Mar 2, 2026

On paper, phentermine and tirzepatide both help people lose weight. Both require a prescription. Both suppress appetite. But the similarities stop right there, and the differences between these two medications could mean the difference between losing 7% of your body weight and losing 22%.
That gap is not small. It is enormous. And it matters because choosing the wrong medication for your situation does not just waste money. It wastes months of effort, creates unnecessary side effects, and delays the results you actually want. Phentermine has been the go-to weight loss prescription for decades, a stimulant that kicks in fast and costs almost nothing. Tirzepatide is the newer, more powerful option, a dual-action GLP-1/GIP receptor agonist that produces weight loss numbers researchers have never seen from any other medication. One works through raw appetite suppression. The other rewires how your body handles hunger, fullness, and blood sugar at the hormonal level.
This guide breaks down every meaningful difference between phentermine and tirzepatide. Mechanisms. Clinical trial data. Side effect profiles. Cost. Duration of use. And the practical question everyone actually needs answered: which one should you choose? Whether you are considering your first weight loss medication, switching from phentermine to something stronger, or trying to understand why your doctor recommended one over the other, the comparison that follows will give you specific numbers and evidence to make a genuinely informed decision. SeekPeptides has analyzed the clinical data, community experiences, and real-world outcomes to build the most thorough comparison available.
How phentermine works: the stimulant approach
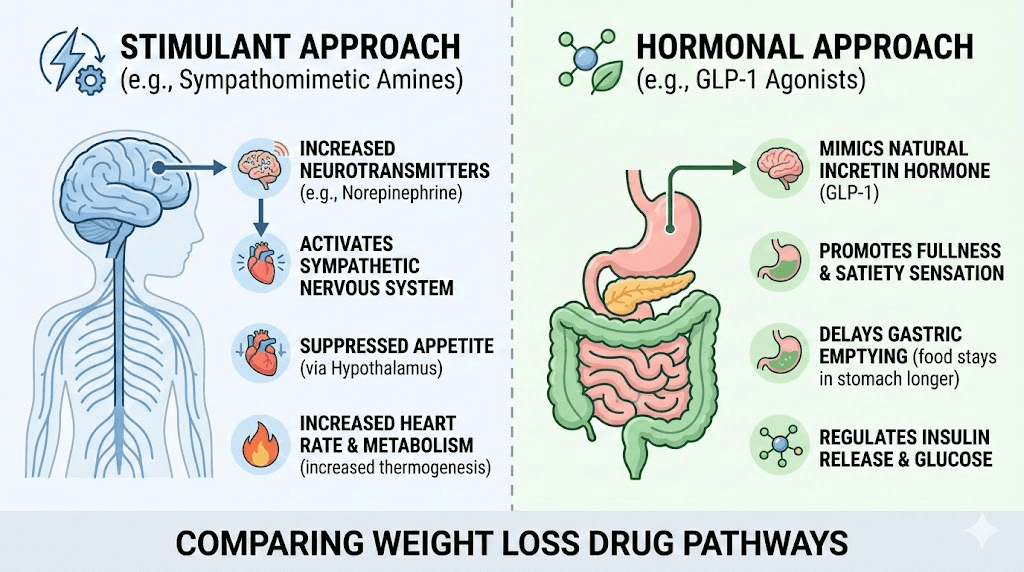
Phentermine is a sympathomimetic amine. In plain language, it is a stimulant that tells your brain to release more norepinephrine, the same neurotransmitter behind your fight-or-flight response. That flood of norepinephrine suppresses hunger signals in the hypothalamus, the part of your brain that controls appetite.
Think of it like drinking strong coffee, but specifically targeted at hunger. Your appetite drops. Your energy goes up. You eat less because you genuinely feel less hungry, not because you are white-knuckling through cravings.
The mechanism is straightforward. Phentermine does one thing, and it does it fast. Within days of your first dose, appetite suppression kicks in. Most people notice a dramatic reduction in hunger within the first week. That rapid onset is one of phentermine biggest advantages, because there is no slow titration period and no waiting weeks to feel something happening. The medication works differently from GLP-1 drugs in almost every way, targeting the central nervous system rather than gut hormones.
But that stimulant mechanism comes with limitations. Your body adapts. Tolerance develops. The appetite suppression that felt dramatic in week one starts fading by week eight or twelve. This is why the FDA approved phentermine only for short-term use, typically 12 weeks or less. Some physicians prescribe it longer, and research supports extended use in certain cases, but the fundamental problem remains: phentermine is fighting your biology with a blunt instrument, and your biology eventually fights back.
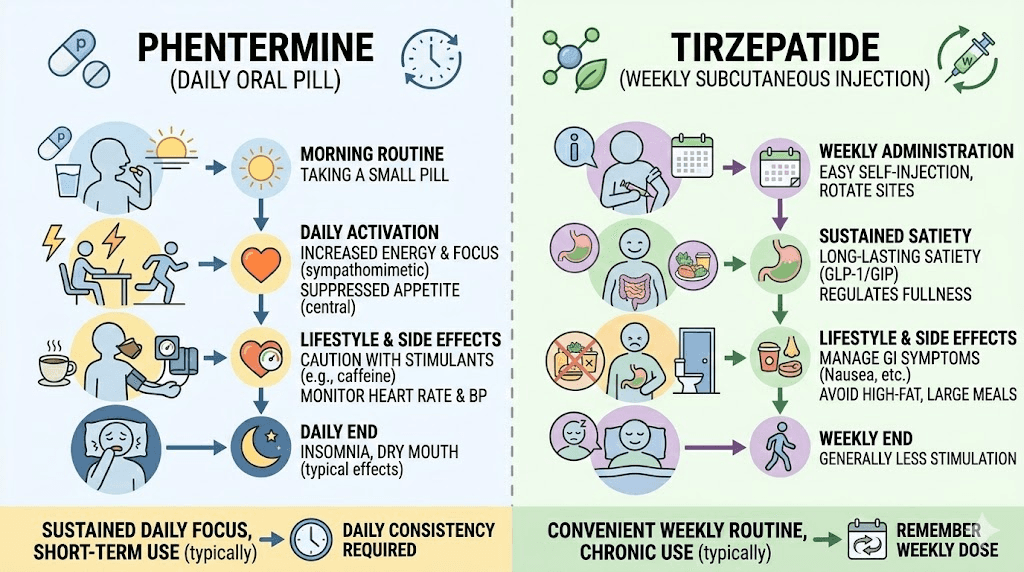
The standard dose is 37.5 mg taken once daily in the morning. Some doctors start at 15 mg or 30 mg. You take it orally, and the timing matters. Take it too late in the day and the stimulant effects will keep you awake at night, which is exactly the problem you want to avoid with medication-related insomnia.
How tirzepatide works: the hormonal approach
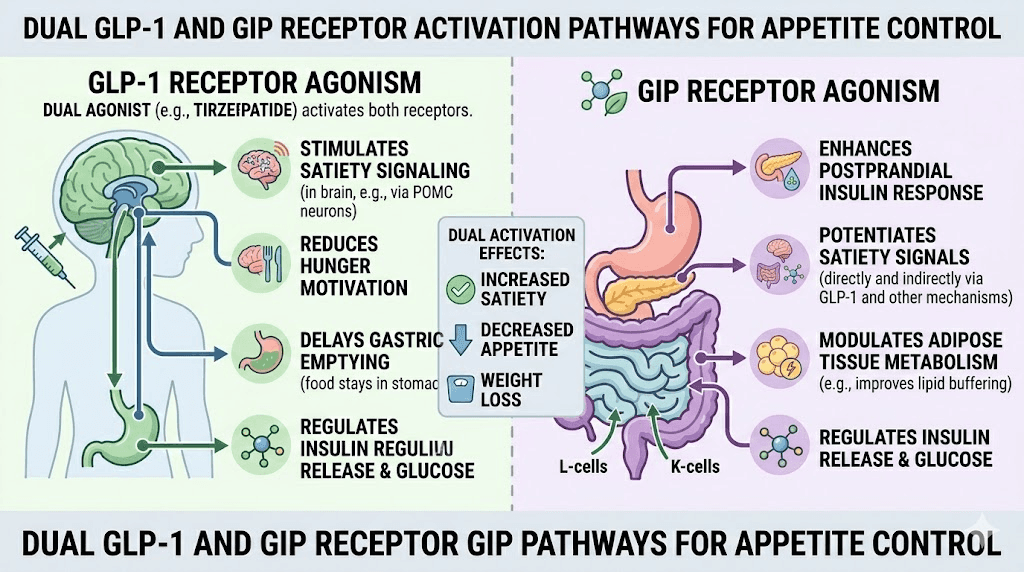
Tirzepatide operates on an entirely different level. Instead of stimulating your nervous system, it mimics two natural hormones that your gut already produces: GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide). This dual-agonist mechanism is what makes tirzepatide unique among all available weight loss medications, and it is the reason the weight loss results are so dramatically different from everything that came before.
GLP-1 slows gastric emptying. Food sits in your stomach longer. You feel full sooner and stay full longer. GIP amplifies that effect while also improving how your body handles insulin and glucose. Together, these two pathways create a multi-layered approach to appetite control that phentermine simply cannot match.
Here is what that looks like in practice. With phentermine, you lose interest in food because a stimulant is overriding your hunger signals. With tirzepatide, your body genuinely believes it is full. The satiety signals are real, coming from actual hormonal pathways rather than artificial stimulation. This distinction matters enormously for long-term adherence, because people on tirzepatide report that they simply do not think about food as much. The mental burden of dieting, the constant negotiation with cravings, largely disappears.
Tirzepatide is administered as a weekly subcutaneous injection, typically in the abdomen, thigh, or upper arm. Dosing starts low at 2.5 mg per week and increases gradually over several months. The standard titration schedule moves from 2.5 mg to 5 mg after four weeks, then to 7.5 mg, 10 mg, 12.5 mg, and potentially 15 mg, with each increase separated by at least four weeks. This slow ramp-up is critical because it allows the body to adjust and minimizes the gastrointestinal side effects that are most common in the early weeks. You can reference a complete tirzepatide dose chart for the full schedule.
The brand names are Mounjaro (approved for type 2 diabetes) and Zepbound (approved specifically for weight management). Both contain tirzepatide. The medication itself is identical.
Weight loss results: the numbers tell the story
Clinical data does not lie. And in this comparison, the clinical data is devastating for phentermine.
Phentermine weight loss data
In clinical studies, phentermine produces an average weight loss of 5% to 10% of body weight over 12 weeks to 6 months. A randomized controlled trial found that patients taking 37.5 mg of phentermine daily lost an average of 6.7 kg (about 14.8 pounds). Another 12-week study showed 95% of participants lost at least 5% of their body weight, while 62% lost at least 10%. A six-month study demonstrated weight reductions of 7.5 kg at three months and 10 kg at six months.
Those are decent numbers. Not transformative, but meaningful.
Longer-term data is encouraging but limited. Patients who used phentermine continuously for more than 12 months maintained a 7.4% weight loss at the 24-month mark. Importantly, no increased cardiovascular risk was observed with longer-term use up to three years, which challenges the old assumption that phentermine becomes dangerous over time.
For someone weighing 200 pounds, phentermine typically produces a loss of 10 to 20 pounds. For someone at 250 pounds, expect 12.5 to 25 pounds. Real results. But not the kind of dramatic transformation that most people looking into weight loss medications are hoping for, especially when they have struggled with other approaches.
Tirzepatide weight loss data
The SURMOUNT clinical trial program tells a completely different story. In SURMOUNT-1, the landmark trial for tirzepatide in weight management, participants without diabetes achieved the following results over 72 weeks:
5 mg dose: 16.0% average body weight reduction
10 mg dose: 21.4% average body weight reduction
15 mg dose: 22.5% average body weight reduction
Read that again. At the highest dose, the average participant lost nearly a quarter of their body weight. Not the best responders. The average.
The responder rates were equally striking. Between 89% and 91% of participants on the 10 mg or 15 mg doses achieved at least 5% weight loss. Between 78% and 84% achieved at least 10%. And between 50% and 57% lost 20% or more of their body weight. For someone starting at 250 pounds, a 22.5% reduction means losing over 56 pounds. That is not just weight loss. That is a complete transformation in body composition, metabolic health, and quality of life.
SURMOUNT-4 demonstrated that continued treatment maintained these results. Participants who completed a 36-week lead-in period showed a mean weight reduction of 20.9%, with those continuing tirzepatide reaching an overall reduction of 25.3% from baseline to week 88. People who switched to placebo after the lead-in regained significant weight, proving that the medication needs to be continued for sustained results. Understanding how to maintain weight loss after tirzepatide is critical for long-term planning.
SURMOUNT-2, which studied participants with type 2 diabetes, showed up to 15.7% mean weight loss with tirzepatide versus 3.3% with placebo. Even in a population where weight loss is typically harder to achieve, tirzepatide outperformed every other available option.
Head-to-head comparison table
Metric | Phentermine | Tirzepatide |
|---|---|---|
Average weight loss | 5-10% of body weight | 16-22.5% of body weight |
Study duration | 12 weeks to 6 months | 72 weeks (SURMOUNT-1) |
Patients losing 5%+ | 80-95% | 89-91% (10-15 mg) |
Patients losing 10%+ | 62% | 78-84% (10-15 mg) |
Patients losing 20%+ | Not typically measured | 50-57% (10-15 mg) |
Absolute weight loss (200 lb person) | 10-20 lbs | 32-45 lbs |
The gap is not subtle. Tirzepatide produces roughly two to three times more weight loss than phentermine across every measure. For individuals who need significant weight reduction, whether for health reasons, quality of life, or to reduce the risk of obesity-related conditions, tirzepatide delivers results that phentermine simply cannot approach. Understanding your BMI requirements for GLP-1 medications can help determine eligibility.
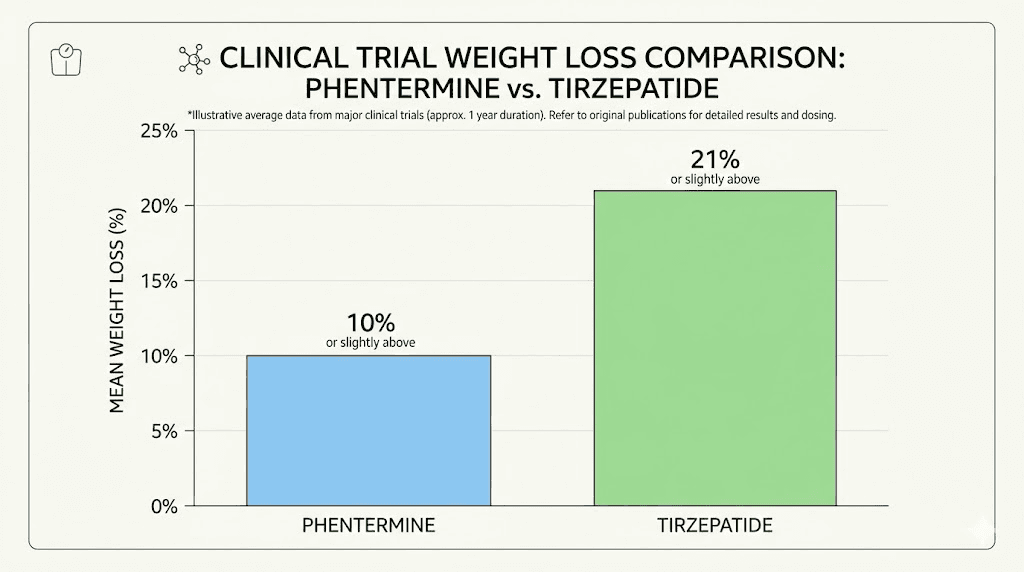
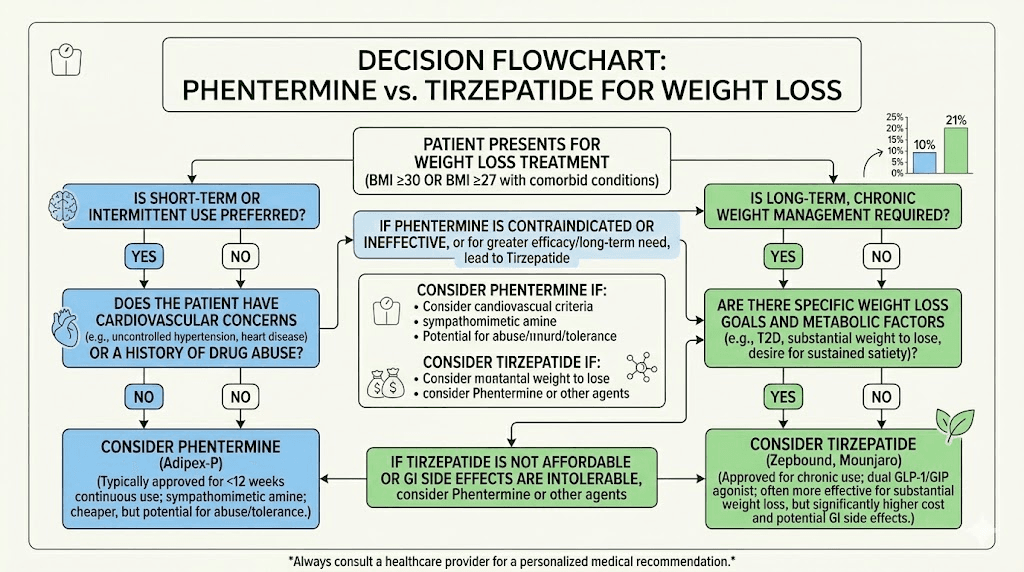
Alt: Phentermine vs tirzepatide clinical trial weight loss results comparison chart
Speed of results: how quickly each medication works
Speed matters. When someone starts a weight loss medication, they want to know when results become visible. And here, phentermine has one genuine advantage.
Phentermine works fast. Most people notice appetite suppression within days, sometimes within hours of the first dose. Weight loss often begins in the first week. By the end of month one, many patients have already lost 3-5% of their body weight. That immediate feedback is psychologically powerful, reinforcing the behavior changes that support continued weight loss.
Tirzepatide takes longer to ramp up. The first four weeks at 2.5 mg are essentially a tolerability phase. Meaningful appetite suppression usually begins around weeks two to four for some people, while others do not feel a significant effect until reaching the 5 mg or 7.5 mg dose. Most people who track the first dose experience notice subtle changes early, but dramatic results typically appear between months two and four as the dose increases.
But here is where the comparison gets interesting. By month three, tirzepatide has usually caught up to and surpassed phentermine total weight loss, despite the slower start. And by month six, tirzepatide users have typically lost double what phentermine users have achieved. The slow start is a feature, not a bug. It is the careful titration that allows people to reach higher, more effective doses without intolerable side effects.
Week-by-week timeline comparison
Timepoint | Phentermine | Tirzepatide |
|---|---|---|
Week 1 | Appetite drops noticeably, 1-2 lb loss | Mild appetite changes, adjusting to medication |
Week 4 | 3-5% body weight lost | 1-3% body weight lost, increasing to 5 mg |
Week 8 | 5-7% body weight lost, possible tolerance | 3-5% body weight lost, increasing to 7.5 mg |
Week 12 | 7-10% body weight lost (typical endpoint) | 5-8% body weight lost, reaching higher doses |
Week 24 | Maintenance or slight regain if stopped | 10-15% body weight lost |
Week 48 | Significant regain without medication | 16-20% body weight lost |
Week 72 | Most gains reversed if not maintained | 20-22.5% body weight lost |
The early speed advantage of phentermine evaporates entirely when you look at six-month and twelve-month outcomes. Tirzepatide wins the marathon by a massive margin, even though phentermine wins the sprint. For people who want to understand tirzepatide speed in more detail, the trajectory becomes clearer once you see the dose-response relationship at each titration step.
Side effects compared: stimulant problems vs. gut problems
Every weight loss medication comes with trade-offs. The side effect profiles of phentermine and tirzepatide are dramatically different because their mechanisms are fundamentally different. One creates stimulant-based problems. The other creates gastrointestinal problems. Understanding which set of side effects you can tolerate is often more important than the weight loss numbers alone.
Phentermine side effects
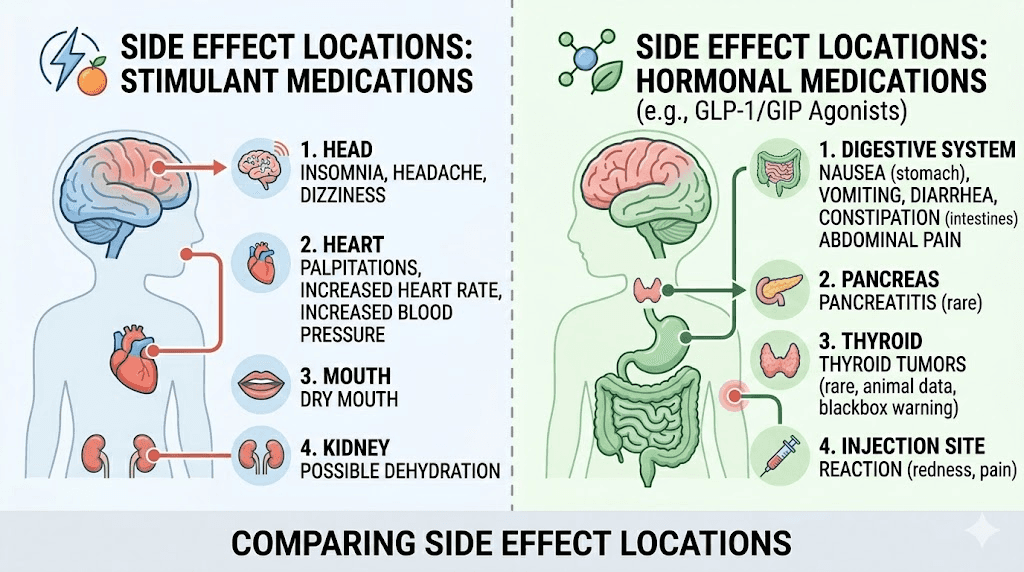
Phentermine is a stimulant, and it behaves like one. The most common side effects include:
Insomnia: The number one complaint. Phentermine increases alertness, and if taken too late in the day, sleep becomes difficult or impossible. Morning dosing is essential.
Dry mouth: Phentermine reduces saliva production as part of its nervous system stimulation. Extremely common and persistent throughout treatment.
Increased heart rate: Resting heart rate may increase by 5-15 beats per minute. This is the side effect that concerns doctors most, particularly for patients with existing cardiovascular conditions.
Elevated blood pressure: The sympathomimetic effect raises blood pressure in many patients, requiring monitoring.
Restlessness and jitteriness: Similar to consuming too much caffeine. Some patients feel anxious, on edge, or unable to relax.
Headaches: Common in the first week or two, usually resolving as the body adjusts.
Constipation or diarrhea: Digestive changes occur in some patients, though less commonly than with GLP-1 medications.
Rare but serious risks include pulmonary hypertension, heart valve disease, and psychological dependence. Phentermine is classified as a Schedule IV controlled substance because of its stimulant properties and potential for abuse. It should never be used in patients with coronary artery disease, arrhythmias, uncontrolled hypertension, or a history of drug abuse. The anxiety-related side effects are worth comparing across medication classes.
Most common side effects diminish within one to two weeks as the body adapts. But the cardiovascular effects, specifically the increased heart rate and blood pressure, persist throughout treatment and require regular monitoring.
Tirzepatide side effects
Tirzepatide side effects center almost entirely on the gastrointestinal system. This makes sense given the mechanism: slowing gastric emptying and altering gut hormone signaling naturally affects the digestive tract. The most common side effects include:
Nausea: The most frequently reported side effect, affecting roughly 20-30% of patients. Usually worst during dose increases and improves as the body adjusts. Understanding which foods to avoid can significantly reduce this problem.
Diarrhea: Affects about 15-20% of patients. Most common during the titration phase and usually resolves within a few weeks at each new dose. See the guide on how long tirzepatide diarrhea lasts for specific timelines.
Constipation: The opposite problem affects another subset of patients. Slowed gastric motility means food moves more slowly through the entire digestive tract. There are effective constipation treatment strategies specifically for tirzepatide users.
Decreased appetite: Technically a therapeutic effect, but some patients find the appetite suppression too aggressive, especially at higher doses, leading to inadequate calorie intake.
Fatigue: Reported by some patients, particularly early in treatment. The relationship between tirzepatide and tiredness is complex, sometimes related to reduced calorie intake rather than the medication itself. GLP-1 fatigue management strategies can help.
Injection site reactions: Redness, itching, or mild swelling at the injection site. Usually minor and temporary. Learn about injection site reaction treatment if this occurs.
Headaches: Less common than with phentermine but reported by some patients. The tirzepatide headache connection is typically dose-related.
Rare but serious risks include pancreatitis, gallbladder problems, and thyroid C-cell tumors (observed in animal studies, clinical significance in humans unclear). Tirzepatide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2.
The critical difference: tirzepatide side effects are almost entirely gastrointestinal and typically improve with time, while phentermine side effects include cardiovascular concerns that persist and require ongoing monitoring. For most patients, GI discomfort that fades over weeks is far more manageable than chronic elevated heart rate and blood pressure. Some people also experience body aches, insomnia, or muscle pain on tirzepatide, though these are less common than the GI effects.
Side effect comparison table
Side effect category | Phentermine | Tirzepatide |
|---|---|---|
Primary system affected | Cardiovascular/CNS | Gastrointestinal |
Insomnia | Very common | Uncommon |
Increased heart rate | Common | Rare |
Nausea | Uncommon | Very common (20-30%) |
Constipation | Occasional | Common (10-15%) |
Diarrhea | Occasional | Common (15-20%) |
Dry mouth | Very common | Uncommon |
Jitteriness/anxiety | Common | Rare |
Fatigue | Rare (usually energizing) | Common early on |
Side effects improve over time? | Partially (tolerance develops) | Yes (most resolve within weeks) |
Cardiovascular monitoring needed? | Yes (BP and heart rate) | Minimal |
Abuse potential | Yes (Schedule IV) | None |
Duration of treatment: short-term fix vs. long-term solution
This is where the fundamental philosophy behind each medication becomes clear. Phentermine was designed as a short-term intervention. Tirzepatide was designed as a long-term treatment. That distinction shapes everything about how they are prescribed, how they perform over time, and what happens when you stop.
Phentermine treatment duration
The FDA approved phentermine for short-term use only, defined as a few weeks, typically up to 12 weeks. The reasoning is straightforward: tolerance develops, effectiveness wanes, and the stimulant risks accumulate. Most prescribing guidelines recommend 8 to 12 weeks of treatment, followed by a break.
Some physicians prescribe phentermine for longer periods. A large retrospective study found that patients who used phentermine continuously for more than 12 months maintained greater weight loss at 24 months (7.4% more than the referent group) without increased cardiovascular risk. This has shifted the conversation somewhat, and off-label longer-term use is becoming more common in obesity medicine. But the fundamental limitation remains: phentermine effectiveness plateaus and often declines over time as the body adapts to the stimulant effect.
Weight regain after stopping phentermine is the norm, not the exception. Without the artificial appetite suppression, hunger returns to baseline levels. Most patients who do not implement sustained lifestyle changes regain a significant portion of lost weight within 6 to 12 months of discontinuation. This is not a character flaw. It is biology. The same neurological pathways that adapted to the stimulant adapt back when the stimulant is removed.
Tirzepatide treatment duration
Tirzepatide is designed for ongoing treatment. The SURMOUNT clinical trials studied participants for 72 to 88 weeks, and real-world use is expected to continue indefinitely for many patients. The medication does not lose effectiveness over time in the same way phentermine does, because it works through hormonal pathways that do not develop the same kind of tolerance.
SURMOUNT-4 provided the strongest evidence for continued treatment. Participants who switched from tirzepatide to placebo after 36 weeks of treatment regained substantial weight, while those who continued tirzepatide maintained their weight loss and continued losing. This confirmed what obesity researchers have argued for years: obesity is a chronic condition that requires ongoing treatment, just like hypertension or diabetes.
The weight regain pattern after stopping tirzepatide is significant. Studies show that patients regain approximately two-thirds of lost weight within a year of discontinuation. This does not mean the medication failed. It means the underlying biology that caused the weight gain still exists, and the medication was managing it effectively. Understanding how to maintain weight loss after tirzepatide requires a comprehensive strategy that some patients can implement with lower maintenance doses or careful weaning protocols.
For people who need long-term weight management, tirzepatide offers something phentermine cannot: sustained effectiveness over months and years of continuous use. The question is not whether tirzepatide works long-term. It does. The question is whether you can afford and access it long-term, which brings us to cost.
Cost comparison: the price gap is enormous
If cost were the only factor, this comparison would be over before it started. Phentermine is one of the cheapest prescription medications available. Tirzepatide is one of the most expensive. The gap between them is not 2x or 3x. It is often 10x to 30x.
Phentermine cost
Generic phentermine costs between $15 and $50 per month at retail prices. With discount cards from programs like GoodRx or SingleCare, the price drops to $8 to $20 per month. The brand-name version, Adipex-P, costs around $110 per month but offers no clinical advantage over generics.
Most insurance plans cover generic phentermine with minimal copays. Even without insurance, the out-of-pocket cost is trivial. For a three-month course of treatment, the total cost ranges from $24 to $150. This accessibility is one of phentermine biggest advantages and a major reason it remains widely prescribed despite the availability of more effective alternatives.
Tirzepatide cost
The list price for brand-name tirzepatide (Mounjaro or Zepbound) is approximately $1,080 per 28-day supply. That works out to roughly $1,100 to $1,200 per month at retail pricing. Without insurance or discount programs, tirzepatide costs $300 to $700 per month through various compounding pharmacies and direct programs. Checking options for affordable tirzepatide and cheap compounded tirzepatide can reveal significant savings.
Insurance coverage varies wildly. If you have type 2 diabetes, your insurance may cover Mounjaro with a copay as low as $25 through Eli Lilly savings programs. For weight management (Zepbound), coverage is less common, though it is expanding. Some employers and insurance plans now cover GLP-1 medications for obesity, but many do not. For the latest insurance coverage details by provider, it is worth checking your specific plan.
Compounded tirzepatide through 503B compounding pharmacies has become a popular alternative. Prices for compounded versions range from $150 to $400 per month depending on the pharmacy, dose, and whether additional compounds like B12, glycine, or niacinamide are included. Providers like Empower Pharmacy, Strive Pharmacy, and others offer various pricing structures.
Cost comparison table
Cost factor | Phentermine | Tirzepatide |
|---|---|---|
Monthly cost (generic/retail) | $15-50 | $300-700 (compounded) / $1,080+ (brand) |
Monthly cost (with discounts) | $8-20 | $150-400 (compounded) / $25-150 (insured) |
3-month total cost | $24-150 | $450-3,240+ |
12-month total cost | $96-600 | $1,800-12,960+ |
Insurance coverage | Almost always covered | Variable, improving |
Generic available | Yes (decades old) | No (patent protected) |
When you calculate cost per pound lost, the math gets more interesting. Phentermine at $30/month for 3 months ($90 total) producing 15 pounds of weight loss equals $6 per pound. Tirzepatide at $400/month for 12 months ($4,800 total) producing 50 pounds of weight loss equals $96 per pound. Tirzepatide is far more expensive per month and per pound, but it also produces results that phentermine cannot achieve at any price. For some people, the additional weight loss justifies the cost. For others, phentermine provides adequate results at a fraction of the price. Use the peptide cost calculator to estimate your specific expenses.
Who should choose phentermine
Phentermine is not the wrong choice for everyone. There are clear situations where it makes more sense than tirzepatide, and dismissing it entirely because tirzepatide produces more weight loss would be a mistake.
Phentermine may be the better choice if:
You need to lose a moderate amount of weight (10-20 pounds). If your goal is modest, phentermine can get you there without the cost, injections, or months-long titration of tirzepatide.
You need results quickly. If you have a medical procedure coming up, a health milestone to hit, or simply need the psychological boost of fast visible results, phentermine immediate onset is a genuine advantage.
Cost is a major barrier. At $15-50 per month, phentermine is accessible to almost everyone. If tirzepatide is financially out of reach and insurance will not cover it, phentermine provides real, measurable weight loss at minimal cost.
You want a short-term jumpstart. Some physicians use phentermine as a bridge, kickstarting weight loss and motivation while patients implement lifestyle changes that will sustain results long-term.
You cannot tolerate GI side effects. If you have a sensitive stomach, history of GI issues, or know from past experience that nausea is intolerable for you, phentermine avoids those problems entirely.
You prefer oral medication over injections. Phentermine is a daily pill. Tirzepatide requires weekly injections, although oral tirzepatide options and sublingual drops are emerging.
Phentermine is also a reasonable first-line option for younger patients without cardiovascular risk factors who want to try medication-assisted weight loss without committing to a more intensive and expensive regimen. If phentermine works, and for some people it works very well, there is no reason to move to tirzepatide. Understanding how phentermine compares to semaglutide provides additional context for the broader medication landscape.
Who should choose tirzepatide
Tirzepatide is the clear winner for anyone who needs substantial weight loss and can access it. The clinical data is unambiguous. No other available medication produces comparable results.
Tirzepatide may be the better choice if:
You need to lose 15% or more of your body weight. Phentermine rarely achieves this level of weight loss. Tirzepatide routinely does. If your BMI is 35+ and you need significant reduction, tirzepatide is the stronger tool.
You have type 2 diabetes or prediabetes. Tirzepatide addresses both weight and blood sugar simultaneously. The GLP-1/GIP mechanism improves insulin sensitivity, reduces HbA1c, and produces weight loss. Phentermine does none of this.
You want long-term treatment. If you understand that obesity often requires ongoing management, tirzepatide offers sustained effectiveness that phentermine cannot provide beyond a few months.
Previous weight loss attempts have failed. If phentermine did not produce adequate results, if diet and exercise alone were insufficient, or if you have hit a plateau with other approaches, tirzepatide offers a fundamentally different mechanism that may succeed where others have failed.
You have cardiovascular concerns. Unlike phentermine, tirzepatide does not increase heart rate or blood pressure. For patients with existing cardiovascular risk factors, this safety profile matters significantly.
You have sleep problems. Phentermine causes insomnia. Tirzepatide does not. If you already struggle with sleep, the stimulant effects of phentermine could make things significantly worse.
You want to reduce food noise. The hormonal mechanism of tirzepatide reduces the mental preoccupation with food that many people with obesity experience. Phentermine suppresses appetite through stimulation, but the underlying food noise often persists. Understanding when tirzepatide appetite suppression kicks in helps set expectations.
Insurance coverage and cost are the primary barriers to tirzepatide. If you can access it through insurance, a savings program, or affordable compounding options, tirzepatide is the more effective choice for most patients seeking significant weight loss. SeekPeptides provides detailed guidance on navigating the various access pathways available.
Can you take phentermine and tirzepatide together?
This is one of the most frequently asked questions in weight loss forums, and the answer requires careful nuance. The short version: there is no FDA-approved combination of phentermine and tirzepatide, no published randomized controlled trials studying the pairing, and phentermine labeling specifically warns against combining it with other weight loss medications.
That said, some physicians do prescribe them together off-label. The rationale is appealing on paper. Phentermine addresses appetite through central nervous system stimulation. Tirzepatide addresses it through hormonal pathways. In theory, hitting two different mechanisms simultaneously could produce additive benefits.
In practice, the risks are real. Combining the two amplifies certain side effects. Phentermine raises heart rate and blood pressure. Adding tirzepatide, which can cause dehydration through reduced food and fluid intake, creates conditions where cardiovascular monitoring becomes even more important. Both medications can cause nausea and headache, and those effects may intensify when combined. Blood sugar management gets more complex, especially for patients with diabetes, because tirzepatide affects insulin sensitivity while phentermine does not. We have a detailed guide on whether you can take phentermine and tirzepatide together that covers the safety data in depth.
The practical reality is that most patients who respond well to tirzepatide do not need phentermine. Tirzepatide at therapeutic doses (10-15 mg) produces enough appetite suppression and weight loss that adding a stimulant provides minimal additional benefit while introducing unnecessary risks. The combination is most commonly considered when a patient is in the early titration phase of tirzepatide and wants appetite suppression while the GLP-1/GIP effects are still building.
Bottom line: do not combine these medications without explicit physician supervision, thorough screening for contraindications, and regular monitoring of blood pressure, heart rate, and metabolic markers.
Switching from phentermine to tirzepatide
Many people start with phentermine, achieve some results, and then consider transitioning to tirzepatide for continued or greater weight loss. This is a sensible progression, and it is increasingly common in clinical practice.
The transition is generally straightforward. Phentermine has a short half-life (about 19-24 hours), so it clears your system within a few days of the last dose. Most physicians recommend stopping phentermine before starting tirzepatide, rather than overlapping them. The typical protocol:
Stop phentermine. The last dose is usually taken the day before or two days before the first tirzepatide injection.
Start tirzepatide at 2.5 mg. Even if you were tolerating phentermine well, the standard tirzepatide titration schedule applies. Do not skip the initial low doses.
Expect a transition period. The first two to four weeks on tirzepatide 2.5 mg may feel like a step backward. Appetite may increase compared to what phentermine was providing. This is normal and temporary. The effects build as the dose increases.
Monitor weight trends, not daily numbers. A few pounds of regain during the transition is common and expected. Focus on the trajectory over weeks and months, not individual weigh-ins.
People who switch from phentermine to tirzepatide typically report that the quality of appetite suppression feels different. Phentermine suppression is sharp and stimulant-driven, almost like the hunger signal gets overridden by force. Tirzepatide suppression is more natural and gradual, like genuine fullness rather than artificial hunger blocking. Many find the tirzepatide experience more sustainable because it requires less willpower to maintain. The semaglutide to tirzepatide conversion chart provides additional switching context if you are coming from a different GLP-1 medication first, and understanding compounded tirzepatide starting doses is important when beginning the new regimen.
Beyond these two: the broader medication landscape
Phentermine and tirzepatide represent two ends of the weight loss medication spectrum, but they are not the only options. Understanding the broader landscape helps contextualize this comparison.
Semaglutide (Wegovy/Ozempic) sits between phentermine and tirzepatide in effectiveness. A single GLP-1 agonist, semaglutide produces approximately 15-17% body weight reduction, which is significantly better than phentermine but somewhat less than tirzepatide maximum doses. The side effect profiles between semaglutide and tirzepatide are similar, though tirzepatide dual mechanism often provides more robust appetite control.
Phentermine-topiramate ER (Qsymia) combines phentermine with an anticonvulsant that independently promotes weight loss. The combination produces better results than phentermine alone, typically 12-14% body weight loss, approaching but not matching GLP-1 medications. The generic version became available recently, making it more affordable.
Newer options are also emerging. Orforglipron is an oral GLP-1 receptor agonist in development that could eventually offer tirzepatide-level results in pill form. Survodutide targets GLP-1 and glucagon receptors. CagriSema combines cagrilintide (an amylin analog) with semaglutide. And retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown even greater weight loss than tirzepatide in early trials. Understanding where each option fits in the landscape helps you make informed decisions with your healthcare provider. SeekPeptides covers all these medications in detail through comprehensive comparison guides and dosing resources.
Practical considerations most guides ignore
Diet and nutrition on each medication
Phentermine users can generally eat a normal reduced-calorie diet without specific restrictions. The stimulant effect reduces appetite, but food tolerance is not significantly affected. Standard nutritional advice applies: reduce calories, increase protein, eat whole foods.
Tirzepatide requires more dietary attention. Because gastric emptying is slowed, large meals and high-fat foods can cause significant discomfort, bloating, and nausea. Many tirzepatide users find they need to eat smaller, more frequent meals and avoid foods that sit heavily in the stomach. Detailed guides on what to eat on tirzepatide, tirzepatide diet plans, and meal plan templates can make a significant difference in tolerability. The same principles apply to understanding foods to avoid on GLP-1 medications in general.
Protein intake becomes critical on tirzepatide because the dramatic appetite reduction can lead to inadequate protein consumption, which accelerates muscle loss during rapid weight loss. Protein shakes formulated for GLP-1 users can help bridge the gap. Key supplements to take with tirzepatide include protein, multivitamins, and potentially electrolytes.
Alcohol interactions
Phentermine combined with alcohol is generally discouraged because both affect the central nervous system. Alcohol can amplify phentermine side effects, particularly dizziness and impaired judgment.
Tirzepatide and alcohol is a different concern. Slowed gastric emptying means alcohol may be absorbed differently, potentially leading to stronger effects from smaller amounts. Many tirzepatide users report significantly reduced alcohol tolerance. If you choose to drink, understanding the interaction between tirzepatide and alcohol and knowing the best alcohol choices on tirzepatide can help minimize problems.
Exercise compatibility
Phentermine stimulant properties can actually enhance exercise performance in some people by increasing energy and alertness. However, the elevated heart rate means that high-intensity cardiovascular exercise requires caution, especially in the heat. Heart rate monitoring is advisable.
Tirzepatide does not directly affect exercise capacity, but the reduced calorie intake that comes with aggressive appetite suppression can lead to fatigue during workouts. Some people find that understanding tirzepatide energy effects and whether the metabolism-boosting claims hold up helps them plan training around medication timing. Resistance training is strongly recommended on tirzepatide to preserve lean mass during rapid weight loss.
Impact on hormones and reproductive health
Both medications can affect hormonal balance through weight loss. Fat tissue produces estrogen, so significant weight loss changes estrogen levels. Tirzepatide dramatic weight loss makes this effect more pronounced.
For women, both medications can affect menstrual cycles. Tirzepatide specifically has documented effects on menstrual regularity and cycle timing. The fertility implications of tirzepatide are also worth understanding, as improved metabolic health can increase fertility in women with PCOS or obesity-related anovulation. Tirzepatide should be discontinued before planned pregnancy, and understanding breastfeeding considerations is essential for women of childbearing age.
Hair loss risk
Rapid weight loss from any cause can trigger telogen effluvium, a form of temporary hair shedding. Because tirzepatide produces more rapid and significant weight loss than phentermine, the risk of noticeable hair thinning is higher. This is not caused by the medication itself but by the metabolic stress of rapid weight change. The complete guide to GLP-1 hair loss covers prevention and treatment strategies.
The verdict: which one is better for weight loss?
If you measure purely by weight loss effectiveness, tirzepatide wins. It is not close. The average 22.5% body weight reduction at the highest dose is roughly triple what phentermine produces. The responder rates are higher. The duration of effectiveness is longer. The metabolic benefits extend beyond weight loss into blood sugar control and cardiovascular risk reduction.
But effectiveness is not the only factor that matters.
Phentermine wins on cost. It wins on simplicity. It wins on speed of onset. It wins on accessibility. And for a subset of patients who need modest, short-term weight loss without injections, GI side effects, or monthly bills exceeding $300, it remains the right choice.
The decision framework is straightforward:
Need to lose less than 10% of body weight? Phentermine is a reasonable first-line option. Effective, cheap, and proven.
Need to lose 10-20%+ of body weight? Tirzepatide is the clear clinical leader. The investment is higher, but the results are proportionally much greater.
Have type 2 diabetes? Tirzepatide. Not even a question. The dual benefit of weight loss and glucose control makes it the obvious choice.
Have cardiovascular concerns? Tirzepatide. No stimulant effects, no elevated heart rate, no increased blood pressure.
Cannot afford $300+/month? Phentermine. Effective weight loss at a fraction of the cost.
Afraid of needles? Phentermine now, but watch for oral tirzepatide, tirzepatide tablets, and orally dissolving tirzepatide as those options expand availability.
Final comparison summary
Factor | Phentermine | Tirzepatide | Winner |
|---|---|---|---|
Weight loss (% body weight) | 5-10% | 16-22.5% | Tirzepatide |
Speed of onset | Days | Weeks to months | Phentermine |
Duration of use | Short-term (12 weeks) | Long-term (ongoing) | Tirzepatide |
Monthly cost | $15-50 | $300-1,080+ | Phentermine |
Side effect profile | Cardiovascular/CNS | Gastrointestinal | Tirzepatide (GI resolves) |
Administration | Daily oral pill | Weekly injection | Phentermine (convenience) |
Blood sugar benefits | None | Significant | Tirzepatide |
Cardiovascular safety | Raises HR and BP | Neutral to beneficial | Tirzepatide |
Weight maintenance | Poor after stopping | Good with continued use | Tirzepatide |
Insurance coverage | Almost always | Variable | Phentermine |
Abuse potential | Yes (Schedule IV) | None | Tirzepatide |
The weight loss medication landscape has changed fundamentally with the arrival of GLP-1 and dual GIP/GLP-1 agonists. Phentermine served its purpose for decades and continues to serve it for patients who need an affordable, fast-acting option for modest weight loss. But for anyone seeking transformative, sustained weight reduction, tirzepatide represents a genuine breakthrough that produces results no previous medication could achieve.
For researchers and individuals serious about optimizing their weight management protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, detailed dosing references, dosage calculators, and a community of thousands who have navigated these exact decisions.
Frequently asked questions
Is tirzepatide just a stronger version of phentermine?
No. They work through completely different mechanisms. Phentermine is a central nervous system stimulant that suppresses appetite by increasing norepinephrine. Tirzepatide is a dual GLP-1/GIP receptor agonist that mimics natural gut hormones to control hunger, fullness, and blood sugar. Different drug classes, different side effect profiles, different durations of use.
Can I switch from phentermine to tirzepatide mid-treatment?
Yes. Most physicians recommend stopping phentermine one to two days before starting tirzepatide. You will begin the standard tirzepatide titration at 2.5 mg regardless of your previous phentermine dose. Expect a brief transition period where appetite suppression may temporarily decrease before tirzepatide effects build. Review the compounded tirzepatide starting dose guide for protocol details.
How much weight will I lose on tirzepatide compared to phentermine?
Clinical trials show phentermine produces 5-10% body weight loss over 3-6 months. Tirzepatide produces 16-22.5% body weight loss over 72 weeks. For a 220-pound person, that is roughly 11-22 pounds with phentermine versus 35-50 pounds with tirzepatide. Individual results vary based on dose, diet, exercise, and adherence. Check the tirzepatide before and after results for real-world examples.
Is phentermine safer than tirzepatide?
Not necessarily. Phentermine carries cardiovascular risks including elevated heart rate and blood pressure, and it is classified as a Schedule IV controlled substance with abuse potential. Tirzepatide has primarily gastrointestinal side effects that typically improve over time and carries no cardiovascular stimulant risks. Long-term safety data for tirzepatide is still accumulating, but for most patients, the side effect comparison favors tirzepatide.
Can phentermine and tirzepatide be taken at the same time?
There are no FDA-approved combinations and no published clinical trials studying this pairing. Some physicians prescribe them together off-label, but the combination requires careful screening, monitoring, and medical supervision. The cardiovascular effects of phentermine combined with the metabolic effects of tirzepatide create potential risks that require close oversight.
What happens when you stop taking each medication?
Weight regain occurs with both medications after discontinuation, but the pattern differs. After stopping phentermine, hunger returns to baseline within days and weight regain is common within months. After stopping tirzepatide, patients typically regain about two-thirds of lost weight within a year. This is why many physicians view tirzepatide as a long-term or indefinite treatment rather than a short course. Learning how to wean off tirzepatide properly can help minimize rebound weight gain.
Do I need a special diet on tirzepatide that I would not need on phentermine?
Yes. Tirzepatide slows gastric emptying, which means large meals, high-fat foods, and heavy meals can cause significant nausea and discomfort. Most tirzepatide users need to eat smaller, more frequent meals and pay attention to protein intake. The tirzepatide foods to avoid guide and best foods for GLP-1 users can help with meal planning. Phentermine generally does not require specific dietary modifications beyond standard calorie reduction.
Which medication is better for someone with anxiety?
Tirzepatide. Phentermine is a stimulant that can worsen anxiety symptoms, cause jitteriness, and increase restlessness. Tirzepatide has no stimulant properties. While some patients report anxiety on tirzepatide, it is far less common and typically related to the adjustment period rather than a direct pharmacological effect.
External resources
Obesity Medicine Association: Weight Loss Medications Overview
NEJM: Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1)
Safety and Effectiveness of Longer-Term Phentermine Use (PubMed)
Weight Loss Pharmacotherapy: Current and Future Therapies (PMC)
In case I do not see you, good afternoon, good evening, and good night. May your weight loss stay consistent, your side effects stay manageable, and your medication choice stay informed.