Feb 24, 2026

Tired of scrolling through conflicting advice about how to bring up GLP-1 medications with your doctor? You are not the only one struggling with this. Millions of people know that GLP-1 receptor agonists could change their trajectory, yet they freeze up the moment they sit down in that exam room. The words vanish. Confidence evaporates. And what should be a straightforward medical conversation turns into an awkward exchange that ends with "let us try diet and exercise first."
That frustration is real. And it is completely preventable.
This guide breaks down exactly what to say when requesting GLP-1 options from your healthcare provider. Not vague suggestions. Not generic talking points. Actual phrases, preparation checklists, documentation strategies, and step-by-step scripts that help you walk into that appointment feeling informed and ready to have a productive conversation about your health. Whether you are exploring semaglutide, tirzepatide, or newer options like retatrutide, the approach is the same. Know your numbers. Know your history. Know how to frame the request. Doctors respond to prepared patients, and you are about to become one.
What GLP-1 medications are and why they matter
Before you walk into any medical appointment, you need to understand what you are actually asking for. GLP-1 receptor agonists are a class of medications that mimic a hormone your body already produces. That hormone, glucagon-like peptide-1, regulates appetite, slows gastric emptying, and improves insulin sensitivity. When functioning normally, it sends signals to your brain that say "you are full" after eating. For many people with obesity or type 2 diabetes, those signals are weak or disrupted. GLP-1 medications restore what the body is not doing on its own.
This is not a willpower issue. It is a biological one.
The FDA has approved several GLP-1 medications for different conditions. Semaglutide is the active ingredient in both Ozempic (approved for type 2 diabetes) and Wegovy (approved for chronic weight management). Tirzepatide, a dual GIP/GLP-1 receptor agonist, powers both Mounjaro (diabetes) and Zepbound (weight management). Liraglutide appears in Victoza (diabetes) and Saxenda (weight loss). Each works through similar mechanisms but with meaningful differences in potency, side effect profiles, and weight loss outcomes. Understanding these differences gives you the vocabulary to have an intelligent conversation with your prescriber.
The numbers tell the story. In clinical trials, patients on semaglutide 2.4mg lost an average of 14.9% of their body weight over 68 weeks. Tirzepatide at the highest dose produced even more dramatic results, with average weight loss reaching 20.2% in the SURMOUNT-5 trial. Compare that to the 2-3% typically achieved through lifestyle modifications alone. These are not marginal improvements. They represent a fundamental shift in how medicine approaches weight management, and understanding this data helps you communicate to your doctor that you have done your homework.
The mechanism matters for your conversation too. When your doctor asks why you want a GLP-1, you should be able to explain that these medications address the neurohormonal pathways that regulate appetite and energy balance. That language shows you understand this is medical treatment, not a shortcut. Doctors respond differently to patients who frame the discussion in clinical terms versus those who simply say they want to lose weight. One framing invites a medical conversation. The other invites a lecture about eating less and moving more.
For a deeper understanding of how GLP-1 medications work and their timeline, research the specific mechanisms before your appointment. SeekPeptides offers comprehensive guides on every major GLP-1 medication, helping you understand exactly what you are asking for when you sit across from your provider.
Checking if you qualify for a GLP-1 prescription
Do not walk into your appointment hoping you qualify. Walk in knowing you do.
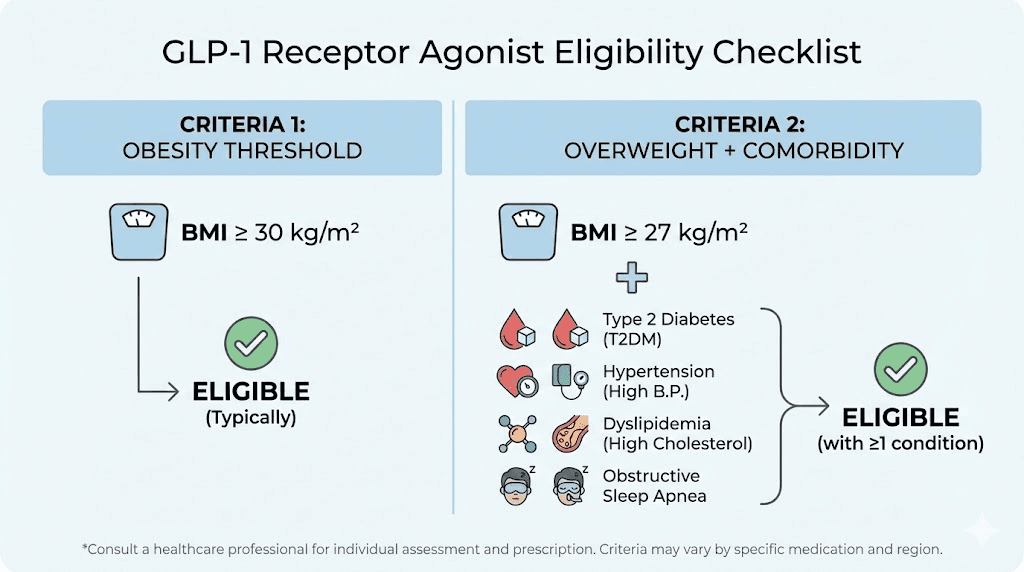
The FDA has established clear eligibility criteria for GLP-1 weight loss medications. You need a body mass index of 30 or higher, which classifies as obesity. Alternatively, a BMI of 27 or higher with at least one weight-related health condition also qualifies you. Those qualifying conditions include type 2 diabetes, hypertension, high cholesterol, obstructive sleep apnea, cardiovascular disease, polycystic ovary syndrome, and non-alcoholic fatty liver disease. If you have a BMI of 28 and take blood pressure medication, you qualify. If your BMI is 31 with no other conditions, you qualify.
Know your exact BMI before the appointment. Calculate it. Write it down.
Here is where preparation separates successful requests from failed ones. Many patients walk in and say "I want to lose weight." The doctor hears a cosmetic concern. But if you walk in and say "My BMI is 32, I have been diagnosed with prediabetes, and I would like to discuss GLP-1 receptor agonists as part of a comprehensive treatment plan," the doctor hears a medically informed patient requesting evidence-based treatment. Same goal. Entirely different conversation.
The qualifying comorbidities deserve attention because many people have them without realizing it. High blood pressure affects nearly half of American adults. Prediabetes affects roughly 38% of the population, and most do not know they have it. Sleep apnea, joint pain from excess weight, high triglycerides, elevated fasting glucose, insulin resistance, and PCOS all count. If you have not had bloodwork done recently, schedule it before your GLP-1 appointment. Those lab results become powerful documentation for your request and for any insurance prior authorization that might follow.
Insurance eligibility adds another layer. Most commercial insurance plans require prior authorization for GLP-1 weight loss medications. Common requirements include documented BMI meeting the threshold, proof of previous weight loss attempts (usually 3-6 months of supervised diet and exercise), at least one qualifying comorbidity, and sometimes evidence that other treatments have been tried and failed. Knowing these requirements ahead of time means you can bring the documentation your doctor needs to start the authorization process during your visit, rather than requiring multiple follow-up appointments.
For patients interested in GLP-1 medications specifically for type 2 diabetes rather than weight management, the path is often simpler. Many insurers cover GLP-1s for diabetes without the extensive prior authorization required for weight loss indications. If you have a diabetes diagnosis, your doctor may be able to prescribe semaglutide or tirzepatide as a diabetes medication that also supports weight management. This distinction matters. Ask your doctor which indication gives you the clearest path to coverage.
You can use the semaglutide dosage calculator and other tools on SeekPeptides to familiarize yourself with dosing schedules before your appointment. Walking in with knowledge about standard dosing protocols shows your provider that you have invested time in understanding the treatment.
How to prepare before your appointment
Preparation wins prescriptions. It is that simple.
Start with your weight history. Write down your highest adult weight, your current weight, and every significant weight loss attempt you have made. Include commercial programs like Weight Watchers, Noom, or Jenny Craig. Include gym memberships, personal trainers, meal delivery services, calorie counting apps, and any previous medications like phentermine or orlistat. Include the dates, the duration, and the results. If you lost 30 pounds on a program but regained it within a year, document that. If you maintained a caloric deficit for six months and still did not reach your goal, document that too. This history proves you are not looking for an easy way out. It proves that conventional approaches have been insufficient.
Next, compile your medical documentation. Bring your most recent lab results, including fasting glucose, HbA1c, lipid panel, thyroid function, and liver enzymes. Bring a list of every current medication with dosages. Bring documentation of any weight-related diagnoses. If your primary care physician diagnosed you with prediabetes two years ago, bring that record. If your sleep study showed moderate obstructive sleep apnea, bring those results. Every piece of documentation strengthens your case and makes your doctor job easier when submitting prior authorization paperwork.
Then prepare your talking points. Write them down on an index card or in your phone notes. You do not need to memorize a speech, but you do need to remember three things: your specific health goals (not "lose weight" but "reduce my A1c from 6.1 to below 5.7 and lose enough weight to reduce my blood pressure medication"), the treatments you have already tried, and your awareness of GLP-1 side effects and commitment to managing them.
Consider requesting a longer appointment. Standard office visits run 15 minutes, and that is barely enough time to discuss a new medication class, review eligibility, answer questions, and initiate prior authorization. Many practices offer extended appointments or dedicated medication management visits. Call ahead and ask. A 30-minute slot gives you and your doctor the breathing room to have a real conversation rather than a rushed exchange.
One more thing. Bring a notebook. Write your main question at the top: "I would like to discuss GLP-1 receptor agonists as a treatment option for my weight and metabolic health." Take notes during the appointment. Doctors notice patients who come prepared, who take the conversation seriously, who treat this like the medical decision it is. That preparation earns respect, and respect earns thoughtful consideration of your request.
Research the specific GLP-1 medications you are most interested in. Knowing the difference between semaglutide and tirzepatide shows genuine engagement with your treatment options. Understand the dosing schedules and titration protocols so you can discuss them intelligently. Review common side effects like constipation, fatigue, and dizziness so your doctor knows you understand the commitment involved. Look into dietary modifications and meal planning that support GLP-1 therapy, because mentioning these shows you are planning for comprehensive lifestyle change, not just a pill solution.
Exactly what to say when you sit down with your doctor
You are sitting in the exam room. The door opens. Here is how to start.
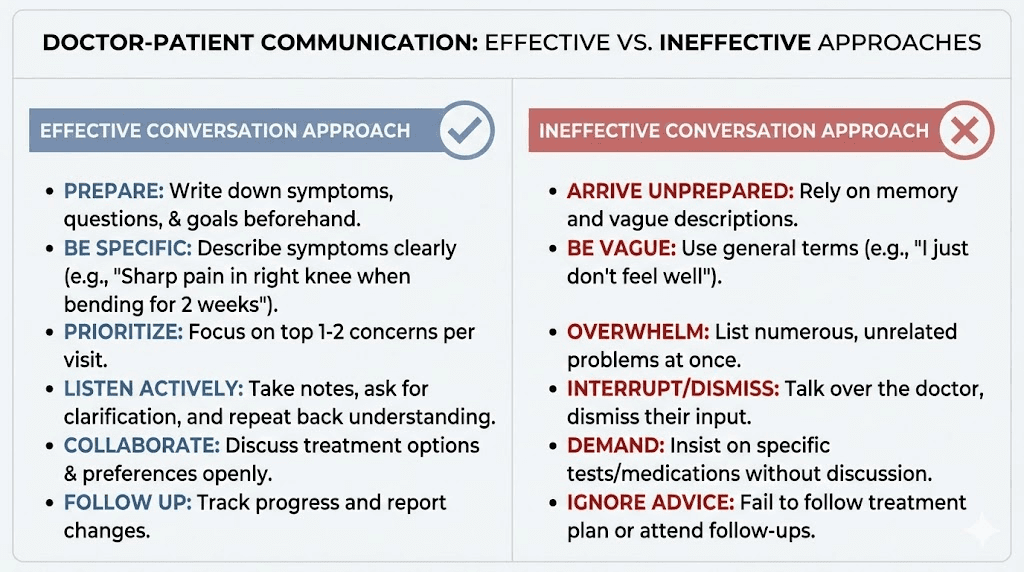
Do not lead with "I want Ozempic" or "Can I get one of those weight loss shots?" Those opening lines immediately put some doctors on the defensive. They hear a brand request driven by social media rather than a medical conversation driven by health goals. Instead, lead with your health concern and let the medication become part of the solution.
Opening script: "Doctor, I would like to discuss my weight and metabolic health. My BMI is [number], I have [condition], and I have been working on this for [time period] using [methods]. I have been reading about GLP-1 receptor agonists and I think they might be a good addition to my current approach. Can we talk about whether I am a candidate?"
That single paragraph accomplishes five things. It frames the conversation around health rather than appearance. It demonstrates you know your numbers. It establishes your history of effort. It shows you have researched the medication class. And it asks for a collaborative discussion rather than demanding a specific drug.
If your doctor asks why you are interested in GLP-1 medications specifically, be ready with this: "I understand that GLP-1 receptor agonists work on the neurohormonal pathways that regulate appetite and glucose metabolism. Given my history of [specific condition] and the difficulty I have had achieving sustained weight loss through lifestyle modification alone, this seems like an evidence-based treatment that could address the underlying biology."
Notice the language. "Evidence-based treatment." "Underlying biology." "Neurohormonal pathways." You are speaking your doctor language, and that matters more than most people realize.
If your doctor seems hesitant: "I understand there may be concerns about prescribing this medication. Could you help me understand what specific factors are giving you pause? I want to make sure I am addressing any legitimate medical concerns you have."
This is crucial. Do not get defensive if the initial response is lukewarm. Some doctors are cautious about GLP-1 medications for valid clinical reasons, and some are simply unfamiliar with the newer options. Asking them to articulate their concerns opens a dialogue rather than creating a confrontation.
If your doctor brings up lifestyle changes first: "Absolutely, I agree that lifestyle modification is foundational. I have been [describe specific efforts] for [time period], and I plan to continue. I see GLP-1 therapy as complementary to those efforts, not a replacement. The research shows that combined pharmacological and behavioral approaches produce the best outcomes."
This response does something powerful. It validates your doctor concern while redirecting the conversation back to evidence. Most physicians know that behavioral intervention alone has limited long-term efficacy for patients with BMI over 30. By agreeing with the importance of lifestyle changes AND citing the superiority of combined approaches, you disarm the objection without confrontation.
If your doctor asks about your diet and exercise routine: Be specific. "I currently eat approximately 1,800 calories per day, focusing on lean protein and vegetables. I exercise four times per week, combining 30 minutes of cardio with resistance training. I have been doing this consistently for [time period]. Despite this, my weight has plateaued at [number] and my A1c remains elevated at [number]."
Specificity kills skepticism. When you quote exact calorie counts, exercise frequency, and duration, it becomes very difficult for anyone to suggest you simply need to try harder. The more specific your data, the stronger your case.
When discussing which medication to try: "I have been researching the different options, including semaglutide and tirzepatide. I understand tirzepatide is a dual-action GIP/GLP-1 agonist and may produce stronger weight loss results, while semaglutide has a longer track record. Which do you think would be most appropriate given my specific health profile and insurance coverage?"
Framing it as a question about appropriateness rather than a demand for a specific drug shows respect for your doctor clinical judgment while demonstrating your own knowledge. It invites collaboration. And mentioning insurance coverage shows practical awareness that helps your doctor think about what they can actually get approved for you.
Understanding the GLP-1 options you can discuss
Knowledge is leverage. The more you understand about available GLP-1 medications, the more productive your conversation becomes.
Semaglutide is the most widely recognized GLP-1 receptor agonist. As a weekly injectable, it comes in two brand names: Ozempic for type 2 diabetes management and Wegovy for chronic weight management. The dosing schedule starts at 0.25mg weekly for the first month, then titrates up gradually to the maintenance dose. For weight loss, the target dose is 2.4mg weekly. For diabetes, it typically maxes at 2mg. Clinical trials showed average weight loss of 14.9% with the 2.4mg dose. Oral formulations also exist, giving patients who dislike injections an alternative route.
The side effect profile for semaglutide is well-documented. Appetite suppression begins within the first few weeks for most patients. Common side effects include nausea (affecting roughly 40% of patients, usually most pronounced during dose increases), constipation, sulfuric burping, and fatigue. Most of these resolve within 4-8 weeks as the body adjusts. Knowing this timeline helps you discuss realistic expectations with your doctor.
Tirzepatide represents the newer generation. As a dual GIP/GLP-1 receptor agonist, it targets two hormonal pathways instead of one. The brand names are Mounjaro for diabetes and Zepbound for weight management. Dosing starts at 2.5mg weekly and can increase to 15mg. Head-to-head clinical trials showed tirzepatide producing superior weight loss compared to semaglutide, with the highest dose achieving an average 20.2% body weight reduction. That is roughly 45-50 pounds for someone weighing 220 pounds.
Side effects for tirzepatide mirror semaglutide in many ways. Headaches, fatigue, constipation, and diarrhea are all reported. Muscle pain and injection site reactions occasionally appear as well. But the same general pattern holds: most side effects peak during dose titration and diminish with continued use.
Liraglutide deserves mention as the older option. Available as Saxenda for weight loss and Victoza for diabetes, it requires daily injections rather than weekly ones. Average weight loss is more modest, typically 5-10% of body weight. Many patients and doctors consider it a starting point when newer agents are unavailable or too expensive.
Emerging options are worth knowing about too. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, showed up to 24% weight loss in phase 2 trials. CagriSema combines semaglutide with cagrilintide (an amylin analog) and is advancing through trials. Orforglipron is a non-peptide oral GLP-1 that could change accessibility entirely. Survodutide and mazdutide round out the pipeline. Mentioning that you are aware of these developments signals to your doctor that you are genuinely engaged with the science, not just chasing a trend.
The comparison between the two primary options matters for your conversation. Review the detailed semaglutide versus tirzepatide comparison to understand the practical differences. If your insurance covers one but not the other, that information helps you and your doctor make a pragmatic choice. Some patients start with semaglutide because coverage is easier to obtain, then switch to tirzepatide if results plateau or if coverage changes. Understanding this flexibility makes you a more empowered participant in treatment planning.
Compounded versions represent another option to discuss with your provider. During periods of drug shortage, compounding pharmacies have been allowed to produce semaglutide and tirzepatide formulations. These are typically more affordable than brand-name options. Some compounded formulations include additional ingredients like B12, glycine, or methylcobalamin. Your doctor can help you evaluate whether compounded options are appropriate for your situation and how they compare to brand-name medications.
Essential questions to ask about each GLP-1 medication
Do not leave the appointment without answers to these questions. Print this list. Bring it with you.
About your specific eligibility:
"Based on my BMI, health history, and current medications, which GLP-1 would you recommend for me?"
"Are there any contraindications in my medical history that would prevent me from using a GLP-1?"
"Do I need any additional lab work or screening before starting?"
These questions accomplish two things. They show deference to your doctor expertise while also establishing that you expect a thorough evaluation. A good prescriber will check for personal or family history of medullary thyroid carcinoma, multiple endocrine neoplasia type 2, pancreatitis, or severe gastrointestinal conditions. If your doctor does not ask about these, bring them up yourself. Your safety matters more than getting a prescription quickly.
About the practical aspects:
"What is the titration schedule, and how quickly will we increase the dose?"
"How should I handle injection technique and site selection?"
"What is the best time of day to take this medication?"
"How should I store the medication?"
"What happens if I miss a dose or need to adjust timing?"
Practical questions demonstrate that you are already thinking about adherence and implementation, not just acquisition. Doctors want patients who will use medications correctly, and these questions signal that commitment.
About side effects and management:
"What are the most common side effects during the first few weeks?"
"How should I adjust my diet to minimize gastrointestinal side effects?"
"When should I call your office about side effects versus managing them at home?"
"Are there any supplements I should take alongside this medication?"
"Could this medication interact with anything I currently take?"
Side effect questions show maturity and realism. You are not expecting a magic pill. You are preparing for a medical treatment with a known side effect profile, and you want to manage it intelligently. Many doctors report that patients who ask about side effect management upfront tend to have better adherence and outcomes.
About insurance and cost:
"Which GLP-1 is most likely to be covered under my insurance plan?"
"Will your office handle the prior authorization, and how long does that typically take?"
"If the first option is denied, what is the appeal process?"
"Are there manufacturer savings programs or coupons available?"
"Would a compounded version be an option if brand-name is too expensive?"
Cost conversations are not awkward. They are practical. Doctors deal with insurance barriers constantly, and most appreciate patients who ask directly rather than silently abandoning treatment when they see the price. Some practices have staff dedicated to navigating prior authorizations, and knowing this resource exists can save you weeks of frustration.
About long-term planning:
"What happens if I stop taking it?"
"How will we monitor my progress and adjust treatment?"
"At what point would we consider switching to a different medication?"
Long-term questions impress doctors because they show you understand this is not a quick fix. Weight management with GLP-1 medications is typically ongoing. Research consistently shows that discontinuing the medication leads to weight regain in most patients. Discussing this upfront sets realistic expectations and demonstrates your commitment to sustained treatment.
Navigating insurance coverage and prior authorization
Insurance is where many GLP-1 journeys stall. But they do not have to.
Understanding the prior authorization process before your appointment saves weeks of frustration. Most commercial insurance plans require prior authorization for GLP-1 weight loss medications like Wegovy and Zepbound. Some plans cover them readily for type 2 diabetes indications (Ozempic, Mounjaro) but require extensive documentation for weight management. Medicare Part D coverage for obesity medications has expanded, though specific formulary placement varies by plan. Medicaid coverage differs dramatically by state.
The documentation your insurer typically wants includes a recorded BMI meeting the threshold (30 or above, or 27 with comorbidities), proof of at least one qualifying comorbidity, evidence of previous weight loss attempts (usually 3-6 months of documented lifestyle intervention), current lab work showing relevant metabolic markers, and a letter of medical necessity from your prescribing physician. Some plans add requirements like nutritional counseling, behavioral therapy documentation, or evidence that other weight loss medications were tried first.
Here is the key insight most patients miss: much of this documentation already exists in your medical record. Those blood pressure readings from your last three physicals? Documentation. That conversation about prediabetes? Documentation. The nutritionist referral you followed up on? Documentation. Your doctor office can compile this, but you can make the process faster by knowing what is needed and pointing them to the relevant records.
When your doctor submits the prior authorization, the turnaround time varies from 24 hours to several weeks. Ask the office staff who handles prior authorizations and get their direct contact information. Follow up every 3-5 days. Insurance companies sometimes deny first requests as a default strategy, knowing that many patients give up. Do not be that patient.
If the prior authorization is denied, you have the right to appeal. The appeal process typically involves three levels. First, an internal appeal where your doctor provides additional documentation and clinical reasoning. Second, an external review by an independent medical reviewer. Third, a state insurance commissioner complaint if both appeals are denied. Most successful appeals include a detailed letter from your doctor explaining why the medication is medically necessary for your specific situation, citing relevant clinical guidelines and your documented treatment history.
Step therapy requirements represent another common obstacle. Some insurers require you to try (and fail) less expensive treatments before approving a GLP-1. This might mean documenting a trial of metformin, phentermine, or orlistat first. If your doctor believes these are inappropriate or insufficient for your condition, they can submit a step therapy exception request. Having your documented weight history and previous treatment failures ready makes this process smoother.
Manufacturer savings programs can dramatically reduce out-of-pocket costs. Eli Lilly and Novo Nordisk both offer savings cards for eligible patients. These programs typically work for commercially insured patients but not for those on government insurance. Ask your doctor or pharmacist about current program availability, as terms change frequently.
For patients without adequate insurance coverage, telehealth platforms and online providers sometimes offer GLP-1 medications at lower cash-pay prices, particularly compounded versions. These can be legitimate alternatives when traditional insurance routes fail, but verify that any provider you use requires proper medical evaluation before prescribing.
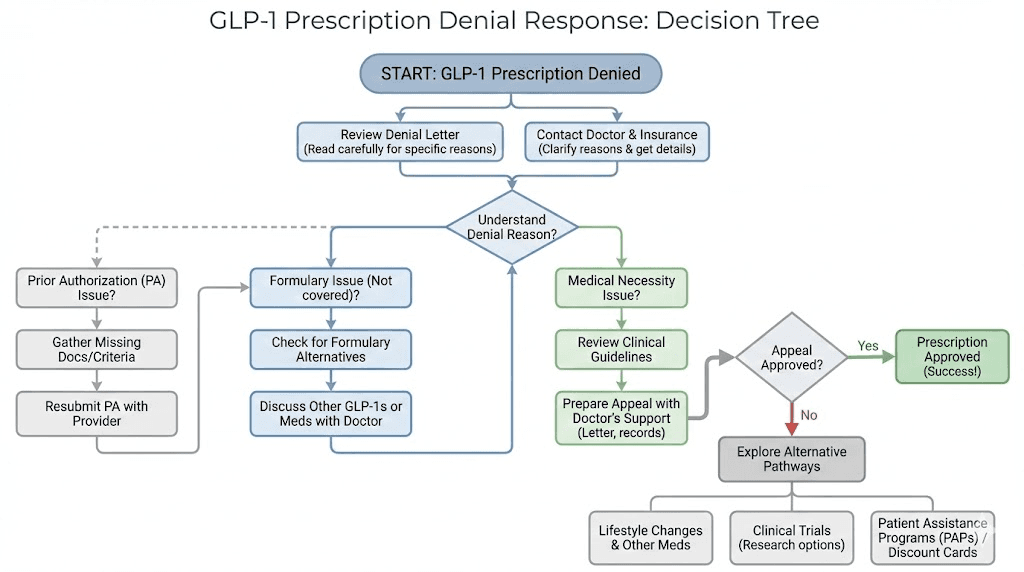
What to do when your doctor says no
A no is not a dead end. It is a detour.
First, understand why. Ask your doctor to explain the specific clinical reasoning behind the refusal. There are legitimate medical reasons a doctor might decline to prescribe a GLP-1. If you have a personal or family history of medullary thyroid carcinoma, a history of pancreatitis, or severe gastroparesis, GLP-1 medications may genuinely not be safe for you. In that case, ask about alternative treatments and respect the clinical judgment.
But many refusals are not clinical. Some are philosophical.
Some doctors remain skeptical of pharmacological weight management. They believe diet and exercise should always be the first, second, and third line of treatment. This perspective, while understandable from a historical context, conflicts with current American Medical Association guidelines that recognize obesity as a chronic disease requiring multimodal treatment including pharmacotherapy when appropriate. If your doctor refusal seems based on this philosophy rather than your specific medical situation, you have options.
Option one: educate gently. "I understand the importance of lifestyle modification, and I am committed to continuing those efforts. However, the American Medical Association, the Endocrine Society, and the Obesity Medicine Association all recommend considering pharmacotherapy for patients with my BMI and comorbidity profile. Could we discuss this within those guidelines?"
Option two: request a referral. If your primary care physician is not comfortable prescribing GLP-1 medications, ask for a referral to an endocrinologist or a board-certified obesity medicine specialist. These specialists prescribe GLP-1 medications regularly and are more familiar with the nuances of dosing protocols, insurance navigation, and side effect management. The American Board of Obesity Medicine maintains a directory of certified practitioners.
Option three: seek a second opinion. You are not obligated to accept one doctor assessment as final. A second opinion from another primary care physician or specialist may yield a different outcome, particularly if the refusing doctor reasoning was not clinically specific to your situation. This is not doctor shopping. This is patient advocacy.
Option four: explore telehealth providers. Multiple legitimate telehealth platforms now specialize in GLP-1 prescribing. They require medical evaluations, lab work, and ongoing monitoring. While not appropriate for every patient, they fill an important gap for people whose local providers are unfamiliar with or resistant to obesity pharmacotherapy. Verify that any platform you consider employs licensed physicians, requires comprehensive health assessments, and provides ongoing medical supervision.
Option five: document everything. If you believe your insurance or doctor is wrongfully denying access to medically appropriate treatment, keep records. Save denial letters. Document conversations. Note dates and names. This documentation matters if you pursue formal appeals through your insurance company or file complaints with your state insurance commissioner.
Whatever path you take, do not default to unregulated sources. The safety risks of obtaining GLP-1 medications from unverified vendors far outweigh any cost savings. Stick to licensed pharmacies and legitimate medical providers.
The GLP-1 options comparison: what to discuss with your provider
Not all GLP-1 medications are created equal, and understanding the differences helps you have a more informed discussion about which option fits your specific situation.
Medication | Active ingredient | Administration | Average weight loss | Primary indication |
|---|---|---|---|---|
Wegovy | Semaglutide 2.4mg | Weekly injection | ~14.9% | Weight management |
Ozempic | Semaglutide (up to 2mg) | Weekly injection | ~10-14% | Type 2 diabetes |
Zepbound | Tirzepatide (up to 15mg) | Weekly injection | ~20.2% | Weight management |
Mounjaro | Tirzepatide (up to 15mg) | Weekly injection | ~15-20% | Type 2 diabetes |
Saxenda | Liraglutide 3mg | Daily injection | ~5-10% | Weight management |
Rybelsus | Semaglutide (oral) | Daily tablet | ~7-10% | Type 2 diabetes |
That table gives you a quick reference, but the real conversation goes deeper.
If your primary concern is maximum weight loss, the data clearly favors tirzepatide. The SURMOUNT-5 head-to-head trial directly compared tirzepatide to semaglutide and found 47% greater weight loss with tirzepatide at 72 weeks. But maximum weight loss is not always the deciding factor. Insurance coverage, availability, your comfort with the titration schedule, and your tolerance for side effects all play roles.
If your insurance is more likely to cover one medication over another, that becomes the practical choice. Ask your doctor which medication has the best formulary placement on your specific plan. Sometimes the answer is neither brand-name option, and a compounded formulation becomes the most accessible path. Compounded semaglutide or compounded tirzepatide with additional ingredients like glycine and B12 may be available through your provider.
For patients with type 2 diabetes, the conversation shifts. Mounjaro and Ozempic are primarily diabetes medications that also produce significant weight loss. Starting with a diabetes indication may bypass some of the stricter prior authorization requirements that weight management indications trigger. Discuss this strategic approach with your doctor, as it can save weeks or months of insurance battles.
If you are uncomfortable with injections, ask about oral formulations. Rybelsus provides oral semaglutide for diabetes management. Oral tirzepatide and tirzepatide drops represent emerging alternatives. Comparing tablets versus injections is a legitimate conversation to have with your provider, as some patients respond differently to different delivery methods.
Newer medications coming through the pipeline may also be relevant to mention. Retatrutide, the triple receptor agonist, showed remarkable efficacy in early trials with clearly defined dosing protocols already emerging from research. Asking your doctor "Are there any newer GLP-1 options that might be available soon?" shows forward-thinking engagement and opens the door to discussion about clinical trial participation if applicable.
Understanding how GLP-1 medications compare to older weight loss drugs like phentermine also helps frame the conversation. Phentermine works through different mechanisms, has limitations on duration of use, and produces less dramatic results. If your doctor suggests phentermine first, you can ask about the comparative evidence and whether a GLP-1 might be more appropriate for sustained, long-term weight management given your specific health profile.
Preparing for side effects and the first conversation after starting
Getting the prescription is step one. Managing the first few weeks is step two.
The most common side effect across all GLP-1 medications is gastrointestinal discomfort, particularly nausea. Roughly 40% of patients experience nausea, most commonly during dose titration. It peaks when you increase your dose and typically resolves within 2-4 weeks at each level. Knowing this timeline prevents panic. Knowing the management strategies prevents unnecessary medication discontinuation.
Start with dietary modifications before your first dose. Begin eating smaller, more frequent meals. Reduce fatty, greasy, and heavily spiced foods. Increase water intake between meals rather than during them. These changes create a foundation that minimizes gastrointestinal distress once the medication kicks in. Review our guides on foods to eat while on semaglutide and what to eat on tirzepatide for specific meal planning guidance. A comprehensive tirzepatide diet plan or semaglutide diet plan can make the transition dramatically smoother.
Beyond nausea, be prepared for these possibilities. Fatigue affects some patients, particularly in the early weeks. This is partly a caloric adjustment and partly a medication effect. It usually improves as your body adapts. Headaches can occur, especially if you are reducing caloric intake rapidly. Staying hydrated helps significantly. Hair thinning has been reported by some patients, likely related to rapid weight loss and caloric restriction rather than the medication itself. Adequate protein intake mitigates this concern.
Constipation is the other major gastrointestinal complaint. GLP-1 medications slow gastric motility, which can affect bowel function. Increasing fiber intake, staying hydrated, and discussing stool softeners with your doctor if needed are standard management approaches. Review the specific guides on semaglutide constipation management or tirzepatide constipation solutions for detailed strategies.
Some less common side effects worth discussing include anxiety, insomnia, sleep disruption, and dizziness. Menstrual changes and cycle disruptions have been reported by some female patients. And there is the important reproductive consideration that improved fertility can occur with weight loss, so contraception should be discussed.
Your follow-up appointment, typically 4-6 weeks after starting, is just as important as the initial visit. Come prepared with a log of your experience: any side effects, their severity, when they occurred relative to your dose, your appetite changes, and your weight trajectory. This data helps your doctor make informed decisions about dose adjustments. If nausea is manageable, you will likely advance to the next dose. If side effects are severe, your doctor may slow the titration or adjust your approach.
The first month results vary considerably. Some patients see dramatic changes in appetite within days. Others need several weeks before the full effect takes hold. Understanding that GLP-1 medications take time to reach therapeutic levels prevents discouragement during the early titration phase. If you reach four weeks with no appetite change on the starting dose, that is expected. The starting dose is designed for tolerance building, not maximum effect.
If your medication stops working as effectively after initial success, or if tirzepatide is not producing results anymore, that is a conversation to have with your doctor about dose adjustment, medication switching, or combination approaches. Weight loss often follows a stair-step pattern rather than a linear decline, and plateaus are normal.
Lifestyle modifications that support GLP-1 therapy
The medication works better when you work with it. Much better.
Your doctor will want to know that you are pairing pharmacotherapy with sustainable lifestyle changes. This is not about justifying your prescription. It is about maximizing your results. The clinical data consistently shows that patients who combine GLP-1 therapy with structured dietary modifications and regular physical activity achieve significantly better outcomes than those relying on medication alone.
Protein intake becomes especially important. GLP-1 medications reduce appetite substantially, which means you eat less overall. Without intentional protein prioritization, you risk losing muscle mass along with fat. Aim for 0.7-1 gram of protein per pound of ideal body weight daily. Consider protein shakes designed for GLP-1 patients to help meet targets when solid food feels challenging.
Resistance training protects muscle mass during rapid weight loss. Even two to three sessions per week targeting major muscle groups makes a meaningful difference. Discuss exercise timing relative to your medication dose. Some patients find that exercising on the day before their injection works better than exercising on injection day, when nausea may be more pronounced.
Hydration requires deliberate attention. The combination of reduced food intake (and therefore reduced water from food) plus potential gastrointestinal effects means dehydration is a real risk. Aim for at least 64 ounces of water daily, more if you exercise regularly. Drinking between meals rather than during meals can help manage the feeling of fullness that GLP-1 medications produce.
Sleep quality affects weight loss outcomes more than most people realize. Research shows that poor sleep disrupts the hormones that regulate appetite, the very same hormones GLP-1 medications are designed to support. Prioritize 7-9 hours of quality sleep. If your medication causes insomnia, discuss timing adjustments with your doctor. The optimal injection timing can vary between patients, and some find that morning injections versus evening injections make a significant difference in sleep quality.
If your doctor asks what dietary changes you plan to make, have specific answers ready. "I am going to follow a Mediterranean-style eating pattern emphasizing lean proteins, vegetables, healthy fats, and complex carbohydrates. I am going to limit processed foods, added sugars, and alcohol. I have already started reducing portion sizes and eating more slowly to prepare for the appetite changes." That level of specificity demonstrates genuine commitment and makes your doctor more confident in the treatment plan.
Alcohol consumption deserves special attention. GLP-1 medications affect how your body processes food and beverages, and many patients find their alcohol tolerance decreases significantly. Discuss this honestly with your doctor, especially if alcohol is a regular part of your routine. The same applies to tirzepatide and alcohol.
Building a long-term partnership with your prescriber
Your first appointment is not the finish line. It is the starting block.
GLP-1 therapy is typically a long-term commitment. Research shows that most patients who discontinue the medication regain a significant portion of lost weight within 12-18 months. Understanding how long you might stay on treatment helps set appropriate expectations from the beginning.
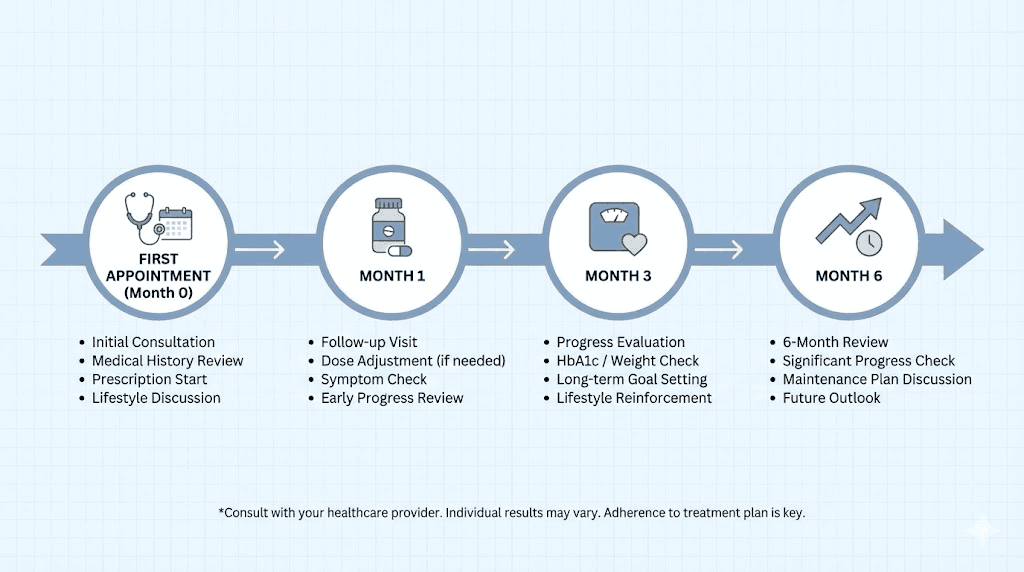
Schedule regular follow-ups. Monthly for the first three months during titration, then quarterly once you reach a stable maintenance dose. Each visit should cover your weight trajectory, side effect management, metabolic markers (periodic lab work), medication adherence, and any new symptoms or concerns. Treat these appointments with the same seriousness as the initial consultation.
Track your progress systematically. Weight is one metric, but it is not the only one. Track measurements, clothing fit, energy levels, sleep quality, blood pressure (if relevant), and blood sugar (if relevant). These data points create a comprehensive picture of treatment effectiveness that goes beyond the scale. They also give your doctor the information needed to make nuanced treatment decisions.
Be honest about challenges. If you are experiencing side effects you are not managing well, say so. If you are struggling with dietary compliance, say so. If you are considering stopping the medication, say so. Your doctor cannot help you navigate obstacles they do not know about. The patients who achieve the best long-term outcomes are consistently the ones who communicate openly with their providers.
If your current medication plateaus or becomes less effective, discuss options proactively. Microdosing strategies can sometimes overcome resistance. Switching between medications is another viable strategy. Combination approaches using GLP-1s with other agents are increasingly common. And dose optimization, sometimes going up, sometimes going down, can reignite progress. The key is communicating with your provider before making any changes on your own.
For those navigating their GLP-1 journey, SeekPeptides offers comprehensive resources including detailed protocol guides, GLP-1 progress tracking tools, and evidence-based information on optimizing treatment outcomes. Having a trusted resource for ongoing education makes you a better partner in your own care.
Special considerations and situations to discuss
Some conversations require extra preparation. These are the situations that catch patients off guard.
If you are a woman of reproductive age: GLP-1 medications are not approved for use during pregnancy. Discuss contraception before starting. Weight loss can improve fertility in women with PCOS or obesity-related anovulation, meaning pregnancy considerations are not theoretical. Most guidelines recommend stopping GLP-1 medications at least two months before planned conception. Be upfront about your reproductive plans.
If you take other medications: Drug interactions with GLP-1 medications are generally minimal, but the delayed gastric emptying can affect absorption of oral medications. This is particularly relevant for oral contraceptives, thyroid medications, and antibiotics. Your doctor should review all current medications and adjust timing if needed. Combining GLP-1s with other weight loss medications like phentermine requires specific medical oversight.
If you have a history of eating disorders: This is a critical conversation. GLP-1 medications alter appetite and relationship with food in profound ways. For someone with a history of restrictive eating, the dramatic appetite suppression could potentially trigger unhealthy patterns. A doctor who understands eating disorder history should be part of the prescribing team. Be honest about this history even if it feels uncomfortable.
If you plan to travel: Discuss medication storage and travel logistics before your trip. GLP-1 injectable medications require refrigeration and cannot go through extreme temperature changes. TSA allows injectable medications in carry-on luggage with proper documentation. Planning ahead prevents missed doses during travel.
If you have had bariatric surgery: GLP-1 medications are increasingly being prescribed to patients who have regained weight after bariatric surgery. If this applies to you, mention your surgical history and discuss whether the medication interaction with your altered anatomy requires any special consideration in terms of absorption or side effect management.
If your primary goal is not weight loss: GLP-1 medications show promise beyond weight management. Research suggests benefits for cardiovascular risk reduction, non-alcoholic fatty liver disease, and even cognitive protection. If your interest in GLP-1 therapy relates to these emerging indications, frame the conversation accordingly. "I am interested in the cardiovascular protective effects of GLP-1 receptor agonists given my family history of heart disease" is a perfectly valid opening statement.
Red flags and when to proceed with caution
Not every provider who prescribes GLP-1 medications does so responsibly. Knowing what to watch for protects you.
Be cautious of any provider who prescribes without proper medical evaluation. A legitimate GLP-1 prescription should involve a comprehensive health assessment, review of medical history, current lab work, and discussion of risks and benefits. If someone offers to prescribe based solely on a questionnaire with no physician review, find a different provider.
Be wary of providers who do not discuss side effects or monitoring. If your prescriber gives you the medication and says "come back in three months," that is inadequate follow-up for a medication that requires titration and monitoring. You deserve a prescriber who checks in regularly, adjusts doses thoughtfully, and monitors your metabolic markers throughout treatment.
Be skeptical of guaranteed weight loss claims. While GLP-1 medications are remarkably effective, individual responses vary. A provider who promises specific weight loss numbers is overpromising. Good prescribers discuss ranges, set realistic expectations, and emphasize that results depend on medication plus lifestyle modification.
If any provider suggests using GLP-1 medications from non-FDA-approved sources or without proper prescription channels, walk away. The safety considerations around peptide medications are serious, and unregulated products carry real risks including contamination, incorrect dosing, and lack of sterility.
Your appointment day checklist
Print this. Bring it. Check each item off before you leave the house.
Documents to bring:
Insurance card and any pre-authorization reference numbers
Most recent lab results (within 3 months: fasting glucose, HbA1c, lipid panel, liver enzymes, thyroid function)
List of all current medications with dosages
Written weight history with dates, methods tried, and outcomes
Documentation of any weight-related diagnoses (hypertension, prediabetes, sleep apnea, PCOS, etc.)
Printed list of questions (from the section above)
Numbers to know:
Your current BMI (calculate beforehand)
Your highest adult weight and the date
Your target weight or goal BMI range
Duration of your most recent lifestyle intervention
Relevant lab values (A1c, fasting glucose, blood pressure trend)
Phrases to remember:
"I would like to discuss GLP-1 receptor agonists as part of a comprehensive treatment plan"
"My BMI is [number], and I have [comorbidity]. I believe I meet the clinical criteria"
"I have tried [specific methods] for [duration] with [results]"
"I understand the side effect profile and am prepared to manage them"
"Which option would you recommend given my specific health profile and insurance coverage?"
That last phrase is perhaps the most important one in this entire guide. It invites collaboration. It respects your doctor expertise. And it frames you as a partner in treatment planning rather than a consumer making a demand.
For researchers serious about navigating their GLP-1 options with confidence, SeekPeptides provides the most comprehensive educational resource available, with evidence-based guides on every major GLP-1 medication, dosage calculators, comparison tools, and a community of knowledgeable members who have navigated these exact conversations successfully.
Frequently asked questions
Can I specifically request a brand-name GLP-1 medication, or do I have to accept whatever my doctor suggests?
You can absolutely express a preference. Telling your doctor "I have researched tirzepatide and believe it might be the best fit based on the SURMOUNT trial data" is reasonable. However, your doctor may recommend a different option based on your insurance formulary, medical history, or available inventory. The best approach is to state your preference and then ask your doctor to explain if they recommend something different and why.
What if my BMI is slightly under the threshold but I have significant health concerns related to my weight?
Some providers will prescribe GLP-1 medications for patients whose BMI falls slightly below the 27 threshold if there is strong clinical justification. Discuss this honestly with your doctor. If you carry weight primarily in your midsection (visceral adiposity), your metabolic risk may be higher than your BMI suggests. Waist circumference, waist-to-hip ratio, and metabolic health markers can all support a case for treatment even when BMI alone does not quite meet the standard cutoff.
How do I bring up GLP-1 medications without sounding like I just want a quick fix?
Frame the conversation around your health journey rather than a destination. Lead with your history of effort, your specific health concerns, and your understanding of GLP-1 medications as a medical treatment that works alongside lifestyle changes. Saying "I have been working on this for two years and I think it is time to add pharmacological support" carries a very different tone than "I want a weight loss shot." Your preparation and knowledge will speak for themselves.
What should I do if I cannot afford brand-name GLP-1 medications even with insurance?
Discuss all options with your provider including manufacturer savings programs, compounded formulations, and more affordable alternatives. Many compounding pharmacies offer semaglutide and tirzepatide at significantly reduced costs during shortage periods. Some telehealth platforms provide competitive cash-pay pricing. Your doctor can help you evaluate which options maintain appropriate medical oversight while fitting your budget.
Is it appropriate to bring research studies to my appointment?
Yes, but do it tactfully. Bringing a printout of a key clinical trial and saying "I found this study interesting and wanted your perspective on whether it applies to my situation" is respectful and collaborative. Bringing a stack of papers and arguing with your doctor based on your internet research is counterproductive. The goal is to show informed engagement, not to challenge your doctor expertise.
How many appointments will it take before I actually get a prescription?
This varies significantly. Some patients leave their first appointment with a prescription in hand, particularly if they came prepared with documentation and meet clear eligibility criteria. Others require lab work, insurance pre-authorization, and follow-up visits, which can take 2-6 weeks. Prior authorization itself can take anywhere from 24 hours to several weeks depending on your insurance company. Coming to your first appointment fully prepared with documentation and lab work gives you the best chance of a quick start.
Should I mention that I have been researching peptides and GLP-1 medications online?
Yes, frame it positively. "I have been educating myself about GLP-1 receptor agonists through medical literature and reputable health education platforms like SeekPeptides" shows proactive engagement with your health. Avoid mentioning forums where people discuss obtaining medications without prescriptions, as this can make providers uncomfortable. Stick to framing your research as educational and focused on making an informed medical decision.
What if I want to try a GLP-1 for a condition other than weight loss or diabetes?
GLP-1 medications are being studied for an expanding range of conditions including autoimmune conditions, cardiovascular risk reduction, non-alcoholic fatty liver disease, and neurodegenerative diseases. If your interest relates to an off-label indication, discuss this openly with your doctor. Some physicians are comfortable prescribing off-label based on emerging evidence, while others prefer to wait for formal FDA approval. Either way, the conversation starts with your honest disclosure of your goals and your understanding that off-label use may not be covered by insurance.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your conversations stay confident, your prescriptions stay approved, and your health goals stay within reach.