Does tirzepatide cause muscle loss that leads to weight gain?
Tirzepatide does not directly cause muscle loss, but the calorie deficit it creates can lead to lean mass reduction. SURMOUNT-1 data shows approximately 25 percent of weight lost comes from lean mass. This muscle loss lowers metabolic rate and can contribute to eventual weight regain. The solution is resistance training and adequate protein intake throughout treatment.
External resources
Weight regain after liraglutide, semaglutide or tirzepatide (PubMed Central)
Tirzepatide and metabolic adaptation in people with obesity (Cell Metabolism)
Tirzepatide once weekly for the treatment of obesity (New England Journal of Medicine)
Body weight reducing effects of tirzepatide review (PubMed Central)
In case I do not see you, good afternoon, good evening, and good night. May your scale readings stay honest, your protocols stay optimized, and your progress stay consistent.