Mar 3, 2026

Nobody warns you about the smell. You start a GLP-1 medication expecting appetite suppression, weight loss, maybe some nausea. What you do not expect is burping up something that smells like rotten eggs at the worst possible moment. In a meeting. On a date. In the car with your kids. And yet here you are, Googling "sulfur burps GLP-1" at 2am because it happened again and you need answers.
You are not alone. Not even close.
Sulfur burps affect anywhere from 2% to 7% of people taking GLP-1 receptor agonists like semaglutide, tirzepatide, and liraglutide, according to clinical trial data filed with the FDA. That might sound like a small number on paper. But when you are the one producing hydrogen sulfide gas from your stomach every few hours, statistics offer zero comfort. The good news is that sulfur burps on GLP-1 medications are well understood, usually temporary, and highly treatable once you know what is actually causing them. This guide covers every angle: the science behind why your body produces that rotten egg gas, which GLP-1 medications trigger it most often, the specific foods making it worse, and the proven remedies that actually work. Not vague advice. Real protocols. Because you deserve to benefit from your medication without clearing a room every time you burp.
What are sulfur burps and why do they smell like rotten eggs
Sulfur burps are exactly what they sound like. Burps that carry hydrogen sulfide gas from your digestive tract up through your esophagus and out of your mouth, producing a distinct smell identical to rotten eggs. The gas itself, hydrogen sulfide (H2S), is produced naturally during digestion when bacteria in your gut break down sulfur-containing compounds found in certain foods.
Everyone produces some hydrogen sulfide during normal digestion. That is just biology.
The problem starts when production increases beyond what your body can handle quietly. Under normal circumstances, hydrogen sulfide gets absorbed into the bloodstream in small amounts, metabolized by the liver, and eliminated without incident. But when your digestive system slows down significantly, and that is exactly what GLP-1 medications do by design, the fermentation process intensifies. More gas accumulates. More of it travels upward instead of downward. And the result is burps that smell like someone cracked open a carton of expired eggs right under your nose.
Regular burps happen when swallowed air escapes from the stomach. Sulfur burps are fundamentally different. They carry hydrogen sulfide produced by bacterial fermentation in the gut, and that is why the odor is so distinctive and so unpleasant. The intensity can range from mildly noticeable to genuinely overwhelming, depending on how much gas has accumulated, what you ate recently, and how effectively your digestive tract is moving food along.
Why GLP-1 medications cause sulfur burps
Understanding why GLP-1 medications trigger sulfur burps requires understanding what these medications actually do to your digestive system. The mechanism is not complicated, but it explains almost everything about this side effect.
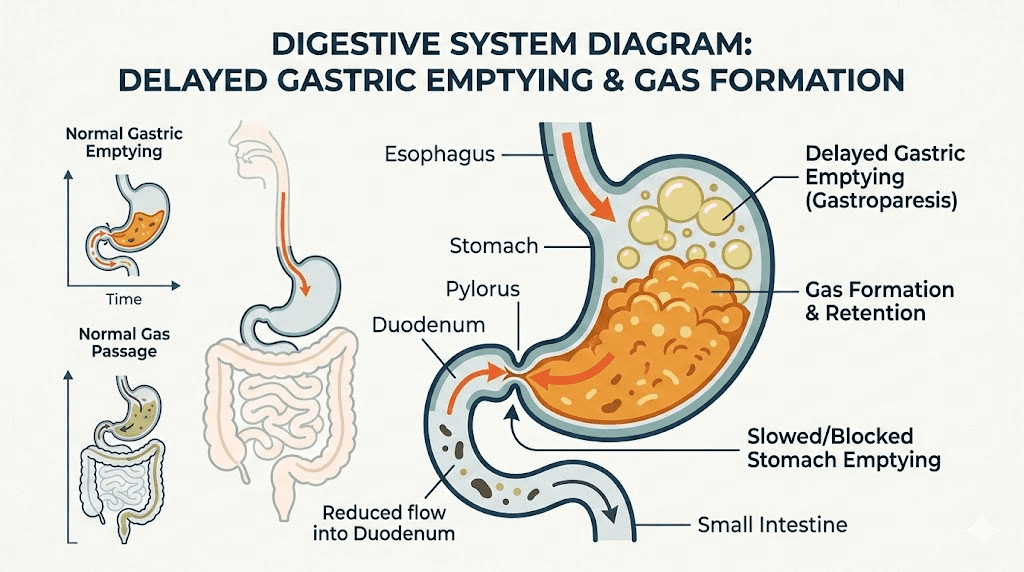
Delayed gastric emptying explained
GLP-1 receptor agonists work partly by slowing gastric emptying, the rate at which food moves from your stomach into your small intestine. This is one of the primary mechanisms behind appetite suppression. When food stays in your stomach longer, you feel full longer. When you feel full longer, you eat less. When you eat less, you lose weight.
Simple enough in theory.
But there is a digestive consequence. Food that normally passes through your stomach in 2 to 4 hours might sit there for 4 to 8 hours or even longer on a GLP-1 medication. That extended residence time creates a perfect environment for bacterial fermentation. The bacteria in your digestive tract do not stop working just because your stomach is emptying more slowly. They keep breaking down food. And when sulfur-containing compounds are present in that food, the bacteria produce hydrogen sulfide gas as a byproduct. That gas has to go somewhere. Often, it goes up, and out comes the sulfur burp.
This is why sulfur burps tend to be worse on GLP-1 medications than in general life. The medication itself does not produce the gas. It creates the conditions where your existing gut bacteria produce more gas than usual because food sits in the digestive tract for an extended period. The appetite-suppressing mechanism you want comes with a digestive side effect you do not.
The fermentation process
Fermentation in the gut is a normal, healthy process. Your gut microbiome contains trillions of bacteria, and they break down food components that your own digestive enzymes cannot handle. Fiber, certain starches, and sulfur-containing amino acids all get processed through bacterial fermentation. Under normal digestive conditions, this process is balanced and produces manageable amounts of gas.
GLP-1 medications tip that balance.
When food ferments for longer periods, several things happen simultaneously. Gas production increases overall. The types of gas produced shift toward more hydrogen sulfide because sulfur-reducing bacteria have more time to work on sulfur-containing substrates. And the accumulated gas creates pressure in the stomach and upper digestive tract that has to be released through burping. It is not that GLP-1 medications introduce new bacteria or change your microbiome composition overnight. They simply give your existing bacteria more time to do what they already do, and that means more fermentation, more gas, and more sulfur burps.
Research shows that digestive slowing on these medications can also contribute to constipation, bloating, and general abdominal discomfort. Sulfur burps are part of that same constellation of digestive side effects, all stemming from the fundamental mechanism of slowed gastric motility.
How hydrogen sulfide gas forms
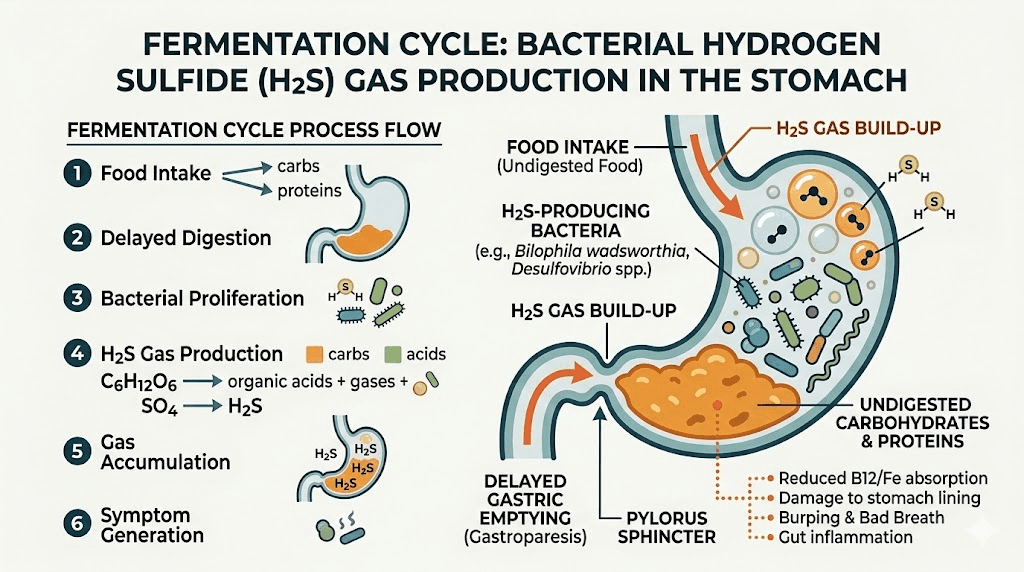
Hydrogen sulfide forms when sulfate-reducing bacteria (SRB) in your gut metabolize sulfur-containing compounds. These compounds come primarily from two sources: the food you eat and the bile your liver produces to help digest fats.
Sulfur-containing amino acids like cysteine and methionine, found in high-protein foods such as eggs, red meat, and dairy, are the primary dietary source. When these amino acids reach your gut bacteria, they get broken down through a process called anaerobic metabolism. One of the byproducts is hydrogen sulfide. Under normal conditions, this gas gets absorbed and processed quickly enough that you rarely notice it.
But when gastric emptying slows down on a GLP-1 medication like semaglutide or tirzepatide, the equation changes dramatically. More substrate sits available for longer. More bacteria get to work on it. More hydrogen sulfide accumulates before it can be absorbed or passed through the system. The result is gas buildup in the upper GI tract that gets released as sulfur-scented burps, sometimes accompanied by a feeling of bloating, nausea, or general stomach discomfort that many people notice early in treatment.
Which GLP-1 medications cause sulfur burps and how often
Not all GLP-1 medications cause sulfur burps at the same rate. Clinical trial data and post-marketing reports show meaningful differences between medications, doses, and formulations. Understanding which medication you are taking and its associated incidence rate helps set realistic expectations and guides management decisions.
Semaglutide (Ozempic, Wegovy, Rybelsus)
Semaglutide is the most widely prescribed GLP-1 receptor agonist, available as both injectable (Ozempic for diabetes, Wegovy for weight management) and oral (Rybelsus) formulations. The burping and eructation side effects vary by formulation and dose.
According to FDA prescribing information, eructation (the medical term for burping) occurs in approximately 3% of patients taking the 0.5 mg dose of injectable semaglutide and about 1% at the 1 mg dose. For Wegovy at the higher 2.4 mg weight management dose, the incidence jumps to approximately 7% of adults. The oral formulation (Rybelsus) reports burping in up to 2% of patients. These numbers represent burping in general, not sulfur burps specifically, but sulfur burps are a subset of the broader burping reported in trials.
What the clinical trial numbers do not capture is the real-world experience where many patients on various semaglutide doses report sulfur burps that come and go, particularly in the first few weeks and after dose escalations. The higher the dose, the more pronounced the gastric emptying delay, and the more likely sulfur burps become.
Tirzepatide (Mounjaro, Zepbound)
Tirzepatide is a dual GIP/GLP-1 receptor agonist, meaning it targets two incretin receptors instead of one. This dual mechanism often produces even more pronounced appetite suppression and weight loss than semaglutide alone, but it also means more aggressive slowing of gastric emptying. Clinical trials report eructation in approximately 2 to 5% of patients taking tirzepatide across the 5 mg, 10 mg, and 15 mg dose range.
The Zepbound (weight management) formulation reports slightly higher rates of around 4 to 5%, likely because patients are maintained at higher doses for longer periods. Many people starting tirzepatide notice that sulfur burps can be particularly intense during the first few weeks at each new dose level. The body gradually adapts, and for most people, the severity decreases over time even as the dose increases.
If you are taking compounded tirzepatide, the sulfur burp experience tends to be similar to brand-name formulations, since the active ingredient and its effect on gastric emptying remain the same regardless of the source.
Liraglutide (Saxenda, Victoza)
Liraglutide was one of the first GLP-1 receptor agonists widely used for weight management (Saxenda) and type 2 diabetes (Victoza). It has a shorter half-life than semaglutide and tirzepatide, requiring daily injections rather than weekly. Clinical trials report burping in approximately 1 to 3% of patients. Because liraglutide produces a less dramatic slowing of gastric emptying compared to the newer weekly medications, sulfur burps tend to be less severe and less frequent, though they still occur.
Retatrutide and newer agents
Retatrutide is a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. While still in clinical trials, early data suggests gastrointestinal side effects, including nausea and burping, occur at rates comparable to or slightly higher than tirzepatide. The triple receptor activation produces even more aggressive appetite suppression, which correlates with more pronounced gastric emptying delays. Researchers tracking retatrutide appetite suppression should be prepared for a similar or slightly elevated sulfur burp profile compared to dual agonists. Those comparing retatrutide versus tirzepatide will want to factor digestive tolerance into their decision alongside efficacy data. The retatrutide dosing schedule follows a similar gradual titration approach designed to minimize exactly these kinds of side effects.
When sulfur burps typically start and how long they last
Timing matters. Knowing when to expect sulfur burps and how long they typically persist helps you plan management strategies and, more importantly, gives you confidence that this is a temporary adjustment rather than a permanent consequence of treatment.
The first few weeks timeline
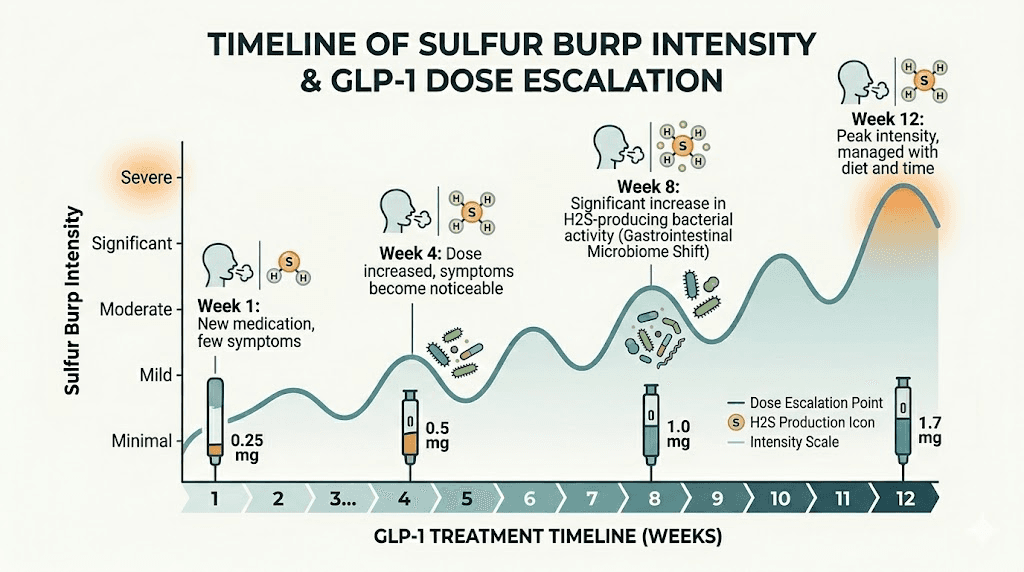
Most people who develop sulfur burps on GLP-1 medications notice them within the first 1 to 3 weeks of starting treatment. The initial dose is typically the lowest available (2.5 mg for tirzepatide, 0.25 mg for semaglutide), specifically designed to let your body adjust to the medication. Even at these starting doses, gastric emptying slows measurably, and that is enough to trigger fermentation-related gas in some people.
The pattern usually looks like this. Days 1 to 3 after your first injection, you might notice mild bloating and a few unusual burps. Days 4 to 7, sulfur burps may become more noticeable as the medication reaches steady state in your system. By week 2, your body begins adapting, and for many people, the frequency starts decreasing even without changing anything about their diet.
But not everyone follows that pattern. Some people barely notice anything at the starting dose, then get hit with significant sulfur burps when they move to the next dose level. Others experience sulfur burps from day one that persist for several weeks before gradually improving. Individual variation in gut microbiome composition, diet, and metabolic response to the medication all play a role.
Dose escalation and symptom patterns
Each dose increase on a GLP-1 medication can trigger a new round of sulfur burps. This is one of the most frustrating aspects for patients who thought they had adjusted to the medication. You spend 4 weeks at 2.5 mg of tirzepatide, finally get past the sulfur burps, move up to 5 mg, and they come right back.
This happens because each dose increase produces a further reduction in gastric emptying rate. Your body had just adapted to the previous level of slowing, and now it needs to adapt again. The good news is that adaptation at higher doses typically happens faster than the initial adjustment. Where the first dose might trigger sulfur burps for 2 to 3 weeks, subsequent dose increases often produce symptoms for only 1 to 2 weeks before your digestive system recalibrates.
If you are following a standard tirzepatide dose escalation schedule or semaglutide dosing chart, expect potential sulfur burp recurrence at each step up. Planning your dose increases around your social calendar, while not always practical, can help you manage the most intense days.
End-of-week patterns and injection timing
Many GLP-1 medication users report a distinct weekly pattern to their sulfur burps. The first 2 to 3 days after injection, when medication levels are highest, tend to produce the most intense gastric emptying delay and therefore the most sulfur burps. By days 5 to 7, as the medication concentration in your blood begins declining, gastric motility improves slightly, and sulfur burps often decrease.
This is the same pattern behind end-of-week hunger returning on these medications. As the drug level drops, gastric emptying speeds up, appetite returns somewhat, and digestive side effects ease. Some people find that adjusting their injection timing helps manage sulfur burps around important events. Injecting on a Friday evening, for example, means the worst of the digestive effects occur over the weekend when you might be at home rather than in an office environment.
For those considering splitting their dose twice a week or splitting semaglutide doses, one potential benefit is that smaller, more frequent doses may produce a more even effect on gastric emptying, potentially reducing the peak sulfur burp intensity that comes with a single large weekly dose.
Foods that make sulfur burps worse on GLP-1 medications
Diet plays a massive role in sulfur burp severity. The medication creates the conditions for increased fermentation, but the food you eat determines how much sulfur-containing substrate is available for bacteria to work on. Reduce the substrate, reduce the gas. It really is that direct.
High-sulfur foods to limit or avoid
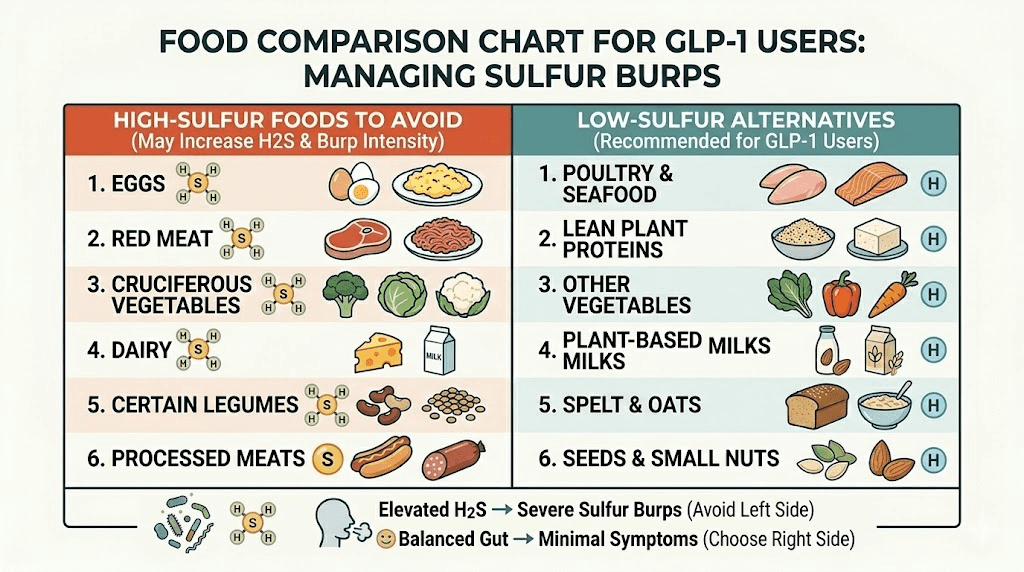
The primary dietary triggers for sulfur burps are foods rich in sulfur-containing amino acids (cysteine and methionine) and sulfur compounds. These include:
Eggs are the single biggest culprit for most people. Egg yolks contain significant amounts of sulfur compounds, and the hydrogen sulfide they produce during digestion is substantial. If you are experiencing severe sulfur burps on a GLP-1 medication, eliminating eggs for 1 to 2 weeks is often the fastest way to see improvement.
Cruciferous vegetables like broccoli, cauliflower, Brussels sprouts, cabbage, and kale contain sulfur compounds called glucosinolates. These are actually beneficial compounds with anti-cancer properties, so eliminating them entirely is not ideal long-term. But reducing portion sizes during the first few weeks of treatment or after dose increases can significantly reduce sulfur burp frequency.
Allium vegetables including garlic, onions, leeks, and shallots are rich in sulfur compounds that give them their characteristic flavor and smell. These same compounds become hydrogen sulfide precursors in your gut. Garlic is particularly potent, as even small amounts can trigger noticeable sulfur burps when gastric emptying is slowed.
Red meat and high-protein foods contain methionine and cysteine, the sulfur-containing amino acids that bacteria convert to hydrogen sulfide. This does not mean you should avoid protein entirely, far from it. Adequate protein intake is essential when taking GLP-1 medications to preserve muscle mass during weight loss. But you might benefit from shifting toward lower-sulfur protein sources like chicken breast, turkey, and plant-based proteins during the adjustment period.
Dairy products, particularly whole milk, aged cheeses, and cream, contain sulfur-containing amino acids that can worsen sulfur burps. People who are also lactose intolerant face a double challenge, as undigested lactose provides additional fermentation substrate for gas-producing bacteria. Paying attention to foods to avoid on tirzepatide and foods that work well on semaglutide can guide your choices.
Carbonated beverages and artificial sweeteners
Carbonated drinks introduce carbon dioxide gas directly into your stomach, which alone can increase burping frequency. When combined with the slowed gastric emptying from a GLP-1 medication, the effect is amplified. The gas has nowhere to go quickly, so it sits in your stomach and comes up as burps, potentially carrying hydrogen sulfide along with it.
Soda, sparkling water, beer, and champagne all fall into this category. If sulfur burps are a significant problem, eliminating carbonated beverages entirely for a trial period of 2 weeks is worthwhile. Many people find that this single change reduces burping frequency by 30 to 50%, even without other dietary modifications.
Artificial sweeteners deserve special attention. Sugar alcohols like sorbitol, mannitol, and xylitol, commonly found in sugar-free gum, diet candies, and "keto" snacks, are poorly absorbed in the small intestine and become prime fermentation fuel when they reach the gut bacteria. They can significantly worsen gas production and sulfur burps. If you have been chewing sugar-free gum to manage dry mouth on tirzepatide or nausea on semaglutide, switch to a product sweetened with stevia or monk fruit extract instead.
Fatty and fried foods
High-fat foods take longer to digest under normal conditions. Add a GLP-1 medication that further slows gastric emptying, and you have a recipe for extended fermentation and increased gas production. Fried foods, fast food, heavy cream sauces, and fatty cuts of meat all extend stomach retention time beyond what the medication alone produces.
This creates a compounding effect. The medication slows gastric emptying. The fatty food further resists digestion. Bacteria have even more time to ferment sulfur-containing compounds. And the result is worse sulfur burps than either factor would produce independently. The tirzepatide diet plan and semaglutide diet plan recommendations to reduce fried and heavily processed foods are partly about managing exactly this kind of digestive side effect.
Foods that help reduce sulfur burps
Just as certain foods worsen sulfur burps, others can actively help reduce them. The strategy is straightforward: choose foods that are low in sulfur compounds, easy to digest, and supportive of healthy gut transit.
Low-sulfur alternatives
When you need to reduce sulfur intake without sacrificing nutrition, these swaps work well:
Instead of eggs, try oatmeal or rice-based breakfast options. Instead of broccoli and cauliflower, choose carrots, bell peppers, cucumbers, spinach, and zucchini. Instead of garlic and onions for flavoring, use herbs like basil, oregano, thyme, and turmeric. Instead of red meat, lean toward chicken, turkey, and fish, which contain less methionine per serving. Instead of aged cheese, try fresh mozzarella or cottage cheese in smaller amounts.
These substitutions do not have to be permanent. Most people find they can gradually reintroduce higher-sulfur foods as their body adapts to the medication over 6 to 12 weeks. The goal is to reduce the sulfur load during the adjustment period when your digestive system is most sensitive.
Fiber-rich options that support digestion
Soluble fiber helps regulate digestive transit and can improve the balance of gut bacteria over time. Good options include sweet potatoes, squash, bananas, avocados, and chia seeds. These foods provide bulk that helps move contents through the digestive tract more efficiently, even when gastric emptying is slowed by medication.
A word of caution: dramatically increasing fiber intake overnight can temporarily worsen gas and bloating. If you are not already eating a fiber-rich diet, increase gradually over 2 to 3 weeks while your gut microbiome adjusts. Pairing increased fiber with adequate hydration is essential, as fiber without water can actually slow transit further and worsen symptoms.
Fermented foods and gut-friendly options
Fermented foods like plain yogurt (low-fat, unsweetened), kefir, kimchi, sauerkraut, and miso contain beneficial bacteria that can help rebalance your gut microbiome. This matters because a diverse, balanced microbiome tends to produce less hydrogen sulfide than one dominated by sulfate-reducing bacteria.
The irony is that some fermented foods, particularly those from cabbage like sauerkraut and kimchi, also contain sulfur compounds. Start with small portions and monitor your response. Plain, unsweetened yogurt or kefir is usually the safest starting point because it provides beneficial bacteria with minimal sulfur content. Building a GLP-1 friendly breakfast routine that includes fermented foods can help establish better gut balance over time.
Proven remedies to stop sulfur burps on GLP-1 medications
This is the section you have been scrolling for. Actual solutions. Not "talk to your doctor" repeated seventeen times (though you should do that too, for certain situations). These are the specific, evidence-based and community-validated remedies that work for sulfur burps on GLP-1 medications.
Dietary strategies that work
The dietary changes outlined above form the foundation of sulfur burp management. To put them into a practical protocol:
Week 1 elimination phase. Remove the biggest triggers: eggs, cruciferous vegetables, garlic, onions, carbonated drinks, and sugar-free gum. Track whether sulfur burps decrease in frequency and intensity. Most people see a 50% or greater reduction within 3 to 5 days of strict elimination.
Weeks 2 to 4 gradual reintroduction. Add back one food category every 3 to 4 days. Start with lower-sulfur options first (small amounts of cooked broccoli, for example) and work up to the bigger triggers (eggs, garlic). This helps you identify your personal trigger foods, which may differ from the general list.
Ongoing management. Once you know your triggers, you can make informed choices. Maybe eggs are fine in small amounts but garlic is a guaranteed sulfur burp trigger for you. Maybe carbonated drinks are the main culprit and eliminating them alone solves 80% of the problem. Personalization matters more than following a generic list.
Meal timing and portion control
How you eat matters as much as what you eat when it comes to sulfur burps on GLP-1 medications.
Smaller meals reduce the load on your already-slowed digestive system. Instead of three large meals, try 4 to 5 smaller meals distributed evenly throughout the day. Each meal gives your stomach a manageable amount to process, reducing the fermentation window and therefore the gas production.
Eating slowly is not just generic wellness advice here, it is specifically relevant. Eating quickly introduces more swallowed air into your stomach, which increases burping frequency. It also means larger food particles reach your gut, requiring more bacterial processing. Taking 20 to 30 minutes per meal, chewing thoroughly, and putting your fork down between bites all reduce the raw material available for fermentation.
Meal timing relative to your injection also matters. Some people find that eating lighter meals for 24 to 48 hours after their weekly injection, when the medication effect is peaking and gastric emptying is most delayed, significantly reduces sulfur burp severity. Then they can eat more normally as the week progresses and the medication effect moderates. This aligns with the general recommendations for managing how semaglutide makes you feel day by day.
Hydration protocols
Water helps food move through your digestive tract. On a GLP-1 medication where transit is already slowed, adequate hydration becomes even more important. Dehydration thickens digestive contents, making them harder to move and extending the fermentation window.
Aim for 8 to 10 glasses (approximately 2 to 2.5 liters) of water daily. Sip throughout the day rather than drinking large amounts at meals, which can further distend your stomach and worsen bloating. Room temperature or warm water is generally easier on the stomach than ice-cold water, which can temporarily slow gastric motility further.
Warm water with fresh lemon juice in the morning is a simple addition that many GLP-1 users find helpful. The warmth can gently stimulate digestive motility, and lemon juice provides a small amount of citric acid that supports stomach acid production. This does not cure sulfur burps on its own, but as part of a comprehensive approach, it contributes to better overall digestive function.
Probiotics and specific strains
Probiotics can help reduce sulfur burps by rebalancing the gut microbiome away from an overgrowth of sulfate-reducing bacteria. Not all probiotics are equal for this purpose, and the specific strains matter.
Lactobacillus plantarum has shown benefits for reducing gas production and bloating in clinical studies. It competes with sulfate-reducing bacteria for resources, effectively crowding them out over time.
Bifidobacterium species (particularly B. lactis and B. longum) are well-studied for reducing gas and bloating in people with IBS and other digestive conditions. They help ferment food through pathways that produce less hydrogen sulfide.
Akkermansia muciniphila is a newer probiotic strain gaining attention for gut health support, particularly in the context of metabolic health and GLP-1 medications. While research is still early, preliminary evidence suggests it may support better gut barrier function and reduce problematic fermentation.
Probiotics take time to work. Do not expect results overnight. Most clinical studies show that meaningful changes in gut microbiome composition require 2 to 6 weeks of consistent supplementation. Take them daily, preferably on an empty stomach or 30 minutes before a meal, and give them at least a full month before evaluating whether they are helping your sulfur burps.
Digestive enzymes
Digestive enzyme supplements can help break down food more completely in the stomach and upper small intestine, reducing the amount of undigested substrate available for bacterial fermentation in the lower gut. This is particularly useful for high-protein meals where incomplete digestion of sulfur-containing amino acids is a major contributor to hydrogen sulfide production.
Look for a broad-spectrum enzyme blend that includes protease (breaks down protein), lipase (breaks down fat), amylase (breaks down starch), and lactase (breaks down dairy sugar). Taking the enzyme supplement at the beginning of each meal gives it time to work on food as it enters your stomach.
Digestive enzymes are especially helpful for people who notice their sulfur burps are directly tied to specific meals. If you consistently get sulfur burps 1 to 3 hours after eating protein-heavy meals but not after lighter meals, a protease-heavy enzyme supplement taken before that protein meal can make a meaningful difference.
Over-the-counter options
Simethicone (Gas-X, Mylanta Gas) works by breaking down gas bubbles in the digestive tract, making them easier to pass. It does not reduce hydrogen sulfide production, but it can reduce the bloating and pressure that accompany sulfur burps. Many people find that taking simethicone after meals reduces overall gas discomfort, even if it does not eliminate the sulfur smell entirely.
Bismuth subsalicylate (Pepto-Bismol) can actually neutralize hydrogen sulfide in the gut, converting it to bismuth sulfide, which is insoluble and odorless. This makes Pepto-Bismol one of the more effective over-the-counter options specifically for the sulfur component of sulfur burps. The typical dose is 2 tablets or 30 ml of liquid after meals. Be aware that bismuth can cause black stools, which is harmless but can be alarming if you are not expecting it.
Activated charcoal supplements can adsorb (bind to) gases including hydrogen sulfide in the digestive tract. The evidence is mixed, but some people find that taking activated charcoal 1 hour before meals helps reduce sulfur burp intensity. Do not take activated charcoal within 2 hours of any medication, including your GLP-1 injection, as it can reduce medication absorption.
Natural remedies
Peppermint tea relaxes the smooth muscle of the digestive tract, which can help trapped gas move through more efficiently. Drinking a cup of peppermint tea 15 to 30 minutes after meals is one of the most commonly recommended natural remedies for digestive gas, and it is gentle enough to use daily without concern.
Ginger has been used for digestive support for thousands of years, and modern research supports its ability to promote gastric motility. This is particularly relevant on GLP-1 medications, where the primary issue is slowed gastric emptying. Fresh ginger tea (steep sliced fresh ginger in hot water for 10 minutes), ginger capsules, or even candied ginger can all help. Some people find that ginger also helps with the nausea that accompanies early GLP-1 treatment.
Fennel seeds contain compounds that reduce gas and bloating. Chewing a teaspoon of fennel seeds after meals or brewing them as tea is a traditional remedy that many GLP-1 medication users find helpful. The anise-like flavor of fennel can also help mask any lingering sulfur taste that accompanies the burps.
Apple cider vinegar in small amounts (1 to 2 tablespoons diluted in a glass of water) before meals may stimulate stomach acid production, which can improve digestion and reduce fermentation. The evidence is largely anecdotal, but the low risk and potential benefit make it worth trying. Always dilute it, as undiluted apple cider vinegar can damage tooth enamel and irritate the esophagus.
Dose adjustments and injection timing strategies
Sometimes dietary changes and supplements are not enough, and addressing the medication itself becomes necessary. This does not mean stopping treatment. It means working smarter with dosing to minimize digestive side effects while maintaining therapeutic benefit.
Slower dose titration
The standard dose escalation schedule for GLP-1 medications moves patients up to the next dose every 4 weeks. For tirzepatide, that means 2.5 mg for 4 weeks, then 5 mg for 4 weeks, then potentially 7.5 mg, 10 mg, 12.5 mg, and 15 mg. For semaglutide, it is 0.25 mg, then 0.5 mg, then 1 mg, then 1.7 mg, then 2.4 mg.
But these are minimum intervals, not mandatory ones.
If sulfur burps are severe enough to affect your quality of life or your willingness to continue treatment, staying at a lower dose for an additional 2 to 4 weeks before advancing is a perfectly valid strategy. The FDA prescribing information for both semaglutide and tirzepatide notes that dose escalation can be extended based on individual tolerance. A slower approach gives your gut microbiome more time to adapt to each level of gastric emptying delay before the next increase.
This is something microdosing protocols address directly. By using smaller dose increments, the transition is smoother and digestive side effects, including sulfur burps, tend to be less pronounced at each step.
Injection day and meal planning
Planning your injection day around your weekly schedule can help you manage the peak sulfur burp period. Most people find that digestive effects are strongest during the first 48 to 72 hours after injection, when medication blood levels are highest.
If your work week is Monday through Friday and your social commitments tend to be on weekends, injecting on Saturday morning gives you Sunday and Monday as the peak effect days, with the worst of the digestive effects likely subsiding by Tuesday. If your social calendar peaks on Friday and Saturday evenings, injecting on Sunday or Monday might be better.
There is no universally "best" day to inject. The right day depends on your personal schedule and when you can most comfortably manage digestive side effects. The best time to take your tirzepatide shot often comes down to lifestyle logistics as much as pharmacology.
Considering dose splitting
Some practitioners and patients have explored splitting the weekly dose into two smaller injections given 3 to 4 days apart. The rationale is that two smaller doses produce a more even medication level throughout the week, avoiding the peak-and-trough pattern that creates intense digestive effects early in the week and diminishing effects late in the week.
Research on splitting tirzepatide doses and splitting semaglutide doses is limited but growing. The theoretical benefit for sulfur burps is that a more stable medication level produces a more consistent (and potentially more moderate) degree of gastric emptying delay, rather than the sharp slowdown immediately after injection followed by a gradual return toward normal. This is a conversation to have with your prescribing provider, as it involves using the medication in an off-label manner.
Sulfur burps with diarrhea on GLP-1 medications
Sulfur burps alone are unpleasant. Sulfur burps combined with diarrhea are miserable. And unfortunately, this combination is not uncommon on GLP-1 medications, particularly during the first few weeks of treatment or after dose increases.
The mechanism is related. When the medication slows gastric emptying, the bolus of food that eventually does pass into the small intestine can be partially fermented and osmotically active, drawing water into the intestinal lumen and triggering loose stools or diarrhea. The same bacterial fermentation producing hydrogen sulfide (sulfur burps) also produces other gases and short-chain fatty acids that can accelerate colonic transit and cause watery stools.
If you experience this combination, all the dietary strategies for sulfur burps apply doubly. Reduce high-sulfur and high-FODMAP foods. Stay hydrated, as diarrhea depletes fluids and electrolytes. Consider adding a soluble fiber supplement like psyllium husk, which can help regulate both ends of the digestive spectrum by absorbing excess water in the intestine while adding bulk to stools.
Bismuth subsalicylate (Pepto-Bismol) is particularly useful for this combination, as it addresses both the sulfur burps and the diarrhea simultaneously. The standard dose of 2 tablets or 30 ml every 30 to 60 minutes as needed, up to 8 doses in 24 hours, can provide meaningful relief during acute episodes.
If the combination persists beyond 2 to 3 weeks or becomes severe enough to cause dehydration, this warrants a conversation with your healthcare provider. Persistent sulfur burps with diarrhea can sometimes indicate an underlying condition like gastrointestinal dysfunction that the medication is exacerbating rather than causing.
When sulfur burps signal something more serious
In most cases, sulfur burps on GLP-1 medications are a nuisance side effect that resolves with dietary changes, time, and the remedies described above. But in some cases, they can indicate an underlying condition that needs medical attention. Knowing the difference between normal medication-related sulfur burps and warning signs is important.
GERD and acid reflux
Gastroesophageal reflux disease (GERD) involves stomach acid flowing back into the esophagus, causing heartburn and sometimes increased burping. GLP-1 medications can worsen existing GERD in some people, partly because slowed gastric emptying means more time for acid to reflux. If your sulfur burps are accompanied by a burning sensation in your chest or throat, a sour taste in your mouth, or worsening heartburn, GERD may be contributing to the problem. Treatment with proton pump inhibitors (PPIs) or H2 blockers can address the acid component, often reducing burping as a secondary benefit.
SIBO (small intestinal bacterial overgrowth)
SIBO occurs when bacteria that normally reside in the large intestine migrate into the small intestine, where they ferment food prematurely and produce excess gas. Symptoms include bloating, abdominal pain, diarrhea, and, notably, sulfur burps. GLP-1 medications may increase SIBO risk because slowed gastric emptying can alter the normal flow patterns that keep bacteria where they belong.
If your sulfur burps are severe, persistent beyond 8 to 12 weeks of treatment, and accompanied by significant bloating and abdominal discomfort, ask your doctor about testing for SIBO. A lactulose breath test can diagnose the condition, and treatment typically involves a course of antibiotics like rifaximin.
H. pylori infection
Helicobacter pylori (H. pylori) is a bacterium that infects the stomach lining and can cause increased gas production, including sulfur-containing gases. Approximately 50% of the global population carries H. pylori, often without symptoms. But when combined with the altered digestive environment created by GLP-1 medications, a previously asymptomatic H. pylori infection can become symptomatic, producing sulfur burps, stomach pain, and nausea beyond what the medication alone would cause.
If your sulfur burps started before your GLP-1 medication and worsened after starting, or if they are accompanied by stomach pain, loss of appetite beyond what the medication explains, or dark stools, H. pylori testing is worth requesting. Treatment is a combination of antibiotics and acid-reducing medication, and it is highly effective.
When to see a doctor
Sulfur burps on their own, while unpleasant, are not dangerous. But seek medical attention if you experience any of the following alongside your sulfur burps:
Severe or persistent vomiting. Significant unexplained abdominal pain. Blood in your stool or black, tarry stools. Sulfur burps that worsen progressively over weeks rather than improving. Unintentional weight loss beyond what your GLP-1 medication would explain. Fever accompanying digestive symptoms. Sulfur burps that persist beyond 12 weeks despite dietary changes and remedies.
These symptoms can indicate conditions like gastroparesis (severe delayed gastric emptying beyond what the medication causes), bowel obstruction, or other digestive pathology that requires medical evaluation. The fatigue, digestive changes, and other effects of GLP-1 medications can sometimes mask symptoms of other conditions, making it important to maintain regular communication with your healthcare provider.
The gut microbiome connection and long-term management
Sulfur burps are ultimately a microbiome story. Your gut contains hundreds of species of bacteria, and the composition of that community determines how much hydrogen sulfide gets produced during digestion. GLP-1 medications do not change which bacteria you have, but they change the environment those bacteria operate in. Understanding this connection opens up longer-term strategies for managing sulfur burps that go beyond treating individual episodes.
Sulfate-reducing bacteria (SRB) are the primary producers of hydrogen sulfide in the gut. The most common genera include Desulfovibrio and Desulfobulbus. These bacteria use sulfate as a terminal electron acceptor in their energy metabolism, producing hydrogen sulfide as a byproduct. When food sits in the digestive tract longer due to GLP-1 medications, SRB have more time and more substrate to work with.
Using tools like the peptide stack calculator and reconstitution calculator helps ensure accurate dosing, which directly affects the intensity of gastric emptying and therefore sulfur burp severity. Reducing the population and activity of SRB is the long-term goal. This happens through three mechanisms: dietary modification (reducing sulfur-containing substrate), competitive exclusion (introducing beneficial bacteria that outcompete SRB), and environmental optimization (maintaining conditions that favor beneficial bacteria over SRB). The probiotics, dietary changes, and lifestyle modifications described in this guide all work through one or more of these mechanisms.
Over 3 to 6 months of consistent GLP-1 medication use with appropriate dietary support, many people find that their gut microbiome adapts to the new digestive environment. SRB populations decrease as beneficial bacteria better adapted to the slowed transit conditions take hold. This is why sulfur burps tend to be worst in the first few months of treatment and gradually improve over time, even without active intervention. Supporting that natural adaptation process with the strategies in this guide simply accelerates the timeline.
Platforms like SeekPeptides provide resources for understanding these physiological processes in detail, helping researchers make informed decisions about supplements to pair with their protocols and dietary strategies that support optimal outcomes.
Sulfur burps and daily life management
Beyond the medical and dietary strategies, there are practical daily life management techniques that can reduce the social impact of sulfur burps while you work through the adjustment period.
Keep mints or breath fresheners available. Not sugar-free ones with sorbitol (those worsen gas), but ones sweetened with stevia or xylitol-free formulations. Having them immediately available reduces the anxiety around potential embarrassing moments.
Identify your peak sulfur burp times. Track your burps for one week, noting when they occur relative to meals, injection timing, and activities. Most people find a distinct pattern that allows them to plan around the worst periods. Knowing that your sulfur burps peak 2 hours after dinner, for example, lets you schedule social activities accordingly.
Communicate with close contacts. Letting a trusted friend, partner, or colleague know that you are on medication that causes temporary digestive effects can reduce the anxiety and embarrassment significantly. You do not need to share every detail, just enough that they understand it is a medication side effect, not a hygiene issue.
Exercise after meals. Light physical activity like walking for 15 to 20 minutes after eating promotes gastric motility and can help move food through your system more quickly, reducing the fermentation window. This is not intense exercise, just a gentle walk. Many people find this simple habit reduces post-meal sulfur burps meaningfully. Exercise also supports the broader benefits of GLP-1 medications beyond weight loss by improving insulin sensitivity and cardiovascular health.
Comparing sulfur burp management across different GLP-1 medications
If sulfur burps are severe and persistent despite all management strategies, switching between GLP-1 medications is sometimes worth considering. Different medications produce different degrees of gastric emptying delay, and individual responses vary significantly.
Medication | Dosing | Burping incidence | Gastric emptying effect | Sulfur burp severity (typical) |
|---|---|---|---|---|
Semaglutide (Ozempic) | Weekly injection | 1-3% | Moderate | Mild to moderate |
Semaglutide (Wegovy) | Weekly injection | Up to 7% | Moderate-high (higher dose) | Moderate |
Tirzepatide (Mounjaro) | Weekly injection | 2-5% | High (dual receptor) | Moderate to high |
Liraglutide (Saxenda) | Daily injection | 1-3% | Mild-moderate | Mild |
Oral semaglutide (Rybelsus) | Daily tablet | Up to 2% | Mild-moderate | Mild |
The table shows general patterns, but your individual response may differ significantly. Some people tolerate tirzepatide with no sulfur burps but cannot handle semaglutide, and vice versa. The dual GIP/GLP-1 mechanism of tirzepatide versus semaglutide does not guarantee worse digestive effects for every individual, even though the population-level data suggests slightly higher incidence.
If you are considering switching from tirzepatide to semaglutide or moving to a different agent, discuss the specific digestive side effect profile with your provider. Sometimes the switch itself introduces a new adjustment period with temporary worsening before improvement. Understanding the side effect differences between these medications helps you make an informed decision about whether switching is likely to help.
Special considerations for compounded GLP-1 formulations
Many people taking GLP-1 medications use compounded formulations rather than brand-name products. Compounded semaglutide and compounded tirzepatide contain the same active ingredient and produce the same pharmacological effects, including the gastric emptying delay that causes sulfur burps.
However, compounded formulations sometimes include additional ingredients that can affect digestive tolerance. Some compounded formulations add vitamin B12, glycine, niacinamide, or L-carnitine to the peptide. These additions are generally well-tolerated, but in some individuals, they can slightly alter digestive response.
If you switched from brand-name to compounded or vice versa and noticed a change in sulfur burp frequency, the additional ingredients in the compound might be worth examining. Ask your compounding pharmacy what excipients and additives are in your specific formulation. In most cases, the sulfur burp profile is identical between brand and compounded versions, but individual variation means some people do notice differences.
Storage and handling of compounded formulations can also affect potency and therefore side effect profiles. Properly stored semaglutide and tirzepatide in the fridge maintains consistent potency, which means consistent effects. A degraded peptide from improper storage might produce inconsistent appetite suppression and, potentially, inconsistent digestive side effects from dose to dose. Understanding proper reconstitution and storage is important for anyone using compounded formulations. Those working with tirzepatide reconstitution should follow established protocols to ensure consistent potency and predictable effects. Even details like bacteriostatic water ratios matter for maintaining the stability of your compounded peptide.
The connection between sulfur burps and other GLP-1 side effects
Sulfur burps rarely occur in isolation. They are part of a broader constellation of gastrointestinal side effects that GLP-1 medications produce, and understanding these connections helps you manage the overall picture rather than just treating individual symptoms.
Nausea and sulfur burps often co-occur because both stem from slowed gastric emptying. The nausea tends to be worse in the morning before eating and immediately after meals, while sulfur burps are typically most frequent 1 to 3 hours after eating. Managing nausea through ginger, smaller meals, and anti-nausea strategies often improves sulfur burps too, since both respond to the same underlying mechanism. The overall feeling on semaglutide and tirzepatide improves significantly as the body adapts.
Constipation and sulfur burps create a particularly frustrating combination. Constipation means contents are backing up in the large intestine, which creates additional fermentation opportunity and can increase gas production throughout the entire digestive tract. Addressing constipation through fiber, hydration, and gentle osmotic laxatives often reduces sulfur burp frequency as a secondary benefit.
Bloating and sulfur burps share the same root cause: excess gas from fermentation. When your stomach feels bloated and distended, it is because trapped gas is creating pressure. Sulfur burps are simply that gas escaping upward. Managing bloating on semaglutide through the same dietary and lifestyle modifications that address sulfur burps creates a synergistic improvement across all these connected symptoms.
Fatigue and digestive symptoms are also connected. When your digestive system is working harder to process food through a slower system, more energy gets directed to digestion, which can contribute to the fatigue some people experience on GLP-1 medications. Improving digestive efficiency through the strategies in this guide can actually help with energy levels too, creating a positive cycle where better digestion means less fatigue, which means more energy for the physical activity that further improves digestion.
Injection site, formulation, and sulfur burps
While the injection site does not directly affect sulfur burp production (the medication ends up in your bloodstream regardless of where you inject it), absorption rate can vary between injection sites, and this can subtly affect the peak medication level and therefore the intensity of gastric emptying delay.
Abdominal injections tend to provide the fastest absorption rate, which means a sharper peak in medication levels and potentially more intense initial digestive effects. Thigh injections, like those described in tirzepatide thigh injection guides, and upper arm injections may provide slightly slower absorption, leading to a more gradual onset of effects. The difference is subtle, but for people who find sulfur burps are worst in the 24 hours after injection and then improve, experimenting with injection site rotation might slightly smooth out the intensity curve.
The best injection site for GLP-1 medications depends on multiple factors beyond sulfur burp management, including comfort, absorption consistency, and injection site reactions. But if you are looking for every possible edge in managing digestive side effects, injection site rotation is one more variable to experiment with.
For those exploring alternative delivery methods, oral semaglutide drops and tirzepatide drops represent different absorption pathways that may produce different digestive effect profiles. Sublingual and oral formulations bypass first-pass metabolism differently than injections, and some users report different patterns of digestive side effects with these alternative routes. The oral versus injection comparison for tirzepatide covers these differences in detail.
Building a complete sulfur burp management protocol
Rather than trying everything at once, a systematic approach to managing sulfur burps on GLP-1 medications gives you the best chance of identifying what works specifically for you. Here is a week-by-week protocol that combines the strategies from this guide into a practical action plan.
Week 1: Foundation. Start the dietary elimination phase (remove eggs, cruciferous vegetables, garlic, onions, carbonated drinks, sugar-free gum). Increase water intake to 8 to 10 glasses daily. Begin eating smaller, more frequent meals. Track sulfur burp frequency and timing in a simple log.
Week 2: Add supplements. Start a broad-spectrum probiotic containing Lactobacillus and Bifidobacterium strains. Take daily with breakfast. Add a digestive enzyme supplement before your two largest meals. Continue dietary elimination and tracking.
Week 3: Optimize timing. Evaluate your tracking log. Identify peak sulfur burp times relative to meals and injection. Adjust injection timing if possible to put peak digestive effects on your least socially demanding days. Add peppermint or ginger tea after meals during your peak burp times.
Week 4: Evaluate and adjust. Compare your Week 4 symptom frequency and severity to Week 1. If improvement is meaningful (50% or more reduction), begin gradual food reintroduction as described earlier. If improvement is minimal, add bismuth subsalicylate (Pepto-Bismol) after meals and consider discussing slower dose titration with your provider.
Weeks 5 to 8: Fine-tune. Continue reintroducing foods one at a time. Maintain the supplements and lifestyle changes that are working. Most people find that by week 8, sulfur burps have reduced significantly from their initial severity. If they remain problematic, consider the medical evaluation outlined earlier (SIBO testing, H. pylori testing, etc.).
For researchers navigating these protocols, SeekPeptides members access comprehensive guides on managing GLP-1 medication side effects, with detailed protocols and community support from thousands of experienced users who have worked through these exact challenges.
Alcohol, caffeine, and sulfur burps on GLP-1 medications
Two of the most common questions about lifestyle and GLP-1 medications involve alcohol and caffeine. Both can affect sulfur burp frequency and severity, though in different ways.
Alcohol is a known gastric irritant that can independently increase burping, bloating, and digestive discomfort. When combined with the slowed gastric emptying from a GLP-1 medication, alcohol sits in the stomach longer and produces more gas during fermentation. Beer is particularly problematic because it is both carbonated and contains fermentable carbohydrates. Wine contains sulfites, which can contribute additional sulfur compounds to the digestive mix. If you are going to drink on tirzepatide or drink on semaglutide, clear spirits with non-carbonated mixers produce the least sulfur burp aggravation. Limiting intake to 1 to 2 drinks and avoiding them on the first 2 days after injection (when gastric emptying is most delayed) is practical advice.
If you prefer choosing the best alcohol while on tirzepatide, vodka or tequila mixed with soda water and lime tends to be the lowest-impact choice for digestive symptoms. But the honest answer is that reducing or eliminating alcohol during the adjustment period produces the most noticeable improvement in sulfur burps.
Caffeine has a more nuanced relationship with sulfur burps. Coffee stimulates gastric acid production and can increase gut motility, which theoretically should help move food through faster and reduce fermentation time. Some GLP-1 medication users find that a cup of coffee after meals actually reduces sulfur burps. Others find that the acid stimulation worsens GERD-related burping. If you already drink coffee, there is likely no need to stop. But monitor whether it improves or worsens your symptoms and adjust accordingly.
Exercise and physical activity for sulfur burp relief
Physical activity deserves its own section because its impact on sulfur burps is significant and often underappreciated. Movement stimulates gastric motility, the process of food moving through the digestive tract. On a GLP-1 medication where gastric emptying is slowed, any activity that increases motility works in your favor.
Walking is the single most effective and accessible exercise for reducing sulfur burps. A 15 to 20 minute walk after meals promotes gastric emptying, reduces bloating, and helps trapped gas pass through the digestive system more efficiently. Multiple studies have shown that post-meal walking reduces gas retention and bloating even in people not taking GLP-1 medications, and the effect is amplified when gastric emptying is already compromised.
Yoga poses that involve gentle twisting and compression of the abdomen can help release trapped gas. Poses like wind-relieving pose (Pavanamuktasana), seated spinal twist (Ardha Matsyendrasana), and child pose (Balasana) are specifically used in traditional practice for digestive relief. While the evidence is more experiential than clinical, many GLP-1 medication users find that a 10 to 15 minute yoga routine focused on these poses reduces both bloating and sulfur burp frequency.
Intense exercise close to meals can actually worsen digestive symptoms by diverting blood flow away from the digestive system. Keep vigorous workouts (running, HIIT, heavy resistance training) at least 1 to 2 hours away from meals. Light to moderate activity (walking, gentle cycling, stretching) is fine immediately after eating and actively beneficial for sulfur burp management. This advice aligns with broader guidance on maintaining results on GLP-1 medications through sustainable exercise habits.
Sleep, stress, and their impact on digestive function
The gut-brain axis means that your psychological state directly affects your digestive function, and vice versa. Stress and poor sleep can both worsen sulfur burps on GLP-1 medications through measurable physiological pathways.
Chronic stress elevates cortisol levels, which can slow digestive motility, alter gut microbiome composition, and increase intestinal permeability. All of these effects compound the digestive slowing already caused by your medication, creating a worse environment for fermentation and gas production. Stress management techniques, whether meditation, breathing exercises, time in nature, or whatever works for you, are not just good general advice. They are specifically relevant to managing digestive side effects of GLP-1 medications.
Poor sleep is equally impactful. Sleep deprivation alters ghrelin and leptin levels (hormones that regulate appetite and digestion), increases cortisol production, and disrupts the circadian rhythm of your gut bacteria. Research shows that as few as two nights of poor sleep can measurably change gut microbiome activity in ways that increase gas production. If your sulfur burps are worse during stressful periods or when you are sleeping poorly, addressing those factors may improve your digestive symptoms more than any supplement.
The connection between sleep, stress, and GLP-1 medication effects goes beyond sulfur burps. Fatigue on tirzepatide and semaglutide-related fatigue can create a cycle where poor sleep worsens digestive symptoms, digestive discomfort disrupts sleep further, and the combined effect makes side effects harder to tolerate. Breaking this cycle by prioritizing sleep hygiene, consistent bedtimes, cool bedroom temperature, limiting screens before bed, often produces surprisingly broad improvements across multiple symptom categories.
For those experiencing anxiety alongside their GLP-1 treatment, the digestive effects can sometimes amplify anxious feelings, particularly the social anxiety around potential embarrassing episodes. Addressing both the physical sulfur burp management and the psychological impact simultaneously produces better outcomes than treating either in isolation.
Frequently asked questions
Are sulfur burps dangerous on GLP-1 medications?
No. Sulfur burps are unpleasant but not dangerous in themselves. They indicate bacterial fermentation in the digestive tract producing hydrogen sulfide gas. This is a normal biological process that becomes more pronounced when GLP-1 medications slow gastric emptying. However, if sulfur burps are accompanied by severe pain, vomiting, bloody stools, or fever, seek medical attention as these could indicate an underlying condition.
How long do sulfur burps last on semaglutide or tirzepatide?
Most people experience the worst sulfur burps during the first 2 to 6 weeks of treatment and after each dose increase. For the majority, symptoms improve significantly by weeks 8 to 12 as the body adapts to the medication. Some people find that dietary modifications and probiotics reduce sulfur burps to a manageable level within 1 to 2 weeks, while others require the full adaptation period.
Will sulfur burps go away on their own?
Often, yes. The gut microbiome adapts to the altered digestive environment over time, and sulfur burp frequency and intensity typically decrease as this adaptation occurs. However, waiting passively can mean weeks or months of discomfort. Active management through dietary changes, probiotics, and the other strategies in this guide can significantly accelerate improvement.
Can I take Pepto-Bismol with my GLP-1 medication?
Bismuth subsalicylate (Pepto-Bismol) is generally safe to take alongside GLP-1 medications for short-term relief of sulfur burps and diarrhea. There are no known significant drug interactions. However, do not take it daily for extended periods (more than 2 weeks) without consulting your doctor, as long-term bismuth use has its own considerations. Also be aware that it can cause black stools, which is harmless but can be startling.
Do sulfur burps mean my medication is not working?
No. Sulfur burps actually indicate that the medication IS affecting your digestive system, which is part of how it works. The same mechanism that slows gastric emptying to suppress appetite also creates the conditions for increased gas production. Having sulfur burps does not mean the medication is ineffective, and their absence does not mean it is not working either.
Should I stop my GLP-1 medication because of sulfur burps?
Sulfur burps alone are not typically a reason to stop treatment. The benefits of GLP-1 medications for weight management and metabolic health significantly outweigh the temporary inconvenience of sulfur burps for most people. Try the management strategies in this guide first. If sulfur burps remain severe and intolerable despite all interventions after 8 to 12 weeks, discuss alternative medications or dose adjustments with your prescriber rather than stopping treatment entirely. Understanding how to properly wean off if necessary is important, as abrupt discontinuation has its own considerations.
Does injection timing affect sulfur burps?
Yes, indirectly. Sulfur burps tend to be most intense during the 24 to 72 hours after injection when medication levels peak. Choosing your injection day strategically allows you to manage the worst symptoms during times that are less socially demanding. Some people also find that injecting in the evening produces milder next-day digestive effects than morning injections, though this varies individually.
Are some people more prone to sulfur burps on GLP-1 medications?
Yes. People with pre-existing digestive conditions (IBS, GERD, SIBO, lactose intolerance), those with diets naturally high in sulfur-containing foods, and those with certain gut microbiome compositions tend to experience more sulfur burps. Additionally, people who are more sensitive to changes in gastric motility, and those on higher medication doses, may be more prone. Using dosage calculators to determine appropriate dosing can help minimize unnecessary side effects from taking more medication than needed.
External resources
PMC: Tirzepatide reduces appetite, energy intake, and fat mass (clinical study)
Medical News Today: Sulfur burps remedies, treatment, and causes
For researchers serious about optimizing their GLP-1 protocols and managing side effects effectively, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your digestion stay comfortable, your burps stay odorless, and your GLP-1 journey stay on track.